Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
A Retrospective Controlled Study on the Effects of Four-Limb Linkage Training on Clinical Efficacy and Antioxidative Mechanisms in Patients with Chronic Obstructive Pulmonary Disease
Authors Liu X, Chen L, Wei Z, Jiang J, Yu Y, Wang Z
Received 24 October 2025
Accepted for publication 6 March 2026
Published 24 March 2026 Volume 2026:21 576646
DOI https://doi.org/10.2147/COPD.S576646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Xijiao Liu,1 Li Chen,2 Zonghui Wei,2 Jinshan Jiang,2 Yunyan Yu,2 Zhishan Wang2
1Department of Respiratory Medicine, Bishan Hospital Affiliated to Chongqing Medical University (Bishan District People’s Hospital), Chongqing, People’s Republic of China; 2Department of Respiratory Medicine, Nanchuan District People’s Hospital, Chongqing, People’s Republic of China
Correspondence: Zhishan Wang, Email [email protected]
Objective: To investigate the effects of systematic four-limb linkage training on pulmonary function, exercise capacity, dyspnea, and quality of life in patients with chronic obstructive pulmonary disease (COPD), and to explore its potential antioxidative mechanisms.
Methods: This retrospective controlled study included 114 patients with COPD admitted between August 2023 and April 2025. Patients were divided into a control group (n=57), receiving lower-limb cycling training, and an observation group (n=57), receiving four-limb linkage training. Both groups underwent continuous rehabilitation intervention for 8 weeks. Pulmonary function indices (FEV1, FVC, FEV1/FVC, FEV1%pred), dyspnea scores (modified Medical Research Council and Borg scales), exercise capacity (6-minute walking distance, 6MWD), disease severity (BODE index), quality of life (St. George’s Respiratory Questionnaire, SGRQ), and oxidative stress markers [thioredoxin (TRX) and thioredoxin-interacting protein (TXNIP) at mRNA and protein levels] were assessed at Pre-intervention and Post 8-week intervention.
Results: At Post 8-week intervention, pulmonary function indices, exercise capacity, and quality-of-life scores were significantly improved, while dyspnea scores and BODE index were significantly reduced in both groups compared with Pre-intervention (P< 0.05). The magnitude of improvement was significantly greater in the four-limb linkage training group than in the control group (P< 0.05). In addition, TRX mRNA and protein expression levels were significantly increased, whereas TXNIP mRNA and protein expression levels were significantly decreased at Post 8-week intervention compared with Pre-intervention, with more pronounced changes observed in the observation group (P< 0.05).
Conclusion: Four-limb linkage training significantly improves pulmonary function, exercise capacity, dyspnea, and quality of life in patients with COPD. These benefits may be mediated, at least in part, by enhanced antioxidative activity through upregulation of TRX and suppression of TXNIP. Compared with lower-limb training alone, four-limb linkage training provides a more comprehensive rehabilitation strategy for COPD management.
Keywords: chronic obstructive pulmonary disease, four-limb linkage training, pulmonary rehabilitation, oxidative stress, thioredoxin, quality of life
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory airway disease characterized by persistent airflow limitation, irreversible progression, frequent recurrence, and a high disability rate.1 Its pathogenesis is complex and involves multiple mechanisms, including chronic inflammation, oxidative stress, imbalance of protease–antiprotease systems, and airway remodeling.2,3 China is among the countries with the highest prevalence of COPD. Epidemiological data indicate that approximately 13.7% of adults aged over 40 years are affected, with a large proportion presenting moderate to severe disease, resulting in a substantial social and economic burden.4 Due to long-term airway inflammation and alveolar destruction, patients with COPD experience decreased lung compliance, impaired gas exchange, and weakened respiratory muscle function, which manifest clinically as dyspnea, reduced exercise tolerance, and poor quality of life.5,6 Although pharmacological treatments can alleviate symptoms and slow disease progression, their effectiveness in improving exercise capacity, relieving dyspnea, and restoring overall physical function remains limited. Consequently, pulmonary rehabilitation has become an essential component of comprehensive COPD management.
Traditional COPD rehabilitation programs primarily focus on lower-limb cycling or walking exercises, which can improve cardiopulmonary function and exercise endurance but often neglect upper-limb involvement and whole-body coordination.7 In daily activities such as combing hair, dressing, or reaching for objects, patients with COPD frequently experience dyspnea due to the dual role of upper-limb muscles in both movement and respiratory assistance, leading to increased oxygen consumption and ventilatory demand.8 Therefore, lower-limb training alone may be insufficient to fully enhance overall exercise capacity and ventilatory efficiency. Four-limb linkage training, a form of whole-body aerobic exercise involving coordinated upper- and lower-limb movements, has been reported to improve systemic circulation, enhance oxygen delivery to peripheral muscles, and optimize ventilatory efficiency, thereby reducing respiratory muscle load and improving functional performance.9 However, existing clinical evidence regarding four-limb linkage training in COPD remains limited, and most previous studies have primarily focused on functional outcomes rather than underlying biological mechanisms.
Beyond improvements in respiratory mechanics, oxidative stress plays a crucial role in the onset and progression of COPD. Long-term exposure to cigarette smoke, particulate matter, and chronic inflammation induces excessive production of reactive oxygen species (ROS), resulting in oxidative lung injury and amplification of airway inflammation.10,11 Thioredoxin (TRX), a key endogenous antioxidant protein, mitigates oxidative injury by scavenging free radicals, regulating intracellular signaling pathways, and inhibiting apoptosis.12 In contrast, thioredoxin-interacting protein (TXNIP), a specific endogenous inhibitor of TRX, suppresses TRX activity and exacerbates oxidative stress and inflammatory responses.13 Accumulating evidence suggests that the TRX/TXNIP signaling pathway plays a pivotal regulatory role in various respiratory diseases, and its imbalance directly affects oxidative damage and repair capacity in airway epithelial cells.14,15 Therefore, elucidating how exercise-based rehabilitation influences the TRX/TXNIP axis is critical for understanding the molecular mechanisms underlying COPD recovery.
At present, there is a lack of systematic clinical studies investigating whether four-limb linkage training can simultaneously improve functional outcomes and modulate antioxidative signaling pathways in patients with COPD. In particular, the potential role of the TRX/TXNIP axis in mediating the beneficial effects of four-limb linkage training remains unclear. Based on perspectives from exercise physiology and molecular biology, this retrospective controlled study aimed to evaluate the effects of four-limb linkage training on pulmonary function, exercise endurance, dyspnea, and quality of life in patients with COPD, while further exploring changes in TRX and TXNIP expression. The findings are expected to provide clinical and mechanistic evidence to support the development of more precise and comprehensive pulmonary rehabilitation strategies for COPD management.
