")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Saudi Women’s Views on Healthcare Leadership in the Era of Saudi 2030 Health Transformation
Authors Aldekhyyel RN , Alhumaid N, Alismail DS
Received 7 September 2023
Accepted for publication 4 December 2023
Published 16 January 2024 Volume 2024:17 Pages 237—249
DOI https://doi.org/10.2147/JMDH.S439146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Raniah N Aldekhyyel,1 Nuha Alhumaid,2 Dina S Alismail3
1Medical Informatics and E-Learning Unit, Medical Education Department, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2College of Public Health and Health Informatics, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 3Learning and Innovation, The Healthcare Leadership Academy, Saudi Commission for Health Specialties, Riyadh, Saudi Arabia
Correspondence: Raniah N Aldekhyyel, Medical Informatics and E-learning Unit, Medical Education Department, College of Medicine, King Saud University, Riyadh, 12372, Saudi Arabia, Tel +966 11 8066580, Email [email protected]
Introduction: Saudi Vision 2030 emphasizes women’s empowerment and their increased participation in the workforce, particularly in healthcare. This study explores perceptions of Saudi women healthcare practitioners in leadership roles across various healthcare settings.
Methods: A national cross-sectional online survey was conducted, guided by the Leadership Effectiveness Model. It assessed the perceptions of Saudi women health practitioners in leadership positions within the country’s healthcare context. Survey questions were adapted from validated surveys. Women classified as “Consultants” by the Saudi Commission for Health Specialties were invited to participate. Descriptive statistics and content analysis were used for analysis. A total of 119 Saudi women consultants participated.
Discussion: Most were physicians (85%) in the Western region (46%) and reported being in leadership roles. Leadership positively impacted their career growth but negatively affected leisure activities. Career progression challenges included further studies (35%) and work-life balance (31%). Leadership commitment to supporting women was seen as crucial (63%). Analysis of responses to Vision 2030 yielded themes like “advancement”, “opportunities”, and “empowerment”. Saudi Vision 2030, combined with evolving organizational cultures and policies, is creating opportunities for women to excel in leadership roles.
Conclusion: National strategies, combined with workplace norm changes and supportive policies, can foster greater representation of qualified women in elite healthcare leadership positions.
Keywords: healthcare transformation, leadership, perception, challenges, Saudi Arabia
Background
The topic of women in healthcare leadership has been the focus of many organizations across the globe, specifically studying the factors that may contribute to the underrepresentation of women in such roles. According to the recent reports published by McKinsey and Company1 and Oliver Wyman,2 there is an underrepresentation of women in senior-leadership positions in the healthcare industry. These reports mainly focused on the current state of women in healthcare leadership in the United States while exploring two main factors: (1) the unique challenges and barriers that women face and (2) recommendations on how to increase women representation in a traditionally male-dominated field. Many research studies have also been designed to explore women challenges and barriers to career progression in the healthcare industry across different countries. Kalaitzi et al explored women healthcare leaders’ perceptions on the barriers to leadership in a Greek context.3 Banerjee et al published the results of a national survey in Europe designed to highlight the challenges facing women oncologists in career development and achieving leadership roles.4 Global organizations that publish articles and develop specific executive leadership training programs to support women in leadership positions play an essential part in the efforts toward increasing women’s representation in senior leadership roles across all industries. The Harvard Business Review5–8 published a series of articles specifically highlighting gender and leadership in the healthcare industry to spread awareness around the topic and address the unique challenges women face in the industry.
In Saudi Arabia, there is scarcity in research studies that focus on women’s experiences in the healthcare workplace. This scarcity has been an area of focus by some researchers and has driven them to explore women’s rights in the field of medicine,9 describe young women student experiences in pursuing a career in science and technology,10 examine the role of women in medical education,11 and explore the careers and lived experiences of women in the fields of science and technology.12,13 While these research papers have specifically focused on the experiences of women in education, training, and career development, specific research is needed to explore the experiences of women in managerial and leadership positions in the field of healthcare. Women in leadership positions, may potentially have different types of experiences to share, as indicated by Burke, in a recent study conducted across five countries.14
Undergoing transformations since the launch of the country’s 2030 Vision in 2016, the Kingdom of Saudi Arabia is actively progressing towards its set national vision plans. This comprehensive initiative covers 11 Vision Realization Programs, including the National Transformation Program, which specifically targets enhancing women’s participation in the labor market.15 The overarching objectives include elevating the percentage of women in the workforce, currently at 38% as of the second quarter of 202316 and promoting a supportive work environment to increase women’s representation in managerial positions. In line with these national goals, the Saudi Commission for Health Specialties released the 2017–2020 strategic plan identifying two key change themes: (1) diversity and flexibility in the workplace and (2) creating future leaders.17 This was translated through the establishment of the Healthcare Leadership Academy in 2017.18 Other national organizations, such as the Ministry of Health, have also announced their strategic objectives in line with the 2030 Vision.19
Saudi women healthcare practitioners in leadership positions are part of the workforce that will lead the healthcare transformation initiative in the country. Understanding the perceptions of these women and their challenges will advance the field and strengthen implementation of these initiatives. This research is focused on Saudi Arabia and is driven by the country’s 2030 Vision with the objective to address the gap in research studies that focus on exploring women’s perceptions in leadership positions within the healthcare sector.
