Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Acupuncture on Post-Stroke Cognitive Impairment: A Systematic Review of Neuroimaging Studies
Authors Yang S ![]() , Bao Q, Zhong W, Wu K, Zhang X, Yao J, Chen Z
, Bao Q, Zhong W, Wu K, Zhang X, Yao J, Chen Z ![]() , Xu P, Yin Z, Liang F
, Xu P, Yin Z, Liang F ![]()
Received 3 June 2025
Accepted for publication 22 September 2025
Published 3 October 2025 Volume 2025:18 Pages 6391—6410
DOI https://doi.org/10.2147/JMDH.S544389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Shiqi Yang,1,2,* Qiongnan Bao,1– 3,* Wanqi Zhong,1,2 Kexin Wu,1,2 Xinyue Zhang,1,2 Jin Yao,1,2 Ziwen Chen,1,2 Ping Xu,1,2 Zihan Yin,1,2 Fanrong Liang1,2
1School of Acu-Mox and Tuina, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Acupuncture Clinical Research Center of Sichuan Province, Chengdu, People’s Republic of China; 3Department of traditional Chinese medicine, The First People’s Hospital of Yunnan Province, The Affiliated Hospital of Kunming University of Science and Technology, Kunming, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fanrong Liang, Email [email protected] Zihan Yin, Email [email protected]
Background: Post-stroke cognitive impairment (PSCI) is a severe central nervous system disorder for which acupuncture demonstrates therapeutic efficacy. Various neuroimaging studies have indicated that acupuncture may exert its effects through modulating central mechanisms. However, owing to the current lack of a systematic summary, this study aimed to integrate the existing evidence.
Methods: Two independent reviewers conducted a search across eight databases and other sources, identifying potential neuroimaging trials on acupuncture for PSCI, spanning from the inception of the databases to August 25, 2024. Eligible studies were screened based on predefined inclusion and exclusion criteria, and their methodological quality was assessed.
Results: Twelve studies, including 671 participants, utilized manual acupuncture (n = 10), electroacupuncture (n = 1), or a combination of both (n = 1). Neuroimaging tools comprised functional magnetic resonance imaging (n = 7), electroencephalography (n = 2), magnetic resonance spectroscopy (n = 2), and functional near-infrared spectroscopy (n = 1). All studies consistently reported positive effects of acupuncture on patients suffering from PSCI. Changes in brain structure and function resulting from acupuncture are commonly observed in the cingulate cortex, parahippocampal gyrus, prefrontal cortex, and fusiform gyrus. Acupuncture appears to modulate cognition-related networks, including the default mode, central executive, frontoparietal, and salience networks, thereby influencing PSCI.
Conclusion: The therapeutic effects of acupuncture on PSCI may be mediated through the regulation of cognition-related brain networks. Yet, these studies remain at an exploratory stage, necessitating a combination of multiple imaging techniques and large, strictly designed multicenter RCTs to validate the neuroimaging findings.
Keywords: acupuncture, post-stroke cognitive impairment, systematic review, neuroimaging, mechanism
Introduction
Stroke, recognized as the second leading cause of death by the World Health Organization, is a prevalent central neurological condition that frequently recurs and contributes significantly to both mortality and long-term disability.1 Post-stroke cognitive impairment (PSCI) is a prevalent complication subsequent to stroke, affecting 53.4% of stroke survivors.2 It encompasses PSCI with no dementia and post-stroke dementia (PSD), with a 1.5-year mortality rate of 50.0% in China for PSD.3,4 Patients with PSCI may experience impairment in one or multiple cognitive domains, including orientation, memory, visuospatial function, executive function, and attention. According to previous reports, over 30% of patients with stroke show a noticeable decline in cognitive function within the first 3 months following their stroke.5,6 Furthermore, relevant literature indicates that nearly 7% of patients develop dementia within 12 months of a stroke.7 PSCI profoundly diminishes patients’ quality of life, functional independence, treatment engagement, and imposes substantial societal and economic burdens.8,9 Therefore, there is growing interest in finding effective treatments for PSCI.10
Currently, the mechanisms of PSCI remain incompletely understood, and no pharmacological treatment has been approved. Several studies have been conducted on cholinesterase inhibitors for the treatment of vascular dementia,11 but only one has specifically focused on PSCI.12 However, this study showed rivastigmine had no significant benefit over placebo on specified cognitive, functional, or behavioral outcomes at 24 weeks. Furthermore, this class of drugs is associated with significant adverse effects, such as bradycardia and syncope.13 Hence, increasing attention is being given to non-pharmacological approaches for PSCI intervention.
Acupuncture, a non-pharmacological treatment commonly used in China, has been extensively adopted both domestically and internationally to address a wide array of health concerns. It is also employed to enhance cognition and memory and to address other forms of functional deterioration.14–16 Acupuncture possesses distinct features that differentiate it from other treatment modalities, incorporating meridian theory and acupoints to activate internal energy and thereby enhance patients’ cognitive abilities. Many systematic reviews (SRs) and clinical studies17–21 have demonstrated that acupuncture has the potential to improve cognitive function in patients with PSCI without evident side effects. However, the lack of a SR on neuroimaging studies of acupuncture for PSCI has hindered a comprehensive elucidation of its mechanisms in promoting cognitive recovery.
Cognitive function relies heavily on the normal operation of the central nervous system. Studies have demonstrated that a decline in cognitive ability is linked to changes in brain regions and networks.22,23 Under certain circumstances, cognitive impairments observed in the initial stages following stroke may be reversible, possibly owing to the plasticity and adaptability of the human brain.24,25 Research indicates that the modulation of brain plasticity can improve cognitive function.26 Given the significance of brain plasticity in neural recovery and cognitive improvement, researchers are actively exploring the neural pathways underlying acupuncture-induced improvements in cognitive ability after PSCI. Rapid technological advancements have enabled the adoption of various non-invasive neuroimaging techniques, including functional magnetic resonance imaging (fMRI), electroencephalography (EEG), functional near-infrared spectroscopy (fNIRS), and magnetic resonance spectroscopy (MRS), to reveal changes in the neural characteristics in patients with PSCI following acupuncture therapy.27–30 However, no SR has yet compiled neuroimaging findings related to the use of acupuncture in treating PSCI to systematically assess the mechanisms of acupuncture therapy and its effects on brain structure and function. Therefore, this SR aims to: (1) Characterize the main features of current neuroimaging studies on acupuncture for PSCI; (2) Synthesize evidence on acupuncture-induced alterations in brain structure, function, connectivity, and metabolism in PSCI patients; (3) Evaluate the efficacy and safety of acupuncture for PSCI based on the included studies; and (4) Identify future research trends and directions in this field. Given the exploratory stage of this research area and the primary goal of capturing neuroimaging evidence on brain changes, both randomized controlled trials (RCTs) and non-RCTs were included to provide a broader perspective.
Materials and Methods
This research was conducted with strict adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines,31 and the PICO framework, which comprised population (patients with PSCI), intervention (acupuncture therapy), control (healthy controls, standard treatment, training, or alternatives), and outcome (neuroimaging changes and cognitive outcomes). The registration of this SR has been completed on the PROSPERO platform (number CRD42024589542).
Selection Criteria for Inclusion and Exclusion
To ensure a more stringent selection process for literature review, the criteria for inclusion and exclusion in the screening were established beforehand. The inclusion criteria were as follows: (1) Chinese or English-language, peer-reviewed, original neuroimaging clinical research; (2) patients met the PSCI diagnostic standards; (3) the neuroimaging techniques utilized were fMRI, MRS, fNIRS, and EEG (4) the intervention group underwent acupuncture treatment, regardless of acupoints, acupuncture methods, or treatment duration; and (5) the control group comprised healthy controls, standard treatment, training, or alternatives.
The exclusion criteria were as follows: (1) duplicate or withdrawn articles; (2) SRs, protocols, letters, experimental research, and comments; or (3) insufficient/unavailable data.
Strategies for Searching
Two independent reviewers (SY and ZY) conducted searches across the following electronic databases: Web of Science, PubMed, Embase, Cochrane Library, China National Knowledge Infrastructure, Chinese Biomedical Literature Database, WanFang Database, VIP Database, Grey Literature Database, as well as additional resources (Chinese Clinical Trial Register [ChiCTR] and ClinicalTrials.gov) from database inception to August 25, 2024. A combination of subject terms and free terms was used, with the language limited to Chinese and English. These terms included “Stroke”, “Post Stroke”, “Apoplexy”, “Cerebrovascular”, “Cerebral Hemorrhage”, “Cognitive Dysfunction”, “Cognitive Impairment”, “Age-Related Memory Disorders”, “Cognitive Decline”, “Mental Deterioration”, “Acupuncture”, “Acupuncture therapy”, “Scalp Needle”, “Warm Acupuncture”, “Electroacupuncture”, “Abdominal Needle”, “Body Acupuncture”, “Fire Acupuncture”, “Neuroimaging”, “Magnetic Resonance Imaging”, “Magnetic Resonance Spectroscopy”, “Functional Magnetic Resonance Imaging”, “fMRI”, and “Functional Near-Infrared Spectroscopy”. Appendix 1 presents the electronic database search strategy used in this study.