Materials and Methods
Study Design and Participants
This study adopted a retrospective controlled design and included 114 patients with stable COPD who were admitted to our hospital between August 2023 and April 2025 and met the inclusion criteria. As a retrospective study, the sample size was determined by the number of available cases. (1) Inclusion criteria: ① Age ≥40 years, clinically diagnosed with COPD and confirmed by spirometry to have airflow limitation (FEV1/FVC < 0.70) in accordance with the GOLD diagnostic criteria;16 ② disease in the stable phase (no acute exacerbation, respiratory failure, or hospitalization within the previous 4 weeks); ③ ability to complete rehabilitation training and related assessments; ④ complete clinical data and intervention records (including training type, frequency, evaluation scales, and laboratory results). (2) Exclusion criteria: ① Presence of severe cardiovascular or cerebrovascular disease affecting exercise capacity (eg, unstable angina, severe cardiac insufficiency, recent myocardial infarction); ② inability to complete training due to severe musculoskeletal or neuromuscular disorders; ③ presence of other progressive respiratory diseases (eg, active tuberculosis, progressive pulmonary fibrosis); ④ pregnancy or lactation; ⑤ patients who previously participated in similar rehabilitation programs and received repeated interventions in a short period; ⑥ incomplete data or insufficient key biochemical samples. According to the actual rehabilitation programs received, patients were divided into the control group (n=57, conventional lower-limb cycling training) and the observation group (n=57, four-limb linkage training). All patients underwent 8 weeks of rehabilitation intervention. This study adhered to the ethical principles of the Declaration of Helsinki and was approved by the Ethics Committee of Nanchuan District People’s Hospital, Chongqing (Approval No.: HXNKKFLC25-05). All patients and their families provided informed consent before participating in the interventions and data analysis, and written consent forms were signed. The retrospective data were used under strict privacy protection and anonymization principles. A flowchart illustrating patient screening, group allocation, intervention procedures, and outcome assessment is provided in Figure 1.
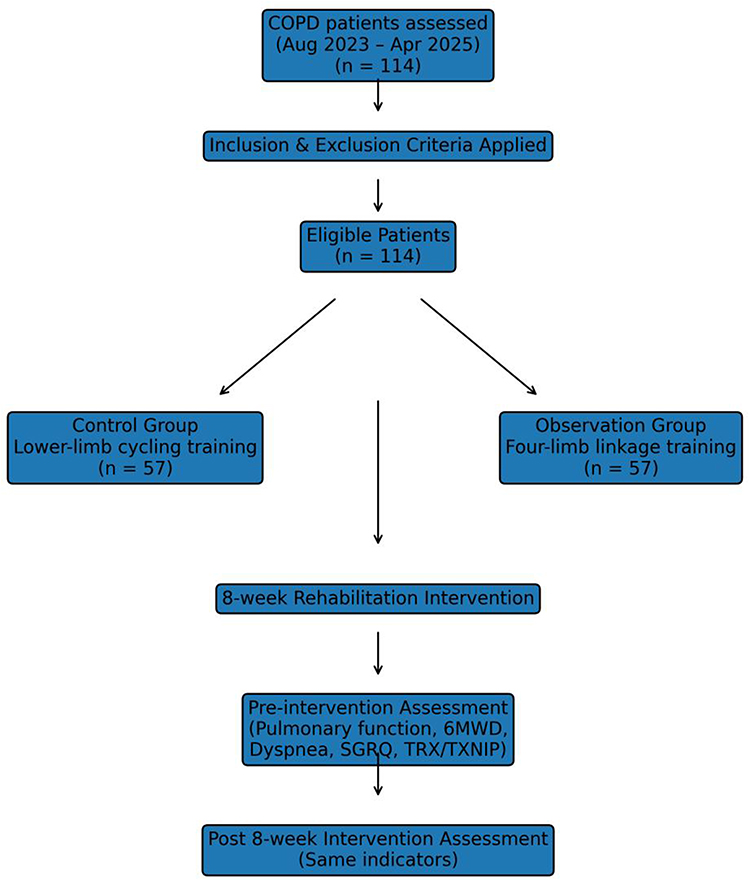 |
Figure 1 Flowchart of patient selection, group allocation, and study procedures. |
Assessment of Comorbidities and Clinical Status
Cardiovascular disease was assessed based on documented medical history, physical examination, resting electrocardiogram (ECG), and echocardiography when available. Patients with unstable angina, decompensated heart failure, recent myocardial infarction (within the previous 6 months), or other cardiovascular conditions that could significantly limit exercise capacity were excluded. The absence of these conditions was considered sufficient to permit participation in rehabilitation training but did not imply the complete absence of subclinical cardiovascular disease. Cerebrovascular disease (CVA), musculoskeletal disorders, and neuromuscular diseases were evaluated based on medical records, neurological examination, and available imaging findings. Patients with conditions that could interfere with safe participation in exercise training were excluded accordingly. Smoking status (current smoker, former smoker, or never smoker) and the use of oxygen therapy (long-term or intermittent) were recorded at baseline for all participants.
Intervention Measures
General Principles and Health Education
Both groups received rehabilitation training in addition to conventional pharmacological treatment, with training intensity and progression adjusted gradually according to patient tolerance. All sessions were conducted under supervision by the rehabilitation or respiratory rehabilitation team. Before each session, patients underwent electrocardiogram (ECG), blood pressure, and oxygen saturation (SpO2) assessment, to ensure sports safety. Safety termination criteria were established—training was immediately stopped if severe arrhythmia, SpO2 <85%, intolerable chest pain, or marked dyspnea occurred. Pulmonary rehabilitation education was provided to all enrolled patients, including disease-related knowledge, self-management, the hazards of smoking, correct medication use, disease prevention, and dietary guidance. Both patients and their families received detailed explanations about the definition, content, and clinical benefits of pulmonary rehabilitation to enhance their awareness of its importance and necessity. During the intervention, psychological support and encouragement were offered to enhance adherence and ensure completion of the 8-week training program.
Control Group: Lower-Limb Cycling Training
Equipment: Stationary lower-limb cycle ergometer (with adjustable resistance and speed display). Frequency and duration: Three sessions per week for 8 consecutive weeks; each session lasted 40 minutes (5–10 minutes warm-up, 20–25 minutes main training, and 5 minutes cool-down). Intensity control: Target intensity was 50%–70% of the maximum heart rate (220 – age) or a Borg subjective fatigue score of 3–4. Initial resistance was set to low, and resistance or main training duration was gradually increased weekly according to patient tolerance. Monitoring and recording: Training duration, average heart rate, maximum heart rate, Borg score, and any adverse events were recorded after each session.
Observation Group: Four-Limb Linkage Training
Equipment: Four-limb linkage training device (with adjustable resistance and coordinated arm-leg movement trajectory). Training mode: Synchronous cyclic movement of upper and lower limbs; the upper limbs performed pushing/pulling motions via handles while the lower limbs performed pedaling movements, emphasizing rhythm and coordination. Frequency and duration: Three sessions per week for 8 consecutive weeks; each session lasted 45 minutes (8–10 minutes warm-up, 25–30 minutes main training, 5–7 minutes cool-down). Intensity and progression: Target heart rate was 50%–70% of the maximum heart rate, or Borg score maintained between 3–4. Initial resistance was low, focusing on familiarizing with motion patterns during the first week. From the second week onward, resistance or main training time was gradually increased. Cardiopulmonary endurance was reassessed in week 4, and intensity was fine-tuned according to the results to ensure a safe and beneficial aerobic load. The main training emphasized good limb coordination, with a rhythm of approximately 50–60 cycles per minute (as shown on the device display), adjusted individually based on tolerance. Additional home practice: Patients were encouraged to perform light upper-limb activities (eg, seated arm flexion-extension) and breathing exercises (abdominal or pursed-lip breathing) on non-training days, though these were not included in quantitative intervention data.