Theoretical Model
Our study is guided by the work of the authors Crystal L. Hoyt and Stefanie Simon addressing gender and leadership, in Northouse’s book Leadership: Theory and Practice.20 The authors argued that effective women leadership should be promoted within a multi-level approach, encompassing individual, interpersonal, organizational, and societal levels. Understanding the many components of this approach addresses bigger, more substantial perceptions about gender and social systems across different cultures. A number of factors, strategies, and policies exist within each and every one of these levels. Examples of individual-level factors include the use of effective leadership styles and enhancing women’s negotiation power, while interpersonal-level factors focus on decreasing gender stereotypes. Organizational-level factors for instance include women’s career development, work-life support, and supporting mentoring relationships. The societal level focuses on changes to the distribution of domestic duties to reach gender equity.
As many organizations are changing their culture towards valuing flexible staff and diversity in their top positions, greater gender equity and representation of women is likely to be achieved. Much of the research exploring gender in leadership has taken place in Western contexts. Research on gender and leadership in other contexts is scarce. Understanding the culture and how women are seen in a certain society, informs the research done in the area of gender and leadership and how these four multi-levels intertwine to promote leadership effectiveness.20 This research aims to explore Saudi women health practitioners’ perceptions across different healthcare work environments in leadership positions, from an organizational-level approach. We aim to explore the following factors: career development, work-life support, and perceived challenges to women leadership advancement within the country’s healthcare context.
Materials and Methods
Survey Design and Procedures
This was a cross-sectional study capturing the perceptions of Saudi women healthcare practitioners in leadership positions in Saudi Arabia using an online survey instrument. The instrument was designed based on questions that were adopted from several validated surveys,3,4 literature findings,21,22 and the expertise of the research team. To ensure the reliability and validity of our survey instrument, a comprehensive process was undertaken. First, the survey underwent rigorous analysis through an expert review. We collected the opinions of three subject matter experts who assessed the content, cognitive, and usability aspects of the instrument. Their feedback guided us in refining and improving the survey questions to align more closely with our research objectives. Following the expert review, a pilot study was conducted involving 10 experts in the relevant field. The pilot study aimed to evaluate the survey questions in a real-world context and gather feedback from those with direct expertise. The feedback received from the pilot study participants was carefully analyzed, leading to further adjustments to the survey questions. This iterative process enhanced the survey’s reliability and validity by aligning it with expert perspectives.
The survey instrument was developed to capture closed-ended and free-text responses. Google form23 was used to design the survey instrument, which included 3-point and 5-point Likert scales and item lists to collect participant responses. The survey was divided into four main sections to capture demographic information, leadership background information, perceptions regarding the impact of a career on personal life and career choices, challenges and suggestions for overcoming challenges, and the meaning of the country’s 2030 vision (free text).
We structured the survey into several sections to capture a wide range of information from participants. The first section focused on demographics, gathering details such as age, marital status, and the number of children, if any. The second section gathered information related to the participants’ leadership background, including their educational degrees, specialties, workplace settings, types of leadership training, years of experience, and current leadership positions.
The third section, which explored the impact of leadership roles on personal life and career choices, employed a combination of closed-ended and open-ended questions. Participants were asked to indicate the positive or negative impact of their leadership roles on various aspects of their lives, such as friends, family, marriage, children, social obligations, leisure activities, personal growth (including continuous education and training), and clinical career growth. Additionally, they were asked to rate the level of impact on these aspects. An open-ended question encouraged participants to identify any other areas of their lives affected by their leadership roles.
In the fourth section, we addressed the challenges participants faced in their career progression and sought suggestions for overcoming these challenges. The challenges were measured using closed-ended questions with a 5-point Likert scale, asking participants to rate the impact of factors like work-life balance, long working hours, family support, childcare responsibilities, further studies, family obligations, maternity leave, marriage, marriage stability, having children, and cultural restrictions. An open-ended question invited participants to share any additional factors affecting their career choices. We also inquired about approaches to increasing the representation of women in healthcare leadership positions using a closed-ended, checkbox format question, with an option to add other suggestions.
