")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Lung Ultrasound Assessment of Lung Hyperinflation in Patients with Stable COPD: An Effective Diagnostic Tool
Authors Chen Y, Li J, Zhu Z, Lyu G
Received 22 September 2023
Accepted for publication 20 January 2024
Published 27 January 2024 Volume 2024:19 Pages 319—330
DOI https://doi.org/10.2147/COPD.S441374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Yongjian Chen,1 Jingyun Li,2 Zhixing Zhu,3 Guorong Lyu1,2
1Department of Ultrasound, the Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian, People’s Republic of China; 2School of Medicine, Quanzhou Medical College, Quanzhou, Fujian, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, the Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian, People’s Republic of China
Correspondence: Guorong Lyu, Department of Ultrasound, the Second Affiliated Hospital of Fujian Medical University, No. 34 North Zhongshan Road, Licheng District, Quanzhou, Fujian, 362000, People’s Republic of China, Tel +86-595-22525702, Email [email protected]
Purpose: To evaluate the degree of lung hyperinflation (LH) in patients with stable chronic obstructive pulmonary disease (COPD) by lung ultrasound score (LUS) and assess its value.
Patients and Methods: We conducted a study of 149 patients with stable COPD and 100 healthy controls recruited by the Second Affiliated Hospital of Fujian Medical University. The pleural sliding displacement (PSD) was measured, the sliding of the pleura in different areas was observed, and LUS was calculated from both of them. The diaphragm excursion (DE), residual capacity (RV), total lung capacity (TLC), inspiratory capacity (IC) and functional residual capacity (FRC) were measured. We described the correlation between ultrasound indicators and pulmonary function indicators reflecting LH. Multiple linear regression analysis was used. The ROC curves of LUS and DE were drawn to evaluate their diagnostic efficacy, and De Long method was used for comparison.
Results: (1) The LUS of patients with stable COPD were positively correlated with RV, TLC, RV/TLC and FRC and negatively correlated with IC and IC/TLC (r1=0.72, r2=0.41, r3=0.72, r4=0.70, r5=− 0.56, r6=− 0.65, P < 0.001). The correlation was stronger than that between DE at maximal deep inspiration and the corresponding pulmonary function indices (r1=− 0.41, r2=− 0.26, r3=− 0.40, r4=− 0.43, r5=0.30, r6=0.37, P < 0.001). (2) Multiple linear regression analysis showed that LUS were significantly correlated with IC/TLC and RV/TLC. (3) With IC/TLC< 25% and RV/TLC> 60% as the diagnostic criterion of severe LH, the areas under the ROC curves of LUS and DE at maximal deep inspiration for diagnosing severe LH were 0.914 and 0.385, 0.845 and 0.543, respectively (P < 0.001).
Conclusion: The lung ultrasound score is an important parameter for evaluating LH. LUS is better than DE at maximal deep inspiration for diagnosing severe LH and is expected to become an effective auxiliary tool for evaluating LH.
Keywords: chronic obstructive pulmonary disease, lung hyperinflation, ultrasound, pleural sliding displacement, pulmonary function
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic respiratory disease characterized by incomplete reversible airflow limitation and progressive development.1,2 Due to airflow limitation, the air trapped in the lungs during exhalation in COPD patients easily causes lung hyperinflation (LH) and increased intrathoracic pressure. LH can be divided into static lung hyperinflation (sLH) and dynamic lung hyperinflation (dLH). It is characterized by an increase in functional residual capacity (FRC) and a decrease in inspiratory capacity (IC), which eventually lead to dyspnea3 and reduce exercise capacity.4 It also can affect the ventilatory load and respiratory muscle capacity, and even affect the cardiovascular system in severe cases.5 Therefore, the assessment of LH is of great help in the treatment, exercise endurance, and quality of life of COPD patients.
