Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Electro-Acupuncture for Diminished Ovarian Reserve: Protocol for a Randomized, Placebo-Controlled Trial
Authors Tang H, Wang JX, Zheng SZ, Jia YF, Yu X, Zhao NN, Yang YH, Lin LP ![]() , Li SY, Zhao H
, Li SY, Zhao H
Received 21 March 2025
Accepted for publication 18 July 2025
Published 30 July 2025 Volume 2025:18 Pages 4341—4352
DOI https://doi.org/10.2147/JMDH.S529775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Han Tang,1,2 Jia-Xuan Wang,1 Shi-Zhong Zheng,1 Yan-Fei Jia,1 Xin Yu,1 Na-Na Zhao,1 Yun-Hong Yang,1,2 Lv-Ping Lin,1,2 Si-Yuan Li,2 Hong Zhao1,2
1Department of Acupuncture, Shenzhen Hospital of Shanghai University of Traditional Chinese Medicine, Shenzhen, Guangdong, People’s Republic of China; 2Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: Hong Zhao, Email [email protected]
Introduction: Diminished ovarian reserve (DOR) is characterized by a reduced response to ovarian stimulation and a decline in fertility potential among women of reproductive age. Although previous research has suggested potential benefits of acupuncture for DOR, the evidence remains inconclusive. This study evaluates the effectiveness of electro-acupuncture in patients with DOR by examining changes in ovarian reserve indicators and reproductive outcomes. The study aims to determine whether electro-acupuncture significantly improves ovarian reserve markers and reproductive outcomes in women with DOR, thereby informing clinical decision-making.
Methods and Analysis: A randomized, subject- and assessor-blinded, placebo-controlled trial will be conducted in two hospitals in Shenzhen, China. A total of 112 participants (20– 48 yr) will be allocated to either the electro-acupuncture (EA) group or the sham electro-acupuncture (SA) group in a 1:1 ratio. Each participant will receive 3 treatment sessions per week over a continuous period of 12 weeks. The primary outcome is the change in antral follicle count, with an anticipated mean increase of approximately 2.2 follicles based on previous meta-analytic findings. Secondary outcomes will include changes in serum basal hormone levels, serum anti-Müllerian hormone levels, and self-rating anxiety, depression, and Kupperman Index scores compared to baseline. Subgroup analyses will explore variations in pregnancy outcomes (eg, clinical pregnancy rate, live birth rate), age groups (≤ 32, 32– 40, ≥ 40 years), and ovulation induction outcomes (eg, number of oocytes retrieved, MII oocyte rate). Adverse events will be recorded following each session of treatment, and a blinded evaluation is conducted upon the completion of the treatment. Study results will be primarily analyzed using the full analysis set, supplemented by the per-protocol set.
Ethics and Dissemination: This protocol have been approved by the Ethics Committee of Shenzhen Hospital of Shanghai University of Traditional Chinese Medicine (No.2023-LHQZYYYXLL-KY-147) and Luohu People’s Hospital (No.2024-LHQRMYY-KYLL-009). The results will be disseminated to participants, the public, and other relevant groups through open-access journals and conferences.
Trial Registration Number: ISRCTN:69623204. Registered on 10 January 2024.
Keywords: acupuncture, diminished ovarian reserve, study protocol, randomized controlled trial
Introduction
Diminished ovarian reserve (DOR) is defined as a condition in which women of reproductive age with regular menstrual cycles exhibit a reduced response to ovarian stimulation or a decreased ability to conceive compared to peers.1 The etiology of DOR is multifactorial, with primary associations found with aging,2 psychological factors3 and autoimmune diseases, among others.4 The incidence of infertility attributed to DOR is increasing. Data from the American Society for Assisted Reproductive Technology revealed that the prevalence of DOR among the assisted reproductive population rose from 19% in 2004 to 26% in 2011.5 By 2021, infertility affected 19% of the American population, with 26.9% of these cases using assisted reproductive technology (ART) due to DOR, highlighting a concerning upward trend in reproductive health.6 The most common symptoms of DOR are menstrual irregularities (amenorrhea or oligomenorrhea), reduced estrogen levels, and infertility. Severe consequences encompass heightened risks of cardiovascular diseases,7 osteoporosis,8 and diabetes,9 due to the lack of estrogen’s protective role. Although hormone replacement therapy (HRT) can mitigate symptoms of estrogen deficiency, the side effects of hormonal treatments remain contentious,10 with potential risks of stroke11 and venous thromboembolism.12 ART is a crucial intervention for DOR patients with fertility needs, yet clinical pregnancy and live birth rates remain low.13 Patients with DOR exhibit a weaker ovarian response and lower pregnancy rates compared to those with normal ovarian reserve, indicating a reduced likelihood of conception.14 Given the adverse effects of HRT and the desire to increase pregnancy odds, more DOR patients are exploring alternatives like acupuncture, noted for its safety and non-pharmacological benefits.
The Chinese Consensus of Clinical Diagnosis and Treatment recommends acupuncture as a treatment option for DOR.15 Recent meta-analyses indicated that acupuncture can decrease follicle-stimulating hormone (FSH) levels (SMD = −1.07, 95% CI [−1.79, −0.36], p = 0.003) and increase antral follicle count (AFC) (MD = 1.87, 95% CI [0.96, 2.79], p < 0.0001), though with considerable heterogeneity.16 Unlike HRT, which passively supplements exogenous hormones and suppresses the hypothalamic-pituitary-ovarian (H-P-O) axis,17 acupuncture has been shown to promote endogenous ovarian recovery through multi-system regulation. Specifically, studies suggest that acupuncture regulates folliculogenesis, reduces oxidative stress and inflammation, and enhances cellular resilience by modulating apoptotic and autophagic pathways.18 These effects are associated with improved follicular recruitment, increased numbers of high-quality oocytes and embryos, enhanced fertilization and retrieval rates, and reduced cycle cancellation and implantation failure.19 In addition, acupuncture may offer psychological benefits by reducing stress and anxiety, further reinforcing its appeal among DOR patients.20 However, many of these studies are limited by methodological flaws, including inadequate statistical power, lack of sham controls or blinding, inconsistent outcome measures, and reliance on subjective or short-term endpoints. Despite its widespread clinical use in China, acupuncture still faces limited international acceptance due to regional differences in medical paradigms and a shortage of high-quality randomized controlled trials conducted under rigorous biomedical standards. Therefore, methodologically sound studies are needed to generate cross-cultural evidence and promote broader global recognition of acupuncture-based interventions in reproductive medicine. To bridge this evidence gap and enhance global understanding of acupuncture’s therapeutic value in DOR, we have applied our clinical experience with electro-acupuncture in the design of a robust randomized controlled trial. The study features a sham acupuncture control using non-meridian, non-acupoint stimulation to minimize placebo effects. Objective and clinically validated biomarkers (eg, anti-Müllerian hormone, FSH, and AFC) are employed as primary outcomes to rigorously assess changes in ovarian reserve. Recognizing that prior studies in this field have often been limited by inadequate statistical power, we conducted a formal sample size calculation based on the expected change in AFC, drawing from a published systematic review. The calculation applies conservative variance estimates and a one-sided test under a superiority framework. A total of 112 participants will be enrolled to achieve 80% statistical power with a type I error rate of 2.5%, accounting for an anticipated dropout rate of up to 20%. Through this well-controlled design, standardized outcome measures, and rigorous statistical methodology, this trial aims to provide high-quality evidence supporting the integration of traditional therapies into modern reproductive care and contribute meaningfully to the field of evidence-based integrative medicine.