Finally, the fifth and last section of the survey was dedicated to an open-ended question: “What does the country’s Vision 2030 mean to you?” This question allowed participants to express their thoughts and sentiments regarding this vision.
Recruitment
In December 2021, following institutional review board approval from the Saudi Commission for Health Specialties, we collaborated with the Commission’s Data Governance Department to send email invitations to women meeting our sample criteria “Saudi women healthcare practitioners registered as healthcare Consultants” via their demographic classification system database. Due to confidentiality policies governing database access, we, as researchers, were unable to directly access the sample. To address the need for the most current information on the “Consultant” position within the database, we included a self-identification statement in the invitation email, asking participants to confirm their leadership roles within healthcare organizations or academic health colleges. The Data Governance Department facilitated the distribution of email invitations, which included a consent to participate in the study and the survey link. To enhance responses, reminder emails were sent approximately 1, 2, and 3 weeks after the initial invitation. Given the limited pool of Saudi women healthcare practitioners in leadership positions,24 a challenge also observed globally,25,26 our sample size was smaller than ideal. This limitation was also combined with our inability to directly access the sample database, as indicated by confidentiality policies managed by the Saudi Commission for Health Specialties, preventing us from calculating the response rate. Upon completion of the survey, participants were given an option to receive a free virtual leadership training session sponsored by the Healthcare Leadership Academy.
Data Analysis
No questionnaires were excluded from the analysis due to incomplete answers. For closed-ended responses, data analysis was carried out using SPSS 21.0. Descriptive statistics (frequencies and percentages) were calculated to characterize study variables. The free-text responses were subjected to a content analysis aimed at identifying dominant themes related to the specific questions.
Results
Demographics
In total, 119 replies were received. Most participants were 51 years old or older (27%), followed by 36 to 40 years old (26%). Most participants were married (61%), have children (66%), and have 3–4 children (34%). The top three work settings the participants worked at were the Ministry of Health (31%), followed by private hospitals (21%), and governmental hospitals (16%). Most participants (46%) were located in the Western and the Central region (32%). (Table 1).
 |
Table 1 Participant demographics |
Career and Leadership Background
The majority of participants were physicians, representing 85% of the sample. The participants exhibited a diverse range of work experience, with 8% having five years or less and 23% holding 26 years or more. A notable percentage (26%) held a master’s degree. More than half of the participants (56%) were in leadership positions during the study period, and approximately 38% reported having received leadership training. Among those in leadership roles, 27% had between 1 and 2 years of experience (Table 2).
 |
Table 2 Career and Leadership Background |
Leadership Impact
When asking the participants to indicate whether their leadership role had a positive, negative, or no impact on specific areas, such as career growth, clinical career growth, friends, family, children, marriage, leisure activities, and social obligations, the top positive impact of a leadership role indicated by participants was career growth (60%). The most negatively impacted areas cited by participants were leisure activities (55%) and social obligations (54%), while the most mentioned areas having no impact were marriage (58%) and children (54%) (Figure 1).
 |
Figure 1 Impact of leadership positions (n=119). (participants could choose more than one option. Answers “missing/not applicable” were excluded). |
The participants were asked an open-ended question, which stated “Is there any other area in your life, which you feel was impacted by your career in a leadership role?” We obtained 16 free-text answers, which resulted in eight new areas identified to have had an impact by the being in a leadership role. The new identified areas include time with children, finance, personal development, physical activity/exercise, research, stress, teaching, and health including physical and mental. Health was the most occurring theme, followed by stress, and physical activity/exercise.
Challenges Towards Career Progression
Participants’ challenges for career progression were assessed by having them indicate the degree of impact on a 5-point Likert scale (ranging from extremely to not at all) in specific areas affecting their career choices. Balancing work and life emerged as the most extremely impacting factor on participants’ career choices, with a percentage of 31%. Pursuing further studies was identified as the most “considerably” impacted area, accounting for 35%. Having children was reported to have a “somewhat” impact on career choices (31%), while cultural restrictions emerged as the most “non-impacted” area on career choices, constituting 44% (Figure 2).
 |
Figure 2 Areas impacting career choices (n=119). (participants could choose more than one option. Answers “missing/not applicable” were excluded). |
Additionally, participants were asked an open-ended question: “Is there anything else that you feel impacted your career choices?” In response, we received 11 answers, five of which introduced new topics, including night shifts, organizational culture, competition, and passion.