Rehabilitation Evaluation Indicators and Measurement Methods
Pulmonary Function
Measured at Pre-intervention and Post 8-week intervention using a pulmonary function analyzer to determine forced expiratory volume in one second (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, and percentage of predicted FEV1 (FEV1%pred).
Dyspnea Degree
Assessed at Pre-intervention and Post 8-week intervention using the modified Medical Research Council (mMRC) dyspnea scale (Cronbach’s α = 0.819, validity = 0.805)17 and the Borg scale (Cronbach’s α = 0.837, validity = 0.806).18 The mMRC scale ranges from grade 0–4, with higher grades indicating more severe dyspnea. The Borg scale uses a 0–10 visual analog format, where 0 represents no dyspnea and 10 represents extreme dyspnea.
Exercise Endurance
Evaluated at Pre-intervention and Post 8-week intervention using the 6-minute walking test (6MWT). The test was conducted in a 30-meter straight corridor, where patients were instructed to walk as far as possible within 6 minutes. Standardized encouragement phrases were provided, and SpO2 and heart rate were continuously monitored.
Disease Severity
Evaluated at Pre-intervention and Post 8-week intervention using the BODE index for COPD (Cronbach’s α = 0.846, validity = 0.811).19 The BODE index includes four components: body mass index (BMI), degree of airflow limitation (FEV1%pred), dyspnea severity (mMRC score), and exercise endurance (6MWD). The total score is the sum of these components, with higher scores indicating greater disease severity and poorer prognosis.
Quality of Life
Assessed at Pre-intervention and Post 8-week intervention using the St. George’s Respiratory Questionnaire (SGRQ, Cronbach’s α = 0.832, validity = 0.795),20 which includes three dimensions: respiratory symptoms, activity limitation, and disease impact on daily life. Each domain is scored on a 100-point scale, with higher scores indicating poorer quality of life.
Biological Indicator (TRX/TXNIP) Detection
Peripheral Blood Collection and Processing
At Pre-intervention and Post 8-week intervention, 10 mL of fasting peripheral venous blood was collected from each patient in the morning and divided equally into two EDTA anticoagulant tubes, which were gently inverted several times to prevent coagulation. The first tube was used for plasma ELISA detection, and the second tube was used for peripheral blood mononuclear cell (PBMC) isolation and mRNA detection. The first tube was centrifuged at 3000 rpm for 10 min to separate the upper plasma layer, which was then aliquoted, labeled, and stored at −80°C until analysis. The second tube was processed by density gradient centrifugation (Ficoll method) to isolate PBMCs: 2 mL of whole blood was diluted with 0.5 mL of normal saline and gently layered onto 3 mL of lymphocyte separation solution in a 15 mL centrifuge tube to maintain a clear interface. After centrifugation at 2200 rpm for 18 min, four layers were visible: plasma, a white PBMC layer, the separation medium, and red blood cells. The PBMC layer was carefully aspirated using a pipette into a new tube, resuspended with 10 mL PBS, centrifuged at 2500 rpm for 10 min, and the supernatant was discarded. The washing procedure was repeated once. The final cell pellet was resuspended in 1 mL Trizol reagent, thoroughly mixed by pipetting, transferred to a 1.5 mL cryovial, labeled, and stored at −80°C for later use.
mRNA Extraction and Quantitative Real-Time PCR (qRT-PCR) Detection
Total RNA was extracted from PBMC samples using the Trizol method. After adding 0.2 mL chloroform and mixing for 15s, samples were kept on ice for 10 min, then centrifuged at 2000 rpm for 10 min. The upper aqueous phase was transferred to a new tube, and an equal volume of isopropanol was added to precipitate RNA. After incubation at 4°C for 15 min, samples were centrifuged at 12,000 rpm for 10 min. The supernatant was discarded, and the RNA pellet was washed twice with 75% ethanol. After air drying, 30 μL RNase-free water was added to dissolve the RNA. RNA purity was assessed using a UV spectrophotometer at A260/A280 (acceptable range 1.8–2.0), and concentration was calculated based on OD260. RNA integrity was confirmed by 1% agarose gel electrophoresis showing distinct 28S and 18S bands. Qualified RNA (1 μg) was used for reverse transcription. The total reaction volume was 20 μL, containing 4 μL 5×RT Buffer, 4 μL dNTP Mix (2.5 mM each), 2 μL Primer Mix, 2 μL DTT (0.1 M), 1 μL HiFiScript reverse transcriptase, and 7 μL RNA template. Reaction conditions were: 50°C for 50 min, followed by 95°C for 5 min to terminate the reaction, yielding cDNA. TRX and TXNIP mRNA expression levels were measured using SYBR Green-based qRT-PCR. The reaction volume was 15 μL, including 2 μL cDNA template, 1 μL forward primer, 1 μL reverse primer, 10 μL 2×SYBR Green qPCR Mix, and RNase-free water to final volume. Amplification protocol: pre-denaturation at 95°C for 10 min; followed by 40 cycles of 95°C for 10s and 60°C for 30s. GAPDH served as the internal reference gene. Each sample was tested in triplicate. Relative expression levels were calculated using the 2−ΔΔCt method. Primer sequences for TRX and TXNIP are shown in Table 1.
 |
Table 1 Primer Sequence Information |
Protein Expression Detection
Plasma TRX and TXNIP protein concentrations were measured using enzyme-linked immunosorbent assay (ELISA). All reagents were equilibrated to room temperature for 30 min before use, and all procedures were performed strictly in accordance with the kit instructions. The experimental steps were as follows: set up standard and sample wells; add 100 μL of standards or samples to each well and incubate at 37°C for 2 h; discard the liquid and add 100 μL of biotin-labeled antibody working solution to each well, then incubate at 37°C for 1 h; wash the plate three times (200 μL washing buffer per well, 2 min each); add 100 μL of HRP-labeled streptavidin and incubate at 37°C for 1 h; wash the plate five times, then add 90 μL of substrate solution and incubate for 20 min in the dark; add 50 μL of stop solution to terminate the reaction. The optical density (OD) value of each well was measured at 450 nm within 5 min, and sample concentrations were calculated according to the standard curve.
Quality Control
All experiments were performed under identical conditions. Baseline and post-intervention samples were tested in the same batch to minimize inter-assay variability. Negative, positive, and blank controls were included in each assay, and each test was repeated three times with the mean value recorded. All instruments were calibrated with standard samples before analysis. All procedures were performed by the same trained technician to reduce human error.
Statistical Methods
Data visualization was performed using GraphPad Prism 8, and statistical analysis was conducted using SPSS 25.0. The normality of measurement data was tested using the Shapiro–Wilk test, and all data were normally distributed. Measurement data were expressed as ( ), and comparisons between groups were analyzed using independent-samples t-tests. Paired t-tests were used for within-group comparisons (Pre-intervention vs. Post 8-week intervention). Categorical data were expressed as frequencies or percentages and compared between groups using the χ2-test or Fisher’s exact test. A P value < 0.05 was considered statistically significant. As this was a retrospective single-center study, no formal sample size calculation was performed. The sample size was determined by the number of eligible patients during the study period, which may limit the statistical power and generalizability of the findings.
