Back to Journals » Journal of Pain Research » Volume 19
A Scoping Review and Content Analysis of Available Chronic Pain Education Programs and Resources for Children, Adolescents and Young Adults with Diverse Abilities
Authors Smith MG ![]() , Schaly S, Berryman C
, Schaly S, Berryman C ![]() , Khillan A, Ostojic K, Harvey A
, Khillan A, Ostojic K, Harvey A
Received 5 February 2026
Accepted for publication 17 April 2026
Published 13 May 2026 Volume 2026:19 601477
DOI https://doi.org/10.2147/JPR.S601477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Helen Koechlin
Meredith G Smith,1,2 Sabrina Schaly,3 Carolyn Berryman,4,5 Aayushi Khillan,6,7 Katarina Ostojic,8 Adrienne Harvey7,9
1School of Allied Health & Human Performance, Adelaide University, Adelaide, SA, Australia; 2Novita, Adelaide, SA, Australia; 3Biomedical Engineering, Faculty of Engineering, The University of Sydney, Sydney, NSW, Australia; 4Innovation IMPlementation and Clinical Translation (IIMPACT) in Health, College of Health, Adelaide University, Adelaide, Kaurna Country, SA, Australia; 5Women’s and Children’s Hospital Network, Adelaide, Kaurna Country, SA, Australia; 6Medicine, Dentistry and Health Sciences, University of Melbourne, Parkville, VIC, Australia; 7Neurodisability and Rehabilitation, Murdoch Children’s Research Institute, Parkville, VIC, Australia; 8Community Paediatrics Research Group, Faculty of Medicine and Health, The University of Sydney, Sydney, NSW, Australia; 9School of Primary and Allied Health Care, Faculty of Medicine, Nursing and Health Science, Monash University, Frankston, VIC, Australia
Correspondence: Meredith G Smith, School of Allied Health and Human Performance, Adelaide University, Adelaide, SA, 5005, Australia, Email [email protected]
Abstract: Approximately one-in-five children and adolescents experience chronic pain. Pain education, where people are provided with information, supports and skills to better manage pain, is a key component of effective pain management. This review identified and synthesised the content of existing chronic pain education programs/resources for individuals aged 5– 25 years and examined their accessibility for those with diverse abilities. Searches of research databases, publicly available websites, and a global call for innovations identified 89 records representing 69 unique programs/resources. The most frequently referenced were “Web-based Management for Adolescent Pain (Web-MAP)”, “The ComfortAbility Program”, and “iCanCope with Pain”. Programs/resources were analysed using content analysis and mapped to seven recommended chronic pain education categories (Partnerships, self-management skills, lifestyle habits, emotional coping, social role support, informed decisions, and explaining pain) and five accessibility domains (cognition, communication, vision, hearing and movement). Accessibility was assessed through content review by coding each resource for explicit or potential consideration of accessibility. Educational content was commonly delivered through websites or face-to-face sessions, and emerging digital approaches (including mobile applications, virtual reality, chatbots, podcasts, social media). Most delivery approaches were online and self-directed. Of the analysed programs/resources, only four addressed all seven recommended chronic pain education categories. The category most frequently addressed involved promoting active cognitive and behavioural strategies to improve function and reduce symptoms. Accessibility analysis suggested that while over half of the resources were likely suitable for individuals with diverse visual (56.5%), communication (82.6%), auditory (84.1%), or movement abilities (91.3%), accessibility for those with cognitive impairment was markedly underrepresented and by far the least addressed domain (14.5%). Overall, while many pain education programs and resources exist for young people with chronic pain, few address all recommended education domains. Future development should emphasise inclusive design and equitable accessibility, particularly cognitive accessibility, to ensure resources effectively meet diverse needs.
Keywords: pain education, chronic pain, children, adolescents, young adults, accessibility
Introduction
Chronic pain is defined as persistent or recurring pain, usually lasting longer than 3 months or the expected time to heal.1 Chronic pain is a common condition in both adult and pediatric populations globally. Approximately 1 in 4 adults2 report unspecified ongoing pain and 1 in 5 children and adolescents3 report chronic pain. Chronic pain is associated with significant functional impact and caregiver burden.3
Management of chronic pain is complex and requires consideration of the interplay of biological, psychological, and social factors.4 Chronic pain can adversely affect an individual’s wellbeing, including mood, cognition, sleep, and activity.3 Pain education is a fundamental component of chronic pain management, where people are provided with information, supports, and skills to better manage their pain.5 Historically, pain education has focused heavily on pain neuroscience education, which seeks to align a person’s understanding, beliefs, and attitudes about pain with current scientific understanding that pain is a marker of the perceived need to protect the body tissue, not a measure of damage.6 However, pain neuroscience education represents only one component of pain education. Broader self-management education, which includes practical skill-building in self-regulation, personal wellbeing and strategies to support meaningful engagement, is also crucial for helping individuals actively manage their pain.5 As self-management focused pain education is clinically recommended as part of multimodal and interdisciplinary chronic pain interventions, this review focuses on this more holistic understanding of pain education.5
Delivering effective pain education requires a highly individualised and tailored approach, taking into consideration a person’s unique abilities, strengths, and challenges. For children and young people with diverse needs, this involves ensuring pain education is developmentally appropriate and accessible for those with intellectual impairment, physical disability, or those who use augmentative and alternative communication. This is especially important given children and young people with physical disabilities, such as cerebral palsy, experience higher rates of chronic pain than the general pediatric population;7,8 and effective pain management strategies are lacking.9
Previous research by Ickmans et al10 reviewed available pediatric pain education programs, however this had a focus on pain neuroscience education and was limited to pediatric (<18 years) populations only. Similarly, Betting et al11 reviewed pediatric pain education resources with a focus on the integration of lifestyle factors, however neither have considered the needs of children, adolescents and young adults with diverse abilities. By taking a broader and more inclusive approach, examining programs and resources across ages 5–25 years and evaluating their potential accessibility for individuals with diverse communication, cognitive, vision, hearing and movement abilities, this review provides a unique opportunity to identify which existing options may be most adaptable for children and young people with diverse needs and abilities.
The overarching aim of this review was to evaluate the content of currently available chronic pain education programs and resources for people aged 5–25 years and explore considerations for the accessibility of the available programs/resources for children and young people with diverse abilities. The following research questions were used to guide the review:
- What pain education programs and resources are available for children, adolescents and young adults with chronic pain (aged 5–25 years)?
- What areas of content are covered in existing pain education programs and resources?
- To what extent do existing pain education programs and resources include accessibility considerations for children, adolescents and young adults with diverse abilities, including diverse cognitive, communication and movement abilities?
Methods
Protocol and Registration
The protocol for this review was guided by the Joanna Briggs Institute Manual for Evidence Synthesis for Scoping Reviews.12 The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews Guidelines were followed for quality reporting.13 The review protocol was pre-registered and published on Open Science Framework (https://osf.io/9yaxj).
Eligibility Criteria
Inclusion and exclusion criteria were defined using the PCC (population, concept, context) criteria (Table 1). 12 Programs (eg. courses, modules, sessions) or resources (eg. handouts, websites), or studies reporting on them, were included if the program/resource 1) was evidence-based, grounded in scientific research and/or developed by experts in the field, and targeted pain education, defined as aiming to improve understanding of pain for successful self-management;14 2) was developed within the past fifteen years (2010–2025), reflecting changes in chronic pain education and management over this period;6,15 3) targeted individuals aged 5–25 years with chronic pain; and 4) was available in English. The 5–25 year age range was selected to encompass childhood, adolescence and young adulthood, allowing examination of pain education programs and resources across key developmental stages and the transition to adulthood. This broader range also supported the focus on accessibility, as some resources developed for younger children may be appropriate for adolescents and young adults with accessibility needs, such as cognitive impairment. Programs/resources or related studies were excluded if they focused on acute pain, addressed pain neuroscience education only (defined as teaching people about neurobiological and neurophysiological processes involved in their chronic pain experience),16 originated from unverified sources or if the program content was not available or obtainable upon request from the authors.