Approaches to Increasing Women Representation
Figure 3 shows the approaches to increasing women representation in healthcare leadership positions as suggested by the participants. Results show that leadership commitment to supporting women in leadership positions was the single most important approach to increasing women healthcare practitioners’ representation in leadership positions (63%). Promoting women role models in healthcare was cited by the participants as the least approach to increasing women representation in healthcare (34%).
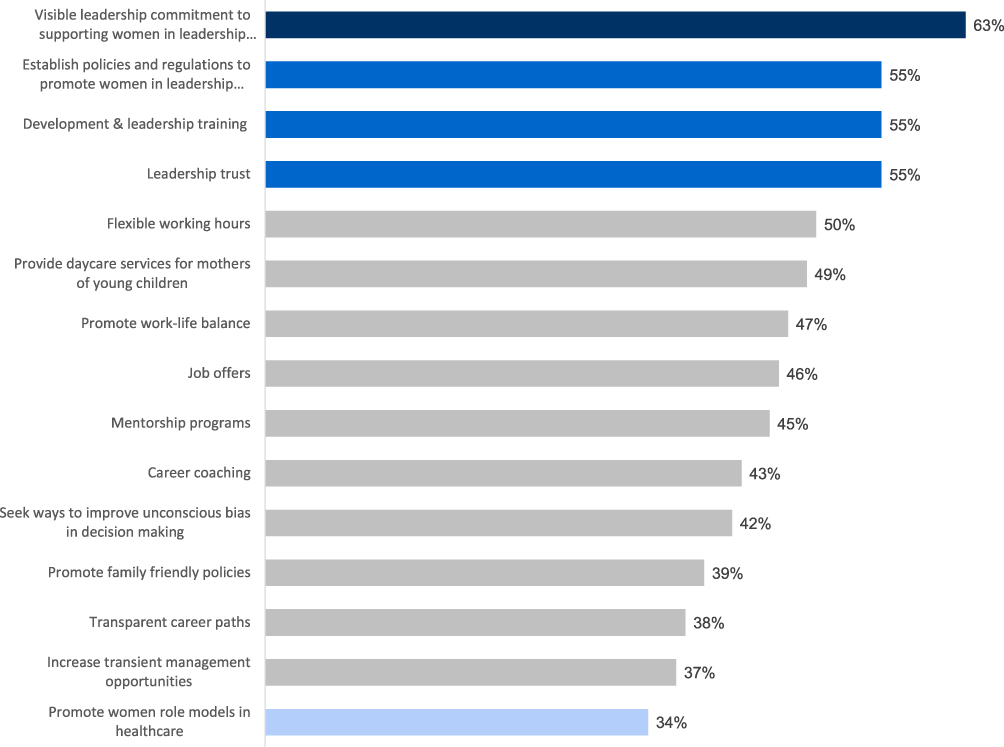 |
Figure 3 Approaches to increasing women representation in healthcare leadership positions (n=119). (participants could choose more than one option. Answers “missing/not applicable” were excluded). |
Table 3 presents the content analysis results for the question “What does the country’s Vision 2030 mean to you?” A total of 115 responses were obtained and analyzed, revealing nine distinct themes. The top three occurring themes were “advancement” (n=50), “opportunities” (n=28), and “empowerment” (n=20). The theme “advancement” included statements that reflected development, improvement, innovation, better future, and better health. “Opportunities” theme included statements that reflected opportunities, leadership opportunities, opportunities for woman, and opportunities for both men and woman. Others have answered the question with few words stating that the Vision 2030 means to them, such as “freedom”, and “a dream come true”.
