Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Adjunctive Cannabidiol for Drug-Resistant Epilepsy: A Systematic Review and Meta-Analysis of Randomized Trials Across Syndromes, Formulations, and Dose Ranges
Authors Pratama R ![]() , Muhaimin M
, Muhaimin M ![]() , Khairinisa MA
, Khairinisa MA ![]() , Chaerunisaa AY
, Chaerunisaa AY ![]()
Received 2 March 2026
Accepted for publication 11 May 2026
Published 18 May 2026 Volume 2026:22 601774
DOI https://doi.org/10.2147/TCRM.S601774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Reza Pratama,1,2 Muhaimin Muhaimin,3 Miski Aghnia Khairinisa,4 Anis Yohana Chaerunisaa5
1Doctoral Program, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, 45363, Indonesia; 2Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmacy, Universitas Bhakti Kencana, Bandung, 40614, Indonesia; 3Department of Pharmaceutical Biology, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, 45363, Indonesia; 4Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, 45363, Indonesia; 5Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, 45363, Indonesia
Correspondence: Anis Yohana Chaerunisaa, Email [email protected]
Background: Cannabidiol (CBD) has emerged as a promising adjunctive therapy for drug-resistant epilepsy, yet clinical findings remain heterogeneous across trials. This meta-analysis aimed to evaluate the efficacy, safety, and formulation-dependent performance of CBD in patients with treatment-resistant epilepsies.
Methods: A systematic review and meta-analysis were conducted in accordance with PRISMA 2020 guidelines, including randomized, double-blind, placebo-controlled trials of adjunctive CBD in drug-resistant epilepsy. Literature was sourced from PubMed/MEDLINE, Scopus, and the Cochrane Central Register of Controlled Trials (CENTRAL). Data were synthesized using random-effects models to estimate pooled risk ratios (RRs) with 95% confidence intervals (CIs) for seizure reduction and adverse events. Subgroup analyses explored the influence of epilepsy syndrome, CBD dose, and formulation type.
Results: Seven randomized controlled trials involving 1154 participants met inclusion criteria. Adjunctive CBD significantly reduced seizure frequency compared with placebo (pooled RR = 0.72, 95% CI 0.71– 0.73; p < 0.0001). The effect was consistent across Dravet syndrome, Lennox–Gastaut syndrome, and tuberous sclerosis complex, with optimal efficacy observed at 20 mg/kg per day of highly purified oral CBD. Liposomal CBD produced modest benefit, whereas transdermal formulations showed no short-term efficacy. Adverse events were predominantly mild and comparable to placebo, although elevations in hepatic enzymes and somnolence occurred more frequently in patients receiving concomitant valproate or clobazam.
Conclusion: Adjunctive oral CBD provides a reproducible and clinically meaningful reduction in seizures in drug-resistant epilepsy, with an acceptable safety profile. Oral CBD at 20 mg/kg per day represents the current benchmark for efficacy, while alternative formulations require further evaluation. Future research should address long-term outcomes, optimal dosing strategies, and formulation refinement to improve tolerability and accessibility in diverse epileptic populations.
Keywords: cannabidiol, seizure, epilepsy, meta-analysis, randomized controlled trials, oral CBD
Introduction
Epilepsy affects more than 50 million people worldwide and remains one of the most common chronic neurological disorders.1 Although approximately two-thirds of newly diagnosed patients achieve seizure control with current therapies, the remaining one-third continue to experience uncontrolled seizures, leading to drug-resistant or treatment-resistant epilepsy.2 This persistent seizure activity is associated with substantial disability, cognitive decline, and a marked reduction in quality of life.3,4 The need for effective therapies is particularly urgent in severe developmental and epileptic encephalopathies such as Dravet syndrome (DS) and Lennox–Gastaut syndrome (LGS), which are characterized by frequent, pharmacoresistant seizures, cognitive impairment, and high mortality.5–7 Despite the availability of multiple antiseizure medications (ASMs), fewer than 10% of patients with LGS achieve seizure freedom, and the polytherapy required to manage these syndromes often results in intolerable adverse effects.5,8
The limited efficacy and tolerability of conventional ASMs, most of which target neuronal hyperexcitability through a single molecular pathway, have underscored the need for treatments with novel mechanisms of action.8 Cannabidiol (CBD), a non-euphoric phytocannabinoid derived from Cannabis sativa L., has emerged as a promising therapeutic candidate.9,10 Unlike tetrahydrocannabinol (THC), CBD exhibits negligible affinity for classical cannabinoid receptors and therefore lacks psychoactive properties.11 Preclinical and mechanistic studies demonstrate that CBD exerts anticonvulsant, anti-inflammatory, and neuroprotective effects through multiple molecular targets, suggesting a broader therapeutic potential.12–14 Clinical translation of these findings has been substantiated by randomized controlled trials showing that highly purified oral CBD (Epidiolex/Epidyolex) significantly reduces convulsive seizures in DS and drop seizures in LGS, providing high-quality evidence for its efficacy in severe treatment-resistant epilepsies.5–7,15
While randomized controlled trials (RCTs) have established the efficacy of adjunctive cannabidiol (CBD) for treatment-resistant epilepsy, substantial heterogeneity among studies limits the generalizability of their findings. A prior meta-analysis attempted to synthesize this evidence.16 However, one of the included papers was not an independent RCT but a post hoc analysis of two existing trials17 focusing only on the time to onset of seizure reduction and adverse events. Consequently, that analysis did not represent a fully randomized evidence base. The present meta-analysis therefore provides a more rigorous synthesis by including more primary RCT data to evaluate the overall efficacy, safety, and tolerability of adjunctive CBD across epilepsy types. It also examines differences between delivery systems—highly purified oral formulations, liposomal preparations, and transdermal gels—to determine whether alternative routes mitigate first-pass metabolism–related adverse effects such as gastrointestinal events and hepatic enzyme elevations.
Methods
This meta-analysis followed the PRISMA 2020 guidelines and was prospectively registered in the PROSPERO database (Registration No.: CRD420251167897).
Search Strategy
A comprehensive and sequential literature search was conducted across multiple electronic databases, including PubMed/MEDLINE, Scopus, and the Cochrane Central Register of Controlled Trials (CENTRAL) from inception to October 7, 2025. The search identified 62 articles in PubMed/MEDLINE, 5170 articles in Scopus (including 2292 original research articles and 105 labeled as clinical trials), and 184 records in Cochrane CENTRAL. The search strategy used the following keywords and Boolean operators: (cannabidiol OR CBD) AND (epilepsy OR seizure OR epileptic) AND (clinical trial OR randomized controlled trial). No language, country, journal source, and funding restrictions were applied. Additionally, the reference lists of all included studies, along with prior systematic reviews and meta-analyses, were manually screened to identify any relevant trials not captured in the electronic search.