Methods and Analysis
Study Design
This is a randomized, subject-and assessor-blinded, placebo-controlled trial, and will conduct at Shenzhen Hospital of Shanghai University of Traditional Chinese Medicine and Luohu People’s Hospital, Shenzhen, China., from January 2024 to October 2026. A total of 112 participants will be randomly assigned to 2 groups according to a ratio of 1:1. The report of trial protocol is based on the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 Checklist21 (see Supplemental File 1). The trial has been approved by the ethics committees of Shenzhen Hospital of Shanghai University of Traditional Chinese Medicine (No. 2023-LHQZYYYXLL-KY-147) and Luohu People’s Hospital (No. 2024-LHQRMYY-KYLL-009), and is registered on ISRCTN (No. 69623204). The trial flowchart is shown in Figure S1. The schedule for enrollment, interventions and assessments are presented in Table 1.
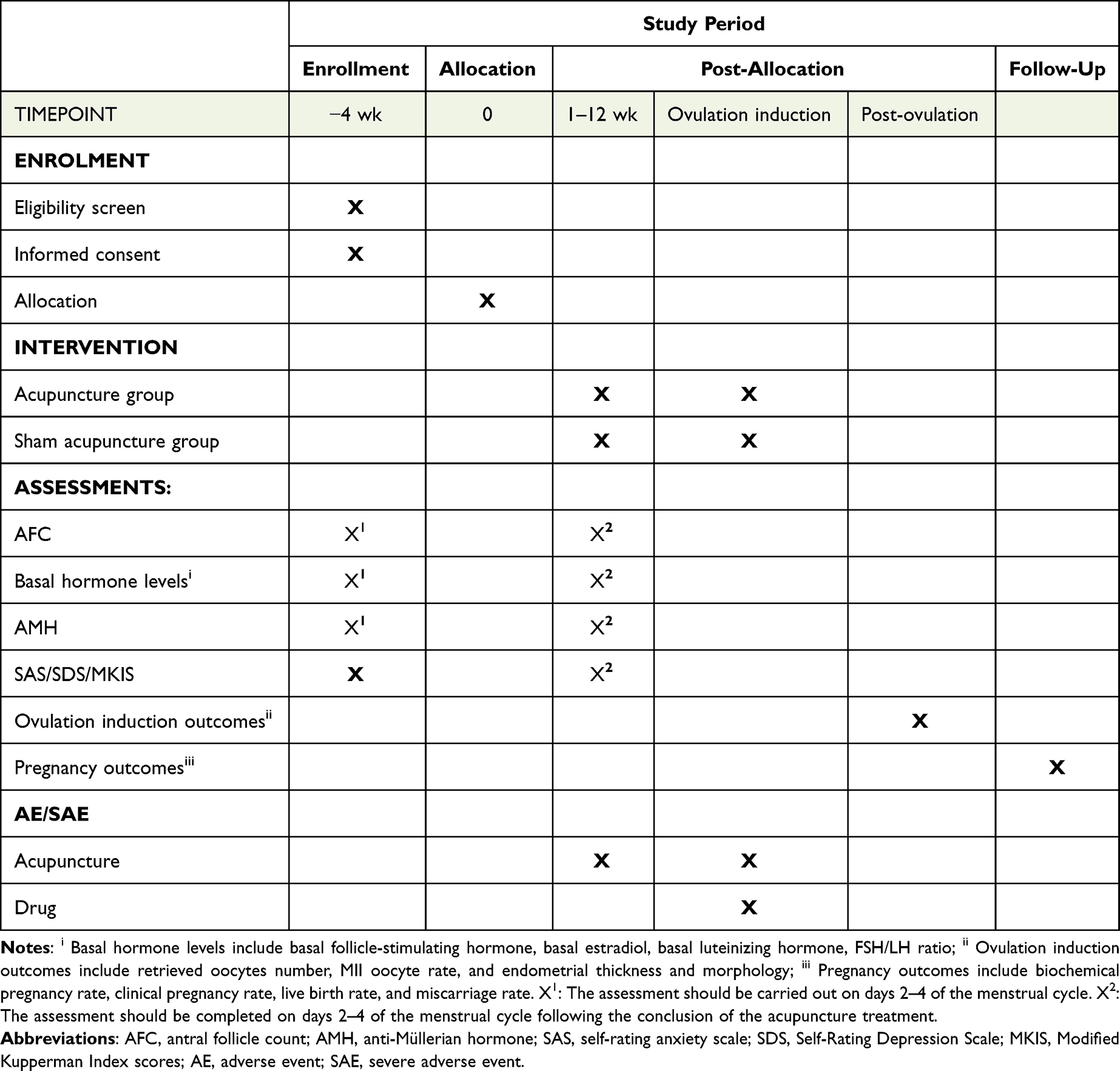 |
Table 1 SPIRIT Figure of Schedule of Enrolment, Interventions, and Assessments |
Participants Recruitment
Participants will be recruited through online recruitment advertisements and posters of these two hospitals. Research assistants are responsible for screening potential eligible participants. Before allocation, participants will be informed about the content of the research as well as their related rights and obligations, and they will complete demographic characteristic collection, medical history surveys, and laboratory examinations. Each participant voluntarily attends the trial and a written informed consent form will be required before enrollment.