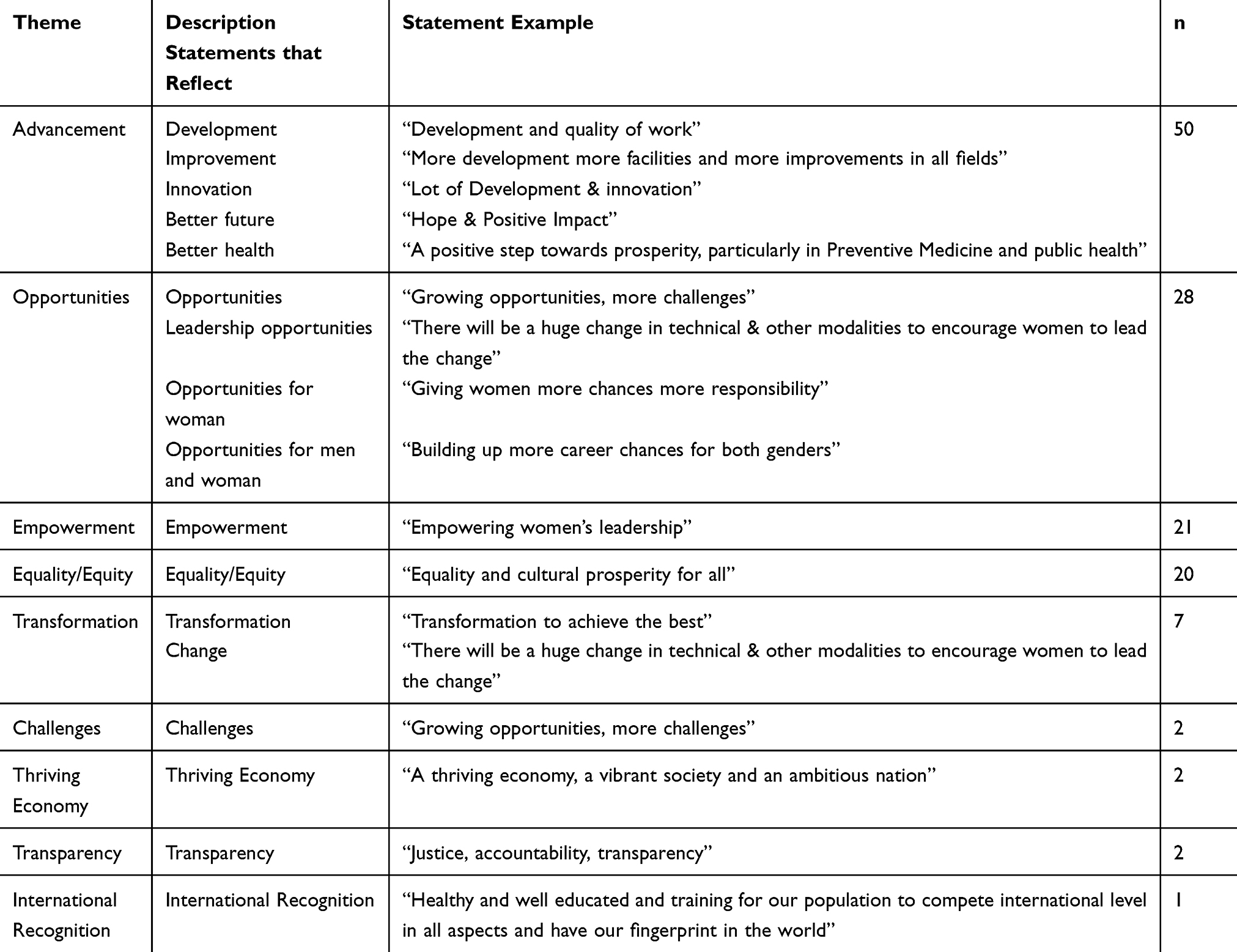 |
Table 3 Meaning of the Country’s 2030 Vision |
Discussion
The advancement of women in leadership in the health sector and beyond can be addressed on several levels: individual, interpersonal, organizational and societal levels. Our study aimed at exploring the perceptions of women health practitioners as leaders in Saudi Arabia, to understand how organizational factors are conceptualized and perceived by these women. Our data was gathered from Saudi women consultants working in leadership positions. Almost a third of these women were 36 to 40 years old, and about two-thirds had four years or less of leadership experience. These findings likely reflect the recent governmental support and advancement that is transforming women’s roles as leaders in a number of sectors in the country including the healthcare sector, where more women, especially younger ones, are leading organizations at different leadership levels.
When exploring social and family-related aspects/factors and how they are linked to women’s perceptions in leadership roles, our findings indicated that women’s leadership career choices were highly affected by factors related to balancing work and life, caring for children, and maternity leave policies. Participants also emphasized that being in leadership positions can and has negatively affected their social obligations. Such findings were not surprising, since it was found in previous studies that although early career men and women doctors progress similarly in their early career stages, women are five times more likely to have career distractions that are family related, which significantly impact their career advancement.26 In addition, several studies indicated that work-life balance, a significant factor for career progression of women leaders, was improved by family-friendly policies and incentives in healthcare organizations, especially with high levels of policy awareness and active implementation of such strategies and policies.27–29 We therefore recommend the active integration of family friendly policies and regulations that help women leaders with work-life balance, as it is a significant organizational factor that should constantly be initiated and revisited in the Saudi healthcare sector to better serve and support women leaders in healthcare.
