")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Prevalence and Determinants of Knowledge of Musculoskeletal Disorders Among Healthcare Providers and Students in Saudi Arabia: A Cross-Sectional Study
Authors Alrwaily M, Alanazi F
Received 18 May 2022
Accepted for publication 29 July 2022
Published 25 August 2022 Volume 2022:15 Pages 1789—1797
DOI https://doi.org/10.2147/JMDH.S375207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Muhammad Alrwaily,1,2 Fahad Alanazi3
1Division of Physical Therapy, School of Medicine, West Virginia University, Morgantown, WV, 26506-9226, USA; 2Department of Physical Therapy, King Fahad Specialist Hospital, Dammam, Saudi Arabia; 3Department of Physical Therapy and Health Rehabilitation, College of Applied Medical Sciences, Jouf University, Jouf Region, Saudi Arabia
Correspondence: Muhammad Alrwaily, Health Sciences Center South, Morgantown, WV, 26506-9226, USA, Tel +1 304-293-0264, Fax +1 304-293-7105, Email [email protected]
Background: Musculoskeletal disorders (MSDs) are rapidly rising in Saudi Arabia and considered the 3rd reason for hospital visits across the country. Despite their prevalence, the adequacy of knowledge in diagnosing and treating MSDs has not been assessed. The purpose of this study is to assess MSD knowledge amongst healthcare providers (orthopedists, physicians, and physical therapists) and medical and physical therapy students and interns.
Methods: In this cross-sectional study, a web-based 25-question MSD test was given to licensed physical therapists, primary care physicians and orthopedists, as well as final-year physical therapy and medical students and interns in Saudi Arabia. Two multivariable linear regression analysis models were used to determine MSD test score differences amongst (1) orthopedists, primary care physicians, and physical therapists and (2) amongst medical and physical therapy students and interns.
Results: A total of 680 participants were included (response rate is 22.7%). The overall MSD test score was 48.2%, and the passing rate was 14%. Model 1 showed that orthopedist’s group had a significantly higher mean score on MSD test than physical therapists (t482= 8.12, p < 0.001) and primary care physician (t482= 6.00, p < 0.05). However, primary care physician scores did not significantly differ from physical therapy group (t482= 6.47, p = 0.07). Model 2 showed that medical interns had significantly higher mean score on MSD test than physical therapy students (t240=4.46, p < 0.001), physical therapy interns (t240= 4.7, p < 0.05), and medical students (t240= 2.79, p < 0.05). There was also a significant difference between medical students and physical therapy interns (t240= 2.5, p < 0.05). However, there was no significant difference between medical students and physical therapy students.
Conclusion: Except for orthopedists, the MSD knowledge appears inadequate amongst healthcare providers, medical and physical therapy students and interns in Saudi Arabia. To improve knowledge in MSDs, increasing content of MSDs in undergraduate education and postgraduate training is necessary.
Keywords: musculoskeletal disorders, competency, education, Saudi Arabia, primary care providers, physical therapists, students, interns
Introduction
Musculoskeletal disorders (MSDs) are rapidly rising in Saudi Arabia, reaching levels similar to those of the western world.1,2 MSDs are the 3rd reason to visit a hospital in Saudi Arabia3 and account for 38% of visits in family practice.4 Despite the prevalence of MSDs, physicians in Saudi Arabia reported low level of confidence in MSD physical examination and had self-perception of incompetency in managing MSDs appropriately.5 This can partly be explained by inadequate preparation of physicians to deal with MSDs in both undergraduate and postgraduate medical training.6 Medical schools, worldwide, spend less than 3% of their curricula on MSDs system compared to other body systems.7 In Canada, only 2.26% of the medical school curriculum is devoted to MSD education.8 In the United Kingdom, 2% of the clinical years is devoted to orthopedics.9 Recently, the Association of American Medical Colleges recognized MSD education as one area of deficiency in medical schools and called for strategies to increase MSD contents.10
Knowledge in MSDs among medical practitioners was first assessed using a standardized MSDs test developed by Freedman and Bernstein.11 Eighty-five physicians underwent the test during the first week following graduation. The physicians had a mean score of 59.6%, with only 18% achieving the passing score. Following Freedman and Bernstein study,11 several medical schools and residencies used the MSD test to evaluate students and physicians.12–15 Except for orthopedists, most of these studies found that students or physicians from various specialties had less than adequate knowledge in MSDs.
