Back to Journals » Journal of Pain Research » Volume 18
Efficacy of Cognitive Behavioral Therapy for Kinesiophobia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Authors Zhu S ![]() , Xu Y, Wang L, Chen J, Luo A
, Xu Y, Wang L, Chen J, Luo A
Received 12 March 2025
Accepted for publication 12 July 2025
Published 6 August 2025 Volume 2025:18 Pages 3919—3932
DOI https://doi.org/10.2147/JPR.S526179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Shuyi Zhu,1 Yanxin Xu,1 Lin Wang,2 Jing Chen,1 Aoxiang Luo1
1School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong, 510310, People’s Republic of China; 2Department of Spinal Orthopedics, Guangdong Second Provincial General Hospital, Guangzhou, Guangdong, 510317, People’s Republic of China
Correspondence: Aoxiang Luo, School of Nursing, Guangdong Pharmaceutical University, No. 283 Jiang-Hai Lane, Haizhu District, Guangzhou, Guangdong, 510310, People’s Republic of China, Email [email protected]
Background: Kinesiophobia presents a significant barrier to rehabilitation across multiple conditions. While cognitive behavioral therapy (CBT) holds potential for addressing phobic responses, its specific efficacy against kinesiophobia requires clarification.
Purpose: To systematically evaluate CBT’s efficacy in reducing kinesiophobia among adults.
Methods: Following Cochrane guidelines, two independent reviewers searched six international databases (PubMed, Cochrane Library, Embase, EBSCO, Web of Science, Scopus) and four Chinese databases (SinoMed, CNKI, VIP, WanFang) for randomized controlled trials (RCTs) on CBT interventions targeting kinesiophobia, from inception through November 2024. Independent dual review was conducted for study selection, data extraction, and quality assessment (Cochrane Risk of Bias tool). Random-effects meta-analyses were performed using RevMan 5.4 and Stata 12, with heterogeneity quantified by I² statistics.
Results: Eight trials with 938 participants were included. CBT demonstrated significantly greater reduction in kinesiophobia scores versus controls (MD=− 5.67, [95% CI:− 6.99, − 4.35], P< 0.001). Notably, effects were more pronounced for lumbar conditions (MD=− 6.97, 95% CI [− 9.97, − 3.96], P< 0.01). Compared with CBT combined with other therapies (MD=− 5.23, 95% CI [− 7.95, − 2.51], P< 0.01), monotherapy CBT demonstrates greater superiority(MD=− 5.96, 95% CI [− 7.66,-4.26], P< 0.01). In terms of follow-up duration, medium and long-term (3 months < follow-up time ≤ 6 months) (MD=− 8.61, 95% CI [− 9.72,-7.50], P< 0.01), 6 months < follow-up time ≤ 12 months (MD=− 11.63, 95% CI [− 13.41,-9.84], P< 0.01) achieves better outcomes in reducing patients’ kinesiophobia levels than short-term (follow-up time ≤ 3 months) (MD=− 7.69, 95% CI [− 9.47,-5.90], P< 0.01).
Conclusion: This meta-analysis provides robust evidence that CBT effectively reduces kinesiophobia, particularly as monotherapy for lumbar conditions with sustained follow-up. Clinicians should prioritize CBT implementation to enhance recovery. While results are compelling, confirmatory trials with rigorous methodology and adequate power are warranted.
Keywords: kinesiophobia, cognitive behavioral therapy, meta-analysis, randomized controlled trials
Introduction
The management of exercise-related behavioral modifications represents a fundamental component of modern rehabilitation science. According to the UK Medical Research Council’s framework for complex interventions, sustained behavioral modification serves as both a therapeutic target and outcome measure in neuro-musculoskeletal rehabilitation.1 However, a significant proportion of patients develop exercise-related fears and activity avoidance due to multifactorial causes.2 Kinesiophobia is defined as an excessive, irrational, and extreme panic or avoidance of physical movement and activity, stemming from patients’ perceived vulnerability to painful injury or re-injury.3 Originally conceptualized through the fear-avoidance model,4 kinesiophobia manifests as an irrational preoccupation with movement-induced injury, transcending mere pain anticipation to encompass multidimensional psychological barriers. Critically, kinesiophobia aligns well with established cognitive models of anxiety and fear, such as Beck’s cognitive model.5 This model posits that dysfunctional beliefs and cognitive distortions (eg, catastrophizing, overgeneralization) shape an individual’s interpretation of experiences, leading to maladaptive emotional and behavioral responses. In the context of kinesiophobia, patients may harbor core dysfunctional beliefs about their bodily fragility (“My body is broken”, “Movement is dangerous”) and catastrophize sensations associated with movement or exertion (interpreting normal muscle fatigue or transient discomfort as signals of imminent, catastrophic re-injury).6 These distorted cognitions automatically trigger intense fear and anxiety, which in turn drive the avoidance behavior characteristic of kinesiophobia. At present, most of the research in this field focuses on patients with chronic pain, while there are still few studies on groups such as cardiac rehabilitation patients. Epidemiological studies demonstrate notable prevalence rates: 62.4% post-percutaneous coronary intervention,7 58.2% in individuals with chronic obstructive pulmonary disease,8 and 55.8% in patients following total knee arthroplasty.9 Notably, the prevalence of kinesiophobia reached as high as 79% among patients with musculoskeletal pain.10 Research indicates that kinesiophobia not only impacts patients’ treatment adherence, leading to organ function stagnation and regression, but also significantly affects their quality of life and even survival rates.11 This phobic response establishes a self-perpetuating cycle - diminished physical activity precipitates muscle atrophy and joint stiffness, thereby exacerbating pain perception and reinforcing movement avoidance.12 Simultaneously, kinesiophobia is recognized as a modifiable factor. Through proactive prevention and education, it is possible to achieve early pain relief and functional recovery, thereby enhancing the overall quality of life.13
Modern medicine emphasizes not only treating patients’ physical diseases, but also paying attention to their mental health. Cognitive behavioral therapy (CBT) is a psychological therapy that combines cognitive process with behavioral change.14 By correcting the patient’s bad cognition and combining behavioral training, it reduces the patient’s negative emotions, so as to achieve the rehabilitation effect. CBT can be divided into traditional cognitive behavioral therapy, online cognitive behavioral therapy and group cognitive behavioral therapy, among which digital cognitive behavioral therapy has attracted much attention due to the progress of information technology, which provides CBT guidance and training to patients through Internet technology.15 Compared with drug treatment and surgical treatment, CBT treatment does not have any drug side effects, and can effectively improve psychological problems and promote patients to form an objective self-health assessment.16 The application of CBT to pain-induced early fear of exercise has been shown to be based on a structured cognitive restructuring and behavioral activation protocol that allows patients to recalipay catastrophic thought patterns (“movement will cause irreversible damage”) to enhance movement and promote recovery, while gradually rebuilding activity tolerance.17 Currently, CBT has been empirically validated to significantly reduce kinesiophobia levels in patients with chronic low back pain,18 post-joint replacement19 and temporomandibular joint disorders.20 Despite these promising signals, critical evidence gaps persist. First, existing studies exhibit substantial methodological heterogeneity: intervention protocols range from 4-week digital modules to 12-week multimodal programs,12,19 with outcome measures spanning 11- to 17-item Tampa Scale variants.21,22 Second, the comparative effectiveness of CBT monotherapy versus hybrid approaches (eg, CBT combined with physiotherapy) remains contested. Third, durability of therapeutic effects shows inconsistent patterns across follow-up durations (3–24 months).23,24 These discrepancies hinder clinical protocol standardization and resource allocation decisions.