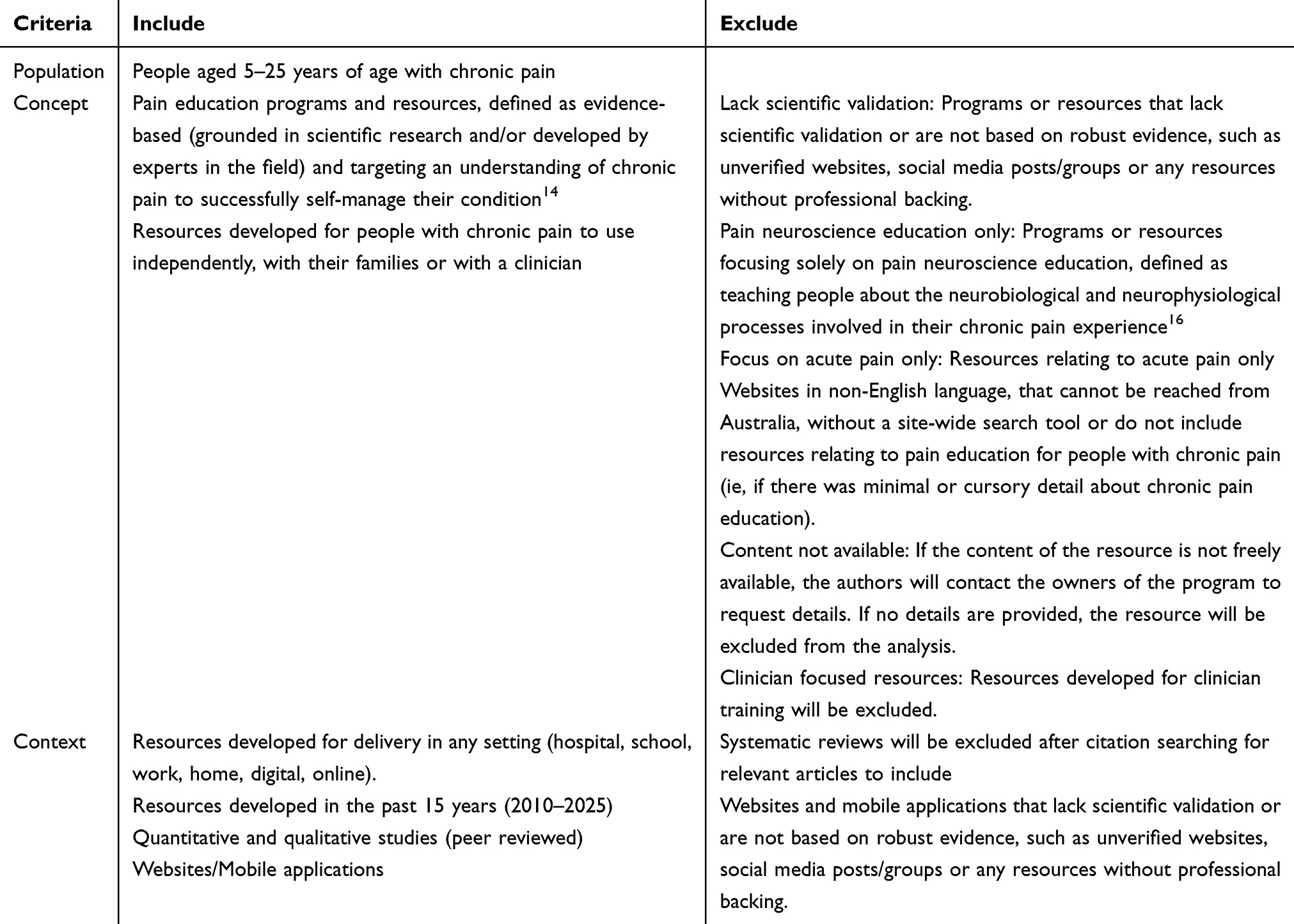 |
Table 1 Inclusion and Exclusion Criteria for Study Screening |
Search Strategy
The search strategy was developed collaboratively by the research team and a health sciences librarian. Four databases (MEDLINE, CINAHL, PsycInfo, and PubMed) were searched on 1 May 2025. To capture unpublished studies and grey literature, a tailored Google search was conducted, screening the first ten pages of results. Full database search strings are provided in Supplementary Material 1. Additional records were identified through citation searching of included studies and a public call via the Pain in Child Health (PICH) List Serv (https://paininchildhealth.ca/), an international Email network of clinicians and researchers in pediatric pain. Recipients were invited to share details of programs or resources that may have been missed in the initial search.
Study Screening
All identified records were collated and uploaded into EndNote 21 (Clarivate Analytics, PA, USA) and duplicates removed. These were then imported into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at https://www.covidence.org). Following pilot testing, titles and abstracts (where relevant) were screened by two of nine independent reviewers (MS, AK, SS, CD, JH, CB, GH, KO, IH). Six reviewers from this group completed full-text screening (MS, AK, SS, KO, JH, CB) with at least two reviewers reviewing each abstract and full text. Where conflicts occurred, these were resolved through consensus with another project team member (AH). Training sessions took place prior to the beginning of the screening, and regular consensus meetings were held to clarify criteria and resolve any concerns.
Data Extraction
Data was extracted from the included records by the same six team members from the full-text phase (MS, AK, SS, KO, JH, CB), using a custom data extraction tool developed by the project team. Pilot testing was conducted prior to commencing the data extraction phase to refine the data extraction tool and criteria, with regular consensus meetings held to address discrepancies, refine extraction criteria and ensure a consistent approach across all reviewers. One reviewer completed data extraction for the remaining records, with a second reviewer from the team of six independently checking a 20% random sample. No disagreements were noted. Reviewers also had access to AI-assisted extraction outputs generated by Elicit (https://elicit.com) for comparison after completing manual extraction of research papers included in the review.
The following data was extracted from the included records: 1) study characteristics (ie, author, publication year, funding, country of study, study design/resource type, population), 2) basic information on the pain education delivery (ie, setting, resource requirements) and content and 3) accessibility considerations for people with diverse cognitive, communication, motor, visual and auditory ability.
On 30 September 2025, all authors or owners of identified pain education programs/resources were contacted via Email to request access to the program/resource if it was not freely available. A follow-up reminder was sent 2 weeks later. Where access or additional content information was not provided, the content analysis was based on descriptions available in published sources (where possible). The content analysis process followed methods similar to those described by Hurley-Wallace et al (2021)17 and Healthcote et al (2019)18 to assess both content and accessibility. Coding was guided by the six categories of chronic pain self-management education outlined by LeFort & McGillion (2021),19 adapted from Bodenheimer’s (2002)14 chronic condition self-management framework. An additional category, “explaining pain”, was included, to capture content related to pain neuroscience education, which is not explicitly represented in the six self-management categories.