MSDs are not only managed by physicians but also by other healthcare practitioners including physical therapists. Early use of physical therapy for the management of MSDs is supported by consistent recommendations from various clinical practice guidelines, including the American College of Physicians.16,17 Physical therapy has evolved in the past two decades to become an autonomous practice where physical therapists can see patients without a physician referral (ie, direct access).18 However, assessment of physical therapists’ knowledge in managing MSDs was done in very few studies.13,14,19 Childs et al showed that physical therapists with orthopedic or sports board certification had higher scores on the MSD test than medical students, interns, residents and most medical specialties except orthopedists.13,19
In Saudi Arabia, however, physical therapy has not fully evolved into an autonomous practice and is still a secondary care that requires physician referral to manage patients with MSDs.20 Physical therapy programs in Saudi Arabia grant bachelor’s degrees (except for two universities), and their curricula do not adequately emphasize the contents of medical screening or differential diagnosis.21 Physical therapy services are highly demanded in Saudi Arabia, with more than 1.5 million visits a year.22 Visits to primary care physicians and specialists related to MSDs in Saudi Arabia are just under 1.1 million.23 Despite the high demand for physical therapy services to treat MSDs, the competency of physical therapists in managing MSDs in Saudi Arabia is unknown. Therefore, the purpose of this study was to assess knowledge of MSDs among healthcare providers in Saudi Arabia. We aimed to evaluate MSD knowledge among (1) orthopedists, primary care physicians and physical therapists, as well as (2) physical therapy and medical students and interns.
Method
Research Design and Setting
This was a cross-sectional study that included a single online session that was conducted from 4th of March 2019 to 30th of April 2019.
Participants and Sample Size
We included licensed physical therapists, physicians (including residents) and orthopedists, as well as final-year physical therapy and medical students and interns in Saudi Arabia. We excluded physical therapists, physicians and orthopedists who are not licensed to practice in Saudi Arabia and students who are not in their final year.
At the time of the data collection, the Saudi Ministry of Health had 2645 orthopedists, 9531 primary care physicians, and 4466 physical therapists.22 We used calculator.net to obtain a sample that represents the targeted population of 16,642 with a margin of error of ±5 and 95% confidence interval.24 The needed sample was approximately 376 practitioners (orthopedists, primary care physicians, and physical therapists). Response rate amongst healthcare practitioners was estimated to be between 10% and 17%;25,26 thus, we planned to send invitations to 3000 or more potential participants.
Musculoskeletal Knowledge Test
We used a standardized MSDs test developed by Freedman and Bernstein.11 The test contains 25 questions that assessed MSDs knowledge (Appendix 1). The questions include commonly encountered MSDs in primary care setting such as fractures, dislocations, arthritis, spinal pain, or conditions that warrant emergency referrals. The passing score was determined to be 70% (at least 18 correct answers out of 25). The test was used to assess the MSD knowledge of physical therapy and medical practitioners and was validated in previous studies.11,12
The original format of the test was paper based and required short-answers. However, for practicality purposes, we modified the test to a web-based multiple-choice-question format that included 1 correct answer as determined in the original answer key of the test and 3 distractors that we developed. To ensure that the distractors were appropriate, an expert item writer with an orthopedic physical therapy specialty certificate with 10 years’ experience reviewed the distractors and made changes mostly related to word selection or grammar.
Data Collection
The data were collected using onlineexambuilder.com platform.27 This platform had many test-taking features necessary for our study. It had a front page where participants could be informed and consented to take the test as part of this research study and allowed for requesting participants’ information, timing the test, restricting the number of attempts to 1 per participant, knowing how much time each participant spent taking the test, and exporting the data into a spreadsheet for analysis.
An electronic link to the test was sent to email lists of specialized groups of physical therapy and medical students and practitioners. Also, invitations to take the test were posted on several social media channels. Additionally, physical therapy and medical educational programs and hospitals in the northern, southern, central and western regions of Saudi Arabia were invited to participate via phone or direct visits. A reminder to take the MSDs test was sent 6 times over the period of the study.
After the participants consented, they were asked for demographics and specialty information. The test was in English and limited to 20 minutes. The test was not proctored, but questions and answers were presented in random order. Only one correct answer per question was allowed. As soon as the participant finished and submitted the test, they were not allowed to take it again. The results of the test were automatically saved on the platform, which was protected with a password for subsequent analysis.
This study was approved by the Research Ethics Committee at West Virginia University (1903492338).
Statistical Analysis
Data were analyzed using SPSS 26 (Armonk, NY). Descriptive statistics were used with sample demographics and characteristics. For aim 1, multivariable linear regression analysis was performed between MSD test score as dependent variable and age, gender, years of experience and specialty as independent variables. Specialty variable involved orthopedists, primary care physicians, and physical therapists as the reference group. Age was centered around the mean to enable interpretation of the constant. For aim 2, multivariable linear regression was also performed between MSD test score as dependent variable and age, gender and specialty as independent variables. Specialty variable involved physical therapy students as a reference group, physical therapy interns, medical students and medical interns. For all analyses, assumptions were tested, and alpha level of significance was set at p < 0.05.
Results
Out of 3000 invitations, we were able to approach 784 practitioners. Of the 784 potential respondents, 35 were excluded because they did not answer any question; another 51 appeared to have dropped out of the study after answering 2–3 questions and no time was recorded for them; and another 18 did not specify their specialty. We included 680 participants, and the response rate was 22.7%. The participants’ demographics and specialty information are listed in Figure 1 and Table 1.