By synthesizing evidence from randomized controlled trials, this work aims to conduct a comprehensive systematic meta-analysis to evaluate whether CBT can improve kinesiophobia levels in patients, whether used alone or in combination with other therapies. By comparing the short-term and long-term efficacy of CBT, this research not only deepens our understanding of the clinical role of CBT but also provides valuable insights to identify the optimal protocols and duration for CBT implementation. Ultimately, these findings will guide future clinical decision-making and rehabilitation strategies.
Methods
Protocol and Registration
This systematic review was conducted in accordance with the PRISMA 2020 guidelines25 and Cochrane recommendations for systematic reviews. The study protocol was prospectively registered on PROSPERO (CRD42023411556), and a completed PRISMA checklist is provided in Appendix S1.
Eligibility Criteria
Eligibility criteria were defined using the PICO framework.
(1) Study design: Randomized controlled trials (RCTs) were included regardless of blinding status.
(2) Population: Participants with any medical diagnosis were eligible, whereas individuals with language barriers or psychiatric comorbidities (eg, schizophrenia spectrum disorders) were excluded.
(3) Interventions: CBT-based interventions (either as monotherapy or in combination with adjunctive therapies).
(4) Comparisons: routine care or any other interventions that did not involve cognitive behavioral therapy.
(5) Outcome: Kinesiophobia severity was quantified using validated scales: TSK-17, TSK-11, or FABQ. The TSK-17 Scale26 represents the most widely utilized assessment tool. It consists of 17 items with a total score ranging from 17 to 68 points. A total score >37 points indicates the presence of kinesiophobia in patients, with higher scores reflecting a higher level of kinesiophobia. The TSK-11 scale27 a psychometrically validated short-form adaptation of the TSK-17. A score exceeding 26 points meets the diagnostic threshold for kinesiophobia. The Fear-Avoidance Beliefs Questionnaire (FABQ)28 evaluates fear-avoidance beliefs associated with physical activity and occupational participation.
(6) Language: Publications were restricted to English or Chinese languages.
Exclusion criteria: Research protocols, ongoing studies, reviews and conference abstracts were excluded. Studies unrelated to the target study design, duplicate publications, unavailable full-text or abstract-only papers, and Studies with inaccessible full texts despite contacting the corresponding authors were excluded.
Search Strategy
A systematic search was conducted across ten databases (PubMed, Cochrane Library, Embase, EBSCO, Web of Science, Scopus, China Biology Medicine, China National Knowledge Infrastructure, VIP Data and WanFang Data) from their respective inception dates through November 2024. To search each database, we combined subject terms and free terms, employing Boolean logic operators to connect the search terms. The retrieval strategies were adjusted according to the specific requirements of each database, although the search strategy in PubMed served as a foundation: “((‘Cognitive Behavioral Therapy’[Mesh])” OR (Behavioral Therapies, Cognitive[Title/Abstract])) AND ((Kinesiophobia [Mesh]) OR (Fear of Movement[Title/Abstract]))”. Only RCTs were included in the retrieved results. We manually screened reference lists of included studies to identify additional eligible trials, with the aim of identifying relevant systematic reviews and references of included papers that had not been initially retrieved. The full search strategies and their complete details are shown in Appendix S2.
Study Selection
The literature screening was independently conducted by two trained researchers in strict accordance with the predefined inclusion and exclusion criteria. First, the literature was imported into Endnote X9 for duplicate checking, and then the titles and abstracts were read based on the predefined criteria to exclude irrelevant literature. Subsequently, the full texts were reviewed to further exclude ineligible studies and determine the final inclusion. Two independent reviewers performed screening, data extraction, and cross-verification. In case of disagreements, a third party was consulted to assist in making a decision and reaching a consensus.
Data Extraction
Data extraction was executed independently by two reviewers using Microsoft Excel (Microsoft Corporation). In cases of discrepancies between extracted information, a third researcher was consulted to reach a consensus decision. Discrepancies in data extraction were resolved through discussion with a third reviewer until consensus was achieved. The extracted data encompassed: (1) basic characteristics of included studies (authors, publication year, study region, sample size, mean age); (2) baseline demographic and clinical profiles of participants; (3) intervention protocols and duration; (4) the instruments of outcomes; and (5) quality grading. To ensure comprehensive data acquisition, corresponding authors were contacted via Email to request clarification or supplementation of missing or ambiguous data. Studies with unresolved discrepancies in critical data were excluded from subsequent meta-analysis.
Risk of Bias Assessment
Two independent reviewers conducted the risk of bias assessment of each study according to the Cochrane Handbook of Quality Standards for Literature risk of bias tool for randomized controlled trials.29 The risk of bias assessment should consider the generation of randomized sequence, the concealment of randomized scheme allocation, the blinding of study population and interveners, the blinding of outcome assessors, the integrity of outcome indicators, the selective reporting of outcomes, and other sources of bias in the study. For each included literature, the above six items were judged as “low bias”, “high bias” and “unclear” (lack of relevant information or uncertain bias). Finally,All indicators rated as entirely low bias were classified as Grade A, those with partial low bias as Grade B, and those without any low bias as Grade C. In this study, literature rated as Grade B or higher was included for analysis.30
Statistical Analysis
Statistical analyses were conducted using Review Manager (RevMan) version 5.4. For continuous data, the effect size was calculated as the mean difference with standard deviation (MD±SD), along with the 95% confidence interval (CI). Heterogeneity among studies was initially assessed using the Q-test. A threshold of P ≥ 0.10 indicated study homogeneity, while a P-value < 0.1 suggested the presence of heterogeneity. The degree of heterogeneity was evaluated using the I² statistic, with I² values of 0% to 40% indicating low heterogeneity, 30% to 60% representing moderate heterogeneity, 50% to 90% denoting substantial heterogeneity, and 75% to 100% indicating high heterogeneity.30 In cases of heterogeneity, a random-effects model was employed for effect size pooling. Subgroup analyses were conducted to explore potential sources of heterogeneity, stratified by disease type (lumbar disorders, knee disorders, or other conditions), intervention content (cognitive behavioral therapy alone or combined with other therapies), and follow-up duration (≤3 months, 3–6 months, >6 months). Methodological quality assessment of included studies was performed using RevMan 5.4, and a risk of bias assessment graph was generated. Sensitivity analyses were performed by sequentially excluding individual studies to assess the robustness of pooled results. Publication bias was evaluated through funnel plot analysis and Egger’s regression asymmetry test.31
Results
Study Selection
Our systematic search identified 3111 records from electronic databases, with 4 additional records identified through manual searching. After removing 1,335 duplicates through automated deduplication in EndNote X9 complemented by manual verification Two independent reviewers screened the remaining records against predefined eligibility criteria. Following title and abstract review, 1610 articles were excluded as they clearly did not meet the inclusion criteria. The full texts of the remaining 166 articles were retrieved and thoroughly reviewed, ultimately yielding 8 studies that met all predefined criteria for inclusion in the qualitative synthesis. Finally, this study included 8 studies for meta-analysis. A total of 938 participants were included in the analysis, with 470 assigned to the control group and 468 to the intervention group. A PRISMA flow diagram of the selection process is presented in Figure 1.