), and comparisons between groups were analyzed using independent-samples t-tests. Paired t-tests were used for within-group comparisons (Pre-intervention vs. Post 8-week intervention). Categorical data were expressed as frequencies or percentages and compared between groups using the χ2-test or Fisher’s exact test. A P value < 0.05 was considered statistically significant. As this was a retrospective single-center study, no formal sample size calculation was performed. The sample size was determined by the number of eligible patients during the study period, which may limit the statistical power and generalizability of the findings.
Results
Comparison of General Data Between the Two Groups
As shown in Table 2, there were no significant differences between the two groups in terms of gender, age, BMI, disease duration, smoking history, and comorbidities (hypertension, diabetes mellitus, coronary heart disease) (P>0.05), indicating comparability between groups.
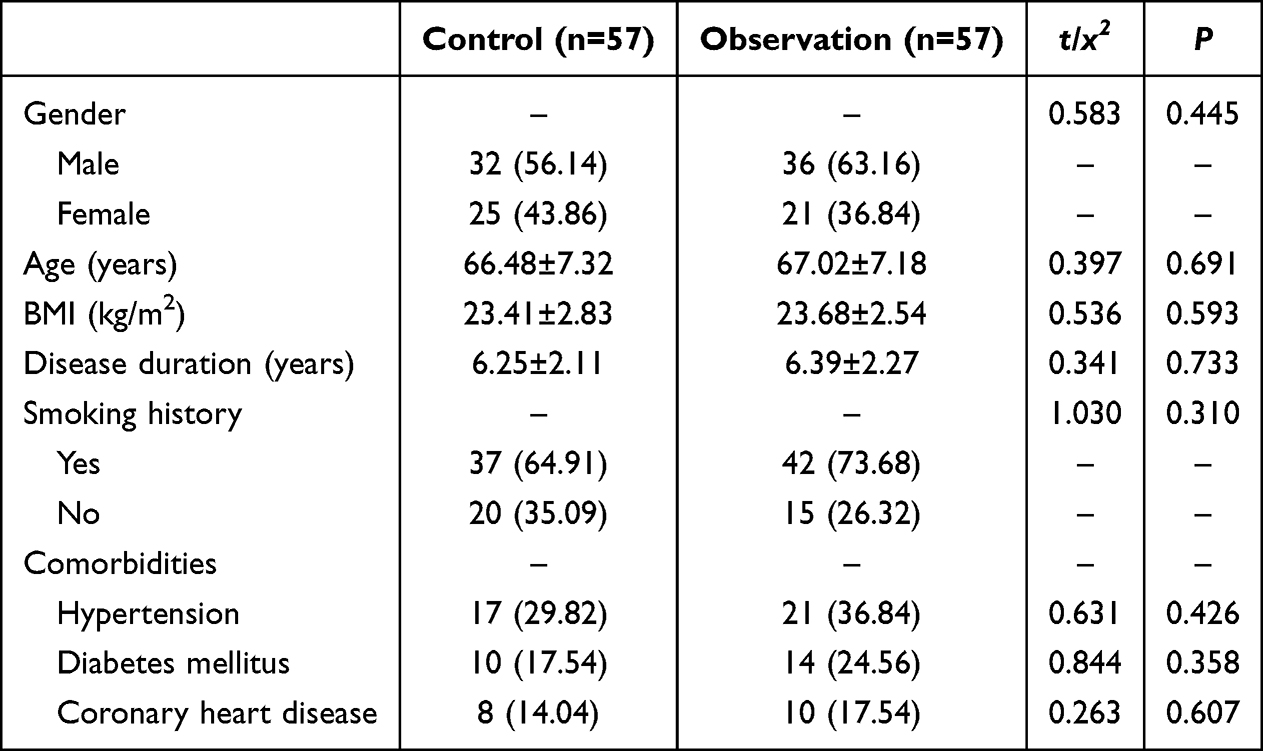 |
Table 2 Comparison of General Data Between the Two Groups ( |

Comparison of Pulmonary Function Between the Two Groups
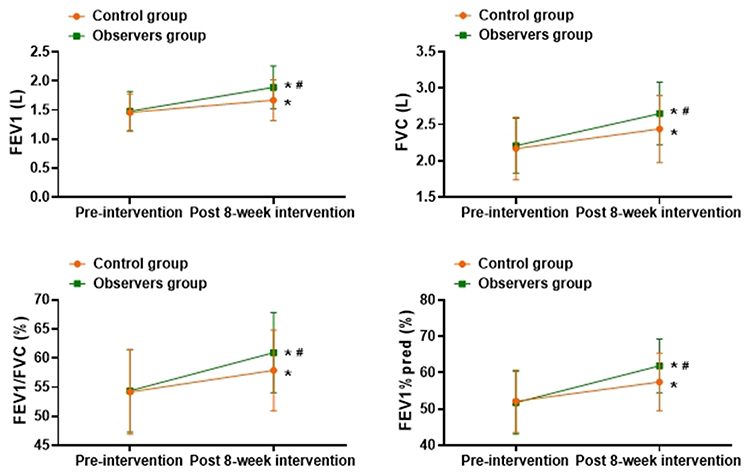
As shown in Figure 2, Post 8-week intervention, FEV1, FVC, FEV1/FVC, and FEV1%pred levels in both groups were significantly higher than those Pre-intervention, with greater improvements observed in the observation group compared with the control group (P<0.05).

Comparison of Dyspnea Severity Between the Two Groups
As shown in Table 3, Post 8-week intervention, mMRC scores and Borg scores of both groups were significantly lower than those Pre-intervention, and the degree of reduction was greater in the observation group compared with the control group (P<0.05).
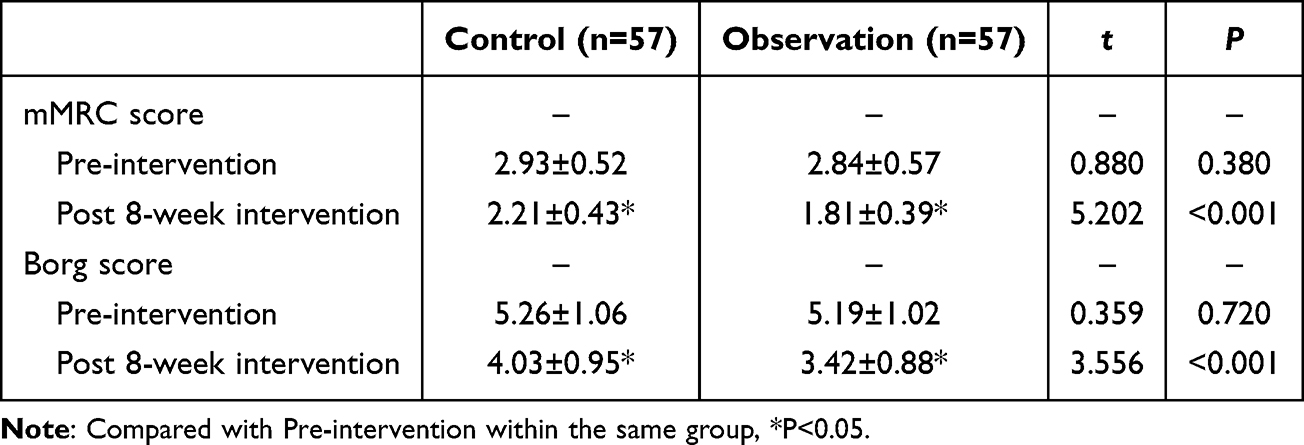 |
Table 3 Comparison of Dyspnea Severity Between the Two Groups ( |

Comparison of Exercise Endurance and Disease Severity Between the Two Groups
As shown in Table 4, Post 8-week intervention, 6MWD in both groups was significantly higher and BODE scores were significantly lower than those Pre-intervention, with greater changes in the observation group compared with the control group (P<0.05).