Pulmonary function tests are commonly used to evaluate LH in clinical practice. Total lung capacity (TLC), reserve volume (RV), IC, RV/TLC, IC/TLC, etc., can reflect LH to varying degrees.6–8 Usually, the change in the IC in COPD patients during exercise is monitored to assess dLH,9 but this method assumes that the TLC value remains the same, when in fact COPD exacerbations and bronchial relaxation affect the TLC; therefore, this method has certain limitations. Among these pulmonary function indicators, RV/TLC > 60% and IC/TLC < 25% are indicators of severe LH and are also prerequisites for lung volume reduction surgery,9–11 and their value for evaluating LH has been widely recognized. In addition to the lung function indicators described above for evaluating LH, the area under the forced expiratory flow-volume loop (AreaFE) is expressed as a percentage of the reference value (AreaFE%), and manual/metronome paced tachypnea (MPT), metronome-paced incremental hyperventilation (MPIH) and the impulse moisturizer oscillometry system (IOS) can also be used to evaluate LH.12–17 However, the above evaluation methods have their own shortcomings, such as a lack of large-sample-size research verification, lack of unified standards for reference values, relatively few comparative studies, and easy overdiagnosis. Therefore, RV/TLC and IC/TLC are still more commonly used in pulmonary function tests to evaluate LH.
Pulmonary function tests require the cooperation of patients, which is time-consuming and is likely to make the patients uncomfortable.18 Whether there is a more convenient auxiliary examination method for assessing the severity of LH in COPD patients has become a key issue in clinical research. Ultrasound has the advantages of no radiation, simple operation, and real-time observation, which has a certain research prospect. Compared with the extensive research performed on the application of ultrasound in COPD,19 the study on ultrasound assessment of LH is less well established and needs further evaluation. Because LH can promote the decline of diaphragm contractility in COPD patients,20 current research has focused on diaphragm excursion (DE) and similar phenomena.21 Relevant study22 has found that pleura sliding displacement (PSD) can be reduced and the pleura sliding can be weakened or disappeared in COPD patients with the increase in lung capacity indicators reflecting LH such as TLC and RV. This inspires us that lung ultrasound is expected to predict the severity of LH in COPD patients to a certain extent, which is worthy of further research.
Materials and Methods
Participants
A total of 149 patients with stable COPD were selected from the ultrasound department of our hospital from December 2020 to August 2023, and 100 healthy adults were randomly selected as the control group. Inclusion criteria for stable COPD patients: According to the 2020 edition of the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD), the diagnosis was confirmed based on clinical symptoms, signs, chest X-ray or CT, lung function and other examinations. The exclusion criteria for the stable COPD group were as follows: (1) history of chronic respiratory diseases other than COPD; (2) history of pleural and peritoneal diseases; (3) history of chest or abdominal trauma or surgery; (4) chronic metabolic disease; (5) history of drug use affecting the skeletal muscle tissue structure; (6) inability to cooperate with clinical examinations (such as HRCT, ultrasound, etc.), threatening the integrity of the clinical data; and (7) history of respiratory infection in the month prior to study. The inclusion criteria for the control group were as follows: forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) ≥70% and FEV1≥80% of the predicted value. Participants with no previous history of respiratory disease were eligible. The other inclusion criteria were the same as those in the stable COPD group. The general data of the subjects, including sex, body mass index, age and smoking, were collected, and all participants completed the COPD Assessment Test (CAT), modified Medical Research Council (mMRC) Dyspnea Scale, pulmonary function tests and ultrasound. This study was approved by the hospital ethics committee, and all subjects agreed to undergo the examinations and signed the informed consent form.
Instruments and Methods
A color Doppler ultrasound diagnostic apparatus (Mindray Resona I9S, Shenzhen, China) was used to detect the pleural sliding displacement (PSD) and observe the pleural sliding condition with a high-frequency linear array probe (frequency 4–15 MHz). Sliding of the pleura was observed by scanning the anterior chest wall, lateral chest wall and posterior chest wall in 72 intercostal spaces, and the chest wall was divided into 16 lung regions, as shown in Figure 1. The probe was scanned longitudinally and vertically in each intercostal space. (1) Anterior chest wall and lateral chest wall examination: The patient was placed in the supine position or lateral position, and the hands were held to widen the intercostal space. The patient was observed along the bilateral parasternal line, midclavicular line, anterior axillary line, and midaxillary line from top to bottom according to the prescribed intercostal space. (2) Posterior chest wall examination: The patient was in a sitting position, with hands crossed and folded in front of the torso, and the body was bent forward so that the scapula was moved up and the posterior intercostal space was widened as far as possible. The patient was observed along the bilateral spinal paravertebral line, scapular line, and posterior axillary line from top to bottom according to the prescribed intercostal space. To detect PSD, the probe was placed in the midaxillary line of the diaphragm section of the patient, and the movement of the pleura and lung tissue toward or away from the liver was observed, along with the respiratory movement. The distance between the junction of the lung and the liver and the left edge of the acoustic window of the ultrasound instrument was measured along the direction of the pleural line at the end of expiration and the end of inspiration, respectively, and the difference between the two was the PSD, as shown in Figure 2. The normal critical value of PSD was < 12 mm for males and < 10 mm for females. The patients were scored according to the following lung ultrasound scoring criteria: 0 points: normal pleural sliding and PSD≥ normal low; 1 point: PSD < normal low and no pleural sliding sign in either lung area; 2 points: PSD < normal low value and disappearance of the pleural sliding sign in 1–4 lung areas; 3 points: PSD < normal low value and disappearance of the pleural sliding sign in 5–8 lung areas; 4 points: PSD < normal low value and disappearance of the pleural sliding sign in 9–12 lung areas; and 5 points: PSD < normal low value and disappearance of the pleural sliding sign in more than 12 lung regions.
