Back to Journals » Risk Management and Healthcare Policy » Volume 18
Addressing the Unmet Educational Needs of Students with Epidermolysis Bullosa in Saudi Arabia
Authors Alheggi A ![]() , Bin Shlhoob R
, Bin Shlhoob R ![]() , Alharthi R, Bukhari A, Alkhodair R
, Alharthi R, Bukhari A, Alkhodair R
Received 24 December 2024
Accepted for publication 25 July 2025
Published 5 August 2025 Volume 2025:18 Pages 2565—2573
DOI https://doi.org/10.2147/RMHP.S512984
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Ashjan Alheggi,1 Reem Bin Shlhoob,2 Raghad Alharthi,3 Abrar Bukhari,1 Rayan Alkhodair4– 6
1Department of Dermatology, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, Saudi Arabia; 2College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, Saudi Arabia; 3Department of Dermatology, King Abdulaziz Medical City, Riyadh, Saudi Arabia; 4Division of Pediatric Dermatology, Department of Pediatrics, King Abdullah Specialized Children’s Hospital, Riyadh, Saudi Arabia; 5College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 6Research Office Department, King Abdullah International Medical Research Center, Riyadh, Saudi Arabia
Correspondence: Ashjan Alheggi, Department of Dermatology, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), P.O. Box 7544, Riyadh, 4233-13317, Saudi Arabia, Tel +447375430305, Email [email protected]
Purpose: Epidermolysis bullosa (EB) is a rare genodermatosis characterized by fragility and blistering of the skin and mucous membranes following minor trauma. Attending school presents unique educational and psychosocial challenges for students with EB. This study aimed to investigate perceptions of school climate and educational experiences among students with EB in Saudi Arabia.
Methods: A cross-sectional observational study was conducted involving students with EB, aged 3– 22 years, recruited from the Saudi EB registry. Data were collected using a self-reported 23-item multidimensional questionnaire assessing physical, psychological, social, financial, and learning domains. Data were collected from January 2024 to April 2024. Descriptive and inferential statistical analyses were performed using SPSS software.
Results: Thirty-one students with EB were enrolled in this study. The EB subtypes were as follows: EB simplex (n=10), junctional EB (n=7), dystrophic EB (n=11), Kindler EB (n=1), and two patients with unknown types. Participants had an overall negative perception of school climate (mean, 58.5± 14.3). A significant proportion of students experienced delayed entry into elementary school due to EB (41.9%). Students with junctional EB, those in high school, late-entry grade 1 students, and those from low-income families reported more negative perceptions of the school climate. Key challenges included difficulty in physical education classes, stigmatization, bullying, social isolation, and chronic wound-related pain and itching. Frequent absences were reported by 51.6% of the students. Homeschooled students demonstrated better learning scores than those attending traditional schools. Students with severe EB subtypes (junctional and dystrophic EB) demonstrated a higher preference for homeschooling.
Conclusion: This study highlights the unmet needs of students with EB and provides insights into recommendations to enhance their adjustment in schools. Students with EB face substantial educational and psychosocial challenges. Tailored accommodations are needed to promote inclusion and improve school experiences for this population.