Eligibility Criteria
The research question was structured using the PICO (Population, Intervention, Comparator, Outcome) model. Specifically, the analysis targeted: P: patients diagnosed with treatment- or drug-resistant epilepsy; I: adjunctive treatment with cannabidiol (CBD) in any standardized formulation; C: placebo administered under comparable trial conditions; and O: reduction in seizure frequency as the primary efficacy outcome, with adverse event incidence as a key safety outcome.
Participants were included if the study was a randomized, double-blind, or triple-blind, placebo-controlled clinical trial involving human subjects diagnosed with drug-resistant or treatment-resistant epilepsy. Eligible patients must have failed to achieve adequate seizure control with at least two appropriately chosen and tolerated antiseizure medications (ASMs), either used sequentially or in combination. The intervention had to involve cannabidiol (CBD) administered as an adjunctive (add-on) therapy in any standardized formulation, including oral solution, liposomal, or transdermal preparations, with a placebo serving as the comparator.
Concomitant ASMs and nonpharmacologic interventions such as the ketogenic diet or vagus nerve stimulation were required to remain stable for at least four weeks before baseline assessment or randomization. Studies were eligible when participants exhibited a minimum baseline seizure frequency during the observation period, defined as ≥4 convulsive seizures per 28 days for Dravet syndrome, ≥2 drop seizures per week for Lennox–Gastaut syndrome, ≥8 seizures over a 4-week baseline for tuberous sclerosis complex (TSC), or at least one seizure per month for focal or frontal lobe epilepsy. The primary efficacy outcome was required to be clinical seizure frequency to allow for consistent quantitative synthesis across studies.
Studies were excluded if they were nonclinical investigations, including animal experiments or in vitro studies, or if they focused on nonpharmacological or nontherapeutic outcomes, such as cost-effectiveness analyses, pharmacokinetic evaluations, or drug–drug interaction studies. Trials were also excluded if they employed observational or uncontrolled designs, including cohort studies, open-label or single-arm trials, pilot studies, case series, or case reports. Additionally, studies that did not use cannabidiol (CBD) as the primary intervention, lacked a placebo or active control group, or failed to report quantitative seizure outcomes were excluded.
Research Questions
This meta-analysis addresses both primary and subgroup research questions derived from randomized controlled trials investigating adjunctive cannabidiol (CBD) therapy in treatment-resistant epilepsy.
The primary research questions are as follows:
- What is the overall efficacy of adjunctive CBD, across all epilepsy syndromes, compared with placebo in reducing the frequency of countable seizures (convulsive, drop, or TSC-associated) during the treatment period?
- What are the comparative incidences of the most common treatment-emergent adverse events associated with cannabidiol compared with placebo across randomized controlled trials?
The subgroup research questions focus on potential sources of heterogeneity:
- Does the magnitude of seizure reduction differ between patients with developmental and epileptic encephalopathies (eg, Dravet syndrome, Lennox–Gastaut syndrome) and those with focal seizure syndromes (eg, tuberous sclerosis complex, focal/frontal lobe epilepsy)?
- Does evidence from randomized controlled trials support 20 mg/kg/day as the optimal and clinically meaningful benchmark dose of oral cannabidiol for treatment-resistant epilepsy?
- Does the formulation of cannabidiol (CBD) into specific dosage forms enhance its efficacy compared to the pure compound in patients with treatment-resistant epilepsy?
These research questions collectively aim to define the therapeutic efficacy and safety profile of CBD across epilepsy syndromes, dosing strategies, concomitant medication contexts, and formulation types.
Data Extraction
Data extraction was performed independently and in duplicate by two reviewers (Reza Pratama and Muhaimin) using a standardized form adapted from the Cochrane Handbook for Systematic Reviews of Interventions. The extraction form was piloted on a sample of studies to ensure consistency and clarity before full data collection. Extracted variables included study characteristics (author, year, country, design, and sample size), participant characteristics, epilepsy type, cannabidiol (CBD) formulation and dosage, treatment duration, comparator, primary and secondary outcomes, and reported adverse events. All data were recorded in Microsoft Excel and cross-checked by the reviewers. Discrepancies were documented and resolved through discussion, and any unresolved differences were adjudicated by a senior reviewer (Anis Yohana Chaerunisaa).
Risk of Bias Assessment
The risk of bias for each included randomized controlled trial was evaluated using the Cochrane Risk of Bias Tool implemented in Review Manager (RevMan version 5.4; The Cochrane Collaboration, London, UK). The assessment covered seven domains: random sequence generation and allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other potential sources of bias. Each domain was rated as low, uncertain, or high risk of bias. The overall risk-of-bias judgments were summarized and visualized using traffic light plots generated in RevMan. Additional quantitative assessments of bias, including publication bias evaluation, are described in the Statistical Analysis section.
Statistical Analysis
Effect sizes were synthesized using a random-effects model based on the DerSimonian–Laird method to account for potential between-study variability. For continuous outcomes, pooled estimates were expressed as mean difference (MD) or standardized mean difference (SMD), whereas dichotomous outcomes were summarized using risk ratios (RRs) with corresponding 95% confidence intervals (CIs). Statistical heterogeneity among studies was evaluated using Cochran’s Q test (with p < 0.10 considered statistically significant) and quantified using the I2 statistic, with values of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. Publication bias was assessed through visual inspection of funnel plot asymmetry in Review Manager and further evaluated using Egger’s regression test implemented in the metafor package in R (version 4.2.1, 2025-06-13 ucrt; RStudio Inc., Boston, MA, USA). Post hoc Tukey analyses were performed to compare the percentage reduction in seizure frequency across different cannabidiol (CBD) formulations and epilepsy syndrome types.
Leave One Out Analysis
Influence of individual studies was examined using leave-one-out sensitivity analyses, repeating the meta-analysis after removing each study in turn and recalculating pooled RRs, 95% CIs, and heterogeneity statistics (τ2 and I2). Stability was defined as preservation of direction and broadly similar magnitude of effect across iterations, and results were considered when interpreting heterogeneity and certainty of evidence.
Results
Study Selection
A total of 5416 records were identified through database searching, including PubMed (n = 62), Scopus (n = 5170), and Cochrane Central (n = 184). After sequential screening and removal of irrelevant records, 35 full-text articles were assessed for eligibility. Of these, 29 were excluded because they were non-randomized designs (eg, open-label, post hoc, or cohort studies) or focused primarily on pharmacokinetics and safety rather than efficacy. An additional 10 unique clinical trial records were retrieved from Scopus, of which 9 were excluded for not being seizure-focused or not meeting randomized controlled trial criteria. Ultimately, 7 randomized controlled trials met the inclusion criteria and were incorporated into the final quantitative synthesis (Figure 1).