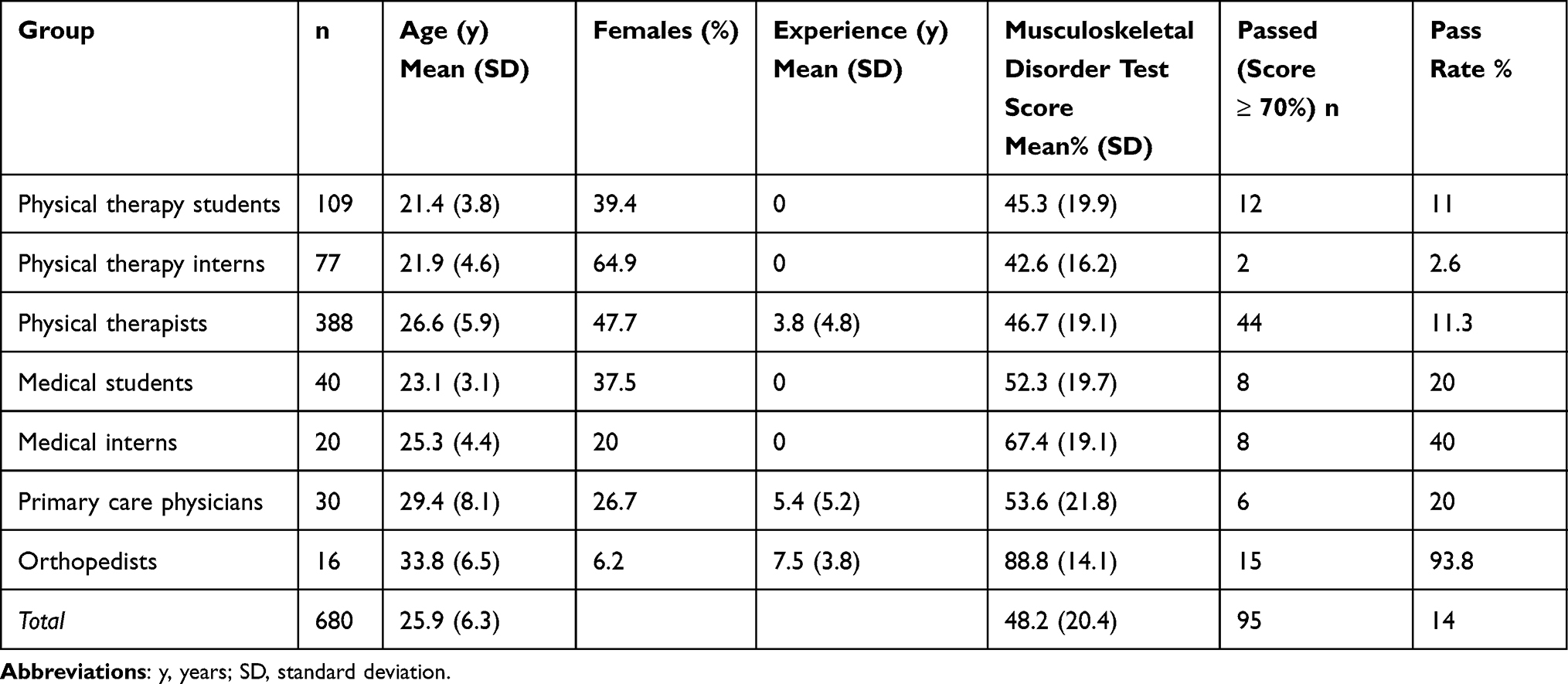 |
Table 1 Demographics, Scores and Passing Rates for Participants in the Musculoskeletal Test |
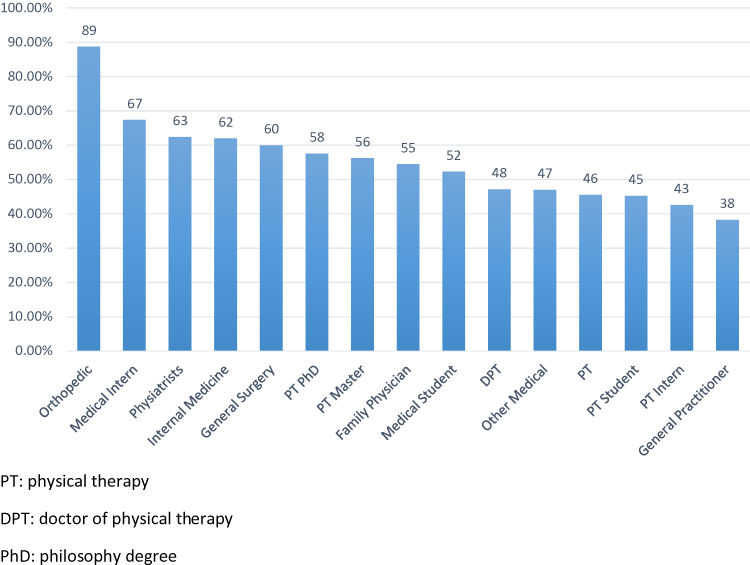 |
Figure 1 Scores of the musculoskeletal test for each specialty of participants. |
The overall passing rate was 14% (Table 1). The passing rate was 93.8% for orthopedists, 20% for primary care physicians, and 11.3% for physical therapists.