Keywords: epidermolysis bullosa, school, students, education, unmet need, challenges
Introduction
Epidermolysis bullosa (EB) is a rare group of genodermatoses characterized by skin and mucosal fragility, with blistering following minimal trauma.1 Severe subtypes of EB can have extracutaneous manifestations, such as abnormalities in the epithelial tissues and other organs, and may be associated with increased mortality.2 The prevalence of EB varies across countries, with a global estimate of 500,000 people living with the condition.3
EB is classified into four main types based on the level of skin cleavage: EB simplex (EBS), junctional EB (JEB), dystrophic EB (DEB) with recessive (RDEB) and dominant (DDEB) forms, and Kindler EB (KEB).4 Over 30 clinical subtypes have been identified, involving mutations in at least 21 different genes.4,5 Although blistering typically begins at birth or in early infancy, some cases may not clinically manifest until puberty or later.6 As several emerging therapies are under clinical development for severe subtypes of EB,7 current management remains primarily supportive and significantly impacts the daily lives of patients and their families.8
School attendance presents challenges for students with EB, who are at greater risk of psychosocial difficulties than their peers.9 Affected individuals report social isolation, lower school attendance, and reduced participation in school activities.10,11 Students with EB are sometimes perceived as having intellectual disabilities and may be more likely to experience bullying.9,12 Consequently, these challenges can severely affect their quality of life.13,14 Physical symptoms, such as visible skin wounds, extensive bandaging, persistent pain, and itching, can substantially impair concentration and contribute to significant distress during school days.15–18
It is imperative to understand the unmet needs of students with EB in the school environment. Adjusting the school environment to support students with EB may positively influence their school experience. Previous studies have addressed a range of challenges, from psychological burdens and family dynamics to school inclusion and peer relationships; however, targeted evidence concerning educational trajectories and support within academic environments remains sparse.9–14 The complex interplay of physical symptoms, emotional distress, altered self-image, and socioeconomic burden highlights the urgency for research focusing on the educational experiences of students with EB.9–14 Therefore, this study aimed to gain comprehensive insights into the perceptions of school climate among students with EB in Saudi Arabia and to examine factors influencing their school-related choices.
Materials and Methods
Study Design and Participants
This cross-sectional study evaluated the educational experiences of students with EB. All patients listed in the Saudi EB registry who met the inclusion criteria were invited to participate. Respondents were eligible if they were school-age or undergraduate students, diagnosed with any type of EB, and resided in Saudi Arabia. Informed consent was obtained prior to completing the questionnaire, and confidentiality and voluntary participation were ensured.
Survey Methods
Data were collected using a self-reported questionnaire (Table S1 and Table S2), which was developed based on a comprehensive literature review spanning psychosocial, educational, and functional challenges faced by individuals with EB.9,10,13,14,19 Additional data were collected during routine clinical care when patients and their parents expressed difficulties related to school attendance, physical functioning, psychosocial well-being, and financial burden. These complaints were documented during clinical encounters, thematically analyzed, and incorporated into the questionnaire design to ensure its relevance to real-life experiences.
The final survey method consisted of 23 items across five domains: physical, psychological, social, financial, and learning. The second section of the survey method focused on school preferences. Items were rated on a five-point Likert scale, with a “Not applicable” option included to reduce missing data. A pilot test was conducted with five participants who were selected using convenience sampling from the Saudi EB registry to assess the clarity, comprehension, and relevance of the questionnaire items. Necessary adjustments, including simplifying the language of some items and adding clarifying examples, were made based on the feedback.
The age of the participants was divided into six categories according to the Saudi Arabian school system: 3–5, 6–8, 9–11, 12–14, 15–17, and ≥18 years. Domain scores were calculated by summing the item responses within each domain. The total score was calculated by summing all domain scores and subsequently transforming it into a scale ranging from 0 to 100, with higher scores representing more negative perceptions or unmet needs regarding the school climate. The 23-item questionnaire demonstrated excellent internal consistency across all items (Cronbach’s α = 0.968).
Procedure
A list of eligible students with EB was retrieved from the Saudi EB database. Patients and their caregivers were invited to participate voluntarily. Although all eligible patients were approached, only a subset of them completed the questionnaire. An online link to the questionnaire was sent to participants via phone or email. Data were collected from the primary caregivers of patients under 18 years of age. The participants received an informed consent form, questionnaire, and clinical research form for demographic and clinical information. Data were collected from January 2024 to April 2024.
Ethical approval was obtained from the Institutional Review Board of Imam Mohammad Ibn Saud Islamic University (589/2023). This study adhered to the ethical principles outlined in the Declaration of Helsinki.
Data Analysis
Statistical analyses were performed using SPSS version 27. Continuous variables were reported as means and standard deviations, whereas categorical variables were reported as frequencies and percentages. To compare continuous variables among independent groups, the t-test, Mann–Whitney U-test, or Kruskal–Wallis test was used, depending on the data distribution. For categorical variables, the chi-squared test or Fisher’s exact test was used, as appropriate. Statistical significance was set at p<0.05. Due to the presence of only one participant with KEB, findings related to this subtype were excluded from the discussion and reported only in the tables for completeness.