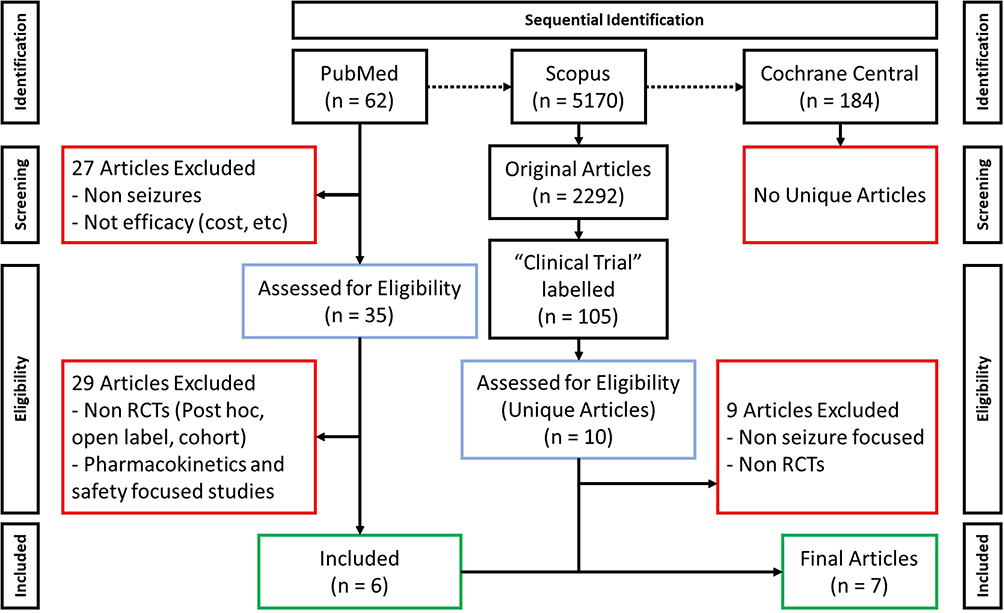 |
Figure 1 PRISMA-style flow diagram of study selection for inclusion in the meta-analysis using a sequential searching method. Boxes with red borders indicate excluded articles, blue borders represent articles assessed for eligibility, and green borders denote articles included in the final analysis. |
Study Characteristics
A total of seven randomized controlled trials (RCTs) comprising 1154 participants were included in the meta-analysis. The studies were published between 2017 and 2023 and collectively evaluated the efficacy of cannabidiol (CBD) as an adjunctive therapy in patients with various forms of drug-resistant epilepsy, including Dravet syndrome, Lennox–Gastaut syndrome (LGS), tuberous sclerosis complex (TSC), and focal seizure syndromes. Participants ranged in age from 1 to 70 years, encompassing both pediatric and adult populations. Summary of included randomized controlled trials can be seen in Table 1.
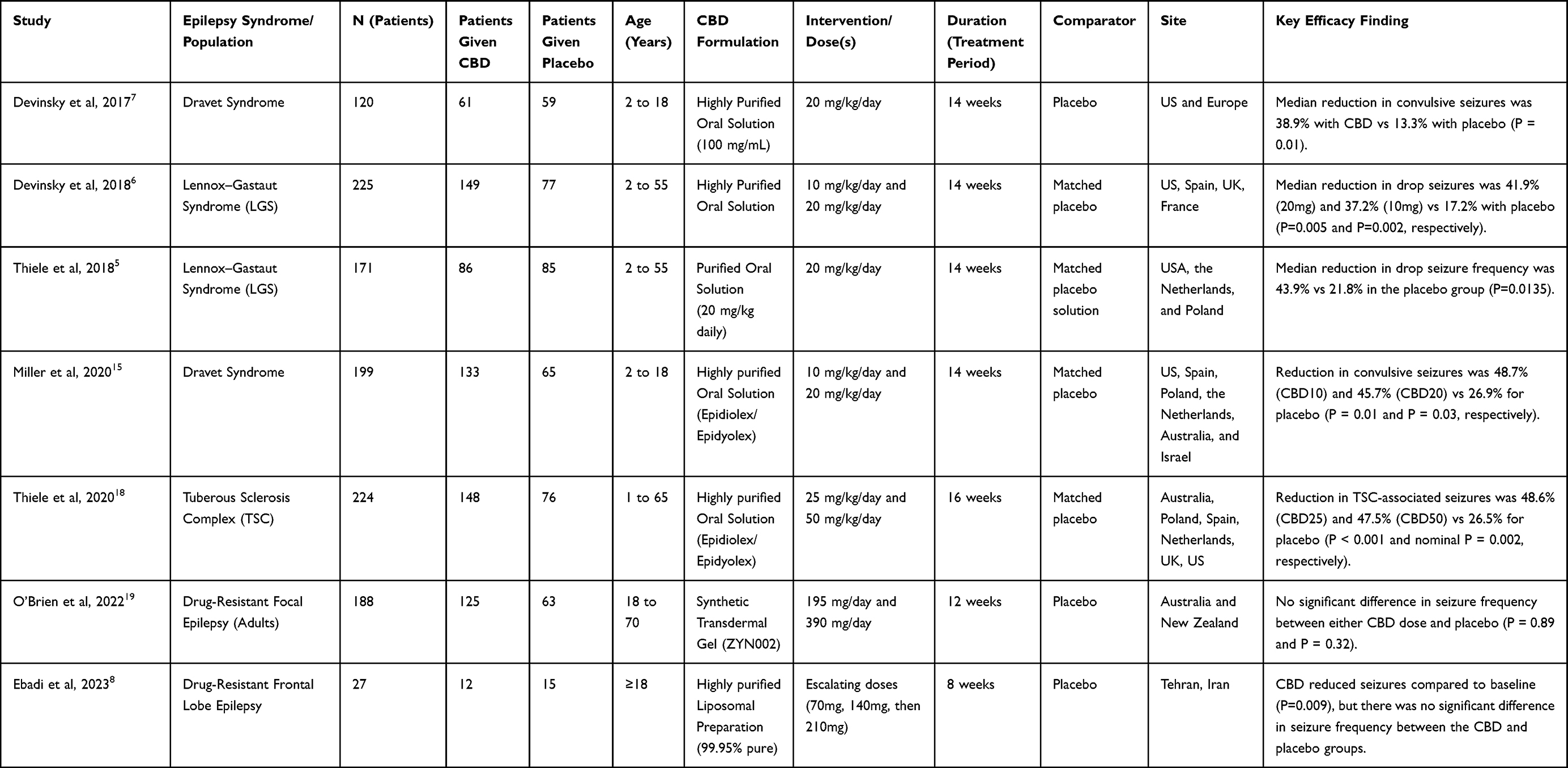 |
Table 1 Overview of Randomized Controlled Trials of Cannabidiol (CBD) for Treatment-Resistant Epilepsy |
Risk of Bias
Several of the included trials were industry-sponsored, raising potential financial conflicts of interest. Both Devinsky et al and Thiele et al were funded by GW Pharmaceuticals, which manufactured and supplied the study drug and employed several of the authors. Similarly, Miller et al and Thiele et al were supported and managed by GW Research Ltd., a subsidiary of GW Pharmaceuticals, with the sponsor actively involved in study design, data analysis, and manuscript preparation. O’Brien et al was funded by Zynerba Pharmaceuticals, Inc., which produced the transdermal cannabidiol formulation and provided financial support or employment to several investigators. In addition, Ebadi et al enrolled a relatively small sample (N = 27), limiting the precision of its effect estimates and increasing the risk of baseline imbalance. These studies were therefore classified as having a high risk of “other bias” according to the Cochrane Risk of Bias 2.0 framework.
