Back to Journals » Journal of Pain Research » Volume 18
Acupuncture at Sensitized Acupoints versus Sham Acupuncture for Neck-Type Cervical Spondylosis: Study Protocol for a Randomized Controlled Trial
Authors Li C, Wang J, Shao X, Wu Y ![]() , Qu X, Cai J, He L, Yu L, Xu R, Xia Y, Wang R, Zhang L, Qiu Y
, Qu X, Cai J, He L, Yu L, Xu R, Xia Y, Wang R, Zhang L, Qiu Y
Received 19 June 2025
Accepted for publication 18 November 2025
Published 23 December 2025 Volume 2025:18 Pages 6963—6976
DOI https://doi.org/10.2147/JPR.S548317
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Chaoran Li,1– 3,* Junyi Wang,2,* Xiaomei Shao,1 Yuanyuan Wu,2,3 Xinyuan Qu,2 Jin Cai,4 Lilan He,5 Liqing Yu,4 Ruocheng Xu,2 Yixiang Xia,2 Ruoyu Wang,6 Lanlan Zhang,7 Yunjing Qiu8
1Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University (Zhongshan Hospital of Zhejiang Province), Hangzhou, People’s Republic of China; 2The Third School of Clinical Medicine (School of Rehabilitation Medicine), Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 3Key Laboratory of Acupuncture and Neurology of Zhejiang Province, Department of Neurobiology and Acupuncture Research, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 4Department of Ultrasound, The Third Affiliated Hospital of Zhejiang Chinese Medical University (Zhongshan Hospital of Zhejiang Province), Hangzhou, People’s Republic of China; 5Department of Ultrasound, The Affiliated Dongguan Songshan Lake Central Hospital, Guangdong Medical University, Dongguan, People’s Republic of China; 6The First School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 7Department of nursing, Hangzhou Fuyang Sunshine Geriatric Hospital, Hangzhou, People’s Republic of China; 8School of Nursing and Midwifery, Faculty of Health, University of Technology Sydney, Sydney, Australia
*These authors contributed equally to this work
Correspondence: Xiaomei Shao, Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University (Zhongshan Hospital of Zhejiang Province), Hangzhou, People’s Republic of China, Email [email protected]
Purpose: Neck-type cervical spondylosis (NTCS) is the most common subtype of cervical spondylosis. Acupuncture is frequently employed in the clinical management of NTCS. According to the traditional Chinese medicine theory of acupoint sensitization, acupoints represent both highly sensitive reactive sites during pathological states and the principal loci for therapeutic stimulation via acupuncture. Stimulating strongly sensitive points has been shown to be effective in treating disease and may enhance clinical efficacy. This study aims to investigate the clinical effect and safety of acupuncture at sensitized acupoints (SA) in alleviating symptoms in patients with NTCS, based on the specificity of acupoint sensitization.
Patients and Methods: This is a single-center, prospective, patient- and assessor-blinded, randomized, sham-controlled trial involving patients diagnosed with NTCS. Participants will be randomly assigned in a 1:1 ratio to two groups: the SA group and sham acupuncture (SHA) group. All participants will be treated with acupuncture three times during the first week, followed by a subsequent assessment scheduled in week five. The primary outcome is the alteration in the intensity of neck pain, assessed with the visual analogue scale. Secondary outcomes include changes in the neck disability index, range of motion, the 12-item short form health survey, cervical musculoskeletal ultrasound findings, and pressure pain threshold values. The intention-to-treat analysis will be applied for statistics.
Conclusion: This trial will be the first randomized controlled trial to investigate the therapeutic efficacy and safety profile of acupuncture SA in the treatment of NTCS. It is also the first trial to combine subjective and objective outcome measures to comprehensively evaluate acupuncture’s curative effect on NTCS management. The findings may provide evidence supporting acupuncture as an effective treatment option for NTCS and offer insights into its underlying biological mechanisms.
Trial Registration: ClinicalTrials.gov (https://clinicaltrials.gov/), identifier: NCT06847945.
Keywords: acupuncture, neck-type cervical spondylosis, sensitized acupoints, study protocol, randomized controlled trial, clinical effect
Introduction
Neck-type cervical spondylosis (NTCS) is the most prevalent form of cervical spondylosis characterized by neck and shoulder pain, restricted cervical mobility, muscle stiffness, and localized tenderness.1 Radiographic imaging often reveals degenerative changes in the cervical spine.2 Although imaging findings may resemble cervical osteoarthritis, the diagnosis of NTCS is based on a comprehensive assessment of symptoms, functional impairment, and imaging, rather than solely on radiographic results. Epidemiological evidence indicates that approximately two-thirds (65.5%) of the general population may suffer from NTCS during lifetime.3 Key risk factors contributing to the onset and clinical progression of NTCS include age, prolonged sedentary work, obesity, and chronic strain.4 NTCS frequently recurs, and 60% to 70% of cases gradually progress to more severe subtypes of cervical spondylosis, such as myelopathic, radicular, or mixed types.5 Beyond its physical symptoms, NTCS can also lead to significant psychological consequences, including reduced quality of life, sleep disturbances, anxiety, and depression.4,6 It also imposes a substantial economic burden through healthcare costs and lost productivity.4
As the early stage of cervical spondylosis, NTCS represents a critical window for therapeutic intervention to prevent disease progression.1 However, no definitive treatment currently exists. Pharmacological interventions, such as nonsteroidal anti-inflammatory drugs, muscle relaxants, and antidepressants, are commonly prescribed to alleviate symptoms.4 While these agents may provide short-term relief, their potential adverse effects limit their suitability as first-line or long-term treatment options.4
Contemporary evidence has substantiated that acupuncture is the key non-pharmacological alternative therapy for NTCS management.7,8 Voluminous clinical evidences have elucidated acupuncture can effectively relieve cervical pain and function, with a favorable safety profile.9,10 Despite its proven efficacy, acupuncture outcomes may vary depending on the specific acupoints selected, as different acupoints are believed to have distinct therapeutic effects. Some research has suggested that needling myofascial trigger points yield significant analgesic effects,11 while another study reported that distal routine acupoints demonstrate superior efficacy over local trigger points in alleviating cervical pain.12 The selection of acupoints constitutes a pivotal determinant for the clinical effectiveness of acupuncture. Consequently, establishing quantifiable acupoint assessment criteria and refining precise acupoint selection method, alongside optimizing the formulation of acupuncture protocols, are essential for determining the therapeutic efficacy of acupuncture.
Acupoint sensitization is a concept rooted in classical Chinese medicine theory, particularly the principle of “Pain as Acupoints” described in the Ling Shu (Miraculous Pivot), which posits that selecting highly sensitive or tender points as acupuncture sites can yield optimal therapeutic effects. Contemporary studies have confirmed that, under pathological conditions, certain acupoints exhibit sensitization phenomena, such as tenderness, nodules, or local heat, with pressure pain sensitivity being the most common manifestation.13,14 Acupuncture targeting sensitized acupoints (SA) has been shown to enhance treatment efficacy and has been validated across various conditions, including musculoskeletal disorders, bronchial asthma, and stable angina pectoris.9,15–18 Clinical studies on neck pain have also indicated the presence of pressure-sensitive acupoints in affected patients, and acupuncture at these sites has demonstrated significant analgesic effects.9 However, no study is focusing on the clinical effect of acupuncture at quantified sensitive acupoints for treating NTCS.