Study Selection and Data Extraction
After duplicates were eliminated, two separate reviewers assessed the titles and abstracts of the potentially relevant studies. The same reviewers then retrieved and examined the full-text versions of these articles to establish whether they met the inclusion criteria. In cases of disagreement, a third reviewer was consulted to mediate the discussion and ensure a unified decision.
Two independent reviewers (SY and QB) performed the data extraction process, utilizing a customized standardized form to gather pertinent information. Neuroimaging metrics were predefined as primary outcome measures. The extracted data encompassed identification details such as the first author’s name, country of origin, and year of publication. Additionally, fundamental information including study design, sample size, diagnostic criteria, age range, and sex was collected. Further specifics included information on the intervention and control groups, assessment tools, clinical outcomes, adverse events and neuroimaging outcomes. To ensure comprehensive reporting of acupuncture interventions, we adhered to the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA)32 and gathered exhaustive details on the acupuncture employed.
Quality Assessment
To evaluate the risk of bias in the RCTs, we used the Cochrane risk-of-bias tool for randomized trials (RoB 2.0).33 The RoB 2.0 tool evaluates five distinct domains for risk of bias assessment. The risk of bias for each domain was estimated and categorized separately as either “low”, “some concerns”, or “high”. In accordance with RoB 2.0, we also determined the overall risk of bias (low, some concerns, high). To assess the risk of bias in non-RCTs, we used the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool.34 The RoB assessment includes the categories: critical, serious, moderate, low, and nonexistent. Methodological quality was evaluated by two authors. In cases of disagreement, a third researcher arbitrated the final decision.
Data Analysis
Given the diversity of neuroimaging methods employed in the studies, a descriptive analytical approach was used to summarize and compare the primary characteristics and results. Narrative analysis was further applied to synthesize acupuncture-induced alterations in brain structure or function, with safety outcomes similarly described in narrative form due to limited reporting. This narrative synthesis adhered to the Synthesis Without Meta-analysis reporting guideline,35 which provides methodological standards for integrating heterogeneous quantitative evidence through structured grouping of studies, standardized presentation of outcomes, and transparent reporting of limitations.
Neuroimaging Data Evaluation Criteria
The evaluation criteria for neuroimaging changes adhered to standardized statistical thresholds for significance testing, consistent with best practices in neuroimaging analysis. For fMRI studies, significance required combined voxel-level (typically p<0.001 uncorrected or p<0.05 corrected) and cluster-level thresholds (p<0.05 after Gaussian Random Field [GRF], False Discovery Rate [FDR], or Alpha Simulation [AlphaSim] correction).36–38 Graph theory analyses employed sparsity ranges to evaluate network properties across biologically plausible connection densities.39 EEG outcomes used established metrics, while MRS relied on metabolic ratios, both with significance set at p<0.05.40
Assessment Tools
Twelve assessment tools were used to evaluate the severity of PSCI. The tools for assessing overall cognitive function included the Montreal Cognitive Assessment (MoCA; n=9; 75%), Mini-Mental State Examination (MMSE; n=5; 41.67%), and Loewenstein Occupational Therapy Cognitive Assessment (LOTCA; n=1; 8.33%). Memory function was assessed using the Revised Wechsler Memory Scale-Chinese Version (WMS-RC; n=2; 16.67%), the Auditory Verbal Learning Test (n=1; 8.33%), and the Digit Span Test (DS; n=1; 8.33%). Executive function and attention were assessed using the Trail Making Test (TMT; n=2, 16.67%). The tools used to assess neurological deficits and motor function encompassed the National Institutes of Health Stroke Scale (n=2, 16.67%) and the Fugl–Meyer Assessment (n=1, 8.33%). Finally, the tools for assessing daily living abilities and functional independence included the Modified Barthel Index (MBI; n=1; 8.33%), the Activities of Daily Living Scale (ADL; n=1; 8.33%), and the Functional Independence Measure (FIM; n=1; 8.33%).
Results
Searching and Screening
The PRISMA flowchart, presented in Figure 1, outlines the methodical process of searching for and screening the appropriate literature. Overall, 131 articles were identified using the primary search strategy. After removing duplicates, 99 trials remained. Following initial screening, 17 studies were included in analysis. Upon conducting a second, more thorough examination of full-text articles, five studies were excluded based on the inclusion criteria: two lacked neuroimaging data, and three featured ineligible treatments. Therefore, 12 studies remained27,30,41–50 for the final assessment. Appendix 2 contained the detailed rationale for excluding these five studies.
 |
Figure 1 PRISMA flowchart. Systematic searches were performed across multiple electronic databases (Web of Science [WOS], PubMed, Embase, Cochrane Library, China National Knowledge Infrastructure [CNKI], Chinese Biomedical Literature Database [CBM], WanFang [WF], VIP, Grey Literature Database) and trial registries (Chinese Clinical Trial Register [ChiCTR] and ClinicalTrials.gov) from inception to August 25, 2024. |
Characteristics of Study
The summary of the characteristics of the selected studies is presented in Table 1. The studies were published between 2014 and 2023, with all trials conducted in China. One study (8.33%) was published in English, while the remaining eleven were published in Chinese.
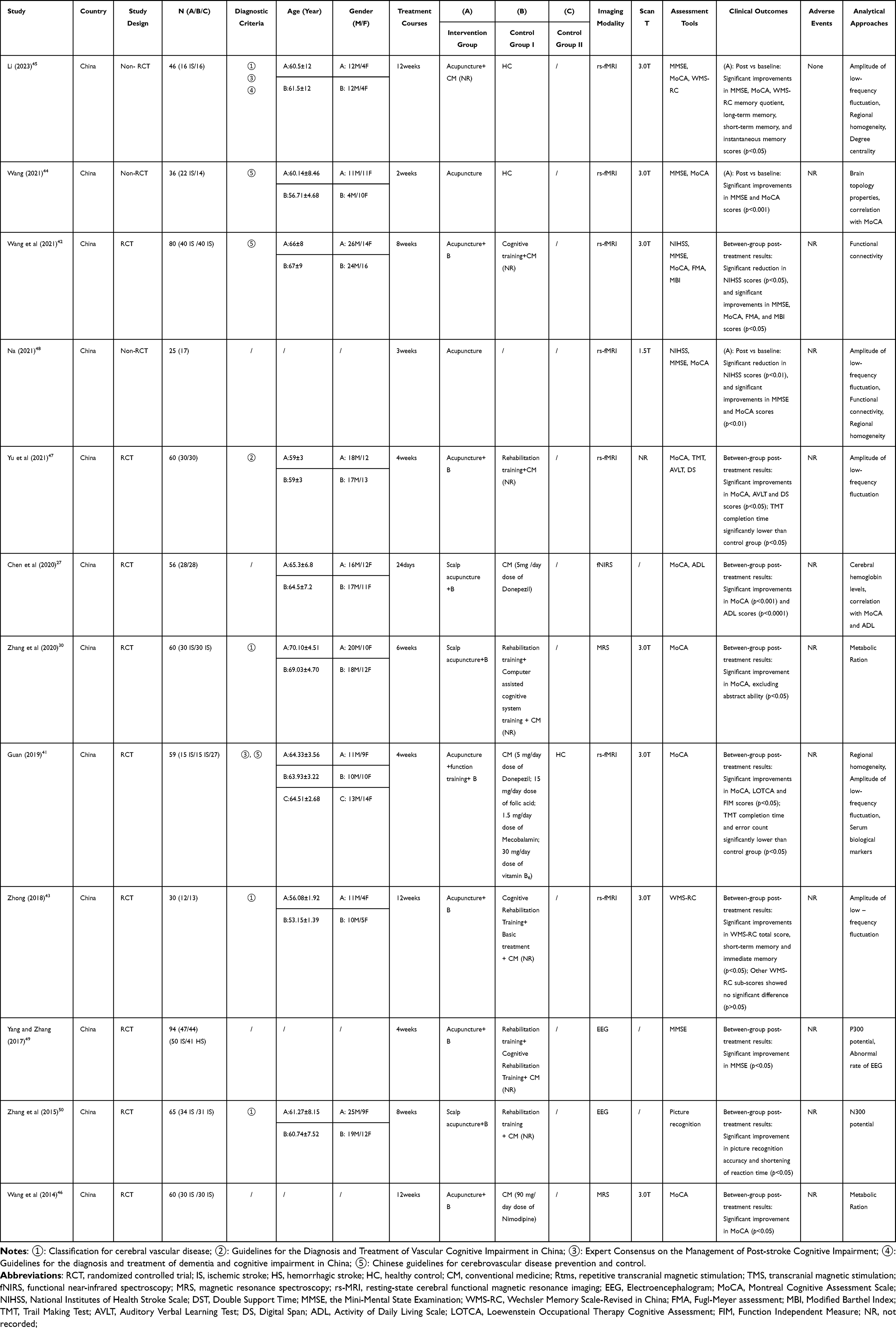 |
Table 1 Characteristics of Selected Studies |
The analysis encompassed nine RCTs and three non-RCTs. The number of participants ranged from 25 to 94. Ten trials aimed to explore whether acupuncture elicits cerebral responses, while two focused on investigating the impact of acupuncture on neural networks within the brain.