Results
A total of 31 students with EB participated in the study, including 17 females (54.8%) and 14 males (45.2%). The most represented age group was 6–8 years (elementary school-aged children; 29%). Table 1 shows the demographic characteristics of the participants. The cohort included ten (32.3%) patients with EBS, seven (22.6%) with intermediate JEB, 11 (35.5%) with DEB (one DDEB and 10 RDEB), one (3.2%) with KEB, and two (6.5%) with an unknown type. EB subtypes were determined by clinical diagnosis confirmed through genetic blood testing. Most of the respondents were Saudi nationals (77.4%) from various regions of the country. More than half of the families (51.6%) reported annual incomes <32,000 United States dollar (USD). Most students (61.3%) were enrolled in public schools. Notably, 41.9% of students experienced delayed entry into elementary school because of their medical conditions.
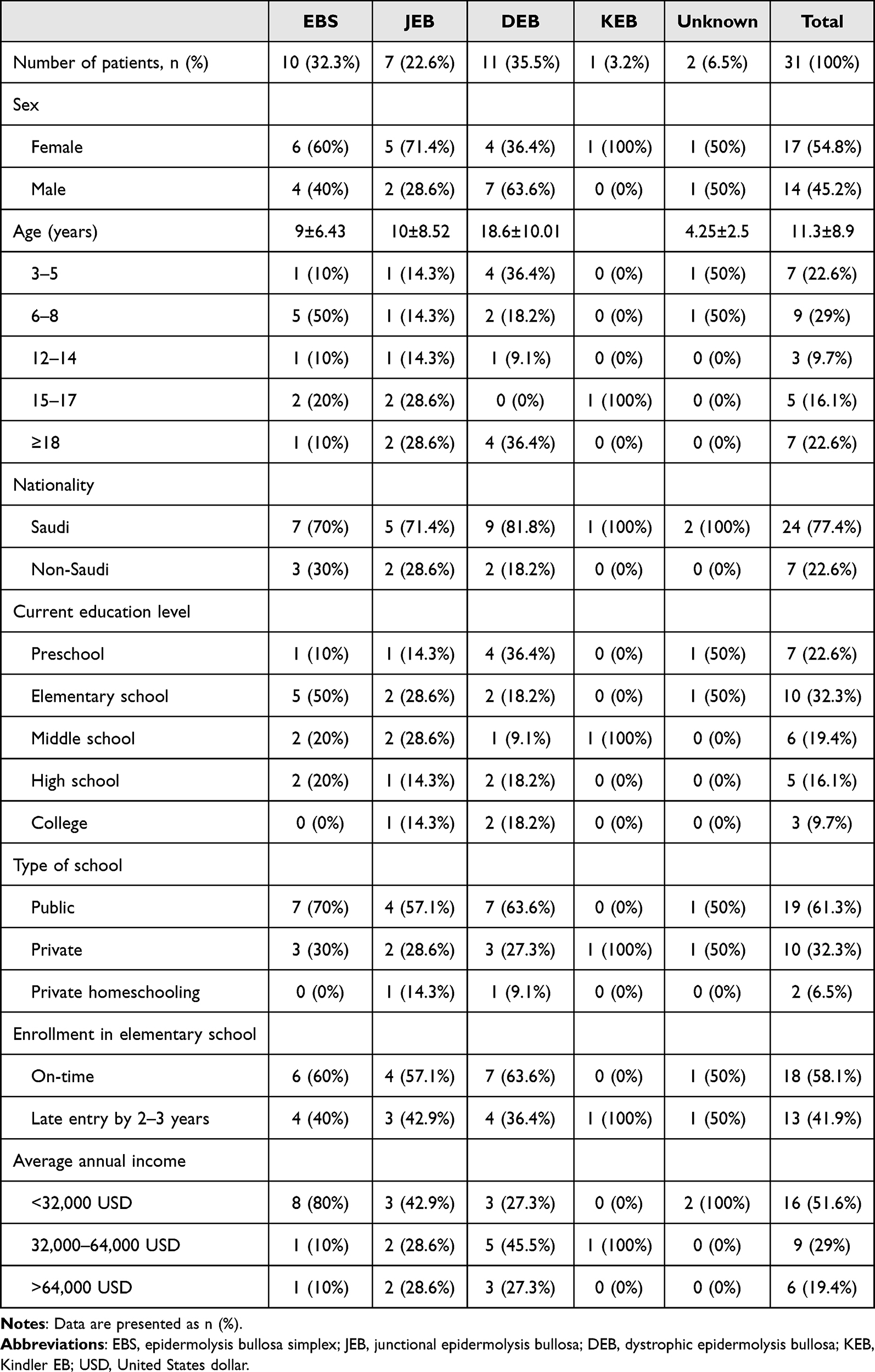 |
Table 1 Demographic and Clinical Characteristics of Students with Epidermolysis Bullosa |
Students with EB demonstrated an overall negative perception of school climate, with a mean total score of 58.5±14.3 (range, 35.3–89.7; Table 2). Students with JEB reported a lower perception of school climate than students with other subtypes. Students from families with annual incomes <32,000 USD had higher mean scores than those from families with higher incomes (61.3±15.4 versus 48.8±12.2). High school students reported more negative perceptions of school climate than younger students (77.1±11.3, p=0.012). Students who delayed entry into elementary school reported a lower perception of school climate than those who entered on time (64.5±13.4 versus 54.2±13.7).