Therefore, we have designed a randomized controlled trial (RCT) to evaluate the efficacy and safety of acupuncture at the strongly SA in the treatment of NTCS. The study uses the visual analogue scale (VAS) as the primary outcome measure and incorporates both objective indicators (musculoskeletal ultrasound [MSKUS] and pressure pain threshold [PPT]) and subjective indicators (neck disability index [NDI], range of motion [ROM], and 12-item short form health survey [SF-12]). This comprehensive approach is designed to assess the therapeutic outcome of acupuncture in improving cervical dysfunction, including neck pain, muscle stiffness, and mobility, as well as overall quality of life in NTCS patients. The findings are expected to provide high-quality clinical evidence to support optimized acupoint selection strategies and improve treatment outcomes in acupuncture for NTCS.
Materials and Methods
Study Design
This is a prospective, single-center, patient- and assessor-blinded, randomized, parallel-group controlled trial. The trial protocol was formulated under the guidance of internationally recognized triple standards:
- Recommendations for Interventional Trials (SPIRIT) statement for protocol design.19
- Consolidated Standards of Reporting Trials (CONSORT) for outcome reports.20
- Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines for standardized manipulation of acupuncture.21
Using the random number table, eligible NTCS patients will be assigned 1:1 to one of two treatment arms: a SA group or a sham acupuncture (SHA) group. Patients in the intervention group will receive acupuncture at SA, while those in the control group will receive SHA. All participants will receive three treatment sessions over the course of one week. The flow diagram and schedule are presented in Figure 1, and Table 1, respectively.
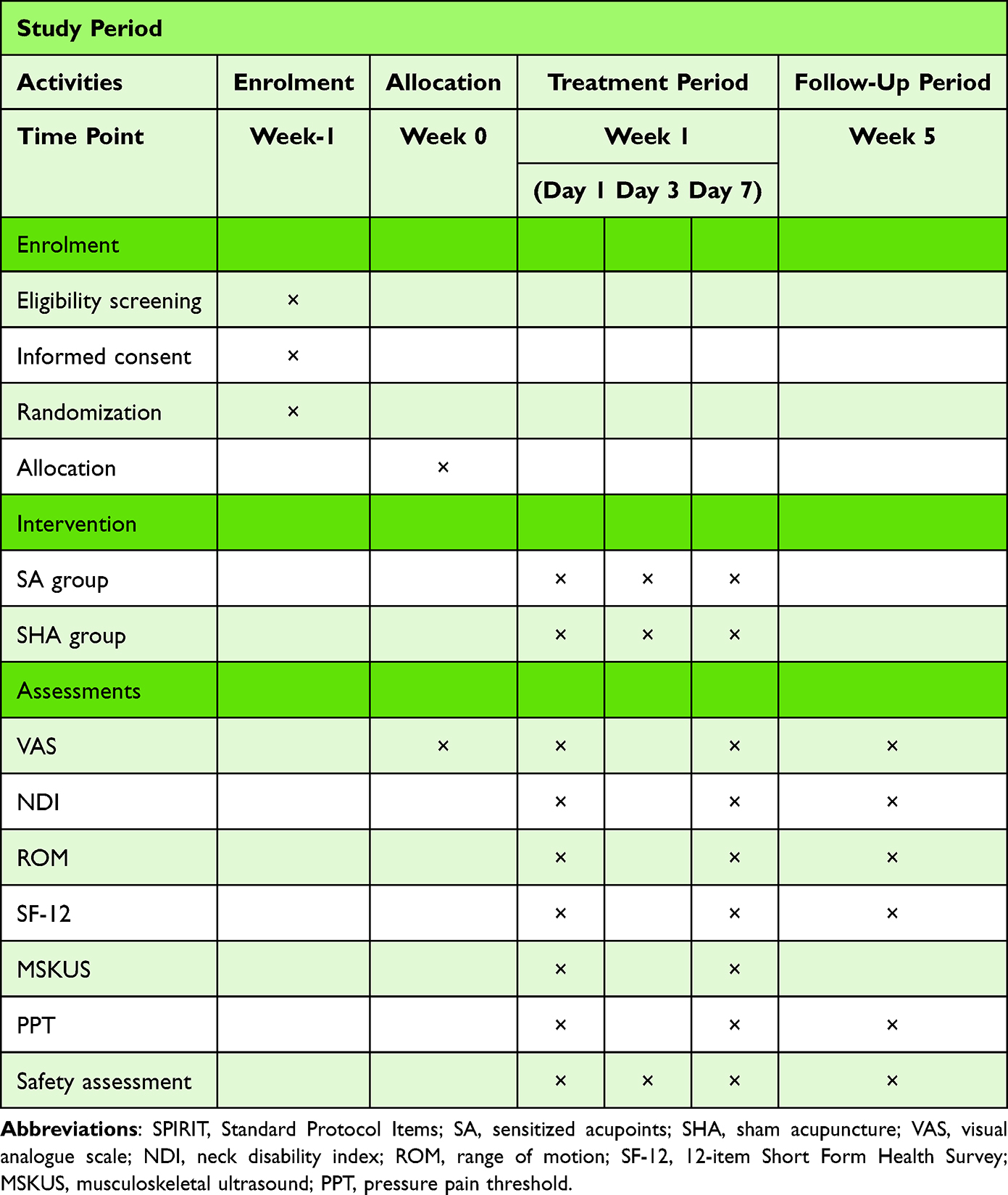 |
Table 1 The SPIRIT Schedule of Enrolment, Interventions, and Assessments |
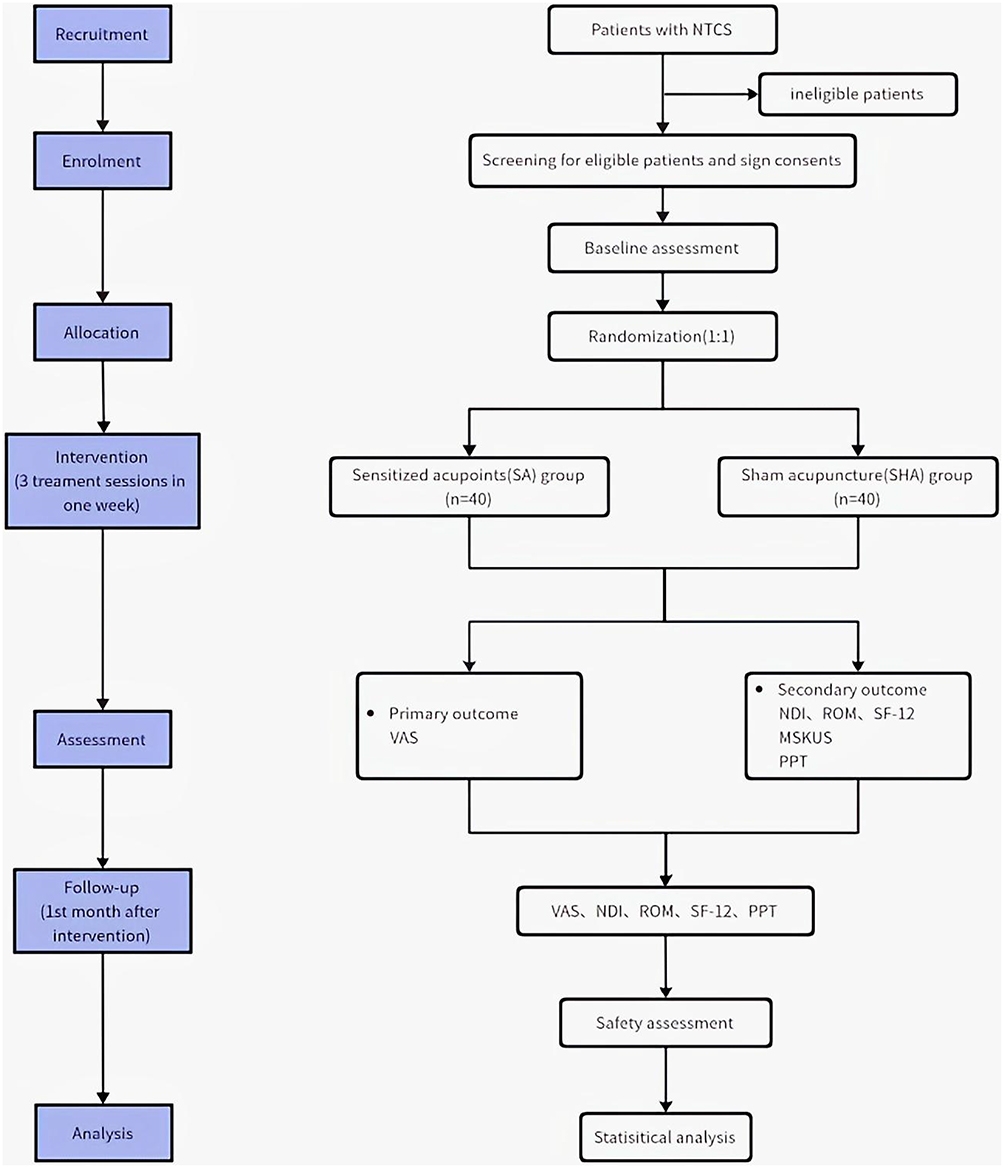 |
Figure 1 Flow diagram of the study. Abbreviations: NTCS, neck-type cervical spondylosis; VAS, visual analogue scale; NDI, neck disability index; ROM, range of motion; SF-12, 12-item Short Form Health Survey; MSKUS, musculoskeletal ultrasound; PPT, pressure pain threshold. |
The protocol received ethical approval from the Institutional Review Board of the Third Affiliated Hospital of Zhejiang Chinese Medical University on 5 February 2025 (Approval number: ZSLL-KY-2023-040-03). It has been prospectively registered with ClinicalTrials.gov on 22 February 2025 (Identifier: NCT06847945).
Recruitment
All the NTCS patients will be consecutively recruited through the acupuncture department outpatient clinic of the Third Affiliated Hospital of Zhejiang Chinese Medical University. Recruitment will be conducted through advertisements, including both online and onsite posters. Eligible patients with NTCS will be screened strictly and systematically in compliance with the diagnostic, inclusion, and exclusion criteria. Those who fulfill the eligibility verifications will be formally invited for participation, and written informed consent will be voluntarily secured prior to enrolment.