Research Participants
Overall, the study included 582 patients diagnosed with PSCI and 57 healthy volunteers. Among those diagnosed with PSCI, 383 had ischemic stroke, and 41 had hemorrhagic stroke, and the stroke type for the remaining 158 patients was not specified or differentiated. Four neuroimaging trials used the classification for cerebral vascular disease,51 three used the Chinese guidelines for cerebrovascular disease prevention and control,52 and two used the expert consensus on the management of PSCI.53 One study used a different criterion, whereas four omitted details on the diagnostic criteria. Three studies compared patients with PSCI with healthy participants, while the remaining studies solely focused on patients with PSCI. The age of the enrolled patients ranged from 53.15 to 70.1 years. Nine studies provided information on the sex of patients (265 males and 205 females). In the nine studies that only recruited patients with PSCI, the maximum and minimum sample sizes were 47 and 12 per group, respectively. In three studies that compared patients with PSCI and healthy volunteers, the matched sample sizes for PSCI/healthy controls were 1/1, 11/7, and 10/9, respectively.
Acupuncture Details
Acupuncture-related information gathered from the studies is displayed in Table 2, following the STRICTA guidelines. Eleven studies (91.7%) mentioned rationale of acupuncture, including the types of acupuncture and the reasons for providing the treatment. Participants underwent between 1 and 56 needle insertions per session. The acupoints that were most frequently used were GV 20 (Baihui) and EX-HN1 (Sishencong). Acupuncture insertion depth was 7.5–37.5 mm. Four studies (33.3%) emphasized the needle sensation (deqi) during acupuncture stimulation. Ten studies (83.3%) used manual acupuncture, one study (8.3%) employed electroacupuncture, and one (8.3%) utilized both. The most commonly used needle diameters were 0.25, 0.30, and 0.35 millimeters, with the most frequently used lengths being 25 and 40 millimeters. The number of therapy sessions ranged from 10 to 72. Only four studies (33.3%) provided details on acupuncturists.
 |
Table 2 Acupuncture-Related Information Based on Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) |
Comparison
The 12 studies included the following four comparison types: three studies (25%) compared acupuncture with healthy volunteers, one study (8.3%) used a self-control design to compare before and after treatment, two studies (16.7%) contrasted acupuncture combined with conventional medicine against conventional medicine alone and six studies (50%) compared acupuncture plus conventional medicine and training to conventional medicine and training without acupuncture.
Clinical Efficacy and Safety Outcomes
Among the 12 included studies, all 12 (100%) reported at least one clinical efficacy outcome. The most commonly used standardized cognitive measures were MoCA and MMSE. All 12 studies reported statistically significant improvements (p < 0.05) in primary clinical outcomes following acupuncture-based interventions. In RCTs, between-group comparisons demonstrated acupuncture’s significant superiority over controls across multiple domains, including global cognition, functional independence and task-based neuropsychological measures. Notably, one study observed no significant between-group differences in specific secondary memory sub-scores (WMS-RC, p> 0.05) despite confirming efficacy in primary outcomes.43 Due to substantial heterogeneity in study designs (eg, non-RCT vs RCT), interventions (eg, acupuncture alone vs combined with cognitive training), and outcome measures, a meta-analysis was not feasible. Results are summarized descriptively in Table 1.
Among the studies incorporated in this SR, only one article45 explicitly documented the absence of acupuncture-related adverse events during the intervention period. The remaining studies failed to report safety outcomes or adverse event monitoring data.
Imaging Techniques in PSCI Acupuncture Research
Studies utilized fMRI, fNIRS, EEG, and MRS to explore functional changes in the brain, event-related potentials, and metabolic ratios triggered by acupuncture in patients with PSCI. Among these, two articles specifically assessed metabolic ratios through MRS. One study used fNIRS for the evaluation of hemodynamic responses. Two studies analyzed event-related potentials (ERP) derived from EEG recordings to assess the neural responses associated with specific events. Ten trials assessed the functional alterations resulting from acupuncture. Seven studies utilized resting-state fMRI (rs-fMRI) to assess various aspects of brain activity patterns: two trials focused on functional connectivity (FC), three on regional homogeneity (ReHo), and five on the amplitude of low-frequency fluctuations (ALFF). Figure 2 displays the percentages of the various imaging tools.
 |
Figure 2 Percentages of various imaging tools. Distribution of imaging techniques used across the included studies (n = 12). Each study utilized only one technique. |
Evaluation of Quality
The methodological assessment’s results are shown in Appendices 3 and 4.
Using the RoB 2 tool, a moderate RoB was identified across all nine RCTs. When evaluating the randomization process, six studies were assessed as low risk because they provided detailed randomization descriptions, while three were categorized as having some concern due to insufficient information. In terms of deviation from the intended intervention, one study had low bias, while eight studies had some concern owing to brief representations. Two studies had participant dropout but did not report the methods for handling missing data in detail, which raised several concerns. Other studies showed low bias. It is worth noting that all studies were deemed to have low bias regarding result measurements. However, concerns arose about selective reporting of outcomes in all RCTs, owing to the absence of detailed information on protocols and registrations.
Using the ROBINS-I tool, a moderate RoB was observed in all three non-RCTs. In terms of confounders, two studies exhibited low bias, while one showed moderate RoB due to a lack of information. Regarding missing data, one study had low bias, while two studies demonstrated moderate RoB due to dropouts. It is worth mentioning that all studies demonstrated low bias concerning participant recruitment, categorization of interventions, adherence to intended interventions, assessment of outcomes, and the choice of reported data.
Results From Neuroimaging
Underlying Neural Mechanisms for Acupuncture
Evaluation criteria for neuroimaging outcomes, including statistical thresholds and correction methods, along with detailed results of acupuncture-induced brain alterations across all 12 predefined studies, are cataloged in Appendix 5. Brain alterations most frequently associated with repeated acupuncture in patients with PSCI are situated in the cingulate gyrus (a key node in the default mode network [DMN] and salience network [SN]; n=4), parahippocampal gyrus (a DMN-associated region; n=4), prefrontal cortex (a key node in the central executive network [CEN] and frontoparietal network [FPN]; n=4), and fusiform gyrus (a key region for visual processing and recognition; n=3). The DMN, CEN, FPN, and SN are crucial components formed by the brain areas mentioned in these trials. Except for the EEG results, all other observations were derived from resting-state conditions.
Using fNIRS, a study27 demonstrated that repeated acupuncture enhanced the hemodynamic response in the prefrontal and motor cortices of both hemispheres in patients with PSCI. Furthermore, two MRS trials30,46 demonstrated an increase in the ratio of N-acetylaspartate to creatine and a decrease in the ratios of choline to creatine and myo-inositol to creatine within the hippocampus (a DMN-associated region) and cerebral infarction areas of patients with PSCI, which could be attributed to routine acupuncture.
Two studies that used EEG in conjunction with ERP49,50 revealed that repeated acupuncture can shorten the latency of the P300/N300 potential and prolong its amplitude in patients with PSCI. Specifically, the results revealed a significant shortening of the P300 component latency in the EEG recordings of these patients. This is a well-established indicator of enhanced cognitive processing speed and efficiency, primarily observed in the frontal lobe, parietal lobe, precentral gyrus, and postcentral gyrus for P300, and in the frontal lobe, precentral gyrus, postcentral gyrus, and fronto-central region for N300. Additionally, an increase in the amplitude of the P300/N300 complex was observed, suggesting that acupuncture stimulates neural activity within the brain regions corresponding to these EEG components.