For both regression models, the assumptions were met. There was a significant prediction of MSD test score by age, gender, years of experience and specialty for model 1, F(5482)=15.57, p<0.001, R2=0.154. There was also a significant prediction of MSD test score by age, gender, and specialty for model 2, F (5240) = 6.71, p < 0.001, R2 = 0.123.
Table 2 presents the unstandardized regression coefficients (B), standard errors (SEB), t-test and significance level for model 1. Age, gender and years of experience did not significantly predict MSDs test score (P > 0.05). The t-test for each regression coefficient of the specialty predictors tested whether there was a significant difference between the indicator coded groups (ie, primary care physicians, and orthopedists) and the reference group (physical therapists). The result indicates that orthopedist’s group had significantly higher mean score on MSD test than physical therapists (t482= 8.12, p < 0.001) and primary care physician (t482= 6.00, p < 0.05). However, the result indicates that primary care physician scores did not significantly differ from physical therapy group (t482= 6.47, p = 0.07).
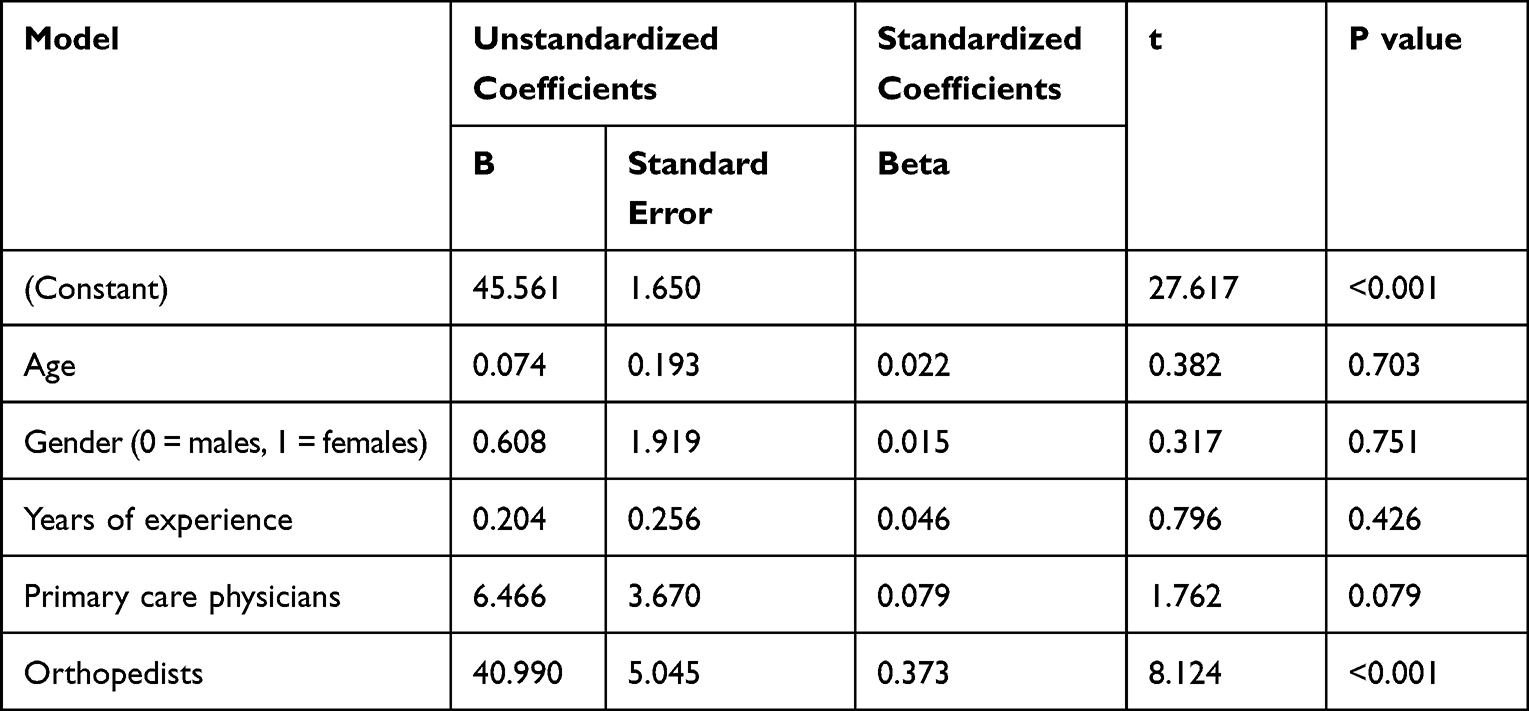 |
Table 2 Regression Analysis Summary for Musculoskeletal Disorder Test on Various Healthcare Providers |
Table 3 presents the unstandardized regression coefficients (B), standard errors (SEB), t-test and significance level for model 2. Age and gender did not significantly predict MSDs test scores (P > 0.05). The t-test for each regression coefficient of the specialty predictors tested whether there was a significant difference between the indicator coded groups (ie, physical therapy interns, medical students, and medical interns) and the reference group (ie, physical therapy students). The result indicates that medical interns had significantly higher mean score on MSD test than physical therapy students (t240=4.46, p<0.001), physical therapy interns (t240=4.7, p<0.05), and medical students (t240=2.79, p<0.05). There was also a significant difference between medical students and physical therapy interns (t240=2.5, p<0.05). However, there was no significant difference between medical students and physical therapy students (Table 3).