Following consent, candidates will be randomly allocated to either SA group or SHA group. This study adopts a controlled, assessor-blind design to ensure allocation concealment and minimize bias in outcome assessment.
Diagnostic Criteria
The diagnostic criteria for NTCS are based on the “Standards for Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine” and are complemented by objective imaging evidence. The diagnosis requires the following:
- Primary clinical symptoms and signs: occipital and cervical pain, restricted cervical range of motion, neck muscle stiffness, and identifiable tenderness points.
- Radiographic findings: X-ray imaging demonstrating cervical degenerative changes, including one or more of the following:
- Alteration in the physiological curvature of the cervical spine at affected segments;
- Intervertebral space narrowing;
- Osteophyte formation along the anterior or posterior margins of vertebral bodies.
Inclusion Criteria
NTCS Patients need to fulfill all the following conditions:
- Fulfill the prescribed diagnostic criteria for NTCS;
- Aged between 18 and 65 years, regardless of gender;
- Mentally alert, with good compliance and willingness to participate in the study and adhere to all experimental procedures;
- May present with or without musculoskeletal signs on physical examination (that is, restricted ROM, local tenderness);
- Present with a baseline VAS pain score greater than 3 but less than 7 (range: 0–10);
- Provide written informed consent.
Exclusion Criteria
NTCS Patients will be excluded if they fulfill any of the specified conditions:
- Failure to fulfill the predefined diagnostic or inclusion criteria for NTCS;
- Are younger than 18 or older than 65 years;
- Have received treatment for NTCS or taken related medications within two weeks prior to the start of the study;
- Are diagnosed with other types of cervical spondylosis (that is, radiculopathy, vertebral artery type, myelopathy, or sympathetic type), or have neck/shoulder pain caused by non-cervical conditions;
- Have severe comorbidities affecting the cardiovascular, cerebrovascular, hepatic, renal, gastrointestinal, or hematologic systems; or have bleeding disorders, dermatological conditions, or are pregnant or breastfeeding;
- Have a history of cervical surgery or fracture;
- Have cognitive impairment, psychiatric illness, or impaired consciousness;
- Have scars, swelling, or inflammation at the acupoint testing sites that may affect the outcome measures.
Withdrawal Criteria
NTCS Patients will be withdrawn under any of the predetermined circumstances below:
- Voluntary withdrawal of consent;
- Inability to continue treatment for any reason;
- Receipt of any treatment other than the assigned study intervention;
- Occurrence of serious adverse events(AEs) from the acupuncture, or acute onset illnesses, such as myocardial infarction or pneumonia;
- Clinical worsening of NTCS or the emergence of other types of cervical spondylosis necessitating study discontinuation, as judged by the investigator.
Randomization and Blinding
The research assistant (RA) will undertake the baseline evaluation and the trial randomization of NTCS participants. All eligible individuals will be randomized in a 1:1 ratio to two parallel intervention groups (SA group or SHA group).