 |
Figure 1 Zones of lung ultrasound score measurement. A 72 intercostal spaces scan of bilateral anterior, lateral, and posterior chest wall, in which we divided the entire chest into 16 zones as shown. |
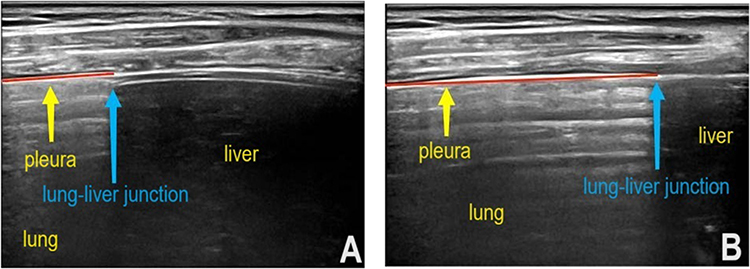 |
Figure 2 Pleural sliding displacement (PSD) measurement method. (A) The distance between the lung–liver junction and the left edge of the acoustic window of the ultrasound instrument was measured along the pleural line at the end of expiration. (B) The distance between the lung–liver junction and the left edge of the acoustic window of the ultrasound instrument was measured along the pleural line at the end of inspiration. The difference between the two values is the PSD. |
Diaphragm excursion scan: A 5-MHz convex array probe was placed between the mid-clavicular line under the right costal margin of the subject in the supine position. The probe direction was oblique to the head side during scanning. Due to the different movements of the diaphragm, it was necessary to adjust the direction of the probe in real time during the examination. The diaphragm excursion was measured at this position. The diaphragm excursion was measured as the vertical distance between the trough and the peak of the wave. The measurement was performed during the two phases of tidal inspiration and maximal deep inspiration of the subject, and the average value was taken from 3 scans, as shown in Figure 3.
 |
Figure 3 Measurement of diaphragmatic excursion. (A) The diaphragm excursion in one respiratory cycle of tidal inspiration is the vertical distance h. (B) The diaphragm excursion in one respiratory cycle of maximal deep inspiration is the vertical distance H. |
According to the standards of the European Respiratory Society, the values of pulmonary function parameters such as TLC, RV, IC, RV/TLC, IC/TLC, functional residual capacity (FRC), FEV1/FVC, and FEV1 predicted value were recorded.23
Statistical Analysis
SPSS (version 19.0; SPSS) was used for all of the analyses. Normally distributed measurement data are expressed as the mean±SD. The inspection level α was 0.05. Nonnormally distributed data are presented as the median [IQR] or n (%), as appropriate. Measurement data that were normally distributed were compared between groups by the two-independent-sample t test. The Mann‒Whitney U-test was used for comparisons between groups that did not conform to the normal distribution. For count data, the chi-square test was used for comparison between groups. Pearson’s correlation coefficient was calculated between ultrasound results and pulmonary function measurement data that were normally distributed. Spearman correlation coefficient was calculated between ultrasound and pulmonary function measurement data that were nonnormally distributed. The correlations were compared by the Z test. Multiple linear regression analysis was used to analyze the factors affecting LH. Taking RV/TLC > 60% and IC/TLC < 25% as the criteria for the diagnosis of severe LH, receiver operating characteristic (ROC) curves of lung ultrasound score (LUS) and DE at maximal deep inspiration for the diagnosis of severe LH were constructed, and the corresponding sensitivity and specificity were calculated. The area under the curve (AUC) in each case was calculated, and the DeLong method was used to compare them. P < 0.05 was considered statistically significant.