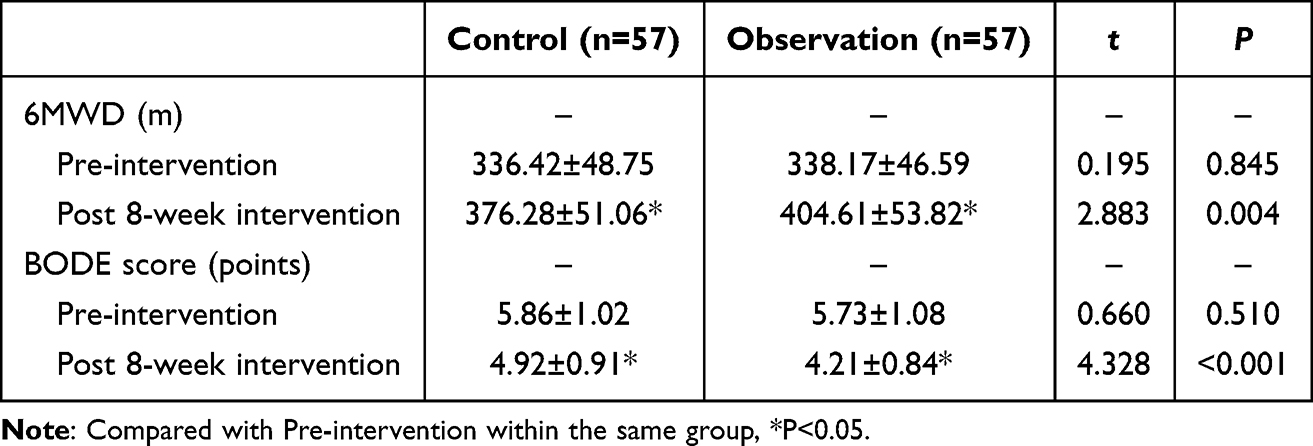 |
Table 4 Comparison of Exercise Endurance and Disease Severity Between the Two Groups ( |

Comparison of Quality of Life Between the Two Groups
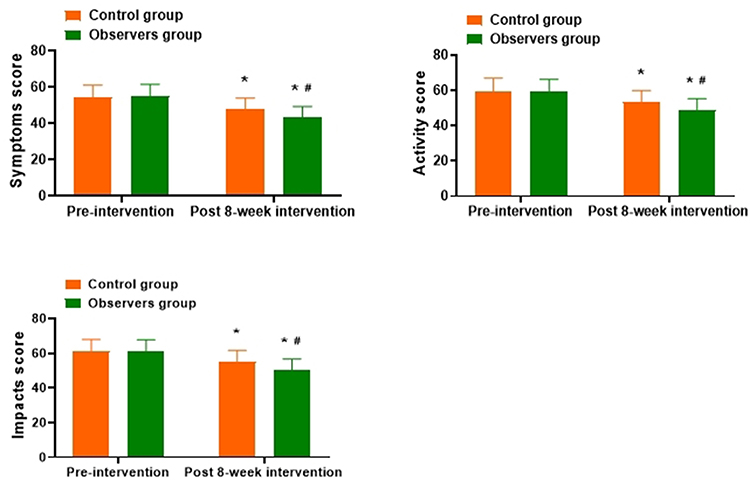
As shown in Figure 3, Post 8-week intervention, the respiratory symptoms score, activity limitation score, and disease impact score in both groups were significantly lower than those Pre-intervention, and the changes were greater in the observation group compared with the control group (P<0.05).

Comparison of Antioxidative Stress Indicators Between the Two Groups
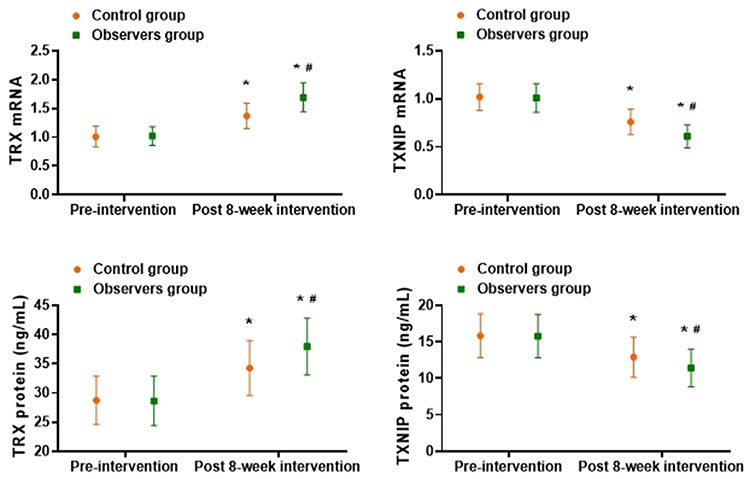
As shown in Figure 4, Post 8-week intervention, both TRX mRNA and protein expression levels in peripheral blood were significantly increased, while TXNIP mRNA and protein expression levels were significantly decreased in both groups compared with Pre-intervention. The changes in the observation group were more pronounced than those in the control group (P<0.05).

Summary of Key Findings
Taken together, the results demonstrated that four-limb linkage training was associated with greater improvements in pulmonary function, exercise capacity, dyspnea severity, and quality of life compared with lower-limb training alone, accompanied by significant modulation of TRX and TXNIP expression levels. These findings provide integrated clinical and molecular evidence supporting the potential antioxidative role of four-limb linkage training in COPD rehabilitation.
Discussion
The results of this study demonstrated that systematic four-limb linkage training can significantly improve lung function, exercise endurance, dyspnea, and quality of life in patients with COPD. It also modulated the expression levels of oxidative stress–related molecular markers, as reflected by upregulated TRX and downregulated TXNIP. These findings suggest that four-limb linkage training not only promotes respiratory rehabilitation at the functional level but may also improve the pulmonary oxidative and inflammatory microenvironment at the molecular level, thereby delaying disease progression. While the present findings are consistent with the study objectives and supported by both functional and molecular data, further validation through prospective, multicenter studies with larger sample sizes is warranted to confirm their generalizability and long-term clinical impact.