Blinding will be implemented for the RA, study participants, outcome assessors and statistical analysts. Due to the nature of acupuncture interventions, double blinding is not feasible. Therefore, this study adopts a single-blinded design, whereby patients, outcome assessors and data analysts remain blind to group allocation, while acupuncturists delivering the intervention are unblinded. All acupuncture procedures will be performed by licensed acupuncturists. Outcome assessments will be collected and collated by people who are blinded to participant allocation. These assessors will receive standardized training to ensure consistency in data collection and documentation using case report forms (CRFs). All CRFs will be protected confidentially at The Third Affiliated Hospital of Zhejiang Chinese Medical University. Statistical analysis will be carried out by an independent statistician, fully blinded to the RCT allocation and intervention details to minimize bias.
Interventions
SA Group
According to systematic reviews, the Gallbladder Meridian of Foot Shaoyang is the most frequently used meridian in acupuncture treatment for NTCS, accounting for 21.9% of clinical applications.22,23 Clinically, acupuncture points along this meridian are commonly selected for the management of NTCS.24 Preliminary studies conducted by our research team have identified sensitized (that is, pressure-sensitive) points along the Gallbladder Meridian of Foot Shaoyang in NTCS patients. The six acupoints Fengchi (GB-20), Jianjing (GB-21), Yanglingquan (GB-34), Yangjiao (GB-35), Waiqiu (GB-36), and Xuanzhong (GB-39) were assessed using PPT measurements in NTCS patients and healthy controls. Acupoints with statistically significant lower PPT in NTCS patients (p<0.05) were defined as sensitized acupoints. Preliminary studies identified Yanglingquan (GB-34), Yangjiao (GB-35), Waiqiu (GB-36), and Xuanzhong (GB-39) as strongly sensitized NTCS-related acupoints. These acupoints will be identified in accordance with the China Standard for the Name and Location of Acupoints (GB/T 12346–2021). The anatomical positions of the SA are mapped in Figure 2 and are detailed depicted in Table 2.
 |
Figure 2 Location of sensitized acupoints and corresponding sham acupuncture for NTCS treatment. Notes: The four main sensitized acupoints evaluated in this study (red dots) are Yanglingquan (GB-34), Yangjiao (GB-35), Waiqiu (GB-36), and Xuanzhong (GB-39). The corresponding non-acupoint locations used in the sham acupuncture group (blue dots) are approximately 2 cm away from each respective sensitized acupoints, avoiding any known meridians. |
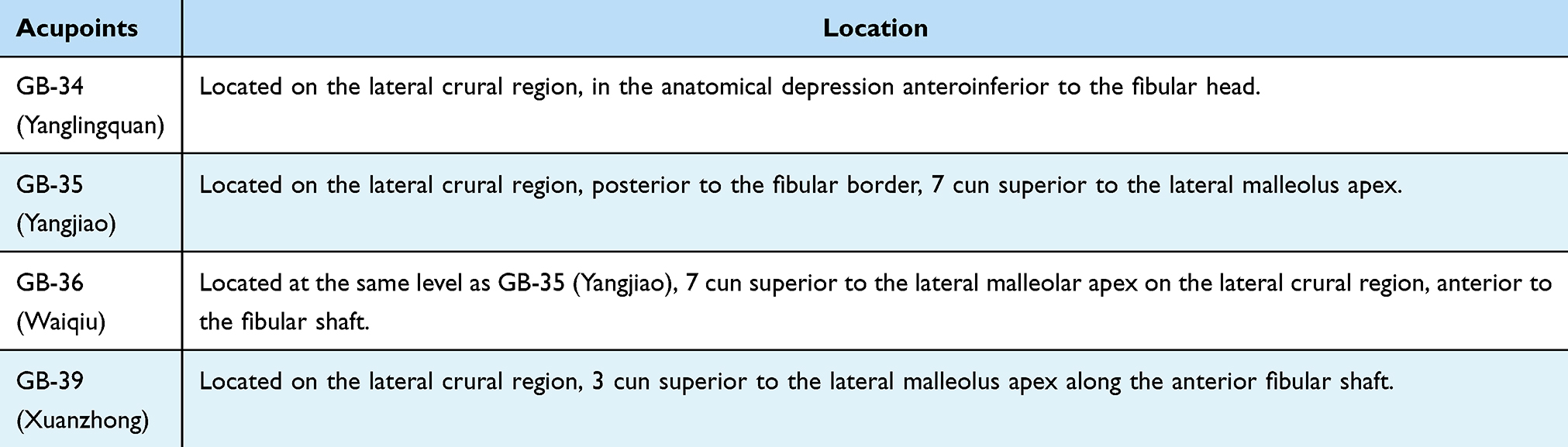 |
Table 2 Locations of Acupoints in SA Group |
A sterile, single-use stainless steel needle (Huato Medical Instruments, Huato Needles, Suzhou, China) will be utilized. Acupuncture needles (specifications: length = 40 mm, diameter = 0.25 mm) will be inserted to a depth of 15–30 mm at the selected acupoints. Manual stimulation techniques, including lifting, thrusting, twirling and rotating, will be applied to elicit the deqi sensation, which includes soreness, numbness, distention or pain paresthesias. Each acupuncture treatment session will last 30 minutes. Based on the pre-experimental results and published literature,25,26 participants in this group will undergo three therapeutic sessions within 7 days, conducted every other day.
SHA Group
A shallow needling approach at non-acupoint locations was used as the blinding method for the SHA group. This approach has been adopted in several previously published high-quality RCTs.27–29 Non-acupoints were defined as locations situated 2cun away from each corresponding SA (see Figure 2 and Table 3). Superficial needling will be performed by inserting the needle 2–3 mm into the skin without eliciting the deqi sensation or employing manipulation techniques. The same type of acupuncture needles and treatment schedule will be used for both the SHA and the SA groups.
 |
Table 3 Locations of Non-Acupoints in SHA Group |
Outcomes
Primary Outcome
Pain is one of the hallmark symptoms of NTCS, and VAS is the currently predominant clinical instrument for quantifying pain intensity due to its high specificity and sensitivity.30 The VAS has also been widely adopted in clinical studies evaluating neck pain intensity because of its straightforward design and ease of administration.31,32 Higher VAS scores indicate increasing pain severity.
Secondary Outcomes
In addition to the primary outcome, a series of secondary outcomes will be assessed to provide a comprehensive evaluation of the intervention effects in patients with NTCS. These include MSKUS measurements, PPT, NDI, cervical ROM, and SF-12.
MSKUS Assessment
Measurement of Cervical Muscle Thickness
MSKUS provides high-resolution imaging of soft tissues such as muscles, tendons, and ligaments, and is commonly used for diagnosing and monitoring musculoskeletal conditions.33,34 MSKUS allows for the visualization and quantification of muscle morphology, stiffness, and elasticity with objective and reproducible measures. It has been widely used in evaluating treatment effects in patients with cervical spondylosis.