Results
Basic Clinical Measurement and Lung Function
Table 1 compares clinical baseline measures and lung function measures between patients with stable COPD and controls. The two groups were similar in terms of sex, age and body mass index. Compared with the control group, the FEV1% predicted value, FEV1/FVC, IC and IC/TLC of the COPD group were lower, and the number of smoking years, TLC, RV, RV/TLC, FRC, CAT score and mMRC score were higher.
 |
Table 1 Clinical Characteristics of Participants |
Changes in Ultrasound Parameters in Patients with Stable COPD
The ultrasound parameters between the control group and stable COPD patients were compared. There was no significant difference in DE at tidal inspiration between the COPD stable group and the control group. Compared with the control group, PSD and DE at maximal deep inspiration were decreased and LUS were increased in stable COPD patients. (Table 2).
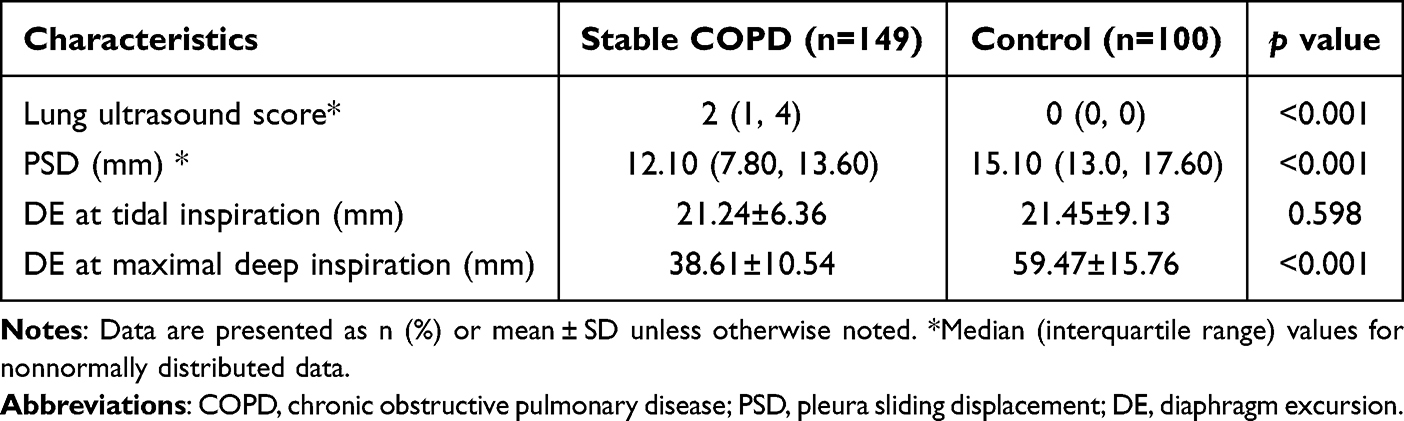 |
Table 2 Ultrasound Characteristics of Participants |
Correlation Analysis of the Ultrasound Parameters and Pulmonary Function Indices Reflecting LH
The LUS of patients was negatively correlated with IC/TLC and IC and was positively correlated with RV/TLC, RV, TLC and FRC. The correlations were stronger than those of DE at maximal deep inspiration. PSD was positively correlated with IC/TLC and IC and negatively correlated with RV/TLC, RV, TLC and FRC. There was no significant correlation between DE at tidal inspiration and any pulmonary function index (Table 3).