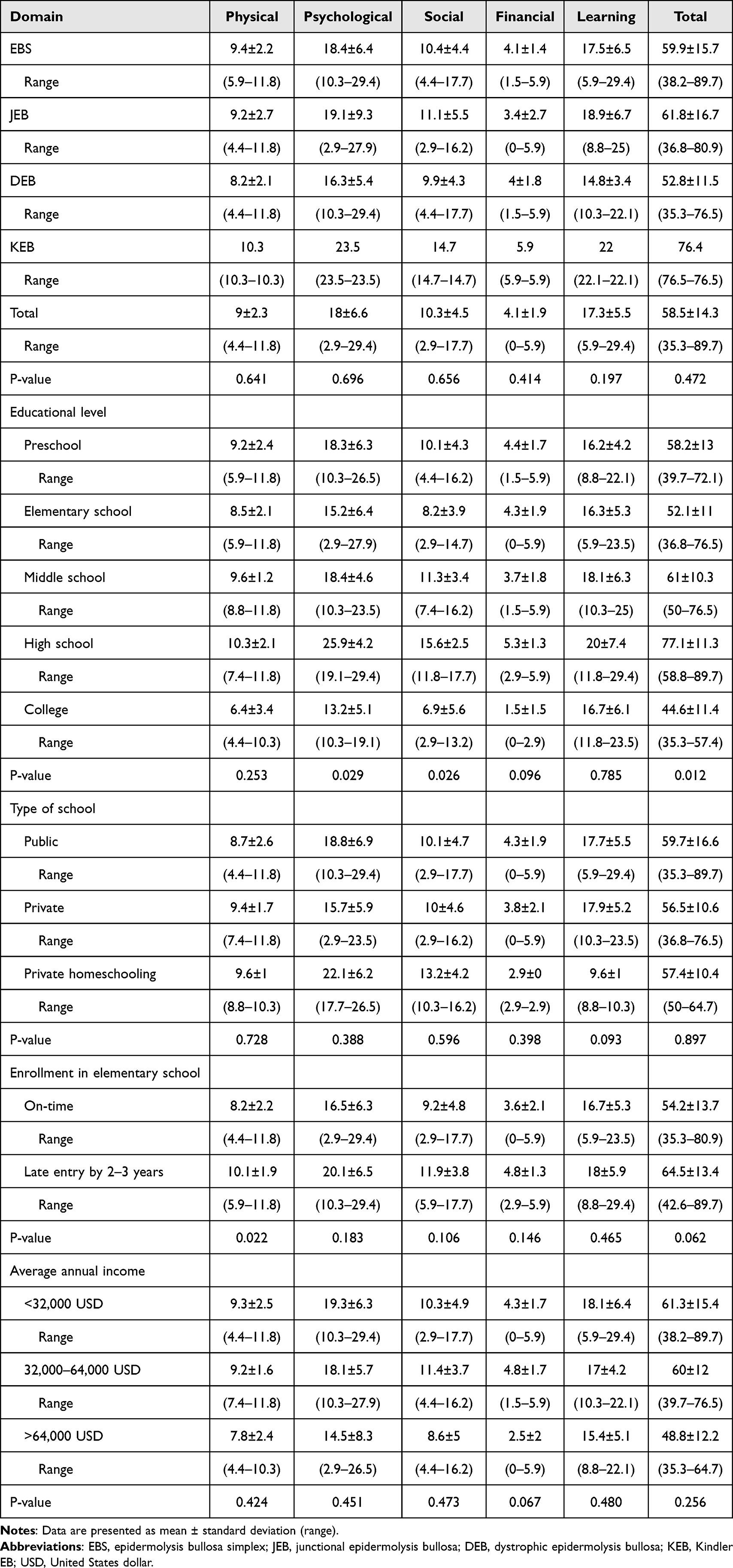 |
Table 2 Questionnaire Domain and Total Scores According to Baseline Characteristics and Epidermolysis Bullosa Subtypes |
Regardless of the EB subtype, most students with EB (87.1%) reported that it was consistently difficult to participate in physical education classes. The visibility of the disease was one of the greatest challenges, with 80.6% of students frequently or always trying to cover their wounds. Approximately half of the students with DEB experienced stigmatizing behaviors at school, such as being stared at. Overall, 22.6% reported being frequently or always bullied by others. More than one-third had difficulty maintaining friendships. Itching and pain were major social burdens, with 54.9% expressing fear of itchy or painful skin. Almost half of the participants indicated that others perceived them as having intellectual disabilities.
Most participants (58.1%) required extra lessons or online tutoring, which strained their family budget. Lower elementary and high school students were more likely to require additional lessons, at rates of 77.7% and 60%, respectively. Difficulty with handwriting was reported by 61.3% of students, and frequent school absences were noted in 51.6%.