In this study, MSKUS assessments will be performed utilizing the Mindray-Resona 6T diagnostic system equipped with a linear-array transducer (L14-5WU). Participants will be positioned prone, with their hands folded under the forehead and shoulders externally rotated to maintain a relaxed, neutral head and neck posture (see Figure 3A). The transducer will be placed longitudinally 2 cm lateral to the C4 spinous process to begin the scan (see Figure 3B). Once a stable and clear image is obtained, the ultrasound system’s built-in software will be used to measure the muscle thickness of the trapezius, splenius capitis, semispinalis capitis, semispinalis cervicis, and multifidus at the C4 transverse process level bilaterally (see Figure 3C). Each muscle will be measured three times, with the mean value recorded. Measurements will be taken first on the left side, followed by the right.
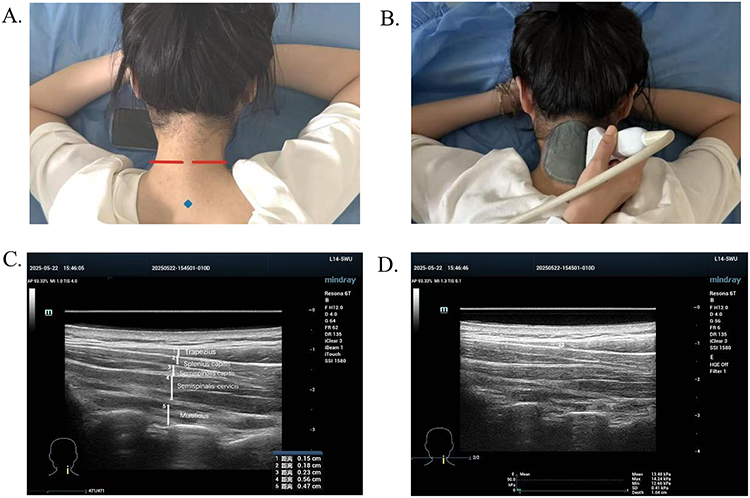 |
Figure 3 Musculoskeletal ultrasound (MSKUS) assessment of the neck. Notes: (A) Participant in prone position; C7 spinous process marked (blue dot) as reference. Scan extended cranially to ~2 cm lateral to C4 (red line); (B) Standardized placement of the MSKUS probe; (C) Representative ultrasound image showing muscle thickness of the trapezius, splenius capitis, semispinalis capitis, semispinalis cervicis, and multifidus (indicated by white vertical lines); (D) Ultrasound image demonstrating muscle elastography. |
Measurement of Cervical Muscle Elasticity
The participant will remain in the previously described position, ensuring a relaxed, neutral head and neck posture. Cervical muscle elasticity will be assessed using two ultrasound elastography techniques: strain elastography (to obtain strain ratio, SR) and shear wave elastography (to obtain Young’s modulus, E-value).
SR Value
For strain elastography, the transducer will be gently and repeatedly pressed vertically to obtain stable elastographic images lasting approximately 3–4 seconds. The reference region will be defined as the central third of the ultrasound gel pad, and the region of interest (ROI) will be placed over the target cervical muscle. The ultrasound software will automatically calculate the strain ratio (SR) between the ROI and the reference region (see Figure 3D).
E-Value
Once a stable and clear B-mode (2D) ultrasound image is obtained, the system will be switched to shear wave elastography (SWE) mode. The ROI, fixed at 3 mm × 3 mm, will be adjusted to fully encompass the muscle tissue. The Elasto imaging mode will then be activated to visualize tissue elasticity, and the system will automatically calculate the Young’s modulus (E-value) for the targeted area. Each site will be measured three times, first on the left side and then on the right, with the average value recorded.
All collected images and data will be systematically stored for analysis. During data analysis, all the results from the affected and unaffected sides will be compared.
PPT
The PPT refers to the minimum amount of pressure applied to body tissue that elicits a sensation of pain.35 In this study, the improvement in tenderness at SA will be assessed by measuring PPT. A handheld pressure algometer (Wagner Instruments, FDX25, American) will be used to evaluate changes in PPT at four sensitive points before and after treatment in both groups. The algometer probe will be placed perpendicularly at the four sensitive acupoints successively. The measurer applies gradual and stable pressure until the PPT is reached. PPT value will be recorded from the display at that moment. Each acupoint will be assessed three times, with five-minute intervals between measurements, and the mean value will be used for analysis.
NDI
The NDI is a reliable and valid self-reported instrument used to evaluate the extent of neck dysfunction. It consists of 10 items addressing various aspects of daily functioning affected by NTCS, including pain intensity, reading, and recreational activities. Higher scores indicate greater functional impairment.36 The NDI is valuable for determining the severity of cervical conditions and assessing the effectiveness of therapeutic interventions.30
Cervical ROM
Restricted cervical mobility is a common clinical feature among patients with NTCS. Changes in cervical ROM are indicative of overall cervical spine function.37 Measurements will be taken for flexion (0–45°), extension (0–45°), lateral flexion (0–45°), and rotation (0–60°). Each direction of movement will be tested three times randomly, and the average value will be recorded. This approach provides an objective reflection of the degree and extent of cervical joint dysfunction.
SF-12
Quality of life is increasingly recognized as an important outcome in patients with musculoskeletal disorders. SF-12 provides a comprehensive overview of patient’s health status, covering two main domains: physical functioning and mental well-being. It is frequently applied in studies involving individuals with cervical spine conditions.38
Safety Evaluation and AEs
All AEs occurring during the study period will be recorded and promptly evaluated. Potential events include local bleeding, bruising, pain at the needle site, or acupuncture-related fainting. Detailed documentation will include the date of occurrence, duration, severity, and any actions taken in response. Investigators will assess the relationship between AEs and the intervention. Participants experiencing AEs will receive timely and appropriate care. Serious AEs must be promptly notified to both the principal researcher and the ethics committee. Any individuals experiencing such events will be removed from the trial immediately.
Sample Size
The main outcome focuses on the variations in VAS scores from baseline to the end of treatment and follow-up. Based on existing studies and preliminary findings conducted by our research team, it is assumed that the mean VAS score at the end of treatment in the SHA group will be 4.71 with a standard deviation of 1.26. A clinically meaningful reduction of 1.5 points in the VAS score is expected in the SA group.39 Using the formula for comparing means between two-tailed independent samples, with = 0.05, and 90% power (= 0.1), the corresponding Z-values are Zα = 1.96 and Zβ = 1.28. Based on statistical analysis, 36 NTCS patients are needed in the SA or SHA group, respectively. Accounting for a 10% dropout rate,40,41 a minimum of 40 NTCS subjects will be recruited per group, resulting in the final total sample size of 80.
n=36
Statistical Analysis
An independent statistician not involved in the trial will conduct all analyses using SPSS version 25.0. Analyses will be performed based on the Full Analysis Set (FAS), Per Protocol Set (PPS), and Safety Set (SS). The FAS includes all randomized NTCS patients with available primary outcome data. The PPS is a subset of the FAS and includes patients who completed the assigned interventions. The SS includes all randomized patients who received at least one needling session and will be used for safety evaluation.
Descriptive statistics will summarize baseline characteristics. Continuous variables with normal distributions will be presented as mean ± standard deviation, while non-normally distributed variables will be reported as median (interquartile range). Categorical variables will be summarized as frequency (percentage). Between-group comparisons at baseline will use independent samples t-tests or Mann–Whitney U-tests for continuous variables and Chi-square or Fisher’s exact tests for categorical variables.