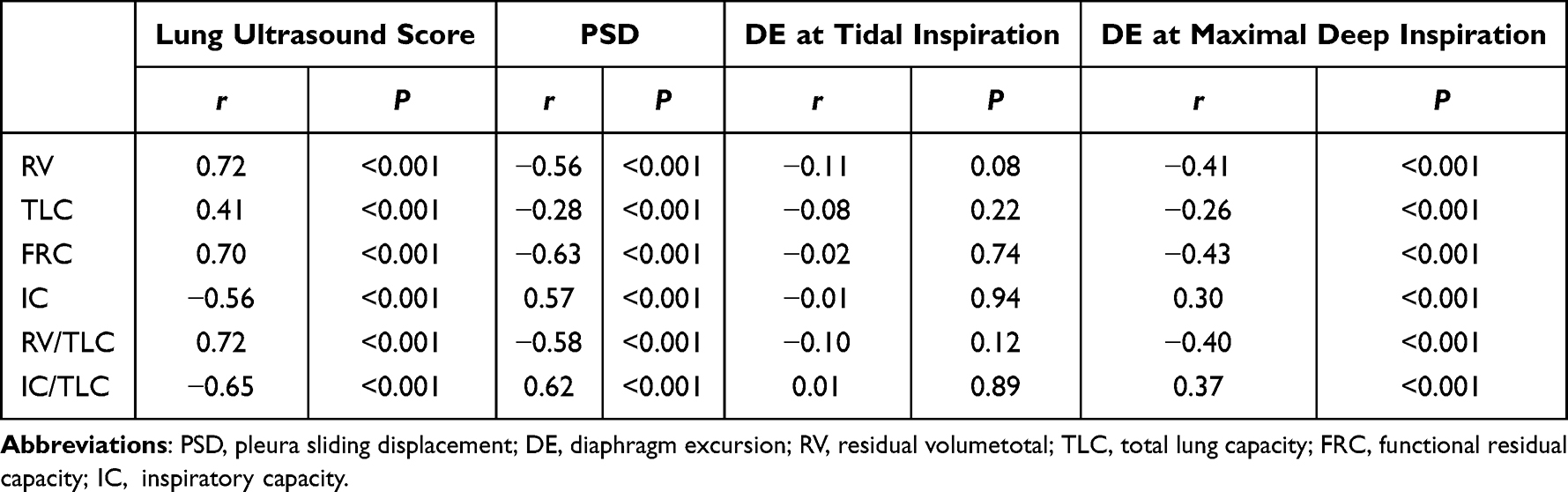 |
Table 3 Correlation Between the Ultrasound Parameters and Pulmonary Function Indexes Reflecting LH |
Correlation Analysis of the Ultrasound Parameters and COPD Score
The LUS of patients was positively correlated with mMRC score and CAT score. PSD and DE at maximal deep inspiration were negatively correlated with mMRC score and CAT score. There was no significant correlation between DE at tidal inspiration mMRC score and CAT score (Table 4).
 |
Table 4 Correlation Between the Ultrasound Parameters and COPD Score |
Multiple Linear Regression Analysis
With IC/TLC as the dependent variable, 9 factors were selected as independent variables for linear regression, including LUS, PSD, FEV1% predicted value, FEV1/FVC, age, smoking years, mMRC score, CAT score, and DE at maximal deep inspiration, according to the clinical significance and the results of single-factor analysis. RV, TLC, FRC, IC, and RV/TLC were excluded because the condition index was > 30, the variation composition was > 0.5, and there was multicollinearity between the corresponding variables. Multiple linear regression analysis (stepwise method) was performed. The results showed that the LUS, PSD and FEV1/FVC were significantly correlated with IC/TLC (Table 5). The regression model was significant and could explain 59.9% of the total variation (R2 = 0.599, F = 121.891, P < 0.001). In another multiple linear regression with RV/TLC as the dependent variable, LUS, PSD, FEV1% predicted value, FEV1/FVC, age, smoking years, mMRC score, CAT score, and DE at maximal deep inspiration were tested as independent variables, given their clinical significance and the results of the single-factor analysis. RV, TLC, FRC, IC, and RV/TLC were excluded because they each had a condition index > 30, the variation composition was > 0.5, and there was multicollinearity between the corresponding variables. This multiple linear regression analysis (stepwise method) showed that LUS, mMRC score and CAT score were significantly correlated with RV/TLC. (Table 6). The regression model was significant and could explain 59.9% of the total variation (R2 = 0.610, F = 127.599, P < 0.001).
