Back to Journals » Patient Preference and Adherence » Volume 17
Patient’s Perceptions and Attitudes Towards Medical Student’s Involvement in Their Healthcare at a Teaching Hospital in Jordan: A Cross Sectional Study
Authors Taha HA ![]() , Al Saqer JK, Al Harbi NR, Younis RN, Al Dawoud F, Nawaiseh MB
, Al Saqer JK, Al Harbi NR, Younis RN, Al Dawoud F, Nawaiseh MB ![]() , Berggren V
, Berggren V
Received 6 November 2022
Accepted for publication 25 February 2023
Published 13 March 2023 Volume 2023:17 Pages 629—641
DOI https://doi.org/10.2147/PPA.S396035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Hana Ahmad Taha,1– 3 Jawaher Khaled Al Saqer,2 Noora Rashed Al Harbi,2 Rand Nidal Younis,2 Fatma Al Dawoud,2 Mohammed Bassam Nawaiseh,4 Vanja Berggren3
1Department of Pharmacology, Public Health, and Clinical Skills, Faculty of Medicine, The Hashemite University, Zarqa, 13133, Jordan; 2Department of Family and Community Medicine, School of Medicine, The University of Jordan, Amman, 11942, Jordan; 3Department of Neurobiology, Caring Science and Society, Karolinska Institutet, Huddinge, 141 52, Sweden; 4Jordanian Royal Medical Services, Amman, 11855, Jordan
Correspondence: Hana Ahmad Taha, Department of Pharmacology, Public Health, and Clinical Skills, Faculty of Medicine, The Hashemite University, P.O. Box 330127, Zarqa, 13133, Jordan, Tel +962-5-3903333, Email [email protected]
Background: Medical students’ involvement in patients’ care varies according to patient’s willingness, as some might consider it a privacy invasion. Thus, exploring patients’ perceptions and attitudes towards this interaction should be thoroughly investigated, to better understand it and to provide evidence-based data for improving the training of future doctors.
Methods: A cross-sectional study was conducted at Jordan University Hospital. A questionnaire was answered by 420 patients from the out-patients’ clinics.
Results: Of the patients interviewed, 94% were aware that they were in a teaching hospital, 92% approved the presence of medical students during their consultation and 80% accepted to be observed and examined by medical students in the presence of a senior doctor. However, this decreased to 30.5% if there was no senior doctor. Almost 83% of the patients believed that their consent should be obtained first. However, only 58% of them indicated that the student asked for consent prior to interacting with them. Patients who were more likely to approve the existence of medical students during consultation and allow students to perform procedures on them, respectively, were those who were asked for consent by students (P = 0.001 and P = 0.021), considered seeing medical students’ enjoyable (P < 0.001 and P < 0.001), thought that their privacy was not violated (P < 0.001 and P < 0.001), and were provided with useful information about their health problems (P < 0.001 and P < 0.001).
Conclusion: Patients showed an overall positive stance towards the involvement of medical students in their healthcare. The majority were delighted to see medical students while some expressed concerns over their privacy due to the large number of students and because several students do not ask for their consent. It is essential to apply medical ethics practices together with patient-centered approach.
Keywords: students, medical, education, undergraduate, curriculum, teaching hospital, patient perception
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Lam has been published for this article.
Introduction
Best practices in medicine stipulate that the medical student should be fully equipped with clinical skills to meet the competence standards before being declared fit to practice the profession.1 This capacity building is best achieved through frequent interaction with patients at every possible opportunity. Therefore, clinical teaching in the presence of the patient is an integral part of the learning process for medical students.2,3
The face-to-face interaction with patients and the constant contact with them is not only important for building a good doctor–patient relationship but it also enriches their clinical knowledge and learning experience.4 Cooperative patients who are willing to elaborate and give detailed description of their disease and their experience with it, from symptoms development to treatment plans and disease progression, can be more informative than the enhancement of the skills acquired through reading or listening lectures.4,5 This produces more competent doctors on the long-term and instills a feeling of pride and satisfaction in the patient for contributing to the education of a future doctor.6–9
However, not all patients are willing to participate in the medical students’ teaching. Some patients might consider it as an invasion of their privacy and an unnecessary step in their health care. Additional concerns might arise if the patient perceives his/her health issue as a private matter and they do not feel comfortable discussing it with students.10–13 Patients have the right to refuse the presence of medical students during their consultation. However, patients who seek health care in a teaching hospital usually know that medical students could be involved in their consultation.14–16
Variation in the patients’ acceptance and comfort level towards medical students’ involvement in their care are attributable to numerous factors including patients’ sociocultural and educational levels, and nature of examination or procedure as well as the kind of students’ involvement, such as the student’s gender, seniority level and behavior.16–18 According to a study conducted in Western Saudi Arabia, young patients and female patients were more prone to exhibit negative attitudes against the involvement of medical students. Additionally, there was no statistically significant correlation between patients’ attitudes and marital status, education level, hospital type, or prior interactions with medical students.19
Exploring patients’ perceptions and attitudes towards their interaction with medical students is necessary for responding to their expectations and for enhancing the quality of the health care provided to them. This will be the first study to assess this subject in Jordan. This research is also important for providing evidence-based data that could be used to improve the training of future doctors and build their capacity in medical, clinical, communication and behavioral skills. Thus, this research aimed to better understand the perceptions and attitudes of Jordanian patients towards the presence of medical students’ during their consultations in different departments at the Jordan University Hospital (JUH), and if the reaction varies depending on the department and what grounds they might have for accepting or refusing the presence of medical students.