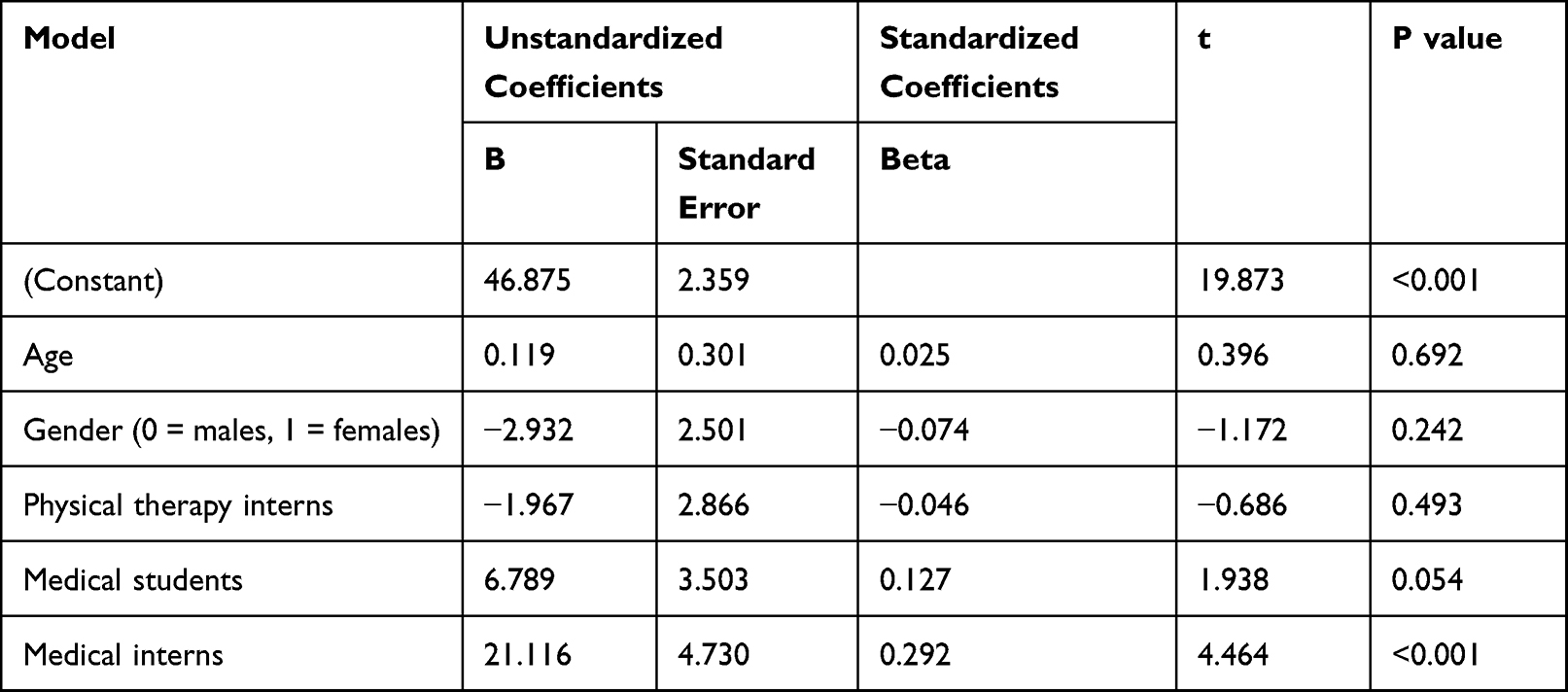 |
Table 3 Regression Analysis Summary for Musculoskeletal Disorder Test Score Using Various Student Groups |
Discussion
Orthopedists, Physicians and Physical Therapists
This study highlights the inadequacy of MSD knowledge among various health specialties in Saudi Arabia. Orthopedists in Saudi Arabia achieved the highest scores and passing rates on the MSD test compared to primary care physicians and physical therapists (Tables 1 and 2). Also, our findings showed that primary care physician scores averaged 53.6% with a passing rate of 20%, which is similar to Matzkin et al study showing MSDs test scores for physicians in the United States of 50% with a passing rate of 21%.12 However, our finding showed that physical therapists achieved the lowest scores of 46.72% with a passing rate of 11.3%, which is in sharp contrast to previous studies from the United States showing that physical therapists come next to orthopedists on the MSD test with scores between 74% and 81% and a passing rate of 58%–88%.13 These low scores among physicians and physical therapists are quite disturbing provided that MSD complaints are the 3rd reason to visit primary care clinics in Saudi Arabia and up to 83% of rehabilitation visits require physical therapy.22,23 This discrepancy between the volume of MSDs and inadequate knowledge in management of MSDs might be a factor that contributes to the rising health care expenditure and the MSDs-related disability in Saudi Arabia.1 National plans to improve musculoskeletal knowledge are necessary.