 |
Table 5 Multiple Linear Regression Analysis of Influencing Factors of LH Index IC/TLC |
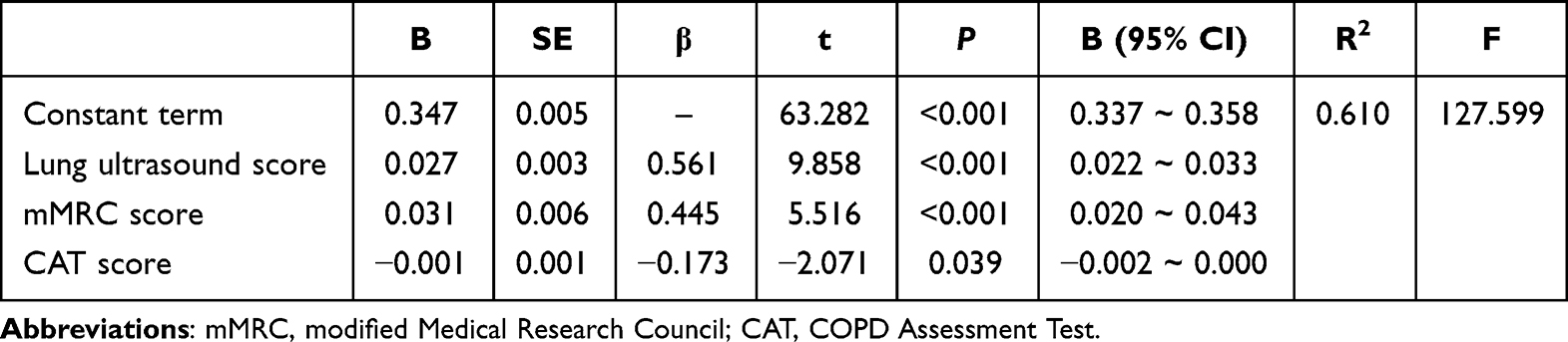 |
Table 6 Multiple Linear Regression Analysis of Influencing Factors of LH Index RV/TLC |
Comparison of the Efficacy of Lung Ultrasound Score and DE at Maximal Deep Inspiration in the Assessment of Severe LH
With IC/TLC < 25% as the diagnostic criterion of serious LH, the AUC for the diagnosis of severe LH by the LUS was greater than that by DE at maximal deep inspiration (P <0.001). With RV/TLC > 60% as the diagnostic criterion of severe LH, the AUC for the diagnosis of severe LH by the LUS was again greater than that by DE at maximal deep inspiration (P <0.001) (Figure 4 and Table 7).
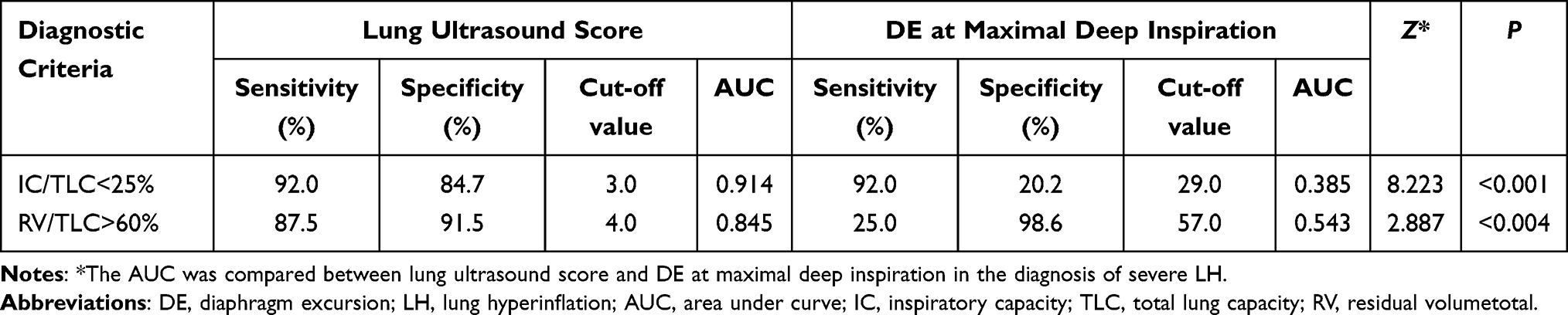 |
Table 7 Efficacy of Lung Ultrasound Score and DE at Maximal Deep Inspiration in the Diagnosis of Severe LH |
 |
Figure 4 ROC curve of lung ultrasound score and DE at maximal deep inspiration for diagnosis of severe LH. (A) With IC/TLC < 25% as serious LH diagnostic criteria, the ROC curve of severe LH was diagnosed by lung ultrasound score and DE at maximal deep inspiration. (B) With RV/TLC > 60% as serious LH diagnostic criteria, the ROC curve of severe LH was diagnosed by lung ultrasound score and DE at maximal deep inspiration. |
Discussion
In COPD patients, chronic inflammation involves the atmospheric tract and small airways (especially small airways), resulting in obstruction and stenosis of small airways, coupled with alveolar damage caused by inflammation, which easily leads to lung overinflation.24,25 Lung hyperinflation in COPD patients is closely related to the evaluation of their prognosis, dyspnea and exercise ability,26 so whether there is a more convenient way to evaluate lung hyperinflation in COPD patients is of great clinical significance.