Materials and Methods
Study Setting
In 1972, Jordan established the first medical school for undergraduate medical education at The University of Jordan. After that, four other public medical universities were established and until today there are no private medical universities in Jordan. Jordan’s medical schools’ graduates have an important role in the national health-care delivery system and the quality of their medical education is highly recognized in the Middle East and globally.20 This research was conducted at JUH between September 1st, 2019, and February 5th, 2020. JUH is a tertiary hospital that is the first academic teaching hospital in the Hashemite Kingdom of Jordan with 600 beds. The majority of the patients who attend JUH has an insurance provided from the University of Jordan or from the Ministry of Health, and the rest has no medical insurance and pay out of pocket.21
The undergraduate medical education in Jordan entails passing 6-years full time curricula divided into a 3-years pre-clinical stage followed by the clinical training phase that lasts for another 3 years.22 In the pre-clinical phase, the students study basic sciences in the first year, followed by basic medical sciences courses in the second and the third year. They can also freely choose some non-medical courses to complete their predefined academic credit hours. In the clinical phase, clerkship rotations start at the fourth academic year and continue until the end of year six. During their clinical training, the students are supervised by senior physicians, and they must pass mandatory two to twelve weeks rotations in different clinical units. During these rotations, students are expected to interact with patients, learn the competencies of ethical behavior, communication, interviewing patients, history taking, physical examination and clinical skills.
Study Design
This is a cross-sectional study that was conducted at JUH using a questionnaire that was developed by the research team in Arabic language based on the literature. The questionnaire consisted of two sections; the first part included a set of eleven items about the patients’ socio-demographic characteristics. Patients were asked to provide information about their age, gender, marital status, educational level, current occupation, income, health insurance status, consultation department, residence, and nationality. The second section consisted of 32 statements, about their feelings and perspectives toward the involvement of medical students in the clinic during their consultations, the role of medical students, and their preferences regarding medical students’ involvement in their care and whether they mind having a medical student conducting the physical examination in the presence or absence of a senior doctor. In this study, we performed a brief literature review to build our Arabic-language questionnaire that can measure all aspects that may affect patients’ perceptions and attitudes towards the presence of medical students’.9,16,23 When two or more statements had similar meaning or idea, only one of them was chosen. The questionnaire was pilot tested in eight face-to-face interactions to assess the questions clarity, flow and arrangement, and to evaluate the average time it takes the respondents to complete each question. The pilot testing enabled us to adjust any questions that the respondents found hard to understand in order to avoid ambiguity that could lead to incorrect answers. We assessed the internal consistency of the data collection instrument; the following items were determined to be a measure of the patients’ acceptance of medical students’ contribution in their care: approving the existence of medical students during consultation, allowing medical students to observe the history taking or physical examination, allowing medical students to examine the patients in the presence or absence of senior doctor, allowing students to assist in formulating the plan of care, and permitting medical students to perform procedures on patients. The reliability between the aforementioned items was estimated to be good (Cronbach alpha = 0.704).
Most of the questions had the option of ticking (YES) or (NO). The research team preferred using a yes/no format to have the answers falling on one side of the scale or the other and because they are quicker to answer than questions that rely on 4–7 Likert considering the setting and the targeted population. Four medical students/co-authors were assigned to conduct the data collection separately from the waiting areas of the outpatient’s clinics of Internal Medicine, Obstetrics and Gynecology, Pediatrics, and Surgery departments. In every department, we counted two patients and approached the third patient and continued to do that until we collected the data randomly from all departments. The student approached the patient, introduced him/herself and informed the patient about the research aim and the anonymous nature of the study. The patient had the choice to accept or refuse. All the participants were able to write and read Arabic fluently. The students who conducted the data collection requested from the participant to write his/her answers to the questionnaire and were available to clarify any items during the process of the data collection.
We used EpiCalc 2000 software to calculate the minimal sample size needed, assuming a population of 100,000 patients with a precision of 5%, which was around 398 patients. However, in this study, a total 432 patients were randomly approached, 12 of them were in a hurry and refused to participate in the study and 420 patients accepted to participate. Each survey lasted between 15 and 20 minutes and the number of participants was almost equal among the patients from the four departments to avoid bias (Internal Medicine 110, Obstetrics and Gynecology 106, Pediatrics 102, Surgery 102).