Even though there was no significant difference between primary care physicians and physical therapists on the MSD test score, both professions exhibited inadequate level of knowledge in managing MSDs and several reasons may explain such low performance. For primary care physicians, multiple studies suggested that lack of exposure to essential elements of MSDs such as orthopedic physical examination skills, radiographic evaluation, and overall time devoted to training MSDs clinical skills was minimal or nonexistent.6 In Saudi Arabia, one study showed management of spinal MSDs by primary care physician was improper.28 Fifty percent of primary care physicians indicated they would prescribe lumbar support, 62% would recommend bed rest, 57% would not refer a patient when they suspected a spinal fracture, and up to 72% underestimated neurological risks post spinal surgery.28 Spinal MSDs are the 4th major cause of disability in Saudi Arabia and represent a large portion of MSD complaints,1 yet primary care physicians seem inadequately prepared to manage such conditions. While we recognize that further research is needed to identify the reasons underpinning such practice patterns, we believe MSD training can help bridge the gap in knowledge of how to manage MSDs.
For physical therapists, the lower performance on the MSD test score may be partly explained by the lack of postgraduate clinical training in Saudi Arabia.20,21 Once physical therapists graduate, there are no residency or fellowship opportunities they can pursue to improve their clinical experiences.21 Graduate education in Saudi Arabia involves master or doctor of philosophy degrees; however, these degrees are research-oriented more so than clinically oriented and may not be associated with improved clinical knowledge. Previous research in the United States showed that physical therapists with clinical orthopedic or sports board certification or fellowship achieved the highest scores and passing rates on the MSD test compared to other specialties (except orthopedists).13,14 Also, Jette et al showed that physical therapists with orthopedic board specialization were twice as likely to make correct clinical decision when presented with MSDs than those without.29 Further, physical therapists with orthopedic board specialization were more efficient in MSDs management using fewer visits, lower cost, and utilization of treatment procedures.30 Thus, establishing orthopedic and sport residency and fellowship programs in Saudi Arabia has the potential to improve MSD knowledge amongst physical therapists in Saudi Arabia.
The other reasons, we believe, for the low performance of physical therapists in Saudi Arabia are the professional legislation. In Saudi Arabia, physical therapy is a secondary care service that relies on physician referral that sometimes involve directions on what intervention should be used. Because of this, physical therapists in Saudi Arabia might be continuously under the impression that patients with MSDs had already been screened and diagnosed by the physician, which leave them less prepared to conduct their own screening and examination, and only ready to conduct interventions. This lack of opportunity for physical therapists to practice autonomously as primary care providers may have its impact on their clinical skills to practice proper management of MSDs. Nonetheless, the poor performance on the MSD test implies that physical therapists in Saudi Arabia might not be ready to see patients in direct access settings. Before such privilege is legislated, adequate training in MSDs must be instated.
Medical and Physical Therapy Students and Interns
At the level of students and interns, medical interns and students in Saudi Arabia showed higher MSDs test scores than physical therapy students and interns (Tables 1 and 3). Medical interns in Saudi Arabia, noticeably, achieved higher scores and passing rate (40%) than the whole sample of participants in this study, except orthopedists. This performance is better than we anticipated and may be explained by that medical interns are actively involved in preparing for the licensure examination, which may have provided them an advantage in exam-taking skills over other participants. Nevertheless, the overall average scores of medical interns and students were suboptimal (67% and 52% respectively), and comparable to the scores reported by Freedman and Bernstein for medical interns (60%) and students (54%) in the United States.11 The lower scores of medical interns and students reinforce the finding from one survey that reported that medical undergraduates perceived that MSDs were not emphasized, nor competency in MSDs was required.5 Similar findings were reported in many parts of the world, and we join the Bulletin of the World Health Organization call to increase the contents of MSDs in medical curricula.6 Also, this finding begs the question whether future physicians are being adequately prepared to deal with the increasing volume of MSDs once they enter the workforce.
Physical therapy students and interns were amongst the lower scores on the MSD test (Table 1). This finding concurs with our prior survey that examined the entry-level competency of 149 graduating physical therapists in Saudi Arabia using a 70-question multiple-choice exam and found that the average score in various clinical skills to be 34%.31 Also, Bindawas et al evaluated the competency of graduating physical therapists in Saudi Arabia from the perspective of clinicians and academicians and found that skills of evaluation, examination, and treatment were all rated less than 3 out 5 on the Clinical Internship Evaluation Tool.32 These suboptimal scores from the current study and previous ones are likely due to the variability in physical therapy curricula and lack of emphasis on MSD education.21 One study showed that physical therapy students and interns uniformly agree there is a need to increase manual therapy contents and establish orthopedic residencies.21 We believe that there is a critical need to reform physical therapy education and training in Saudi Arabia, not only in MSD contents but in all other subjects.