Using fMRI trials, four neuroimaging studies documented increases or decreases in ReHo or ALFF across various brain regions following continuous acupuncture treatment.41,45,47,48 In terms of ALFF, increases were observed in the parahippocampal gyrus, precuneus (a key node in the DMN), and middle temporal gyrus (a DMN-associated region) within the memory region; the superior parietal gyrus (a key node of the FPN) and fusiform gyrus within the visuospatial region; the cingulate gyrus, insula (a key node of the SN), and thalamus (a key node of the SN) within the emotional processing and cognitive function regions; and the inferior frontal gyrus (a key node of the FPN) and middle frontal gyrus (a key node of the FPN) within the language/executive function regions. However, decreases in ALFF were noted in the inferior temporal gyrus, fusiform gyrus, superior occipital gyrus, inferior occipital gyrus, and superior parietal lobule within the visuospatial region, and the superior frontal, inferior frontal, and middle temporal gyri within the language/executive function regions. Regarding ReHo, increases were found in the parahippocampal gyrus, temporal pole, and precuneus within the memory region; the middle frontal gyrus within the language/executive function region; and the superior parietal gyrus within the visuospatial region. Nevertheless, decreases in ReHo were observed in the parahippocampal and middle temporal gyrus within the memory region, the lenticular and ventrolateral thalamic nuclei within the emotional processing and cognitive function regions, and the inferior frontal gyrus within the language/executive function region. Furthermore, one study43 compared the differences in ALFF values, revealing significant disparities in these changes within memory areas (eg right middle temporal gyrus), visuospatial areas (eg parietal lobule), cognitive function areas (eg cingulate gyrus) and emotional-affective processing, and language/executive function areas (eg frontal lobe, postcentral gyrus, and inferior frontal gyrus).
The ALFF and ReHo results indicated that acupuncture can exert extensive and complex effects on the functional brain regions of patients with PSCI, bidirectionally regulating activity disturbances in certain associated brain regions. It is noteworthy that following acupuncture treatment, changes in ALFF within the fusiform and inferior frontal gyri and changes in ReHo within the parahippocampal gyrus exhibited a dual nature. This duality may be associated with various factors, such as the specific parameters of acupuncture treatment, individual differences, and disease states. Additionally, increases or decreases in ALFF/ReHo do not necessarily imply an absolute enhancement or decline in function. Rather, they may represent a functional reorganization or optimization of the brain in response to acupuncture.
Moreover, one study44 reported that nodal properties were mainly altered in patients with PSCI after acupuncture treatment. Graph theory analysis was employed to investigate these changes. The results indicated an increase in nodal centrality and local efficiency within brain areas related to cognitive functions, particularly in visuospatial areas (eg the fusiform gyrus, inferior occipital gyrus, and lingual gyrus) and memory areas (eg the precuneus and parahippocampal gyrus).
By performing an FC analysis, one study48 demonstrated increased FC in the superior marginal gyrus, superior temporal gyrus, anterior cuneiform lobe, angular gyrus, superior occipital gyrus, inferior parietal lobe, posterior cingulate gyrus, and decreased FC in the middle occipital gyrus after acupuncture. Furthermore, employing FC analysis focused on specific regions of interest, another study44 found that frequent acupuncture led to an enhancement in FC. Specifically, there was an increase in connectivity between the left hippocampus and regions, such as the middle frontal and right inferior gyri, as well as between the right hippocampus and areas including the left middle gyrus, inferior gyrus, parietal lobe, and superior frontal gyrus (a key node of the FPN).
The brain regions mentioned in previously conducted studies can generally be grouped according to their participation in four distinct neural pathways: DMN (eg, precuneus, anterior cingulate, parahippocampal gyrus, hippocampus, and middle temporal gyrus), CEN (eg, anterior cingulate, inferior parietal lobule, and superior dorsolateral frontal gyrus), FPN (eg, superior frontal gyrus, middle frontal gyrus, inferior frontal gyrus, and inferior parietal lobule), and SN (eg, parahippocampal gyrus, insula, anterior cingulate, and thalamus). The primary results from the consistent acupuncture are displayed in Figure 3.
 |
Figure 3 Results from consistent acupuncture. Lateral view of the left hemisphere. The reviewed studies indicated that sustained acupuncture primarily impacts specific brain regions and networks. Brain regions: ACG (anterior cingulate gyrus): Involved in emotion regulation, attention, and conflict monitoring; Hip (hippocampus): Critical for memory formation and spatial navigation; IFG (inferior frontal gyrus): A key node in the language network and also involved in cognitive control; IPL (inferior parietal lobule): Associated with sensory integration, mathematical cognition, and language processing; INS (insula): Plays a central role in interoceptive awareness, emotion, and pain processing; MFG (middle frontal gyrus): Implicated in working memory and executive functions; MTG (middle temporal gyrus): Involved in semantic memory and language comprehension; PCUN (precuneus): A key hub of the default mode network, associated with self-referential thought and consciousness; PHG (parahippocampal gyrus): Important for memory encoding and retrieval, and contextual association; SFG/SFGdor (superior frontal gyrus, dorsolateral): Primarily responsible for higher-order cognitive functions like planning, decision-making, and working memory; THA (thalamus): Acts as the central relay station for sensory and motor signals to the cerebral cortex. Brain networks: blue network, default mode network; green network, central executive network; yellow network, frontoparietal network; red network, salience network. |
The Relationship Between Neuroimaging Results and Clinical Outcomes
Three studies reported a relationship between the overall cognitive function and neuroimaging outcomes. Specifically, MoCA scores negatively correlated with degree centrality in the left inferior occipital gyrus of patients with PSCI after acupuncture treatment (r= −0.461, p= 0.031).44 However, MoCA scores are positively correlated with activity levels in the right frontal gyrus and inferior temporal gyrus (r= 0.365, p= 0.047; r= 0.387, p=0.035).41 Furthermore, LOTCA scores are positively correlated with activity levels in the right fusiform gyrus and right dorsolateral prefrontal cortex (r= 0.448, p=0.013; r =0.361, p=0.05).41 One study explored the relationship between neuroimaging outcomes and various memory function indicators. Total WMS-RC scores positively correlated with neural activity intensities in the right middle frontal gyrus and right inferior parietal lobule (r= 0.537, p=0.02; r =0.505, p=0.02). Moreover, the neural activity intensity in the right middle frontal gyrus was positively correlated with short-term memory (r= 0.479, p= 0.048), whereas the neural activity intensity in the left posterior cingulate gyrus was positively correlated with long-term memory (r= −0.424, p= 0.035).43 Regarding executive function indicators, TMT-A performance is negatively correlated with activity levels in the right inferior temporal gyrus (r= −0.394, p= 0.031).41
Discussion
To date, 12 articles measuring brain activity have been considered, providing visual evidence for a deeper understanding of the underlying central mechanisms of acupuncture in the treatment of PSCI. Subsequently, here, we discuss three essential areas: evaluating the current design and suggesting methodologies for improvement, assessing neuroimaging findings in PSCI after acupuncture, and outlining future research directions.
Evaluating Current Design and Suggesting Methodologies for Improvement
This section evaluates methodological weaknesses and outlines key recommendations for improving the design of future acupuncture-neuroimaging studies in PSCI.
Our review of 12 neuroimaging research revealed that, in terms of design, three were non-RCTs, while nine were RCTs. However, none of these studies exhibited high methodological quality, primarily due to issues with result selection and biases from missing data. Therefore, to ensure the validity of neuroimaging trials investigating the effects of acupuncture in the treatment of PSCI, future research should adhere to the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions.54,55 Notably, only two studies had sample sizes of 80 or larger, whereas 10 studies had sample sizes of 65 or smaller. In the field of neuroscience, the dependability and reproducibility of predicted outcomes may be jeopardized by limited sample sizes.56 Therefore, increasing the sample size through standardized procedures is expected to improve the statistical significance of the research findings.
Variability in diagnostic criteria for PSCI was observed across studies. To enhance research quality, it is necessary to adopt a unified and stricter set of inclusion and exclusion criteria for defining PSCIs. Four studies employed the classification for cerebral vascular disease,51 which are widely used for the clinical diagnosis of apoplexy. Three studies adopted the Chinese guidelines for cerebrovascular disease prevention and control.52 However, the expert consensus on the management of PSCI,53 used by two studies for diagnosing PSCI, may offer a more specialized and comprehensive diagnostic approach than the general cerebrovascular criteria.