In recent years, several studies have proposed the use of IC/TLC, RV/TLC and IC as indicators to evaluate lung hyperinflation.27 The worth of IC/TLC in evaluating LH in COPD patients is well recognized, as it reflects end-expiratory lung volume.28,29 With the progression of COPD, IC and the IC/TLC ratio gradually decrease, reflecting the aggravation of lung hyperinflation.8,30 IC/TLC corrects for the value of TLC to eliminate errors caused by different TLC values. It not only reflects the level of functional residual capacity - static lung hyperinflation - but also reflects the inspiratory reserve of patients with COPD.11,31 RV/TLC > 60% and IC/TLC < 25% are considered criteria for severe LH and can be used to determine the surgical indications for lung volume reduction surgery.9–11 Therefore, ICV/TLC and RV/TLC were selected as diagnostic criteria for LH in our study.
However, the above pulmonary function examination operation is complicated, time-consuming and laborious and requires the patient’s cooperation.18 Ultrasound examination, with its advantages of simple operation, safety, practicality, bedside operation and real-time observation, has unique advantages as a supplementary examination method in the assessment of lung hyperinflation. So far, ultrasound evaluation of lung hyperinflation has been limited to DE and related variables.21
Lung hyperinflation shortens the diaphragm muscle, which is the main power source of the respiratory pump, and its shape changes from arched to flat, which weakens its contraction ability, seriously affects the effective respiratory movement,20 and reduces the tidal volume and other indicators. Therefore, the diaphragm movement index DE is negatively correlated with lung hyperinflation, so it well reflects the development of COPD,21 especially the development of shortness of breath. However, ultrasound detection of DE still requires patients to take deep breaths, which may make it less useful in patients with more serious conditions. Therefore, our team has explored lung ultrasound evaluation methods that are easier to operate and not affected by patients’ breathing ability.
During respiratory movements, the visceral pleura moves with the expansion and retraction of the lung, while the parietal pleura moves with the expansion and retraction of the thoracic cavity, and the magnitude of visceral pleura sliding is generally larger than that of parietal pleura, resulting in the pleural sliding sign visible to the naked eye during ultrasound examination.32 LH causes excessive expansion and weak retraction of the lung, and the movement of visceral pleura weakened. While the movement of parietal pleura, which is more affected by the expansion and retraction of thoracic cavity, is weakened relatively insignificantly, resulting in the weakening of the relative movement of the visceral pleura and parietal pleura, which means the weakening of pleural slip. When COPD patients are not complicated with infection, the A-line dominates both lungs, and the pleural slip sign weakens or even disappears to varying degrees.32 Patients with severe bronchial asthma who have characteristics similar to COPD, such as lung hyperinflation, may have a reduced or absent pleural slip.33,34 Therefore, the weakening or even disappearance of pleural slip may have some connection with LH, which is worth further exploration.
In the judgment of a mildly weakened pleural slip, there may be some error based only on the subjective judgment of the examining physician of the pleural slip sign.35 Zhao22 found that TLC and RV increased in COPD patients, tidal volume decreased significantly and PSD decreased during inspirations. Although PSD is not equivalent to the traditional pleural slip sign, PSD can clearly reflect the situation of pleural slipping,22 and PSD can help judge the weakening of pleural slip. Referring to the results of relevant studies22 and the results of the control group in this study, the normal critical value of PSD was < 12 mm for males and < 10 mm for females.