Diagnosis Criteria
The diagnosis of DOR is established according to the 2011 European Society of Human Reproduction and Embryology (ESHRE) guidelines:22 1) serum basal FSH ≥ 10IU/L; 2) serum anti-Müllerian hormone (AMH) < 1.1ng/mL; 3) the total number of AFC < 7 (measuring 2~10mm in diameter in both ovaries); a diagnosis of DOR can be made if any two of the three criteria are met.
Inclusion Criteria
Participants will be deemed eligible for inclusion if they meet all of the following criteria:
- Women aged 20 to 48 years.
- Conforming to the clinical diagnostic criteria for DOR.
- Voluntary and written informed consent.
Exclusion Criteria
Participants will be excluded if they meet any of the following criteria:
- Endocrine disorders such as hyperprolactinemia, hyperandrogenemia, chronic adrenal insufficiency, and severe thyroid dysfunction.
- Reproductive system anomalies such as severe hydrosalpinx, significant tubal or pelvic adhesions, and myomas invading the endometrium, which adversely affect the outcome of pregnancies.
- Immune system disorders such as immune nephritis and systemic lupus erythematosus, which may lead to infertility.
- Contraindications to pregnancy or uterine non-viability for gestation.
- Infertility attributable to congenital malformations of the reproductive system, chromosomal anomalies, or other genetic etiologies.
- Severe comorbidities include serious cardiovascular, hepatic, renal, hematopoietic system diseases, malignancies, and mental health disorders.
- Received DOR-related interventions within 3 months.
- Deemed unsuitable for participation in the trial by the researcher.
Randomization and Blinding
Following confirmation of eligibility, participants are randomly assigned to either the electro-acupuncture or sham electro-acupuncture group in a 1:1 ratio, using a random allocation sequence generated by version 25.0 of the Statistical Package for the Social Sciences (SPSS, Inc., Chicago, United States). The concealment of the random sequence uses sequentially numbered, opaque, and sealed envelopes.
Randomization and group assignment are managed by research assistants who are not involved in the treatment or evaluation. Acupuncturists, informed about group allocations, facilitate the implementation of distinct intervention strategies but are excluded from the randomization and data analysis. Participants, outcome assessors, and statisticians will be blinded to treatment assignment until the conclusion of the trial. To preserve the integrity of blinding among participants, each subject will be individually visited and be treated in separate, curtain-partitioned rooms. Within 5 minutes following the final acupuncture intervention session in the 12th week, a brief blinded assessment survey will be conducted to ascertain the efficacy of the blinding procedure.
Procedure for Unblinding if Needed
If a participant’s condition deteriorates and the research team determines that continuing the blinding may endanger their safety, the blinding can be lifted. Our Emergency Response Plan (see Supplemental File 2) outlines the definition of serious adverse events (SAEs). In cases of emergencies, such as SAEs or unexpected serious adverse reactions, particularly those that are life-threatening or require hospitalization, unblinding is permitted to protect the participant.
Intervention Description
Permitted and Prohibited Concomitant Treatments
During the 12-week acupuncture intervention period specified by this study, participants are generally not permitted to use medications or other therapies related to DOR. Initiating ART during the intervention period is discouraged, however, participants have the right to terminate the trial at any time to start a cycle. Subsequent to the 12-week acupuncture intervention, the reproductive medicine center will determine the appropriate protocol for initiating ovulation induction and cycles. Any medications used or the initiation of a cycle during the trial must be documented in the case report forms (CRFs).
Acupuncture Intervention
The acupuncture intervention scheme and the selection of acupoints in this trial were strategically chosen based on our previous clinical experience in treating DOR. Acupuncture treatments are administered by licensed acupuncture practitioners (JXW, SZZ, YFJ), who have at least 2 years of clinical experience in acupuncture. The procedure utilizes sterile, disposable acupuncture needles (0.30mm × 25mm, 0.30mm × 40mm, and 0.35mm × 75mm) produced by SuZhou Acupuncture & Moxibustion Appliance Co., Ltd., brand Hua Tuo. The electro-acupuncture device used in this study is the KWD-808I Pulse Acupuncture Machine, manufactured by Changzhou Yingdi Electronic Medical Equipment Co., Ltd.
Acupuncture treatments will be conducted for a continuous 12 weeks, with 3 sessions per week. This study consists of a 4-week baseline period, a 12-week treatment period, and follows up with patients who are planning to conceive until the end of pregnancy, with a maximum follow-up duration of 12 months after the treatment concludes (see Figure S2).
Electro-Acupuncture (EA)
The acupoints in the EA group will include as follows: Liangmen (ST 21), Huangshu (KI 16), Guanyuan (CV 4), Zhongji (CV 3), Zigong (EX-CA 1), Zusanli (ST 36), Sanyinjiao (SP 6), Baihui (GV 20) and Shenting (GV 24). The location of acupoints are referenced to the WHO Standard Acupuncture Point Locations in the Western Pacific Region23 and EX-CA 1 referenced to the 2021 National Standard of the People’s Republic of China (GB/T40997—2021), as detailed in Table 2 and Figure S3. The patient lies in a supine position, and after routine disinfection of the skin at the acupoint area, acupuncture is performed using needles of appropriate length (see Table 2). Acupuncture is performed by experienced practitioners using a balanced reinforcement and reduction technique. When the de qi sensation occurs, patients may experience feelings such as soreness, numbness, or swelling. From the practitioner’s perspective, de qi is often described as a sensation similar to a fish biting on a line. After achieving the sensation of de qi with the needle insertion, connect the two pairs of electrodes to the same side acupoints (EX-CA 1, KI 16). The electro-acupuncture parameters are set as follows: continuous wave, frequency of 2–6 Hz, intensity of 2–8 mA, with the patient’s abdominal muscles showing slight tremors and the intensity being tolerable for the patient. The duration of needle retention is 30 minutes.
 |
Table 2 Locations and Manipulations of Electro-Acupuncture Group Acupoints |
Sham Electro-Acupuncture (SA)
Participants in the SA group will undergo superficial needling at non-meridian, non-acupoint sites approximately one B-cun lateral to the real acupoints employed in the EA group, as shown in Table 2 and Figure S4. The needles are inserted to a depth of 1 to 2 mm without employing any lifting, thrusting, twisting, or rotating movements to avoid inducing the de qi sensation. Electrodes are attached to the non-meridian, non-acupoint sites corresponding to EX-CA 1 and KI 16. The electro-acupuncture device settings are as follows: a continuous wave at a frequency of 0.1 Hz and an intensity between 0.1 and 0.5 mA. The duration of needle retention is 30 minutes, with the device being deactivated 30 seconds after activation.