Increasing Saudi women’s representation in healthcare leadership is key to the country’s movement towards empowerment and equal opportunities. Our participants perceived leadership commitment to support women in leadership, having policies and regulations that promote and support women in their leadership journey, and the trust of higher leadership in women leaders to be significant factors that promote effective women leadership. As discussed in Hoyt and Simon’s model, these factors fall mainly under the organizational level. According to the authors, recent changes in organizations are paving the way for women to reach top positions. For example, many organizations are adopting flexible working hours and diversity in their top positions, providing work-life support, and offering career development programs for women.21 The Saudi Arabian Labor Law, for example, indicated that women workers are entitled to ten weeks maternity leave fully paid. Marriage and mourning leave due to death of an immediate family member has been adjusted in 2016 to be increased from three to five days.30 Our findings support cultural shifts in organizations and policy initiation that ensure Saudi women have equivalent opportunities in reaching leadership positions in the healthcare sector.
Leadership development and training were also found to be key elements that Saudi women believed would help them become effective leaders. Previous studies demonstrated comparable findings, emphasizing the significance of leadership development and training programs which offer both short- and long-term benefits for women in healthcare leadership.31–35 Systematic reviews of interventions that advance women in healthcare leadership concluded that implementing effective, affordable, and evidence-based leadership development programs, would have the potential to improve competencies and core skills of leaders, leading to improved individual and organizational objectives in gender equity.36
Several organizations in the country have launched training programs specifically designed for training current and future leaders to reach their highest potential. The Healthcare Leadership Academy, for example, was established in 2017 to play an essential role in leading the healthcare transformation with the aim of developing present and emerging leaders within the healthcare system and equip them with the managerial and leadership skills required to support health transformational initiatives in the country.17 Another example is the 2030 Leaders program. A nine-month comprehensive leadership development program delivered by Misk Foundation.37 While these programs are designed for both genders, The Qiyadat Global - GeorgeTown is unique in that it’s focus is on developing leadership skills for women leaders in collaboration with Georgetown University’s McDonough School of Business in the United States.38
It was interesting to see that women in our sample found promoting women role models to have minimal effects on their leadership representation, while other studies indicated that promoting women role models to be an effective strategy that advance women in leadership.36 It is of importance to understand how Saudi women leaders use mentors to guide their own development. Do they seek mentors from a variety of domains or from a single ideal match with themselves?39 Understanding Saudi women leaders’ approach towards mentorship within the healthcare field may shed light on why the women in our sample found role models to have minimal effect on their advancement.
In this study, we comprehensively explored Saudi women health practitioners’ perceptions in leadership positions across diverse healthcare work environments, with a specific focus on organizational-level factors. This research carries significant implications. It provides insights for policymakers, supporting informed decisions to promote gender diversity and women’s leadership in healthcare, aligning with the objectives of the Saudi Vision 2030 for increased women’s representation in leadership positions. Understanding career development, work-life balance, and the unique challenges women face in leadership roles can lead to improve workplace environment. The study motivates future research and may potentially inform tailored leadership development programs. On a global context, our research findings may provide a foundation for comparisons when it comes to gender diversity in the healthcare workplace.
Future studies should focus on incorporating a multifaceted in-depth examination of career development, work-life support, and the perceived challenges to women’s leadership advancement. Research should also consider their experiences during critical events, such as the COVID-19 pandemic, building on the foundation laid by previous studies in this area.40–42 Investigating deeper into different predictors, alongside studying the individual, interpersonal, and societal layers20 contributing to effective leadership within the unique Saudi Arabian context, is essential for a more comprehensive understanding of the culture of gender and leadership dynamics. Such research initiatives are expected to enhance our insights into the experiences of Saudi women health practitioners in leadership roles, aligning with the goals of the Saudi 2030 Vision, and providing valuable insights for creating strategies to promote women’s leadership within the healthcare sector.
Limitations
Limitations of this study include the relatively small sample size of the participants, and our inability to calculate the participants’ response rate. With the low number of women in leadership positions in different sectors,43,44 our study aim was focused on exploring the perceptions of women in healthcare, representing a small sample within the country. Although we intended to be as systematic as possible in reaching as many Saudi women consultants in leadership positions as we could, the responses were limited to those women who self-identified as “holding a leadership position” and who were able to open their work emails on the days and times when messages to participate in the study were sent. Another limitation concerns the generalizability of our findings, arising from both the absence of a response rate and the restricted sample size.
Conclusion
The 2030 vision has tremendously empowered Saudi women in numerous sectors including the health sector. This was reflected in participants’ responses as they emphasized the advancement, leadership opportunities, and empowerment that they are experiencing with the movement towards the country’s vision. The 2030 vision is creating national strategies that are reinforced by shifting organizational culture and structures, offering women better chances in leadership. Once these national strategies are combined with changes in workplace norms, and active implementation of supportive organizational policies, there will potentially be more representation of qualified women in elite leadership positions in the Saudi healthcare sector.
