Back to Journals » Journal of Inflammation Research » Volume 19
Acupuncture Activates PI3K/Akt Pathway to Promote Spinal Microglial M2 Polarization and Alleviate Spastic Hemiplegia Following Ischemic Stroke
Authors Ma LH, Ma LX ![]() , Qian X
, Qian X ![]() , Xiu JY, Chen MY, He JL
, Xiu JY, Chen MY, He JL
Received 9 January 2026
Accepted for publication 2 April 2026
Published 17 April 2026 Volume 2026:19 592917
DOI https://doi.org/10.2147/JIR.S592917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Ling-Hui Ma,1 Liang-Xiao Ma,1,2 Xu Qian,1 Jing-Yun Xiu,1 Meng-Yu Chen,1 Jia-Ling He1
1School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2The Key Unit of State Administration of Traditional Chinese Medicine for Evaluation of Characteristic Acupuncture Therapy, Beijing University of Chinese Medicine, Beijing, People’s Republic of China
Correspondence: Liang-Xiao Ma, School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, No. 11 Bei San Huan Dong Lu, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]
Purpose: Studies showed that post-ischemic spastic hemiplegia can be linked to neuroinflammation mediated by microglial polarization. Microglial M1/M2 polarization is regulated by the PI3K/Akt pathway. We previously reported that acupuncture alleviated spasticity after permanent middle cerebral artery occlusion (p-MCAO). This study investigated whether its antispastic effects were associated with activation of the spinal PI3K/Akt pathway and promotion of microglial M2 polarization.
Methods: p-MCAO was induced in Sprague-Dawley rats to establish a model of spastic hemiplegia. Yanglingquan (GB34) was needled using waggle needling, a motion‑style acupuncture technique. Its association with spasticity alleviation and motor recovery was evaluated by behavioral assessments, TTC staining, and the H-reflex test. Molecular analyses were performed to investigate the underlying mechanisms. Minocycline was used to examine the role of microglial polarization, while LY294002 and 740Y-P were used to determine whether the effects of acupuncture were mediated through the PI3K/Akt pathway.
Results: Rats with p-MCAO-induced spastic hemiplegia exhibited neurological deficits, increased muscle tone, motor dysfunction, and spinal hyperexcitability, together with microglial M1 polarization, inflammatory responses, spinal excitatory/inhibitory imbalance, and suppressed PI3K/Akt activity. Acupuncture at GB34 alleviated spasticity and promoted motor recovery. It also activated the spinal PI3K/Akt pathway, promoted microglial M2 polarization, reduced IL-6 and TNF-α, and increased IL-10 and TGF-β. In addition, acupuncture attenuated spinal hyperexcitability, as indicated by improvement in the H-reflex, and restored spinal excitatory/inhibitory balance, as reflected by regulation of vGluT1/vGAT-associated synaptic markers and Glu/GABA levels. Minocycline produced partially similar improvements, whereas LY294002 partially blocked the effects of acupuncture and 740Y-P only partially mimicked them.
Conclusion: Acupuncture alleviates spastic hemiplegia by activating the PI3K/Akt pathway and promoting spinal microglial M2 polarization. These findings support its potential clinical application for post-stroke spasticity and identify the PI3K/Akt pathway as a potential therapeutic target.
Keywords: ischemic stroke, spastic hemiplegia, neuroinflammation, microglial, PI3K/Akt, acupuncture
Introduction
Ischemic stroke remains a major cause of long-term disability despite advances in recanalization therapy.1–3 Post-stroke spastic hemiplegia is a key contributor to persistent motor dysfunction and reduced quality of life, and its development is closely associated with neuroinflammation.4–6 Microglia represent one of the quintessential immune cell populations within the central nervous system, orchestrating neuroinflammatory responses via a finely tuned equilibrium between the M1 and M2 polarization states.7,8 M1-polarized microglia intensify the inflammatory cascade by secreting a repertoire of proinflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), whereas M2-polarized microglia counteract this process by releasing anti-inflammatory cytokines such as interleukin-10 (IL-10) and transforming growth factor-beta (TGF-β), along with neurotrophic factors.9,10 Therefore, driving M1-to-M2 phenotypic polarization represents a promising strategy for functional recovery after stroke.
Current research on modulating microglial polarization to improve post-stroke functional recovery has predominantly focused on the primary brain lesion site.11–13 While it is crucial to note that the critical circuits for motor execution reside at the spinal level. Following upper motor neuron injury, the distal spinal cord undergoes adaptive reorganization, resulting in sensory-motor abnormalities and hyperreflexia.14 This is driven by increased proprioceptive afferents, impaired Ia presynaptic inhibition, and KCC2 downregulation, together raising motor neuron excitability.15,16 Spinal microglia are involved in this process, particularly within the subacute and chronic stages of stroke, indicating their importance in motor disorders such as spasticity.17,18 Available evidence suggests that spinal microglial activation emerges early after ischemia and remains prominent during the first week after MCAO.19,20 Moreover, marked spinal microglial activation, together with pathological changes related to spinal circuit remodeling and hyperreflexia, can still be detected on postoperative day 10 after corticospinal tract injury.17,18 Previous studies have also shown that muscle tone in MCAO rats begins to increase on postoperative day 3 and remains elevated until day 10 before gradually recovering thereafter.21,22 These temporal dynamics support postoperative days 4 to 10 as a biologically relevant intervention window in the present study.
Recent studies have shown that activation of the PI3K/Akt signaling pathway contributes to post-stroke recovery by exerting protective effects through anti-apoptosis, anti-inflammation, anti-oxidation, angiogenesis, and neurogenesis, thereby facilitating the restoration of brain tissue structure and neurological function.23,24 In particular, emerging evidence has demonstrated that modulation of the PI3K/Akt signaling pathway promotes microglial M2 polarization and alleviates microglia-mediated neuroinflammation, thereby ameliorating neurological deficits and motor dysfunction after ischemic stroke.25–27 Previous studies have further shown that acupuncture may modulate PI3K/Akt signaling in the central nervous system after ischemic injury, thereby contributing to neuroprotection through multiple mechanisms, including suppression of neuroinflammation, promotion of angiogenesis, and enhancement of neural repair, ultimately improving stroke outcomes.27–30 Collectively, these findings suggest that PI3K/Akt signaling may represent an important molecular link between acupuncture and microglia-mediated recovery after stroke.
Clinical guidelines recommend acupuncture for post-stroke rehabilitation, particularly for improving motor function and alleviating spasticity.31–33 Meta-analyses have demonstrated that acupuncture reduces post-stroke spasticity, especially when combined with conventional rehabilitation (standardized mean difference [SMD] = −0.73), while acupuncture alone also provides modest benefit (SMD = −0.22).34 Higher treatment frequency and more sessions may improve outcomes, but optimal timing and standardized parameters remain unclear. Thus, preclinical studies are needed to elucidate the mechanisms and reinforce the translational value of acupuncture for post-stroke spasticity. Yanglingquan (GB34), known as the influential point of sinews in classical acupuncture theory, is commonly used in acupuncture for post-stroke lower limb motor dysfunction.35 Previous clinical and experimental studies have suggested that GB34 stimulation is associated with improvement in motor recovery and spasticity-related abnormalities after stroke.36–39 Notably, sensory signals evoked by acupuncture at lower-limb acupoints are conveyed by somatic afferents to the relevant spinal segments, where they may directly modulate spinal circuits involved in spasticity and motor function, before being integrated at supraspinal levels.40,41 Consistent with this, GB34 has been shown to modulate spinal motor-related neural activity and reduce lumbar spinal neuronal hyperexcitability, which supports its potential to influence spinal circuits regulating spasticity and motor function.21,39,42
Studies have shown that acupuncture mitigates acute ischemic brain injury by modulating microglial activation and polarization, suppressing neuroinflammation, and promoting vascular remodeling and neurogenesis, thereby improving neurological and motor outcomes.43–45 Therefore, elucidating the spinal molecular mechanisms underlying acupuncture’s anti-spasticity effects following stroke is of paramount importance.
Hyperexcitability of the spinal cord is a hallmark of post-stroke spasticity, involving enhanced excitatory synaptic transmission and attenuated inhibitory control, and can be functionally reflected by an augmented H-reflex.46 In spinal motor circuits, vGluT1, together with its cognate neurotransmitter Glu, reflects excitatory glutamatergic input, whereas vGAT, along with GABA and Gly, reflects inhibitory GABAergic and glycinergic transmission.47,48 When these excitatory and inhibitory systems become dysregulated, the excitatory/inhibitory (E/I) balance is disrupted, thereby contributing to spinal hyperexcitability and spasticity.49 Moreover, pro-inflammatory microglial activation may further aggravate this process by weakening inhibitory signaling and promoting inflammatory synaptic remodeling.50,51 Such sustained spinal hyperexcitability may in turn obstruct adaptive neuroplasticity and impede motor recovery. Our prior research has confirmed that acupuncture administered during the subacute phase post-cerebral ischemia can mitigate the heightened excitability of the spinal cord, alleviate limb spasticity, and facilitate motor recovery by upregulating spinal KCC2 expression.39
However, the precise spinal mechanisms by which acupuncture modulates inflammation and improves post-stroke spasticity remain unclear. In particular, whether acupuncture regulates spinal microglial polarization through the PI3K/Akt pathway has yet to be elucidated. Therefore, we hypothesize that acupuncture at GB34 may modulate spinal microglial polarization through a PI3K/Akt-mediated anti-inflammatory pathway, normalizing the aberrant hyper-excitability of motor neurons after stroke, facilitating adaptive synaptic plasticity, thereby promoting functional motor recovery.
Materials and Methods
Animals
Healthy male Sprague-Dawley rats (260 ± 20 g, 7–8 weeks of age, Vital River Laboratory, China) were used for this study. All rats were acclimatized for one week and kept in cages of 4 under standard SPF housing conditions at room temperature (22 ± 2°C) with a 12-h light/dark cycle with standard rodent food and water. All experimental procedures were approved by the Ethics Committee of Animal Experimentation at Beijing University of Chinese Medicine (BUCM-1-2,025,010,501-1042), were conducted in accordance with the Guide for the Care and Use of Laboratory Animals, and adhered to the principles of Replacement, Reduction, and Refinement (3Rs).
Drug Preparation and Treatment
Minocycline hydrochloride (HY-17412, MedChemExpress), a widely used microglial activation inhibitor, was shown to selectively suppress M1 polarization of microglia.52 It was administered intraperitoneally at a dose of 45 mg/kg, dissolved in phosphate-buffered saline before injection,53 once daily for one week.
The PI3K agonist 740 Y-P (HY-P0175, MedChemExpress; 10 mg/kg) and inhibitor LY294002 (HY-10108, MedChemExpress; 20 mg/kg) were used at doses selected on the basis of previous in vivo studies involving central nervous system injury and PI3K/Akt pathway modulation.54–56 All drugs were administered intraperitoneally once daily for one week, from postoperative day 4 to day 10, 30 minutes before acupuncture treatment.
Study Design
To assess acupuncture’s efficacy on MCAO rats with spastic hemiplegia, four groups were set: sham-operated group (S), Spastic hemiplegia following MCAO group (M), acupuncture at acupoint group (M+AP), and acupuncture at control non-acupoint group (M+CP). To probe the role of microglial polarization, the minocycline hydrochloride (MC) was administered, four groups were set: S, M, M+MC, and vehicle group (M+Veh). To define the involvement of the PI3K/Akt pathway, the inhibitor LY294002 (LY) and agonist 740Y-P were administered, five groups were set: M, M+AP+LY, M+AP+Veh, M+Veh, and M+740Y-P.
All animals were randomly allocated to distinct groups before the model- establishing surgical procedure based on a random number table generated by Microsoft Excel 2019. The assessment and analysis of experimental indices were conducted by independent investigators who remained blinded to the treatment group assignments throughout the study. The experimental design and reporting in this study adhered to the ARRIVE guidelines.