 |
Figure 1 PRISMA flow diagram of the search. |
Study Characteristics
The final analysis included 8 studies conducted across five countries: Sweden,32 Italy,23 China,21,33–35 Spain,22 and the United Kingdom,24 with publication dates spanning from 2010 to 2024. These studies collectively enrolled 938 participants, comprising the following populations: 208 patients who underwent total knee arthroplasty,21,35 231 patients who received lumbar spinal fusion,23,32 172 patients with conservatively treated lumbar disc herniation,33 260 patients who underwent radical resection for lung cancer,34 19 patients with hemophilia,22 and 48 patients with chronic low back pain.24 Regarding intervention approaches, three studies employed CBT in combination with additional therapies, specifically integrated with functional exercise,23 physical therapy,22 and traditional Chinese medicine psychological nursing,33 respectively. Five studies implemented CBT as monotherapy. Outcome measures were assessed using three distinct instruments: six studies employed the TSK-17 scale,21,23,32–35 while the TSK-11 scale22 and FABQ scale24 were each used in one study. Key features of the included studies are summarized in Table 1.
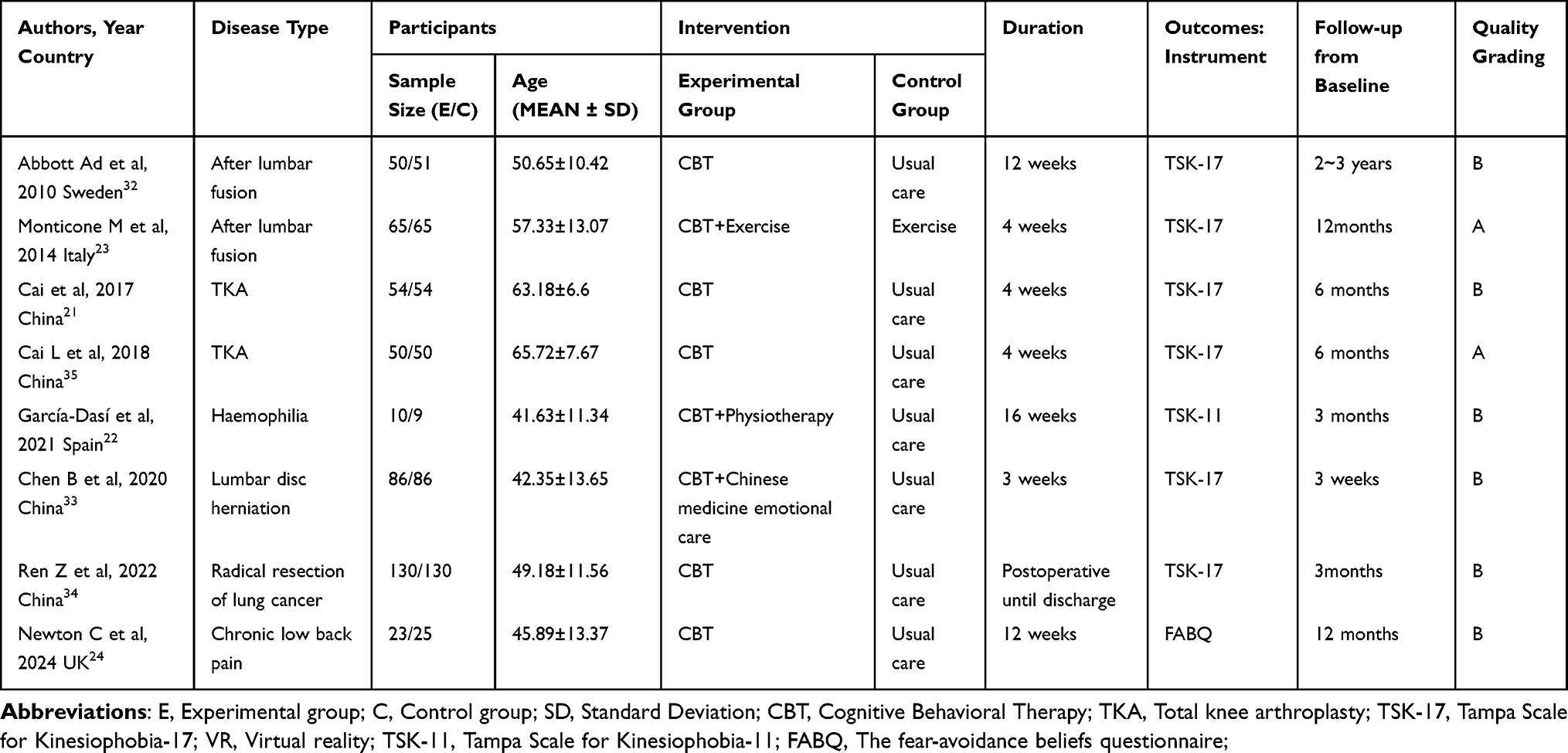 |
Table 1 Characteristics of the 8 Included Trials |
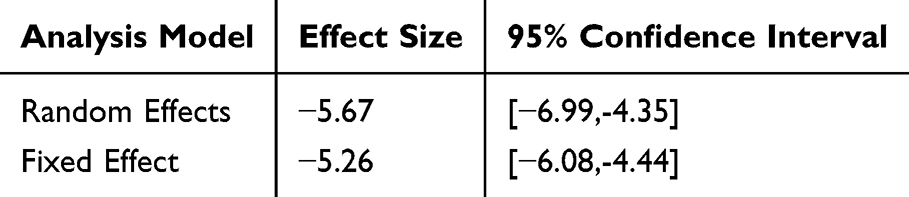 |
Table 2 Sensitivity Analysis of Kinesiophobia Scores Using Different Effect Models |
Risk of Bias
Risk of bias assessments are visualized in Figures 2 and 3. We included a total of eight articles, and the quality of the included literature was assessed using the evaluation criteria outlined in the Cochrane Handbook for Systematic Reviews.30 Regarding random sequence generation, three studies explicitly employed a random number table for allocation,21,33,35 while two studies utilized computer-generated randomization.23,24 Two studies reported randomization without methodological details,22,32 and one study was rated as high risk due to its sequential allocation based on patient admission order.34 In terms of allocation concealment, two studies implemented sealed envelope methods.24,32 Due to the inherent nature of the interventions, blinding was challenging to implement; only three studies mentioned blinding procedures, including one double-blind35 and two single-blind studies,22,23 with two rated as high risk.24,32 The remaining studies did not provide clear descriptions of blinding. For data completeness, one study was assessed as high risk due to insufficient outcome data,22 while the others demonstrated low risk. Two studies experienced proportional data loss in both experimental and control groups due to extended follow-up periods,32,35 whereas the remaining studies maintained complete data without any loss. Two studies deviated from “intention-to-treat (ITT)” analysis.24,32 Overall, among the eight studies included in the analysis, two were rated as Grade A in quality assessment, while the remaining six received Grade B ratings, indicating that the included studies were of moderate quality.