According to the World Health Organization (WHO) regulations that prohibit pediatric patients who are under 19 to provide information in clinical studies; the guardian of the pediatric patient was surveyed, gave the answers to the questionnaire and stated his/her relation to the patient.24
This research received the ethical approval number 2021/159 from the Institutional Review Board (IRB) committee in JUH. Confidentiality of the data, voluntary participation and full autonomy of the respondents were ensured. The participants had been informed of the purpose of the study before they signed a written consent.
Statistical Analysis
After the data was configured properly, we imported it into Statistical Package for the Social Sciences (SPSS, (version 25.0)). Continuous data (ie, age) were expressed as mean ± standard deviations (SD) and categorical data (ie, gender and nationality) by frequency and percentage (Tables 1–3). The tests for normality, including skewness, kurtosis and the Shapiro–Wilks test, indicated that the age variable data was normally distributed. Thus, the parametric test Independent samples t-test was conducted to test if there was a difference in age among patients who approved the existence of medical students’ during consultation and patients who did not. Chi square and Fisher’s exact test were used to determine the relation between categorical variables (Table 4 and Table 5). Fisher’s exact test was used if any expected frequencies were less than five.
 |
Table 1 Socio-Demographic Characteristics of Patients Included in the Study |
 |
Table 2 Patients’ Perceptions About the Role of Medical Students |
 |
Table 3 Patients’ Experiences with Medical Students in Clinical Settings |
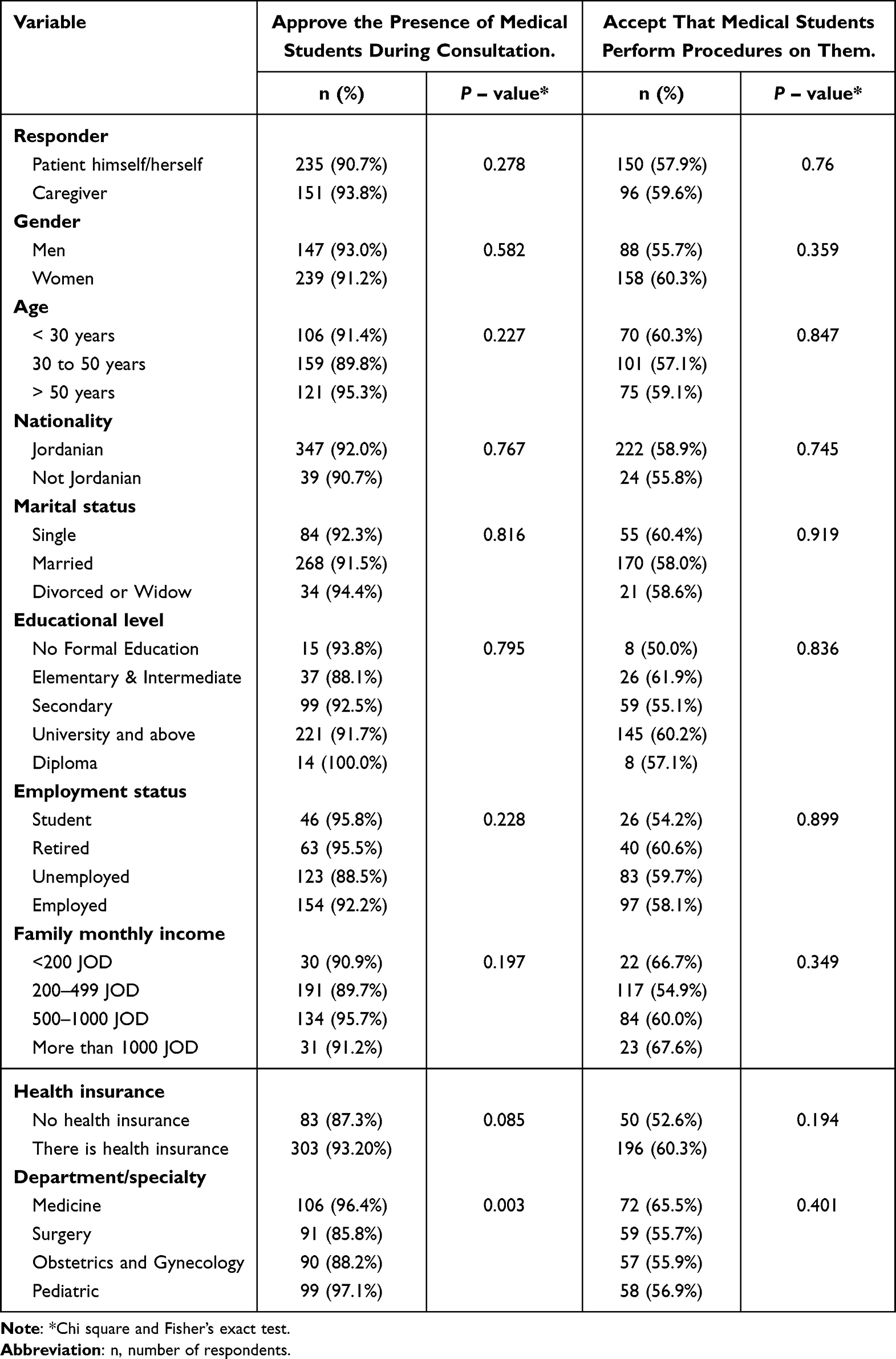 |
Table 4 Socio-Demographic Characteristics of the Patients Who Approve the Presence of Medical Students During Consultation or Perform Procedures on Them |
 |
Table 5 Patients’ Perceptions About the Role of Medical Students in Relation to Their Approval on the Presence of Medical Students During Consultation or the Students Perform Procedures on Them |
We pooled patients’ answers into two groups: patients who approved the existence of medical students’ during consultation and patients who allowed students to perform procedures on them. The reliability (internal consistency) of the questions that measure the patients’ acceptance of medical students’ contribution in their care was estimated using Cronbach’s alpha (α). We adopted a P-value of 0.05 as the significance threshold.