Funnel plot inspection revealed a symmetrical distribution of study effect sizes around the pooled risk ratio (Figure 2), indicating no visual evidence of publication bias. Both large and small studies were evenly distributed on either side of the overall effect estimate, and no conspicuous asymmetry or outliers were observed. This pattern suggests that the likelihood of selective publication of positive cannabidiol trials is low. Consistent with the visual assessment, Egger’s regression test did not indicate significant funnel plot asymmetry (p > 0.05), further supporting the absence of small-study or publication bias.
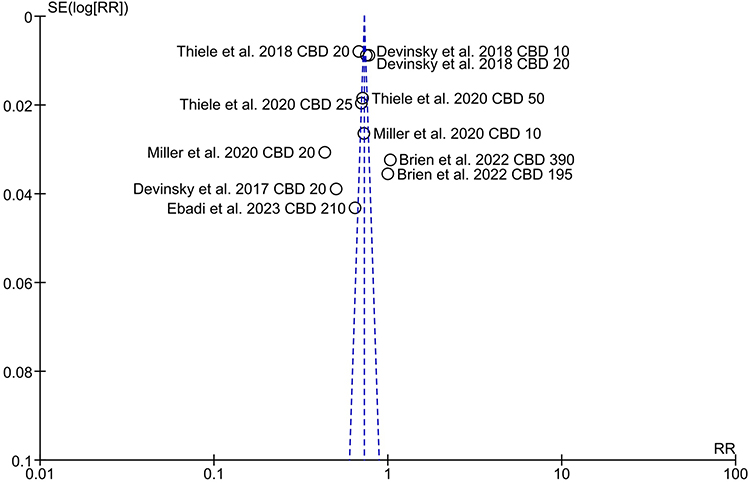 |
Figure 2 Funnel plot of the included randomized controlled trials assessing the efficacy of oral cannabidiol (CBD) for seizure reduction. |
Effectivity of Cannabinoid and Its Formulation
A comprehensive pooled analysis of all eligible randomized controlled trials demonstrated a significant reduction in seizure frequency among patients receiving adjunctive cannabidiol (CBD) compared with placebo (pooled risk ratio [RR] = 0.72, 95% confidence interval [CI] 0.71–0.73; P < 0.0001; Figure 3). Across seven treatment arms encompassing 1154 participants (CBD = 714; placebo = 440), CBD therapy was associated with an approximate 28% relative reduction in seizure occurrence. This consistent benefit was observed across a range of doses (10–50 mg/kg/day) and epilepsy syndromes, including Dravet syndrome, Lennox–Gastaut syndrome (LGS), and focal seizure syndromes. In Dravet syndrome, pooled data from three trials (Devinsky et al, 2017; Miller et al, 2020) indicated a more pronounced effect (RR = 0.57, 95% CI 0.55–0.59; P < 0.00001), corresponding to an estimated 43% reduction in seizure frequency, with the highest efficacy at 20 mg/kg/day. Similarly, in LGS, studies by Devinsky et al and Thiele et al reported a pooled RR of 0.73 (95% CI 0.73–0.74; P < 0.00001), suggesting a 27% decrease relative to placebo. Although heterogeneity was substantial across analyses (I2 ≈ 99%), the uniform direction of effect suggests that clinical diversity—rather than inconsistency in therapeutic response—accounts for the dispersion observed.
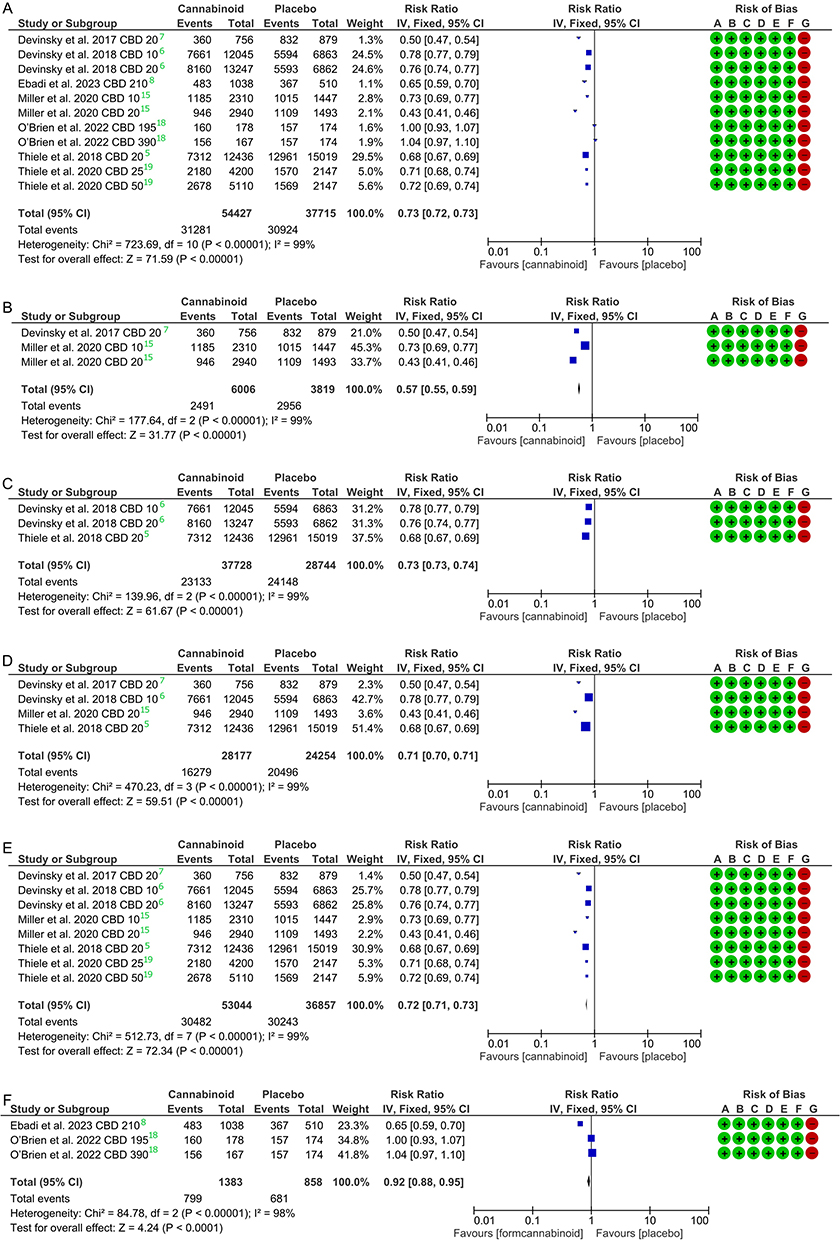 |
Figure 3 Pooled effect of adjunctive cannabidiol (CBD) on seizure event reduction in pharmacoresistant epilepsy. (A) All included randomized controlled trials; (B) subgroup analysis for Dravet syndrome; (C) subgroup analysis for Lennox–Gastaut syndrome; (D) trials using a 20 mg/kg/day CBD dose; (E) studies evaluating the oral CBD solution; and (F) subgroup analysis for Focal Seizure syndrome and studies assessing formulated (liposomal or transdermal) CBD preparations. Risk of bias for each included study is summarized on the right. |
When analyses were restricted to studies administering the standardized 20 mg/kg/day oral CBD solution, results remained robust, with a pooled RR of 0.72 (95% CI 0.71–0.73; P < 0.00001). This convergence of efficacy across diverse epileptic populations underscores the reproducibility of CBD’s therapeutic signal and positions 20 mg/kg/day as a clinically meaningful benchmark dose. In focal seizure syndromes—including tuberous sclerosis complex and focal or frontal lobe epilepsy—the combined effect across oral, liposomal, and transdermal formulations produced a modest yet statistically significant reduction in seizure events (RR = 0.92, 95% CI 0.88–0.95; P < 0.00001). However, the benefit was formulation-dependent: liposomal CBD (Ebadi et al, 2023) demonstrated a clear therapeutic advantage (RR = 0.65, 95% CI 0.59–0.70), whereas transdermal preparations (O’Brien et al, 2022) showed near-null effects (RR ≈ 1.0), likely reflecting lower systemic bioavailability. Despite the high statistical heterogeneity (I2 ≈ 98–99%), the collective evidence supports the consistent clinical efficacy of purified oral CBD as an adjunctive treatment for drug-resistant epilepsy, while highlighting formulation and pharmacokinetic factors as key modulators of therapeutic response.