The final seven categories were:
- Building partnerships with health-care providers
- Using active cognitive and behavioural strategies to maximise function and reduce pain and other symptoms
- Modifying family, social, and work/school responsibilities as needed to maintain important relationships and meaningful life roles
- Dealing with the emotional ups and downs of living with a chronic pain condition
- Maintaining and/or building a healthy lifestyle that features stress management, regular exercise, healthy eating, and sound sleep habits
- Using appropriate resources and managing decisions for interventions such as medication use, surgical procedures, and complementary therapies
- Explaining pain: defined as ‘meeting the person at their current level of understanding and experience, to facilitate an understanding of pain that aligns with both their context and modern scientific evidence of mechanisms thought to underpin pain’6
Each category was coded as 0 = absent, 1 = vaguely represented, 2 = clearly represented using the same coding system as Hurley-Wallace et al17. In addition, each resource was coded as 0 = no or 1 = yes to indicate whether it explicitly considered accessibility for individuals with diverse cognitive, communication, vision, hearing, and movement abilities, or could potentially be made accessible with minimal adaptation (ie, utilise closed-caption function on a video for hearing impairment). To enhance consistency in coding, operational definitions were established by the authors for each accessibility domain. Cognitive accessibility was coded “1” when the resource appeared understandable to individuals with cognitive abilities equivalent to approximately 8 years of age or younger. Communication accessibility was coded “1” if the resource could be used by individuals with diverse expressive communication abilities, including those who use augmentative and alternative communication (AAC), and “0” when spoken responses or complex expressive communication were required. Visual accessibility was coded “1” if the resource could be accessed or understood without relying solely on visual information. Movement accessibility was coded “1” when full motor function (eg, independent ambulation or upper-limb control) was not required to use the resource. Hearing accessibility was coded “1” if the resource could be accessed or understood without relying exclusively on auditory information (eg, through captions or visual cues).
An initial period of familiarisation was undertaken by two authors completing the content analysis (MS, AH), whereby programs/resources were read/viewed, and the coding spreadsheet was piloted. After reviewing two programs/resources, the authors met and compared coding and reached consensus on any discrepancies, providing an initial check of agreement before continuing with independent coding. The remaining programs/resources were then coded independently by two authors (MS, AH), with discrepancies during the coding process resolved through consensus and consultation with a third author where necessary (CB).
Results
Database searching identified 4449 records. An additional 200 records were found through the Google search, citation searching and the PICH List Serv. After removing 1012 duplicates, 3637 records remained for screening. Of these, 3320 were excluded and full text of 317 records were sought for retrieval with 315 retrieved and screened against the inclusion and exclusion criteria (see Table 1) and a final total of 89 records were included in the review. Reasons for exclusion are shown in the PRISMA flow diagram in Figure 1. 13 A complete list of records and their characteristics is provided in Supplementary Material 2.
 |
Figure 1 PRISMA 2020 flow diagram of study identification and screening20 This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/. |
Record Characteristics
The searches identified a variety of record types, including traditional research papers, books (both fiction and non-fiction), manuals, guidelines, videos, and websites (Full record list provided in Supplementary Material 2). The most frequently reported record type was papers reporting randomised controlled trials (RCTs) (n = 25, 28.1%), followed by websites (n = 17, 19.1%) and papers reporting non-randomised experimental studies (n = 11, 12.4%).
The most common target population was unspecified chronic pain (n = 52, 58.4%), followed by musculoskeletal chronic pain (n = 15, 16.9%), headache/migraine chronic pain (n = 11, 12.4%), and abdominal chronic pain (n = 8, 9.0%). Other populations included complex regional pain syndrome (n = 3), fibromyalgia (n = 1), lupus (n = 2), osteogenesis imperfecta (n = 1), sickle cell disease (n = 4), arthritis (n = 1), and temporomandibular disorder (n = 1).
Pain Education Programs and Resources
Of the 89 records identified,5,21–108 74 unique pain education resources or programs were found. Five were excluded from content analysis because they were no longer available, leaving 69 for analysis. Of the 69 analysed, 53 were uniquely titled, and sixteen were mentioned within articles but not individually named. The most frequently reported titled programs/resources were Web-based Management for Adolescent Pain (Web-MAP) (n = 9 records), The ComfortAbility Program (n = 4), and iCanCope with Pain™ (n = 4). Of the uniquely titled programs/resources (n = 53), seventeen were available in more than one language, while 36 were only available in English. A full list of programs/resources, including details on content, delivery methods, and access, is provided here (https://doi.org/10.25909/31908319) in spreadsheet form and also available on a dedicated webpage (https://www.cp-pain.org.au/resources).
The most common program/resource type was websites (n = 19, 27.5%), followed by face-to-face individual education (n = 11, 15.9%), videos (n = 10, 14.5%), and books (n = 8, 11.6%). Other less common formats included mobile applications, face-to-face group education, hybrid interventions, games, podcasts, social media, virtual reality, and chatbots. Most resources targeted adolescents (12–17 years) (n = 49, 71.0%), with fourteen (20.3%) specifically developed for children (<12 years) and eighteen (26.1%) for young adults. Ten programs/resources (14.5%) spanned more than one age category. Program/resource type was similar across age groups: websites were most common for all, books were more frequent for children, and face-to-face individual sessions were more common for adolescents and young adults. Websites often combined written information with videos.
Education was most often delivered online (n = 33, 47.8%), followed by hospital (n = 7, 10.1%), home (n = 7, 10.1%), and school (n = 4, 5.8%) settings. Three programs/resources used community-based clinics, and two used residential camps. Nine programs/resources combined settings (eg, school and home), and four did not specify a location. Delivery was primarily self-directed (n = 39) or health professional-led (n = 19). Seven programs/resources used mixed facilitators (eg, health professional and peer), and only two relied solely on peer education. At the time of writing, 48 programs/resources were publicly available (n = 26 free, n = 22 paid), while 21 need to be requested from authors. Co-design involvement was absent in 45 programs/resources (65.2%); the remaining 24 (34.8%) involved health professionals, children/adolescents/young adults with chronic pain, and/or parents/caregivers in their development. Almost half of the programs/resources were available on-demand (n = 32, 46.4%), while others required sequenced access, were one-off, or combined both approaches.
Pain Education Content
The pain education content included in each program/resource is detailed in Table 2. Across the 69 programs/resources, the most frequently reported category was “Using active cognitive and behavioural strategies to maximise function and reduce pain and other symptoms” (n = 61, 88.4%), and the least commonly reported category was “Using appropriate resources and managing decisions for interventions such as medication use, surgical procedures, and complementary therapies” (n = 23, 33.3%). Table 2 summarises the most commonly included pain education content categories across these programs/resources. There were four programs/resources which clearly represented all seven of the pain education categories: Dolores (chatbot),24 PainBytes (https://aci.health.nsw.gov.au/chronic-pain/painbytes),72 Power over Pain Portal Youth (https://www.popyouth.ca/)99 and Young painHEALTH (https://youngpainhealth.com.au/).94
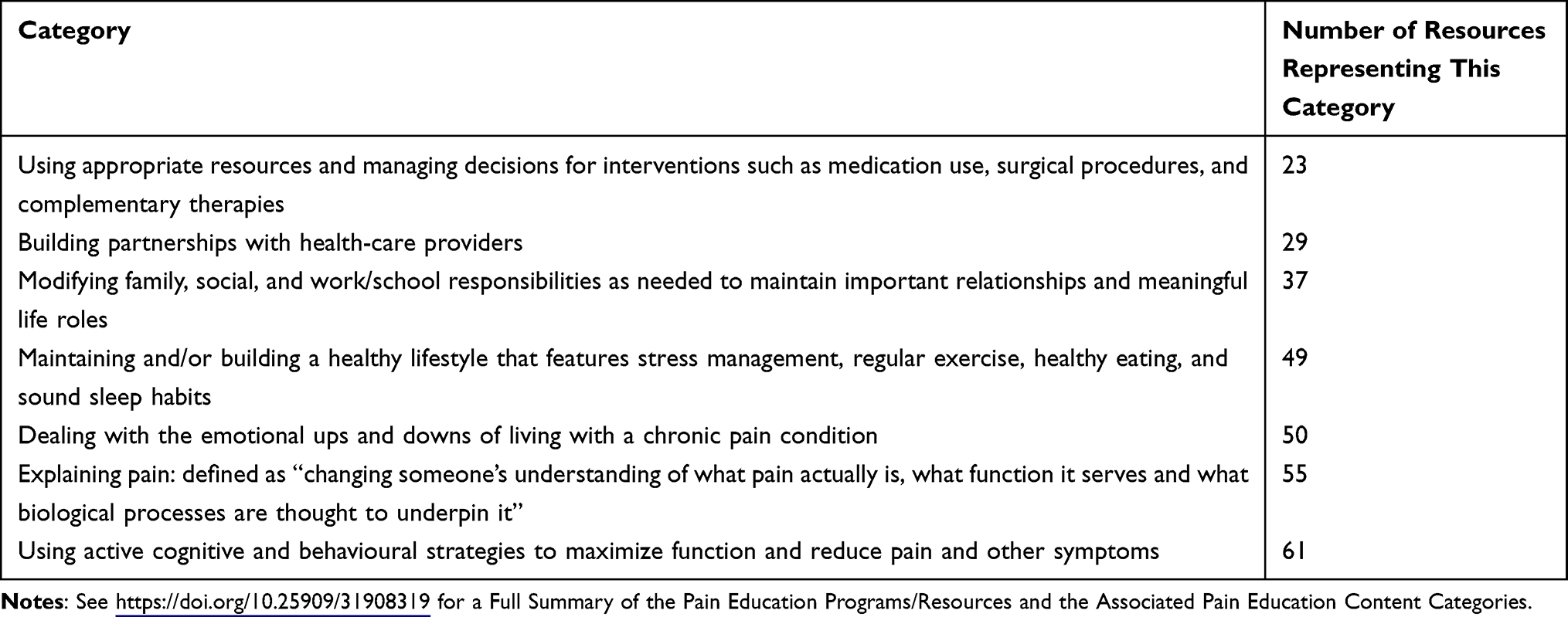 |
Table 2 Frequency of Included Categories of Pain Education Content Across 69 Resources |
Accessibility of the Pain Education Programs and Resources
None of the included programs/resources explicitly reported accessibility considerations during development or delivery for individuals with cognitive, communication, or movement impairments. In fact, ten studies56,59,61,75–78,92,93,96 specifically excluded participants with intellectual disability.