Results
The number of patients who agreed to participate in the study was 420 (158 men, 262 women) with a mean age of 42.25 (SD = 16.08) years. The youngest patient was 14 years old and the oldest was 85 years old. The Mean age for men and women were 46.86 (SD = 16.56) and 39.46 (SD = 15.15) years, respectively. The men-to-women ratio in each department was 1.00 in medicine, 0.85 in surgery, 0.03 in Obstetrics and Gynecology and 1.00 in pediatric departments. Independent samples t-test showed that there was no difference in age between patients who approved the existence of medical students during consultation (Mean = 42.51, SD = 16.3) and patients who did not (Mean = 39.17, SD = 13.03), P = 0.168.
The responder to the questionnaire was the patient himself/herself in (61.7%, n = 259) of the cases. The most frequent caregiver to accompany the patients was mother (16%, n = 70) followed by father (14%, n = 59). Participants who completed secondary or university level of education were 25.5% (n = 107) and 60.7% (n = 255), respectively (Table 1).
The percentage of patients who were aware that JUH is an academic teaching hospital was 94.3% (n = 396) and who approved the existence of medical students’ during consultation was 91.9% (n = 386). Although 82.9% (n = 348) of patients believe that medical students should obtain their consent and 84.8% (n = 356) think that they have the right to approve or disapprove the existence of medical students’ during the clinical encounter, only 57.9% (n = 243) of patients indicated that students take their consent to be part of their health care, according to the patients.
Most patients indicated that there was no preferred gender when they interact with a medical student (63.8%, n = 268), and only 31.4% (n = 132) preferred women students. Nearly 80% (n = 329) of patients accept that medical students observe and examine them in the presence of a senior doctor. However, this will decrease to 30.5% (n = 128) if there was no senior doctor. If a procedure were to be done by a medical student (eg, ultrasound, wound care, steroids injection, etc.), almost 58% (n = 246) of patients will allow this. Participants who were provided with useful information about their health problems by medical students were 252 (60%) of patients.
Around two-thirds of patients indicated that the appearance and manners of students affect their perception and interaction with them. Most of the patients indicated that formal clothes are the most appropriate appearance for medical students (Table 2).
Most of the participants (88.1%, n = 370) stated that the presence of students in the clinic impacts the quality of their training as doctors. Moreover, 64% (n = 269) recommended that the optimal number of students in each clinic is 2–3 students and 59% (n = 248) indicated that there is no preferred training year. Around 35% (n = 148) of patients preferred to interact with 6th year medical students’ as they were perceived as more experienced and knowledgeable than younger students as well as closest to being an official doctor (Table 3).
With regard to the quality of care, 29.8% (n = 125) and 53.8% (n = 226) stated that the presence of medical students in the clinic affects the quality of care and makes consultation time longer, respectively. Patients indicated that their privacy was violated by the presence of medical students, and that they were bothered by that in 16% (n = 67) of cases. Moreover, about 75% (n = 318) felt free to explain their health complaints in front of medical students’. In contrast, only 54.8% (n = 230) felt free to explain their personal issues. Regarding the pros of the presence of medical students in the clinic, 54% (n = 227) agreed that it is in the student’s interest to gain experience, knowledge, and opportunity to learn how to deal with patients. In addition, 61.4% (n = 258) of the patients stated that there are no drawbacks to their presence, while only one-third of them believe that overcrowding can lead to embarrassment during the physical examination, especially with different genders, as well as elongation of the visit time and violation patient’s privacy.