Post hoc Tukey analysis was performed to compare the percentage reduction in seizure frequency across different formulations and epilepsy syndromes. The analysis confirmed that there were no statistically significant differences in efficacy between the oral solution, liposomal, and transdermal groups, nor between the investigated epilepsy syndromes (all p > 0.05). These findings suggest that CBD generally exerts a consistent therapeutic effect across the tested epilepsy syndromes, regardless of the specific formulation used.
Sensitivity analysis using the leave-one-out method confirmed that the pooled effect estimate (RR 0.71) is robust and consistent. No single study significantly altered the direction or magnitude of these clinical findings (see Figure 4). Although the heterogeneity was found to be very high (I2 > 98%), the stability of the RR values upon individual study omission indicates that the meta-analysis results are reliable, though interpretation should be exercised with caution given the persistent inter-study variation.
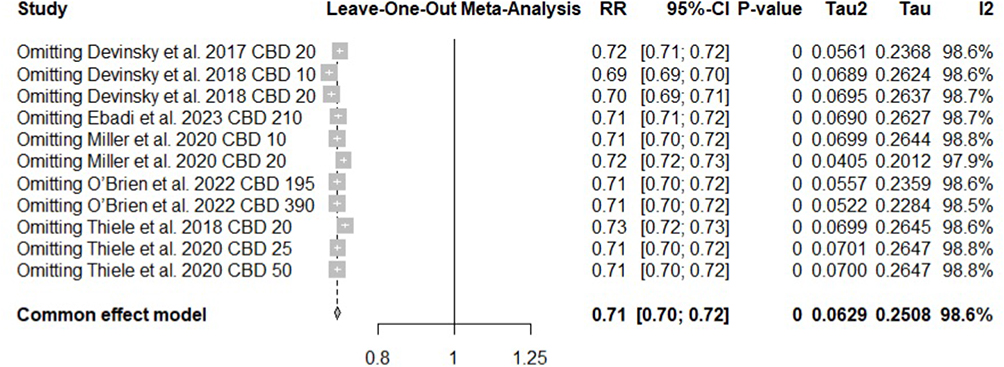 |
Figure 4 Sensitivity analysis using leave-one-out method. The results remain consistent (mean RR 0.71), confirming that no single study dominates the overall finding. |
Main Side Effects of Cannabinoid
Across all included trials, the most frequently reported adverse events associated with cannabidiol were mild and occurred at rates comparable to placebo. Appetite loss showed a slightly higher incidence in the cannabidiol group, though the difference was not statistically significant (RR = 1.02, 95% CI 0.85–1.22; p = 0.81). Similarly, diarrhea occurred with nearly identical frequency between groups (RR = 1.03, 95% CI 0.89–1.20; p = 0.68), while rates of somnolence were virtually indistinguishable (RR = 1.00, 95% CI 0.86–1.17; p = 0.98). No heterogeneity was detected in any of these analyses (I2 = 0% for all), suggesting consistent findings across study designs, populations, and cannabidiol doses. Although the direction of effect for appetite loss and diarrhea slightly favored placebo, the magnitudes were clinically negligible (Figure 5).