Outcomes
Primary Outcome
Compared to baseline, the change in antral follicle count of bilateral ovarian diameters measuring 2–10 mm is observed via ultrasound after 12 weeks of treatment.
Secondary Outcomes
- Basal hormone levels (follicle-stimulating hormone, estradiol, luteinizing hormone, FSH/LH ratio) measured using blood samples at baseline and after 12 weeks of treatment.
- Anti-Müllerian hormone measured using blood samples at baseline and after 12 weeks of treatment.
- Anxiety, depression, and menopause symptoms measured using the Self-Rating Anxiety Scale (SAS), Self-Rating Depression Scale (SDS), and Modified Kupperman Index scores at baseline and after 12 weeks of treatment.
- Endometrial thickness and morphology measured using ultrasound on the day of embryo transfer.
- The number of retrieved oocytes and MII oocyte rate measured using data collection within 1 to 7 days for patients undergoing ovulation induction cycles.
- Pregnancy outcomes (biochemical pregnancy rate, clinical pregnancy rate, live birth rate, and miscarriage rate) are assessed using data collection about on-site visits, telephone calls, and WeChat communications up to 12 months after treatment for patients planning pregnancy.
Adverse Event Reporting and Harms
We have set up Emergency Response Plan for adverse events (AEs) and SAEs. Acupuncture-related AEs including broken needles, fainting needles, unbearable acupuncture pain (visual analogue score ≥ 8), local hematoma, infection or abscess, and other discomforts after acupuncture (eg, fatigue, palpitations, dizziness, headache, insomnia). Drug-related AEs including ovarian hyperstimulation syndrome, gastrointestinal reactions (eg, nausea, diarrhea), dizziness, headache, and abnormal liver or kidney function. SAEs including those threatening the life of the patient, causing persistent or significant functional loss or disability, or other serious medical events. To ensure comprehensive monitoring of potential AEs during the intervention, patients will complete a “Per-Session Treatment and Adverse Event Record” (see Table 3) after each electro-acupuncture session. This form will document the treatment date and any AE that may have occurred. Both the patient and the acupuncturist will review and sign the form to confirm the accuracy of the information. Detailed records of the time of occurrence, duration, and severity of these events will be kept, assessing their potential relation to the acupuncture treatment of this study. Treatment will be paused and follow-up will continue until the adverse reaction resolves. Any SAE related to the study will be reported to the Ethics Committee of Shenzhen Hospital of Shanghai University of Traditional Chinese Medicine within 24 hours.
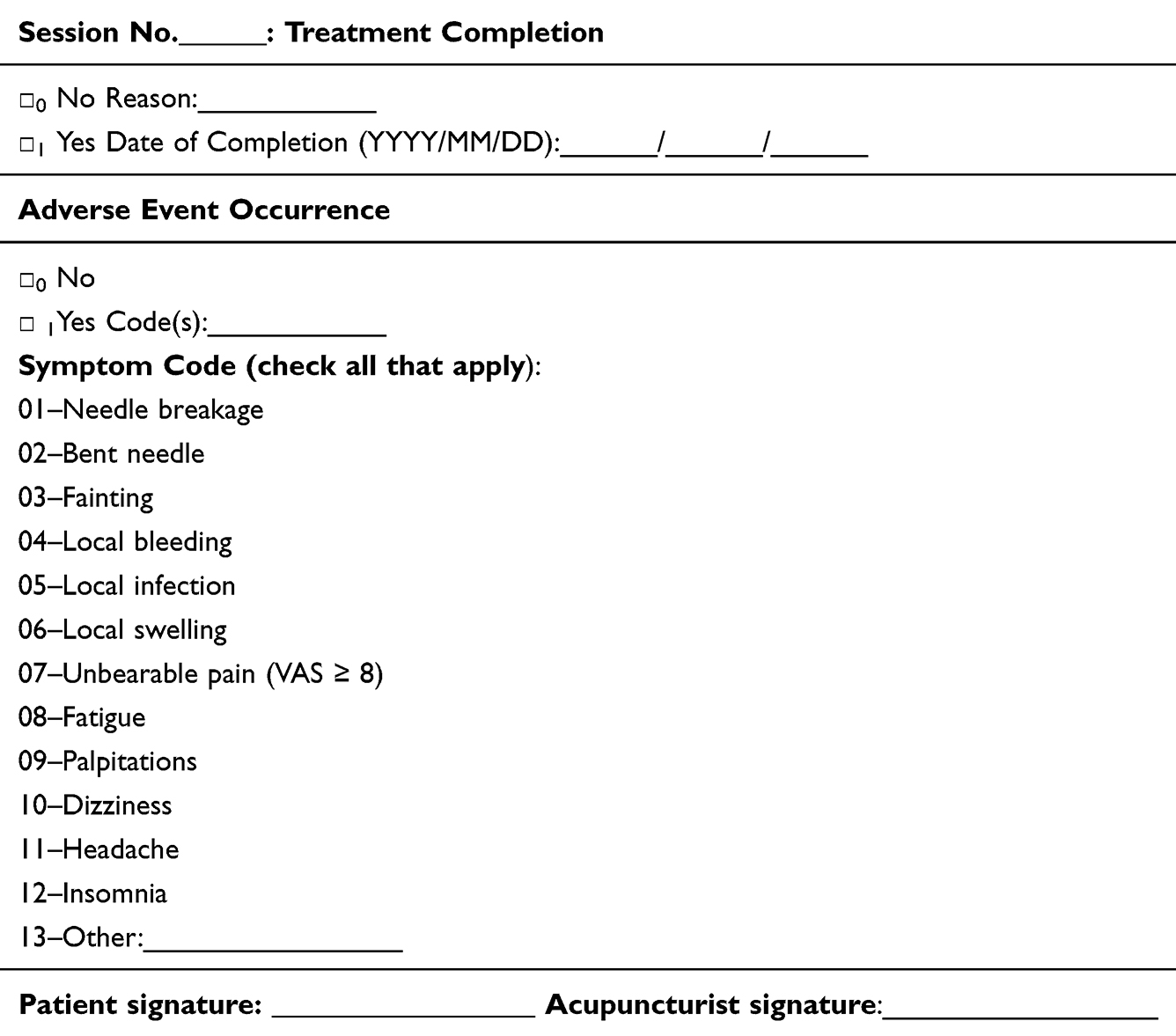 |
Table 3 Per-Session Treatment and Adverse Event Record |
Sample Size
The primary endpoint of this study is the change in AFC from baseline to 12 weeks post-treatment. The sample size calculation is based on the primary outcome. According to a systematic review,16 the expected difference in AFC between acupuncture and control groups is approximately 2.2, with the control group having a standard deviation of about 2, and a set margin of Δ = 1. Given this evidence base and the directional hypothesis that electro-acupuncture is superior to sham acupuncture in improving ovarian reserve, the study is designed as a superiority trial, and a one-sided test was used for the sample size calculation. Assuming equal standard deviations across groups and using a one-sided test with α = 0.025 and β = 0.20 (power = 80%), participants will be randomly assigned to the EA or SA group in a 1:1 ratio. Using the Power Analysis and Sample Size (PASS, NCSS, Kaysville, Utah, USA) version 15 software for calculations, the required sample size is 90 participants. Allowing for a dropout rate of up to 20%, the final sample size was set at 112 participants (56 per group).