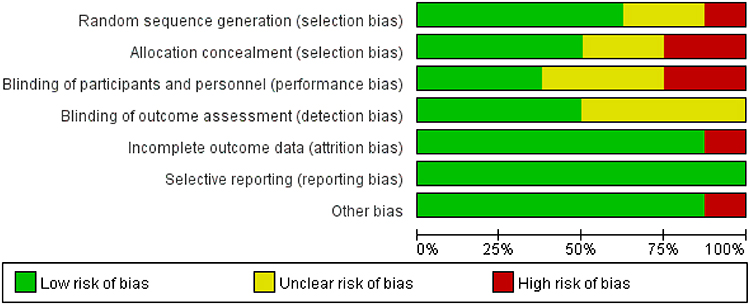 |
Figure 2 Risk of bias graph. |
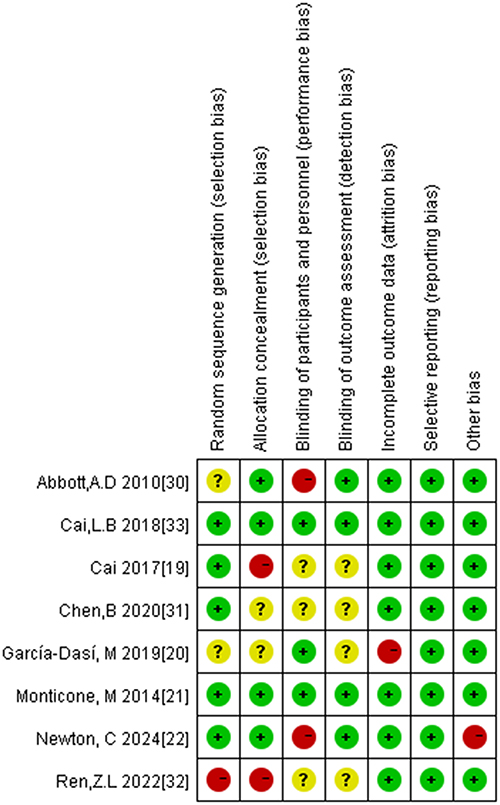 |
Figure 3 Risk of bias summary. |
Results of Meta-Analysis Meta
Effects of CBT on Kinesiophobia
A total of eight studies were incorporated in this analysis, encompassing 938 participants, of which 468 were allocated to the cognitive behavioral therapy group and 470 to the standard care group. Heterogeneity analysis revealed an I2 value of 52%, indicating moderate heterogeneity. Hence, the random effect model was used for effect size combination. The random-effects meta-analysis showed a significant treatment effect (MD = −5.67, 95% CI[−6.99, −4.35]; P< 0.01), indicating CBT significantly reduced kinesiophobia scores compared to control conditions as shown in Figure 4.
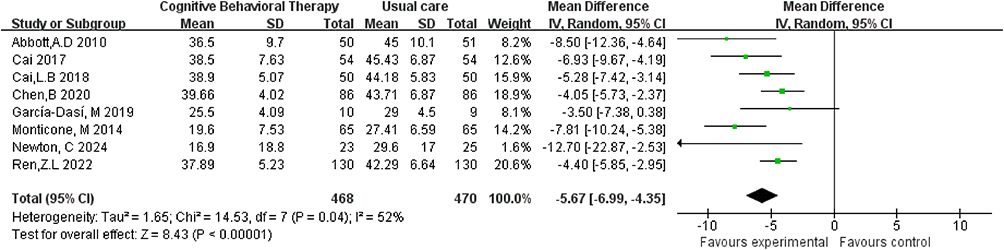 |
Figure 4 Forest plot of the effect of CBT on kinesiophobia scores compared to routine care (random-effects model). |
Subgroup Analyses
Subgroup analyses were conducted based on disease categories among the eight included studies. Four studies involving patients who underwent lumbar spinal fusion,23,32 those with conservatively treated lumbar disc herniation,33 and individuals with chronic low back pain24 were categorized into the lumbar spine subgroup. Two studies21,35 focusing on patients who received total knee arthroplasty were classified into the after total knee arthroplasty subgroup. The remaining two studies, which included patients with hemophilia22 and those who underwent radical resection for lung cancer,34 were grouped into the “other conditions” category. Lumbar spine subgroup analyses demonstrated substantial heterogeneity (MD=−6.97, 95% CI[−9.97, −3.96]; I²=71%, P< 0.01), whereas heterogeneity was negligible in the total knee arthroplasty (I²=0%) and other conditions (I²=0%) subgroups (Figure 5).
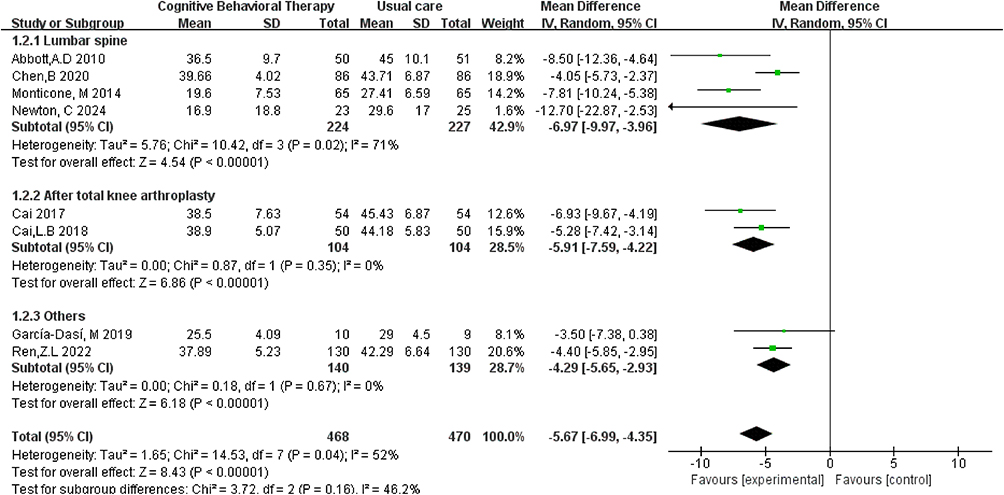 |
Figure 5 Subgroup analyses of disease type for kinesiophobia. |
Subgroup analyses were performed on the eight included studies based on intervention types, categorizing them into the cognitive behavioral therapy (CBT) alone group and the CBT combined with other therapies group. Among these, five studies employed CBT as the sole intervention and were included in the CBT alone group.21,24,32,34,35 The remaining three studies implemented CBT in combination with other approaches, specifically integrating functional exercise,23 physical therapy,22 and traditional Chinese medicine psychological nursing,33 respectively, and were classified into the CBT combined with other therapies group. The subgroup analysis results demonstrated that CBT alone was more effective in reducing kinesiophobia compared to CBT combined with other therapies. The CBT alone group exhibited low heterogeneity (MD=−5.96, 95% CI [−7.66,-4.26], P< 0.01, I2=47%), while the CBT combined with other therapies group showed substantial heterogeneity (MD=−5.23, 95% CI [−7.95, −2.51], P< 0.01, I2=71%) (refer to Figure 6).