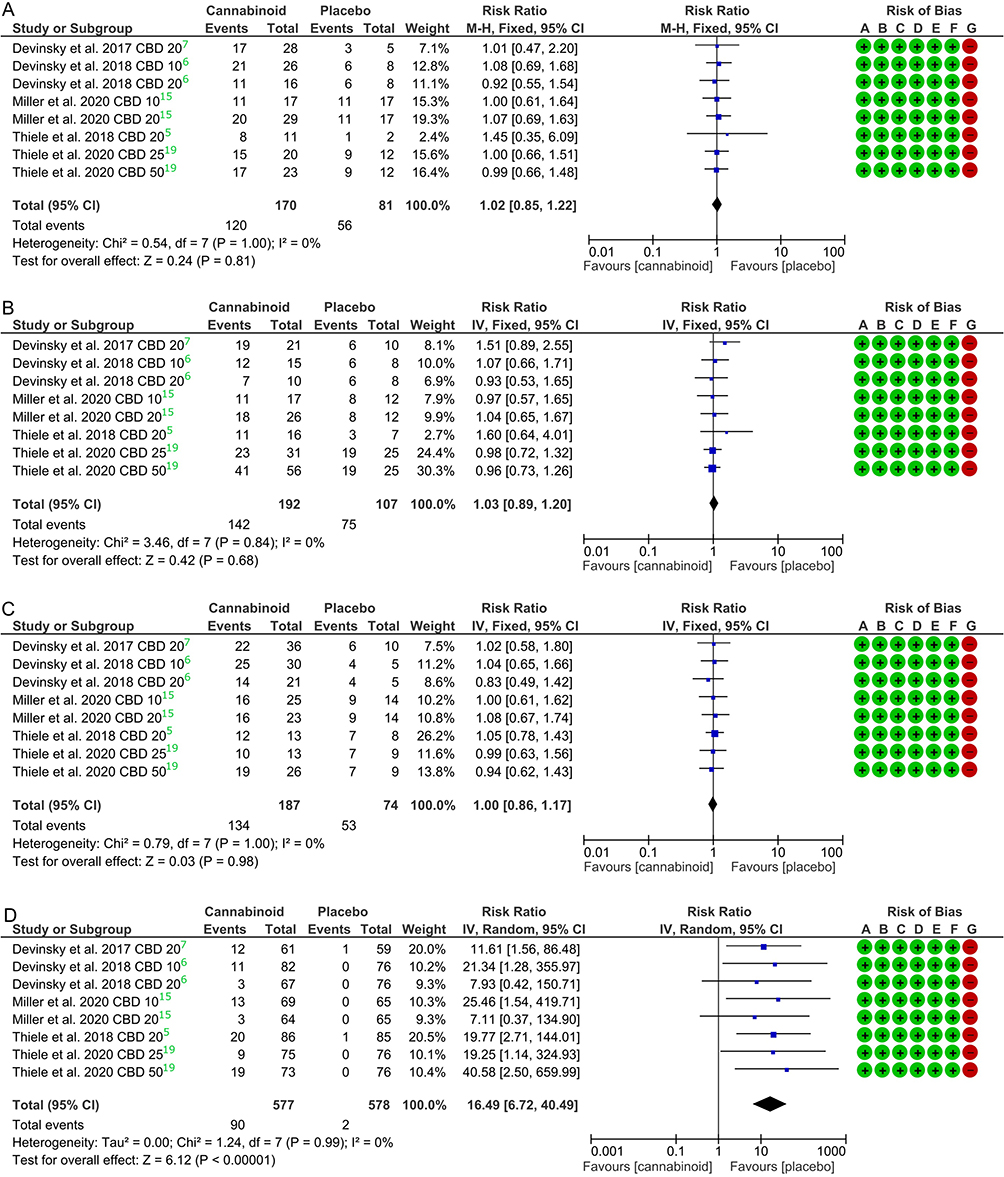 |
Figure 5 Pooled effects of adjunctive cannabidiol (CBD) on common adverse events. Forest plots showing the pooled risk ratios (RR) for (A) decreased appetite, (B) diarrhea, (C) somnolence, and (D) liver enzyme elevation (specifically aminotransferase levels >3 times the upper limit of normal) events among participants receiving adjunctive CBD compared with placebo. No significant differences were observed between the CBD and placebo groups across all adverse events. Risk of bias for each included study is summarized on the right. |
Post hoc Tukey analysis was performed to compare the incidence rates among the most frequently reported adverse events within the cannabidiol group. The analysis showed no statistically significant difference in the occurrence rates between appetite loss, diarrhea, and somnolence (p > 0.05). This indicates that no single adverse event was significantly more dominant than the others, suggesting a relatively uniform distribution of these primary side effects.
Discussion
The pivotal data derived from multiple randomized, double-blind, placebo-controlled trials represent a critical advancement in the management of drug-resistant epilepsies, confirming the efficacy and characterizing the safety profile of highly purified cannabidiol (CBD) as an adjunctive treatment.6,7,15,19 These analyses collectively substantiate the therapeutic role of CBD in specific developmental and epileptic encephalopathies (DEEs) and highly refractory epilepsy syndromes, while also highlighting nuanced findings in broader focal epilepsies.
Efficacy Profile Across Drug-Resistant Syndromes
CBD demonstrated significant and clinically meaningful reductions in seizure frequency across three severe DEEs: Dravet Syndrome (DS), Lennox–Gastaut Syndrome (LGS), and Tuberous Sclerosis Complex (TSC).5–7,18 These patient populations were notably treatment-resistant, often having failed multiple previous anti-epileptic drugs (AEDs) (median of four to six previous AEDs tried) and receiving regimens including multiple concomitant AEDs.
In DS, the addition of 20 mg/kg/day CBD resulted in a significantly greater reduction in convulsive seizure frequency than placebo.7 A dose-ranging study (GWPCARE2) subsequently confirmed that both 10 mg/kg/day and 20 mg/kg/day doses were similarly effective, resulting in percentage reductions in convulsive seizure frequency of 48.7% and 45.7%, respectively, compared to 26.9% for placebo.6
Similarly, for LGS, multiple Phase 3 trials demonstrated robust efficacy against drop seizures (atonic, tonic, or tonic-clonic seizures that lead to a fall or slumping).5,6 GWPCARE3, comparing 10 mg/kg/day and 20 mg/kg/day, found median reductions of 37.2% and 41.9%, respectively, versus 17.2% for placebo, with both active doses showing significant improvement.6 GWPCARE4, utilizing a 20 mg/kg/day dose, reported a 43.9% median reduction in monthly drop seizure frequency compared to 21.8% in the placebo group.5 The percentage of patients achieving a ≥50% reduction in drop seizures in LGS ranged from 36% to 44% in the CBD groups across trials, consistently exceeding the placebo rate (22% to 27%).5,6,18
In TSC, which is characterized by primarily focal seizures, add-on CBD (25 mg/kg/day or 50 mg/kg/day) significantly reduced TSC-associated seizures by approximately 48% compared to a 26.5% reduction in the placebo group.18 Importantly, the treatment effect, across DS, LGS, and TSC trials, was often observed early during the 14-week treatment period (sometimes during the initial 4 weeks of maintenance phase) and maintained throughout the study duration.5,7,15,18
Comparative Efficacy and Alternative Delivery
Comparative dosing across the DEE studies consistently indicated that higher doses (20 mg/kg/day in DS/LGS, 50 mg/kg/day in TSC) offered no appreciable increase in efficacy over the lower tested doses (10 mg/kg/day in DS/LGS, 25 mg/kg/day in TSC) but were associated with a less favorable safety profile.15,18 This suggests that dose escalation above 10 mg/kg/day for DS/LGS or 25 mg/kg/day for TSC should be tailored to individual efficacy and tolerability. The effect was also more consistent in DS than in other forms of epilepsy (Figure 6).