When assessed for potential accessibility, defined as either having explicit considerations for these needs or being adaptable with minimal effort, the following proportions were identified across the 69 programs/resources (see also (https://doi.org/10.25909/31908319):
- Cognitive accessibility: 10 programs/resources (14.5%)
- Visual accessibility: 39 programs/resources (56.5%)
- Communication accessibility: 57 programs/resources (82.6%)
- Auditory accessibility: 58 programs/resources (84.1%)
- Movement accessibility: 63 programs/resources (91.3%)
Examples of barriers and facilitators to accessibility for these programs/resources are provided in Table 3. Of the 69 programs/resources evaluated, four were identified as being likely accessible for all five accessibility categories, which included two face-to-face, individual cognitive behavioural therapy programs63,71 and two video-based resources.66,97 Of these, only one was publicly available, a video resource “What is Chronic Pain” by The Hospital for Sick Children.97
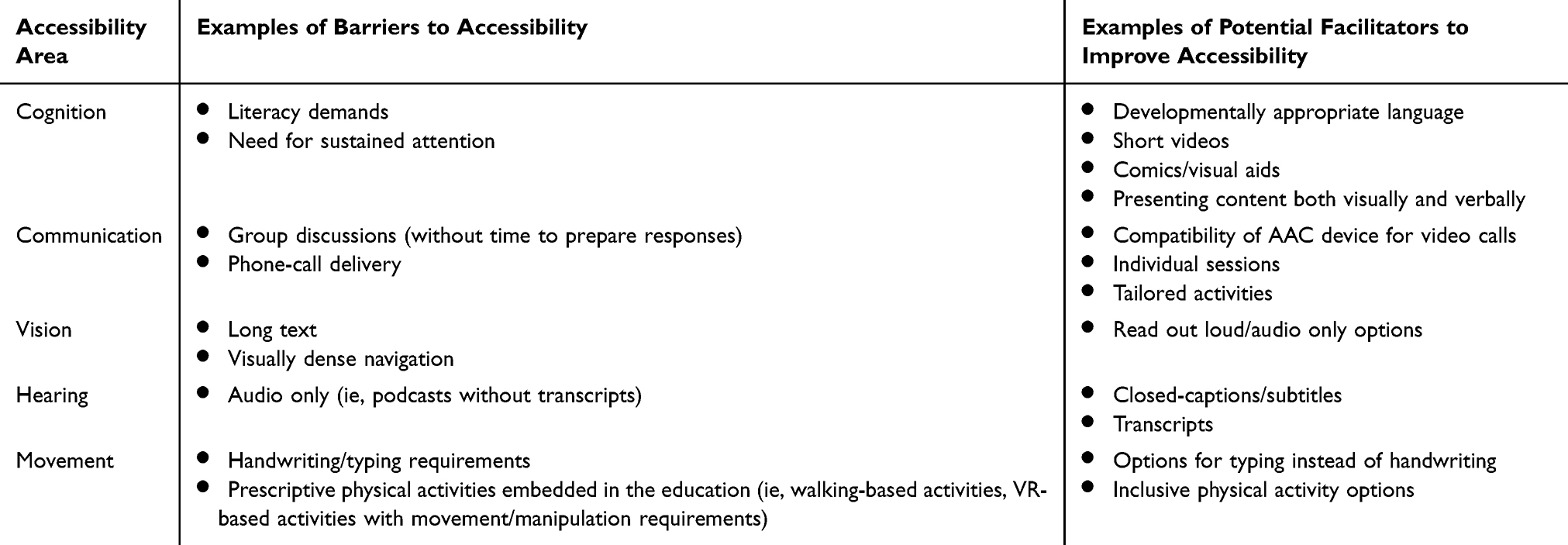 |
Table 3 Examples of Barriers and Facilitators to Accessibility for the Included Pain Education Programs/Resources |
Discussion
This scoping review has identified 69 unique pain education programs or resources (48 publicly available) currently available with a variety of delivery methods such as websites, face-to-face sessions, and other digital platforms. Delivery of included pain education content is mostly online and typically self-directed. Only four programs/resources address all seven chronic pain education categories, with the most frequently reported category being “using active cognitive and behavioural strategies to maximise function and reduce pain and other symptoms”. Preliminary accessibility analysis suggests over half of the programs/resources are likely suitable for individuals with diverse visual, communication, auditory, or movement abilities. However, only a small proportion appear suitable for those with cognitive impairment.
Pain Education Content & Delivery Methods
In this review, our aim was to move beyond pain neuroscience education alone and explore which pain education programs or resources promote learning practical self-management and self-regulation strategies to improve comfort, and support meaningful engagement in activities, decision making, and the development of autonomy. Self-management of chronic pain refers to an intentional, active effort to manage pain and its impact on physical and emotional functioning.109 This review found few programs/resources addressing education categories of “building relationships with healthcare providers” or “building decision making capability in managing intervention decisions”. Given that building relationships with healthcare providers is known to be a key contributor to successful self-management of chronic pain,109 it is important to consider how content on this topic can be improved for existing programs/resources or developed for new resources. Furthermore, building decision-making capability is especially important for people with disability, who have historically had reduced agency and autonomy in health management decision making.110 Given these findings, future pain education programs and resources should aim to incorporate all seven of the recommended content categories,14 with a particular focus on building relationships with healthcare providers and decision-making capability. Including all categories is likely to best equip children, adolescents and young adults with chronic pain and diverse abilities with the knowledge, skills and autonomy to most effectively manage their condition.