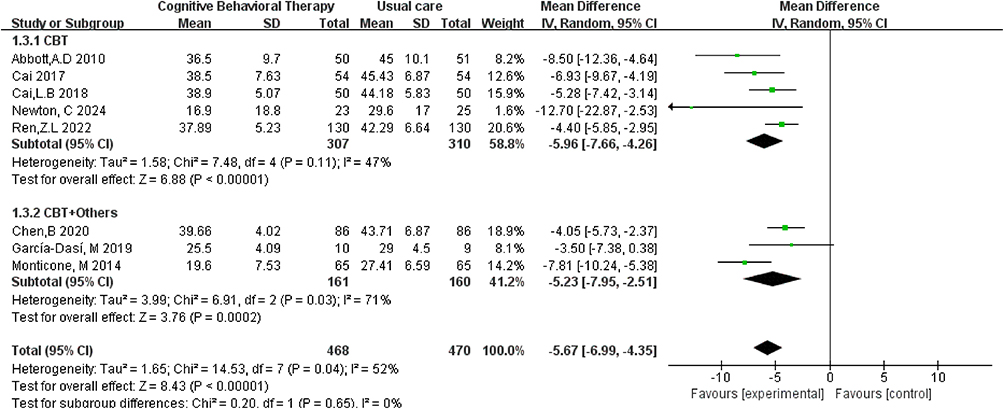 |
Figure 6 Subgroup analyses of intervention content for kinesiophobia. |
The eight included studies were stratified into four subgroups based on follow-up duration. The analysis revealed that cognitive behavioral therapy (CBT) for reducing kinesiophobia levels exhibited substantial heterogeneity (I2=67%) in the short-term efficacy subgroup (follow-up≤3 months) (MD=−7.69, 95% CI [−9.47,-5.90], P< 0.01), while demonstrating low heterogeneity in the subgroups with follow-up durations of 3 to 6 months and 6 to 12 months (I2=0%). Longitudinal analysis revealed sustained CBT superiority over routine care across all follow-up intervals (Figure 7), with the largest effect size observed in the 6 to 12-month follow-up period (MD=−11.63, 95% CI [−13.41,-9.84]).
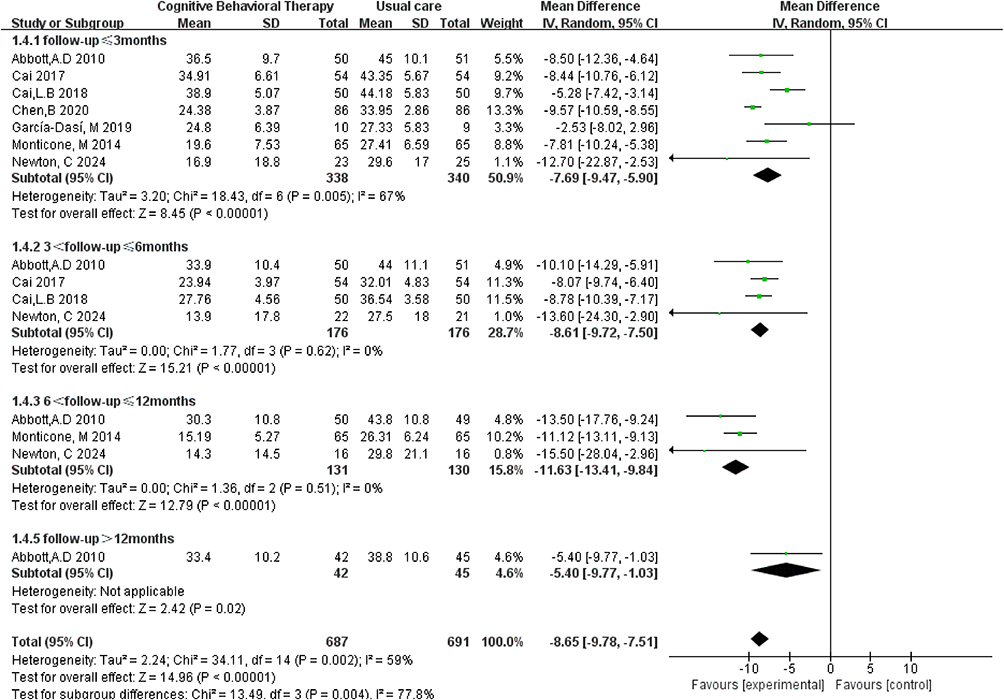 |
Figure 7 Subgroup analyses of follow-up duration for kinesiophobia. |
Sensitivity Analyses
Upon switching between random-effects and fixed-effects models and re-performing the statistical analyses, no significant changes were observed in all statistical outcomes, indicating robust results (Table 2).
Publication Bias Analyses
As shown in Figure 8, although the funnel plot asymmetry suggested potential publication bias, Egger’s test did not reach significance (P=0.539>0.05), possibly due to the limited number of included studies.