Surgical Procedure and Model Evaluation
Following anesthesia with 3% isoflurane in 97% oxygen, rats were subjected to the permanent middle cerebral artery occlusion (p-MCAO).57 After a midline skin incision on the ventral neck, the right common carotid artery was exposed, and a poly-L-lysine-coated monofilament nylon suture with a diameter of 0.36 ± 0.02 mm (Beijing Cinontech, China) was precisely advanced through the right external carotid artery to the internal carotid artery and further to the origin of the middle cerebral artery to achieve significant occlusion of its blood flow.58 Subsequently, the suture was secured, and the incision was closed in layers. Throughout surgery, body temperature was maintained at 37.0 ± 0.5°C. Postoperative care included thermoregulation and the provision of a soft diet. Sham-operated rats received the same anesthesia, scalp incision and muscle dissection as the MCAO group, but without middle cerebral artery occlusion. This procedure controlled for non-specific effects such as surgical stress and handling, enabling clear distinction between specific effects of MCAO and acupuncture.
Cerebral blood flow (CBF) in the middle cerebral artery territory was monitored before and after modeling using laser speckle contrast imaging (PeriCam PSI system, Stockholm, Sweden) to confirm successful occlusion (Figure 1A). The spastic hemiplegia model after MCAO was considered successful only if the following criteria were met: the reduction in CBF of >70%, the Zea Longa score of 1–3 immediately after recovery from anesthesia, and the Modified Ashworth Scale (MAS) grade ≥ 1 together with a swim test score ≥ 1 on postoperative day 3. All assessments were performed by independent investigators blinded to the group assignments.
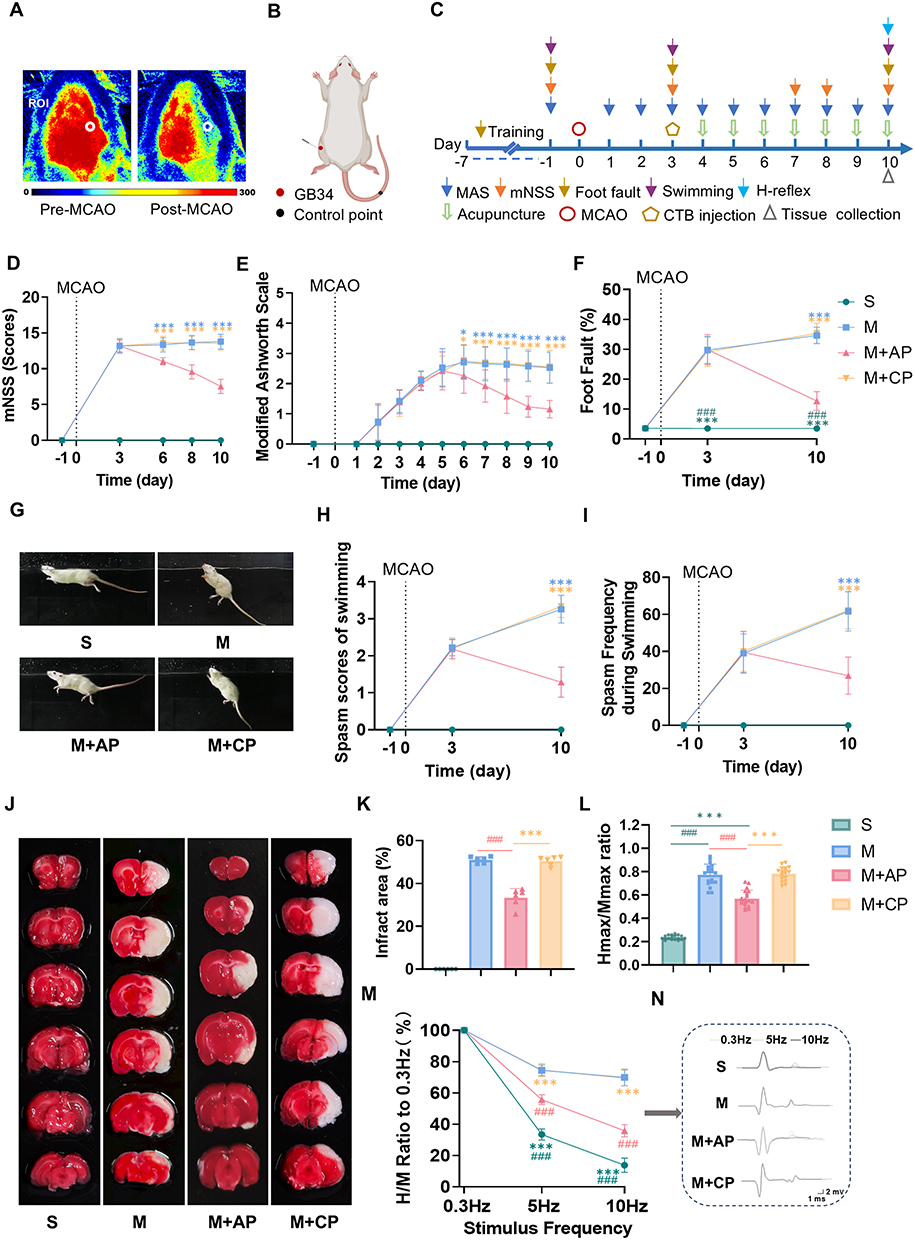 |
Figure 1 Acupuncture ameliorated neurological deficits, muscle spasticity, motor dysfunction, spinal hyperreflexia and ischemic brain injury in MCAO rats with spastic hemiplegia. (A) Representative laser speckle images for illustrating cortical blood flow dynamic following MCAO. (B) Locations of acupuncture sites. (C) Experimental procedures. (D) mNSS for neurologic deficits assessments. (E) MAS for muscle tension evaluations. (F) Foot fault test for motor coordination assessments. Swimming test for lower limb spasticity evaluations: representative pictures (G); spasm scores (H); spasm frequency (I). TTC staining (J) and quantitative analysis (K) in cerebral infarcted areas (n=6). H-reflex for spinal excitability assessments: Hmax/Mmax ratio (L), frequency-dependent depression (FDD) of the H-reflex (M) and representative traces recorded at 0.3 Hz, 5 Hz, and 10 Hz (N). S (sham-operated) group (n = 18), M (model) group (n = 19), M+AP (model + acupuncture point) group (n = 19), M+CP (model + control point) group (n = 18). Data were expressed as mean ± SD. *P<0.05, ***<0.001 versus M+AP group; ###P<0.001 versus M group. |
A total of 355 rats were employed in this experiment. Sample size was determined based on preliminary data and prior research findings,21,39,59 which indicated a spasticity incidence rate of approximately 65% in the p-MCAO model. This parameter was used to calculate the minimum number of rats required for each surgical group to ensure adequate statistical power for detecting inter-group differences. Excluding 36 rats assigned to the sham-operation group, 319 rats were subjected to p-MCAO surgery. Of these, 207 rats fulfilled the inclusion criteria for the spastic hemiplegia model and were thus incorporated into the experimental cohort (Supplementary Table 1).
Acupuncture Intervention
From postoperative day 4 to day 10, the M+AP and M+CP groups received daily acupuncture treatment. All acupuncture procedures were performed by the same trained and licensed acupuncturist. In the M+AP group, a sterile acupuncture needle (0.18 × 13 mm) was inserted perpendicularly to a depth of 4–5 mm at GB34 on the affected (left) side, which is located in the depression distal to the head of the fibula on the hind limb (Figure 1B). The needle was then withdrawn to the subcutaneous level, and a motion-style acupuncture technique, waggle needling, was performed according to a previously described standardized protocol,59 involving multi-directional lifting and thrusting at GB34 for 1 min combined with passive movement of the affected left hind limb for 1 min. Finally, the needle was reinserted to a depth of 4–5 mm and retained for 30 min. In the M+CP group, a sterile needle was inserted superficially (1 mm) at the midpoint of the tail and retained for 30 min without any manipulation. This site was selected as a non-acupoint control because it has been commonly used as a control point in previous acupuncture studies.21,39,60,61
Behavioral Assessments
Modified Neurological Severity Score (mNSS)
To evaluate overall neurological function, the mNSS (0–18 points) was performed, where score 0 meant normal neurological function and score 18 indicated the maximum neuronal injury. This composite score examines motor function, sensory response, beam walking, as well as reflex absence and abnormal movements.62
MAS
To measure muscle tone, the MAS was applied. All MAS scoring was performed by two independent investigators blinded to group allocation using a standardized scoring procedure. In this study, the scale ranged from 0 to 5, with a grade of “1+” counted as 2 points for the purpose of data analysis. Higher scores represent more severe hypertonia and greater limitation of joint movement.63
Swimming Test
To quantify hindlimb spasticity of rats, a swimming test was conducted in a water tank maintained at a constant 23°C. Spasticity was scored (0–4) based on the angle between the torso and the water surface during swimming. The scoring criteria were as follows: a non-spastic posture (torso parallel to water surface, angle 10°–30°) was scored as 0. For rats that swam for less than half of the trial in a mild spastic position (angle 30°–55°) or a severe spastic position (angle 55°–90°), scores of 1 and 3 were assigned, respectively. Scores of 2 and 4 were given when rats swam for more than half of the trial in a mild or severe spastic position, respectively.64 The frequency was expressed as the percentage of spastic episodes observed over 10 trials.65
Foot Fault Test
To assess motor coordination, rats underwent the foot-fault test on a horizontal ladder (1 m long, 30 cm high) with variable rung intervals (1–3 cm). The performance was quantified by calculating the percentage of hindlimb slips as described previously.66
Electrophysiological Evaluation
The excitability of spinal cord was assessed through recording the H-reflex from spastic muscles using a BL420n bio-functional data acquisition system (Chengdu Taimeng Technology). Under anesthesia, the left sciatic nerve was isolated and connected to a bipolar hook electrode. A pair of electrodes (approximately 2 mm apart) were inserted into the interosseous muscles of the left hind paw for electromyography recording, and the reference electrode was inserted superficially into the tail. Consistent with previous studies,21,39,59 the H-reflex was elicited by delivering single bipolar electrical pulses (100 μs width) to the sciatic nerve at incrementally increased intensities ranging from 0.1 to 10 mA in 0.2 mA steps. Both H-waves and M-waves were continuously monitored and recorded across all stimulating intensities. Using the stimulus intensity that evoked Hmax, the H-reflex amplitude was recorded at frequencies of 0.3, 5, and 10 Hz. Frequency-dependent depression (FDD) was determined as the percentage of the response amplitude at 5 Hz and 10 Hz relative to that at 0.3 Hz.
2,3,5-Triphenyltetrazolium Chloride (TTC) Staining
Cerebral infarct size was measured by TTC staining. Coronal brain sections with a thickness of 2 mm were prepared after brief freezing, stained with 0.3% TTC solution at 37°C for 20–30 min in darkness. The cerebral infarct area was determined from photographed sections using ImageJ software (U.S. National Institutes of Health). The infarct area percentages were calculated as: (Contralateral area - Non-infarcted ipsilateral area)/Contralateral area × 100%.67
Motor Neuron Tracing
For retrograde labeling of motor neurons innervating the hindlimb calf muscles, after anesthetization, 5 μL of Cholera Toxin Subunit B (CTB, BrainVTA) was microinjected into the epineurium of the left sciatic nerve near its branches to the tibial, common peroneal, and gastrocnemius nerves, on postoperative day 3.68
Immunofluorescence
After perfusion, the lumbar spinal cord segments L4–L6 were harvested and sectioned into 10 μm slices. After blocking with 10% goat serum, the slices were incubated overnight at 4°C with various primary antibodies: CD32 (1:1000, #AF4348, Affinity Biosciences), CD206 (1:100, AG2664, Beyotime), Iba-1 (1:500, ab178847, Abcam), VGAT (1:500, sc-166711, HUABIO), and vGluT1 (1:500, ab272913, Abcam). Following washes, the sections were incubated with appropriate fluorescence secondary antibodies for 1 h at room temperature. After rinsing, the sections were mounted. Images were acquired using a laser scanning confocal microscope (Olympus FV3000). For each group, six animals were analyzed, with three non‑consecutive sections per animal. Analysis of the mean fluorescence intensity for microglial polarization markers was performed using Fiji software.69 The number of vGluT1 boutons on CTB-labeled motor neurons, and the ratio of vGluT1 boutons adjacent to vGAT to the total vGluT1 boutons, were counted and calculated manually separately, as described in previous studies.46 All immunofluorescence quantification was performed by an investigator blinded to group allocation.
