")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Management of Chronic Migraine in Children and Adolescents: Where are We in 2022?
Authors Gibler RC, Knestrick KE, Reidy BL, Lax DN, Powers SW
Received 28 April 2022
Accepted for publication 10 August 2022
Published 9 September 2022 Volume 2022:13 Pages 309—323
DOI https://doi.org/10.2147/PHMT.S334744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Robert C Gibler,1 Kaelynn E Knestrick,1 Brooke L Reidy,1,2 Daniel N Lax,3,4 Scott W Powers1,2,4
1Division of Behavioral Medicine and Clinical Psychology, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA; 2Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, OH, USA; 3Division of Neurology, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA; 4Headache Center, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA
Correspondence: Robert C Gibler, Division of Behavioral Medicine and Clinical Psychology, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA, Email [email protected]
Abstract: Migraine is a neurological disorder that affects millions of children and adolescents worldwide. Chronic migraine is a subtype of migraine in which patients experience headaches for more days than not each month, with accompanying symptoms of phonophobia, photophobia, nausea or vomiting for most of these headaches. The burden and impact of chronic migraine in the daily lives of children and adolescents is substantial, requiring a holistic, multidisciplinary, and biopsychosocial approach to conceptualization and treatment. The purpose of this review is to provide a comprehensive “ 2022” overview of acute and preventive treatments for the management of chronic migraine in youth. We first describe diagnostic criteria for chronic migraine and highlight the state of evidence for acute and preventive treatment in children and adolescents. We then discuss emerging treatments currently receiving rigorous clinical research effort, special considerations for the treatment of chronic migraine in children and adolescents, and avenues for improving existing treatments and expanding access to evidence-based care.
Keywords: chronic migraine, migraine, headache, children, adolescents, pediatrics
Introduction
Migraine is a primary headache disorder affecting up to 7 million children and adolescents in the United States.1–3 Females are disproportionately affected by migraine, and the prevalence of the disease increases over the course of development.4,5 The impact of migraine on quality of life among children and adolescents is comparable to that of other chronic illnesses such as rheumatic disease and cancer,6 and unfortunately, migraine tends to persist into adulthood.7
Chronic migraine is a subtype of migraine that affects approximately 1–2% of youth,5 and is typically characterized by a gradual progression (ie, chronification) of episodic symptoms over the course of weeks or months.8 Youth with chronic migraine may experience co-occurring medical concerns for which subspecialty care may be required, including abdominal or musculoskeletal pain complaints, clinically significant sleep disturbances, and other neurological conditions such as epilepsy.9 Children and adolescents with chronic migraine often report substantial impairment in school-related functioning,10,11 challenges related to engaging in leisure activities and spending time with friends,12 and difficulties in family relationships.13,14 Thus, the management of chronic migraine in children and adolescents requires a holistic, integrative, and multimodal intervention approach that incorporates both medical and non-pharmacological treatments to address the symptoms and functional impairment associated with this debilitating headache disorder.
The purpose of this narrative review is to provide an overview of current best practices for acute and preventive treatment of chronic migraine in children and adolescents, direct attention to the most recent developments in the field, and emphasize important avenues for clinical research. In this review, we use guidelines set forth by the American Academy of Neurology (AAN) and the American Headache Society as frameworks to highlight treatments that represent the current standard of care for pediatric patients with chronic migraine and identify relevant gaps in intervention research. We then highlight treatment options that are currently receiving rigorous clinical research attention, provide a discussion of novel directions for research focused on improving existing interventions for chronic migraine in pediatric populations, and describe targeted research strategies that may expand access to evidence-based care for these patients and their families.
Chronic Migraine: Evaluation and Differential Diagnosis Considerations
Accurate diagnosis of chronic migraine requires thorough physical and neurologic examinations and assessment of headache history including pain location(s), headache frequency, severity, and associated symptoms. The diagnosis of migraine and chronic migraine is made in accordance with the International Classification of Headache Disorders, 3rd edition (ICHD-315) criteria. Accurate diagnosis typically requires a recorded history of headaches and symptoms that occur during an attack using a headache diary.
The majority of treatment-seeking patients present with migraine or probable migraine; a diagnosis of probable migraine may be assigned when a patient meets all but one of the ICHD-3 diagnostic criteria for migraine. As Table 1 highlights, migraine is characterized by headaches of moderate-to-severe intensity that are accompanied by nausea, vomiting, photophobia, and/or phonophobia. The primary differentiating feature between youth with migraine and chronic migraine relates to headache frequency, as youth diagnosed with chronic migraine must experience 15 or more days with headache per month for at least 3 months, and the majority of these headaches must have migraine features.15 Some patients experience an aura (ie, a “warning signal”) with their migraine, which include visual, sensory, motor, and other central nervous system disturbances that precede headache onset.
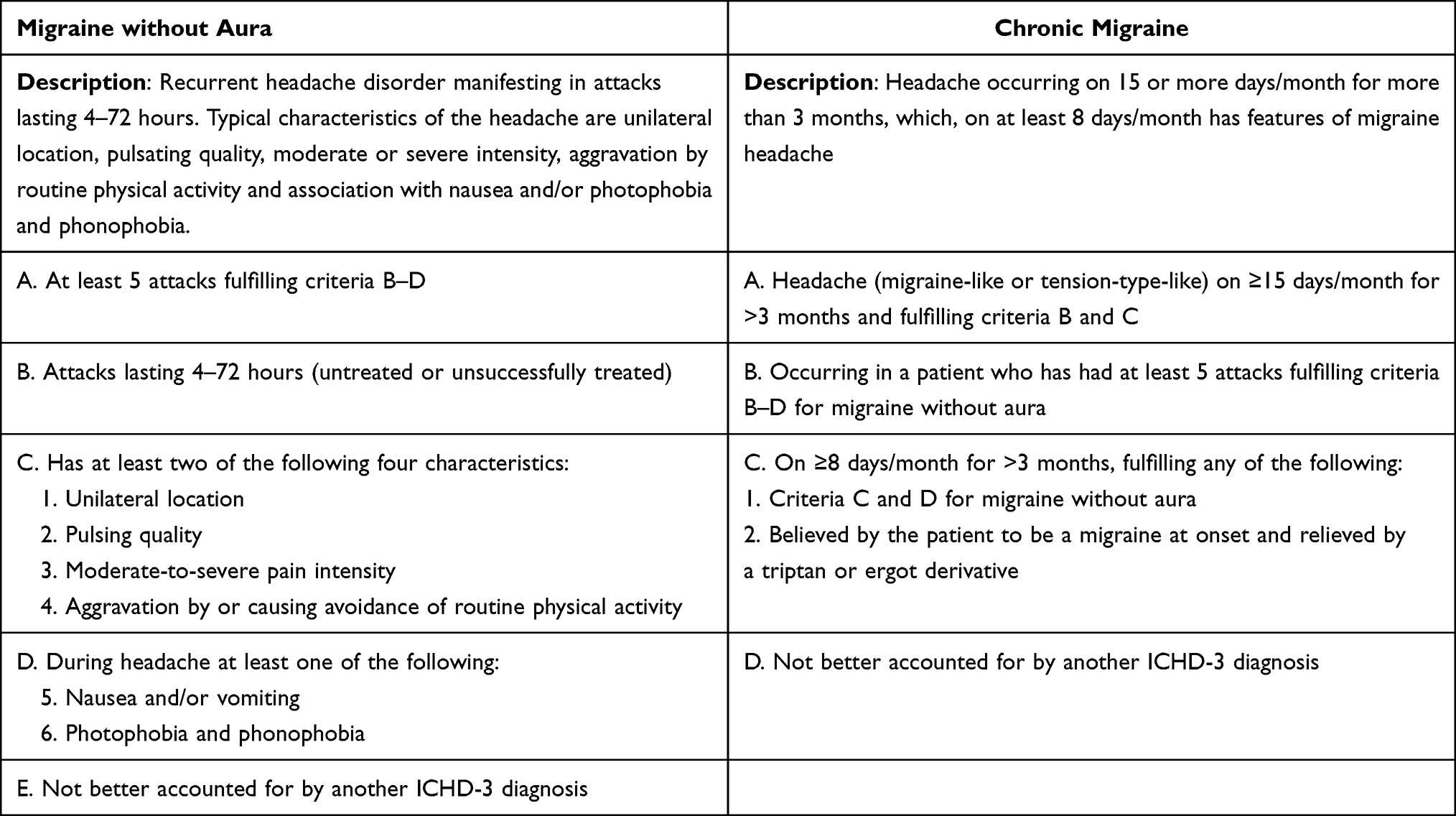 |
Table 1 International Classification of Headache Disorders (ICHD-3) Diagnostic Criteria for Migraine without Aura and Chronic Migraine |
Some children and adolescents also present with chronic tension-type headache (CTTH), a headache disorder in which the frequency of headache episodes is similar to that of chronic migraine. However, patients with CTTH typically do not experience migraine features such as photophobia, phonophobia, and severe nausea or vomiting, and their headaches are typically not as severe in intensity. In rare cases, youth may present for treatment with new daily persistent headache (NDPH), a primary headache disorder characterized by a rapid onset of unremitting headache. Patients with NDPH may or may not have migraine features with their continuous headache. Patients often recall the date their unremitting headache began due to its abrupt onset, and therefore do not endorse a history of increasing headache frequency. Chronic migraine can also be characterized by daily or continuous headache presentations; however, this presentation—as highlighted above—typically occurs via gradual chronification of headaches over time.