Effects of Four-Limb Linkage Training on Pulmonary Function and Dyspnea
The core pathophysiological features of COPD are persistent airflow limitation and chronic inflammation, leading to reduced lung elasticity, ventilation–perfusion imbalance, and respiratory muscle dysfunction.21 Conventional lower-limb cycle training mainly focuses on enhancing lower-limb endurance but provides limited engagement of respiratory accessory muscles and upper-limb systems, thus offering only modest improvement in ventilation efficiency. In contrast, four-limb linkage training coordinates simultaneous upper- and lower-limb movements, enhancing skeletal muscle metabolism and promoting thoracic expansion and synergistic contraction of respiratory muscles.22 This coordination improves respiratory muscle mechanics and ventilation distribution. In this study, the improvements in FEV1 and FVC in the observation group after the 8-week intervention were significantly greater than those in the control group, with a notable increase in the FEV1/FVC ratio, suggesting that four-limb coordination exercises can more effectively enhance airflow dynamics. Compared with the study by Qiao et al,23 which demonstrated improvements in pulmonary function following lower-limb training alone, the present study observed a greater magnitude of improvement, particularly in FEV1, in patients undergoing four-limb linkage training. This discrepancy may be attributed to differences in training modality, muscle group involvement, and exercise intensity regulation. Lower-limb training primarily enhances peripheral muscle endurance, whereas four-limb linkage training engages both upper- and lower-limb muscle groups simultaneously, thereby increasing ventilatory demand, respiratory muscle recruitment, and cardiopulmonary interaction. And, coordinated whole-body movement may induce more pronounced systemic adaptations, including improved thoracic mobility and peripheral circulation, which together contribute to enhanced ventilation and gas exchange efficiency. Improvement in microcirculation may play a crucial role in these effects. Enhanced peripheral and pulmonary microvascular perfusion facilitates oxygen delivery to both respiratory and skeletal muscles, improves oxygen utilization efficiency, and reduces local hypoxia-induced oxidative stress. Improved microcirculation may also accelerate metabolic waste clearance and attenuate exercise-induced fatigue, thereby contributing to better ventilatory mechanics and symptom relief in COPD patients. Additionally, the significant reductions in mMRC and Borg scores indicate that four-limb linkage training can alleviate dyspnea symptoms in COPD patients. Previous studies24 have shown that dyspnea is not only associated with airflow limitation but also with respiratory muscle load, exercise tolerance, and emotional state. Coordinated limb exercise increases muscle oxygen supply and reduces lactic acid accumulation, thereby decreasing exercise-induced dyspnea. Moreover, exercise itself modulates the autonomic nervous system, reduces sympathetic overactivity, and stabilizes respiratory rhythm and anxiety, indirectly reducing subjective breathing burden.25
Effects of Four-Limb Linkage Training on Exercise Endurance and Disease Severity
In this study, the 6MWD of the observation group increased significantly after the intervention, with a greater improvement than that of the control group, indicating that four-limb linkage training effectively enhances exercise endurance. Previous evidence26 suggests that reduced exercise capacity in COPD patients is mainly due to skeletal muscle atrophy, mitochondrial dysfunction, and impaired peripheral oxidative metabolism. Four-limb linkage training, by engaging large muscle groups in coordinated movement, can promote mitochondrial recovery and enhance muscle oxygen utilization efficiency. Consistent with the findings of Zhang et al,27 who reported an average increase of over 60 m in 6MWD and a significant reduction in BODE scores following comprehensive whole-body training, this study also found a marked decrease in BODE scores, suggesting that four-limb linkage training may delay disease progression and improve prognostic indicators. The underlying mechanisms likely involve enhanced cardiopulmonary interaction, improved oxygen delivery–consumption balance, and reduced systemic inflammation.
Improvements in Quality of Life and Psychological Benefits
Quality of life is a key outcome indicator in evaluating COPD rehabilitation interventions. In this study, the observation group showed significantly lower SGRQ scores in symptom, activity limitation, and disease impact domains than the control group, indicating a superior effect of four-limb linkage training in enhancing daily functioning and life satisfaction. Previous studies28,29 have shown that long-term exercise interventions can enhance self-efficacy, health control perception, social participation, and emotional well-being, thereby facilitating sustained disease management. Notably, the rhythmic and visual feedback characteristics of four-limb linkage training may enhance motivation and compliance. Compared with monotonous lower-limb training, coordinated four-limb exercises are more engaging, reduce training fatigue, and improve adherence. Moreover, regular exercise can upregulate brain-derived neurotrophic factor (BDNF) and dopaminergic activity, thereby exerting positive effects on emotional regulation and cognitive function,30 which indirectly enhances psychological well-being and overall quality of life.
Mechanistic Insights into Antioxidative Stress Effects
Oxidative stress is recognized as a central pathological process driving COPD progression. Chronic airway exposure leads to lipid peroxidation, protein oxidation, and DNA damage, while weakening antioxidant defenses, thus perpetuating redox imbalance, inflammation, and tissue remodeling.31,32 The TRX system acts as a critical endogenous antioxidant barrier, repairing oxidized proteins through its disulfide-reducing capacity and suppressing excessive apoptotic signaling.33 Conversely, TXNIP negatively regulates TRX by direct binding, reducing the cell’s ability to eliminate ROS and amplifying inflammatory injury.34 In this study, four-limb linkage training significantly upregulated TRX mRNA and protein levels while downregulating TXNIP expression, consistent with Chaves et al,35 who reported that exercise interventions activate the TRX system and attenuate oxidative inflammation. Mechanistically, moderate aerobic exercise activates the PI3K/Akt and Nrf2 pathways, promoting antioxidant enzyme expression and suppressing proinflammatory cytokine release.36,37 Additionally, exercise improves tissue perfusion and mitochondrial oxidative phosphorylation, thereby reducing ROS generation at the source.38 Thus, four-limb linkage training may exert its effects through a “multi-target” mechanism—enhancing antioxidation, suppressing inflammation, and optimizing metabolism—to collectively improve the pulmonary microenvironment in COPD. Taken together, these findings suggest that four-limb linkage training may improve COPD outcomes through an integrated mechanism involving enhanced microcirculation, reduced oxidative stress, and restoration of redox homeostasis mediated by the TRX/TXNIP pathway.
Comparative Perspective and Clinical Implications
Compared with existing studies on COPD rehabilitation, this study introduces an innovative training model. Most prior research has focused on isolated lower-limb endurance or respiratory muscle training. For instance, Chen et al39 reported that lower-limb training improved 6MWD but had limited effects on FEV1. The current study shows that whole-body coordination training more effectively synchronizes respiratory and systemic circulation functions, leading to superior outcomes. Clinically, the four-limb linkage training device is simple, safe, and easily implemented, particularly suitable for home-based or outpatient rehabilitation in moderate-to-severe COPD patients. By enhancing respiratory efficiency and antioxidative defense across multiple dimensions, it may reduce exacerbation frequency, slow disease progression, and improve long-term prognosis. Future COPD management should consider combining this training with nutritional support, psychological intervention, and pharmacological therapy to achieve comprehensive physiological and psychological rehabilitation.
Limitations of the Study
This study has several limitations that should be considered. (1) This was a single-center retrospective study with a relatively limited sample size. Although baseline characteristics were comparable between groups, the retrospective design may introduce selection bias and limit the generalizability of the findings. Therefore, prospective, multicenter randomized controlled trials with larger sample sizes are needed to further confirm the clinical efficacy and antioxidative mechanisms of four-limb linkage training in patients with COPD. (2) The intervention and follow-up period was limited to 8 weeks, which allowed assessment of short-term functional and biochemical outcomes but did not permit evaluation of long-term clinical endpoints. Important outcomes such as acute exacerbation frequency, rehospitalization rate, disease progression, and mortality were not assessed. Future studies should incorporate longer intervention durations and extended follow-up to determine the sustainability and long-term prognostic benefits of this training modality. (3) Although the present study explored the TRX/TXNIP pathway as a representative antioxidative mechanism, oxidative stress and inflammation in COPD are mediated by multiple interacting pathways. Other antioxidant enzymes and inflammatory biomarkers, were not measured. Comprehensive assessment of these markers would provide a more complete understanding of the molecular mechanisms underlying exercise-based pulmonary rehabilitation. (4) Exercise intensity was adjusted according to patient tolerance; however, fully individualized exercise prescriptions based on objective cardiopulmonary exercise testing or stratification by COPD severity were not implemented. Standardized yet personalized training protocols tailored to different disease stages may further optimize both the safety and effectiveness of four-limb linkage training. (5) Psychological and emotional outcomes were not systematically evaluated in this study. Given the close association between COPD, anxiety, depression, and impaired quality of life, future research should incorporate validated psychological assessment tools to better elucidate the mental health benefits of four-limb linkage training and its role in comprehensive pulmonary rehabilitation.