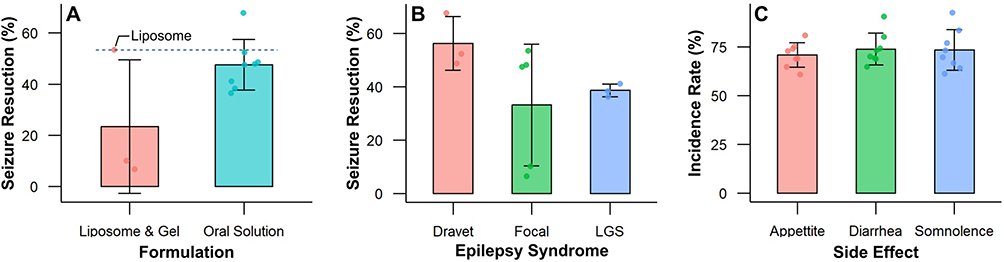 |
Figure 6 Comparative efficacy and safety outcomes of cannabidiol (CBD) formulations and epilepsy syndromes. (A) Pooled seizure reduction rates across CBD formulations. (B) Mean seizure reduction by epilepsy syndrome. (C) Incidence rates of the three most common treatment-emergent adverse events. No statistically significant differences were observed among the groups (p > 0.05). |
For focal epilepsies outside of the specific syndromes, the evidence is mixed and heavily influenced by the preparation and delivery method investigated. A trial using a highly pure liposomal preparation of CBD in drug-resistant frontal lobe epilepsy (FLE) patients (a highly refractory subtype) found that CBD was effective in significantly reducing seizure occurrence at the final 8-week timepoint compared to baseline, which was not observed in the placebo group.8 Furthermore, QoL was significantly improved in the CBD group at 8 weeks.
Conversely, a trial investigating transdermal CBD delivery (195 mg or 390 mg/day) in adults with general drug-resistant focal epilepsy found no significant difference in total seizure frequency compared to placebo during the 12-week double-blind period19 Researchers hypothesize that this lack of effect might be due to lower effective dosing, the time needed for onset of effect, or differences in the patient population. However, the median percentage reduction in seizures in the open-label extension of the transdermal study reached 50% by month six, suggesting long-term efficacy may warrant further investigation with higher doses.
Safety, Tolerability, and Drug-Drug Interactions
Oral CBD was generally well tolerated, although associated with higher rates of adverse events (AEs) than placebo, often leading to trial withdrawal.5–7,15,18 Common treatment-emergent AEs included diarrhea, somnolence, decreased appetite, vomiting, pyrexia, and fatigue.
A critical and consistently reported safety concern is the elevation of liver aminotransferase enzymes (ALT or AST levels >3 times the upper limit of normal), an event that occurred in 9% to 26% of patients receiving oral CBD in the dose-ranging groups, but rarely or never in the placebo groups.5–7,15,18 This hepatotoxicity risk was significantly higher in patients taking concomitant valproate. This drug-drug interaction appears to be pharmacodynamic rather than pharmacokinetic, as CBD does not significantly alter systemic valproate plasma levels.6,15 All cases of elevated liver enzymes eventually resolved, either spontaneously, after CBD tapering/discontinuation, or following reduction of concomitant AEDs (usually valproate), and no patients met Hy’s law criteria for severe drug-induced liver injury.5–7,15,18
Another notable interaction involves clobazam, a common concomitant AED (used by 49% to 65% of patients across trials).5–7,15,18 CBD inhibits CYP2C19, resulting in increased exposure to clobazam’s active metabolite, N-desmethylclobazam, which likely contributes to CNS AEs such as somnolence. Somnolence rates were markedly higher when CBD was co-administered with clobazam. Although this interaction exists, efficacy appears largely independent of clobazam use, although the effect may be enhanced by its presence.15,18
Interestingly, the transdermal CBD trial reported substantially better tolerability, with fewer gastrointestinal side effects (eg, diarrhea 4% vs 31% with oral solution) and no abnormal liver enzyme AEs over 18 months, suggesting the transdermal route might bypass certain metabolic pathways associated with hepatotoxicity.19
The substantial statistical heterogeneity observed (I2 ≈ 99%) primarily stems from the vast range of baseline seizure frequencies across participants, a common occurrence in pediatric and drug-resistant epilepsy populations where monthly seizure counts can vary from single digits to hundreds. To mitigate this, a random-effects model was employed to provide a conservative estimate of the treatment effect. Despite the high I2 value, the consistency in the direction of the effect across all subgroups, regardless of syndrome or formulation, suggests that the findings possess strong clinical validity, even amidst significant numerical dispersion.
Functional and Quality of Life Outcomes
Beyond objective seizure reduction, the perceived clinical relevance of CBD treatment was consistently positive as assessed by the Caregiver Global Impression of Change (CGIC) scale.5–7,15,18 Caregivers reported that the patient’s overall condition improved in significantly higher proportions in the CBD groups across DS (62% vs 34% placebo)7 and LGS (57% to 66% vs 34% to 44% placebo).5 In the FLE study, CBD treatment led to significant improvement in Quality of Life (QoL) scores at 8 weeks.8 Intriguingly, in the CBD group specifically in the FLE study, QoL improvement was not correlated with reduction in seizure frequency or severity, suggesting CBD may convey multimodal benefits independent of seizure control alone.8 However, general QoL scales (Quality of Life in Childhood Epilepsy questionnaire and Vineland-II scores) in the large DS and LGS trials often showed no significant difference between treatment groups.7,15
Limitations and Directions for Future Research
The robustness of these findings is challenged by inherent limitations characteristic of epilepsy trials in highly drug-resistant populations. The pervasive use of multiple concomitant AEDs (polypharmacy) necessitates ongoing vigilance regarding complex drug-drug interactions, particularly with valproate and clobazam.15,18,19 The long-term efficacy and safety of CBD beyond the initial treatment periods (14–16 weeks) remain a crucial area for investigation, currently addressed through open-label extension studies.5,7,15,18,19 Furthermore, trial populations were predominantly composed of white patients and children/adolescents, limiting generalizability to other ethnic groups and the adult population (except for the focal epilepsy trials).5,7,15,19 Future research should focus on optimizing dosing, particularly evaluating doses lower than 10 mg/kg/day, and continuing to explore alternative formulations like liposomal or targeted delivery. Finally, investigating the molecular targets of CBD—including its potential anti-inflammatory and neuroprotective actions—may help define its mechanism beyond seizure control and account for the perceived non-seizure-related improvements reported by caregivers.
A significant consideration in interpreting these findings is the concentration of industry sponsorship within the current evidence base. Five of the seven trials included in this meta-analysis were funded or managed by the manufacturers of the investigated CBD products (GW Pharmaceuticals/Jazz Pharmaceuticals and Zynerba Pharmaceuticals). While these studies followed rigorous randomized controlled protocols, the involvement of sponsors in study design, data analysis, and manuscript preparation introduces a risk of “other bias” that may impact the perceived strength of the evidence. This heavy reliance on industry-funded data may limit the generalizability of the results to broader clinical settings where such high-level institutional support and specific product formulations might not be present. Consequently, there is an urgent need for large-scale, independent (non-industry) replication studies.
Conclusions
In this systematic review and meta-analysis of randomized controlled trials, adjunctive cannabidiol (CBD) demonstrated reproducible and clinically meaningful efficacy in reducing seizure frequency among patients with treatment-resistant epilepsy, particularly in Dravet syndrome, Lennox–Gastaut syndrome, and tuberous sclerosis complex. The therapeutic effect was most consistently observed with highly purified oral CBD at 20 mg/kg per day, confirming this formulation and dose as a benchmark standard in resistant epileptic encephalopathies. Adverse events were generally mild to moderate and manageable, with liver enzyme elevations and somnolence confined mainly to patients receiving concomitant valproate or clobazam. While liposomal preparations showed potential benefit and transdermal delivery yielded limited efficacy, these alternative formulations remain investigational. Based on these findings, the evidence supports adjunctive oral CBD as a validated and mechanistically distinct therapy for refractory epilepsy. Future trials should focus on long-term safety, optimal dosing thresholds, and comparative performance of emerging delivery systems to refine its role in clinical practice.