The study’s findings, while specific to the context of Saudi Arabia, hold implications that may be adopted beyond national borders. Addressing the identified challenges in supporting women’s leadership in healthcare is not only vital for the Saudi context but also offers valuable insights for diverse populations and countries. By recognizing and adapting strategies to fit different cultural norms, our study contributes to the broader conversation on promoting gender equity in healthcare leadership globally, emphasizing the need for context-specific approaches to empower women in leadership roles across various settings.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Saudi Commission For Health Specialties (protocol code SRP-00000182 on Oct 5th, 2021).
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
This research was supported by the Healthcare Leadership Academy, the Saudi Commission for Health Specialties. We thank Ms Safa Alakhdair for her coordination and support. We also thank our exceptional leaders, Dr Manal AlNasser, Dr Yousra AlAteeq, Dr Abeer AlTamimi, Dr Noura AlZamil, Dr Ghazwa Kareem, and Dr Ameera Cluntun as they provided insight and expertise that greatly assisted the research, although they may not agree with all the interpretations/conclusions of this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially funded by the Saudi Commission for Health Specialties.
Disclosure
The authors declare no conflict of interest.
References
1. Berlin G, Darino L, Greenfield M, Starikova I. Women in the healthcare industry. McKinsey & Co; 2019. Available from: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/women-in-The-healthcare-industry#.
2. Stone T, Miller B, Southerlan E, Raun A Women in Healthcare Leadership 2019. Oliverwyman.com. Available from: https://www.oliverwyman.com/our-expertise/insights/2019/jan/women-in-healthcare-leadership.html.
3. Kalaitzi S, Cheung KL, Hiligsmann M, Babich S, Czabanowska K. Exploring women healthcare leaders’ perceptions on barriers to leadership in Greek context. Front Public Health. 2019;7:68. doi:10.3389/fpubh.2019.00068
4. Banerjee S, Dafni U, Allen T, et al. Gender-related challenges facing oncologists: the results of the ESMO women for oncology committee survey. ESMO Open. 2018;3(6):e000422. doi:10.1136/esmoopen-2018-000422
5. Fixing the gender imbalance in health care leadership. Harvard Business Review. Available from: https://hbr.org/2018/10/fixing-The-gender-imbalance-in-health-care-leadership.
6. How Lilly Is Getting More Women into Leadership Positions. Harvard Business Review. Available from: https://hbr.org/2018/10/how-lilly-is-getting-more-women-into-leadership-positions.
7. What’s holding women in medicine back from leadership. Harvard Business Review. Available from: https://hbr.org/2018/06/whats-holding-women-in-medicine-back-from-leadership.
8. When Medical Institutions Hire Leaders, External female candidates have an extra disadvantage. Harvard Business Review. Available from: https://hbr.org/2019/11/when-medical-institutions-hire-leaders-external-female-candidates-have-an-extra-disadvantage.
9. Al-Amoudi S. Health empowerment and health rights in Saudi Arabia. Saudi Med J. 2017;38(8):785–787. doi:10.15537/smj.2017.8.19832
10. Makarova E, Aeschlimann B, Herzog W. Why is the pipeline leaking? Experiences of young women in STEM vocational education and training and their adjustment strategies. Empir Res Vocat Educ Train. 2016;8(1):1. doi:10.1186/s40461-016-0027-y
11. Alwazzan L, Rees C. Women in medical education: views and experiences from the Kingdom of Saudi Arabia. Med Educ. 2016;50(8):852–865. doi:10.1111/medu.12988
12. Amon M, Wang L, Wu H. Looking through the glass ceiling: a qualitative study of STEM women’s career narratives. Front Psychol. 2017;8:8. doi:10.3389/fpsyg.2017.00008
13. Aldekhyyel R, Almulhem J, Binkheder S, Muaygil R, Aldekhyyel S. What it means to be a woman in the field of biomedical informatics: exploring the lived experiences of women managers in the kingdom of Saudi Arabia. J Am Med Inf Assoc. 2020;28(2):311–321. doi:10.1093/jamia/ocaa165
14. Burke R. Managerial women’s career experiences, satisfaction and well‐being: a five country study. Cross Cult Manage. 2001;8(3/4):117–133. doi:10.1108/13527600110797254
15. National Transformation Program. Vision; 2030. Available from: https://www.vision2030.gov.sa/v2030/vrps/ntp/.
16. General Authority for Statistics. Labor market second quarter; 2023. Available from: http://www.stats.gov.sa.
17. Saudi Commission for Health Specialties. The strategic plan; 2018. Available from: https://www.scfhs.org.sa/about/Pages/strategicPlan.aspx.
18. Health Leadership Academy Services. Scfhs.org.sa. Available from: https://www.scfhs.org.sa/en/eservices/Pages/HLA.aspx.