One other type of continuous headache presentation is hemicrania continua. Patients with this headache disorder may experience migraine-like symptoms with their continuous headache, but their pain is isolated to one half of the face and head with ipsilateral autonomic features such as conjunctival injection or with agitation, and the headache is responsive to one particular drug (indomethacin). This is incredibly rare in youth16 but is important to consider in those with unremitting unilateral pain that is refractory to treatment. Similarly, clinicians should consider idiopathic intracranial hypertension as a possible diagnosis for pediatric patients, as these youth most commonly present with intermittent diffuse headache that often occurs with migraine-like symptoms such as nausea and vomiting. However, IIH is most clearly identified by the presence of papilledema, significant visual disturbances (eg, blurred or double vision), tinnitus, and neck stiffness.17
Treatment Planning for Pediatric Patients with Chronic Migraine
Once a chronic migraine diagnosis has been established, a biopsychosocial approach to care that incorporates both medical treatment and non-medicine intervention strategies is recommended. The gold-standard biopsychosocial intervention plan incorporates acute treatment, preventive treatment, healthy lifestyle habit recommendations, and relaxation and/or cognitive-behavioral interventions. Goals of treatment include reducing headache frequency, reducing disability associated with headaches, and improving the child or adolescent’s quality of life.18 The following subsections will review each of these treatment components in more detail, and a summary of the reviewed acute and preventive treatment options is presented in Table 2.
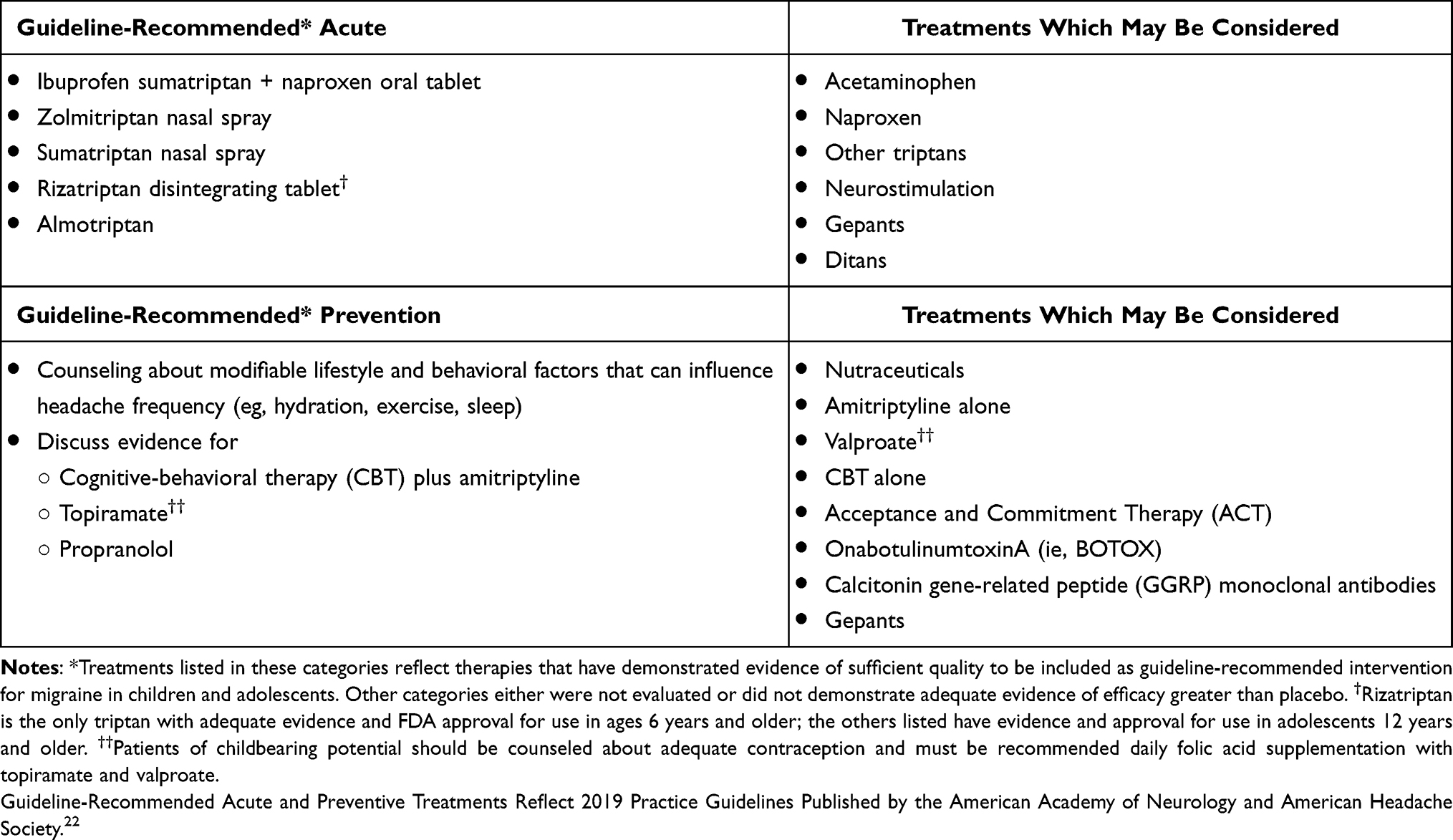 |
Table 2 Summary of Reviewed Acute and Preventive Treatment Options for Chronic Migraine in Children and Adolescents. |
One challenge that can complicate a child or adolescent’s diagnostic picture and treatment planning relates to use of acute medications. Some youth with migraine can experience headache chronification related to overuse of analgesic or headache rescue medications (see Acute Treatments section for more information). Medication-overuse headache (MOH) can be diagnosed if a patient with a pre-existing primary headache disorder (eg, migraine, chronic migraine) uses acute medication on 10 or 15 (depending on the medication) or more headache days per month for more than 3 months. Research suggests that approximately half of youth with chronic migraine overuse acute medications to manage their symptoms.19
According to ICHD-3 criteria, a diagnosis of chronic migraine should still be assigned even if a patient also meets criteria for MOH. This is notable because epidemiologic studies have shown that the estimated prevalence of chronic migraine decreases from approximately 2% to roughly 0.8% when children and adolescents with MOH are excluded.19 Thus, it is imperative to diagnose MOH where appropriate to guide appropriate treatment planning and counseling. For patients with comorbid chronic migraine and MOH, a comprehensive acute medication weaning plan should be established. An emphasis on prevention therapy is also especially important for patients with MOH.20
Acute Treatments
Pharmacological Treatments
The purpose of acute migraine treatment is to ameliorate pain and associated symptoms that occur during an attack, minimize side effects, and facilitate a return to typical functioning as quickly as possible.21 Headache specialists work with school systems and caregivers to ensure that children and adolescents are able to access acute treatments in school and at home to treat headaches at onset and minimize the disruptive impact of migraine on daily life. The most recent (2019) guidelines from the AAN emphasize early intervention that is tailored to the specific features of an individual’s headache attack.22
The most commonly studied and prescribed acute migraine medications generally fall into three categories: nonsteroidal anti-inflammatory drugs (NSAIDs) (eg, ibuprofen, naproxen), analgesics (eg, acetaminophen), and the migraine-specific triptans (eg, sumatriptan). In addition, novel therapies known as “gepants” and “ditans” are used in adults and will be discussed later. Current evidence supports use of ibuprofen as an initial treatment for both children and adolescents experiencing an acute migraine attack. Naproxen and diclofenac are commonly used as well, though with less objective evidence for their efficacy. Oral sumatriptan plus naproxen or almotriptan may be also be prescribed for adolescents aged 12 and older. For patients who cannot tolerate oral formulations, sumatriptan and zolmitriptan are United States Food and Drug Administration (FDA) approved in nasal spray formulations for ages 12 and older. Of the seven triptans available, rizatriptan is the only FDA-approved triptan for use in children down to age 6.