The likelihood of patients approving the existence of medical students during consultation differed (P = 0.003) between the medical (96.4%, n = 106), pediatric (97%, n = 99), surgical (85%, n = 91) and the gynecological (88%, n = 90) departments (Table 4).
There was a statistically significant difference between patients who approve the existence of medical students’ during consultation and patients who do not, according to patient relationship to caregiver (P = 0.016); namely, a husband or a wife is less likely to approve the existence of medical students’ during the consultation than other caregivers.
Moreover, patients displayed more acceptance of medical students during consultation if they were aware that JUH is an academic teaching hospital (92.7% vs 79.2%, P = 0.036), if they do not think that the quality of care is affected by the presence of medical students in the clinic (96.6% vs 80.8%, P = 0.001), if they do not consider that the presence of students during consultation makes its time longer (94.8% vs 89.4%, P = 0.048), and if they considered seeing a medical student enjoyable (97.0% vs 83.2%, P < 0.001). In contrast, patients were less likely to accept the existence of medical students’ during consultation if they preferred women students during the encounter (83.3%, P = 0.001) compared to patients who did not have any preference to gender (95.9%), and if the type of the body part examined affected their decision (88.9% vs 95.1%, P = 0.03). Patients who had not any preference for gender were more likely (63.4%, P = 0.027) to allow students to perform procedures on them compared to patients (50.0%) who preferred men or women students (Table 5).
Patients who were more likely to approve the existence of medical students during consultation and allow students to perform procedures on them (Table 5), respectively, were those who were asked for consent by students (P = 0.001 and P = 0.021), considered seeing medical students’ enjoyable (P < 0.001 and P < 0.001), thought that their privacy was not violated by the presence of medical students’ (P < 0.001 and P < 0.001), and were provided with useful information about their health problems by medical students (P < 0.001 and P < 0.001).
Discussion
This study recruited 420 patients from an academic teaching hospital in Jordan and found that the majority of them approved the medical students’ presence during their consultation. Age, nationality, marital status, educational level, employment status, family income, health insurance, and previous experience with medical students did not affect patients’ acceptance of medical students’ involvement in their health care. Additionally, 94.3% of the patients in this study were aware that JUH is an academic teaching hospital.
We compared the findings of this study with previous literature to test the coherence of existing evidence. First, regarding patient’s approval of medical students’ presence during their consultation, one study was implemented at University of Medical Sciences and Technology in Sudan revealed that the participants’ approval was 95.2%, while in another study conducted by Aljoudi et al, at King Abdelaziz Medical City in Saudi Arabia reported that the participants’ approval was 88%. Those findings correspond with our study results which showed that 91.9% of the participants approved of medical students’ existence during their consultation.19,25 However, this depends on the type and characteristics of the encounter. For example, more than 80% approved medical students to take medical history from them, and 74.5% allowed students to assist in the plan of care. On the other hand, physical examination encounters depend on presence or absence of a senior doctor and the type of body part examined.
Eighty percent of the participants in our study accepted to interact with medical students in their consultation procedures (observation, taking medical history and examination) in the presence of a senior doctor. This is consistent with the Sudan study results which indicated that 79.8% of the respondents agreed to be examined by students in the presence of a doctor.25 Another study that took place in Hospital Kuala Lumpur and Hospital Kulim in Malaysia showed that most of their patients accepted the involvement of medical students during their clinical examination, by 77.9% and 73.4%, respectively.26 Comparably, a study at King Abdelaziz Medical City in Saudi Arabia stated that 51% of the participants have a positive attitude towards involving medical students’ in clinical examination and care.19 The maximum overall mean comfort score was with medical students taking history followed by observations and less invasive examination. In another study conducted by Ghobain et al; on 430 patients admitted to the medical and surgical wards at the King Abdelaziz Medical City, Riyadh, Saudi Arabia, 98% of the patients were willing to be asked about their medical history and 89% of them would permit physical examinations by medical students.27 In another study in King Abdulaziz University Hospital, only 39.4% of the study participants believed that they have the right to refuse the presence of medical students’ involvement in their health care, although nearly 80% believed that medical students should specifically obtain their consent prior to observing them in the operating room vice versa. Our study indicated that nearly 82.9% of the participants believed the same, which emphasizes the importance of obtaining consent prior to patient student interaction.28
Around 82.9% of our study participants believed that medical students should obtain their consent before clinical encounter, which agrees with a study conducted at University of Medical Sciences and Technology in Sudan as 89.5% of their participants preferred to be consented.25 Only 57.9% of our study participants were consented, this shows a deviation from the standard procedures at JUH which stipulate that the senior consultant should introduce the students and get the consent from the patient before involving them in the care provided. Additionally, in rare cases, if the consultant is not present, the procedures mandate the student to introduce himself and get the consent of the patient prior to any clinical encounter.