For primary and secondary continuous outcomes measured at multiple time points (baseline, week 1, week 5), Linear mixed-effects models will serve as the primary analytical method. Fixed effects will include treatment group, time, and group-by-time interaction, with a random intercept for each subject to account for within-subject correlations. This approach allows robust handling of missing data under the missing-at-random assumption. If a significant group-by-time interaction is observed, post-hoc analyses will be performed to compare groups at specific time points.
A p-value <0.05 will be considered statistically significant. The statistical analyses ensure that the effects of acupuncture at SA versus SHA on cervical symptom relief and functional recovery are evaluated accurately and rigorously.
Discussion
NTCS represents the most prevalent and earliest subtype of cervical spondylosis. It is primarily characterized by cervical discomfort and restricted mobility without the involvement of the nerve roots or spinal cord.1 NTCS is known for its high prevalence and recurrent nature.4 Early and timely intervention is critical to prevent or delay its progression to other forms of cervical spondylosis.1
This study primarily focuses on the early validation of short-term therapeutic effects. Its core objective is to establish an initial intervention protocol for treating NTCS using acupoint sensitization through acupuncture. Based on the specificity of sensitized acupoints, the study aims to propose a novel therapeutic strategy. A short treatment course is considered more conducive to capturing such “early and specific” effects. If significant intergroup differences can be observed after a short-term treatment, this would provide strong evidence supporting the specific efficacy of sensitized acupoints.
Although the clinical effect of acupuncture for NTCS has been widely acknowledged, outcome assessments have predominantly relied on subjective patient-reported measures, and robust objective clinical evidence remains limited. This study integrates both subjective and objective outcome measures to assess the therapeutic effectiveness of acupuncture for treating NTCS. In addition to four subjective scales (that is VAS, ROM, NDI, and SF-12), two objective indicators are included: PPT and MSKUS parameters (muscle thickness, SR, and E-values of the cervical muscles). This combined approach aims to provide a more rigorous and scientific basis for assessing acupuncture outcomes in NTCS.
PPT is a validated objective measure for quantifying local pain sensitivity, particularly in musculoskeletal pain disorders.35 Acupoints exhibit sensitization properties: in pathological states, the PPT of relevant acupoints typically decreases, and the degree of change reflects the intensity of sensitization.9,17,42,43 Prior studies have demonstrated that acupuncture at highly sensitized, disease-relevant acupoints can effectively relieve pain.9,44 Using PPT to identify these points, researchers have shown that targeted acupuncture reduces symptoms in patients with neck pain.9 This trial compares the PPT changes of sensitive points before and after acupuncture to further validate the clinical efficacy of this approach. Additionally, this study introduces a potential objective method for acupoint selection based on sensitization, offering insights for optimizing point selection in acupuncture therapy.
The exact pathogenesis of NTCS remains unclear, but existing evidence suggests that pathological changes in cervical muscles play a central role.1,45 Chronic muscle tension and strain in NTCS patients may lead to excessive acetylcholine release,46 reduced muscle oxygen saturation and blood flow, and poor local soft tissue perfusion.47 These changes can cause compensatory hypertrophy of cervical muscles, increased muscle tone, and imbalanced cervical biomechanics, ultimately resulting in neck pain and stiffness.48,49 MSKUS offers a non-invasive and convenient technique to objectively evaluate the morphology and function of muscle.33,34 In this study, ultrasound imaging is employed as an adjunct tool to assess the effects of acupuncture on NTCS, specifically focusing on the cervical extensor muscles to examine changes in muscle thickness and stiffness (via SR and E-values). This focus is particularly relevant as NTCS patients are often in a prolonged forward-leaning posture with sustained neck flexion.
Furthermore, the use of non-acupoints in the control group enables evaluation of the placebo effect of acupuncture and allows for participant blinding, thereby reducing potential bias in outcome assessments.
We acknowledge several limitations in this study. First, the relatively small sample size (n = 40 per group), though adequate for detecting primary outcome differences, may limit the detection of smaller yet clinically meaningful effects and reduce generalisability. Second, as a single-centre study, potential selection bias may exist, restricting external validity; future multicentre research is warranted for confirmation. Third, the short intervention (one week, three sessions) and four-week follow-up limit assessment of long-term efficacy. Extending both treatment and follow-up durations in future studies would allow evaluation of sustained effects. Fourth, blinding of acupuncturists was not feasible, which may introduce performance bias despite standardised protocols. Lastly, although sham acupuncture was used to control non-specific effects, participant expectations could still influence subjective outcomes; a waiting-list control may help address this in future trials.
Conclusion
This RCT protocol is the first clinical study designed to evaluate the efficacy and safety of acupuncture for NTCS based on the concept of acupoint sensitization. It also represents the first attempt to combine MSKUS and PPT measurements to objectively explore the underlying biological mechanisms of acupuncture in NTCS. The integration of a sham acupuncture control and both subjective and objective outcome measures ensures a robust study design aimed at providing reliable evidence for the specific therapeutic effects of acupuncture at sensitized acupoints. Although this study has certain limitations, such as a single-centre design, modest sample size, and short treatment and follow-up periods, it is expected to generate valuable preliminary evidence to optimise acupuncture protocols for NTCS. Moreover, it may lay the groundwork for future large-scale, multicentre RCTs and further research into the mechanisms of acupoint sensitization.
Abbreviations
NTCS, neck-type cervical spondylosis; SA, sensitized acupoints; SHA, sham acupuncture; VAS, visual analogue scale; NDI, neck disability index; ROM, range of motion; SF-12, the 12-item short form health survey; MSKUS, musculoskeletal ultrasound; PPT, pressure pain threshold; RCT, randomized controlled trial; SPIRIT, Standard Protocol Items: Recommendations for Interventional Trials; CONSORT, Consolidated Standards of Reporting Trials; STRICTA, Standards for Reporting Interventions in Clinical Trials of Acupuncture; AEs, adverse events; RA, research assistant; CRFs, case report forms; ROI, region-of-interest; SR, strain ratio; SWE, shear wave elastography; FAS, Full Analysis Set; PPS, Per Protocol Set; SS, Safety Set.
Data Sharing Statement
No datasets were generated or analyzed during the current study. All relevant data will be made available upon completion of the research.
Ethics Statements
This study has received ethical approval from the Institutional Review Board of the Third Affiliated Hospital of Zhejiang Chinese Medical University (Approval No. ZSLL-KY-2023-040-03). The trial will comply with the Declaration of Helsinki. The findings will be disseminated through peer-reviewed publications.
Acknowledgments
The authors sincerely thank all individuals who contributed to the development and implementation of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by the Zhejiang Provincial Health Commission, the Zhejiang Provincial Administration of Traditional Chinese Medicine(No. 2023ZL070), the Youth Fund of the National Natural Science Foundation of China (No. 82405546), the Natural Science Foundation of Zhejiang Province (No. LQ24H270009), the Zhejiang Provincial Medical and Health Science and Technology Program (No. 2024KY1235), and the Zhejiang Medical Talent “New Talent” Project (No. ytxx202401).