Antiemetic treatments should also be offered for youth who commonly experience nausea and vomiting with migraine, as none of the available treatments demonstrate significant efficacy for treatment of these symptoms.22 Dopamine antagonists such as prochlorperazine, chlorpromazine, promethazine and metoclopramide have pain relieving attributes in addition to their antiemetic characteristics23 but patients should be warned about the potential for extrapyramidal side effects such as muscle stiffness, akathisia or agitation which is more common with recurrent use, in younger patients, and among those already taking antidopaminergic agents.24 Finally, ondansetron has not demonstrated pain relief but may be considered for those with prior adverse reaction to antidopaminergic agents or other contraindications to them.25 It is generally safe but may cause QT prolongation and dysrhythmia, especially with recurrent use.26
Because overuse of triptans and analgesics can be associated with MOH27 and migraine chronification,28 clinicians should recommend that all abortive medications be used on no more than three headache days per week21 and triptans be used no more than 2 days per week.29 There are currently no evidence-based recommendations to guide treatment of MOH in children and adolescents. In clinical practice, management of MOH may include abrupt cessation or weaning of acute medications with immediate or later initiation of preventive therapy.30 A 6-week washout period of all acute medications has been shown to result in recovery of specific gene expression changes related to medication overuse.29,31
Neurostimulation
Given that pill-based therapies can be associated with the development of medication overuse headache and migraine chronification, considerable clinical research effort has been dedicated to the development of nonpharmacologic treatment options for acute migraine management. Neurostimulation (also termed neuromodulation) has gained attention in the adult migraine literature as an alternative approach to migraine management for patients who do not respond to available pill-based treatments. Neuromodulation aims to inhibit pain signaling by delivering electrical impulses to nerves involved in sensory processing and pain perception. A number of non-invasive (eg, single-pulse transcranial magnetic stimulation or vagal nerve stimulation) and invasive (eg, occipital nerve stimulation) techniques have been developed and tested in adults with migraine, and these are generally associated with fewer side effects relative to traditional pharmacologic treatment options (see32 for review). The following two devices are FDA-cleared for use in adolescents with migraine.
A non-invasive vagus nerve stimulation (nVNS) device is FDA approved for acute and preventive therapy of migraine and other headache disorders in adults and adolescents over age 12. The device is held at the neck for two cycles of 1–2 minutes, which can then be repeated after 20 minutes and again after 2 hours if needed. A small open-label study by Grazzi et al33 showed that nearly half (46.8%) of attacks were effectively treated without need for rescue medication and did not report any device-related adverse events. This pilot study provides the foundation for larger studies of nVNS for acute and preventive migraine therapy in adolescents.
Recently, an open-label study conducted by Hershey et al34 examined the safety, tolerability, and initial efficacy of a remote electrical neuromodulation (REN) device for treatment of acute migraine attacks among adolescents with migraine. This sample included a subset of participants who met criteria for chronic migraine based on their number of monthly headaches with migraine features. In the study, participants used the REN device—which was worn on the lateral upper arm—to deliver electrical stimulation during four migraine attacks over an 8-week period. Results showed that use of the device was not associated with any significant adverse events or participant study withdrawal; 71% of the participants experienced pain relief and 35% achieved pain freedom within 2 hours of symptom onset. Sustained pain relief was demonstrated among 90% of the participants at 24 hours. These preliminary data resulted in FDA clearance for use among adolescents for acute treatment of migraine.
Further studies are underway to assess the utility of the REN device in the Emergency Department setting, and others are being planned as a preventive option. Though preliminary, the promising findings discussed above suggest that the safety and efficacy of REN should be tested in a larger, randomized placebo-controlled trial to determine whether this acute treatment option could be integrated into routine clinical practice, or even in the Emergency Department setting for youth with chronic migraine, particularly those who present with comorbid MOH.
Preventive Treatments
Lifestyle Modifications
Counseling patients about the roles of lifestyle and behavioral factors that reduce the likelihood of headaches occurring is a primary emphasis of preventive care. Inadequate hydration, skipping meals, poor sleep, and insufficient exercise are factors associated with increased headache risk.35,36 Conversely, engaging in routine aerobic activity, eating regular meals, getting sufficient sleep, and obtaining sufficient daily fluid intake can reduce headache frequency and intensity.37–39
Recently, Robblee and Starling40 published practical guidelines for clinicians with detailed information about lifestyle factors that promote migraine prevention. These guidelines recommend that clinicians provide patients with guidelines about obtaining a sufficient number of hours of sleep for their developmental stage (eg, 9–12 hours for school-age children; 8–10 hours for teenagers); practicing good sleep hygiene (eg, maintaining a consistent sleep-wake schedule, discontinuing use of electronics 30–60 minutes before bedtime; and practicing a consistent bedtime routine that can incorporate relaxation practices); maintaining a healthy and well-balanced diet that includes protein, leafy green vegetables, and fruit; avoiding skipping meals; engaging in regular aerobic exercise; and obtaining adequate daily fluid intake. For teenagers with chronic migraine, between 80 and 100 ounces of fluid per day is recommended.
Pharmacological Treatments
A variety of medications are currently used for pediatric migraine prevention, and include antidepressants (eg, amitriptyline), antiepileptics (eg, topiramate, gabapentin), and calcium channel blockers (eg, flunarizine).41 One preventive medication that is frequently used as a first-line drug therapy is amitriptyline, which is a tricyclic antidepressant that has shown to be effective in reducing headache frequency and disability in children while minimizing side effects when titrated slowly.42 Topiramate, a drug of the anticonvulsant class, is the only FDA-approved pediatric preventive migraine medication. Although topiramate has been shown to reduce headache frequency in youth,22,43 it is associated with more side effects than amitriptyline.44 Valproic acid, another anticonvulsant, has shown efficacy in youth with migraine, but its teratogenic (class X) and ovarian effects limit its use in females.45
Practice guidelines emphasize a 50% reduction in headache frequency as a “benchmark” for which the effectiveness of a preventive treatment can be evaluated. That all said, it should be noted that the largest comparative effectiveness trial of preventative medication for youth with migraine to date—the Childhood and Adolescent Migraine Prevention (CHAMP) trial—was discontinued early due to futility after interim results revealed that amitriptyline and topiramate were not superior to placebo in reducing headache days.44 Results from this study showed that up to 70% of youth in both the active drug and placebo groups exhibited a 50% reduction in headache days over the course of the trial. Further, meta-analytic evidence has demonstrated that there are limited data to support use of medication alone as an effective preventive treatment for youth with chronic migraine.46 These findings have led to an increasing call for pediatric headache providers to promote behavioral treatments as frontline preventive interventions.
Cognitive-Behavioral Therapy Plus Amitriptyline
The best available evidence, as described in current guidelines from the AAN and American Headache Society, supports use of a combined pharmacotherapy (ie, amitriptyline) and behavioral approach (ie, cognitive-behavioral therapy) for migraine prevention in children and adolescents. These recommendations were created after a large randomized controlled trial demonstrated that the combined treatment with cognitive-behavioral therapy (CBT) and amitriptyline was superior to amitriptyline and headache education in reducing youth headache frequency by at least 50% (from a baseline average of 21 headache days per month to approximately 10 after 20 weeks).47 An ancillary analysis from this trial revealed a linear trend and quadratic trend in headache day change, indicating that although decreases in headache days continued throughout the trial, the majority of clinical improvement occurred by the 8-week time point in the CBT+AMI group.48 These data suggest that these youth make relatively rapid treatment gains that can be sustained over time. The evidence base for CBT for pediatric migraine prevention continues to grow; a 2018 Cochrane review of all published clinical trials concluded that CBT is effective in reducing headache days and headache-related disability among youth with migraine.49
CBT is a skills-oriented treatment that provides training in coping techniques and behavioral strategies that can be applied to manage and prevent headaches.50,51 Typically, treatment begins with headache education and an introduction to the gate control theory of pain.52 In the initial stages of treatment, the therapist reviews family guidelines with youth and their caregivers; these guidelines offer practical steps to support the child’s pain management and address family factors that may interfere with the patient’s daily functioning or increase their focus on current symptoms. Patients then receive instruction and practice several relaxation exercises including diaphragmatic breathing, progressive muscle relaxation, and guided imagery. These techniques decrease autonomic arousal and muscle tension that can be associated with pain, and serve as a means of distraction from symptoms. Relaxation training may be used in conjunction with biofeedback technology to allow youth to “see for themselves” how practicing relaxation skills results in physiological changes such as increased peripheral body temperature and decreased muscle tension.