This finding is relatively higher in comparison with a study implemented at King Abdelaziz University Hospital in Saudi Arabia which showed that only 42% of their participants consent has been taken.19
We recommend that medical schools instruct students on the method and importance of obtaining consent from patients prior to their encounters with them. It is important to conduct more studies to assess the challenges that students may face when obtaining patients’ consent.
Moreover, the same Saudi Arabia study stated that only 50% of its participants felt more comfortable interacting with 2–3 medical students per consultation,19 while 64% of our study participants indicated that the optimal number is 2–3 medical students during consultation. In addition, 59.1% of the patients in the Saudi study participants preferred that the medical students to be from the 6th year,19 which contradicts with our findings as 59% of the participants have no preferred training year among medical students and only 35% preferred 6th year medical students. Furthermore, it was demonstrated in the same Saudi study that there is preference towards students of the same gender and 39% of the respondents found it difficult to interact with students of the opposite gender.19 A study conducted at Hospital Kuala Lumpur and Hospital Kulim in Malaysia found that 52.5% of women patients appeared to be less receptive towards medical students’ compared to 47.5% of men patients,26 whereas in our study 63.8% of patients indicated that there was no preferred gender when they interact with medical students, while only 31.4% preferred to interact with women students. This could be due to the distribution of our questionnaires to women patients in the Obstetrics and Gynecology department, who will show higher comfort levels with female students.
The results of this study are conforming previous studies regarding the patients’ perception of the importance of medical students’ involvement and presence in the clinical consultation by 88.1%, to enhance their clinical experience and the quality of their training as doctors.19,25–27 In a study conducted in a teaching hospital in Saudi Arabia to investigate patients’ perception regarding medical students’ role in the operating theatre. The results indicated that 46.4% think that it was important for the future doctors to be in theater during surgery. Around 60% thought that medical students only observed surgeons in the theatre and 39% thought that medical students can perform minor procedures in the theatre.28 A further study at University Family Practice Center in Sri Lankan exhibited that 95.5% of their patients felt comfortable discussing personal problems in front of medical students, which means that doctor–patient interaction or the relationship is not affected to a greater extent by the presence of a medical student. On that account, our study showed that 54.8% of the participants felt secure to explain their personal issues in front of medical students.29
In general, the patients in this study had a positive perception of medical students, with most patients acknowledging the educational benefit of student participation in patient care. As patients’ perceptions of students’ professionalism, confidence and respect for privacy were significantly related to acceptance of care; education on these aspects should be a priority in medical curricula. In inference, our study supported previous studies and showed overall positive standpoints towards the involvement of medical students in the patient’s health care.19,25–29
Clinical Relevance of This Research
Our findings are applicable on the daily practice of medical students in the sense that certain changes can be made to make the clinical consultation experience better for patients. The communication between the patient and the medical student can be explained in the framework of the Calgary–Cambridge Guides (CCG).30 The CCG were developed to explain effective physician–patient communication skills and provide an evidence-based construct for teaching of these proficiencies. CCG presents a range of skills to be used as required, not a list to be routinely followed in every encounter. There are 71 detailed skills that are nested within a broad process that include: Initiating the session; gathering information, providing structure to the consultation, building relationship; explanation and planning, and closing the session.
We need to reinforce the teaching of the CCG principles to all medical students early in their clinical training. The students must initiate the session by asking for the patient’s permission and consent, always introducing oneself by name, year of study and maintaining a professional attire as well as a professional attitude. Senior physicians in teaching hospitals need to explain to the patient the objectives behind the medical students’ presence in the consultation. This is so important to take away a lot of confusion from the patient’s side, and it will help medical students to have a smoother, and better experience as well.
Based on the above, the following points are recommended. Medical students should take patient’s consent, be polite, respectful and provide useful information to patient about his case. This could enhance the patient’s acceptance of the medical student’s involvement in health care. Senior doctors should try their best not to violate patient’s privacy, nor extend the timing of the patient’s visit; if needed further explanation for the students can be provided later. Moreover, medical schools along with teaching hospitals should explain to patients that this is an academic teaching hospital and the interaction between patients and medical students is essential for their education, particularly in the Obstetrics and Gynecology and Urology departments when there is gender difference between the patient and the students. Additionally, the number of medical students encountered with the patients in each clinic should be restricted to provide better health-care services. Lastly, more studies should be conducted to explore the perceptions and attitudes of medical students towards their bedside training experience so as to compare results and design a context sensitive and effective clinical training program that abide the basic principles related to patients’ rights and quality of care.
Limitations of the Study
Some of the limitations that we faced in this study were the lack of cooperation from some patients, but the researchers handled this by reading the questionnaire to them and answering their inquiries to ensure that they fully comprehended the meaning of the questions. Although the patients interviewed were selected randomly, still the findings of this study cannot be generalized because the sample was relatively small. Moreover, the study was conducted only in the outpatient departments, thus we could not generalize our results to patients from the inpatient departments and more studies should be done on this subpopulation.