Western Blotting
Proteins were extracted from the lumbar spine tissues, and the protein concentrations were determined with a BCA assay kit (#23225, Thermo Fisher Scientific). Equal amounts of protein (30 μg per lane) were separated by SDS-PAGE and transferred to PVDF membranes. After blocking with 5% BSA, membranes were incubated overnight at 4°C with the following primary antibodies:anti-CD32 (1:1000, AF4648, Affinity Biosciences), anti-CD206 (1:1000, DF4149, HUABIO), anti-vGAT (1:1000, ab42939, Abcam), anti-vGluT1 (1:2000, ab272913, Abcam), anti-PI3K (1:1000, bs-10657R, Bioss), anti-phospho-PI3K (1:2000, bs-6417R, Bioss), anti-Akt (1:2000, bsm-52010R, Bioss), anti-phospho-Akt (1:2000, bsm-52130R, Bioss), and anti-GAPDH (1:5000, bsm-33033M, Bioss). After incubating with secondary antibodies, images were visualized using an ECL kit (#34096, Thermo Fisher Scientific) and a chemiluminescence imaging system (Liuyi Biotechnology). Each sample was analyzed in triplicate, and band intensity was semi‑quantitatively analyzed using ImageJ software, with GAPDH as the loading control.
RT-qPCR
Total RNA was isolated from the spinal cord tissues of rats using the RNA Easy Fast Tissue/Cell Kit (DP451, Tiangen). Subsequently, one-step reverse transcription and qPCR amplification were performed on a CFX Connect RT-PCR Detection System (Bio-Rad) using the Evo M-MLV One Step RT-PCR Kit (AG11606, Accurate Biology). GAPDH served as the internal control, and the relative gene expression was quantified using the 2^ (−ΔΔCt) method. Primer sequences used are provided in Supplementary Table 2. Each sample was analyzed in triplicate. All primer sequences were validated by melt curve analysis, which showed a single peak for each target gene, and the amplification efficiency of all primers ranged from 90% to 110%.
ELISA
The concentrations of neurotransmitters and inflammatory cytokines in the spinal cord were detected using ELISA kits according to the manufacturers’ instructions. The levels of TNF-α (EK0526, Boster Biological), IL-6 (EK0412, Boster Biological), and TGF-β (EK0514, Boster Biological), IL-10 (EK0418, Boster Biological) were determined to assess neuroinflammation. Meanwhile, the concentrations of the excitatory and inhibitory neurotransmitters, Glutamate (Glu, ZC-141377, Beijing Zhichao Weiye Biotechnology) and Gamma-aminobutyric acid (GABA, ZC-141160, Beijing Zhichao Weiye Biotechnology) were quantified. Absorbance was read at 450 nm using a microplate reader (PerkinElmer Enspire). The levels of all targets were calculated based on their respective standard curves.
Statistical Analyses
Data analyses of the present study were performed using SPSS Statistics 25.0 and GraphPad Prism 9.5.0. One-way ANOVA or two-way repeated-measures ANOVA, with Bonferroni or Tukey post hoc testing, were used appropriately to assess the significance. Data were presented as mean ±SD, and a P value of less than 0.05 was considered statistically significant.
Results
Acupuncture Ameliorated Neurological Deficits, Muscle Spasticity, and Motor Dysfunction and Reduced Infarct Area in MCAO Rats with Spastic Hemiplegia
First, to evaluate the therapeutic effects of acupuncture, behavioral tests were conducted at multiple time points after surgery and the experimental timelines are shown in Figure 1C. All rats exhibited no neurological deficits before surgery. Significant differences were observed over time (F[3,159] = 38.328, P < 0.001), between groups (F[2,53] = 150.528, P < 0.001), and in their interaction (F[6,159] = 67.233, P < 0.001). Except for the sham-operated group, the mNSS scores increased in other three groups on day 3 postoperatively, indicating MCAO-induced neurological deficits. Following intervention, the mNSS scores in the M+AP group decreased significantly (P < 0.001, Figure 1D), demonstrating that acupuncture alleviated neurological deficits following MCAO.
Before surgery, all rats had a comparable MAS score of 0. There was a gradual increase in muscle tone starting from day 3 in the M group, which remained elevated over the following 10 days, consistent with previous findings.21 Significant differences in MAS scores were observed across time points (F[8,46] = 63.212, P < 0.001), between groups (F[2,53] = 13.41, P < 0.001), and in their interaction (F[16,92] = 6.006, P < 0.001). The MAS scores in the M+AP group started to decrease from day 6 post-surgery (p < 0.05, Figure 1E) and continuously declined on day 10 following surgery (P < 0.001), indicating acupuncture’s effect of reducing spasticity induced by MCAO.
No differences in foot-fault rates were observed among the groups prior to modeling. The foot-fault rates began to increase on postoperative day 3 in all groups. Significant differences were observed across time points (F[2,69] = 1431.232, P < 0.001), between groups (F[3,70] = 319.355, P < 0.001), and in their interaction (F[6,138] = 289.807, P < 0.001). On postoperative day 10, the M+AP group showed a significant reduction in foot-fault rate (P < 0.001, Figure 1F), suggesting that acupuncture improved motor coordination after ischemic stroke.
In addition to MAS scoring, we employed swimming test to monitor changes in spasticity of the rat hindlimbs. Swimming spasm scores and spasm frequency showed no differences among all groups at baseline prior to modeling, starting to increase on postoperative day 3. Spasticity scores were significantly influenced by time (F[1,53] = 76.851, P < 0.001), group (F[2,53] = 97.179, P < 0.001), and their interaction (F[2,53] = 184.867, P < 0.001). Following intervention, rats in the M+AP group exhibited a significantly smaller trunk-water surface angle and a marked reduction in spasticity scores (P < 0.001, Figure 1G and H). Significant differences in spasm frequency were observed across time points (F[1,53] = 32.751, P < 0.001), groups (F[2,53] = 30.877, P < 0.001), and their interaction (F[2,53] = 39.152, P < 0.001). Spasm frequency significantly decreased in the M+AP group following intervention as well (P < 0.001, Figure 1I). These results suggested that acupuncture resisted MCAO-induced increased muscle tone.
TTC staining exhibited distinct infarct lesions in all groups except the sham-operated group (F[2,15] = 73.27, P < 0.001). Results revealed that, after acupuncture, the infarct area in the M+AP group rats was significantly reduced compared to the M group on day 10 following surgery (P < 0.001, Figure 1J and K), indicating that acupuncture reduced cerebral injury after ischemia.
In contrast, the M+CP group showed no significant differences from the M group at any time point for all of these indicators (all P > 0.05). This suggested that acupuncture at a control non-acupoint was unable to perform the above effects.
Acupuncture Decreased Spinal Excitability in MCAO Rats with Spastic Hemiplegia
We further evaluated the effect of acupuncture on spinal hyperexcitability through objective recording of the H-reflex. Supplementary Table 3 summarizes the characteristics of H-reflex of each group. There were significant differences in Hmax/Mmax ratios among groups (F(3,70) = 273.2, P < 0.001). The results showed that acupuncture intervention at GB34 significantly decreased the Hmax/Mmax ratios (P < 0.001; Figure 1L). Generally, in post-stroke spasticity, FDD of the H-reflex is typically impaired, defined by sustained high Hmax/Mmax ratios across different stimulation frequencies.70 There were significant differences in FDD of the H-reflex under different stimulation frequencies (F[1,70] = 310.639, P < 0.001). The effects of different groups on FDD were also statistically significant (F[3,70] = 1179.863, P < 0.001). Meanwhile, the interaction between stimulation frequency and group was also statistically significant (F[3,70] = 38.724, P < 0.001). The FDD in the M+AP group showed significant improvement at both 5 Hz and 10 Hz stimulation (both P < 0.001; Figure 1M and N). In contrast, the M+CP group showed no significant effects on any of these parameters (all P > 0.05). The above findings indicated that acupuncture at GB34 effectively reduced motor neuron excitability and promoted spinal reflex regulation, whereas acupuncture at the control non-acupoint was ineffective.
Acupuncture Shifted Spinal Microglia Toward the M2 Phenotype and Modified Spinal Inflammation Milieu in MCAO Rats with Spastic Hemiplegia
We subsequently aimed to clarify whether the polarization state of spinal microglia was associated with above therapeutic effects of acupuncture on spastic hemiplegia induced by MCAO. Mean fluorescence intensity, mRNA expression, and protein expression of CD32 (F[3,20] = 127.6; F[3,20] = 147.9; F[3,20] = 791.7, all P < 0.001) and CD206 F[3,20] = 112.8; F[3,20] = 346.9; F[3,20] = 385.5, all P < 0.001) all showed significant differences among the four groups. IF analysis showed that acupuncture significantly decreased the mean fluorescence intensity of the CD32/Iba-1 cells (P < 0.001; Figure 2A and C) while increasing that of the CD206/Iba-1 cells (P < 0.001; Figure 2B and D). RT-qPCR and WB results confirmed that acupuncture concurrently suppressed mRNA and protein expression of the CD32 and up-regulated those of the CD206 (all P < 0.001; Figure 2I–K and 2–Q). Meanwhile, the spinal cord levels of TNF‑α, IL‑6, TGF‑β, and IL‑10 in the four groups measured by ELISA differed significantly (F[3,20] = 359.1; F[3,20] = 149.3; F[3,20] = 314.1; F[3,20] = 132.0, all P < 0.001). ELISA results demonstrated that acupuncture significantly reduced pro-inflammatory cytokine (TNF-α, IL-6) levels and conversely elevated anti-inflammatory factor (TGF-β, IL-10) levels (all P < 0.001; Figure 2R–U). No significant difference was observed in these indicators between the M group and the M+CP group (all P > 0.05). These results suggested that acupuncture at GB34 drove microglia polarization toward the M2 anti-inflammatory phenotype, thereby alleviating the spinal inflammatory milieu, while acupuncture at the control non-acupoint failed to exert such effects.