Statistical Analysis
Data analysis will be based on the full analysis set (FAS), which operates under the intention-to-treat (ITT) principle, aiming to exclude as few participants as reasonably possible. Those who have been allocated and have received at least one intervention are included in the FAS, with missing data imputed using the last-observation-carried-forward (LOCF) method. Sensitivity analyses will be performed using multiple imputation techniques to assess the robustness of the outcome results under different missing data assumptions. All participants who have received at least one treatment post-allocation will be included in the Safety Set (SS) for the analysis of safety data.
Statistical analyses will be performed using SPSS software (version 25.0; IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test will be utilized for normality testing, and Levene’s test for homogeneity of variances. If the data meet the assumptions of normality and homogeneity, independent samples t-tests will be used for between-group comparisons, and paired t-tests for within-group comparisons. If these assumptions are violated, non-parametric alternatives will be applied: the Mann–Whitney U-test for between-group comparisons and the Wilcoxon signed-rank test for within-group comparisons. The Pearson Chi-square test or Fisher’s exact test will be applied to categorical data. All statistical tests will be one-sided (α = 0.025), with a test power of 80%, and a P-value of less than 0.05 will be considered statistically significant.
Subgroup analyses will be conducted based on the method of conception (ie, natural conception, ovulation induction, or assisted reproduction), patient age (ie, stratified into ≤32 years, 32–40 years, and ≥40 years), and ovulation induction outcomes (eg, number of oocytes retrieved and MII oocyte rate). Stratified analyses will be conducted to examine differences in treatment effects across predefined subgroups. To formally evaluate the potential effect modification, interaction terms (eg, treatment × age group, treatment × conception method) will be incorporated into multivariable regression models, where appropriate. These models will also adjust for relevant baseline covariates, including patient age, infertility duration, and male factor infertility, to account for potential confounding and enhance the validity and interpretability of the estimated treatment effects.
Data Collection and Management
Trained research assistants will be tasked with collecting data and entering the data into CRFs. Before CRFs are submitted to the data analysts, data monitoring staff will verify their authenticity and reliability. The same data will be independently entered into SPSS software version 25.0 by two trained data entry personnel, with any inconsistencies being reconciled against the original CRFs. For any issues related to the data, research assistants will conduct thorough checks and provide responses. All dropout cases will be tracked from their most recent assessment, with detailed documentation of the reasons and timing of dropout in the CRFs.
Monitoring and Quality Control
A comprehensive quality control framework was implemented to ensure data integrity and consistency throughout the trial. Prior to trial initiation, all study personnel—including recruiters, acupuncturists, outcome assessors, and data collectors—participated in a centralized training session led by the principal investigator. This training covered the entire trial protocol, standard operating procedures, outcome definitions, CRF completion guidelines, and standardized acupuncture techniques.
To ensure treatment consistency, all acupuncturists were required to have a minimum of two years of clinical experience, thereby reducing variability stemming from differences in practitioner proficiency. After the initial training, a senior acupuncturist with over 20 years of reproductive acupuncture experience conducted a standardized skills assessment of all three practitioners. During the trial, the senior acupuncturist and the trial coordinator supervise treatments regularly to ensure continued protocol adherence and consistency in needling techniques. Deviations from protocol, if any, are recorded and reviewed in investigator meetings.
During the treatment period, all patients are prohibited from receiving any other treatments or medications that could affect the disease, to prevent any interference with the accuracy of the study results. The consistency of clinical research operations is ensured by assigning specific individuals to perform acupuncture. Detailed records are maintained for participants who drop out, including the reasons and the timing of their departure.
To minimize inter-individual and inter-institutional variation and uphold the scientific integrity of the data collection process, all laboratory and ultrasound assessments are scheduled within specific time windows to account for the menstrual cycle-dependent variability in ovarian reserve biomarkers, such as follicle count and sex hormone levels. For participants with regular menstrual cycles, testing is scheduled between days 2 and 4 of menstruation. For those with irregular cycles or amenorrhea, assessments are performed during the early follicular-like phase (defined as no follicles >10 mm), between 8:00 a.m. and 12:00 p.m. To ensure standardization while maintaining assessor blinding, all ultrasound and laboratory assessments are conducted by qualified technicians in tertiary-grade A hospitals. All personnel are professionally trained and operate under consistent clinical protocols.
Data collection is managed by designated personnel to ensure uniformity in the timing, method, and standards. Additional staff are assigned to verify the authenticity of the data, and specialized personnel rigorously evaluate and process the data according to statistical principles, ensuring the scientific integrity and reliability of the study.
Discussion
The primary challenge in treating DOR is the limited effectiveness of available therapies, further complicated by significant individual variability in patient response. Although pharmacological interventions are commonly used to improve menstrual health and ART cycle outcomes, their efficacy remains suboptimal.24 Patients with DOR often experience lower clinical pregnancy and live birth rates, requiring multiple treatment cycles. Many may also seek complementary and alternative fertility treatments to achieve conception, leading to increased financial burdens and emotional stress.25
Acupuncture treatment for menstrual diseases and infertility has been documented for thousands of years. Two systematic reviews have highlighted the benefits of acupuncture on endocrine hormone levels26 and its potential to improve clinical pregnancy rates and live birth rates.27 Recent studies suggest that acupuncture enhances ovarian function by regulating the H-P-O axis, enhancing uterine tissue morphology, and strengthening the immune system through the regulation of the nerve-endocrine-immune network.28 Additionally, acupuncture has been shown to improve ovarian reserve by regulating key signaling pathways such as PI3K/Akt, Nrf2/ARE, and Bcl-2/Caspase-3, balancing hormone levels, and reducing granulosa cell apoptosis.18,29,30 Further research highlights that acupuncture can improve ovarian function by exerting antioxidant and anti-apoptotic effects.31 While these mechanisms have not yet been clinically validated, they offer a biologically plausible framework for understanding how acupuncture may enhance ovarian reserve and support reproductive function. Collectively, they provide a theoretical foundation for its potential use as a complementary treatment option for patients with DOR.