Although four comparison models were used, most studies focused solely on comparing acupuncture with other methods, without exploring factors such as variations in acupuncture insertion depth and other influences on efficacy. However, variations in acupuncturist qualifications, sensation of deqi, and the interval and length of treatments influenced outcomes. Hence, standardizing acupuncture protocols by establishing clear guidelines is crucial. Among the studies reviewed, only four provided descriptions of the acupuncturists involved, leaving information on the acupuncturists uncertain in other studies. Thus, to ensure consistency and reliability, it is recommended that each study use a single, skilled acupuncturist to conduct the treatments.
Despite the use of various assessment tools to comprehensively evaluate PCSI severity in the 12 studies, these tools have practical limitations that require further improvement. Specifically, regarding the assessment of overall cognitive function, the applicability of the MoCA is limited in illiterate and low-educated elderly individuals. To address this, the MOCA Basic, a revised version designed specifically for populations with low education or literacy levels, is recommended for future use in appropriate populations. To assess daily living abilities and functional independence, tools such as the MBI, ADL scale, and FIM provide comprehensive evaluations of patients’ self-care abilities, social skills, and work capabilities. However, these instruments may overly rely on patient self-reports, neglecting the observations and judgments of assessors. Research indicates that self-report measurement methods may not fully reflect an individual’s true capabilities, particularly when confronted with complex ADL tasks.57 Consequently, future research should emphasize training and standardization of assessors to enhance the objectivity and accuracy of the assessments. Additionally, incorporating objective indicators, such as motion trajectory analysis, into the assessment system could offer a more comprehensive evaluation of patients’ daily living abilities and functional independence.
Although all 12 studies unanimously reported statistically significant improvements in primary clinical outcomes (p < 0.05), limitations in safety reporting undermine the translational potential of these findings. Only one study explicitly documented the absence of acupuncture-related adverse events,45 while the remaining 11 failed to report any safety monitoring data. This constitutes a methodological gap that contravenes CONSORT and STRICTA guidelines.32,54 Future trials must prioritize safety documentation using standardized tools and report adverse events as a core outcome. Although acupuncture demonstrated statistically significant superiority in global cognition and functional independence compared to control groups, methodological heterogeneity across studies precluded quantitative data synthesis via meta-analysis, thereby compromising the interpretability of clinical implications. To address this limitation, future research should employ validated sham acupuncture controls and standardized acupoint regimens to ensure intervention consistency. Furthermore, variability in statistical thresholds and correction methods across studies (eg, GRF vs FDR vs AlphaSim) may affect the comparability of neuroimaging outcomes. Future consensus on standardized thresholds is critical for cross-study synthesis.
Assessment of Neuroimaging Findings for PSCI After Acupuncture
This section synthesizes and interprets the key neuroimaging findings regarding the central mechanisms through which acupuncture may exert its therapeutic effects on PSCI.
The following neuroimaging techniques have been used to evaluate cerebral responses to acupuncture therapy for PSCI: fMRI, EEG, fNIRS, and MRS. fMRI was employed to detect alterations in the oxygenation levels of brain tissue, which reflect metabolic changes elicited by task-evoked neural activity or spontaneous neural fluctuations occurring in the absence of conscious cognition.58 EEG, which directly detects electrical signals generated by neural activity in the cerebral cortex through electrodes, has been used to characterize post-stroke recovery mechanisms for motor, language, and cognitive deficits and to predict treatment responses to experimental therapies.59 ERP, as a neuroelectrophysiological detection method with high temporal resolution, offers advantages such as real-time capability, objectivity, and broad accessibility, making it promising for diagnosing PSCI.60 MRS measures neurotransmitter levels and examines changes in brain metabolites.61 fNIRS monitors and assesses alterations in neuronal activity patterns by detecting optical absorption properties within cerebral tissue.62
Studies using fNIRS have demonstrated that acupuncture enhances cerebral hemodynamic responses in patients with PSCI, indicating it can improve brain function. Furthermore, MRS trials have revealed that acupuncture also positively impacts brain metabolism. Together, these findings provide mechanistic support for the potential use of acupuncture in treating PSCI. Studies employing task-state EEG, specifically analyzing ERPs associated with auditory and visual stimuli, have collectively revealed a significant positive impact of acupuncture on neural processing speed in patients with PSCI. In task-state EEG studies involving auditory stimuli, the P300 component has emerged as a crucial indicator of the brain’s response speed and cognitive processing efficiency to auditory stimuli. As an ERP component closely associated with attention, memory, and decision-making processes, the shortened latency and increased amplitude of P300 reflect the enhanced auditory stimulus processing capabilities of the brain. In contrast, in task-state EEG studies involving visual stimuli, the N300 component serves as a key component for evaluating the brain’s ability to process visual stimuli. Similar to the P300, the shortened latency and increased amplitude of the N300 are also indicative of accelerated visual stimulus processing speed and enhanced neural activity, suggesting that acupuncture not only improves auditory processing but also significantly enhances visual information recognition and processing efficiency.
The cingulate cortex (a key node in the DMN), parahippocampal gyrus, prefrontal cortex, and fusiform gyrus are among the common brain regions influenced by acupuncture in PSCI. These regions align with established pathological markers of post-stroke cognitive decline, as evidenced by neuroimaging findings demonstrating significantly reduced FC in the posterior cingulate cortex and altered FC patterns in the medial prefrontal cortex and hippocampus in stroke patients, especially those with PSCI,63 while parahippocampal gyrus atrophy is linked to episodic memory deficits.64 Our study found that patients with PSCI exhibit significantly reduced regional coherence in the anterior and posterior cingulate cortices, indicating impaired FC. This reduction in FC may affect cognitive functions such as attention, executive abilities, and memory, suggesting that cognitive impairments in patients with PSCI are associated with cingulate cortex dysfunction.65 The parahippocampal gyrus, the central region of the medial temporal lobe, is vital for information storage and retrieval, and damage to this area may lead to memory impairment and other cognitive issues.66 The prefrontal cortex is a crucial region of the brain responsible for higher-order cognitive functions, including executive function, attention, working memory, and decision-making.67 One study has shown that patients with prefrontal cortex injuries may exhibit increased error rates and alterations in contrast perception thresholds during memory tasks.68 Additionally, the interplay between the prefrontal cortex and basal nuclei constitutes a vital component of cognitive dysfunction following stroke. Research has demonstrated that supplementary connectivity routes within the neural framework, which govern effective communication between the prefrontal cortex and basal nuclei in patients with stroke, may aid in the recovery of cognitive impairments post-stroke.69 The fusiform gyrus, the brain region vital for processing visual information and language comprehension, may experience impairments in visual memory and language processing following damage.70 Therefore, these brain regions serve as primary targets for acupuncture in modulating PSCI.
Notably, neuroimaging analyses evaluating the neurological effects of acupuncture on PSCI have demonstrated the potential of acupuncture in modulating brain networks. The essential pathways implicated in acupuncture-induced improvement of PSCI can be outlined as follows: regions within the DMN (eg, precuneus, anterior cingulate, parahippocampal gyrus, hippocampus, and middle temporal gyrus), CEN (eg, anterior cingulate, inferior parietal lobule, and superior dorsolateral frontal gyrus), FPN (eg, superior frontal gyrus, middle frontal gyrus, inferior frontal gyrus, and inferior parietal lobule), and SN (eg, parahippocampal gyrus, insula, anterior cingulate, and thalamus) play pivotal roles in mediating the brain alterations observed in response to acupuncture-based interventions for PSCI. These brain networks, which align with the “triple-network model” (encompassing the DMN, CEN, and SN) implicated in cognitive processing across neurodegenerative conditions,71 are closely associated with the pathological processes of PSCI. Altered connectivity within the DMN in patients with stroke may serve as the underlying basis for the reduction in episodic memory following stroke.72 The DMN, associated with internalized cognitive processes,73 plays a pivotal role in the neuropathophysiology of PSCI.65 It is noteworthy that acupuncture’s enhancement of DMN integrity parallels mechanisms observed in non-stroke cognitive disorders.74 The CEN serves as a crucial executive control center in the brain and is responsible for a multitude of advanced cognitive functions, including working memory, attentional control, decision making, and emotional regulation.75 The FPN is central to cognitive control and behavioral coordination, exhibiting dynamic interactions with other functional brain networks.76 One study indicated that patients with PSCI exhibit impaired FC centered on the FPN, suggesting that this incomplete FPN-centered connection may be the underlying pathological mechanism of PSCI, emphasizing the crucial significance of the FPN in cognitive control functions that are disrupted by stroke.77 The SN dynamically coordinates the functions of other brain networks, ensuring effective allocation of attention and resources in response to internal and external challenges, thereby maintaining a balance between cognition and emotion.78 Acupuncture exerts therapeutic effects on PSCI by targeting the DMN, CEN, FPN, and SN.