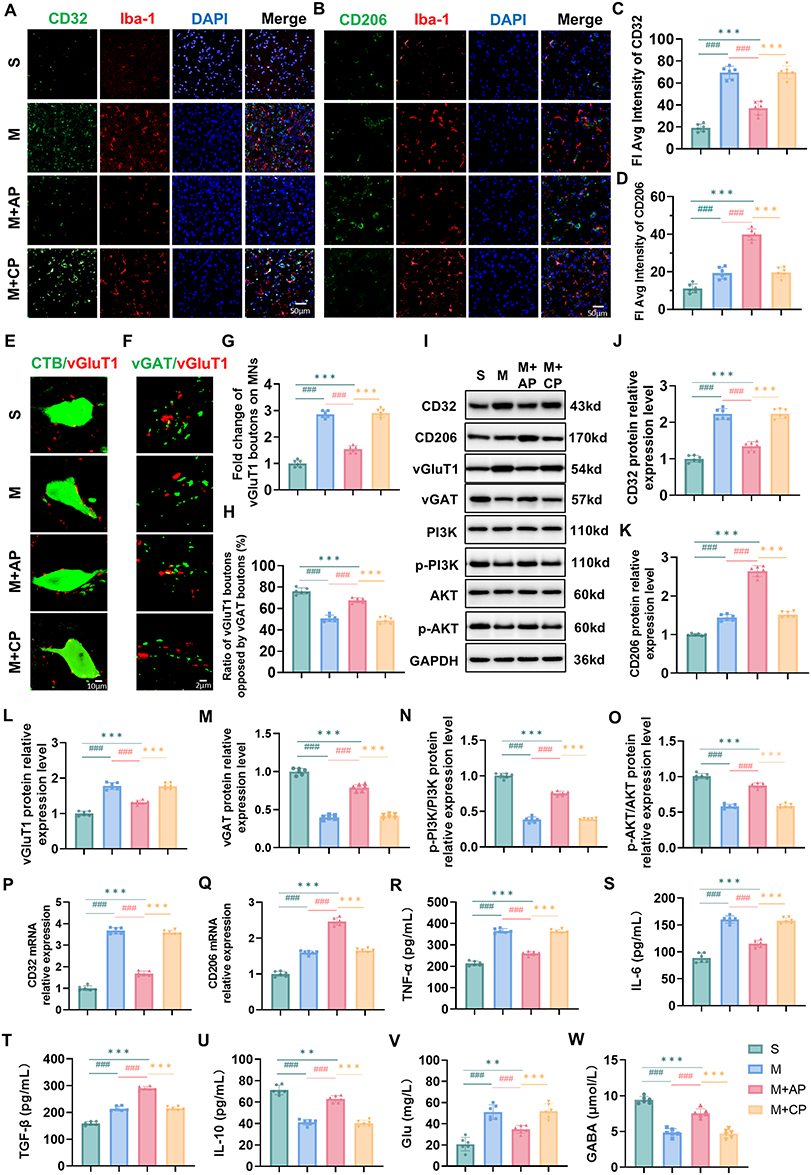 |
Figure 2 Acupuncture shifted spinal microglia toward the M2 phenotype, modified spinal inflammation milieu, restored the E/I balancing in the spinal motor circuit and activated the spinal PI3K/Akt pathway in MCAO rats with spastic hemiplegia. Immunofluorescence of microglial polarization state: representative images of CD32 (M1 marker, green) and Iba-1 (microglial marker, red) co-localization by immunofluorescence (A); representative images of CD206 (M2 marker, green) and Iba-1 (red) co-localization by immunofluorescence (B) with all nuclei of cells stained by DAPI (blue); scale bar, 50 μm; the semi-quantitative fluorescent intensity results of CD32 (C) and CD206 (D). Immunofluorescence of synaptic boutons in motor circuit: representative images of vGluT1 immunoreactive boutons (marking the proprioceptive terminals, red) on CTB-labeled motor neurons (MNs, green) (E); representative images of vGluT1 boutons (red) contacting vGAT immunoreactive boutons (marking GABAergic synapses, green) (F); scale bar, 10 μm, 2 μm; fold change of vGluT1 boutons on MNs (G); ratio of vGluT1 boutons opposed by vGAT boutons (H). Representative Western blot bands (I) and quantitative results for CD32 (J), CD206 (K), vGluT1 (L), vGAT (M), p-PI3K/PI3K (N), and p-Akt/Akt (O) protein expressions relative to GAPDH protein. The mRNA levels of CD32 (P) and CD206 (Q) were detected by RT-qPCR. The concentrations of TNF-α (R), IL-6 (S), TGF-β (T), IL-10 (U), Glu (V), GABA (W) were detected by ELISA. N = 6 per group. Data were expressed as mean ± SD. **P<0.01,***P<0.001 versus M+AP group; ###P<0.001 versus M group. |
Acupuncture Restored the E/I Balancing in the Spinal Motor Circuit of MCAO Rats with Spastic Hemiplegia
To investigate how acupuncture modulates excitatory input to spinal motor neurons, we labeled and analyzed relevant synaptic boutons of the motor circuit by immunofluorescence. Significant differences were observed in both the number of vGluT1-positive excitatory synapses (F[3,20] = 293, P < 0.001) and the proportion of vGluT1 synaptic boutons adjacent to vGAT (F[3,20] = 126.3, P < 0.001) in the spinal cord among the four groups. Results showed that after MCAO, VGluT1 immunoreactive boutons (marking the proprioceptive terminals) on CTB-labeled motor neurons were significantly increased (P < 0.001; Figure 2E, and Supplementary Figure 1), whereas VGluT1 boutons contacting vGAT immunoreactive boutons (marking GABAergic synapses) were markedly reduced (P < 0.001; Figure 2F, and Supplementary Figure 2). Acupuncture effectively reversed these abnormalities, significantly reducing the excessive proprioceptive afferents (P < 0.001; Figure 2E and G) and enhancing presynaptic inhibition (P < 0.001; Figure 2F and H). Furthermore, WB and ELISA results showed that the relative expression levels of vGluT1 and vGAT (F[3,20] = 142.2; F[3,20] = 393.2, all P < 0.001) as well as the concentrations of Glu and GABA (F[3,20] = 35.42; F[3,20] = 96.29, all P < 0.001) in the spinal cord were significantly different among the four groups. Acupuncture downregulated the vGluT1 protein expression and the concentration of the excitatory neurotransmitter Glu (P < 0.001; Figure 2I, and V), while simultaneously upregulating the vGAT protein expression and the concentration of the inhibitory neurotransmitter GABA (P < 0.001; Figure 2I, and W). Compared with the M group, the M+CP group showed no significant differences in the above indicators (all P > 0.05). The above results indicated that acupuncture at GB34 restored the E/I balance in the spinal motor circuit. While acupuncture at the control non-acupoint produced none of these effects.
Acupuncture Activated the PI3K/Akt Pathway in the Spinal Cord of MCAO Rats with Spastic Hemiplegia
To explore the mechanism by which acupuncture promotes M2 polarization, we examined the PI3K/Akt pathway. The relative protein expression levels of p‑PI3K and p‑AKT showed significant differences among groups (F[3,20] = 514.7; F[3,20] = 242.1, both P < 0.001). WB results showed that MCAO significantly suppressed the expression of p-PI3K and p-Akt (both P < 0.001; Figure 2I, and O). In contrast, acupuncture intervention effectively reversed this trend, significantly increasing the phosphorylation levels of both proteins (both P < 0.001), indicating that acupuncture activates the PI3K/Akt pathway in vivo. No such effect was observed in the M+CP group (both P > 0.05), suggesting that acupuncture at the control non-acupoint failed to activate this pathway.
Inhibition M1 Polarization of Spinal Microglia Partially Reproduced the Benefits of Acupuncture on Enhancing Motor Recovery and Reducing Spinal Hyperexcitability in MCAO Rats with Spastic Hemiplegia
To verify whether inhibiting M1 polarization of spinal microglia is a key mechanism underlying acupuncture’s effects, we administered minocycline to MCAO rats (Figure 3A) and the experimental timelines are shown in Figure 3B. Behavioral results showed that, compared with the M group, minocycline significantly improved neurological deficit scores (all P < 0.001; Figure 3C), reduced muscle tone (all P < 0.05; Figure 3D), and decreased the foot-fault rate (P < 0.001; Figure 3E), swimming spasticity score (P < 0.001; Figure 3F and H, and spasticity frequency (P < 0.001; Figure 3G). Electrophysiological results indicated that minocycline lowered the Hmax/Mmax ratio (P < 0.001; Figure 3I) and improved FDD at 5Hz and 10Hz (both P < 0.001; Figure 3J and K). No significant difference was observed in these indicators between the M+veh group and the M group at any time point (all P > 0.05). These results demonstrated that inhibiting M1 polarization could mimic the effect of acupuncture in improving post-stroke functional recovery, whereas the vehicle had no impact on this effect.
 |
Figure 3 Inhibition of M1 polarization of spinal microglia partially reproduced the therapeutic benefits of acupuncture on enhancing motor recovery and reducing spinal hyperexcitability in MCAO rats with spastic hemiplegia. (A) Experimental Intervention Diagram. (B) Experimental procedures. MC, minocycline hydrochloride; Veh, vehicle. (C) mNSS for neurologic deficits assessments. (D) MAS for muscle tension evaluations. (E) Foot fault test for motor coordination assessments. Swimming test for lower limb spasticity evaluations: spasm scores (F); spasm frequency (G); representative pictures (H). H-reflex for spinal excitability assessments: Hmax/Mmax ratio (I); FDD (J) and representative traces recorded at 0.3 Hz, 5 Hz, and 10 Hz (K). S (sham-operated) group (n = 18), M (model) group (n = 19), M+MC (model + minocycline hydrochloride) group (n = 20), M+Veh (model + vehicle) group (n = 18). Data were expressed as mean ± SD. *P<0.05, **P<0.01, ***P<0.001 versus M+MC group; ###P<0.001 versus M group. |
Inhibition of M1 Polarization of Microglia Mitigated Spinal Inflammatory Milieu and Facilitated the Restoration of Spinal E/I Balance in MCAO Rats with Spastic Hemiplegia
To confirm the specific inhibitory effect of minocycline on M1 polarization, we assessed related indicators following minocycline intervention. IF, Western blot, and RT-qPCR results consistently demonstrated that minocycline specifically suppressed CD32 expressions (P < 0.001; Figure 4A and N) and promoted CD206 expressions (P < 0.001; Figure 4B and O) compared with the M group, accompanied by decreased TNF-α, IL-6 levels and increased TGF-β, IL-10 levels (all P < 0.001; Figure 4P–S). The aforementioned outcomes in the M+Veh group were not different from those of the M group (P > 0.05), demonstrating that minocycline effectively inhibited microglia M1 polarization and ameliorated the spinal inflammatory milieu, while the vehicle was unable to exert this effect.
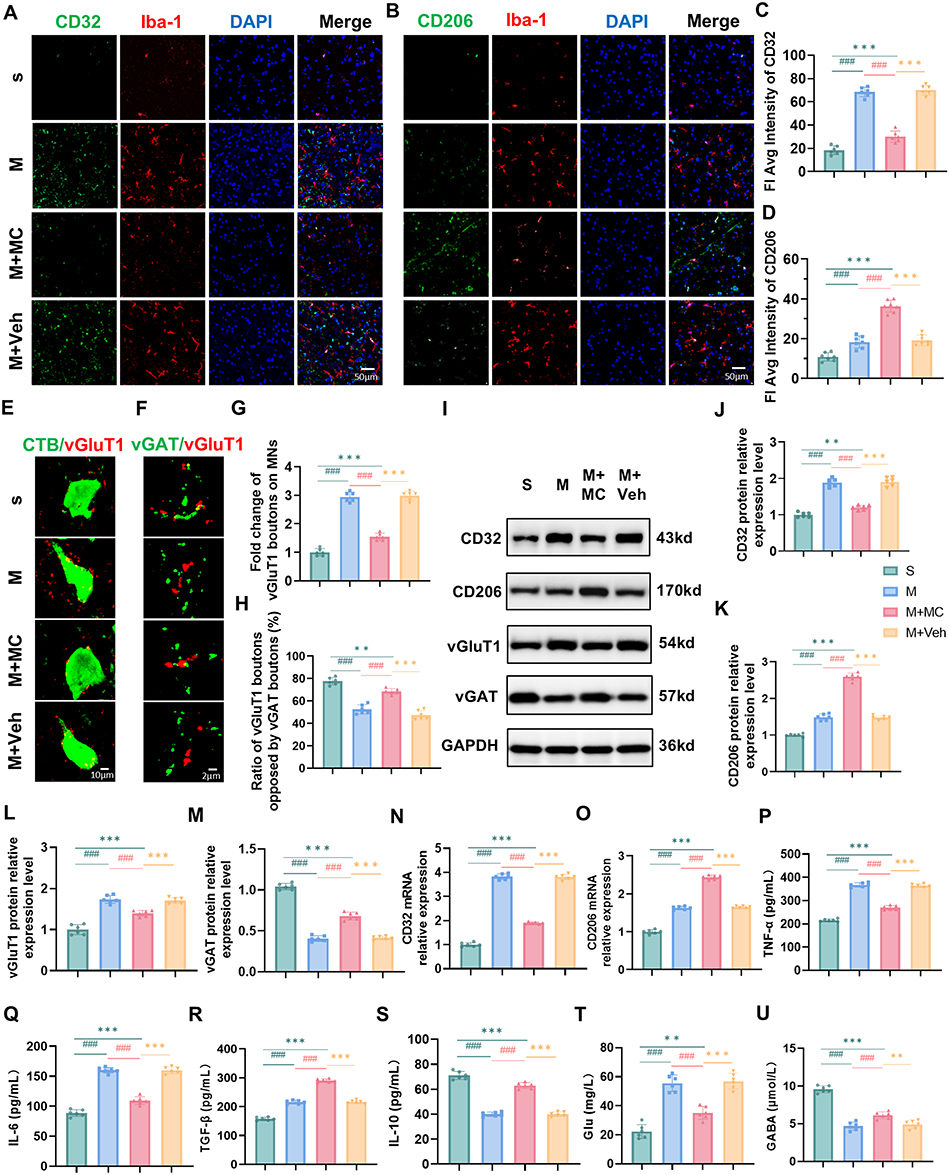 |
Figure 4 Inhibition of M1 polarization of microglia mitigated spinal inflammatory milieu and facilitated the restoration of spinal E/I balance in MCAO rats with spastic hemiplegia. Immunofluorescence of microglial polarization state: representative images of CD32 (green) and Iba-1 (red) co-localization by immunofluorescence (A) representative images of CD206 (green) and Iba-1 (red) co-localization by immunofluorescence (B) with all nuclei of cells stained by DAPI (blue); scale bar, 50 μm; the semi-quantitative fluorescent intensity results of CD32 (C) and CD206 (D). Immunofluorescence of synaptic boutons in motor circuit: representative images of vGluT1 immunoreactive boutons (red) on CTB-labeled MNs (green) (E) representative images of vGluT1 boutons (red) contacting vGAT immunoreactive boutons (green) (F) scale bar, 10 μm, 2 μm; fold change of vGluT1 boutons on MNs (G) ratio of vGluT1 boutons opposed by vGAT boutons (H). Representative Western blot bands (I) and quantitative results for CD32 (J) CD206 (K) vGluT1 (L) vGAT (M) protein expression relative to GAPDH protein. The mRNA levels of CD32 (N) and CD206 (O) were detected by RT-qPCR. The concentrations of TNF-α (P) IL-6 (Q) TGF-β (R) IL-10 (S) Glu (T) GABA (U) were detected by ELISA. N = 6 per group. Data were expressed as mean ± SD. **P<0.01, ***P<0.001 versus M+MC group; ###P<0.001 versus M group. |
To investigate whether inhibition of microglial M1 polarization modulates E/I balance in the spinal motor circuit, we assessed the relevant indicators. Results showed that minocycline reduced abnormal excitatory input to motor neurons, as evidenced by decreased vGluT1 immunoreactive boutons on Motor Neurons (MNs) and increased vGluT1 immunoreactive boutons adjacent to vGAT immunoreactive boutons (both P < 0.001; Figure 4E–H and Supplementary Figures 3, 4). In addition, it downregulated the vGluT1 protein expression and decreased the Glu concentration (both P < 0.001; Figure 4L and T), upregulated the vGAT protein expression and increased the GABA concentration (both P < 0.001; Figure 4M and U). None of these effects were observed in the M+Veh group (all P > 0.05). These data showed that minocycline effectively reversed MCAO-induced E/I imbalance in the spinal cord, while the vehicle had no effect.