The wide range of pain education programs and resources identified in this review is encouraging, as a single approach is unlikely to suit all age groups or individuals with co-occurring conditions. For example, play-based strategies are recommended for children (6–11 years), whereas inquiry-based approaches that incorporate technology are better suited for adolescents and young adults.111 This highlights the need for developmentally appropriate programs. However, rigid age-based approaches may not work well for populations with diverse abilities (ie, cognition), such as people with cerebral palsy and chronic pain. Therefore, pain education programs/resources should be designed with maximum flexibility and inclusivity in mind, using multimodal content and flexible delivery options, to ensure they can be tailored to a wide audience.
Accessibility
This review identified a wide range of pain education programs/resources which have the potential to be adapted for greater accessibility. Programs and resources considered accessible, or those only requiring simple adaptations, were most commonly identified for auditory and movement needs, followed by communication and visual needs. Cognitive accessibility was addressed less frequently, highlighting a significant gap for individuals with intellectual or cognitive challenges. This suggests that while many programs/resources can be adapted for physical or sensory needs, there is limited consideration for cognitive diversity in pain education program or resource design. Furthermore, the exclusion of individuals with intellectual disability from several studies in this review highlights this as an area for future focus. While it can be challenging to accommodate wide variation in accessibility needs, one consideration could be utilizing existing accessibility guidelines (such as the UN disability inclusive communications guidelines112 or the Web-based Content Accessibility Guidelines 2.2113), and incorporating co-design approaches for future development to allow for inclusive and individualised content for people with accessibility needs. For example, recommendations for co-design for children with cerebral palsy makes particular mention of strategies to involve developmentally diverse children, such as advocating for children’s self-expression, using low-tech interactions to design high tech interventions, working together from organically occurring groups and involving parents, carers and siblings along with children themselves.114,115 Incorporating these recommendations into pain education development studies would help ensure that the resulting programs and resources are widely accessible, ultimately benefiting all users rather than only individuals with disabilities.
Strengths and Limitations
This review has several strengths, including a rigorous search and screening process and the supplemented use of artificial intelligence-informed data extraction as a “cross-check” with the human data extraction. While agreement was not formally quantified, the two approaches generally produced similar outputs, offering an added layer of assurance that key data were captured. The review examined programs and resources that extended beyond pain neuroscience education to include integration of self-management strategies for chronic pain. It additionally introduced a summary table and web page (https://doi.org/10.25909/31908319 and https://www.cp-pain.org.au/resources) designed to help researchers, clinicians, and clients identify useful resources. This feature supports the practical application of the review’s findings, making it easier to translate them into clinical practice.
The review does, however, have some limitations. The accessibility analysis provides general findings only, as it was neither mapped to established accessibility guidelines nor tested by individuals with accessibility needs. Neither options were possible given the broad scope of the review (considering cognition, movement, hearing, vision, and communication), and even within more specific categories of accessibility needs there will always be unique requirements for the individual person. As such it is not possible to definitively claim a program or resource is accessible or not, and instead we refer to pain education programs/resources as “likely accessible” or “with potential for accessibility with minimal adaptation”. This provides the user with some guidance on potential options, which they can further investigate. A Google search was used to complement the database searches to identify programs/resources which may be publicly available but not reported in scientific studies. Although the Google search was conducted in “incognito” mode, the results were likely still influenced by the location of the server (Adelaide, Australia). To minimise the impact of this, the authors emailed the PICH List Serv to ensure resources available outside of Australia were represented. As such, this is not considered a significant limitation. Furthermore, although formal quality appraisal is not usual practice in a scoping review, the included records varied substantially in methodological rigour and format (eg, Randomised controlled trials, non-randomised studies, books, websites, videos), and this heterogeneity should be considered when interpreting the findings. Finally, content analysis was only performed on programs/resources available in English language, or where the program/resource could be translated into English. As the review authors were only fluent in English, it was not deemed appropriate to perform content analysis on programs/resources in other languages. Further investigation of programs and resources available in other languages is an area for future work.
Conclusion
Many pain education programs and resources are available for children, adolescents and young adults aged 5–25 years with chronic pain. While over half of the identified pain education programs and resources have the potential for accessibility for those with communication, auditory, visual or movement impairment with minimal adaptation, suitability for people with cognitive impairment is lacking. Future pain education program/resource design and development should consider the needs of people with cognitive impairment to ensure equitable and accessible chronic pain management. These findings also highlight an opportunity for policymakers and clinical guideline developers to embed accessibility requirements, particularly cognitive accessibility, into the standards and recommendations guiding the development of pain education programs and resources.
Abbreviations
PCC, Population, Concept, Context; PICH, Pain in Child Health; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials and online (https://doi.org/10.25909/31908319 and https://www.cp-pain.org.au/resources)
Acknowledgments
The authors acknowledge the assistance of Ingrid Honan and Caitlin Doyle in the title and abstract screening phase. The authors also acknowledge the work of Jordan Hefferan in running the searches and assisting with title/abstract and full-text screening. The authors acknowledge the use of Microsoft Copilot (Generative Artificial Intelligence) in the editing of the manuscript. The authors acknowledge the use of Elicit (Generative Artificial Intelligence) as a ‘cross-check’ during data extraction.
Funding
This review was funded by a University of Adelaide Faculty of Health and Medical Science Early Grant Development Award.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–13. doi:10.1097/j.pain.0000000000001939
2. Zimmer Z, Fraser K, Grol-Prokopczyk H, Zajacova A. A global study of pain prevalence across 52 countries: examining the role of country-level contextual factors. Pain. 2022;163(9):1740–1750. doi:10.1097/j.pain.0000000000002557
3. Chambers CT, Dol J, Tutelman PR, et al. The prevalence of chronic pain in children and adolescents: a systematic review update and meta-analysis. PAIN. 2024; 165(10):2215–2234.
4. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
5. Coakley R, Wihak T, Kossowsky J, Iversen C, Donado C. The comfort ability pain management workshop: a preliminary, nonrandomized investigation of a brief, cognitive, biobehavioral, and parent training intervention for pediatric chronic pain. J Pediatr Psychol. 2018;43(3):252–265. doi:10.1093/jpepsy/jsx112
6. Moseley GL, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain. 2015;16(9):807–813. doi:10.1016/j.jpain.2015.05.005
7. McKinnon CT, Meehan EM, Harvey AR, Antolovich GC, Morgan PE. Prevalence and characteristics of pain in children and young adults with cerebral palsy: a systematic review. Dev Med Child Neurol. 2019;61(3):305–314. doi:10.1111/dmcn.14111
8. Ostojic K, Paget S, Kyriagis M, Morrow A. Acute and chronic pain in children and adolescents with cerebral palsy: prevalence, interference, and management. Arch Phys Med Rehabil. 2020;101(2):213–219. doi:10.1016/j.apmr.2019.08.475
9. Ostojic K, Paget SP, Morrow AM. Management of pain in children and adolescents with cerebral palsy: a systematic review. Dev Med Child Neurol. 2019;61(3):315–321. doi:10.1111/dmcn.14088
10. Ickmans K, Rheel E, Rezende J, Reis FJJ. Spreading the word: pediatric pain education from treatment to prevention. Arch Physiother. 2022;12(1):25. doi:10.1186/s40945-022-00151-4
11. Betting K, Laekeman M, De Kooning M, Carvalho GF. Critical appraisal of pediatric pain education materials and the integration of lifestyle factors: a scoping review. Disability Rehabil. 2025;1–23. doi:10.1080/09638288.2025.2595180
12. Peters MDJGC, P M, Munn Z, Tricco AC, Khalil H. Scoping Reviews. 2020. Available from: https://synthesismanual.jbi.global.
13. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Internal Med. 2018;169(7):467–473. doi: 10.7326/m18-0850
14. Bodenheimer T, Lorig K, Holman H, Grumbach K. Patient self-management of chronic disease in primary care. JAMA. 2002;288(19):2469–2475. doi:10.1001/jama.288.19.2469
15. Moseley GL, Leake HB, Beetsma AJ, et al. Teaching patients about pain: the emergence of pain science education, its learning frameworks and delivery strategies. J Pain. 2024;25(5). doi:10.1016/j.jpain.2023.11.008
16. Moseley GL, Nicholas MK, Hodges PW. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin J Pain. 2004;20(5):324–330. doi:10.1097/00002508-200409000-00007
17. Hurley-Wallace AL, Nowotny E, Schoth DE, Liossi C. Online multidisciplinary interventions for paediatric chronic pain: a content analysis. Eur J Pain. 2021;25(10):2140–2154. doi:10.1002/ejp.1827
18. Heathcote LC, Pate JW, Park AL, et al. Pain neuroscience education on youtube. PeerJ. 2019;7:e6603. doi:10.7717/peerj.6603
19. LeFort S, McGillion M. Promoting Chronic Pain Self-Management Education. International Association for the Study of Pain; 2021.
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71.
21. Amarante C. The Dream Machine. Tellwell Talent; 2022.
22. Andias R, Neto M, Silva AG. The effects of pain neuroscience education and exercise on pain, muscle endurance, catastrophizing and anxiety in adolescents with chronic idiopathic neck pain: a school-based pilot, randomized and controlled study. Physiother Theory Pract. 2018;34(9):682–691. doi:10.1080/09593985.2018.1423590
23. Andias R, Sa-Couto P, Silva AG. Blended-learning pain neuroscience education and exercise in high school students with chronic neck pain: a randomized controlled trial. PTJ. 2022;102(6):1–13. doi:10.1093/ptj/pzac048
24. Andrews NE, Ireland D, Vijayakumar P, et al. Acceptability of a pain history assessment and education chatbot (Dolores) across age groups in populations with chronic pain: development and pilot testing. JMIR Format Res. 2023;7:e47267. doi:10.2196/47267
25. Bickel J, Connelly M. Headache Relief Guide. Available from: https://www.headachereliefguide.com/about.php.
26. Boston Children’s Hospital. Chronic Pain as You’ve Never Heard It Before | The Comfort Ability Program. 2025. Available from: https://chronicpainasyouveneverhearditbefore.podbean.com/.
27. Brem P. Can pain neurophysiology education contribute to improving the functional abilities of chronic pain patients from a physiotherapeutic perspective? Manuelle Therapie. 2010;14(1):22–28.
28. MyCarePath Modules. Available from: https://mycarepath.ca/courses.
29. Cañeiro J, Ng L, Burnett A, Campbell A, O’Sullivan P. Cognitive functional therapy for the management of low back pain in an adolescent male rower: a case report. J Orthopaedic Sports Phys Ther. 2013;43(8):542–554.
30. Chen AT, Swaminathan A, Kearns WR, Alberts NM, Law EF, Palermo TM. Understanding user experience: exploring participants’ messages with a web-based behavioral health intervention for adolescents with chronic pain. J Med Internet Res. 2019;21(4):e11756. doi:10.2196/11756
31. Chen J, Zhang Y, Barandouzi ZA, et al. The effect of self-management online modules plus nurse-led support on pain and quality of life among young adults with irritable bowel syndrome: a randomized controlled trial. Int J Nurs Stud. 2022;132:104278. doi:10.1016/j.ijnurstu.2022.104278
32. Chronic Pain Australia. Kids In Pain - Chronic Pain Australia. 2024.
33. Coakley R, Bujoreanu S. Mobilizing the psychology evidence base for the treatment of pediatric chronic pain: the development, implementation, and impact of the Comfort Ability Program. Paediatric Neonatal Pain. 2020;2(4):148–159. doi:10.1002/pne2.12019
34. Cooke M, Richards J, Tjondronegoro D, et al. myPainPal: co-creation of a mHealth app for the management of chronic pain in young people. Inform Health Soc Care. 2021;46(3):291–305. doi:10.1080/17538157.2021.1892697
35. Cora Health Group. Flippin’ Pain. Available from: https://www.flippinpain.co.uk/#.
36. Creative Healing for Youth in Pain. Creative healing for youth in pain. Available from: https://mychyp.org.
37. Cunningham N. HELP Lab: healing Emotional Illness Pain. 2023. Available from: https://www.youtube.com/@MSUhelplab.
38. Davis KD. How does your brain respond to pain? (TED-Ed). 2014. Available from https://www.youtube.com/watch?v=I7wfDenj6CQ.
39. Dawson S, Scott E, Elder L, Omodior E, B.e.a.r HAHK. Pain: a Pediatric Psychosocial Chronic Pain Protocol. Therapeut Recreation J. 2023;57(2). doi:10.18666/TRJ-2023-V57-I2-11885
40. de la Vega R, Ritterband L, Palermo TM. Assessing digital health implementation for a pediatric chronic pain intervention: comparing the RE-AIM and BIT frameworks against real-world trial data and recommendations for future studies. J Med Internet Res. 2020;22(9):e19898. doi:10.2196/19898
41. de la Vega R, Roset R, Galán S, Miró J. Fibroline: a mobile app for improving the quality of life of young people with fibromyalgia. J Health Psychol. 2016;23(1):67–78. doi:10.1177/1359105316650509
42. Dudeney J, Scott AJ, Hathway T, et al. Internet-delivered psychological pain-management for young adults with chronic pain: an investigation of clinical trial data. J Pain. 2024;25(6):104447. doi:10.1016/j.jpain.2023.12.004
43. Eyer JC, Thorn BE. The Learning About My Pain study protocol: reducing disparities with literacy-adapted psychosocial treatments for chronic pain, a comparative behavioral trial. J Health Psychol. 2016;21(9):2063–2074. doi:10.1177/1359105315570985
44. Fales J, Palermo TM, Law EF, Wilson AC. Sleep outcomes in youth with chronic pain participating in a randomized controlled trial of online cognitive-behavioral therapy for pain management. Behav Sleep Med. 2015;13(2):107–123. doi:10.1080/15402002.2013.845779
45. Fors A, Wallbing U, Alfvén G, et al. Effects of a person-centred approach in a school setting for adolescents with chronic pain-The HOPE randomized controlled trial. Eur J Pain. 2020;24(8):1598–1608. doi:10.1002/ejp.1614
46. Galán-Martín MA, Montero-Cuadrado F, Lluch-Girbes E, Coca-López MC, Mayo-Iscar A, Cuesta-Vargas A. Pain neuroscience education and physical exercise for patients with chronic spinal pain in primary healthcare: a randomised trial protocol. BMC Musculoskel Disorders. 2019;20(1). doi:10.1186/s12891-019-2889-1
47. German Paediatric Pain Centre. Our aim: you’ve got control of your pain! Available from: https://www.deutsches-kinderschmerzzentrum.de/en/.
48. German Pediatric Pain Centre. myHeadeggs. Available from: http://headeggs.org/.
49. Gmuca S, Weiss PF, McGill M, et al. The feasibility and acceptability of resilience coaching for adolescent chronic musculoskeletal pain: a single-arm pilot trial. Children. 2022;9(10):1432–N.PAG. doi:10.3390/children9101432
50. Goldenberg D, Payne LA, Hayes LP, Zeltzer LK, Tsao JCI. Peer mentorship teaches social tools for pain self-management: a case study. J Pain Manag. 2013;6(1):61–68.
51. Groß M, Warschburger P. Evaluation of a cognitive-behavioral pain management program for children with chronic abdominal pain: a randomized controlled study. Int J Behav Med. 2013;20(3):434–443. doi:10.1007/s12529-012-9228-3
52. Hall AL, Karvounides D, Gelfand AA, et al. Improving the patient experience with migraine camp, a one-day group intervention for adolescents with chronic headache and their parents. Headache. 2019;59(8):1392–1400. doi:10.1111/head.13570
53. Hickman C. The acceptability, feasibility, and preliminary effects of a cognitive behavioral skills building intervention in adolescents with chronic daily headaches. 2012:379.