Conclusion
This study suggests that systematic four-limb linkage training is associated with significant improvements in pulmonary function, exercise tolerance, dyspnea, and quality of life in patients with COPD, accompanied by favorable modulation of oxidative stress–related markers through the TRX/TXNIP signaling pathway. Compared with conventional lower-limb training, four-limb linkage training demonstrated more comprehensive benefits in cardiopulmonary coordination, systemic metabolism, and antioxidative defense.
However, given the retrospective design and relatively short intervention period, causal relationships and long-term clinical effects cannot be definitively established. Further prospective, multicenter studies with extended follow-up are warranted to confirm the sustainability, generalizability, and long-term clinical value of this rehabilitation strategy. Nevertheless, as a safe, feasible, and easily implementable exercise-based intervention, four-limb linkage training represents a promising adjunctive approach for comprehensive COPD rehabilitation.
Funding
2023 Chongqing Science and Health Joint Medical Research Project General Project “Study on the Clinical Efficacy and Antioxidant Mechanism of Limb Linkage Training on Patients with Chronic Obstructive Pulmonary Disease” (No. 2023MSXM062).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Han YP, He BF, Zhang J. Research progress of chronic obstructive pulmonary disease in young people and pre-COPD. Zhonghua Yu Fang Yi Xue Za Zhi. 2023;57(8):1164–14. doi:10.3760/cma.j.cn112150-20220929-00939
2. Cui J, Guo YF, Tong YQ, et al. Prevalence, patterns and prognosis of multimorbidity among middle-aged and elderly inpatients with chronic obstructive pulmonary disease. Zhonghua Yu Fang Yi Xue Za Zhi. 2023;57(5):701–709. doi:10.3760/cma.j.cn112150-20230216-00117
3. Wang JW, Huang YN, Zhang M, et al. Comparison of lung function and inflammatory markers and analysis of risk factors for acute exacerbations in patients with chronic obstructive pulmonary disease and persistent airflow limitation asthma. Zhonghua Yi Xue Za Zhi. 2025;105(24):1981–1988. doi:10.3760/cma.j.cn112137-20250208-00278
4. Wu J, Tang YY, Jiang S, et al. Analysis of mortality trend and characteristic of chronic obstructive pulmonary disease among residents in China from 2004 to 2020. Zhonghua Yu Fang Yi Xue Za Zhi. 2023;57(8):1135–1140. doi:10.3760/cma.j.cn112150-20230103-00005
5. Peng LG, Liu SM, Pu JQ, et al. Predictors of adverse outcomes in patients with chronic obstructive pulmonary disease and pulmonary embolism and the predictive value of the simplified pulmonary embolism severity index. Zhonghua Yi Xue Za Zhi. 2024;104(42):3889–3895. doi:10.3760/cma.j.cn112137-20240603-01255
6. Yang TY, Qumu MSW, Li XP, et al. Correlation of body composition indicators with exercise capacity and nutritional status in male patients with chronic obstructive pulmonary disease. Zhonghua Yi Xue Za Zhi. 2024;104(36):3402–3408. doi:10.3760/cma.j.cn112137-20240129-00227
7. Brunton NM, Barbour DJ, Gelinas JC, et al. Lower-limb resistance training reduces exertional dyspnea and intrinsic neuromuscular fatigability in individuals with chronic obstructive pulmonary disease. J Appl Physiol. 2023;134(5):1105–1114. doi:10.1152/japplphysiol.00303.2022
8. Kohlbrenner D, Aregger C, Osswald M, et al. Blood-flow-restricted strength training combined with high-load strength and endurance training in pulmonary rehabilitation for COPD: a case report. Phys Ther. 2021;101(6). doi:10.1093/ptj/pzab063
9. Huo C, Xu G, Li Z, et al. Limb linkage rehabilitation training-related changes in cortical activation and effective connectivity after stroke: a functional near-infrared spectroscopy study. Sci Rep. 2019;9(1):6226. doi:10.1038/s41598-019-42674-0
10. Zhao Y, Qi QL, Hu MJ, et al. The mechanism of mitochondrial damage in chronic obstructive pulmonary disease induced by cigarette smoke and its therapeutic implications. Zhonghua Jie He He Hu Xi Za Zhi. 2025;48(10):970–978. doi:10.3760/cma.j.cn112147-20250603-00298
11. Zhang MZ, Zhang RY, Liu J, et al. Advances in the role of autoimmune mechanisms in chronic obstructive pulmonary disease. Zhonghua Jie He He Hu Xi Za Zhi. 2023;46(11):1131–1136. doi:10.3760/cma.j.cn112147-20230731-00037
12. Gao X, Bao R, Feng Y, et al. Heme oxygenase-1 reduces inflammatory response by inhibiting thioredoxin interacting protein/NOD-like receptor protein 3 inflammasome activation in RAW264.7 cells. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022;34(7):689–692. doi:10.3760/cma.j.cn121430-20211223-01913
13. Ni HQ, Ou ZY, Xia RF, et al. XBP1 modulates hypoxia/reoxygenation injury in mouse renal tubular epithelial cells through TXNIP-NLRP3 signaling pathway. Zhonghua Yi Xue Za Zhi. 2020;100(48):3863–3869. doi:10.3760/cma.j.cn112137-20201102-02996
14. Sharma I, Yadav KS, Mugale MN. Redoxisome and diabetic retinopathy: pathophysiology and therapeutic interventions. Pharmacol Res. 2022;182:106292. doi:10.1016/j.phrs.2022.106292
15. Li QY, Li M, Feng Y, et al. Chronic intermittent hypoxia induces thioredoxin system changes in a gender-specific fashion in mice. Am J Med Sci. 2012;343(6):458–461. doi:10.1097/MAJ.0b013e318235b03e
16. Vestbo J, Hurd SS, Rodriguez-Roisin R. An overview of global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (GOLD) (revised 2011). Zhonghua Yi Xue Za Zhi. 2012;92(14):937–938. Danish
17. Wang YX, Sun TY, Li YM, et al. Correlation between pulmonary quantitative CT measurement indicators and respiratory symptoms in patients with chronic obstructive pulmonary disease in stable stage. Zhonghua Yi Xue Za Zhi. 2023;103(38):3017–3025. doi:10.3760/cma.j.cn112137-20230418-00627
18. Sang PP, Li J, Tan X-D, et al. Associations between Borg’s rating of perceived exertion and changes in urinary organic acid metabolites after outdoor weight-bearing hiking. World J Psychiatry. 2023;13(5):234–246. doi:10.5498/wjp.v13.i5.234
19. Demircioğlu H, Cihan FG, Kutlu R, et al. Frequency of sarcopenia and associated outcomes in patients with chronic obstructive pulmonary disease. Turk J Med Sci. 2020;50(5):1270–1279. doi:10.3906/sag-1909-36
20. Wan Q, Guo Z, Caikai S, et al. Expression of serous fibroblast growth factor 7 and related inflammatory factors in patients with acute exacerbation of chronic obstructive pulmonary disease. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021;33(4):421–426. doi:10.3760/cma.j.cn121430-20201231-00786