Future Research Directions
This section outlines critical future research priorities to advance mechanistic understanding of acupuncture for PSCI.
The present investigation did not directly address the influence of acupuncture on specific cerebral regions in the context of PSCI. Hence, while research has explored acupuncture’s general neurological effects, the precise mechanisms underlying its action in distinct brain areas remain elusive. Given the gaps in current research and the crucial role of specific brain regions, further studies are needed to clarify the neurological impacts of acupuncture on regions such as the cingulate cortex, parahippocampal gyrus, prefrontal cortex, and fusiform gyrus. These efforts will deepen our understanding of acupuncture’s therapeutic mechanisms in PSCI, and may provide new perspectives on the effects of acupuncture on other neurodegenerative disorders or cognitive impairments.
Neuroimaging trials are crucial for elucidating brain function. Recent research has shown that acupuncture influences brain function, particularly within the triple-network model comprising the DMN, CEN, and SN, which are vital for cognitive processing and brain function.79–81 However, no existing neuroimaging trials have specifically explored the impact of acupuncture on PSCI using this model. Therefore, designing specialized neuroimaging experiments to directly assess how acupuncture modulates triple-network activity in patients with PSCI will help reveal the specific neural mechanisms responsible for its beneficial effects.
Acupuncture has demonstrated efficacy in treating PSCI; however, the trials included in this SR focused solely on its sustained effects, without considering its immediate impact. Consequently, future studies should establish various time points (eg, immediately after acupuncture treatment, a few hours post-treatment, and a several days after treatment) to assess both immediate and sustained effects. This approach will provide a more comprehensive understanding of acupunctures’ mechanisms and offer theoretical support for its clinical application.
Current neuroimaging studies have primarily focused on correlational relationships between acupuncture therapy and functional brain changes.82,83 Most existing evidence relies on cross-sectional designs, which capture associations but cannot establish temporal or causal pathways. However, to gain deeper insights into how acupuncture therapy influences brain function, it is essential to determine whether these effects are directional or causal. Future studies should adopt longitudinal or interventional neuroimaging designs with repeated measurements to trace neuroplastic changes over time and better infer causality. This will enable more accurate assessment of the acupuncture’s efficacy and provide a foundation for further exploration of its mechanisms. Furthermore, all 12 trials concentrated on structural or functional brain changes, using a single neuroimaging method. However, PSCI is a multifaceted disorder of the central nervous system, caused by stroke lesions that destroy the function of corresponding brain regions.84 Therefore, integrating diverse methodologies is crucial. In particular, multimodal neuroimaging approaches are needed to capture the complexity of PSCI. Such approaches generate high-dimensional and complex datasets. To analyze these data effectively, machine learning algorithms play a particularly crucial role. These models are capable of extracting key features from vast amounts of multimodal data, which are related to both acupuncture treatment and changes in brain function. Through this process, underlying correlations and mechanisms can be revealed.85,86 Accordingly, future research should not only collect and analyze multimodal data but also fully leverage machine learning to enhance data processing accuracy and efficiency, enabling more precise assessments of the mechanistic response to acupuncture treatment for PSCI.
Strengths and Limitations
To our knowledge, this is the first SR focusing specifically on neuroimaging evidence for acupuncture in PSCI. Specifically, this SR highlights the brain regions and networks influenced by acupuncture, evaluates its effectiveness and safety, and analyzes correlations between clinical indicators and neuroimaging outcomes to provide practical insights for future clinical applications. However, this review had some limitations. First, despite extensive research efforts, the scarcity of studies meeting the inclusion criteria severely limits the scope and generalizability of our findings. Second, the use of varied analytical imaging methods in the included studies made it challenging to conduct a quantitative meta-analysis. Third, critical safety assessments were neglected. Fourth, heterogeneity restricted the synthesis to descriptive reporting rather than quantitative pooling, precluding effect size estimation. Finally, these studies focused solely on the effects of sustained acupuncture, neglecting its immediate impact, which limits our understanding of the comprehensive effects of acupuncture.
Conclusion
Acupuncture for PSCI is effective, and its neural mechanisms may involve regulating cognition-related brain networks. However, to validate these findings beyond the limitations of current low-quality, small-sample studies, future research should integrate multi-modal imaging techniques within multicenter, large-sample, rigorously designed RCTs, while systematically collecting safety data.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author, Zihan Yin.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing. All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by the National Natural Science Foundation of China (Grant number 82505760), the Central Financial Transfer Payment to Local Projects in 2022 of the National Administration of Traditional Chinese Medicine, and the Sichuan Province Science and Technology Innovation Cultivation Program (Grant numbers MZGC20240094 and 25QNJJ0414).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Kuriakose D, Xiao Z. Pathophysiology and treatment of stroke: present status and future perspectives. Int J Mol Sci. 2020;21:7609. doi:10.3390/ijms21207609
2. Douiri A, Rudd AG, Wolfe CDA. Prevalence of poststroke cognitive impairment. Stroke. 2013;44:138–145. doi:10.1161/STROKEAHA.112.670844
3. Du Y, Zhang L, Liu W, et al. Effect of acupuncture treatment on post-stroke cognitive impairment: a randomized controlled trial. Medicine. 2020;99:e23803. doi:10.1097/MD.0000000000023803
4. Qu YJ, Zhuo L, Zhan SY. Epidemiological characteristics of poststroke cognitive impairment in China: a systematic review. Chin J Geriatr Heart Brain Vessel Dis. 2013;15:1294–1301. doi:10.3969/j.issn.1009-0126.2013.12.018
5. Liu YT, Chen HJ, Zhao K, He WL, Lin SS, He JC. High levels of plasma fibrinogen are related to post-stroke cognitive impairment. Brain Behav. 2019;9:e01391. doi:10.1002/brb3.1391
6. Zhang Q, Fu Y, Lu YH, et al. Impact of virtual reality-based therapies on cognition and mental health of stroke patients: systematic review and meta-analysis. J Med Internet Res. 2021;23:e31007. doi:10.2196/31007
7. Rost NS, Brodtmann A, Pase MP, et al. Post-stroke cognitive impairment and dementia. Circ Res. 2022;130:1252–1271. doi:10.1161/CIRCRESAHA.122.319951
8. Droś J, Klimkowicz-Mrowiec A. Current view on post-stroke dementia. Psychogeriatrics. 2021;21:407–417. doi:10.1111/psyg.12666
9. Kim KY, Shin KY, Chang K-A. Potential biomarkers for post-stroke cognitive impairment: a systematic review and meta-analysis. Int J Mol Sci. 2022;23:602. doi:10.3390/ijms23020602
10. Chi NF, Chao SP, Huang LK, et al. Plasma amyloid Beta and Tau levels are predictors of post-stroke cognitive impairment: a longitudinal study. Front Neurol. 2019;10:715. doi:10.3389/fneur.2019.00715
11. Kavirajan H, Schneider LS. Efficacy and adverse effects of cholinesterase inhibitors and memantine in vascular dementia: a Meta-analysis of randomised controlled trials. Lancet Neurol. 2007;6:782–792. doi:10.1016/S1474-4422(07)70195-3