Disclosure
The authors declare no potential conflicts of interest.
References
1. Hongwei X, Hua Z. Advance in diagnosis and pathogenesis of neck type of cervical spondylosis. J Spinal Surg. 2021;19:136–140. doi:10.3969/j.issn.1672-2957.2021.02.013
2. Societies WFOC, Medicine LHSU, Hospital CF, et al. Expert consensus on integrated traditional Chinese and western medicine diagnosis and treatment of cervical spondylosis. World J Chin Med. 2023;18:918–922.
3. Binder AI. Cervical spondylosis and neck pain. BMJ. 2007;334:527–531. doi:10.1136/bmj.39127.608299.80
4. Kuo DT, Tadi P. Cervical spondylosis; 2025.
5. Xiao D, Chen L, Yang C, Hu B. Advances in acupuncture treatment of cervical spondylosis (neck type). Tradit Chin Med J. 2024;23:67–70. doi:10.14046/j.cnki.zyytb2002.2024.06.007
6. Kazeminasab S, Nejadghaderi SA, Amiri P, et al. Neck pain: global epidemiology, trends and risk factors. Bmc Musculoskelet Disord. 2022;23(26). doi:10.1186/s12891-021-04957-4
7. Chen J, Shao G. Acupuncture and motion therapy for cervical spondylosis of cervical type: a case report. Asian J Surg. 2024. doi:10.1016/j.asjsur.2024.08.214
8. Zhang L, Yuan G. Therapeutic effect of modified cervical jiaji acupuncture on mixed type cervical spondylosis. Am J Transl Res. 2024;16:3355–3365. doi:10.62347/OEOL5448
9. Zhao L, Sun M, Yin Z, et al. Long-term effects of individualized acupuncture for chronic neck pain: a randomized controlled trial. Ann Intern Med. 2024;177:1330–1338. doi:10.7326/M23-2425
10. Chen L, Li M, Fan L, et al. Optimized acupuncture treatment (acupuncture and intradermal needling) for cervical spondylosis-related neck pain: a multicenter randomized controlled trial. Pain. 2021;162:728–739. doi:10.1097/j.pain.0000000000002071
11. Cerezo-Téllez E, Torres-Lacomba M, Fuentes-Gallardo I, et al. Effectiveness of dry needling for chronic nonspecific neck pain: a randomized, single-blinded, clinical trial. Pain. 2016;157:1905–1917. doi:10.1097/j.pain.0000000000000591
12. Irnich D, Behrens N, Gleditsch JM, et al. Immediate effects of dry needling and acupuncture at distant points in chronic neck pain: results of a randomized, double-blind, sham-controlled crossover trial. Pain. 2002;99:83–89. doi:10.1016/s0304-3959(02)00062-3
13. Zhu B. The plasticity of acupoint. Zhongguo Zhen Jiu. 2015;35:1203–1208. doi:10.13703/j.0255-2930.2015.11.039
14. Tan H, Tumilty S, Chapple C, Liu L, Othman R, Baxter GD. Acupoints sensitization in people with and without chronic low back pain:a matched-sample cross-sectional study. J Back Musculoskelet Rehabil. 2023;36:137–146. doi:10.3233/BMR-210297
15. Tang L, Jia P, Zhao L, et al. Acupuncture treatment for knee osteoarthritis with sensitive points: protocol for a multicentre randomised controlled trial. BMJ Open. 2018;8:e23838. doi:10.1136/bmjopen-2018-023838
16. Tu J, Wang X, Yan S, et al. Thermal sensitization of acupoints in patients with knee osteoarthritis: a cross-sectional case-control study. J Integr Med. 2025;23(3):289–296. doi:10.1016/j.joim.2025.03.004
17. Huang S, Li L, Liu J, et al. The preventive value of acupoint sensitization for patients with stable angina pectoris: a randomized, double-blind, positive-controlled, multicentre trial. Evid Based Complement Alternat Med. 2021;2021(7228033):1–9. doi:10.1155/2021/7228033
18. Ouyang B, Gao J, Sun G, et al. Impact of acupoint heat-sensitive moxibustion on lung function and life quality of patients with chronic persistent bronchial asthma: a randomized controlled study. Zhongguo Zhen Jiu. 2011;31:965–970. doi:10.13703/j.0255-2930.2011.11.019
19. Chan A, Boutron I, Hopewell S, et al. Spirit 2025 statement: updated guideline for protocols of randomised trials. BMJ. 2025;389:e81477. doi:10.1136/bmj-2024-081477
20. Hopewell S, Chan A, Collins GS, et al. Consort 2025 statement: updated guideline for reporting randomised trials. Lancet. 2025;22:e1004587. doi:10.1371/journal.pmed.1004587
21. Macpherson H, Altman DG, Hammerschlag R, et al. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. Plos Med. 2010;7:e1000261. doi:10.1371/journal.pmed.1000261
22. Guo L, Zhang H, Liu Z, Yang J, Xu D, Wang Y. Systematic review of point selection strategies in acupuncture management of cervical spondylopathy. Chin J Basic Med. 2017;23:989–991. doi:10.19945/j.cnki.issn.1006-3250.2017.07.035
23. Shi Y, Huang Q, Guang Y, et al. Analysis of the clinical application rules of acupuncture in the treatment of cervical spondylosis using data mining technology. Shanghai J Acup Moxib. 2024;43:1196–1203. doi:10.13460/j.issn.1005-0957.2024.11.1196
24. Li X. Experience in treating neck stiffness and pain with acupoints of the gallbladder Meridian of foot-shaoyang. Inform Tradit Chin Med. 2002;19:51–52. doi:10.19656/j.cnki.1002-2406.2002.05.030
25. Zhang W, Fang Y, Shi M, Zhang M, Chen Y, Zhou T. Optimal acupoint and session of acupuncture for patients with chronic prostatitis/chronic pelvic pain syndrome: a meta-analysis. Transl Androl Urol. 2021;10:143–153. doi:10.21037/tau-20-913
26. Yan C, Huo J, Wang X, et al. Different degree centrality changes in the brain after acupuncture on contralateral or ipsilateral acupoint in patients with chronic shoulder pain: a resting-state fmri study. Neural Plast. 2020;2020(5701042):1–11. doi:10.1155/2020/5701042
27. Sun J, Liang Y, Luo K, et al. Efficacy of different acupuncture techniques for pain and dysfunction in patients with knee osteoarthritis: a randomized controlled trial. Pain Ther. 2025;14:737–751. doi:10.1007/s40122-025-00713-x
28. Khodaie F, Saeedi R, Soleimany G, et al. Effects of acupuncture on cognitive functions in patients with relapsing-remitting multiple sclerosis: a randomized controlled trial. Chin J Integr Med. 2025;31(10):928–936. doi:10.1007/s11655-025-3814-0