54. Hoiyan KL. Helping adolescents with chronic pain. Austr Psycholog Soc. 2016;2016:1.
55. Kisling S, Claus BB, Stahlschmidt L, Wager J. The efficacy of an educational movie to improve pain and dysfunctional behavior in school children: a randomized controlled trial. Eur J Pain. 2021;25(7):1612–1621. doi:10.1002/ejp.1777
56. Kohut SA, Stinson JN, Ruskin D, et al. iPeer2Peer program: a pilot feasibility study in adolescents with chronic pain. PAIN. 2016;157(5):1146–1155. doi:10.1097/j.pain.0000000000000496
57. Lalloo C, Nishat F, Zempsky W, et al. Characterizing user engagement with a digital intervention for pain self-management among youth with sickle cell disease and their caregivers: subanalysis of a randomized controlled trial. J Med Internet Res. 2022;24(8). doi:10.2196/40096
58. Lauder GR. Complex Regional Pain Syndrome (CRPS) Explained: For Teenagers, by Teenagers “Info That Clicks”. Xlibris Corp; 2010.
59. Law EF, Beals-Erickson SE, Noel M, Claar R, Palermo TM. Pilot randomized controlled trial of internet-delivered cognitive-behavioral treatment for pediatric headache. Headache. 2015;55(10):1410–1425. doi:10.1111/head.12635
60. Law EF, Murphy LK, Palermo TM, Law EF, Murphy LK, Palermo TM. Evaluating treatment participation in an internet-based behavioral intervention for pediatric chronic pain. J Pediatric Psychol. 2012;37(8):893–903. doi:10.1093/jpepsy/jss057
61. Law EF, Tham SW, Howard W, Ward TM, Palermo TM. Executive functioning and self-management processes mediate the relationship between insomnia and pain-related disability. J Pain. 2024;25(1):273–283. doi:10.1016/j.jpain.2023.08.010
62. Leake HB, Heathcote LC, Ferencz N, et al. Codesign and evaluation of pain science messages on social media with adolescents with a history of chronic pain. J Pain. 2024;25(9). doi:10.1016/j.jpain.2024.104580
63. Lynch-Jordan AM, Sil S, Peugh J, Cunningham N, Kashikar-Zuck S, Goldschneider KR. Differential changes in functional disability and pain intensity over the course of psychological treatment for children with chronic pain. PAIN. 2014;155(10):1955–1961. doi:10.1016/j.pain.2014.06.008
64. Major J, Varga ZK, Gyimesi-Szikszai A, Ádám S. A two-week inpatient programme with a booster improved long-term management of severe chronic paediatric pain. J Child Health Care. 2017;21(2):171–180. doi:10.1177/1367493517697479
65. Marcos-Martín F, González-Ferrero L, Martín-Alcocer N, Paris-Alemany A, La Touche R. Multimodal physiotherapy treatment based on a biobehavioral approach for patients with chronic cervico-craniofacial pain: a prospective case series. Physiother Theory Pract. 2018;34(9):671–681. doi:10.1080/09593985.2017.1423522
66. Marti L, Castarlenas E, Sole E, de la Vega R, Miro J. Video-based pain education in schools: a study with adolescents. Clin J Pain. 2021;37(3):199–205. doi:10.1097/AJP.0000000000000906
67. Matthie N, Jenerette C. Knowledge and experience of in-home virtual reality for chronic pain in sickle cell disease. J Pain. 2024;25(12):104668. doi:10.1016/j.jpain.2024.104668
68. Mead J. Translating Emma. Dettori Publishing; 2025.
69. Meg Foundation. Chronic Pain Resources. https://www.megfoundationforpain.org/chronic-pain-resources/.
70. Moore P, Bird J. My PainToolkit: for young people and teenagers living with pain.
71. Noel M, Petter M, Parker JA, Chambers CT. Cognitive behavioral therapy for pediatric chronic pain: the problem, research, and practice. J Cognit Psychother. 2012;26(2):143–156. doi:10.1891/0889-8391.26.2.143
72. PainBytes. Available from: https://aci.health.nsw.gov.au/chronic-pain/painbytes.
73. Pack R, Gilliland R, Mecham A. The treatment of central sensitization in an adolescent using pain neuroscience education and graded exposure to activity: a case report. Physiother Theory Pract. 2020;36(10):1164–1174. doi:10.1080/09593985.2018.1551454
74. Pain Revolution. Pain Revolution: pain Facts. Available from: https://www.painrevolution.org/painfacts.
75. Palermo TM, de la Vega R, Murray C, Law E, Chuan Z, Zhou C. A digital health psychological intervention (WebMAP Mobile) for children and adolescents with chronic pain: results of a hybrid effectiveness-implementation stepped-wedge cluster randomized trial. PAIN. 2020;161(12):2763–2774. doi:10.1097/j.pain.0000000000001994
76. Palermo TM, Law EF, Fales J, Bromberg MH, Jessen-Fiddick T, Tai G. Internet-delivered cognitive-behavioral treatment for adolescents with chronic pain and their parents: a randomized controlled multicenter trial. PAIN. 2016;157(1): 174–185.
77. Palermo TM, Law EF, Zhou C, Holley AL, Logan D, Tai G. Trajectories of change during a randomized controlled trial of internet-delivered psychological treatment for adolescent chronic pain: how does change in pain and function relate? PAIN. 2015;156(4):626–634. doi:10.1097/01.j.pain.0000460355.17246.6c
78. Palermo TM, Zempsky WT, Dampier CD, et al. iCanCope with Sickle Cell Pain: design of a randomized controlled trial of a smartphone and web-based pain self-management program for youth with sickle cell disease. Contemp Clin Trials. 2018;74(101242342):88–96. doi:10.1016/j.cct.2018.10.006
79. Pas R, Meeus M, Malfliet A, et al. Development and feasibility testing of a pain neuroscience education program for children with chronic pain: treatment protocol. Braz J Phys Ther. 2018;22(3):248–253. doi:10.1016/j.bjpt.2018.02.004
80. Pas R, Rheel E, Van Oosterwijck S, et al. Pain neuroscience education for children with functional abdominal pain disorders: a randomized comparative pilot study. J Clin Med. 2020;9(6). 1797. doi:10.3390/jcm9061797.
81. Pate J. Zoe and Zak’s Pain Hacks. 2022.
82. Pate JW, Heathcote LC, Simons LE, Leake H, Moseley GL. Creating online animated videos to reach and engage youth: lessons learned from pain science education and a call to action. Paediatr Neonatal Pain. 2020;2(4):131–138. doi:10.1002/pne2.12015
83. Reis F, Palermo TM, Acalantis L, et al. “A journey to learn about pain”: the development and validation of a comic book about pain neuroscience education for children. Braz J Phys Ther. 2022;26(1):100348. doi:10.1016/j.bjpt.2021.04.009
84. RetrainPain. RetrainPain English resources. Available from: https://www.retrainpain.org/languages/english.
85. Schatz J, Schlenz AM, McClellan CB, et al. Changes in Coping, pain, and activity after cognitive-behavioral training: a randomized clinical trial for pediatric sickle cell disease using smartphones. Clin J Pain. 2015;31(6): 536–547.