Psychologists providing CBT also facilitate activity pacing and adherence to healthy lifestyle recommendations through instruction and collaborative problem-solving. This additional “layer” of intervention may be especially important given that youth with migraine frequently report difficulty with adherence to medical recommendations related to eating and hydration.53 Finally, cognitive reappraisal skills are provided to teach youth how thoughts and feelings are connected to the pain experience, and challenge negative or unrealistic thinking that can contribute to worsening pain and associated symptoms.
Considerations for Optimizing Behavioral and Psychological Interventions for Youth with Chronic Migraine
Despite the growing evidence base for CBT as an effective intervention for pediatric migraine prevention, it is important to consider that it is not a “one-size-fits-all” treatment, and may not meet the needs of each patient with chronic migraine. For example, although a majority of youth with migraine do not meet criteria for a co-occurring psychiatric disorder,54 children and adolescents with migraine are more likely than youth without migraine to report elevated internalizing symptoms (eg, anxiety, depression), attentional difficulties, and somatic complaints.55 Furthermore, the presence of co-occurring clinically elevated depressive or anxiety symptoms is associated with greater disability and diminished quality of life in youth with migraine.56,57 Thus, routine screening for co-occurring psychiatric comorbidities and appropriate follow-up should be routinely provided in specialty headache centers. If a clinically significant psychological disorder is detected in this assessment process, it should be considered a treatment priority.
The severity and disabling nature of chronic migraine in youth also presents numerous challenges for which traditional CBT may not promote effective management of symptoms. For example, some children and adolescents with chronic migraine have undergone several trials of preventive medication with varying success, and may therefore have different beliefs about how to best manage pain, what to expect from treatment, and goals for treatment relative to youth with less frequent or disabling headache presentations. The primary aim of CBT for migraine is to improve a patient’s functioning while reducing the frequency of symptoms. Other interventions may be needed to more specifically target disability and psychological factors that can impact day-to-day functioning in this patient population.
Third-wave psychological interventions, such as Acceptance and Commitment Therapy (ACT) and mindfulness-based approaches, focus primarily on increasing patients’ psychological flexibility and engagement in activity that they value as opposed to focusing on decreasing their pain or symptoms. Mindfulness, which is a core component of ACT, is derived from Buddhist spiritual traditions and involves bringing attention to the present moment, adopting a nonjudgmental, accepting stance about pain and symptoms, and flexibly adapting to daily fluctuations in pain and symptoms.58 The evidence for ACT in the treatment of pediatric chronic pain is growing.59 Two investigations of mindfulness-based interventions for chronic migraine in children and adolescents, including one recent open-label trial, have shown promising results in reducing migraine-related disability,60,61 mirroring findings from trials of mindfulness-based interventions among adults with migraine.62,63
Other Preventive Treatment Options
Clinical research efforts have been devoted to studying alternative treatments that reduce risks associated with traditional pill-based migraine therapies given current practice guidelines. What follows is a discussion of alternative treatment options that have been studied extensively in adults with migraine, and may be recommended for pediatric patients who have not responded to available preventive treatments.
Supplements and Nutraceuticals
Youth with chronic migraine and their families often request trials of dietary supplements or nutraceuticals as alternative pill-based treatment options. Nutraceuticals, which are compounds derived from foods such as fruits and vegetables, are a form of complementary and integrative medicine (CAM) and are among the most commonly used treatments among pediatric patients with chronic pain conditions, including migraine.64 Despite the popularity and widespread use of nutraceuticals in pediatric pain populations, there are no practice guidelines regarding their use for acute migraine treatment or prevention.
Orr65 published, to our knowledge, the only existing review of nutraceuticals for the treatment of migraine in youth. The review summarized results from 11 observational studies, seven randomized controlled trials, and three systematic reviews. The reviewed nutraceuticals included vitamin D, riboflavin, coenzyme Q10, magnesium, butterbur, and polyunsaturated fatty acids. The review concluded that, given the relative absence of rigorous clinical trials, there is limited evidence for the efficacy of nutraceuticals for migraine prevention and acute treatment in children and adolescents. Coenzyme Q10 has demonstrated initial efficacy for migraine prevention compared to placebo, and oral magnesium may reduce pain intensity when acute headaches are treated with ibuprofen or acetaminophen. However, in the absence of clear, rigorous safety and efficacy data for nutraceutical use, clinicians should discuss with their patients that there is currently no evidence that these treatments are superior to placebo.
Orr65 also informs clinicians about differences in regulatory practices between pharmaceuticals and nutraceuticals, and encourages providers to educate patients about risks associated with nutraceuticals given the frequent assumption that they are safe if available without a prescription.66 For example, butterbur—which has a long history of use in adults with migraine and has been recommended in guidelines from the American and Canadian Headache Societies—has hepatotoxic properties and is generally not recommended for treatment of migraine among children and adolescents.65
OnabotulinumtoxinA
OnabotulinumtoxinA (OBTA; ie, BOTOX) was approved in 2010 by the FDA for treatment of chronic migraine in adults. Data examining the efficacy of OBTA for treatment of youth with chronic migraine are limited. OBTA did not gain FDA approval in adolescents after failing to demonstrate greater efficacy compared to placebo.67 A later crossover trial of OBTA for treatment of youth with chronic migraine showed that, compared to a placebo group, youth who received a trial of OBTA injections administered in 3-month intervals and 6-week follow-up visits demonstrated a statistically significant decrease in migraine frequency and intensity, but not duration.68 Multiple retrospective reviews of outcomes for pediatric patients with chronic migraine who received treatment with OBTA after failing oral therapies showed a statistically significant reduction in headache days and disability, and that OBTA was well-tolerated.69,70 Current guidelines from the AAN state that there is currently insufficient evidence to support the use of OBTA for migraine prevention in youth. In practice, OBTA injections may be recommended when a patient with chronic migraine has not responded to two or more preventive therapies.
Novel Therapeutics Undergoing Evaluation in Children and Adolescents
Calcitonin Gene-Related Peptide (CGRP) Monoclonal Antibodies
The calcitonin gene-related peptide (CGRP) is an amino acid peptide found in sensory fibers throughout the body, and particularly in the central nervous system. The CGRP pathway is involved in sensory processing and pain modulation, and has been implicated in the pathophysiology of migraine.71 In adults, antagonism of the CGRP pathway is associated with diminished headache days and medication usage.72 Monoclonal antibodies (mAbs) to CGRP or its receptor—which require subcutaneous (erenumab, galcanezumab, fremanezumab) or intravenous administration (eptinezumab)—have shown safety and efficacy in trials of adults with migraine,73–77 some with open-label data for 1 to 5 years.78,79
To date, there are no published placebo-controlled trials of mAbs in children and adolescents with migraine. In 2018, Szperka et al published a set of recommendations for the use of anti-CGRP mAbs in children and adolescents with migraine.80 These guidelines emphasized that consideration of anti-GGRP mAbs should be limited to youth with a frequent migraine presentation and for whom established migraine preventive therapies have not been effective. These therapies should include oral treatments and may also include CBT, neuromodulation devices and nutraceuticals. The authors note that rigorous clinical research effort is needed to establish long-term safety and efficacy data for use of anti-CGRP mAbs in children and adolescents with migraine, and emphasize those youth with more severe migraine presentations (eg, continuous headache) should be included in future trials as these youth have the greatest need for targeted therapeutics.
Greene et al reported a multicenter retrospective study of children and adolescents treated with mAbs for chronic headaches including chronic migraine, persistent post-traumatic headache and NDPH.81 This report of 112 patients with nearly daily or continuous headaches was the first to provide safety and efficacy data in this group. Their data showed that side effects in adolescents are similar to those reported in adult trials and that mAb treatment may benefit youth who are otherwise refractory to other prevention therapies. Notably, severity of pain and functional status improved in more than half of cases. Several randomized controlled trials of mAbs in children and adolescents with episodic and chronic migraine are underway.