Acknowledgment
This publication charge is funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025). ChatGPT was used to assist with writing. No AI was used in the creation of images, tables, or data.
Funding
The APC is funded by Universitas Padjadjaran through the EQUITY Program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Beghi E, Giussani G, Nichols E, et al. Global, regional, and national burden of epilepsy, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(4):357–14. doi:10.1016/S1474-4422(18)30454-X
2. Panebianco M, Bresnahan R, Marson AG. Pregabalin add-on for drug-resistant focal epilepsy. Cochrane Database Syst Rev. 2022;2022(4). doi:10.1002/14651858.CD005612.pub5
3. Rosenberg EC, Louik J, Conway E, Devinsky O, Friedman D. Quality of Life in Childhood Epilepsy in pediatric patients enrolled in a prospective, open‐label clinical study with cannabidiol. Epilepsia. 2017;58(8). doi:10.1111/epi.13815
4. Gaston TE, Szaflarski M, Hansen B, Bebin EM, Szaflarski JP. Quality of life in adults enrolled in an open-label study of cannabidiol (CBD) for treatment-resistant epilepsy. Epilepsy Behav. 2019;95:10–17. doi:10.1016/j.yebeh.2019.03.035
5. Thiele EA, Marsh ED, French JA, et al. Cannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391(10125):1085–1096. doi:10.1016/S0140-6736(18)30136-3
6. Devinsky O, Patel AD, Cross JH, et al. Effect of cannabidiol on drop seizures in the Lennox–Gastaut syndrome. N Engl J Med. 2018;378(20):1888–1897. doi:10.1056/nejmoa1714631
7. Devinsky O, Cross JH, Laux L, et al. Trial of cannabidiol for drug-resistant seizures in the Dravet syndrome. N Engl J Med. 2017;376(21):2011–2020. doi:10.1056/nejmoa1611618
8. Ebadi SR, Saleki K, Adl Parvar T, et al. The effect of cannabidiol on seizure features and quality of life in drug-resistant frontal lobe epilepsy patients: a triple-blind controlled trial. Front Neurol. 2023;14. doi:10.3389/fneur.2023.1143783
9. Tihăuan BM, Onisei T, Slootweg W, Gună D, Iliescu C, Chifiriuc MC. Cannabidiol—A friend or a foe? Eur J Pharm Sci. 2025;208:107036. doi:10.1016/j.ejps.2025.107036
10. Cassano T, Villani R, Pace L, et al. From Cannabis sativa to cannabidiol: promising therapeutic candidate for the treatment of neurodegenerative diseases. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.00124
11. Gertsch J, Pertwee RG, Di Marzo V. Phytocannabinoids beyond the Cannabis plant – do they exist? Br J Pharmacol. 2010;160(3):523–529. doi:10.1111/j.1476-5381.2010.00745.x
12. Manzoni OJ, Manduca A, Trezza V. Therapeutic potential of cannabidiol polypharmacology in neuropsychiatric disorders. Trends Pharmacol Sci. 2025;46(2):145–162. doi:10.1016/j.tips.2024.12.005
13. Cásedas G, Yarza-Sancho MD, López V. Cannabidiol (CBD): a systematic review of clinical and preclinical evidence in the treatment of pain. Pharmaceuticals. 2024;17(11):1438. doi:10.3390/ph17111438
14. Silvestro S, Schepici G, Bramanti P, Mazzon E. Molecular targets of cannabidiol in experimental models of neurological disease. Molecules. 2020;25(21):5186. doi:10.3390/molecules25215186
15. Miller I, Scheffer IE, Gunning B, et al. Dose-ranging effect of adjunctive oral cannabidiol vs placebo on convulsive seizure frequency in dravet syndrome: a randomized clinical trial. JAMA Neurol. 2020;77:613–621. doi:10.1001/jamaneurol.2020.0073
16. de Oliveira VG, de Almeida NB, Radmann GC, de Oliveira Santos BF. The efficacy of cannabidiol for seizures reduction in pharmacoresistant epilepsy: a systematic review and meta-analysis. Acta Epileptol. 2025;7(1):20. doi:10.1186/s42494-024-00191-2
17. Privitera M, Bhathal H, Wong M, et al. Time to onset of cannabidiol (CBD) treatment effect in Lennox–Gastaut syndrome: analysis from two randomized controlled trials. Epilepsia. 2021;62(5):1130–1140. doi:10.1111/epi.16878
18. Thiele EA, Bebin EM, Bhathal H, et al. Add-on cannabidiol treatment for drug-resistant seizures in tuberous sclerosis complex: a placebo-controlled randomized clinical trial. JAMA Neurol. 2021;78(3):285–292. doi:10.1001/jamaneurol.2020.4607
19. O’Brien TJ, Berkovic SF, French JA, et al. Adjunctive transdermal cannabidiol for adults with focal epilepsy: a randomized clinical trial. JAMA Network Open. 2022;5(7):E2220189. doi:10.1001/jamanetworkopen.2022.20189
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anticonvulsant Activity of Hydro Alcoholic Extract and Solvent Fractions of Biophytum umbraculum Welw. Syn (Oxalidaceae) Root in Mice
Fisseha N, Hammeso WW, Nureye D
Journal of Experimental Pharmacology 2022, 14:291-299
Published Date: 20 October 2022
Anti-Convulsant Activity of Soxhlet Leaf Extracts of Ajuga Integrifolia Buch.-Ham. Ex D.Don (Lamiaceae) in Mice
Desalegn T, Engidawork E
Journal of Experimental Pharmacology 2023, 15:241-253
Published Date: 30 May 2023
Clinical Characteristics, Treatment Outcome and Associated Factors of Epilepsy Among Children at Hospitals of North-West Ethiopia
Nasir M, Abebaw E, Ahmed M, Ketema DB
Pediatric Health, Medicine and Therapeutics 2023, 14:385-404
Published Date: 31 October 2023
Lack of Efficacy of Simvastatin Adjunctive Therapy for Patients with Schizophrenia: A Meta-Analysis of Randomized Controlled Trials
Chen J, Yuan Y, Hu Y, Liang L
Neuropsychiatric Disease and Treatment 2024, 20:1667-1675
Published Date: 6 September 2024
Efficacy of Cognitive Behavioral Therapy for Kinesiophobia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Zhu S, Xu Y, Wang L, Chen J, Luo A
Journal of Pain Research 2025, 18:3919-3932
Published Date: 6 August 2025