12. Narasimhalu K, Effendy S, Sim CH, et al. A randomized controlled trial of rivastigmine in patients with cognitive impairment no dementia because of cerebrovascular disease. Acta Neurol Scand. 2010;121:217–224. doi:10.1111/j.1600-0404.2009.01263.x
13. Kim DH, Brown RT, Ding EL, Kiel DP, Berry SD. Dementia medications and risk of falls, syncope, and related adverse events: meta-analysis of randomized controlled trials. J Am Geriatr Soc. 2011;59:1019–1031. doi:10.1111/j.1532-5415.2011.03450.x
14. Bao X, Li L, Liu H, et al. Effect of acupuncture combined with rehabilitation on cognitive and motor functions in poststroke patients. Anat Rec. 2021;304:2531–2537. doi:10.1002/ar.24700
15. Gao J, Zhao C, Jiang W, Zheng B, He Y. Effect of acupuncture on cognitive function and quality of life in patients with idiopathic trigeminal neuralgia. J Nerv Ment Dis. 2019;207:171–174. doi:10.1097/NMD.0000000000000937
16. Wang X, Zhou H, Yan CQ, et al. Cognitive and hippocampal changes in older adults with subjective cognitive decline after acupuncture intervention. Am J Geriatr Psychiatr. 2024;32:1014–1027. doi:10.1016/j.jagp.2024.03.001
17. Han JZ, Yang Y, Wang YF, et al. Effectiveness and safety of governor vessel acupuncture therapy for post-stroke cognitive impairment: a Meta-analysis of randomized controlled trials. Ageing Res Rev. 2024;99:102355. doi:10.1016/j.arr.2024.102355
18. Kuang X, Fan WJ, Hu JW, et al. Acupuncture for post-stroke cognitive impairment: a systematic review and meta-analysis. Acupunct Med. 2021;39:577–588. doi:10.1177/09645284211009542
19. Li LY, Yang LY, Luo B, et al. Acupuncture for post-stroke cognitive impairment: an overview of systematic reviews. Int J Gen Med. 2022;15:7249–7264. doi:10.2147/IJGM.S376759
20. Zhan J, Pan R, Guo Y, et al. Acupuncture at Baihui(GV 20) and Shenting(GV 24) combined with basic treatment and regular rehabilitation for post-stroke cognitive impairment: a randomized controlled trial. Chin Acupunct Moxibustion. 2016;36:803–806. doi:10.13703/j.0255-2930.2016.08.007
21. Zhou L, Wang Y, Qiao J, Wang QM, Luo X. Acupuncture for improving cognitive impairment after stroke: a Meta-analysis of randomized controlled trials. Front Psychol. 2020;11:549265. doi:10.3389/fpsyg.2020.549265
22. Hoffstaedter F, Grefkes C, Roski C, Caspers S, Zilles K, Eickhoff SB. Age-related decrease of functional connectivity additional to gray matter atrophy in a network for movement initiation. Brain Struct Funct. 2015;220:999–1012. doi:10.1007/s00429-013-0696-2
23. Tomasi D, Volkow ND. Functional connectivity density and the aging brain. Mol Psychiatry. 2012;17:471. doi:10.1038/mp.2012.27
24. Bordet R, Ihl R, Korczyn AD, et al. Towards the concept of disease-modifier in post-stroke or vascular cognitive impairment: a consensus report. BMC Med. 2017;15:107. doi:10.1186/s12916-017-0869-6
25. El Husseini N, Katzan IL, Rost NS, et al. Cognitive impairment after ischemic and hemorrhagic stroke: a scientific statement from the American heart association/American stroke association. Stroke. 2023;54:E272–E291. doi:10.1161/STR.0000000000000430
26. Cespón J, Miniussi C, Pellicciari MC. Interventional programmes to improve cognition during healthy and pathological ageing: cortical modulations and evidence for brain plasticity. Ageing Res Rev. 2018;43:81–98. doi:10.1016/j.arr.2018.03.001
27. Chen J, Li H, Zeng C, Li J, Zhao B. Evaluation of the recovery outcome of poststroke cognitive impairment after cluster needling of scalp acupuncture therapy based on functional near-infrared spectroscopy. Brain Behav. 2020;10:e01731. doi:10.1002/brb3.1731
28. Sun HH, Zhu JF, Liu B, et al. Clinical effects of acupuncture-assisted transcranial magnetic stimulation therapy on cognitive impairment in stroke patients. J Prev Med Chin People’s Liberation Army. 2019;37:188–189. doi:10.13704/j.cnki.jyyx.2019.06.091
29. Xiong D. Exploring the Effect of Scalp Acupuncture Combined with Rtms on Cognitive Function in Stroke Patients Based on Fractional Amplitude of Low Frequency Fluctuation. Hunan University of Chinese Medicine; 2023.
30. Zhang JB, Wei RP, Yang H, Shen YX, Zheng J. Scalp acupuncture combined with computer-assisted cognitive training for treating cognitive impairment after stroke: a magnetic resonance spectroscopy study in the elderly. Chin J Gerontol. 2020;40:4067–4070. doi:10.3969/j.issn.1005-9202.2020.19.011
31. Page MJ, Mckenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–189. doi:10.1016/j.jclinepi.2021.03.001
32. Macpherson H, Altman DG, Hammerschlag R, et al. Stricta revision group. J Chin Integr Med. 2010;8:804–818. doi:10.3736/jcim20100902
33. Sterne JAC, Savović J, Page MJ, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
34. Sterne JAC, Hernán MA, Reeves BC, et al. Robins-i: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
35. Campbell M, McKenzie JE, Sowden A, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020;368:l6890. doi:10.1136/bmj.l6890
36. Eklund A, Nichols TE, Knutsson H. Cluster failure: why fMRI inferences for spatial extent have inflated false-positive rates. Proc Natl Acad Sci U S A. 2016;113:7900–7905. doi:10.1073/pnas.1602413113
37. Nichols TE, Das S, Eickhoff SB, et al. Best practices in data analysis and sharing in neuroimaging using MRI. Nat Neurosci. 2017;20:299–303. doi:10.1038/nn.4500
38. Woo CW, Krishnan A, Wager TD. Cluster-extent based thresholding in fMRI analyses: pitfalls and recommendations. Neuroimage. 2014;91:412–419. doi:10.1016/j.neuroimage.2013.12.058
39. Wang J, Wang X, Xia M, et al. GRETNA: a graph theoretical network analysis toolbox for imaging connectomics. Front Hum Neurosci. 2015;9:386. doi:10.3389/fnhum.2015.00386
40. Jaiswal MK. Toward a high-resolution neuroimaging biomarker for mild traumatic brain injury: from bench to bedside. Front Neurol. 2015;6:148. doi:10.3389/fneur.2015.00148
41. Guan Y. Effect of Acupuncture-Rehabilitation Therapy on Bold-Fmri and Serum Biomarkers in Cognitive Dysfunction After Ischemic Stroke Patients. Heilongjiang University of Chinese Medicine; 2019.
42. Wang F, Gao S, Yang L. Efficacy observation of acupuncture combined with cognitive training for cognitive impairment after ischemic stroke. Shanghai J Acupunct Moxibust. 2021;40:795–800. doi:10.13460/j.issn.1005-0957.2021.07.0795
43. Zhong H. The Effects of Acupuncture at the Shenting and Baihui Acupoints on Memory Function in Post-Stroke Patients: A fMRI Study Based Amplitude of Low Frequency Fluctuation. Fujian University of Traditional Chinese Medicine; 2018.
44. Wang R. A Study of the Brain Function Network in PSCI Patients Treated with Acupuncture. North Sichuan Medical College; 2021.
45. Li XY. A Study on the Central Mechanism of “Regulating Mind and enlightening Wisdom” Acupuncture to Improve the Cognitive Function of Patients with Mild Cognitive Impairment After Stroke Based on Rs-Fmri. Tianjin University of Chinese Medicine; 2023.
46. Wang F, Liang H, Chen S, Huang J, Lin Q. Research on magnetic resonance spectroscopy study of acupuncture regulation of brain tissue metabolism in treating mild cognitive impairment after stroke. J Emerg Tradit Chin Med. 2014;23:1928–1930. doi:10.3969/j.issn.1004-745X.2014.10.072
47. Yu YL, Cheng MD, Ma M, Liu L. Effect of bo’s abdominal acupuncture therapy on the resting-state fMRI in patients with cognitive impairment after stroke. Shanghai J Acupunct Moxibust. 2021;40:1293–1298. doi:10.13460/j.issn.1005-0957.2021.11.1293
48. Na BQ. Resting functional Magnetic Resonance Imaging Study of Cognitive Dysfunction in Convalescent Stroke Patients. Inner Mongolia Medical University; 2021.
49. Yang M, Zhang B. Efficacy observation of acupuncture combined with cognitive function training in treating post-stroke cognitive impairment in 47 cases. Yunnan J Tradit Chin Med Materia Med. 2017;38:64–66. doi:10.16254/j.cnki.53-1120/r.2017.02.028
50. Zhang JB, Han B, Hua Y. Clinic observation of event-related potentials of electro-acupuncture in treating cognitive impairment of cerebral infarction patients. Chin Arch Tradit Chin Med. 2015;33:1384–1386. doi:10.13193/j.issn.1673-7717.2015.06.033
51. Chinese Society of Neurology, and Chinese Society of Neurosurgery. Classification for cerebral vascular disease. Chin J Neurol. 1996;29:376–378.