Based on Traditional Chinese Medicine theory, ovarian function is intricately connected to the Ren, Chong, and Kidney meridians. Accordingly, we selected the CV 4 and CV 3 on the Ren meridian, the KI 16 on the Kidney meridian, and the ST 21 and ST 36 on the Stomach meridian to nourish blood and balance Qi. The EX-CA 1 specifically improves uterine and ovarian disorders, while GV 20 and GV 24 are used to improve sleep quality and reduce anxiety. Our clinical observations have shown that electro-acupuncture at these points is beneficial for regulating menstrual cycles and enhancing the likelihood of clinical pregnancy. A consensus among experts on acupoint selection for DOR aligns with our choices, validating our choice of points as referential.32
Sham acupuncture serves as a common control design to mitigate the placebo effect in acupuncture RCTs. Variations in sham acupuncture include different needling techniques (eg, blunt needles, non-penetrative cotton pads, deactivating electric currents), alternative acupoint locations (eg, non-meridian, non-acupoint sites), and diverse needling details (eg, different insertion depth and number of needles).33 In this study, the treatment frequency, duration, and total treatment period in both groups are identical. The key differences lie in acupoint selection, needling depth, and the activation of the electro-acupuncture device. Given the abdominal location of our chosen acupoints, where the cotton pad method could compromise blinding, we utilize superficial needling at non-meridian, non-acupoint sites to exclude placebo effect. To maintain blinding while distinguishing therapeutic effects from the real electro-acupuncture group, the electro-acupuncture device in the SA group is deactivated after 30 seconds while retaining the needles for the full 30 minutes.
The ovarian reserve represents the number of oocytes available for potential fertilization at a given time and can be assessed through serum tests or ultrasound examination. The ASRM Practice Committee recommends using FSH, E2, AMH, and AFC to evaluate ovarian reserve. Elevated basal FSH is a specific marker for DOR, and normal basal FSH levels with elevated E2 levels (>60–80 pg/mL) may also suggest DOR. AFC is commonly used to estimate the number of available oocytes and ovarian responsiveness,1 while AMH is considered a more sensitive marker that typically declines earlier than FSH.34 In this study, serum basal hormone levels, AMH, and AFC will be collected before and after treatment to evaluate its impact on ovarian function. However, these biomarkers are surrogate endpoints and may not fully predict fertility outcomes. As such, any observed improvements in these indicators will be interpreted cautiously and supplemented by clinical endpoints to assess treatment efficacy. Given the high prevalence of emotional distress among women with DOR, and prior evidence suggesting that acupuncture may exert anxiolytic and mood-stabilizing effects, validated instruments (SAS, SDS, and Modified Kupperman Index) will be included to evaluate potential psychological benefits. Nonetheless, as such outcomes may be partially influenced by non-specific effects or patient expectations, findings related to psychological measures will be interpreted cautiously and contextualized within the limitations of sham-controlled designs.
In rigorous randomized controlled trials, excluding specific patient groups is crucial for ensuring patient safety and maintaining data accuracy.35 In this trial, we excluded participants with conditions that might impact ovarian function, allowing the observed outcomes to be directly attributed to the electro-acupuncture treatment. For instance, endocrine disorders such as hyperprolactinemia or severe thyroid dysfunction can alter hormonal balance, complicating the evaluation of treatments for DOR.36,37 Similarly, reproductive system abnormalities, such as severe hydrosalpinx or invasive fibroids, impair fertility and could mask the true effects of the intervention.38,39 Patients with autoimmune disorders like lupus present additional risks due to the increased likelihood of pregnancy complications and the need for immunosuppressive treatments.40 We also excluded individuals with infertility linked to congenital malformations or genetic abnormalities to focus solely on DOR as the primary cause.
Additionally, for patients seeking to conceive, we conduct a subgroup analysis by collecting data on ovulation induction outcomes (eg, number of oocytes retrieved, MII oocyte rate), along with pregnancy outcomes (eg, miscarriage, clinical pregnancy, and live birth) between both groups. This subgroup analysis is designed to assess and compare the impact of electro-acupuncture on both the quantity and quality of oocytes and the subsequent pregnancy results. Compared to conditions such as premature ovarian insufficiency and premature ovarian failure, which are limited by strict age and clinical criteria, DOR encompasses a broader spectrum of patients experiencing a gradual decline in ovarian reserve.41 To explore age-related differences in etiology and treatment response, we will perform stratified analyses across three age groups: ≥40 years, 32–40 years, and ≤32 years. This exploratory age-based grouping aims to assess whether the effects of electro-acupuncture vary across different reproductive stages and underlying causes of DOR.42 In addition, the study adopts a broad definition of DOR and conducts subgroup analyses based on both age and method of conception to better evaluate the potential differential effects of electro-acupuncture in various clinical contexts and identify its optimal timing and application. Specifically, electro-acupuncture may serve as a non-pharmacological adjunct in ART clinics for women with poor ovarian response or repeated ART failure, and as a standalone option for those with early-stage DOR seeking to improve ovarian function or delay fertility decline. Cost-effectiveness, accessibility, and integration into fertility care pathways will be further explored in follow-up research based on the trial outcomes. Ultimately, this study aims to generate evidence that may inform future clinical research and support the potential integration of acupuncture into reproductive medicine for women with DOR.
Trial Status
The approval of the ethics committee was given on 6 December 2023. The first patient was enrolled on March 3, 2024, and the trial is projected to conclude in October 2026. The current protocol version is 2.0, dated 05 December 2023. This trial is in the recruiting phase at the time of manuscript submission.
Confidentiality
All information regarding potential and enrolled participants in this trial will be kept confidential, accessible only to trial members for administrative purposes. Acupuncturists will not have access to the data before the trial’s completion. Participants’ names will not appear in any public disclosures or reports related to the study. Researchers will make every effort to protect the privacy of the participants’ medical information.
Data Sharing Statement
The full data set will be made available when the trial is completed and published. Application for the data to be released should be made in contact to HZ.