Newer Pill-Based Treatments
Newer targeted therapies known as “gepants” and “ditans” have made their way to market after decades of translational research. Gepants act as antagonists to calcitonin gene-related peptide (CGRP) receptors,82 while ditans likely act as agonists of the serotonin 5HT-1F receptors. In contrast to triptans, gepants and ditans do not cause vasoconstriction and are therefore safe for use in patients with history of cardiac or other vascular conditions including stroke.83 Rimegepant, ubrogepant and lasmiditan are currently FDA-approved for acute therapy in adults with migraine and studies are underway in children and adolescents. These drugs may therefore represent third- or fourth-line options for off-label use in youth with attacks refractory to other medications, or with contraindications or adverse reactions to triptans. Although no head-to-head studies have compared gepants and ditans to other pharmacologically active drugs, a meta-analysis showed that gepants and ditans were associated with a lower odds ratio than most triptans for pain relief or freedom at 2 hours.84
Rimegepant also recently gained FDA approval for migraine prevention in adults after showing superiority to placebo at reducing headache days in those with episodic and chronic migraine when dosed every other day.85 Adolescents who experience excellent and sustained (24–48 hours) relief from headache with acute rimegepant use may be particularly good candidates for preventive therapy with rimegepant. In addition, atogepant is the only gepant with FDA approval solely for preventive therapy in adults with migraine. Finally, though not exclusively a pill-based therapy, zavegepant is currently being studied for prevention in its oral form and has evidence of efficacy for the acute treatment of migraine in its nasal form.86
Discussion
Although there have been numerous advances in acute and preventive treatment over several decades, treatment of youth with chronic migraine continues to evolve. As highlighted in this review, available evidence suggests that pediatric patients with chronic migraine do experience a reduction in headache days when they receive multidisciplinary, biopsychosocially oriented intervention,87 and treatment gains made through preventive care are often maintained over time.88 Current practice guidelines for the prevention of migraine in youth emphasize a combined pill-based and nonpharmacological approach. We anticipate that a holistic approach to migraine management will continue to represent the best standard of care moving forward, even as considerable attention is being devoted to establishing an evidence base for the use of novel interventions such as neuromodulation, GGRP monoclonal antibodies, and targeted pill-based therapies for both acute and preventive treatment. In the following sections, we highlight important and novel avenues for advancing evidence-based care through future clinical research.
Understanding Why, How, and for Whom Nonpharmacological Treatments are Effective
Despite the range of interventions that have been developed for the treatment of chronic migraine, additional research is needed to tailor available treatments for the clinical presentation and treatment needs of youth with chronic migraine and their families. Much of current clinical guidance has been gleaned from studies in adult patients; however, it has become increasingly apparent that children and adolescents with headache disorders can differ substantially from adults in terms of their responses to pharmacological treatments.
Given this, studies highlighted in this review underscore the importance of taking a developmental approach to research involving novel medical and nonpharmacological intervention approaches for youth with chronic migraine. As the field continues to evolve, prospective longitudinal research will be needed to advance our understanding of the developmental contributors to the progression and course of chronic migraine in children and adolescents. For example, epidemiologic studies have shown that pre-pubertal males have a higher prevalence of migraine relative to females, but there is a dramatic increase in migraine prevalence among females post-puberty.89 Prospective longitudinal studies that examine the roles of age and development (eg, puberty, hormonal changes) in relation to the presentation of migraine, or investigate neural changes associated with migraine progression may enhance our identification of targets for early intervention tailored to the needs of each individual. Further, given the strong link between genetics and migraine, studies identifying the monogenic and polygenic contributors to the pathophysiology of migraine disease are crucial as the field works toward precision medicine as a standard of care.31,90
The effectiveness of CBT for prevention of pediatric migraine also raises important questions about how and why this treatment approach works. Recently, our research group published an overview of psychological interventions for pediatric headache disorders,51 in which we discuss the role of mechanistic studies and their importance for elucidating neural alterations associated with CBT treatment. Research has demonstrated that pre-post CBT alterations in resting state brain activation and functional connectivity occur among youth with migraine who have received this intervention for headache.91 Our group is also conducting an ongoing mechanistic study (funded by the National Center for Complementary and Integrative Health and the National Institute of Neurological Disorders and Stroke) may be able to answer why patients with migraine—including chronic migraine—make such rapid treatment gains in response to gold-standard preventive care by determining the extent to which components of CBT intervention are associated with particular neural changes among youth with migraine.
Empirical support for the treatment of migraine in youth is largely based on studies that have included patients recruited from specialty headache centers, patients who meet very specific diagnostic criteria, and patients without medical or psychiatric comorbidities. While this level of rigor in clinical trials increases our confidence in the benefit of available interventions, it is possible that the stringent nature of referrals from tertiary care clinics and inclusion criteria has resulted in many youth with chronic migraine being excluded from clinical trials, leaving a gap in our field’s ability to conceptualize and understand which treatments work best for which patients. Furthermore, participants in migraine research studies tend to be predominantly White, female, and from upper middle–class backgrounds.92 Improving the representativeness and generalizability of our treatments will require prioritizing the inclusion of patients from underrepresented backgrounds in all aspects of the research process, from recruitment and retention to intervention development and dissemination of findings.
As discussed previously, a subset of treatment-seeking children and adolescents who meet the criteria for chronic migraine present with continuous (ie, unremitting) headache. Unfortunately, these patients are often excluded from research studies as they are considered to be much more complex in terms of their psychosocial profile and refractory to treatment relative to other youth with less frequent headache presentations. As the field moves forward, it will be important to recruit subpopulations of pediatric patients with chronic migraine experience continuous headache to determine their patterns of treatment utilization, preferences for treatment, and whether available treatments are also effective for patients with this headache presentation. Understanding the treatment priorities and goals of patients with more severe and disabling chronic migraine presentations may also lead to the development and testing of tailored interventions. It will be exciting to learn whether ACT and mindfulness-based approaches demonstrate efficacy for treatment of headache days and disability among youth with migraine, and whether principles of these treatments could augment traditional CBT intervention.
Improving Access and Equitability of Care
Population-based studies have shown that migraine is more prevalent among youth from lower socioeconomic (SES) backgrounds.93 Moreover, there are considerable racial and ethnic disparities in the prevalence of migraine. For example, in the United States, the prevalence of migraine is highest among Native Americans. These disparities reflect inequities in access to care and treatment practices that lead to poorer long-term health outcomes.94
An unfortunate reality stemming from differences in health equity is that many of the newer and investigational treatment options discussed in this paper, such as neurostimulation and anti-CGRP antibodies, are not consistently covered by third-party payors and have extremely high out-of-pocket costs. Access to adequate healthcare in the United States remains poor for many pediatric patients and their families, and this is a substantial barrier to evidence-based migraine treatment that has not improved in recent years. Indeed, a recent review published by Yu et al showed that percentage of children and adolescents experiencing underinsurance rose from 30.6% in 2016 to 34.0% in 2019.95 Even gold-standard preventive treatments, such as cognitive-behavioral therapy, are not consistently covered by insurance providers. The result of inequality in healthcare access is that under-resourced children and adolescents—the young people who need the best available care the most—are not being seen for care in specialty headache centers. These children and their families understandably rely on the types of care that are available to them, and community clinics or hospitals may not employ neurologists with a specialization in headache medicine or pediatric psychologists who practice behavioral headache medicine.
One tangible approach that begins the process of addressing barriers to patients’ access to equitable care involves leveraging the potential of innovative study designs to expand the reach of evidence-based interventions. For example, a current study funded by the National Center for Complementary and Integrative Health (NCCIH U01 AT010132) is employing a multiphase optimization strategy (MOST;96) to develop a cognitive-behavioral intervention delivered by nursing staff in outpatient neurology clinics. The goal of this study is to identify which components and “doses” of CBT are most effective to promote change in key headache outcomes, with treatment being provided by healthcare professionals besides trained psychologists. The data gleaned from this study will inform the development of a large pragmatic or sequential multiple randomization (SMART) trial that will be conducted in neurology clinics and, in the long term, could also be conducted in primary care or pediatric practices. Expanding the availability of evidence-based pediatric behavioral medicine beyond secondary and tertiary care should be considered a priority as our field works to increase the accessibility of care for all patients and their families.