86. Scottish Government. Management of Chronic Pain in Children and Young People: Summary; 2018.
87. Shaygan M, Jaberi A. The effect of a smartphone-based pain management application on pain intensity and quality of life in adolescents with chronic pain. Sci Rep. 2021;11(1):6588. doi:10.1038/s41598-021-86156-8
88. Shaygan M, Jahandide Z, Zarifsanaiey N. An investigation of the effect of smartphone-based pain management application on pain intensity and the quality-of-life dimensions in adolescents with chronic pain: a cluster randomized parallel-controlled trial. Qual Life Res. 2021;30(12):3431–3442. doi:10.1007/s11136-021-02891-5
89. Shear D, Harrison LE, O’Brien S, et al. Rapid transition to virtual assessment and treatment in an interdisciplinary randomized clinical trial for youth with chronic pain: adaptations and implications for future trials. Clin J Pain. 2022;38(7):459–469. doi:10.1097/AJP.0000000000001040
90. Sil S, Lai K, Lee JL, et al. Preliminary evaluation of the clinical implementation of cognitive-behavioral therapy for chronic pain management in pediatric sickle cell disease. Complementary Ther Med. 2020;49. doi:10.1016/j.ctim.2020.102348
91. Sil S, Lee JL, Klosky J, et al. The comfort ability program for adolescents with sickle cell pain: evaluating feasibility and acceptability of an inpatient group-based clinical implementation. Pediatr Blood Cancer. 2021;68(6):1–10. doi:10.1002/pbc.29013
92. Simmonds MK, Dick BD, Verrier MJ, et al. The effect of a brief physician-delivered neurobiologically oriented, cognitive behavioural therapy (Brief-CBT) intervention on chronic pain acceptance in youth with chronic pain—A randomized controlled trial. Children. 2022;9(9). doi:10.3390/children9091293
93. Simons LE, Harrison LE, Boothroyd DB, et al. A randomized controlled trial of graded exposure treatment (GET living) for adolescents with chronic pain. Pain. 2024;165(1):177–191. doi:10.1097/j.pain.0000000000003010
94. Slater H, Stinson JN, Jordan JE, et al. Evaluation of digital technologies tailored to support young people’s self-management of musculoskeletal pain: mixed methods study. J Med Internet Res. 2020;22(6):e18315. doi:10.2196/18315
95. ImaginAction. Available from: https://imaginaction.stanford.edu/manage-my-chronic-pain/.
96. Stinson JN, Lalloo C, Harris L, et al. iCanCope with Pain™: user-centred design of a web- and mobile-based self-management program for youth with chronic pain based on identified health care needs. Pain Res Manag. 2014;19(5):257–265. doi:10.1155/2014/935278
97. The Hospital for Sick Children. What is chronic pain? 2021. Available from: https://www.youtube.com/watch?v=EL1E54nH_7c.
98. The Hospital for Sick Children. Chronic pain: how to treat and manage in older children. Available from: https://www.aboutkidshealth.ca/healthaz/pain/anaesthesia/chronic-pain-how-to-treat-and-manage-in-older-children/?hub=chronicpain&hubSite=https://www.aboutkidshealth.ca/&collectionHub=pain&topic=chronicpain.
99. The Hospital for Sick Children. Power Over Pain Youth Portal. Available from: https://www.popyouth.ca/.
100. Trautmann E, Kröner-Herwig B. A randomized controlled trial of Internet-based self-help training for recurrent headache in childhood and adolescence. Behav Res Ther. 2010;48(1):28–37. doi:10.1016/j.brat.2009.09.004
101. Foundation USP. Living Well with Chronic Pain. Available from: https://uspainfoundation.org/resources/.
102. University of Oxford. Advice on chronic pain for young people. 2023. Available from: https://www.psych.ox.ac.uk/news/advice-on-chronic-pain-for-young-people.
103. Voerman JS, Remerie S, Westendorp T, et al. Effects of a guided internet-delivered self-help intervention for adolescents with chronic pain. J Pain. 2015;16(11):1115–1126. doi:10.1016/j.jpain.2015.07.011
104. Wager J, Stahlschmidt L, Heuer F, Troche S, Zernikow B. The impact of a short educational movie on promoting chronic pain health literacy in school: a feasibility study. Eur J Pain. 2018;22(6):1142–1150. doi:10.1002/ejp.1202
105. Wallbing U, Nilsson S, Wigert H, Lundberg M. Adolescents’ experiences of Help Overcoming Pain Early—A school based person-centred intervention for adolescents with chronic pain. Paediatric Neonatal Pain. 2023;5(4):119–126. doi:10.1002/pne2.12113
106. Managing Chronic Pain in Schools. Available from: https://www.wch.sa.gov.au/patients-visitors/children/care-and-support/paediatric-chronic-pain-service/managing-chronic-pain-in-schools.
107. Zimney K, Louw A, Puentedura EJ. Use of Therapeutic Neuroscience Education to address psychosocial factors associated with acute low back pain: a case report. Physiother Theory Pract. 2014;30(3):202–209. doi:10.3109/09593985.2013.856508
108. Zoffness R. The Chronic Pain & Illness Workbook for Teens: CBT and Mindfulness-Based Practices to Turn the Volume Down on Pain. Instant Help Books; 2019.
109. Kerns RD, Burgess DJ, Coleman BC, et al. Self-management of chronic pain: psychologically guided core competencies for providers. Pain Med. 2022;23(11):1815–1819. doi:10.1093/pm/pnac083
110. Downs J, Keeley J, Skoss R, et al. Perspectives on the essential skills of healthcare decision making in children and adolescents with intellectual disability. Int J Equity Health. 2024;23(1):119. doi:10.1186/s12939-024-02204-5
111. Saxby N, Ford K, Beggs S, Battersby M, Lawn S. Developmentally appropriate supported self-management for children and young people with chronic conditions: a consensus. Patient Educ Couns. 2020;103(3):571–581. doi:10.1016/j.pec.2019.09.029
112. United Nations. UN Disability-Inclusive Communications Guidelines. Available from: https://unprpd.org/new/wp-content/uploads/2023/12/UN_Disability-Inclusive_Comms_Guidelines_FINAL-d8a.pdf.
113. Web Content Accessibility Guidelines. 2 2. W3C World Wide Web Consortium Recommendation. Available from: https://www.w3.org/TR/WCAG22/.
114. Rajapakse R, Brereton M, Sitbon L. A respectful design approach to facilitate codesign with people with cognitive or sensory impairments and makers. CoDesign. 2021;17(2):159–187. doi:10.1080/15710882.2019.1612442
115. Borzenkova G, Tang J, Niedderer K. Co-designing with children with cerebral palsy: context and co-design principles. IASDR 2023: Life-Changing Design. 2023. doi:10.21606/iasdr.2023.614
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Management of Chronic Migraine in Children and Adolescents: Where are We in 2022?
Gibler RC, Knestrick KE, Reidy BL, Lax DN, Powers SW
Pediatric Health, Medicine and Therapeutics 2022, 13:309-323
Published Date: 9 September 2022
Identifying and Managing Suicidality in Children and Adolescents with Chronic Pain: Evidence-Based Treatment Strategies
Rice T, Sher L
Psychology Research and Behavior Management 2022, 15:3561-3574
Published Date: 5 December 2022
The Psychosocial Characteristics and Somatosensory Function of Children and Adolescents Who Meet the Criteria for Chronic Nociplastic Pain
Ocay DD, Ross BD, Moscaritolo L, Ahmed N, Ouellet JA, Ferland CE, Ingelmo PM
Journal of Pain Research 2023, 16:487-500
Published Date: 15 February 2023
Disease Burden of Dysmenorrhea: Impact on Life Course Potential
MacGregor B, Allaire C, Bedaiwy MA, Yong PJ, Bougie O
International Journal of Women's Health 2023, 15:499-509
Published Date: 3 April 2023
Non-Cognitive Behavioral Therapy Psychological Interventions May Not Make the Difference in Children and Adolescents With Chronic Pain
Perlman L, Malka N, Terry O, Nguyen A, Guimarães Ferreira Fonseca L, Ingelmo JI, Ingelmo P
Journal of Pain Research 2025, 18:1451-1464
Published Date: 20 March 2025