Recommendations
Musculoskeletal disorder education in under- and postgraduate levels can be improved by adopting the recommendations of the World Health Organization Bulletin and the Association of American Medical Colleges.6,10 In undergraduate MSD education of physicians and physical therapists, teaching should include basic sciences needed for understanding the MSD system such as anatomy, pathophysiology of MSDs system, kinesiology and biomechanics of the locomotor system. Clinical MSD education should develop students’ skills in history taking, physical examination, treatment options, decision-making algorithms,33 extend into disease prevention, and communication and attitude skills.6,34 MSD teaching method should focus on problem-based learning that utilizes case studies to further develop deep learning and analytical skills. For postgraduate MSD education, programs for primary care physicians and physical therapists should include rotations in orthopedic and rheumatology or any specialty that deals with MSDs. Specialized training such as residencies and fellowships should be developed to increase knowledge in specific MSDs area such sports, rehabilitation, or pain management. Elaborated details of MSD education contents have been published in the literature.34
Limitations
Our study included many limitations. The study included a convenience sample, so we cannot exclude the possibility of selection bias. Despite our multiple attempts to increase the representation of primary care physicians and orthopedists, the number of participants in these groups was lower, and we cannot be sure that our findings were representative of these populations. Our sample was composed of volunteers who may have chosen to complete the MSD test due to desire for professional self-development and personal growth in practice, which may limit the generalizability to other practitioners. Also, the content of the MSD test may have been more inclined towards physicians more than physical therapists; however, previous studies used the test for physical therapists too.13,14 It is worth noting that our modification of the test to multiple-choice questions did not undergo a process of validation similar to that of the original test.11 Some authors expressed concerns that the MSD test by Freedman and Bernstein did not capture the competency skills for primary care physicians and suggested a modified version that was still under validity investigation.35
Conclusion
Except for orthopedists, the current study showed that MSD knowledge is suboptimal amongst primary care physicians and physical therapists in Saudi Arabia. Even though not significantly different, primary care physicians achieved higher scores than physical therapists. Also, the study identified deficiency in knowledge among medical and physical therapy students and interns. Medical interns had the highest score of all the groups except orthopedists. Our study highlights the need to improve musculoskeletal education in Saudi Arabia for various specialties.
Implications of the Study
Except for orthopedists, MSD knowledge appears inadequate amongst physicians and physical therapists.
Inadequate MSD knowledge may be explained by lack of exposure to skills of history taking, orthopedic physical examination, radiographic evaluation, proper MSD intervention, and overall minimal time devoted to education of MSDs at under- and postgraduate levels.
National plans to improve MSDs knowledge are necessary to bridge the gap between the inadequate knowledge of how to manage MSDs and the increasing volume of patients suffering from MSDs.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author upon request.
Ethical Approval and Consent of Participants
This study was approved by the Office of Research Integrity and Compliance at West Virginia University, School of Medicine # 1903492338.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no funding for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Mokdad AH, Jaber S, Aziz MI, et al. The state of health in the Arab world, 1990–2010: an analysis of the burden of diseases, injuries, and risk factors. Lancet. 2014;383(9914):309–320. doi:10.1016/S0140-6736(13)62189-3
2. Moradi-Lakeh M, Forouzanfar MH, Vollset SE, et al. Burden of musculoskeletal disorders in the Eastern Mediterranean Region, 1990–2013: findings from the Global Burden of Disease Study 2013. Ann Rheum Dis. 2017;76(8):1365–1373. doi:10.1136/annrheumdis-2016-210146
3. Health Mo. Health statistics annual book; 2013. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistics-Book-1434.pdf.
4. Al-Shammari SA, Nass M, Al-Maatouq MA, Al-Quaiz JM. Family practice in Saudi Arabia: chronic morbidity and quality of care. Int J Qual Health Care. 1996;8(4):383–387. doi:10.1093/intqhc/8.4.383
5. Zaini R, Almoallim H, Hafiz W, et al. Musculoskeletal teaching and training in Saudi internal medicine residency programmes. Creat Educ. 2016;7(06):824. doi:10.4236/ce.2016.76085
6. Akesson K, Dreinhöfer KE, Woolf AD. Improved education in musculoskeletal conditions is necessary for all doctors. Bull World Health Organ. 2003;81(9):677–683.
7. Craton N, Matheson GO. Training and clinical competency in musculoskeletal medicine. Identifying the problem. Sports Med. 1993;15(5):328–337. doi:10.2165/00007256-199315050-00004
8. Pinney SJ, Regan WD. Educating medical students about musculoskeletal problems. Are community needs reflected in the curricula of Canadian medical schools? J Bone Joint Surg Am. 2001;83(9):1317–1320. doi:10.2106/00004623-200109000-00004
9. Williams JR. The teaching of trauma and orthopaedic surgery to the undergraduate in the United Kingdom. J Bone Joint Surg Br. 2000;82(5):627–628. doi:10.1302/0301-620X.82B5.0820627
10. Colleges AoAM. Report VII contemporary issues in medicine: musculoskeletal medicine education; 2005. Available from: https://www.aamc.org/system/files/c/2/497662-contemporaryissuesinmedmusculoskeletalmedreportvii.pdf.