It is also crucial that clinicians and researchers continue to advocate for their patients as the field of pediatric headache medicine works toward a more equitable and inclusive scientific practice. The COVID-19 pandemic has exposed vulnerabilities in the healthcare system and further underscored racial and ethnic disparities in healthcare.97 Yet, the proliferation of telemedicine over the past 2 years perhaps represents an opportunity to rigorously study the efficacy of interventions that can be feasibility delivered remotely in the context of a pragmatic clinical trial. As the field works to expand care beyond specialty clinics, pragmatic trials may represent one clear opportunity to advance clinical practice and facilitate the successful dissemination and implementation of migraine treatment. For example, a trial examining the efficacy of CBT delivered entirely remotely—and casting a “wide net” to include patients with chronic migraine, including those who may have been historically excluded from trials (eg, youth with continuous headache)—could facilitate the eventual integration of CBT into traditional clinical practice, thus increasing its accessibility to patients and families. If researchers can leverage the potential of innovative study designs to improve the availability of evidence-based care in a manner that allows patients to access it earlier, the field of pediatric headache medicine may be better positioned to prevent chronic migraine from progressing further and persisting into young adulthood.
Conclusion
Chronic migraine is a disabling migraine subtype that affects a substantial proportion of children and adolescents and tends to persist into adulthood. Over the past several decades, substantial gains have been made in advancing both acute and preventive treatments for this debilitating headache disorder. We have learned that a biopsychosocial approach to the conceptualization and treatment of migraine is most beneficial to patients, and current research is advancing our understanding about why nonpharmacological treatment strategies for migraine prevention work. As the field moves forward, considerable clinical research effort should focus on expanding access to evidence-based care, testing novel therapeutics, leveraging the potential of innovative study designs such as SMART and pragmatic trials to inform precision medicine and wider dissemination of interventions, recruiting patients for research studies who have traditionally been underrepresented, and tailoring existing nonpharmacological interventions to meet the unique needs of each child and their family. We believe the future of pediatric headache medicine is bright, and feel confident that the coming years will provide new insights into the optimal management of chronic migraine in children and adolescents.
Funding
This work was supported by R01 (R01AT010171) and U01 (U01AT010132) grants from the National Center for Complementary and Integrative Health, an R01 grant (R01NS101321) from the National Institute of Neurological Disorders and Stroke, and a training grant from the National Institute of Diabetes and Digestive and Kidney Diseases (T32DK063929).
Disclosure
Dr Robert C Gibler reports grants from National Institutes of Health National Institute of Diabetes and Digestive and Kidney Diseases T32 Training Grant (T32DK063929), outside the submitted work. Dr Brooke L Reidy reports grants from NIH, during the conduct of the study; Frontiers in Headache Research Scholarship (travel award to attend Conference) in 2018 from American Headache Society, Travel Award to attend conference 2018 from International Society for Developmental Psychobiology, outside the submitted work. Dr. Powers reports funding to the Cincinnati Children’s Hospital Medical Center Research Foundation from the National Institutes of Health. The authors report no other conflicts of interest in this work.
References
1. Abu-Arefeh I, Russell G. Prevalence of headache and migraine in schoolchildren. BMJ. 1994;309(6957):765–769. doi:10.1136/bmj.309.6957.765
2. Ozge A, Saşmaz T, Buğdaycı R, et al. The prevalence of chronic and episodic migraine in children and adolescents. Eur J Neurol. 2013;20(1):95–101. doi:10.1111/j.1468-1331.2012.03795.x
3. Wöber-Bingöl Ç. Epidemiology of migraine and headache in children and adolescents. Curr Pain Headache Rep. 2013;17(6):341. doi:10.1007/s11916-013-0341-z
4. Wang SJ, Fuh JL, Lu SR, Juang KD. Chronic daily headache in adolescents: prevalence, impact, and medication overuse. Neurology. 2006;66(2):193–197. doi:10.1212/01.wnl.0000183555.54305.fd
5. Lipton RB, Manack A, Ricci JA, Chee E, Turkel CC, Winner P. Prevalence and burden of chronic migraine in adolescents: results of the chronic daily headache in adolescents study (C-dAS). Headache. 2011;51(5):693–706. doi:10.1111/j.1526-4610.2011.01885.x
6. Powers SW, Patton SR, Hommel KA, Hershey AD. Quality of life in childhood migraines: clinical impact and comparison to other chronic illnesses. Pediatrics. 2003;112(1 Pt 1):e1–5. doi:10.1542/peds.112.1.e1
7. Bille B. A 40-year follow-up of school children with migraine. Cephalalgia. 1997;17(4):
8. Youssef PE, Mack KJ. Episodic and chronic migraine in children. Dev Med Child Neurol. 2020;62(1):34–41. doi:10.1111/dmcn.14338
9. Bellini B, Arruda M, Cescut A, et al. Headache and comorbidity in children and adolescents. J Headache Pain. 2013;14(1):79. doi:10.1186/1129-2377-14-79
10. Powers SW, Gilman DK, Hershey AD. Headache and psychological functioning in children and adolescents. Headache. 2006;46(9):1404–1415. doi:10.1111/j.1526-4610.2006.00583.x
11. Kashikar-Zuck S, Zafar M, Barnett KA, et al. Quality of life and emotional functioning in youth with chronic migraine and Juvenile Fibromyalgia. Clin J Pain. 2013;29(12):1066–1072. doi:10.1097/AJP.0b013e3182850544
12. Larsson B, Sigurdson JF, Sund AM. Long-term follow-up of a community sample of adolescents with frequent headaches. J Headache Pain. 2018;19(1):79. doi:10.1186/s10194-018-0908-5
13. Palermo TM, Putnam J, Armstrong G, Daily S. Adolescent autonomy and family functioning are associated with headache-related disability. Clin J Pain. 2007;23(5):458–465. doi:10.1097/AJP.0b013e31805f70e2
14. Lewandowski AS, Palermo TM. Parent–teen interactions as predictors of depressive symptoms in adolescents with headache. J Clin Psychol Med Settings. 2009;16(4):331–338. doi:10.1007/s10880-009-9173-8
15. Arnold M. Headache Classification Committee of the International Headache Society (IHS) The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
16. Ghosh A, Silva E, Burish MJ. Pediatric-onset trigeminal autonomic cephalalgias: a systematic review and meta-analysis. Cephalalgia. 2021;41(13):1382–1395. doi:10.1177/03331024211027560
17. Albakr A, Hamad MH, Alwadei AH, et al. Idiopathic intracranial hypertension in children: diagnostic and management approach. Sudan J Paediatr. 2016;16(2):67–76.