52. Ministry of Health Disease Control Department, and Chinese Society of Neurology. Chinese guidelines for cerebrovascular disease prevention and control (excerpt). Chin J Contemp Neurol Neurosurg. 2007;7:17–70. doi:10.3969/j.issn.1672-6731.2007.01.031
53. Chinese Stroke Association, and Poststroke Cognitive Impairment Management Expert Committee. Expert consensus on the management of poststroke cognitive impairment. Chin J Stroke. 2017;12:519–531. doi:10.3969/j.issn.1673-5765.2017.06.011
54. Bian Z, Liu B, Moher D, et al. Consolidated standards of reporting trials (CONSORT) for traditional Chinese medicine: current situation and future development. Front Med. 2011;5:171–177. doi:10.1007/s11684-011-0132-z
55. Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. 2019;2019:ED000142. doi:10.1002/14651858.ED000142
56. Moayedi M, Salomons TV, Atlas LY. Pain neuroimaging in humans: a primer for beginners and non-imagers. J Pain. 2018;19:961.e1–961.e21. doi:10.1016/j.jpain.2018.03.011
57. Mlinac ME, Feng MC. Assessment of activities of daily living, self-care, and Independence. Arch Clin Neuropsychol. 2016;31:506–516. doi:10.1093/arclin/acw049
58. Chen JYE, Glover GH. Functional magnetic resonance imaging methods. Neuropsychol Rev. 2015;25:289–313. doi:10.1007/s11065-015-9294-9
59. Keser Z, Buchl SC, Seven NA, et al. Electroencephalogram (EEG) with or without transcranial magnetic stimulation (TMS) as biomarkers for post-stroke recovery: a narrative review. Front Neurol. 2022;13:827866. doi:10.3389/fneur.2022.827866
60. Sun RF, Li XL, Zhu ZM, et al. Effects of dual-task training in patients with post-stroke cognitive impairment: a randomized controlled trial. Front Neurol. 2022;13:1027104. doi:10.3389/fneur.2022.1027104
61. Van Ewijk PA, Schrauwen-Hinderling VB, Bekkers SCAM, Glatz JFC, Wildberger JE, Kooi ME. MRS: a noninvasive window into cardiac metabolism. NMR Biomed. 2015;28:747–766. doi:10.1002/nbm.3320
62. Pinti P, Tachtsidis I, Hamilton A, et al. The present and future use of functional near-infrared spectroscopy (fNIRS) for cognitive neuroscience. Ann NY Acad Sci. 2020;1464:5–29. doi:10.1111/nyas.13948
63. Ding X, Li CY, Wang QS, et al. Patterns in default-mode network connectivity for determining outcomes in cognitive function in acute stroke patients. Neuroscience. 2014;277:637–646. doi:10.1016/j.neuroscience.2014.07.060
64. Köhncke Y, Düzel S, Sander MC, et al. Hippocampal and parahippocampal gray matter structural integrity assessed by multimodal imaging is associated with episodic memory in old age. Cereb Cortex. 2021;31:1464–1477. doi:10.1093/cercor/bhaa287
65. Peng CY, Chen YC, Cui Y, et al. Regional coherence alterations revealed by resting-state fMRI in post-stroke patients with cognitive dysfunction. PLoS One. 2016;11:e0159574. doi:10.1371/journal.pone.0159574
66. Min Y, Liu C, Zuo LJ, Wang YJ, Li ZX. The relationship between altered degree centrality and cognitive function in mild subcortical stroke: a resting-state fMRI study. Brain Res. 2023;1798:148125. doi:10.1016/j.brainres.2022.148125
67. Ott T, Nieder A. Dopamine and cognitive control in prefrontal cortex. Trends Cognit Sci. 2019;23:213–234. doi:10.1016/j.tics.2018.12.006
68. Del Cul A, Dehaene S, Reyes P, Bravo E, Slachevsky A. Causal role of prefrontal cortex in the threshold for access to consciousness. Brain. 2009;132:2531–2540. doi:10.1093/brain/awp111
69. Zhang J, Li ZX, Cao XX, et al. Altered prefrontal-basal ganglia effective connectivity in patients with poststroke cognitive impairment. Front Neurol. 2020;11:577482. doi:10.3389/fneur.2020.577482
70. Bonilha L, Hillis AE, Hickok G, Den Ouden DB, Rorden C, Fridriksson J. Temporal lobe networks supporting the comprehension of spoken words. Brain. 2017;140:2370–2380. doi:10.1093/brain/awx169
71. Menon V. Large-scale brain networks and psychopathology: a unifying triple network model. Trends Cognit Sci. 2011;15:483–506. doi:10.1016/j.tics.2011.08.003
72. Tuladhar AM, Snaphaan L, Shumskaya E, et al. Default mode network connectivity in stroke patients. PLoS One. 2013;8:e66556. doi:10.1371/journal.pone.0066556
73. Lyu D, Pappas I, Menon DK, Stamatakis EA. A precuneal causal loop mediates external and internal information integration in the human brain. J Neurosci. 2021;41:9944–9956. doi:10.1523/JNEUROSCI.0647-21.2021
74. Long X, Huang W, Napadow V, et al. Sustained effects of acupuncture stimulation investigated with centrality mapping analysis. Front Hum Neurosci. 2016;10:510. doi:10.3389/fnhum.2016.00510
75. Sridhar S, Khamaj A, Asthana MK. Cognitive neuroscience perspective on memory: overview and summary. Front Hum Neurosci. 2023;17:1217093. doi:10.3389/fnhum.2023.1217093
76. Marek S, Dosenbach NUF. The frontoparietal network: function, electrophysiology, and importance of individual precision mapping. Dialogues Clin Neurosci. 2018;20:133–140. doi:10.31887/DCNS.2018.20.2/smarek
77. Rao B, Wang SR, Yu MH, et al. Suboptimal states and frontoparietal network-centered incomplete compensation revealed by dynamic functional network connectivity in patients with post-stroke cognitive impairment. Front Aging Neurosci. 2022;14:893297. doi:10.3389/fnagi.2022.893297
78. Hoffmann M, Rossi F, Lima LB, King C. Frontotemporal disorders: the expansive panoply of syndromes and spectrum of etiologies. Front Neurol. 2024;14:1305071. doi:10.3389/fneur.2023.1305071
79. Li J, Zhang JH, Yi T, Tang WJ, Wang SW, Dong JC. Acupuncture treatment of chronic low back pain reverses an abnormal brain default mode network in correlation with clinical pain relief. Acupunct Med. 2014;32:102–108. doi:10.1136/acupmed-2013-010423
80. Xu J, Xie HJ, Liu LY, et al. Brain mechanism of acupuncture treatment of chronic pain: an individual-level positron emission tomography study. Front Neurol. 2022;13:884770. doi:10.3389/fneur.2022.884770
81. Zhao TT, Pei LX, Ning HX, et al. Networks are associated with acupuncture treatment in patients with diarrhea-predominant irritable bowel syndrome: a resting-state imaging study. Front Hum Neurosci. 2021;15:736512. doi:10.3389/fnhum.2021.736512
82. Khan MNA, Ghafoor U, Yoo HR, Hong KS. Acupuncture enhances brain function in patients with mild cognitive impairment: evidence from a functional-near infrared spectroscopy study. Neural Regen Res. 2022;17:1850–1856. doi:10.4103/1673-5374.332150
83. Qu YZ, Peng Y, Xiong Y, Dong XH, Ma PH, Cheng SR. Acupuncture-related therapy for knee osteoarthritis: a narrative review of neuroimaging studies. J Pain Res. 2024;17:773–784. doi:10.2147/JPR.S450515
84. Lim JS, Lee JJ, Woo CW. Post-stroke cognitive impairment: pathophysiological insights into brain disconnectome from advanced. J Stroke. 2021;23:297–311. doi:10.5853/jos.2021.02376
85. Yin T, Ma PH, Tian ZL, et al. Machine learning in neuroimaging: a new approach to understand acupuncture for neuroplasticity. Neural Plast. 2020;2020:8871712. doi:10.1155/2020/8871712
86. Lu MX, Du ZM, Zhao JP, et al. Neuroimaging mechanisms of acupuncture on functional reorganization for post-stroke motor improvement: a machine learning-based functional magnetic resonance imaging study. Front Neurosci. 2023;17:1143239. doi:10.3389/fnins.2023.1143239
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
The Role of Acupuncture and Its Related Mechanism in Treating Chronic Prostatitis/Chronic Pelvic Pain Syndrome
Wang H, Zhang J, Ma D, Zhao Z
International Journal of General Medicine 2023, 16:4039-4050
Published Date: 6 September 2023
Treatment of Depression with Acupuncture Based on Pathophysiological Mechanism
Sun B, Cao X, Xin M, Guan R
International Journal of General Medicine 2024, 17:347-357
Published Date: 31 January 2024
Efficacy of Acupuncture-Related Therapy for Migraine: A Systematic Review and Network Meta-Analysis
Liu Y, Wang Y, Mi C, Wang Z, Han Y, Qi X, Ding X
Journal of Pain Research 2024, 17:1107-1132
Published Date: 15 March 2024
Mechanism of Traditional Chinese Medicine in Treating Migraine: A Comprehensive Review
Chen Q, Wang M, Fu F, Nie L, Miao Q, Zhao L, Liu L, Li B
Journal of Pain Research 2024, 17:3031-3046
Published Date: 17 September 2024