Regarding school support, 54.8% of students valued the classroom adaptations they received; however, fewer than one-third of the participants received assistance with their basic and educational needs, such as feeding, safety, and writing. Homeschooled students had better learning domain scores (9.6±1) than those in private (17.9±5.2) or public (17.7±5.5) schools.
Regarding school preferences, approximately 75.8% of students agreed that school environments needed to be better adapted for students with EB (Figure 1). Social interactions with peers at school were considered essential. Approximately one-third of students preferred homeschooling and believed that it might improve their academic performance. Students who preferred homeschooling tended to have more severe subtypes (JEB or DEB, 70%) compared with those who had EBS (30%, Figure 2). Furthermore, 80% of students who preferred homeschooling were unable to register for home education programs.
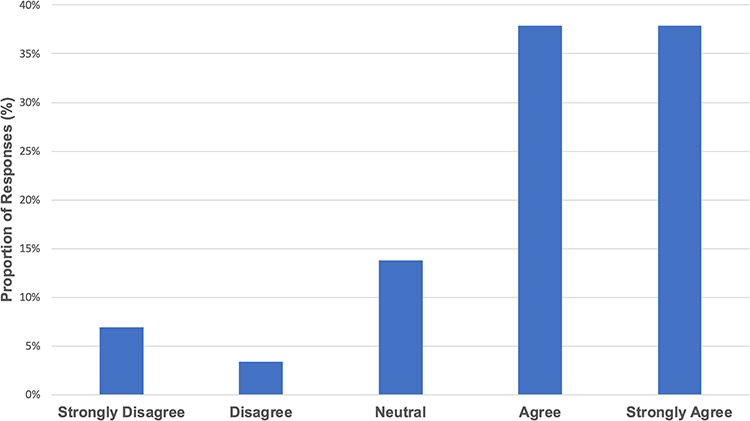 |
Figure 1 Responses of students with epidermolysis bullosa regarding the need for school environment adjustments. |
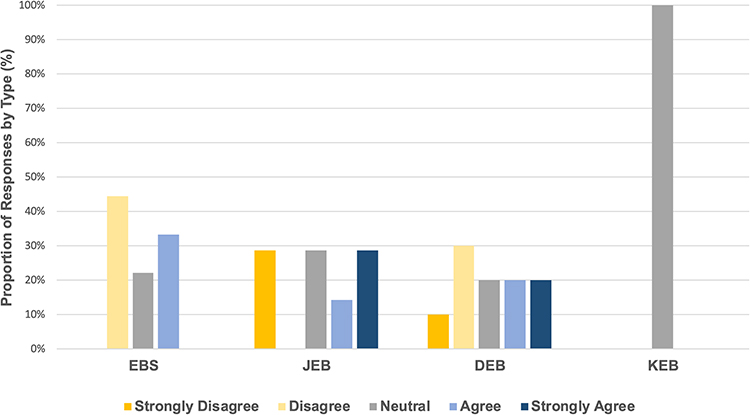 |
Figure 2 Perspectives of students with various types of epidermolysis bullosa regarding homeschooling. |
Discussion
School climate represents the academic, social, and emotional experiences of students, staff, and families.20 Few studies have addressed the educational challenges faced by patients with EB.9–14 In this study, we examined the perceptions of students with EB regarding school climate and their school preferences.