Acupuncture Alleviated Post-Stroke Spastic Hemiplegia by Promoting Spinal Microglial M2 Polarization via the PI3K/Akt Signaling Pathway
To determine the role of the PI3K/Akt signaling pathway in acupuncture-mediated improvement of post-stroke spastic hemiplegia, we administered the pathway inhibitor LY294002 and agonist 740Y-P, and the experimental timelines are shown in Figure 5A. Behavioral and electrophysiological results demonstrated that acupuncture significantly improved neurological function, reduced muscle spasticity, restored motor dysfunction, and decreased spinal excitability (all P < 0.001; Figure 5B–J). While the M+AP+LY group still showed better outcomes than the M+Veh group (all P < 0.01), the effects were partially suppressed compared to the M+AP+Veh group (all P < 0.01). Administration of the agonist 740Y-P also improved these indexes, though its effects were weaker than those in the M+AP+Veh group (all P < 0.01), suggesting that the PI3K/Akt pathway is critical for the therapeutic effects of acupuncture. There were no significant differences between the M+Veh group and the M group in any of the above indicators (all P > 0.05), showing that the vehicle did not influence these effects.
 |
Figure 5 The PI3K/Akt pathway played an essential role in acupuncture-induced post-stroke spastic hemiplegia recovery. (A) Experimental procedures. LY, LY294002. (B) mNSS for neurologic deficits assessments. (C) MAS for muscle tension evaluations. (D) Foot fault test for motor coordination assessments. Swimming test for lower limb spasticity evaluations: spasm scores (E) spasm frequency (F) representative pictures (G). H-reflex for spinal excitability assessments: Hmax/Mmax ratio (H) FDD (I) and representative traces recorded at 0.3 Hz, 5 Hz, and 10 Hz (J). S (sham-operated) group (n = 18), M+AP+LY (model + acupuncture point + LY294002) group (n = 19), M+AP+Veh (model + acupuncture point + vehicle) group (n = 19), M+Veh (model + vehicle) group (n = 20), M+740Y-P (model + 740Y-P) group (n = 18). Data were expressed as mean ± SD. *P<0.05, **P<0.01, ***P<0.001 versus M+AP+Veh group; #P<0.05, ##P<0.01, ###P<0.001 versus M+Veh group. |
Molecular results further revealed that acupuncture significantly suppressed M1 microglial marker and pro-inflammatory factors while promoting M2 microglial marker and anti-inflammatory factors (all P < 0.001; Figures 6A–D and 7A–G, 7–O). LY294002 partially blocked this regulatory effect, whereas 740Y-P partially mimicked it, albeit with weaker efficacy than acupuncture (all P < 0.001). In addition, acupuncture effectively reduced the abnormal excitatory input of proprioceptive sensory information to MNs, enhanced the presynaptic inhibition, downregulated the excitatory neurotransmitter level, and elevated the inhibitory neurotransmitter level (all P < 0.001; Figure 7A–E, H–I, P–Q and Supplementary Figure 5, 6). These effects were also partially inhibited by LY294002 (all P < 0.001) and partially reproduced by 740Y-P (all P < 0.01). No significant difference was observed between the M+Veh group and M group in any of these results (all P > 0.05), indicating that the vehicle had no effect on the above outcomes.
 |
Figure 6 Acupuncture promoted spinal microglial M2 polarization via PI3K/Akt pathway in MCAO rats with spastic hemiplegia. Immunofluorescence of microglial polarization state: representative images of CD32 (green) and Iba-1 (red) co-localization by immunofluorescence (A); representative images of CD206 (green) and Iba-1 (red) co-localization by immunofluorescence (B) with all nuclei of cells stained by DAPI (blue); scale bar, 50 μm, 10μm; the semi-quantitative fluorescent intensity results of CD32 (C) and CD206 (D). Data were expressed as mean ± SD. ***P<0.001 versus M+AP+Veh group; ###P<0.001 versus M+Veh group. |
 |
Figure 7 Acupuncture mitigated excitability of spinal motor circuits and inflammatory milieu via PI3K/Akt pathway in MCAO rats with spastic hemiplegia. Immunofluorescence of synaptic boutons in motor circuit: representative images of vGluT1 immunoreactive boutons (red) on CTB-labeled MNs (green) (A); representative images of vGluT1 boutons (red) contacting vGAT immunoreactive boutons (green) (B); scale bar, 10 μm, 2 μm; fold change of vGluT1 boutons on MNs (C); ratio of vGluT1 boutons opposed by vGAT boutons (D). Representative Western blot bands (E) and quantitative results for CD32 (F) CD206 (G) vGluT1 (H) vGAT (I) protein expression relative to GAPDH protein. The mRNA levels of CD32 (J) and CD206 (K) were detected by RT-qPCR. The concentrations of TNF-α (L) IL-6 (M) TGF-β (N) IL-10 (O) Glu (P) GABA (Q) were detected by ELISA. N = 6 per group. Data were expressed as mean ± SD. ***P<0.001 versus M+AP+Veh group; ##P<0.01, ###P<0.001 versus M+Veh group. |
Discussion
Our study demonstrates that the MCAO rat with spastic hemiplegia exhibits high muscle tone, severe neurological deficits, spinal reflex hyperactivity, and motor dysfunction, accompanied by polarization of spinal microglia towards the M1 pro-inflammatory phenotype, abnormally increased excitation of proprioceptive afferents on motoneurons, an imbalance between Glu and GABA, and suppressed activity of the PI3K/Akt pathway. The polarization state of microglia is closely associated with the therapeutic efficacy of acupuncture. Acupuncture may promote the polarization of spinal microglia towards the M2 anti-inflammatory phenotype by activating the PI3K/Akt signaling pathway, restore normal excitatory input from proprioceptive afferents to motoneurons, and correct the Glu/GABA imbalance, thereby reducing spinal hyperexcitability, alleviating limb spasticity, and facilitating the recovery of motor function after stroke (Figure 8).
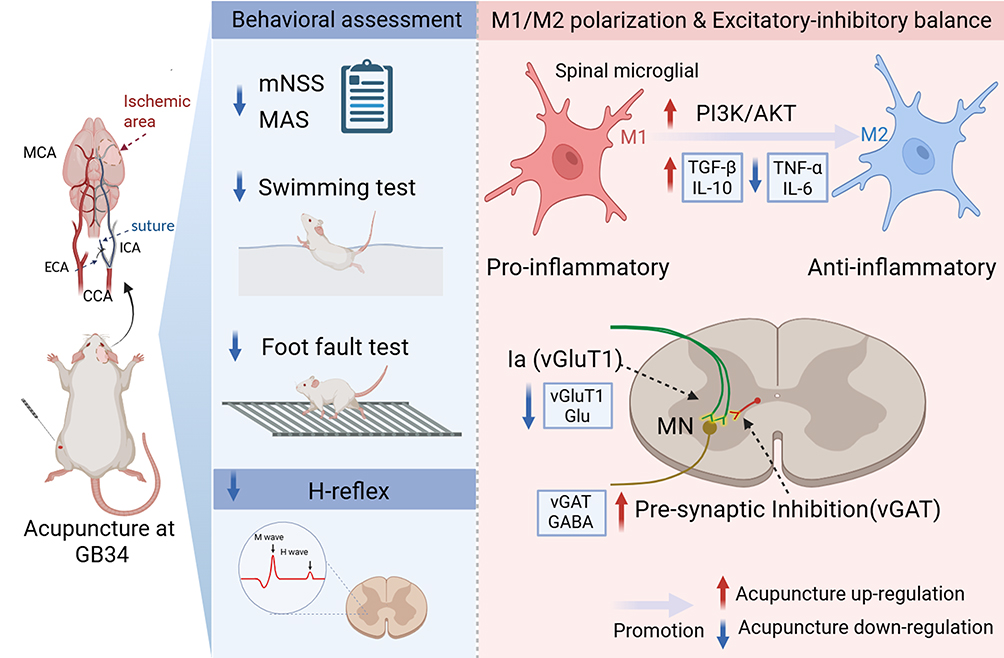 |
Figure 8 Schematic diagram of the mechanism of acupuncture alleviates spastic hemiplegia following ischemic stroke. Acupuncture at GB34 ameliorates post-stroke spastic hemiplegia by activating the PI3K/Akt pathway, promoting spinal M2 microglial polarization, mitigating spinal inflammatory milieu, and restoring spinal excitatory/inhibitory equilibrium, which would provide evidence for acupuncture’s immunomodulatory role in post-stroke functional recovery. |
Microglia exert a pivotal role in initiating inflammatory responses in the post-ischemic inflammatory response.71 Strong evidence indicates that post-ischemic Wallerian degeneration can extend along the corticospinal tract to the spinal cord, which induces early microglial activation and triggers secondary inflammatory responses. This process is strongly associated with poor long-term motor recovery after stroke.72,73 Therefore, this study focused on inflammatory regulation mechanisms at the spinal level. Microglia exhibit a dual role following stroke, exerting both neuroprotective effects and exacerbating neuronal damage, which is a characteristic closely associated with their multi-phenotypic polarization.74 Therefore, blanket inhibition may hinder the repair process, whereas specific targeted modulation holds greater therapeutic value. This study focuses on the inflammatory regulatory mechanisms at the spinal cord level, elucidating for the first time the mechanism by which acupuncture induces polarization of spinal microglia toward the M2 anti-inflammatory phenotype, thereby ameliorating post-stroke spastic hemiplegia.