18. Powers SW, Gilman DK, Hershey AD. Suggestions for a biopsychosocial approach to treating children and adolescents who present with headache. Headache. 2006;46(Suppl 3):S149–150. doi:10.1111/j.1526-4610.2006.00568.x
19. Gelfand AA, Goadsby PJ. Medication overuse in children and adolescents. Curr Pain Headache Rep. 2014;18(7):428. doi:10.1007/s11916-014-0428-1
20. Moavero R, Stornelli M, Papetti L, et al. Medication overuse withdrawal in children and adolescents does not always improve headache: a cross-sectional study. Front Neurol. 2020;11:823. doi:10.3389/fneur.2020.00823
21. Kacperski J, Kabbouche MA, O’Brien HL, Weberding JL. The optimal management of headaches in children and adolescents. Ther Adv Neurol Disord. 2016;9(1):53–68. doi:10.1177/1756285615616586
22. Oskoui M, Pringsheim T, Holler-Managan Y, et al. Practice guideline update summary: acute treatment of migraine in children and adolescents: report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology and the American Headache Society. Neurology. 2019;93(11):487–499. doi:10.1212/WNL.0000000000008095
23. Patniyot IR, Gelfand AA. Acute treatment therapies for pediatric migraine: a qualitative systematic review. Headache. 2016;56(1):49–70. doi:10.1111/head.12746
24. Wijemanne S, Jankovic J, Evans RW. Movement disorders from the use of metoclopramide and other antiemetics in the treatment of migraine. Headache. 2016;56(1):153–161. doi:10.1111/head.12712
25. Talai A, Heilbrunn B. Ondansetron for acute migraine in the pediatric emergency department. Pediatr Neurol. 2020;103:52–56. doi:10.1016/j.pediatrneurol.2019.06.011
26. Freedman SB, Uleryk E, Rumantir M, Finkelstein Y. Ondansetron and the risk of cardiac arrhythmias: a systematic review and postmarketing analysis. Ann Emerg Med. 2014;64(1):19–25.e6. doi:10.1016/j.annemergmed.2013.10.026
27. Diener HC, Limmroth V. Medication-overuse headache: a worldwide problem. Lancet Neurol. 2004;3(8):475–483. doi:10.1016/S1474-4422(04)00824-5
28. Bigal ME, Lipton RB. Overuse of acute migraine medications and migraine chronification. Curr Pain Headache Rep. 2009;13(4):301–307. doi:10.1007/s11916-009-0048-3
29. Orr SL, Kabbouche MA, O’Brien HL, Kacperski J, Powers SW, Hershey AD. Paediatric migraine: evidence-based management and future directions. Nat Rev Neurol. 2018;14(9):515–527. doi:10.1038/s41582-018-0042-7
30. VanderPluym J, Gautreaux J, Burch R, et al. Evidence regarding medication overuse headache in children and adolescents: protocol for a systematic review. Headache. 2020;60(1):171–177. doi:10.1111/head.13726
31. Hershey AD, Burdine D, Kabbouche MA, Powers SW. Genomic expression patterns in medication overuse headaches. Cephalalgia. 2011;31(2):161–171. doi:10.1177/0333102410373155
32. Puledda F, Goadsby PJ. An update on non-pharmacological neuromodulation for the acute and preventive treatment of migraine. Headache. 2017;57(4):685–691. doi:10.1111/head.13069
33. Grazzi L, Egeo G, Liebler E, Padovan AM, Barbanti P. Non-invasive vagus nerve stimulation (nVNS) as symptomatic treatment of migraine in young patients: a preliminary safety study. Neurol Sci. 2017;38(Suppl 1):197–199. doi:10.1007/s10072-017-2942-5
34. Hershey AD, Lin T, Gruper Y, et al. Remote electrical neuromodulation for acute treatment of migraine in adolescents. Headache. 2021;61(2):310–317. doi:10.1111/head.14042
35. Raucci U, Boni A, Evangelisti M, et al. Lifestyle modifications to help prevent headache at a developmental age. Front Neurol. 2021;11:618375. doi:10.3389/fneur.2020.618375
36. Lin YK, Lin GY, Lee JT, et al. Associations between sleep quality and migraine frequency. Medicine. 2016;95(17):e3554. doi:10.1097/MD.0000000000003554
37. Lemmens J, De Pauw J, Van Soom T, et al. The effect of aerobic exercise on the number of migraine days, duration and pain intensity in migraine: a systematic literature review and meta-analysis. J Headache Pain. 2019;20(1):16. doi:10.1186/s10194-019-0961-8
38. Sullivan DP, Martin PR, Boschen MJ. Psychological sleep interventions for migraine and tension-type headache: a systematic review and meta-analysis. Sci Rep. 2019;9(1):6411. doi:10.1038/s41598-019-42785-8
39. Khorsha F, Mirzababaei A, Togha M, Mirzaei K. Association of drinking water and migraine headache severity. J Clin Neurosci. 2020;77:81–84. doi:10.1016/j.jocn.2020.05.034
40. Robblee J, Starling AJ. SEEDS for success: lifestyle management in migraine. Cleve Clin J Med. 2019;86(11):741–749. doi:10.3949/ccjm.86a.19009
41. Papetti L, Ursitti F, Moavero R, et al. Prophylactic treatment of pediatric migraine: is there anything new in the last decade? Front Neurol. 2019;10:771. doi:10.3389/fneur.2019.00771
42. Hershey AD, Powers SW, Bentti AL, Degrauw TJ. Effectiveness of amitriptyline in the prophylactic management of childhood headaches. Headache. 2000;40(7):539–549. doi:10.1046/j.1526-4610.2000.00085.x
43. Sakulchit T, Meckler GD, Goldman RD. Topiramate for pediatric migraine prevention. Can Fam Physician. 2017;63(7):529–531.
44. Powers SW, Coffey CS, Chamberlin LA, et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2017;376(2):115–124. doi:10.1056/NEJMoa1610384
45. Vatzaki E, Straus S, Dogne JM, Garcia Burgos J, Girard T, Martelletti P. Latest clinical recommendations on valproate use for migraine prophylaxis in women of childbearing age: overview from European Medicines Agency and European Headache Federation. J Headache Pain. 2018;19(1):68. doi:10.1186/s10194-018-0898-3
46. El-Chammas K, Keyes J, Thompson N, Vijayakumar J, Becher D, Jackson JL. Pharmacologic treatment of pediatric headaches: a meta-analysis. JAMA Pediatr. 2013;167(3):250–258. doi:10.1001/jamapediatrics.2013.508
47. Powers SW, Kashikar-Zuck SM, Allen JR, et al. Cognitive behavioral therapy plus amitriptyline for chronic migraine in children and adolescents: a randomized clinical trial. JAMA. 2013;310(24):2622–2630. doi:10.1001/jama.2013.282533
48. Kroner JW, Peugh J, Kashikar-Zuck SM, et al. Trajectory of improvement in children and adolescents with chronic migraine: results from the cognitive behavioral therapy and amitriptyline trial. J Pain. 2017;18(6):637–644. doi:10.1016/j.jpain.2017.01.002
49. Fisher E, Law E, Dudeney J, Palermo TM, Stewart G, Eccleston C. Psychological therapies for the management of chronic and recurrent pain in children and adolescents. Cochrane Database Syst Rev. 2018;9:CD003968. doi:10.1002/14651858.CD003968.pub5
50. Kroon Van Diest AM, Powers SW. Cognitive behavioral therapy for pediatric headache and migraine: why to prescribe and what new research is critical for advancing integrated biobehavioral care. Headache. 2019;59(2):289–297. doi:10.1111/head.13438
51. Knestrick KE, Gibler RC, Reidy BL, Powers SW. Psychological interventions for pediatric headache disorders: a 2021 update on research progress and needs. Curr Pain Headache Rep. 2022;26(1):85–91. doi:10.1007/s11916-022-01007-z
52. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979. doi:10.1126/science.150.3699.971
53. Kroon Van Diest AM, Ramsey R, Aylward B, et al. Adherence to biobehavioral recommendations in pediatric migraine as measured by electronic monitoring: the Adherence in Migraine (AIM) study. Headache. 2016;56(7):1137–1146. doi:10.1111/head.12836
54. Gelfand AA. Psychiatric comorbidity and paediatric migraine: examining the evidence. Curr Opin Neurol. 2015;28(3):261–264. doi:10.1097/WCO.0000000000000192
55. Arruda MA, Bigal ME. Behavioral and emotional symptoms and primary headaches in children: a population-based study. Cephalalgia. 2012;32(15):1093–1100. doi:10.1177/0333102412454226
56. Slater SK, Kashikar-Zuck SM, Allen JR, et al. Psychiatric comorbidity in pediatric chronic daily headache. Cephalalgia. 2012;32(15):1116–1122. doi:10.1177/0333102412460776
57. Paschoal JKSF, Lin J, Pinho RS, et al. Psychiatric symptoms may contribute to poor quality of life in adolescents with migraine. Pediatr Int. 2013;55(6):741–747. doi:10.1111/ped.12178
58. Keng SL, Smoski MJ, Robins CJ. Effects of mindfulness on psychological health: a review of empirical studies. Clin Psychol Rev. 2011;31(6):1041–1056. doi:10.1016/j.cpr.2011.04.006