19. Healthcare Transformation Strategy. Moh.gov.sa. Available from: https://www.moh.gov.sa/en/Ministry/vro/Pages/Health-Transformation-Strategy.aspx.
20. Hoyt CL, Simon S. Gender and Leadership. In: Northouse PG, editor. Leadership: Theory and Practice. Sage publications; 2021:397–426.
21. Walker C. Women and Leadership in Health Care. SanFrancisco: Jossey Bass Publishers; 1999.
22. Gabow P. TIME’s NOW for Women Healthcare Leaders. Milton: Productivity Press; 2020.
23. Google Forms: online form creator. Google Workspace. Available from: https://www.google.com/forms/about/.
24. Ministry of Health. Statistical Yearbook; 2021. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx.
25. General Medical Council. The State of medical education and practice in the UK; 2019. Available from: https://www.gmc-uk.org/-/media/documents/somep-2019---full-report_pdf-81131156.pdf.
26. Mannix R, Lee L, Kline JA. Doctoring while woman. Acad Emergency Med. 2020;27(5):434–436. doi:10.1111/acem.13903
27. Villablanca AC, Beckett L, Nettiksimmons J, et al. Career flexibility and family- friendly policies: an NIH-funded study to enhance women’s careers in biomedical sciences. J Womens Health. 2011;20(10):1485–1496. doi:10.1089/jwh.2011.2737
28. D’Agostino M, Levine H. The career progression of women in state government agencies. Gend Manag. 2010;25(1):22–36. doi:10.1108/17542411011019913
29. Villablanca AC, Beckett L, Nettiksimmons J, et al. Improving knowledge, awareness, and use of flexible career policies through an accelerator intervention at the University of California, Davis, School of Medicine. Acad Med. 2013;88(6):771. doi:10.1097/ACM.0b013e31828f8974
30. Duration of Maternity Leave. Labor Education. Available from: https://laboreducation.hrsd.gov.sa/en/labor-education/286.
31. Gaetke-Udager K, Knoepp U, Maturen K, et al. A Women in Radiology Group Fosters Career Development for Faculty and Trainees. Am J Roentgenol. 2018;211(1):W47–W51. doi:10.2214/AJR.17.18994
32. Harris C, Leberman S. Leadership Development for Women in New Zealand Universities. Adv Dev Human Res. 2011;14(1):28–44. doi:10.1177/1523422311428747
33. Pike E, White A, Matthews J, et al. Women and sport leadership: a case study of a development programme. In: The Palgrave Handbook of Feminism and Sport, Leisure and Physical Education. Palgrave McMillan; 2018:809–823.
34. Chang S, Morahan PS, Magrane D, et al. Retaining faculty in academic medicine: the impact of career development programs for women. J Womens Health. 2016;25(7):687–696. doi:10.1089/jwh.2015.5608
35. Isaac C, Kaatz A, Lee B, et al. An educational intervention designed to increase women’s leadership self-efficacy. CBE Life Sci Educ. 2012;11(3):307–322. doi:10.1187/cbe.12-02-0022
36. Mousa M, Boyle J, Skouteris H, et al. Advancing Women in healthcare leadership: a systematic review and meta-synthesis of multi-sector evidence on organisational interventions. EClinicalMedicine. 2021;39:101084. doi:10.1016/j.eclinm.2021.101084
37. Leaders 2030. Misk.org.sa. Available from: https://misk.org.sa/leaders2030/.
38. Qiyadat Global - Georgetown. Available from: https://qiyadatglobal-georgetown.com/en/home.
39. Singh V, Vinnicombe S, James K, Burke RJ. Constructing a professional identity: how young female managers use role models. Women Manage Rev. 2006;21(1):67–81. doi:10.1108/09649420610643420
40. Abuhammad S. Preparing for future pandemics: challenges for healthcare leadership. J Healthcare Leader. 2022;31:131–136. doi:10.2147/JHL.S363650
41. Johnson C, Williams B. Gender and Political Leadership in a Time of COVID. Politics Gender. 2020;16(4):943–950. doi:10.1017/S1743923X2000029X
42. Aldrich AS, Lotito NJ. Pandemic performance: women leaders in the Covid-19 crisis. Politics Gender. 2020;16(4):960–967. doi:10.1017/S1743923X20000549
43. Alsharif D. The challenges associated with women career development at the state universities in Saudi Arabia: a ground theory approach. Int J Gender Women Stud. 2018;6:2.
44. Alsahan, Haneen and George, Rhea, Challenges Women Face in Leadership Positions in the Government Sector in Saudi Arabia; 2022. Available from: https://ssrn.com/abstract=4122606.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.