Ethics Statement
The final revised version of the study protocol (version 2, dated 15 December 2023) and the written informed consent used in the study were assessed and approved by the Ethics Committee of Shenzhen Hospital of Shanghai University of Traditional Chinese Medicine (2023-LHQZYYYXLL-KY-147) and Luohu People’s Hospital (2024-LHQRMYY-KYLL-009). This trial will be performed in accordance with the World Medical Association Declaration of Helsinki, the guidelines for Good Clinical Practice, and relevant Chinese clinical trial research norms and regulations. Written informed consent will be obtained from every participant prior to registration.
Acknowledgments
Thanks to Professor Zhi-shun Liu of Guang’anmen Hospital of China Academy of Traditional Chinese Medicine for his advice on this research programme, and to Dr. Yan-hui Liu of Luohu People's Hospital for their support in participant recruitment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Sanming Project of Medicine in Shenzhen (No. SZZYSM 202101007), 2021 Luohu Soft Science Research Programme Project (No. LX20210102), and Shenzhen Science and Technology Plan Project (No. JCYJ20210324120804012). The funder had no role in the study’s design, data collection, management, analysis, interpretation, results reporting, or the decision to submit the findings for publication.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Practice Committee of the American Society for Reproductive Medicine. Electronic address: [email protected], Practice Committee of the American Society for Reproductive Medicine. Testing and interpreting measures of ovarian reserve: a committee opinion. Fertil Steril. 2020;114:1151–1157. doi:10.1016/j.fertnstert.2020.09.134
2. May-Panloup P, Boucret L, Chao De La Barca JM, et al. Ovarian ageing: the role of mitochondria in oocytes and follicles. Hum Reprod Update. 2016;22:725–743. doi:10.1093/humupd/dmw028
3. Bleil ME, Adler NE, Pasch LA, et al. Depressive symptomatology, psychological stress, and ovarian reserve: a role for psychological factors in ovarian aging? Menopause. 2012;19:1176–1185. doi:10.1097/gme.0b013e31825540d8
4. Zhu Q, Li Y, Ma J, Ma H, Liang X. Potential factors result in diminished ovarian reserve: a comprehensive review. J Ovarian Res. 2023;16:208. doi:10.1186/s13048-023-01296-x
5. Devine K, Mumford SL, Wu M, DeCherney AH, Hill MJ, Propst A. Diminished ovarian reserve in the United States assisted reproductive technology population: diagnostic trends among 181,536 cycles from the Society for Assisted Reproductive Technology Clinic Outcomes Reporting System. Fertil Steril. 2015;104:612–619.e3. doi:10.1016/j.fertnstert.2015.05.017
6. Centers for Disease Control and Prevention. 2021 assisted reproductive technology fertility clinic and national summary report. USA: Department of Health and Human Services; 2023.
7. Quinn MM, Cedars MI. Cardiovascular health and ovarian aging. Fertil Steril. 2018;110:790–793. doi:10.1016/j.fertnstert.2018.07.1152
8. Cheng CH, Chen LR, Chen KH. Osteoporosis due to hormone imbalance: an overview of the effects of estrogen deficiency and glucocorticoid overuse on bone turnover. Int J Mol Sci. 2022;23:1376. doi:10.3390/ijms23031376
9. Verdiesen RMG, Onland-Moret NC, van Gils CH, et al. Anti-Müllerian hormone levels and risk of type 2 diabetes in women. Diabetologia. 2021;64:375–384. doi:10.1007/s00125-020-05302-5
10. Wierman ME, Kiseljak-Vassiliades K. Should Dehydroepiandrosterone be administered to women? J Clin Endocrinol Metab. 2022;107:1679–1685. doi:10.1210/clinem/dgac130
11. Gu H, Zhao X, Zhao X, Yang Y, Lv X. Risk of stroke in healthy postmenopausal women during and after hormone therapy: a meta-analysis. Menopause. 2014;21:1204–1210. doi:10.1097/GME.0000000000000227
12. Meaidi A, Mascolo A, Sessa M, et al. Venous thromboembolism with use of hormonal contraception and non-steroidal anti-inflammatory drugs: nationwide cohort study. BMJ. 2023;382:e074450. doi:10.1136/bmj-2022-074450
13. Hu S, Xu B, Jin L. Perinatal outcome in young patients with diminished ovarian reserve undergoing assisted reproductive technology. Fertil Steril. 2020;114:118–124.e1. doi:10.1016/j.fertnstert.2020.02.112
14. Zhu S, Jiang W, Liao X, Sun Y, Chen X, Zheng B. Effect of diminished ovarian reserve on the outcome of fresh embryo transfer in IVF/ICSI cycles among young women: a retrospective cohort study. BMC Women's Health. 2024;24:230. doi:10.1186/s12905-024-03039-6
15. Expert Group of Consensus on Clinical Diagnosis & Management of Diminished Ovarian Reserve. Reproductive Endocrinology & Fertility Preservation Section of Chinese Society on Fertility Preservation under Chinese Preventive Medicine Association. Consensus on clinical diagnosis and management of diminished ovarian reserve. J Reprod Med. 2022;31:425–434. doi:10.3969/j.issn.1004-3845.2022.04.001
16. Lin G, Liu X, Cong C, Chen S, Xu L. Clinical efficacy of acupuncture for diminished ovarian reserve: a systematic review and meta-analysis of randomized controlled trials. Front Endocrinol. 2023;14:1136121. doi:10.3389/fendo.2023.1136121
17. Sullivan SD, Sarrel PM, Nelson LM. Hormone replacement therapy in young women with primary ovarian insufficiency and early menopause. Fertil Steril. 2016;106:1588–1599. doi:10.1016/j.fertnstert.2016.09.046
18. Fan S, Fang Y-G. Research progress of acupuncture for the improvement of ovarian reserve by regulating different signal pathways. Acupuncture Res. 2022;47:644–648. doi:10.13702/j.1000-0607.20210330
19. Xie Y, Shi W, Tan Y, et al. Acupuncture and moxibustion for diminished ovarian reserve: a scoping review. Complement Ther Med. 2023;77:102973. doi:10.1016/j.ctim.2023.102973
20. Guven PG, Cayir Y, Borekci B. Effectiveness of acupuncture on pregnancy success rates for women undergoing in vitro fertilization: a randomized controlled trial. Taiwan J Obstet Gynecol. 2020;59:282–286. doi:10.1016/j.tjog.2020.01.018
21. Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158:200–207. doi:10.7326/0003-4819-158-3-201302050-00583
22. Ferraretti AP, La Marca A, Fauser BC, et al. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum Reprod. 2011;26:1616–1624. doi:10.1093/humrep/der092
23. World Health Organization Western Pacific Region. World Health Organization Standard Acupuncture Point Locations. Beijing: People’s Medical Publishing House; 2010.