Acupuncture is a safe, simple, and multi-target therapy whose efficacy in improving post-stroke functional recovery has been clinically validated.75 GB34, a standard point for lower limb spasticity, demonstrated treatment specificity in our study, as control non-acupoint needling produced no comparable benefit. In rats, GB34 is located in the lateral lower leg and is mainly innervated by the common peroneal nerve, with afferent projections projecting to the spinal segments.76 Waggle needling at GB34 activates somatic afferent fibers, which convey peripheral sensory signals into the spinal dorsal horn of the lumbar enlargement. This afferent transmission pathway establishes the anatomical basis of the skin-spinal cord axis, through which acupuncture may modulate downstream spinal microglia, synaptic plasticity, and neuroinflammation.
Although prior work implies that microglial polarization may be involved, our study provides direct evidence of a spinal mechanism. In MCAO rats with spastic hemiplegia, we found a pro-inflammatory spinal environment dominated by M1 microglia and hyperexcitability. In this study, we found that acupuncture effectively reversed these abnormalities, and observed elevated levels of M2 polarization-associated factors, including IL-10 and TGF-β, which modulates excitatory and inhibitory transmission and counteracts synaptic dysfunction.77–79 The parallel findings following minocycline treatment further underscore the central role of spinal microglial polarization in post-stroke spasticity recovery.
Previous studies have shown that ischemic stroke leads to decreased p-PI3K and p-Akt expression associated with neurological injuries and inflammation, while PI3K/Akt pathway activation can mitigate neuroinflammation.80,81 Furthermore, this pathway regulates microglial M1/M2 polarization through the Akt protein, and its inhibition promotes M1 phenotypic switching, confirming its crucial role in polarization.82,83 In present study, we further validated the key role of this signaling pathway in acupuncture treatment for MCAO-induced spastic hemiplegia using both PI3K/Akt inhibitors and agonists. Our results demonstrated that acupuncture effectively activates this pathway, whereas the specific inhibitor LY294002 partially blocked acupuncture’s therapeutic effects. Meanwhile, the agonist 740Y-P could only partially mimic the effects of acupuncture. Although the present study highlights the pivotal role of PI3K/Akt signaling in acupuncture-induced spinal microglial M2 polarization, acupuncture is widely considered a multi-target intervention, and its anti-inflammatory effects are unlikely to depend on a single pathway alone. Previous studies have shown that acupuncture can also modulate NF-κB- and MAPK-related signaling in ischemic stroke models, thereby suppressing microglia-mediated neuroinflammation and reducing pro-inflammatory cytokine production.44,84–86 These pathways may interact with PI3K/Akt signaling and together contribute to the regulation of microglial polarization and neural circuit remodeling after stroke. Therefore, in addition to PI3K/Akt, potential complementary pathways such as NF-κB and MAPK deserve further investigation in future studies.
The normal function of spinal motor circuit depends on balanced glutamatergic excitation and GABAergic/glycinergic inhibition, particularly presynaptic GABAergic control over primary afferent inputs.87 However, after stroke, the compensatory enhancement of proprioceptive input,88,89 combined with weakened inhibitory control,90 disrupts this E/I homeostasis, leading to spinal hyperexcitability and facilitating post-stroke spastic hemiplegia development. Studies demonstrate that vGluT1 expression levels exhibit a positive correlation with presynaptic terminal Glu release into the synaptic cleft, and its upregulation enhances excitatory neurotransmission.91 Meanwhile, the vGAT fulfills analogous vesicular loading and release functions within the inhibitory GABA system. Neuroinflammation milieu after stroke further compromises GABAergic function by altering synthesis and release of GABA receptors, while simultaneously promoting aberrant glutamate release, thereby exacerbating excitotoxicity and collectively disrupting spinal motor circuit E/I balance.92,93 Our findings reveal that acupuncture intervention improves the spinal inflammatory microenvironment, downregulates vGluT1 expression to reduce synaptic Glu levels, and upregulates vGAT protein expression to restore GABAergic inhibitory function. These results provide evidence for understanding the mechanism by which acupuncture modulates E/I balance in spinal motor circuit.
Concurrently, our electrophysiological H-reflex data also demonstrated that acupuncture normalized motor neuron hyperexcitability induced by ischemic stroke, rather than suppressing neuronal excitability below physiological levels. This normalization may support synaptic functional remodeling, as evidenced by our present observation of significant increase in the proportion of vGlutT1 boutons inhibited by vGAT boutons around motor neurons. These findings align with the contemporary consensus that precise regulation of E/I balance is essential for post-stroke neuroplasticity.94
Several studies demonstrated that acupuncture, exerted advantages in immunomodulation of inflammation by activating somato-autonomic immune reflexes, since it is a minimally invasive peripheral nerve stimulation technique.95 In this animal model study, the application of motion-style waggle needling technique at the GB34 effectively alleviated post-stroke lower limb spasticity and motor deficits. The underlying mechanism may involve the creation of an anti-inflammatory microenvironment conducive to synaptic remodeling through promoting microglial M2 polarization by acupuncture. Although acupuncture may exert anti-spastic effects via multi-target mechanisms, the findings of present study demonstrate that PI3K/Akt pathway-mediated anti-inflammatory regulation could represent a potential key node. These findings may guide the design of future clinical trials by stratifying patients according to PI3K/Akt pathway activity, thereby enabling the identification of subpopulations most likely to benefit from acupuncture. In addition, comparing acupuncture administered at GB34 alone versus combined with other acupoints may help clarify the optimal therapeutic regimen for post-stroke spasticity. Additionally, this study used fixed acupuncture frequency and duration. Future research should explore dose-response effects, specifically whether increased frequency or prolonged duration enhances spinal microglial polarization and functional recovery, to define optimal acupuncture parameters for stroke rehabilitation. Future studies are also warranted to explore dose‑response relationships regarding acupuncture frequency and duration, as well as the long‑term effects and synergistic efficacy of acupuncture combined with physical therapy or pharmacological interventions. Moreover, incorporating standardized sham/placebo acupuncture controls and extending the work to more clinically relevant human‑based models will help clarify the specific needling effects and further enhance translational value.
Collectively, these results provide a novel paradigm for developing an integrated “immunomodulation-neuroremodeling” therapeutic strategy against post-stroke spastic hemiplegia, offering new perspectives to optimize current symptom-oriented approaches and improve motor rehabilitation protocols for stroke patients.
Several limitations of the present study should be considered. First, MAS scoring was done independently by two blinded investigators with a standardized protocol, but formal inter-rater reliability analysis was not performed and it will be added in future work to enhance behavioral assessment validity. Although we have identified the pivotal role of the PI3K/Akt signaling pathway in acupuncture-induced M2 polarization of spinal microglia, the downstream effector molecules remain to be elucidated. Additionally, although LY294002 and 740Y-P were administered at doses consistent with previous studies, their spinal cord tissue concentrations were not directly measured, and future studies should validate drug exposure and pharmacokinetics in the spinal cord. Moreover, the translational significance of the present findings should be interpreted cautiously. Species differences in microglia and neuroinflammation between rodents and humans may limit their clinical translation. The standardized acupuncture used in this preclinical study also differs from individualized clinical treatment. Further clinical studies are therefore warranted to validate these findings. To minimize sex hormone-related variability, only male rats were used, but this limits the generalizability of the findings, as stroke affects both sexes, and acupuncture effects may vary by sex.96,97 Future research should explore potential sex-dependent effects by including female animals.
Conclusion
In conclusion, our study demonstrates that acupuncture at GB34 alleviates post-stroke spastic hemiplegia by activating the PI3K/Akt pathway, promoting spinal M2 microglial polarization, mitigating the spinal inflammatory milieu, and restoring spinal excitatory/inhibitory equilibrium. Notably, the efficacy was specific to GB34, while non-acupoint needling showed no comparable effect, supporting the critical role of acupoint specificity. This study provides a preclinical basis for clinical trials of acupuncture at GB34 for post-stroke spasticity and identifies PI3K/Akt as a potential adjunctive therapeutic target. Future studies are warranted to clarify optimal acupuncture parameters, long-term efficacy, and synergistic effects with other interventions, while investigating complementary pathways to PI3K/Akt, validating findings in female animals, and translating these results to human-based models to strengthen clinical relevance and broader application.
Abbreviations
MCAO, middle cerebral artery occlusion; IL-1, interleukin-1;IL-6, interleukin-6; TNF-α, tumor necrosis factor-alpha; IL-4, interleukin-4; IL-10, interleukin-10; TGF-β, transforming growth factor-beta; PI3K/Akt, phosphoinositide 3-kinase/protein kinase B; E/I, excitatory-inhibitory; SD, standard deviation; SMD, standardized mean difference; M, model; AP, acupoint; CP, control non-acupoint; MC, minocycline hydrochloride; Veh, vehicle; LY, LY294002; p-MCAO, permanent middle cerebral artery occlusion; CBF, cerebral blood flow; GB34, Yanglingquan; mNSS, Modified Neurological Severity Score; MAS, Modified Ashworth Scale; FDD, frequency-dependent depression; TTC, 2,3,5-triphenyltetrazolium chloride; CTB, Cholera Toxin Subunit B; Glu, Glutamate; GABA, Gamma-aminobutyric acid; MNs, Motor Neurons.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
Ling-Hui Ma: Methodology, Formal analysis, Investigation, Writing-Original Draft, Visualization. Liang-Xiao Ma: Conceptualization, Funding acquisition, Supervision, Writing-Review & Editing. Xu Qian, Jing-Yun Xiu, Meng-Yu Chen: Methodology, Investigation, Writing-Review & Editing. Jia-Ling He: Validation, Writing-Review & Editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (grant number 82274655).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu J, Xu A, Zhao Z, et al. Epidemiology and future trend predictions of ischemic stroke based on the global burden of disease study 1990–2021. Commun Med. 2025;5(1):273. doi:10.1038/s43856-025-00939-y