11. Freedman KB, Bernstein J. The adequacy of medical school education in musculoskeletal medicine. J Bone Joint Surg Am. 1998;80(10):1421–1427. doi:10.2106/00004623-199810000-00003
12. Matzkin E, Smith EL, Freccero D, Richardson AB. Adequacy of education in musculoskeletal medicine. J Bone Joint Surg Am. 2005;87(2):310–314. doi:10.2106/JBJS.D.01779
13. Childs JD, Whitman JM, Sizer PS, Pugia ML, Flynn TW, Delitto A. A description of physical therapists’ knowledge in managing musculoskeletal conditions. BMC Musculoskelet Disord. 2005;6:32. doi:10.1186/1471-2474-6-32
14. Rundle R, Roberts J, Whitney G, et al. A comparison between civilian and military physical therapists’ knowledge in managing musculoskeletal conditions: a descriptive study. Int J Sports Phys Ther. 2016;11(1):115–125.
15. Grunfeld R, Banks S, Fox E, Levy BA, Craig C, Black K. An assessment of musculoskeletal knowledge in graduating medical and physician assistant students and implications for musculoskeletal care providers. J Bone Joint Surg Am. 2012;94(4):343–348. doi:10.2106/JBJS.J.00417
16. Lin I, Wiles L, Waller R, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. 2019;54:79–86.
17. Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
18. Association APT. Direct access in practice; 2020. Available from: http://www.apta.org/DirectAccess/.
19. Childs JD, Whitman JM, Pugia ML, Sizer PS
20. Alghadir A, Zafar H, Iqbal ZA, Anwer S. Physical therapy education in Saudi Arabia. J Phys Ther Sci. 2015;27(5):1621–1623. doi:10.1589/jpts.27.1621
21. Bindawas SM. Physical therapy entry-level education and post-professional training in Saudi Arabia: a comparison of perceptions of physical therapists from five regions. J Phy Ther Sci. 2014;26(9):1377–1382.
22. Health Mo. Statistical yearbook; 2018. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/book-Statistics.pdf.
23. Health Mo. Statistical year book; 2014. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistical-Book-for-The-Year-1435.pdf.
24. Calculator.net. Sample size calculator; 2020. Available from: https://www.calculator.net/sample-size-calculator.html.
25. Hardigan PC, Succar CT, Fleisher JM. An analysis of response rate and economic costs between mail and web-based surveys among practicing dentists: a randomized trial. J Community Health. 2012;37(2):383–394. doi:10.1007/s10900-011-9455-6
26. Hendrick P, Mani R, Bishop A, Milosavljevic S, Schneiders AG. Therapist knowledge, adherence and use of low back pain guidelines to inform clinical decisions – a national survey of manipulative and sports physiotherapists in New Zealand. Man Ther. 2013;18(2):136–142. doi:10.1016/j.math.2012.09.002
27. Builder OE. Online exam builder; 2020. Available from: https://www.onlineexambuilder.com/.
28. Alsaleh KA, Alluhaidan AS, Alsaran YK, et al. Management of spinal disorders by primary care providers in Saudi Arabia: treatment options and referral patterns. Management. 2015;4(3):143–146.
29. Jette DU, Ardleigh K, Chandler K, McShea L. Decision-making ability of physical therapists: physical therapy intervention or medical referral. Phys Ther. 2006;86(12):1619–1629. doi:10.2522/ptj.20050393
30. Hart DL, Dobrzykowski EA. Influence of orthopaedic clinical specialist certification on clinical outcomes. J Orthopaed Sports Phy Ther. 2000;30(4):183–193. doi:10.2519/jospt.2000.30.4.183
31. Alrwaily M, Alanazi F. Assessing physical therapy knowledge among new graduates in Saudi Arabia: competency examination across the nation.
32. Bindawas SM, Vennu V, Azer SA. Are physical therapy interns competent in patient management skills? Assessment of the views of clinical and academic physical therapists. J Phys Ther Sci. 2013;25(5):649–655. doi:10.1589/jpts.25.649
33. Alrwaily M, Timko M, Schneider M, et al. Treatment-based classification system for low back pain: revision and update. Phys Ther. 2016;96(7):1057–1066. doi:10.2522/ptj.20150345
34. Woolf AD, Walsh NE, Akesson K. Global core recommendations for a musculoskeletal undergraduate curriculum. Ann Rheum Dis. 2004;63(5):517–524. doi:10.1136/ard.2003.016071
35. Cummings DL, Smith M, Merrigan B, Leggit J. MSK30: a validated tool to assess clinical musculoskeletal knowledge. BMJ Open Sport Exerc Med. 2019;5(1):e000495. doi:10.1136/bmjsem-2018-000495
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.