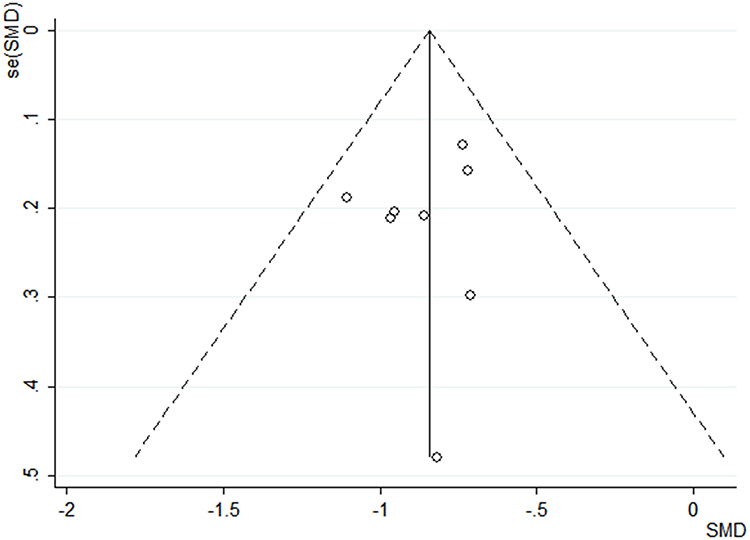 |
Figure 8 The funnel plot for the intervention effect of CBT on kinesiophobia. |
Discussion
This meta-analysis synthesized data from 8 randomized controlled trials (n=938 participants), with two studies classified as low-risk (Grade A) and six as moderate-risk (Grade B) for bias. The overall quality of the included literatures was moderate, and the pooled results provide clinically meaningful evidence, but due to the limitations of the number and quality of included studies, it was still necessary to include higher quality randomized controlled trials for later studies.
This review synthesizes evidence on CBT’s efficacy for kinesiophobia management. The results demonstrated that Cognitive Behavioral Therapy (CBT) exhibits significant efficacy in reducing kinesiophobia levels among patients, which aligns with the findings reported by Vergeld et al.36 The development of kinesiophobia can lead to reduced physical activity, increased pain levels, diminished limb function, and even contribute to negative emotional states, ultimately resulting in a decreased quality of life for patients.37 As shown in Figure 4, the consistency of effect directions across studies strengthens causal inference despite moderate heterogeneity. Brown et al demonstrated that Cognitive Behavioral Therapy (CBT) significantly reduces patients’ fear-avoidance beliefs and enhances their sense of self-control, thereby improving kinesiophobia, alleviating pain, and promoting functional recovery.38 The psychological intervention based on CBT encourages patients to confront adverse experiences associated with their condition and reconstructs their cognition through various approaches to address underlying issues.39 This process effectively reduces avoidance and submission behaviors, ultimately lowering patients’ kinesiophobia levels. Therefore, under the guidance and assistance of healthcare professionals, the implementation of scientific, standardized, and systematic Cognitive Behavioral Therapy (CBT) can effectively reduce patients’ kinesiophobia levels. This approach holds significant clinical value in promoting limb functional recovery, improving disease prognosis, and enhancing overall quality of life.
Subgroup analysis based on disease types in this study revealed that Cognitive Behavioral Therapy (CBT) effectively reduces kinesiophobia levels across various conditions, demonstrating significant clinical value. Notably, CBT exhibited superior efficacy in alleviating kinesiophobia among patients with lumbar spine disorders, potentially attributed to the primary symptom of low back pain in these patients.40 The exacerbation of pain further inhibits paravertebral muscle activity, leading to spinal instability and trunk imbalance, consequently increasing kinesiophobia levels.41 A systematic review indicated that CBT can enhance patients’ beliefs in their ability to achieve improved functional outcomes by targeting self-efficacy, ultimately reducing kinesiophobia levels.42 However, The substantial heterogeneity in the lumbar subgroup may stem from variations in CBT duration (ranging from 3 to 12 weeks across studies) and delivery formats (individual vs group sessions). Additionally, the absence of disease type restrictions in our inclusion criteria resulted in varying disease severity levels. Future research should clarify the relationship between CBT and specific disease types, exploring more comprehensive and scientific protocols for targeted clinical interventions.
Subgroup analysis of different intervention approaches revealed that Cognitive Behavioral Therapy (CBT) alone demonstrated significantly greater efficacy in reducing patients’ kinesiophobia levels compared to CBT combined with other therapies. CBT, as a psychological treatment approach, facilitates the identification and correction of erroneous cognitions to eliminate negative emotions and behaviors, thereby improving kinesiophobia levels and subsequently promoting functional recovery.43 In contrast to conventional nursing interventions, CBT bridges theoretical frameworks with practical application, focusing not only on symptom alleviation but also on the relationship between cognitive states and actual behaviors.44 The superior efficacy of CBT alone may reflect the “therapeutic purity” hypothesis—combined interventions could dilute focus on cognitive restructuring.45 Combined interventions may introduce additional risks (eg, pain from physical therapy potentially exacerbating anxiety), which could inadvertently undermine the cognitive objectives of CBT, leading to lower patient compliance and attentional dispersion.46
Subgroup analysis based on follow-up duration in this study revealed that medium-term (3~6 months) and long-term (>6 months) follow-up periods showed sustained therapeutic benefits in reducing kinesiophobia levels compared to short-term follow-up (≤3 months). Short-term effects may primarily reflect behavioral compliance, whereas lasting fear reduction necessitates deeper cognitive engagement, ensuring treatment continuity and effectiveness. Research indicates that while CBT shows no statistically significant difference in kinesiophobia levels compared to other nursing interventions during short-term follow-up, it demonstrates superior efficacy in improving kinesiophobia during medium-term follow-up periods.20 Conversely, a systematic review demonstrated no statistically significant difference in kinesiophobia levels between Cognitive Behavioral Therapy (CBT) and standard nursing interventions at 3-month and 12-month follow-up periods.47 This discrepancy may be associated with factors such as limited sample sizes and patient follow-up attrition. In our study, the inclusion of studies with relevant measurement indicators was limited, and the small sample sizes may have introduced potential bias into the results.
Limitations
Four key limitations should be acknowledged: First, the restricted pool of eligible RCTs (n=8) may compromise statistical power, particularly in subgroup analyses where some categories contained ≤3 studies. Second, measurement bias is probable as included studies relied solely on self-reported outcomes without objective movement assessment. Third, clinical heterogeneity due to unstratified disease severity levels (eg, ranging from postoperative arthroplasty to chronic pain syndromes) may have inflated the observed statistical heterogeneity (I² = 52%). Fourth, the exclusion of non-English/Chinese studies and grey literature may have introduced language and publication biases. Specifically, the subgroup analyzing CBT as a standalone intervention consisted of merely five studies, while the subgroup evaluating CBT combined with other therapies included only three studies. These limitations highlight the necessity for future investigations with larger sample sizes and more rigorous designs to enhance our understanding of intervention efficacy and optimize therapeutic protocols.
Implications
This study demonstrated that Cognitive Behavioral Therapy (CBT) is effective in clinically reducing patients’ kinesiophobia levels, equipping clinicians with evidence-based CBT strategies for targeted psychological care. This approach provides stronger support for enhancing the quality of care and promoting physical rehabilitation in patients with kinesiophobia. Our findings suggest that future research should focus more intensively on developing reasonable and effective CBT intervention protocols, including intervention methods, timing, frequency, intensity, and duration. This will provide healthcare professionals with more actionable guidance, enabling them to apply this approach more flexibly and develop more scientific and personalized intervention strategies.