24. Zhang J, Jia H, Diao F, Ma X, Liu J, Cui Y. Efficacy of dehydroepiandrosterone priming in women with poor ovarian response undergoing IVF/ICSI: a meta-analysis. Front Endocrinol. 2023;14:1156280. doi:10.3389/fendo.2023.1156280
25. Smith JF, Eisenberg ML, Millstein SG, et al. The use of complementary and alternative fertility treatment in couples seeking fertility care: data from a prospective cohort in the United States. Fertil Steril. 2010;93:2169–2174. doi:10.1016/j.fertnstert.2010.02.054
26. Cao H, Li H, Lin G, et al. The clinical value of acupuncture for women with premature ovarian insufficiency: a systematic review and meta-analysis of randomized controlled trials. Front Endocrinol. 2024;15:1361573. doi:10.3389/fendo.2024.1361573
27. Zheng CH, Huang GY, Zhang MM, Wang W. Effects of acupuncture on pregnancy rates in women undergoing in vitro fertilization: a systematic review and meta-analysis. Fertil Steril. 2012;97:599–611. doi:10.1016/j.fertnstert.2011.12.007
28. Xia L, Xia Y. Clinical research and the effect mechanism on premature ovarian failure treated with acupuncture in recent 20 years. Chin Acupunct Moxibustion. 2018;38:5653–5670. doi:10.13703/j.0255-2930.2018.05.031
29. Zhang H, Qin F, Liu A, et al. Electro-acupuncture attenuates the mice premature ovarian failure via mediating PI3K/AKT/mTOR pathway. Life Sci. 2019;217:169–175. doi:10.1016/j.lfs.2018.11.059
30. Wang S, Lin S, Zhu M, et al. Acupuncture reduces apoptosis of granulosa cells in rats with premature ovarian failure via restoring the PI3K/Akt signaling pathway. Int J Mol Sci. 2019;20:6311. doi:10.3390/ijms20246311
31. Jing Y, Huimin F, Fang Q, et al. Effect on serum metabolomics of rats with premature ovarian insufficiency by Zhibian (BL54) through Shuidao (ST28) acupuncture. J Tradit Chin Med. 2024;44:722–733. doi:10.19852/j.cnki.jtcm.20231226.001
32. Qu F, Li R, Sun W, et al. Use of electroacupuncture and transcutaneous electrical acupoint stimulation in reproductive medicine: a group consensus. J Zhejiang Univ Sci B. 2017;18:186–193. doi:10.1631/jzus.B1600437
33. Lee YS, Kim SY, Lee H, Chae Y, Lee MS. ACURATE: a guide for reporting sham controls in trials using acupuncture. J Evid Based Med. 2023;16:82–90. doi:10.1111/jebm.12524
34. De Vet A, Laven JSE, de Jong FH, Themmen APN, Fauser BC. Antimüllerian hormone serum levels: a putative marker for ovarian aging. Fertil Steril. 2002;77:357–362. doi:10.1016/s0015-0282(01)02993-4
35. U.S. Food and Drug Administration. Evaluating inclusion and exclusion criteria in clinical trials. Workshop Report. Silver Spring, MD: U.S. Food and Drug Administration; 2020.
36. Concepción-Zavaleta MJ, Coronado-Arroyo JC, Quiroz-Aldave JE, et al. Endocrine factors associated with infertility in women: an updated review. Expert Rev Endocrinol Metab. 2023;18:399–417. doi:10.1080/17446651.2023.2256405
37. Dosiou C. Thyroid and Fertility: recent Advances. Thyroid. 2020;30:479–486. doi:10.1089/thy.2019.0382
38. Capmas P, Suarthana E, Tulandi T. Management of hydrosalpinx in the era of assisted reproductive technology: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2021;28:418–441. doi:10.1016/j.jmig.2020.08.017
39. Moini A, Kalhor M, Jahanian Sadatmahalleh S, et al. Evaluation of the relationship between ovarian reserve with congenital anomalies and intramural uterine leiomyoma among infertile women: a cross-sectional study. J Ovarian Res. 2023;16:68. doi:10.1186/s13048-023-01149-7
40. Mao R, Wang X, Long R, Wang M, Jin L, Zhu L. A new insight into the impact of systemic lupus erythematosus on oocyte and embryo development as well as female fertility. Front Immunol. 2023;14:1132045. doi:10.3389/fimmu.2023.1132045
41. Pastore LM, Christianson MS, Stelling J, Kearns WG, Segars JH. Reproductive ovarian testing and the alphabet soup of diagnoses: DOR, POI, POF, POR, and FOR. J Assist Reprod Genet. 2018;35:17–23. doi:10.1007/s10815-017-1058-4
42. Sun W, Stegmann BJ, Henne M, Catherino WH, Segars JH. A new approach to ovarian reserve testing. Fertil Steril. 2008;90:2196–2202. doi:10.1016/j.fertnstert.2007.10.080
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
Evaluating the Efficacy and Underlying Mechanisms of Acupuncture for Chronic Subjective Tinnitus Using Functional Near-Infrared Spectroscopy: Study Protocol for a Randomized Controlled Trial
Hu H, Lin X, Fang L, Li Y, Gao H
Journal of Pain Research 2023, 16:3367-3378
Published Date: 4 October 2023
A Pilot Study for Effectiveness and Safety of Adjunctive Pharmacopuncture to Acupuncture Treatment for Rotator Cuff Diseases: A Pragmatic Randomized Controlled Trial
Cha HJ, Han CH, Jeon JH, Jeong JK, Jung IC, Yang C, Kang BK, Kim MJ, Choi YE, Kim YI
Journal of Pain Research 2024, 17:2203-2221
Published Date: 24 June 2024
Acupuncture at Sensitized Acupoints versus Sham Acupuncture for Neck-Type Cervical Spondylosis: Study Protocol for a Randomized Controlled Trial
Li C, Wang J, Shao X, Wu Y, Qu X, Cai J, He L, Yu L, Xu R, Xia Y, Wang R, Zhang L, Qiu Y
Journal of Pain Research 2025, 18:6963-6976
Published Date: 23 December 2025
Clinical Efficacy of Acupuncture as Adjunctive Therapy for Cough Variant Asthma: Study Protocol for a Pilot Randomized Controlled Trial
Chen X, Liu Y, Li H, Deng X, Li J, Zhang H, Liang F, Xu G
Journal of Asthma and Allergy 2026, 19:586197
Published Date: 25 February 2026