Conclusion
To conclude, patients’ perspectives showed overall positive stance towards the involvement of medical students in their health care. Most expressed comfort, ease and enjoyed seeing medical students, but some expressed concerns over their privacy and the number of students present. Patient’s gender as well as their socioeconomic background does not determine their perspective and preferences. Most patients knew their rights regarding their autonomy to accept or refuse the medical students’ presence during their medical consultations. However, a significant proportion of students did not ask the patients for their consent. Moreover, patients preferred lower number of medical students’ to be involved in their consultation. It is essential to have an ethical, professional practice and more patient-centered approach putting in mind that the goal is to increase the awareness towards the ethics of patients’ involvement in medical teaching.
Abbreviations
CCG, Calgary–Cambridge Guides; IRB, Institutional Review Board; JUH, Jordan University Hospital; JOD, Jordanian Dinar; SD, Standard deviations; SPSS, Statistical Package for the Social Sciences; WHO, World Health Organization.
Data Sharing Statement
All authors had access to the study data that support the publication. The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
This study received the ethical approval number 2021/159 from the Institutional Review Board (IRB) committee in Jordan University Hospital. We confirm that all the methods performed were in accordance with the Helsinki declaration and a written informed consent was signed by all the participants before their enrollment in this research.
Acknowledgments
We thank the management of the Jordan University Hospital for approving and facilitating the data collection in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that there are no conflicts of interest regarding the publication of this article.
References
1. Onotai LO, Asuquo EO, Amadi E, Amadi-Oparelli A, Ali DU. Patients’ perception and attitude towards medical students’ involvement in patients care at a Nigerian university teaching hospital. Educ Res. 2012;3(9):732–743.
2. General Medical Council. Tomorrow’s Doctors: Outcomes and Standards for Undergraduate Medical Education. Manchester, UK: General Medical Council; 2009.
3. Ellaway R, Evans P, Mckillop J, et al. Cross-referencing the Scottish Doctor and Tomorrow’s Doctors learning outcome frameworks. Med Teach. 2007;29(7):630–635. doi:10.1080/01421590701316548
4. British Medical Association Medical Education Subcommittee. Role of the Patient in Medical Education. British Medical Association; 2008.
5. Spencer J, Blackmore D, Heard S, et al. Patient‐oriented learning: a review of the role of the patient in the education of medical students. Med Edu. 2000;34(10):851–857. doi:10.1046/j.1365-2923.2000.00779.x
6. Farmer EA, Vnuk A, Salisbury K. Patients’ views on the training of medical students in Australian general practice settings. Aust Fam Physician. 2004;33(4):281–283.
7. Bentham J, Burke J, Clark J, Svoboda C, Vallance G, Yeow M. Students conducting consultations in general practice and the acceptability to patients. Med Edu. 1999;33(9):686–687. doi:10.1046/j.1365-2923.1999.00410.x
8. Haffling AC, Håkansson A. Patients consulting with students in general practice: survey of patients’ satisfaction and their role in teaching. Med Teach. 2008;30(6):622–629. doi:10.1080/01421590802043827
9. Choudhury TR, Moosa AA, Cushing A, Bestwick J. Patients’ attitudes towards the presence of medical students during consultations. Med Teach. 2006;28(7):e198–203. doi:10.1080/01421590600834336
10. Mavis B, Vasilenko P, Schnuth R, Marshall J, Jeffs MC. Medical students’ involvement in outpatient clinical encounters: a survey of patients and their obstetricians–gynecologists. Acad Med. 2006;81(3):290–296. doi:10.1097/00001888-200603000-00023
11. Shann S, Wilson JD. Patients’ attitudes to the presence of medical students in a genitourinary medicine clinic: a cross sectional survey. Sex Transm Infect. 2006;82(1):52–54. doi:10.1136/sti.2005.016758
12. Jayakumar N. Bedside teaching with unwell patients: can it ever be appropriate? Med Teach. 2017;39(3):323–324. doi:10.1080/0142159X.2016.1248922
13. Ryder N, Ivens D, Sabin C. The attitude of patients towards medical students in a sexual health clinic. Sex Transm Infect. 2005;81(5):437–439. doi:10.1136/sti.2004.014332
14. Thompson AG. The meaning of patient involvement and participation in health care consultations: a taxonomy. Soc Sci Med. 2007;64(6):1297–1310. doi:10.1016/j.socscimed.2006.11.002
15. Sullivan M. The new subjective medicine: taking the patient’s point of view on health care and health. Soc Sci Med. 2003;56(7):1595–1604. doi:10.1016/S0277-9536(02)00159-4
16. Marwan Y, Al-Saddique M, Hassan A, Karim J, Al-Saleh M. Are medical students accepted by patients in teaching hospitals? Med Educ Online. 2012;17(1):17172. doi:10.3402/meo.v17i0.17172
17. Abdulghani HM, Al-Rukban MO, Ahmad SS. Patient attitudes towards medical students in Riyadh, Saudi Arabia. Educ Health. 2008;21(2):69.