Conclusion
This meta-analysis provides a comprehensive evaluation of the application of cognitive behavioral therapy in patients with kinesiophobia. The current findings demonstrated that cognitive behavioral therapy has the potential to reduce kinesiophobia and facilitate rehabilitation, suggesting that its clinical implementation should be encouraged for kinesiophobia intervention. However, given the limitations in quantity and quality of the included original studies, the reliability and generalization of the research results will be affected. Future research should incorporate more rigorously designed, high-quality, multicenter, large-scale, and long-term follow-up randomized controlled trials to further validate the long-term intervention effects of cognitive behavioral therapy on kinesiophobia, thereby providing better guidance for clinical practice.
Data Sharing Statement
The datasets analyzed during this systematic review were obtained from the cited studies and are publicly available in the supplementary files accompanying this publication.
Ethics Approval Statement
Ethical approval was not needed because this is a meta-analysis. This study protocol is registered with PROSPERO (CRD42023411556).
Consent for Publication
All authors give consent for publication.
Acknowledgments
The authors gratefully acknowledge colleagues who provided technical guidance during manuscript preparation and contributors to the cited works that enabled this synthesis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other financial support were received during the preparation of this study.
Disclosure
The authors have no conflicts of interest to disclose for this work.
References
1. Skivington K, Matthews L, Simpson SA, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061. doi:10.1136/bmj.n2061
2. Ohji S, Aizawa J, Hirohata K, et al. Kinesiophobia is negatively associated with psychological readiness to return to sport in patients awaiting anterior cruciate ligament reconstruction. Arthroscopy. 2023;39(9):2048–2055. doi:10.1016/j.arthro.2023.02.016
3. Bäck M, Caldenius V, Svensson L, Lundberg M. Perceptions of kinesiophobia in relation to physical activity and exercise after myocardial infarction: a qualitative study. Phys Ther. 2020;100(12):2110–2119. doi:10.1093/ptj/pzaa159
4. Lethem J, Slade PD, Troup JD, Bentley G. Outline of a fear-avoidance model of exaggerated pain perception--I. Behav Res Ther. 1983;21(4):401–408. doi:10.1016/0005-7967(83)90009-8
5. Leahy RL. Emotional Schemas. Cognit Behav Pract. 2022;29(3):575–580. doi:10.1016/j.cbpra.2022.02.004
6. Yang SY, Woon EYS, Griva K, Tan BY. A qualitative study of psychosocial factors in patients with knee osteoarthritis: insights learned from an Asian population. Clin Orthop Relat Res. 2023;481(5):874–884. doi:10.1097/CORR.0000000000002526
7. Wang H, Zhou L, Cheng P, et al. Construction and validation of a predictive model for kinetophobia in patients after percutaneous coronary intervention. Chin J Nurs. 2024;59(17):2108–2115.
8. Tanaka T, Okita M, Jenkins S, Kozu R. Clinical and psychological impact of chronic pain in people with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:893–903. doi:10.2147/COPD.S359223
9. De Vroey H, Claeys K, Shariatmadar K, et al. High levels of kinesiophobia at discharge from the hospital may negatively affect the short-term functional outcome of patients who have undergone knee replacement surgery. J Clin Med. 2020;9(3):738. doi:10.3390/jcm9030738
10. Perrot S, Trouvin A-P, Rondeau V, et al. Kinesiophobia and physical therapy-related pain in musculoskeletal pain: a national multicenter cohort study on patients and their general physicians. Joint Bone Spine. 2018;85(1):101–107. doi:10.1016/j.jbspin.2016.12.014
11. Luque-Suarez A, Martinez-Calderon J, Falla D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: a systematic review. Br J Sports Med. 2019;53(9):554–559. doi:10.1136/bjsports-2017-098673
12. Alpalhão V, Cordeiro N, Pezarat-Correia P. Kinesiophobia and fear avoidance in older adults: a scoping review on the state of research activity. J Aging Phys Act. 2022;30(6):1075–1084. doi:10.1123/japa.2021-0409
13. Luque-Suarez A, Falla D, Morales-Asencio JM, Martinez-Calderon J. Is kinesiophobia and pain catastrophising at baseline associated with chronic pain and disability in whiplash-associated disorders? A systematic review. Br J Sports Med. 2020;54(15):892–897. doi:10.1136/bjsports-2018-099569
14. Åkerblom S, McCracken LM, Rivano Fischer M, Perrin S. Long-term pain and health economic outcomes in adults receiving multidisciplinary CBT for chronic pain: the role of psychological inflexibility. Front Pain Res. 2025;6:1547540. doi:10.3389/fpain.2025.1547540
15. Schuffelen J, Maurer LF, Gieselmann A. Digital CBT-I in comorbid insomnia and depression: clinical outcomes from a pragmatic randomized controlled trial. Depress Anxiety. 2025;2025:2171041. doi:10.1155/da/2171041
16. Nuraeni A, Suryani S, Trisyani Y, Sofiatin Y. Efficacy of cognitive behavior therapy in reducing depression among patients with coronary heart disease: an updated systematic review and meta-analysis of RCTs. Healthcare. 2023;11(7):943. doi:10.3390/healthcare11070943
17. Wenzel A. Basic Strategies of Cognitive Behavioral Therapy. Psychiatr Clin North Am. 2017;40(4):597–609. doi:10.1016/j.psc.2017.07.001
18. Monticone M, Ambrosini E, Rocca B, Foti C, Ferrante S. Responsiveness and minimal clinically important changes for the Tampa Scale of Kinesiophobia after lumbar fusion during cognitive behavioral rehabilitation. Eur J Phys Rehabil Med. 2017;53(3):351–358. doi:10.23736/S1973-9087.16.04362-8
19. Kazarian GS, Anthony CA, Lawrie CM, Barrack RL. The impact of psychological factors and their treatment on the results of total knee arthroplasty. J Bone Joint Surg Am. 2021;103(18):1744–1756. doi:10.2106/JBJS.20.01479
20. Zhang Q, Zhang J, Ran W, Yu S, Jin Y. Effectiveness of cognitive behavioral therapy on kinesiophobia and oral health-related quality of life in patients with temporomandibular disorders, study protocol for a randomized controlled trial. Medicine. 2020;99(47):e23295. doi:10.1097/MD.0000000000023295
21. Cai L, Liu Y, Zhao H, Xu H, Gao H, Dong Y. Cognitive behavior therapy alleviates kinesiophobia after total knee arthroplasty. Chin J Tissue Eng Res. 2017;21(23):3658–3663.