21. Zhou DS, Xu L, Zhang Y, et al. Establishment and effect evaluation of nomogram model for diagnosis and prediction of pulmonary hypertension in patients with chronic obstructive pulmonary disease. Zhonghua Yi Xue Za Zhi. 2022;102(38):3019–3025. doi:10.3760/cma.j.cn112137-20220512-01045
22. Gopaul U, van Vliet P, Callister R, et al. COMbined Physical and somatoSEnsory training after stroke: development and description of a novel intervention to improve upper limb function. Physiother Res Int. 2019;24(1):e1748. doi:10.1002/pri.1748
23. Qiao Z, Kou Z, Zhang J, et al. Optimal intensity and type of lower limb aerobic training for patients with chronic obstructive pulmonary disease: a systematic review and network meta-analysis of RCTs. Ther Adv Respir Dis. 2025;19:17534666251323190. doi:10.1177/17534666251323190
24. Jiang X, Cong S, Yang M, et al. Prevalence of chronic respiratory symptoms and dyspnea and related factors in residents in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2022;43(3):315–323. doi:10.3760/cma.j.cn112338-20211102-00844
25. Zhu FJ, Fan SL, Liu GX, et al. Effect of early rehabilitation training on motor function and neural function of patients with brainstem hemorrhage after body-oriented individualized surgery. Zhonghua Yi Xue Za Zhi. 2023;103(45):3670–3675. doi:10.3760/cma.j.cn112137-20231012-00722
26. Wu LL, He W, Lin FJ, et al. Advances in pathogenic mechanisms and pulmonary rehabilitation strategies for skeletal muscle dysfunction in chronic obstructive pulmonary disease. Zhonghua Jie He He Hu Xi Za Zhi. 2024;47(12):1163–1169. doi:10.3760/cma.j.cn112147-20240624-00358
27. Zhang JH, Zhang LQ, Yang YP, et al. Clinical effect of nutritional and psychological intervention combined with pulmonary rehabilitation exercise on patients with chronic obstructive pulmonary disease. Zhonghua Yi Xue Za Zhi. 2020;100(2):110–115. doi:10.3760/cma.j.issn.0376-2491.2020.02.006
28. Yu Z, Xie G, Qin C, et al. Study on the benefit of postoperative exercise rehabilitation in patients with lung cancer complicated with chronic obstructive pulmonary disease. Zhongguo Fei Ai Za Zhi. 2022;25(1):14–20. doi:10.3779/j.issn.1009-3419.2021.102.51
29. Hearn B, Biscaldi-Schäfer M, Fleischhaker C. Current state of research on surf therapy and its possible application as an intervention for adolescent depression. Z Kinder Jugendpsychiatr Psychother. 2025;53(1):17–30. doi:10.1024/1422-4917/a001002
30. Lopes EDS, Coelho FGDM, Tribess S, et al. Benefits of multimodal exercise intervention for BDNF and cytokines levels, cognitive function, and motor functionality in alzheimer’s disease: a preliminary study. Int J Environ Res Public Health. 2025;22(8):1245. doi:10.3390/ijerph22081245
31. Rouadi PW, Idriss SA, Naclerio RM, et al. Immunopathological features of air pollution and its impact on inflammatory airway diseases (IAD). World Allergy Organ J. 2020;13(10):100467. doi:10.1016/j.waojou.2020.100467
32. Pinto P, Donzì D, Di Vincenzo S, et al. Increased TSLP and oxidative stress reflect airway epithelium injury upon cigarette smoke exposure. Is there a role for carbocysteine? Toxicology. 2025;515:154160. doi:10.1016/j.tox.2025.154160
33. Kansal H, Chopra V, Garg K, et al. Role of thioredoxin in chronic obstructive pulmonary disease (COPD): a promising future target. Respir Res. 2023;24(1):295. doi:10.1186/s12931-023-02574-4
34. Lin PY, Lee K-Y, Ho S-C, et al. Oxidative stress triggers Itch-mediated TXNIP degradation and NF-κB activation promoting chronic obstructive pulmonary disease. Respir Res. 2025;26(1):286. doi:10.1186/s12931-025-03369-5
35. Chaves AB, Miranda ER, Mey JT, et al. Exercise reduces the protein abundance of TXNIP and its interacting partner REDD1 in skeletal muscle: potential role for a PKA-mediated mechanism. J Appl Physiol. 2022;132(2):357–366. doi:10.1152/japplphysiol.00229.2021
36. Yi XJ, Sun Y-X, Yao -T-T, et al. Effects of acute and chronic exercise on fat PI3K/AKT/GLUT4 signal pathway in type 2 diabetic rats. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2020;36(1):12–16. doi:10.12047/j.cjap.5802.2020.003
37. Sugiura T, Nawaz S, Ferrell BE, Yoshida T. Induced pluripotent stem cells: a new dawn for the treatment of ischemic cardiomyopathy. Innovation Discovery. 2024;1(4):31. doi:10.53964/id.2024031
38. Geng YW, Lin QQ, Wang XY, et al. Effects of aerobic interval training on myocardial oxidative stress and inflammation in rats with myocardial infarction and its mechanism. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2021;37(4):439–444. doi:10.12047/j.cjap.6094.2021.043
39. Chen HX, Zhan Y-X, Ou H-N, et al. Effects of lower body positive pressure treadmill on functional improvement in knee osteoarthritis: a randomized clinical trial study. World J Clin Cases. 2021;9(34):10604–10615. doi:10.12998/wjcc.v9.i34.10604
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum Derivatives of Reactive Oxygen Metabolites are Associated with Severity of Chronic Obstructive Pulmonary Disease and Affected by a p53 Gene Polymorphism
Yamamura K, Nojiri M, Nishiki K, Kato R, Shinomiya S, Takahara Y, Oikawa T, Ishizaki T, Toga H, Mizuno S
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1589-1600
Published Date: 13 July 2022
Dental Pulp Stem Cells Ameliorate Elastase-Induced Pulmonary Emphysema by Regulating Inflammation and Oxidative Stress
Gao X, Liu Z, Wang Z
Journal of Inflammation Research 2023, 16:1497-1508
Published Date: 8 April 2023
Physical Activity, Depression and Quality of Life in COPD – Results from the CLARA II Study
Horner A, Olschewski H, Hartl S, Valipour A, Funk GC, Studnicka M, Merkle M, Kaiser B, Wallner EM, Brecht S, Lamprecht B
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2755-2767
Published Date: 29 November 2023
Lung Ultrasound Assessment of Lung Hyperinflation in Patients with Stable COPD: An Effective Diagnostic Tool
Chen Y, Li J, Zhu Z, Lyu G
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:319-330
Published Date: 27 January 2024
Exercise Prescription Training in Chronic Obstructive Pulmonary Disease: Benefits and Mechanisms
Liu S, Yang A, Yu Y, Xu B, Yu G, Wang H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1071-1082
Published Date: 15 April 2025