Our results showed that students with EB generally had an unfavorable perception of the school climate. Significant differences in educational experiences were observed across age groups, with old-for-grade students reporting more negative school experiences than on-time students. High school students aged ≥15 years reported more negative perceptions of school climate than younger students, which is consistent with the literature wherein adolescence is generally associated with increased self-consciousness.21 In a prior study, young patients with EBS experienced more psychosocial challenges during their transition into adulthood.8 Therefore, these findings highlight the need to provide targeted psychosocial support for adolescents with EB.22
The negative perception of school climate may be attributed to the unmet needs of students with EB. Our study revealed that students with EB often face challenges in their educational environments. Participants reported limited participation in school physical activities regardless of EB type, consistent with previous reports showing that people with any type of EB can experience restrictions in physical activity owing to the risk of blistering.22,23 Encouraging safe and inclusive participation in physical education classes is supported by current best clinical practices for individuals with EB.24
Most participants reported that their condition impaired their social networks at school, and 54.9% indicated that skin pain and itching negatively affected friendships. A study assessing major problems in children with EB revealed that pain and itching were associated with a higher social burden.12 Frequent school absences and difficulties with handwriting were also noted. A previous study showed that 55% of children with RDEB have some difficulty with handwriting.19 A significant burden was also observed among students with visible EB wounds. As a result, students with EB were perceived to have intellectual disabilities and experienced self-concealment, bullying, and stigmatization. The findings of our study align with a qualitative interview of eight participants with EB, who reported frequent peer victimization and were misperceived as having intellectual disabilities; thus, educating teachers, school personnel, and peers about EB is essential.9 Educational programs should promote awareness regarding EB and clarify that it does not affect cognitive abilities.9,14
We found that students with EB were more likely to require additional lessons and online tutoring, adding financial strain to their families. Students from families with annual incomes <32,000 USD reported more negative perceptions of school climate than those from higher-income families, underscoring the socioeconomic burden of EB.
Students with more severe diseases (JEB or DEB) preferred homeschooling over traditional education. Challenges such as time-intensive wound care, chronic pain, itching, and frequent medical appointments contribute to school absenteeism. These findings demonstrate that students with EB face various educational demands that require adjustments to the school environment. The social impact of EB is clear; thus, efforts to encourage social interactions with peers are necessary. Educating teachers and classmates about EB is a key step toward fostering inclusion. Educational resources to support students with EB in school settings should be made available and used.25 Students with EB should receive sufficient support, particularly during the transition phases. School facilities should be made accessible to students with EB to improve their learning experiences. Students with EB may experience limitations in activities of daily living; thus, appropriate assistance that promotes independence should be provided. Adjustments related to handwriting—such as extended time, multiple breaks, and adapted writing tools—can support the autonomy of students with EB. The findings also indicated that students with severe subtypes of EB may benefit from homeschooling, either full-time or in combination with in-school teaching, according to their needs.
This study has some limitations. First, most questionnaires were completed by caregivers rather than by the students themselves. Proxy reporting may not fully capture the perceptions and lived experiences of the students, particularly in subjective areas such as peer relationships and emotional well-being. Second, the use of self- or proxy-reported questionnaires may not capture the full spectrum of experiences among students with different EB subtypes. Third, the small sample size, reflecting the rarity of the disease, limited the statistical power and representativeness of the findings. Moreover, the uneven distribution of EB subtypes further constrains the generalizability of the results. Subtypes with very low representation were not discussed separately in the main text to avoid overinterpretation. Further studies addressing these limitations are needed to validate our findings.