2. Wang J, Xiao C, Cheng Z, Liu H, Zhang W, Yu C. Analysis and prediction of disease burden of stroke and its subtypes in China from 1990 to 2040. Chin Med J. 2025;138(19):2452–22. doi:10.1097/CM9.0000000000003725
3. Xu Y, Hu W, Chen X, et al. Maintaining balance: an update on nonpharmacological cytoprotection therapy for acute ischemic stroke. Stroke. 2025;56(10):e240–e253. doi:10.1161/STROKEAHA.125.051589
4. Glaess-Leistner S, Ri SJ, Audebert HJ, Wissel J. Early clinical predictors of post stroke spasticity. Top Stroke Rehabil. 2021;28(7):508–518. doi:10.1080/10749357.2020.1843845
5. Wissel J, Manack A, Brainin M. Toward an epidemiology of poststroke spasticity. Neurology. 2013;80(3_supplement_2):S13–19. doi:10.1212/WNL.0b013e3182762448
6. Chan TY, Ma BD, Hung TK, Wong JSY, Lo BW. Microglial polarization and therapeutic strategies in post-stroke neuroinflammation. Neurol Ther. 2025;14(6):2277–2293. doi:10.1007/s40120-025-00825-8
7. Hu X, Leak RK, Shi Y, et al. Microglial and macrophage polarization—new prospects for brain repair. Nat Rev Neurol. 2015;11(1):56–64. doi:10.1038/nrneurol.2014.207
8. Zeng J, Bao T, Yang K, et al. The mechanism of microglia-mediated immune inflammation in ischemic stroke and the role of natural botanical components in regulating microglia: a review. Front Immunol. 2023;13:1047550. doi:10.3389/fimmu.2022.1047550
9. Petralla S, De Chirico F, Miti A, et al. Epigenetics and communication mechanisms in microglia activation with a view on technological approaches. Biomolecules. 2021;11(2):306–333. doi:10.3390/biom11020306
10. Zhao JF, Ren T, Li XY, Guo TL, Liu CH, Wang X. Research progress on the role of microglia membrane proteins or receptors in neuroinflammation and degeneration. Front Cell Neurosci. 2022;16:831977. doi:10.3389/fncel.2022.831977
11. Qiao C, Liu Z, Qie S. The implications of microglial regulation in neuroplasticity-dependent stroke recovery. Biomolecules. 2023;13(3):571. doi:10.3390/biom13030571
12. Wang H, Li J, Zhang H, et al. Regulation of microglia polarization after cerebral ischemia. Front Cell Neurosci. 2023;17:1182621. doi:10.3389/fncel.2023.1182621
13. Lu Y, Zhou M, Li Y, Li Y, Hua Y, Fan Y. Minocycline promotes functional recovery in ischemic stroke by modulating microglia polarization through STAT1/STAT6 pathways. Biochem Pharmacol. 2021;186:114464. doi:10.1016/j.bcp.2021.114464
14. Jiang YQ, Sarkar A, Amer A, Martin JH. Transneuronal downregulation of the premotor cholinergic system after corticospinal tract loss. J Neurosci. 2018;38(39):8329–8344. doi:10.1523/JNEUROSCI.3410-17.2018
15. Toda T, Ishida K, Kiyama H, Yamashita T, Lee S. Down-regulation of KCC2 expression and phosphorylation in motoneurons, and increases the number of in primary afferent projections to motoneurons in mice with post-stroke spasticity. PLoS One. 2014;9(12):e114328. doi:10.1371/journal.pone.0114328
16. Bilchak JN, Yeakle K, Caron G, Malloy D, Côté MP. Enhancing KCC2 activity decreases hyperreflexia and spasticity after chronic spinal cord injury. Exp Neurol. 2021;338:113605. doi:10.1016/j.expneurol.2021.113605
17. Tan AM, Chakrabarty S, Kimura H, Martin JH. Selective corticospinal tract injury in the rat induces primary afferent fiber sprouting in the spinal cord and hyperreflexia. J Neurosci. 2012;32(37):12896–12908. doi:10.1523/JNEUROSCI.6451-11.2012
18. Jiang YQ, Armada K, Martin JH. Neuronal activity and microglial activation support corticospinal tract and proprioceptive afferent sprouting in spinal circuits after a corticospinal system lesion. Exp Neurol. 2019;321:113015. doi:10.1016/j.expneurol.2019.113015
19. Dang G, Chen X, Chen Y, Zhao Y, Ouyang F, Zeng J. Dynamic secondary degeneration in the spinal cord and ventral root after a focal cerebral infarction among hypertensive rats. Sci Rep. 2016;6(1):22655. doi:10.1038/srep22655
20. Wu YP, Ling EA. Induction of microglial and astrocytic response in the adult rat lumbar spinal cord following middle cerebral artery occlusion. Exp Brain Res. 1998;118(2):235–242. doi:10.1007/s002210050277
21. He JL, Ma LX, Zhuang YX, et al. Acupuncture modulates NMDAR-PP1/Calpain1-KCC2 pathway to ameliorate spinal hyperexcitability and spastic hemiplegia induced by ischemic stroke. J Integr Neurosci. 2025;24(12):46980. doi:10.31083/JIN46980
22. Shi GX, Yang CY, Wu MM, Guan LP, Wang LP, Liu CZ. Muscle hypertonia after permanent focal cerebral ischemia in rats: a qualitative and quantitative behavioral and electrophysiological study. Int J Neurosci. 2013;123(8):575–581. doi:10.3109/00207454.2013.783578
23. Liu T, Li X, Zhou X, et al. PI3K/AKT signaling and neuroprotection in ischemic stroke: molecular mechanisms and therapeutic perspectives. Neural Regener Res. 2025;20(10):2758. doi:10.4103/NRR.NRR-D-24-00568
24. Zheng T, Jiang T, Ma H, Zhu Y, Wang M. Targeting PI3K/akt in cerebral ischemia reperfusion injury alleviation: from signaling networks to targeted therapy. Mol Neurobiol. 2024;61(10):7930–7949. doi:10.1007/s12035-024-04039-1
25. Jia Z, Yue W, Zhang X, Xue B, He J. Erianin alleviates cerebral ischemia-reperfusion injury by inhibiting microglial cell polarization and inflammation via the PI3K/AKT and NF-κB pathways. Int Immunopharmacol. 2024;141:112915. doi:10.1016/j.intimp.2024.112915
26. Duan Z, Chen H, Miao W, et al. Scutellarin alleviates microglia-mediated neuroinflammation and apoptosis after ischemic stroke through the PI3K/AKT/GSK3 β signaling pathway. J Cell Commun Signal. 2024;18(2):e12023. doi:10.1002/ccs3.12023
27. Rao R, Gan L, Zhao R, Han Y. Electroacupuncture alleviates cerebral ischemia injury by regulating PI3K/AKT/NF-κB signaling in microglia of ischemic stroke rats. Neuroreport. 2025;36(1):22. doi:10.1097/WNR.0000000000002115
28. Xu H, Mu S, Qin W. Microglia TREM2 is required for electroacupuncture to attenuate neuroinflammation in focal cerebral ischemia/reperfusion rats. Biochem Biophys Res Commun. 2018;503(4):3225–3234. doi:10.1016/j.bbrc.2018.08.130
29. Wei L, Zeng K, Gai J, Zhou F, Wei Z, Bao Q. Effect of acupuncture on neurovascular units after cerebral infarction in rats through PI3K/AKT signaling pathway. Clin Hemorheol Microcirc. 2020;75(4):387–397. doi:10.3233/CH-190659
30. Xue X, You Y, Tao J, et al. Electro-acupuncture at points of zusanli and quchi exerts anti-apoptotic effect through the modulation of PI3K/akt signaling pathway. Neurosci Lett. 2014;558:14–19. doi:10.1016/j.neulet.2013.10.029
31. Birch S, Robinson N. Acupuncture as a post-stroke treatment option: a narrative review of clinical guideline recommendations. Phytomedicine. 2022;104:154297. doi:10.1016/j.phymed.2022.154297
32. Wang XY, Qian X, Ma LX, et al. Effects of acupoints-based TENS at different frequencies + tDCS on poststroke spastic hemiplegia: a randomized controlled trial. Am J Ther. 2025;32(2):e125–e134. doi:10.1097/MJT.0000000000001892
33. Lv Q, Xu G, Pan Y, et al. Effect of acupuncture on neuroplasticity of stroke patients with motor dysfunction: a meta-analysis of fMRI studies. Neural Plast 2021;2021:1–10. doi:10.1155/2021/8841720
34. Xue C, Jiang C, Zhu Y, et al. Effectiveness and safety of acupuncture for post-stroke spasticity: a systematic review and meta-analysis. Front Neurol. 2022;13:942597. doi:10.3389/fneur.2022.942597
35. Liu Y, Tang Y, Wang L, et al. Optimal acupuncture methods for lower limb motor dysfunction after stroke: a systematic review and network meta-analysis. Front Neurol. 2024:15. doi:10.3389/fneur.2024.1415792
36. Zhang Z, Mu J, Ma L, et al. Waggle needling yanglingquan (GB34) enhances cerebral blood flow and ameliorates condition of spastic paresis in rats with middle cerebral artery occlusion induced by surgical nylon suture. J Tradit Chin Med. 2023;43(3):514–522. doi:10.19852/j.cnki.jtcm.20230328.001
37. Chen X, Zhang H, Zou Y. A functional magnetic resonance imaging study on the effect of acupuncture at GB34 (yanglingquan) on motor-related network in hemiplegic patients. Brain Res. 2015;1601:64–72. doi:10.1016/j.brainres.2015.01.011
38. Ning Y, Li K, Fu C, et al. Enhanced functional connectivity between the bilateral primary motor cortices after acupuncture at yanglingquan (GB34) in right-hemispheric subcortical stroke patients: a resting-state fMRI study. Front Hum Neurosci. 2017;11:178. doi:10.3389/fnhum.2017.00178
39. Mu JD, Ma LX, Zhang Z, et al. Acupuncture alleviates spinal hyperreflexia and motor dysfunction in post-ischemic stroke rats with spastic hypertonia via KCC2-mediated spinal GABAA activation. Exp Neurol. 2022;354:114027. doi:10.1016/j.expneurol.2022.114027
40. He T, Zheng Y, Yan J, et al. Skin-brain axis: neural pathways in acupuncture treatment. Chin Med. 2025;20(1):163. doi:10.1186/s13020-025-01213-y
41. Li N, Guo Y, Gong Y, et al. The anti-inflammatory actions and mechanisms of acupuncture from acupoint to target organs via neuro-immune regulation. J Inflammation Res. 2021;14:7191–7224. doi:10.2147/JIR.S341581
42. Wang Y, Wang L, Wang Y, et al. Sensorimotor responses in post-stroke hemiplegic patients modulated by acupuncture at yanglingquan (GB34): a fMRI study using intersubject functional correlation (ISFC) analysis. Front Neurol. 2022;13:900520. doi:10.3389/fneur.2022.900520
43. Jung YS, Lee SW, Park JH, Seo HB, Choi BT, Shin HK. Electroacupuncture preconditioning reduces ROS generation with NOX4 down-regulation and ameliorates blood-brain barrier disruption after ischemic stroke. J Biomed Sci. 2016;23(1):32–42. doi:10.1186/s12929-016-0249-0
44. Liu R, Xu NG, Yi W, Ji C. Electroacupuncture attenuates inflammation after ischemic stroke by inhibiting NF- κ B-mediated activation of microglia. Kim YC, ed. Evid-Based Complement Altern Med. 2020;2020(1):8163052. doi:10.1155/2020/8163052
45. Lin X, Zhan J, Jiang J, Ren Y. Upregulation of neuronal cylindromatosis expression is essential for electroacupuncture-mediated alleviation of neuroinflammatory injury by regulating microglial polarization in rats subjected to focal cerebral ischemia/reperfusion. J Inflammation Res. 2021;14:2061–2078. doi:10.2147/JIR.S307841
46. Kathe C, Hutson TH, McMahon SB, Moon LDF. Intramuscular neurotrophin-3 normalizes low threshold spinal reflexes, reduces spasms and improves mobility after bilateral corticospinal tract injury in rats. eLife. 2016;5(e18146). doi:10.7554/eLife.18146
47. Brumovsky PR. VGLUTs in peripheral neurons and the spinal cord: time for a review. ISRN Neurol. 2013;2013:829753. doi:10.1155/2013/829753
48. Shimizu-Okabe C, Kobayashi S, Kim J, et al. Developmental formation of the GABAergic and glycinergic networks in the mouse spinal cord. Int J Mol Sci. 2022;23(2):834. doi:10.3390/ijms23020834
49. Mazzone GL, Mohammadshirazi A, Aquino JB, Nistri A, Taccola G. GABAergic mechanisms can redress the tilted balance between excitation and inhibition in damaged spinal networks. Mol Neurobiol. 2021;58(8):3769–3786. doi:10.1007/s12035-021-02370-5
50. McDonough KE, Hammond R, Wang J, et al. Spinal GABAergic disinhibition allows microglial activation mediating the development of nociplastic pain in male mice. Brain Behav Immun. 2023;107:215–224. doi:10.1016/j.bbi.2022.10.013