22. García-Dasí M, Pérez-Alenda S, Carrasco JJ, et al. Effects of a non-pharmacological approach for chronic pain management in patients with haemophilia: efficacy of cognitive-behavioural therapy associated with physiotherapy. Haemophilia. 2021;27(3):e357–e367. doi:10.1111/hae.14284
23. Monticone M, Ferrante S, Teli M, et al. Management of catastrophising and kinesiophobia improves rehabilitation after fusion for lumbar spondylolisthesis and stenosis. A randomised controlled trial. Eur Spine J. 2014;23(1):87–95. doi:10.1007/s00586-013-2889-z
24. Newton C, Singh G, Nolan D, et al. Cognitive functional therapy compared with usual physiotherapy care in people with persistent low back pain: a mixed methods feasibility randomised controlled trial in the United Kingdom National Health Service. Physiotherapy. 2024;123:118–132. doi:10.1016/j.physio.2024.02.003
25. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
26. French DJ, France CR, Vigneau F, French JA, Evans RT. Fear of movement/(re)injury in chronic pain: a psychometric assessment of the original English version of the Tampa scale for kinesiophobia (TSK). Pain. 2007;127(1–2):42–51. doi:10.1016/j.pain.2006.07.016
27. Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: a shortened version of the Tampa scale for kinesiophobia. Pain. 2005;117(1–2):137–144. doi:10.1016/j.pain.2005.05.029
28. Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2). doi:10.1016/0304-3959(93)90127-B
29. Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011:
30. Higgins J, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions; 2024. Available from: https://training.cochrane.org/handbook.
31. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
32. Abbott AD, Tyni-Lenné R, Hedlund R. Early rehabilitation targeting cognition, behavior, and motor function after lumbar fusion: a randomized controlled trial. Spine. 2010;35(8):848–857. doi:10.1097/BRS.0b013e3181d1049f
33. Chen B, Fu K, Wang Y, Li H. The application of emotion nursing of traditional Chinese medicine combined with cognitive behavior intervention in reducing the kinesiophobia of patients with lumbar disc herniation during rehabilitation. Chin J Pract Nurs. 2020;36(31):2411–2417.
34. Ren Z, Chen X, Liu Z, Xu G, Huang H, Lin H. Effect of cognitive behavioral intervention on postoperative rehabilitation of patients with kinesiophobia after radical resection of lung cancer. J Nurs Administrat. 2022;22(4):235–239,289.
35. Cai L, Gao H, Xu H, Wang Y, Lyu P, Liu Y. Does a program based on cognitive behavioral therapy affect kinesiophobia in patients following total knee arthroplasty? A randomized, controlled trial with a 6-month follow-up. J Arthroplasty. 2018;33(3):704–710. doi:10.1016/j.arth.2017.10.035
36. Vergeld V, Martin Ginis KA, Jenks AD. Psychological interventions for reducing fear avoidance beliefs among people with chronic back pain. Rehabil Psychol. 2021;66(4):386–403. doi:10.1037/rep0000394
37. Aykut Selçuk M, Karakoyun A. Is there a relationship between kinesiophobia and physical activity level in patients with knee osteoarthritis? Pain Med. 2020;21(12):3458–3469. doi:10.1093/pm/pnaa180
38. Brown ML, Plate JF, Von Thaer S, et al. Decreased range of motion after total knee arthroplasty is predicted by the Tampa scale of kinesiophobia. J Arthroplasty. 2016;31(4):793–797. doi:10.1016/j.arth.2015.10.037
39. Kaczkurkin AN, Foa EB. Cognitive-behavioral therapy for anxiety disorders: an update on the empirical evidence. Dialogues Clin Neurosci. 2015;17(3):337–346. doi:10.31887/DCNS.2015.17.3/akaczkurkin
40. Moreira LPC, Mendoza C, Barone M, Rocha RS, Dos Santos RD, Hazime FA. Reduction in pain inhibitory modulation and cognitive-behavioral changes in patients with chronic low back pain: a case-control study. Pain Manage Nurs. 2021;22(5):599–604. doi:10.1016/j.pmn.2021.05.004
41. Lotzke H, Brisby H, Gutke A, et al. A person-centered prehabilitation program based on cognitive-behavioral physical therapy for patients scheduled for lumbar fusion surgery: a randomized controlled trial. Phys Ther. 2019;99(8):1069–1088. doi:10.1093/ptj/pzz020
42. van Hooff ML, Vriezekolk JE, Kroeze RJ, O’Dowd JK, van Limbeek J, Spruit M. Targeting self-efficacy more important than dysfunctional behavioral cognitions in patients with longstanding chronic low back pain; a longitudinal study. BMC Musculoskeletal Disorders. 2021;22(1):824. doi:10.1186/s12891-021-04637-3
43. Thoma N, Pilecki B, McKay D. Contemporary cognitive behavior therapy: a review of theory, history, and evidence. Psychodyn Psychiatry. 2015;43(3):423–461. doi:10.1521/pdps.2015.43.3.423
44. Liu K, Liu Y, Ma X, Fu D, Fan Z. Effect of cognitive behavioral therapy on pain, knee function, and psychological status in patients after primary total knee arthroplasty: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2024;25:280. doi:10.1186/s12891-024-07413-1
45. Hofmann SG, Asnaani A, Vonk IJJ, Sawyer AT, Fang A. The efficacy of cognitive behavioral therapy: a review of meta-analyses. Cogn Ther Res. 2012;36(5):427–440. doi:10.1007/s10608-012-9476-1
46. Ploutarchou G, Savva C, Karagiannis C, Pavlou K, O’Sullivan K, Korakakis V. The effectiveness of cognitive behavioural therapy in chronic neck pain: a systematic review with meta-analysis. Cogn Behav Ther. 2023;52(5):523–563. doi:10.1080/16506073.2023.2236296
47. Ma T, Pei J, Shi F, et al. Effectiveness of cognitive behavioral therapy for patients after total knee arthroplasty: a systematic review and meta-analysis. Psychol Health Med. 2023;28(9):2407–2418. doi:10.1080/13548506.2022.2162934
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effectiveness of Cognitive Behavioral Therapy-Based Intervention on Improving Sleep-Related Outcomes for People with Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Wang H, Li R, Ge L, Xu F, Wiley JA, Tang S, Sun M
Psychology Research and Behavior Management 2024, 17:957-972
Published Date: 9 March 2024
Lack of Efficacy of Simvastatin Adjunctive Therapy for Patients with Schizophrenia: A Meta-Analysis of Randomized Controlled Trials
Chen J, Yuan Y, Hu Y, Liang L
Neuropsychiatric Disease and Treatment 2024, 20:1667-1675
Published Date: 6 September 2024
Evaluating the Overall Safety of Glucokinase Activators in Patients with Type 2 Diabetes Mellitus
Liang TT, Cao MJ, Wang Q, Zou JS, Yang XM, Gu LF, Shi FH
Diabetes, Metabolic Syndrome and Obesity 2024, 17:4539-4552
Published Date: 28 November 2024
The Efficacy and Safety of Ultrasound-Guided Nerve Block in the Treatment of Cervical Spondylotic Radiculopathy: A Systematic Review and Meta-Analysis
Deng M, Wu D, Tang N, Kuang J
Journal of Pain Research 2026, 19:573563
Published Date: 4 March 2026
Pharmacist-Led Integrated Management for Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Li X, Ma X, Qin W, Shi C, Liu L, Wang C
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:589904
Published Date: 16 April 2026