29. Fu Z, Liu C, Kim M, et al. Acupuncture improves the symptoms, serum ghrelin, and autonomic nervous system of patients with postprandial distress syndrome: a randomized controlled trial. Chin Med. 2024;19(162). doi:10.1186/s13020-024-01028-3
30. Wei H, Tian H, Wang X, Wang J. Research advances in evaluation scales for cervical spondylosis. Orthop J China. 2021;29:995–999. doi:10.3977/j.issn.1005-8478.2021.11.08
31. Gross AR, Lee H, Ezzo J, et al. Massage for neck pain. Cochrane Database Syst Rev. 2024;2:CD4871. doi:10.1002/14651858.CD004871.pub5
32. Jones LB, Jadhakhan F, Falla D. The influence of exercise on pain, disability and quality of life in office workers with chronic neck pain: a systematic review and meta-analysis. Appl Ergon. 2024;117(104216):104216. doi:10.1016/j.apergo.2023.104216
33. Gold JE, Hallman DM, Hellström F, et al. Systematic review of quantitative imaging biomarkers for neck and shoulder musculoskeletal disorders. Bmc Musculoskelet Disord. 2017;18(395). doi:10.1186/s12891-017-1694-y
34. Xie Y, Thomas L, Hug F, Johnston V, Coombes BK. Quantifying cervical and axioscapular muscle stiffness using shear wave elastography. J Electromyogr Kinesiol. 2019;48:94–102. doi:10.1016/j.jelekin.2019.06.009
35. Fischer AA. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain. 1987;30:115–126. doi:10.1016/0304-3959(87)90089-3
36. Saltychev M, Mattie R, Mccormick Z, Laimi K. Psychometric properties of the neck disability index amongst patients with chronic neck pain using item response theory. Disabil Rehabil. 2018;40:2116–2121. doi:10.1080/09638288.2017.1325945
37. Kobayashi H, Nikaido T, Watanabe K, et al. Impact of cervical micro-endoscopic laminotomy on postoperative neck pain and range of motion: a case-control study. Spine. 2025. doi:10.1097/BRS.0000000000005305
38. Radcliff K, Jalai C, Vira S, et al. Two-year results of the prospective spine treatment outcomes study: analysis of postoperative clinical outcomes between patients with and without a history of previous cervical spine surgery. World Neurosurg. 2018;109:e144–e149. doi:10.1016/j.wneu.2017.09.122
39. Laigaard J, Pedersen C, Rønsbo TN, Mathiesen O, Karlsen APH. Minimal clinically important differences in randomised clinical trials on pain management after total Hip and knee arthroplasty: a systematic review. Br J Anaesth. 2021;126:1029–1037. doi:10.1016/j.bja.2021.01.021
40. Sun M, Tao S, Geng G, et al. Identification of the optimal points for the acupuncture treatment of neck pain in China: protocol for a multicenter, matched, case-control study. BMJ Open. 2019;9:e29194. doi:10.1136/bmjopen-2019-029194
41. Zuo J, Zeng X, Ma H, et al. Musculoskeletal ultrasound assessment of the clinical efficacy of the combination of acupressure and “three methods of neck movement (tcm)” therapy in the treatment of cervical spondylosis: a study protocol for a randomized controlled trial. J Pain Res. 2024;17:3651–3665. doi:10.2147/JPR.S469511
42. Chen R, Huang X, Xie D, Li H. Discussion of novel mode of acupuncture and moxibustion based on identifying the acupoint sensitization. Zhongguo Zhen Jiu. 2022;42:665–668. doi:10.13703/j.0255-2930.20220121-k0001
43. Chen S, Miao Y, Nan Y, et al. The study of dynamic characteristic of acupoints based on the primary dysmenorrhea patients with the tenderness reflection on Diji (sp 8). Evid Based Complement Alternat Med. 2015;2015:158012. doi:10.1155/2015/158012
44. Wang X, Nie Z, Yu Q, et al. Acupuncture enhances signals at sensitized acupoints to elevate pressure pain threshold in knee osteoarthritis patients. Chin J Integr Med. 2022;28:1105–1110. doi:10.1007/s11655-022-3588-6
45. Liu Q, Yang Z, Liu Y, et al. Cervical spinal instability causes vertebral microarchitecture change and vertebral endplate lesion in rats. J Orthop Translat. 2020;24:209–217. doi:10.1016/j.jot.2019.10.005
46. Gallagher S, Schall MCJ. Musculoskeletal disorders as a fatigue failure process: evidence, implications and research needs. Ergonomics. 2017;60:255–269. doi:10.1080/00140139.2016.1208848
47. Cagnie B, Dhooge F, Van Akeleyen J, Cools A, Cambier D, Danneels L. Changes in microcirculation of the trapezius muscle during a prolonged computer task. Eur J Appl Physiol. 2012;112:3305–3312. doi:10.1007/s00421-012-2322-z
48. Reddy RS, Tedla JS, Alshahrani MS, Asiri F, Kakaraparthi VN. Comparison and correlation of cervical proprioception and muscle endurance in general joint hypermobility participants with and without non-specific neck pain-a cross-sectional study. PeerJ. 2022;10:e13097. doi:10.7717/peerj.13097
49. Wang DM, Li C, Hatchard N, Chang Chien GC, Alm J. Lower trapezius muscle function in people with and without shoulder and neck pain: a systematic review. J Osteopath Med. 2023;123:73–89. doi:10.1515/jom-2022-0056
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
Evaluating the Efficacy and Underlying Mechanisms of Acupuncture for Chronic Subjective Tinnitus Using Functional Near-Infrared Spectroscopy: Study Protocol for a Randomized Controlled Trial
Hu H, Lin X, Fang L, Li Y, Gao H
Journal of Pain Research 2023, 16:3367-3378
Published Date: 4 October 2023
A Pilot Study for Effectiveness and Safety of Adjunctive Pharmacopuncture to Acupuncture Treatment for Rotator Cuff Diseases: A Pragmatic Randomized Controlled Trial
Cha HJ, Han CH, Jeon JH, Jeong JK, Jung IC, Yang C, Kang BK, Kim MJ, Choi YE, Kim YI
Journal of Pain Research 2024, 17:2203-2221
Published Date: 24 June 2024
Electro-Acupuncture for Diminished Ovarian Reserve: Protocol for a Randomized, Placebo-Controlled Trial
Tang H, Wang JX, Zheng SZ, Jia YF, Yu X, Zhao NN, Yang YH, Lin LP, Li SY, Zhao H
Journal of Multidisciplinary Healthcare 2025, 18:4341-4352
Published Date: 30 July 2025
Clinical Efficacy of Acupuncture as Adjunctive Therapy for Cough Variant Asthma: Study Protocol for a Pilot Randomized Controlled Trial
Chen X, Liu Y, Li H, Deng X, Li J, Zhang H, Liang F, Xu G
Journal of Asthma and Allergy 2026, 19:586197
Published Date: 25 February 2026