51. Ferrini F, De Koninck Y. Microglia control neuronal network excitability via BDNF signalling. Neural Plast. 2013;2013:429815. doi:10.1155/2013/429815
52. Kobayashi K, Imagama S, Ohgomori T, et al. Minocycline selectively inhibits M1 polarization of microglia. Cell Death Dis. 2013;4(3):e525–e525. doi:10.1038/cddis.2013.54
53. Naderi Y, Panahi Y, Barreto G, Sahebkar A. Neuroprotective effects of minocycline on focal cerebral ischemia injury: a systematic review. Neural Regener Res. 2020;15(5):773–782. doi:10.4103/1673-5374.268898
54. Wang PC, Wang SX, Yan XL, et al. Combination of paeoniflorin and calycosin-7-glucoside alleviates ischaemic stroke injury via the PI3K/AKT signalling pathway. Pharm Biol. 2022;60(1):1469–1477. doi:10.1080/13880209.2022.2102656
55. Sun Z, Sun L, Tu L. GABAB receptor-mediated PI3K/akt signaling pathway alleviates oxidative stress and neuronal cell injury in a rat model of Alzheimer’s disease. J Alzheimers Dis. 2020;76(4):1513–1526. doi:10.3233/JAD-191032
56. Chen M, Han Y, Que B, Zhou R, Gan J, Dong X. Prophylactic effects of sub-anesthesia ketamine on cognitive decline, neuroinflammation, and oxidative stress in elderly mice. Am J Alzheimers Dis Other Demen. 2022;37:15333175221141531. doi:10.1177/15333175221141531
57. McBride DW, Zhang JH. Precision stroke animal models: the permanent MCAO model should be the primary model, not transient MCAO. Transl Stroke Res. 2017;8(5):397–404. doi:10.1007/s12975-017-0554-2
58. Sommer CJ. Ischemic stroke: experimental models and reality. Acta Neuropathol. 2017;133(2):245–261. doi:10.1007/s00401-017-1667-0
59. Zhang Z, Ma LX, Mu JD, et al. Acupuncture waggle needling alleviates spastic movement disorder in post-stroke rats via GLT-1 activation to modulate glu/GABA-gln cycle. Physiol Behav. 2025;301:115059. doi:10.1016/j.physbeh.2025.115059
60. Lee B, Sur B, Shim J, Hahm DH, Lee H. Acupuncture stimulation improves scopolamine-induced cognitive impairment via activation of cholinergic system and regulation of BDNF and CREB expressions in rats. BMC Complement Altern Med. 2014;14:338. doi:10.1186/1472-6882-14-338
61. Zhao Z, Kim SC, Liu H, et al. Manual acupuncture at PC6 ameliorates acute restraint stress-induced anxiety in rats by normalizing amygdaloid noradrenergic response. Evid-Based Complement Altern Med: eCAM. 2017;2017:4351723. doi:10.1155/2017/4351723
62. Chen J, Sanberg PR, Li Y, et al. Intravenous administration of human umbilical cord blood reduces behavioral deficits after stroke in rats. Stroke. 2001;32(11):2682–2688. doi:10.1161/hs1101.098367
63. Bohannon RW, Smith MB. Interrater reliability of a modified ashworth scale of muscle spasticity. Phys Ther. 1987;67(2):206–207. doi:10.1093/ptj/67.2.206
64. Ryu Y, Ogata T, Nagao M, et al. The swimming test is effective for evaluating spasticity after contusive spinal cord injury. Fehlings MG ed.. PLoS One. 2017;12(2):e0171937. doi:10.1371/journal.pone.0171937
65. Chang YX, Zhao Y, Pan S, et al. Intramuscular injection of adenoassociated virus encoding human neurotrophic factor 3 and exercise intervention contribute to reduce spasms after spinal cord injury. Neural Plast. 2019;2019:1–14. doi:10.1155/2019/3017678
66. Ye XC, Hao Q, Ma WJ, et al. Dectin-1/syk signaling triggers neuroinflammation after ischemic stroke in mice. J Neuroinflammation. 2020;17(1):17–32. doi:10.1186/s12974-019-1693-z
67. Zvejniece L, Svalbe B, Vavers E, et al. Decreased long-chain acylcarnitine content increases mitochondrial coupling efficiency and prevents ischemia-induced brain damage in rats. Biomed Pharmacother. 2023;168:115803. doi:10.1016/j.biopha.2023.115803
68. Cui JJ, Wang J, Xu DS, et al. Alexa fluor 488-conjugated cholera toxin subunit B optimally labels neurons 3–7 days after injection into the rat gastrocnemius muscle. Neural Regener Res. 2022;17(10):2316. doi:10.4103/1673-5374.337055
69. Wang Y, Ma X, Wang X, et al. Traditional Chinese medicine borneol-based polymeric micelles intracerebral drug delivery system for precisely pathogenesis-adaptive treatment of ischemic stroke. Adv Sci. 2025;12(9):2410889. doi:10.1002/advs.202410889
70. Thompson FJ, Reier PJ, Lucas CC, Parmer R. Altered patterns of reflex excitability subsequent to contusion injury of the rat spinal cord. J Neurophysiol. 1992;68(5):1473–1486. doi:10.1152/jn.1992.68.5.1473
71. Planas AM. Role of microglia in stroke. Glia. 2024;72(6):1016–1053. doi:10.1002/glia.24501
72. Sheng W, Li S, Zhao J, et al. Upper limbs muscle Co-contraction changes correlated with the impairment of the corticospinal tract in stroke survivors: preliminary evidence from electromyography and motor-evoked potential. Front Neurosci. 2022;16:886909. doi:10.3389/fnins.2022.886909
73. Mu J, Hao L, Wang Z, et al. Visualizing wallerian degeneration in the corticospinal tract after sensorimotor cortex ischemia in mice. Neural Regener Res. 2024;19(3):636–641. doi:10.4103/1673-5374.380903
74. Stuckey SM, Ong LK, Collins-Praino LE, Turner RJ. Neuroinflammation as a key driver of secondary neurodegeneration following stroke? Int J Mol Sci. 2021;22(23):13101. doi:10.3390/ijms222313101
75. Yi L, Huang L, Chen R, Zhan S, Huang H, Yue Z. Acupuncture for post-stroke spasticity: an overview of systematic reviews. Complement Ther Med. 2024;80:103024. doi:10.1016/j.ctim.2024.103024
76. Lyu T, Liu Z, Yu T, et al. Applying RNA sequencing technology to explore repair mechanism of tuina on gastrocnemius muscle in sciatic nerve injury rats. Chin Med J (Engl). 2022;135(19):2378. doi:10.1097/CM9.0000000000001960
77. Suryanarayanan A, Carter JM, Landin JD, Morrow AL, Werner DF, Spigelman I. Role of interleukin-10 (IL-10) in regulation of GABAergic transmission and acute response to ethanol. Neuropharmacology. 2016;107:181–188. doi:10.1016/j.neuropharm.2016.03.027
78. Gilio L, Fresegna D, Stampanoni Bassi M, et al. Interleukin-10 contrasts inflammatory synaptopathy and central neurodegenerative damage in multiple sclerosis. Front Mol Neurosci. 2024;17:1430080. doi:10.3389/fnmol.2024.1430080
79. Schmidt-Pogoda A, Ruck T, Strecker J, et al. Exercise facilitates post-stroke recovery through mitigation of neuronal hyperexcitability via interleukin-10 signaling. Nat Commun. 2025;16(1):8928. doi:10.1038/s41467-025-62631-y
80. Xu Y, Wen K, Liu A, Wang X, Xu H, Wen H. Efficacy of curculigoside in protecting against ischemic brain injury through regulation of oxidative stress and NF-κB and PI3K/akt expression. J Ethnopharmacol. 2023;301:115804. doi:10.1016/j.jep.2022.115804
81. Li L, Jiang W, Yu B, et al. Quercetin improves cerebral ischemia/reperfusion injury by promoting microglia/macrophages M2 polarization via regulating PI3K/Akt/NF-κB signaling pathway. Biomed Pharmacother. 2023;168:115653. doi:10.1016/j.biopha.2023.115653
82. Shi X, Cai X, Di W, et al. MFG-E8selectively inhibited aβ-induced microglial M1 polarization via NF-κB and PI3K-akt pathways. Mol Neurobiol. 2017;54(10):7777–7788. doi:10.1007/s12035-016-0255-y
83. Vergadi E, Ieronymaki E, Lyroni K, Vaporidi K, Tsatsanis C. Akt signaling pathway in macrophage activation and M1/M2 polarization. J Immunol. 2017;198(3):1006–1014. doi:10.4049/jimmunol.1601515
84. Liu W, Wang X, Yang S, et al. Electroacupunctre improves motor impairment via inhibition of microglia-mediated neuroinflammation in the sensorimotor cortex after ischemic stroke. Life Sci. 2016;151:313–322. doi:10.1016/j.lfs.2016.01.045
85. Xu H, Wang Y, Luo Y. OTULIN is a new target of EA treatment in the alleviation of brain injury and glial cell activation via suppression of the NF-κB signalling pathway in acute ischaemic stroke rats. Mol Med. 2021;27(1):37. doi:10.1186/s10020-021-00297-0
86. Jiang J, Luo Y, Qin W, et al. Electroacupuncture suppresses the NF-κB signaling pathway by upregulating cylindromatosis to alleviate inflammatory injury in cerebral ischemia/reperfusion rats. Front Mol Neurosci. 2017;10:363. doi:10.3389/fnmol.2017.00363
87. Jiang YQ, Zaaimi B, Martin JH. Competition with primary sensory afferents drives remodeling of corticospinal axons in mature spinal motor circuits. J Neurosci. 2016;36(1):193–203. doi:10.1523/JNEUROSCI.3441-15.2016
88. Brownstone RM, Bui TV. Spinal interneurons providing input to the final common path during locomotion. In: Progress in Brain Research. Vol. 187. Elsevier;2010:81–95. doi:10.1016/B978-0-444-53613-6.00006-X
89. Ramírez-Jarquín UN, Lazo-Gómez R, Tovar-y-Romo LB, Tapia R. Spinal inhibitory circuits and their role in motor neuron degeneration. Neuropharmacology. 2014;82:101–107. doi:10.1016/j.neuropharm.2013.10.003
90. Grigoras IF, Stagg CJ. Recent advances in the role of excitation–inhibition balance in motor recovery post-stroke. Fac Rev. 2021;10:58–66. doi:10.12703/r/10-58
91. Chen J, Liu C, Li L, et al. Exogenous leptin alleviates glutamate-excitotoxic injury caused by cerebral ischemia–reperfusion in mice by affecting the expression of glutamate transporters. Brain Res. 2024;1845:149201. doi:10.1016/j.brainres.2024.149201
92. Llansola M, Arenas YM, Sancho-Alonso M, et al. Neuroinflammation alters GABAergic neurotransmission in hyperammonemia and hepatic encephalopathy, leading to motor incoordination. Mechanisms and therapeutic implications. Front Pharmacol. 2024;15:1358323. doi:10.3389/fphar.2024.1358323
93. Ye L, Huang Y, Zhao L, et al.
94. Rocha RP, Zorzi M, Corbetta M. Role of homeostatic plasticity in critical brain dynamics following focal stroke lesions. Sci Rep. 2024;14(1):31631. doi:10.1038/s41598-024-80196-6
95. Pan WX, Fan AY, Chen S, Alemi SF. Acupuncture modulates immunity in sepsis: toward a science-based protocol. Auton Neurosci. 2021;232:102793. doi:10.1016/j.autneu.2021.102793
96. Spychala MS, Honarpisheh P, McCullough LD. Sex differences in neuroinflammation and neuroprotection after ischemic stroke. J Neurosci Res. 2017;95(1–2):462–471. doi:10.1002/jnr.23962
97. Kerr N, Dietrich DW, Bramlett HM, Raval AP. Sexually dimorphic microglia and ischemic stroke. CNS Neurosci Ther. 2019;25(12):1308–1317. doi:10.1111/cns.13267
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neuroprotective Effects of Leptin on the APP/PS1 Alzheimer’s Disease Mouse Model: Role of Microglial and Neuroinflammation
Ma J, Hou YH, Liao ZY, Ma Z, Zhang XX, Wang JL, Zhu YB, Shan HL, Wang PY, Li CB, Lv YL, Wei YL, Dou JZ
Degenerative Neurological and Neuromuscular Disease 2023, 13:69-79
Published Date: 25 October 2023
Neuroprotective Effects of Eugenol Acetate Against Ischemic Stroke
Chen L, Zhang R, Xiao J, Liang Y, Lan Z, Fan Y, Yu X, Xia S, Yang H, Bao X, Meng H, Xu Y, Yu L, Zhu X
Journal of Inflammation Research 2025, 18:133-146
Published Date: 6 January 2025
Acupuncture for Ischemic Stroke: A Critical Evaluation of Biological Mechanisms and Methodological Challenges
Wang Y, Yu H, Chen Y, Hu Y, Zhou H, Zhao J
International Journal of General Medicine 2025, 18:5379-5393
Published Date: 11 September 2025
Circulating MicroRNA Biomarkers for Chronic Pain and Acupuncture Response: An Exploratory High-Dimensional Small-Sample Study
Kang IH, Kim SN
Journal of Pain Research 2025, 18:6591-6605
Published Date: 6 December 2025
Plant-Derived Nanovesicles for Ischemic Stroke Therapy via the Gut Microbiota-Gut-Brain Axis: A New Paradigm of Systemic Regulation
Jiang J, Yu F, He M, Huang R, He H, Murong Z, Xiong S, Liu M
International Journal of Nanomedicine 2026, 21:597334
Published Date: 6 May 2026