18. Sayed-Hassan RM, Bashour HN, Koudsi AY. Patient attitudes towards medical students at Damascus University teaching hospitals. BMC Med Educ. 2012;12:1–8. doi:10.1186/1472-6920-12-13
19. Aljoudi SB, Alsolami SS, Farahat FM, Alsaywid B, Abuznadah W. Patients’ attitudes towards the participation of medical students in clinical examination and care in Western Saudi Arabia. J Family Community Med. 2016;23(3):172. doi:10.4103/2230-8229.189133
20. Abu Hammour K, Al-Heyari E, Allan A, et al. Antimicrobial consumption and resistance in a tertiary care hospital in Jordan: results of an internet-based global point prevalence survey. Antibiotics. 2020;9(9):598. doi:10.3390/antibiotics9090598
21. Jordan University Hospital. Jordan University Hospital; 2022. Available from: http://hospital.ju.edu.jo/medical/juhospital/Lists/HospPages_List/managerword.aspx.
22. Tamimi AF, Tamimi F. Medical education in Jordan. Med Teach. 2010;32(1):36–40. doi:10.3109/01421590903196953
23. Ibingira CB, Mwaka AD, Taremwa S, et al. Patients’ attitudes towards involvement of medical students in their care at three selected university teaching hospitals in Uganda: a cross sectional study. 2021.
24. World Health Organization. Definition of key terms; 2013. Available from: https://www.who.int/hiv/pub/guidelines/arv2013/intro/keyterms/en/.
25. Alawad AAM, Younis FH. Patients’ attitude towards undergraduate medical students at university charity teaching hospital in Sudan. Int J Med. 2014;2(1):28–31. doi:10.14419/ijm.v2i1.2264
26. Khor JYD, Afifah I, Muhsina HD, Normaizatul Afizah ID. A study on patients’ perception and attitude toward medical students in two different hospital setting–hospital kulim and hospital Kuala Lumpur. 2016.
27. Al Ghobain M, Alghamdi A, Arab A, Alaem N, Aldress T, Ruhyiem M. Patients’ perceptions towards the participation of medical students in their care. Sultan Qaboos Univ Med J. 2016;16(2):e224. doi:10.18295/squmj.2016.16.02.014
28. Al-Khatib T, Othman SB, El-Deek B. Patients’ perception toward medical students’ involvement in their surgical care: single center study. Educ Res Int. 2016;2016:1–8. doi:10.1155/2016/8234841
29. Ramanayake R, Sumathipala W, Rajakaruna I, Ariyapala DPN. Patients’ attitudes towards medical students in a teaching family practice: a Sri Lankan experience. J Fam Med Prim Care. 2012;1(2):122. doi:10.4103/2249-4863.104982
30. Main CJ, Buchbinder R, Porcheret M, Foster N. Addressing patient beliefs and expectations in the consultation. Best Pract Res Clin Rheumatol. 2010;24(2):219–225. doi:10.1016/j.berh.2009.12.013
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Determinants of Knowledge of Musculoskeletal Disorders Among Healthcare Providers and Students in Saudi Arabia: A Cross-Sectional Study
Alrwaily M, Alanazi F
Journal of Multidisciplinary Healthcare 2022, 15:1789-1797
Published Date: 25 August 2022
Commentary on Ultrasound Instruction in Undergraduate Medical Education: Perspective from Two Students
Allen AJ, White AB, Bacon DR, Beck Dallaghan GL, Jordan SG
Advances in Medical Education and Practice 2023, 14:1-7
Published Date: 4 January 2023
Knowledge, Perceptions, and Practices on Risks and Disasters Among Medical Students. A Multicenter Cross-Sectional Study in 9 Latin American and Caribbean Countries
Izquierdo-Condoy JS, Montiel-Alfonso MA, Nati-Castillo HA, Saucedo R, Jaramillo-Aguilar DS, Nanjari-Barrientos C, García-Arévalo C, Rivera-Flores D, Díaz Batista MI, Loaiza-Guevara V, Ortiz-Prado E
Advances in Medical Education and Practice 2023, 14:225-235
Published Date: 14 March 2023
Integration of Case-Based Dialogue to Enhance Medical Students’ Understanding of Using Health Communication to Address Social Determinants of Health
King J, Taylor J
Advances in Medical Education and Practice 2023, 14:237-244
Published Date: 15 March 2023
The Tensegrity Curriculum: A Comprehensive Curricular Structure Supporting Cultural Humility in Undergraduate Medical Education

Jones AC, Bertsch KN, Williams D, Channell MK
Advances in Medical Education and Practice 2024, 15:381-392
Published Date: 3 May 2024