Conclusion
Students with EB face significant educational challenges due to their unmet physical, social, and educational needs. Based on our findings, we recommend that educational institutions implement a multifaceted support framework encompassing dedicated psychosocial support; targeted education and awareness programs for staff and peers; inclusive physical education activities; flexible academic accommodations, including handwriting support and accessible facilities; exploration of flexible educational delivery models, such as homeschooling for severe cases; and efforts to address financial barriers to academic support. Further research is needed to investigate additional challenges and necessary adjustments in the school environment to better meet the needs of students with EB and to evaluate the effectiveness of these interventions.
Acknowledgments
We are grateful to all the participants for their contributions to this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Fine JD, Bruckner-Tuderman L, Eady RA, et al. Inherited epidermolysis bullosa: updated recommendations on diagnosis and classification. J Am Acad Dermatol. 2014;70(6):1103–1126. doi:10.1016/j.jaad.2014.01.903
2. Fine JD, Mellerio JE. Extracutaneous manifestations and complications of inherited epidermolysis bullosa: part I. Epithelial associated tissues. J Am Acad Dermatol. 2009;61(3):367–384;quiz385–386. doi:10.1016/j.jaad.2009.03.052
3. Featherstone C. Epidermolysis bullosa: from fundamental molecular biology to clinical therapies. J Invest Dermatol. 2007;127(2):256–259. doi:10.1038/sj.jid.5700731
4. Has C, Bauer JW, Bodemer C, et al. Consensus reclassification of inherited epidermolysis bullosa and other disorders with skin fragility. Br J Dermatol. 2020;183(4):614–627. doi:10.1111/bjd.18921
5. Has C, Liu L, Bolling MC, et al. Clinical practice guidelines for laboratory diagnosis of epidermolysis bullosa. Br J Dermatol. 2020;182(3):574–592. doi:10.1111/bjd.18128
6. Fine JD. Inherited epidermolysis bullosa. Orphanet J Rare Dis. 2010;5(1):12. doi:10.1186/1750-1172-5-12
7. Goldschneider KR, Good J, Harrop E, et al. Pain care for patients with epidermolysis bullosa: best care practice guidelines. BMC Med. 2014;12(1):178. doi:10.1186/s12916-014-0178-2
8. Hou PC, Wang HT, Abhee S, Tu WT, McGrath JA, Hsu CK. Investigational treatments for epidermolysis bullosa. Am J Clin Dermatol. 2021;22(6):801–817. doi:10.1007/s40257-021-00626-3
9. Sangha N, MacLellan AN, Pope E. Psychosocial impact of epidermolysis bullosa on patients: a qualitative study. Pediatr Dermatol. 2021;38(4):819–824. doi:10.1111/pde.14656
10. Williams EF, Gannon K, Soon K. The experiences of young people with epidermolysis bullosa simplex: a qualitative study. J Health Psychol. 2011;16(5):701–710. doi:10.1177/1359105310387954
11. Fine JD, Johnson LB, Weiner M, Suchindran C. Impact of inherited epidermolysis bullosa on parental interpersonal relationships, marital status and family size. Br J Dermatol. 2005;152(5):1009–1014. doi:10.1111/j.1365-2133.2004.06339.x
12. van Scheppingen C, Lettinga AT, Duipmans JC, Maathuis CG, Jonkman MF. Main problems experienced by children with epidermolysis bullosa: a qualitative study with semi-structured interviews. Acta Derm Venereol. 2008;88(2):143–150. doi:10.2340/00015555-0376
13. Bruckner AL, Losow M, Wisk J, et al. The challenges of living with and managing epidermolysis bullosa: insights from patients and caregivers. Orphanet J Rare Dis. 2020;15(1):1. doi:10.1186/s13023-019-1279-y