59. Pielech M, Vowles KE, Wicksell R. Acceptance and commitment therapy for pediatric chronic pain: theory and application. Children. 2017;4(2):E10. doi:10.3390/children4020010
60. Grazzi L, Grignani E, Raggi A, Rizzoli P, Guastafierro E. Effect of a mindfulness-based intervention for chronic migraine and high frequency episodic migraine in adolescents: a pilot single-arm open-label study. Int J Environ Res Public Health. 2021;18(22):11739. doi:10.3390/ijerph182211739
61. Sansone E, Raggi A, Grignani E, et al. Mindfulness meditation for chronic migraine in pediatric population: a pilot study. Neurol Sci. 2018;39(Suppl 1):111–113. doi:10.1007/s10072-018-3365-7
62. Seng EK, Singer AB, Metts C, et al. Does mindfulness-based cognitive therapy for migraine reduce migraine-related disability in people with episodic and chronic migraine? A Phase 2b pilot randomized clinical trial. Headache. 2019;59(9):1448–1467. doi:10.1111/head.13657
63. Wells RE, O’Connell N, Pierce CR, et al. Effectiveness of mindfulness meditation vs headache education for adults with migraine: a randomized clinical trial. JAMA Intern Med. 2021;181(3):317–328. doi:10.1001/jamainternmed.2020.7090
64. Groenewald CB, Beals-Erickson SE, Ralston-Wilson J, Rabbitts JA, Palermo TM. Complementary and alternative medicine use by children with pain in the United States. Acad Pediatr. 2017;17(7):785–793. doi:10.1016/j.acap.2017.02.008
65. Orr SL. The evidence for the role of nutraceuticals in the management of pediatric migraine: a review. Curr Pain Headache Rep. 2018;22(5):37. doi:10.1007/s11916-018-0692-6
66. Ronis MJJ, Pedersen KB, Watt J. Adverse effects of nutraceuticals and dietary supplements. Annu Rev Pharmacol Toxicol. 2018;58(1):583–601. doi:10.1146/annurev-pharmtox-010617-052844
67. Winner PK, Kabbouche M, Yonker M, Wangsadipura V, Lum A, Brin MF. A randomized trial to evaluate onabotulinumtoxinA for prevention of headaches in adolescents with chronic migraine. Headache. 2020;60(3):564–575. doi:10.1111/head.13754
68. Shah S, Calderon MD, Crain N, Pham J, Rinehart J. Effectiveness of onabotulinumtoxinA (BOTOX) in pediatric patients experiencing migraines: a randomized, double-blinded, placebo-controlled crossover study in the pediatric pain population. Reg Anesth Pain Med. 2021;46(1):41–48. doi:10.1136/rapm-2020-101605
69. Kabbouche M, O’Brien H, Hershey AD. OnabotulinumtoxinA in pediatric chronic daily headache. Curr Neurol Neurosci Rep. 2012;12(2):114–117. doi:10.1007/s11910-012-0251-1
70. Ali SS, Bragin I, Rende E, Mejico L, Werner KE. Further Evidence that onabotulinum toxin is a viable treatment option for pediatric chronic migraine patients. Cureus. 2019;11(3):e4343. doi:10.7759/cureus.4343
71. Hershey ADCGRP. The next frontier for migraine. N Engl J Med. 2017;377(22):2190–2191. doi:10.1056/NEJMe1712559
72. Goadsby PJ, Reuter U, Hallström Y, et al. A controlled trial of erenumab for episodic migraine. N Engl J Med. 2017;377(22):2123–2132. doi:10.1056/NEJMoa1705848
73. Mitsikostas DD, Reuter U. Calcitonin gene-related peptide monoclonal antibodies for migraine prevention: comparisons across randomized controlled studies. Curr Opin Neurol. 2017;30(3):272–280. doi:10.1097/WCO.0000000000000438
74. Wang X, Chen Y, Song J, You C. Efficacy and safety of monoclonal antibody against calcitonin gene-related peptide or its receptor for migraine: a systematic review and network meta-analysis. Front Pharmacol. 2021;12:649143. doi:10.3389/fphar.2021.649143
75. Reuter U, Lucas C, Dolezil D, et al. Galcanezumab in patients with multiple previous migraine preventive medication category failures: results from the open-label period of the CONQUER trial. Adv Ther. 2021;38(11):5465–5483. doi:10.1007/s12325-021-01911-7
76. Datta A, Maryala S, John R. A review of eptinezumab use in migraine. Cureus. 2021;13(9):e18032. doi:10.7759/cureus.18032
77. Skljarevski V, Oakes TM, Zhang Q, et al. Effect of different doses of galcanezumab vs placebo for episodic migraine prevention: a randomized clinical trial. JAMA Neurol. 2018;75(2):187–193. doi:10.1001/jamaneurol.2017.3859
78. Ashina M, Goadsby PJ, Reuter U, et al. Long-term efficacy and safety of erenumab in migraine prevention: results from a 5-year, open-label treatment phase of a randomized clinical trial. Eur J Neurol. 2021;28(5):1716–1725. doi:10.1111/ene.14715
79. Bangs ME, Kudrow D, Wang S, et al. Safety and tolerability of monthly galcanezumab injections in patients with migraine: integrated results from migraine clinical studies. BMC Neurol. 2020;20(1):25. doi:10.1186/s12883-020-1609-7
80. Szperka CL, VanderPluym J, Orr SL, et al. Recommendations on the use of anti-CGRP monoclonal antibodies in children and adolescents. Headache. 2018;58(10):1658–1669. doi:10.1111/head.13414
81. Greene KA, Gentile CP, Szperka CL, et al. Calcitonin gene-related peptide monoclonal antibody use for the preventive treatment of refractory headache disorders in adolescents. Pediatr Neurol. 2021;114:62–67. doi:10.1016/j.pediatrneurol.2020.09.014
82. Pak K, Kim J, Lee GH, Cho JW, Kim HW. Effectiveness of calcitonin gene-related peptide receptor antagonists for migraine treatment: a meta-analysis. Eur Neurol. 2022:1–7. doi:10.1159/000521697
83. Tepper D. Gepants. Headache. 2020;60(5):1037–1039. doi:10.1111/head.13791
84. Yang CP, Liang CS, Chang CM, et al. Comparison of new pharmacologic agents with triptans for treatment of migraine: a systematic review and meta-analysis. JAMA Netw Open. 2021;4(10):e2128544. doi:10.1001/jamanetworkopen.2021.28544
85. Croop R, Lipton RB, Kudrow D, et al. Oral rimegepant for preventive treatment of migraine: a phase 2/3, randomised, double-blind, placebo-controlled trial. Lancet. 2021;397(10268):51–60. doi:10.1016/S0140-6736(20)32544-7
86. Dos Santos JBR, da Silva MRR. Small molecule CGRP receptor antagonists for the preventive treatment of migraine: a review. Eur J Pharmacol. 2022;922:174902. doi:10.1016/j.ejphar.2022.174902
87. Kabbouche MA, Powers SW, Vockell ALB, et al. Outcome of a multidisciplinary approach to pediatric migraine at 1, 2, and 5 years. Headache. 2005;45(10):1298–1303. doi:10.1111/j.1526-4610.2005.00261.x
88. Powers SW, Coffey CS, Chamberlin LA, et al. Prevalence of headache days and disability 3 years after participation in the childhood and adolescent migraine prevention medication trial. JAMA Netw Open. 2021;4(7):e2114712. doi:10.1001/jamanetworkopen.2021.14712
89. Lipton RB, Bigal ME. Migraine: epidemiology, impact, and risk factors for progression. Headache. 2005;45(Suppl 1):S3–S13. doi:10.1111/j.1526-4610.2005.4501001.x
90. Sutherland HG, Albury CL, Griffiths LR. Advances in genetics of migraine. J Headache Pain. 2019;20(1):72. doi:10.1186/s10194-019-1017-9
91. Nahman-Averbuch H, Schneider VJ, Chamberlin LA, et al. Alterations in brain function after cognitive behavioral therapy for migraine in children and adolescents. Headache. 2020;60(6):1165–1182. doi:10.1111/head.13814
92. Robbins NM, Bernat JL. Minority representation in migraine treatment trials. Headache. 2017;57(3):525–533. doi:10.1111/head.13018
93. Bigal ME, Lipton RB, Winner P, et al. Migraine in adolescents: association with socioeconomic status and family history. Neurology. 2007;69(1):16–25. doi:10.1212/01.wnl.0000265212.90735.64
94. Loder S, Sheikh HU, Loder E. The prevalence, burden, and treatment of severe, frequent, and migraine headaches in US minority populations: statistics from National Survey studies. Headache. 2015;55(2):214–228. doi:10.1111/head.12506
95. Yu J, Perrin JM, Hagerman T, Houtrow AJ. Underinsurance among children in the United States. Pediatrics. 2022;149(1):e2021050353. doi:10.1542/peds.2021-050353
96. Collins LM, Murphy SA, Strecher V. The Multiphase Optimization Strategy (MOST) and the Sequential Multiple Assignment Randomized Trial (SMART): new methods for more potent eHealth interventions. Am J Prev Med. 2007;32(5 Suppl):S112–S118. doi:10.1016/j.amepre.2007.01.022
97. Núñez A, Sreeganga SD, Ramaprasad A. Access to Healthcare during COVID-19. Int J Environ Res Public Health. 2021;18(6):2980. doi:10.3390/ijerph18062980
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.