14. Barbosa NG, Silva CB, Carlos DM, Brosso L, Levada AF, Okido ACC. School inclusion of children and adolescents with epidermolysis bullosa: the mothers’ perspective. Rev Esc Enferm USP. 2022;
15. Adni T, Martin K, Mudge E. The psychosocial impact of chronic wounds on patients with severe epidermolysis bullosa. J Wound Care. 2012;21(11):528,530–536,538. doi:10.12968/jowc.2012.21.11.528
16. Fine J-D, Johnson LB, Weiner M, Suchindran C. Assessment of mobility, activities and pain in different subtypes of epidermolysis bullosa. Clin Exp Dermatol. 2004;29(2):122–127. doi:10.1111/j.1365-2230.2004.01428.x
17. Brun J, Chiaverini C, Devos C, et al. Pain and quality of life evaluation in patients with localized epidermolysis bullosa simplex. Orphanet J Rare Dis. 2017;12(1):119. doi:10.1186/s13023-017-0666-5
18. Chateau AV, Blackbeard D, Aldous C, Dlova N, Shaw CM. Lived experiences of patients with epidermolysis bullosa: a rare genetic skin disease. Health SA. 2024;29:2824. doi:10.4102/hsag.v29i0.2824
19. Eismann EA, Lucky AW, Cornwall R. Hand function and quality of life in children with epidermolysis bullosa. Pediatr Dermatol. 2014;31(2):176–182. doi:10.1111/pde.12262
20. Thapa A, Cohen J, Guffey S, Higgins-D’Alessandro A. A review of school climate research. Rev Educ Res. 2013;83(3):357–385. doi:10.3102/0034654313483907
21. Bowker JC, Rubin KH. Self-consciousness, friendship quality, and adolescent internalizing problems. Br J Dev Psychol. 2009;27(Pt 2):249–267. doi:10.1348/026151008x295623
22. Martin K, Geuens S, Asche JK, et al. Psychosocial recommendations for the care of children and adults with epidermolysis bullosa and their family: evidence based guidelines. Orphanet J Rare Dis. 2019;14(1):133. doi:10.1186/s13023-019-1086-5
23. Horn HM, Tidman MJ. Quality of life in epidermolysis bullosa: quality of life in epidermolysis bullosa. Clin Exp Dermatol. 2002;27(8):707–710. doi:10.1046/j.1365-2230.2002.01121.x
24. Weisman A, Chan JM, LaPointe C, et al. Physiotherapy for epidermolysis bullosa: clinical practice guidelines. Orphanet J Rare Dis. 2021;16(1):406. doi:10.1186/s13023-021-01997-w
25. School resources. Debra.org. Available from: https://www.debra.org/other-resources/school-resources.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Determinants of Knowledge of Musculoskeletal Disorders Among Healthcare Providers and Students in Saudi Arabia: A Cross-Sectional Study
Alrwaily M, Alanazi F
Journal of Multidisciplinary Healthcare 2022, 15:1789-1797
Published Date: 25 August 2022
Experience and Perception of Healthcare Workers on the Challenges of Follow-Up and Treatment of Tuberculosis Patients in Southern Ethiopia: An Exploratory-Descriptive Qualitative Study
Abebe A, Nuriye S, Baza D, Markos M, Woldeyohanes S, Gelgelu TB
Risk Management and Healthcare Policy 2022, 15:1931-1945
Published Date: 12 October 2022
Are We Scared of Clinical Trials if Not Sufficiently Informed and Educated?
Burnazovic-Ristic L, Todic A, Maleskic Kapo S, Kusturica J, Kulo Cesic A, Loga-Zec S, Aganovic-Musinovic I, Rakanovic-Todic M
Advances in Medical Education and Practice 2022, 13:1359-1366
Published Date: 27 October 2022
Patient’s Perceptions and Attitudes Towards Medical Student’s Involvement in Their Healthcare at a Teaching Hospital in Jordan: A Cross Sectional Study
Taha HA, Al Saqer JK, Al Harbi NR, Younis RN, Al Dawoud F, Nawaiseh MB, Berggren V
Patient Preference and Adherence 2023, 17:629-641
Published Date: 13 March 2023
Saudi Women’s Views on Healthcare Leadership in the Era of Saudi 2030 Health Transformation
Aldekhyyel RN, Alhumaid N, Alismail DS
Journal of Multidisciplinary Healthcare 2024, 17:237-249
Published Date: 16 January 2024