Related studies36 also found that the disappearance of pleural sliding was related to subpleural pulmonary bullae, which was confirmed by CT results. With the progression of lung hyperinflation, the incidence of pulmonary bullae in patients with COPD increases. Its essence is that the pressure in the alveolar cavity is increased for a variety of reasons, and no gas moves in or out with respiratory movement. The pulmonary bullae that can be observed by ultrasound are located under the pleura, and the typical ultrasound indication is the disappearance of the A-line with the sliding of the pleura, while the distribution range of the focal A-line does not change with respiration.37 However, the wide distribution of the A-line in the lungs of COPD patients makes it difficult to distinguish their subpleural pulmonary bullae, so we often only observe the disappearance of the focal pleural sliding sign. Pulmonary bullae may increase end-expiratory lung volume in COPD patients,38 which is closely related to RV/TLC.39 Therefore, the disappearance of pleural sliding caused by pulmonary bullae is also related to pulmonary function indicators reflecting LH and may have certain value in the evaluation of LH.
Therefore, in our study, a PSD less than the normal critical value combined with the disappearance of pleural sliding in each lung area caused by lung hyperinflation and subpleural bullae was used to calculate a comprehensive LUS. This study showed that in patients with COPD, PSD decreased, and pleural sliding often weakened or disappeared. The LUS based on pleural sliding and PSD increased with increasing RV/TLC, an indicator of lung hyperinflation, and increased with decreasing IC/TLC, an indicator of lung hyperinflation. It is also closely related to lung volume indicators. This further suggests that the LUS may be an effective ultrasound evaluation system for the evaluation of lung hyperinflation.
Our results show that the LUS based on pleural slip and PSD had a stronger correlation with pulmonary function indicators reflecting lung hyperinflation than did diaphragm excursion in patients with COPD. LH causes excessive expansion of the lung, and weak retraction directly causes the weakening of pleural friction. By reducing the ability of the diaphragm to form flow and pressure, LH indirectly leads to decreased mobility of the diaphragm. In addition, the diaphragm has a strong compensatory function, and the compensatory phenomenon can partially offset the adverse effects of LH on the contractility and inspiratory effect of the diaphragm in COPD patients.40 Therefore, the LUS can reflect LH more directly, so its correlation with LH is stronger than that with DE.
Our study also found that lung ultrasound scores were significantly correlated with RV/TLC and IC/TLC through multiple linear regression analysis. At the same time, the diagnostic efficacy of severe LH based on the pulmonary function index (RV/TLC > 60% and IC/TLC < 25%) was better than that of DE at maximal deep inspiration, and the area under the ROC curve was significantly greater than that of DE at maximal deep inspiration deep breathing (P < 0.05). We speculated that the reason why LUS had better diagnostic efficacy than DE at maximal deep inspiration may be that the assessment of the former was more comprehensive. This involved an assessment of pleural sliding in 16 lung zones and the PSD, which could be used for a more comprehensive assessment of excessive expansion and weak retraction of the lung caused by LH. However, the assessment of DE at maximal deep inspiration was limited because it involved only the diaphragm. For patients with severe COPD, pulmonary function examination is often unable to be performed in clinical practice due to the patient’s inability to cooperate. The lung ultrasound scoring system constructed in this study is expected to become a new auxiliary examination means, providing an effective reference for clinical follow-up observation of the basic situation of lung hyperinflation in COPD patients and helping to guide treatment. Combining our results with previous ones, we speculate that lung ultrasound scoring may be a better imaging method to supplement and assist with pulmonary function examination, especially in the evaluation and follow-up of patients with severe COPD.
The results of our study showed that LUS was positively correlated with RV, TLC, and RV/TLC and negatively correlated with FRC and IC, which suggested that lung ultrasound may be used to monitor the deterioration of lung function in COPD patients. Longitudinal studies can be conducted in the future to explore the monitoring effect. In addition, our study focused mainly on patients with stable COPD, and LUS can also be used in the future to monitor the process of acute exacerbation in COPD patients and thereby explore the role of LUS in acute exacerbation of COPD.
Related studies22 have shown that factors such as chronic obstructive pulmonary disease (COPD) and pneumonia easily lead to pleural thickening and a decrease in PSD compared with those in healthy controls. Therefore, to exclude the interference of non-COPD factors (such as pneumonia, pleurisy, pleural effusion, and other diseases causing abnormal pleural thickening) in our study, patients with a history of chronic respiratory diseases other than COPD, a history of pleural disease, or a history of respiratory infection in the month before the study were excluded at the time of enrolment. However, the above non-COPD factors may play a certain role in the sensitivity and specificity of detection, especially in patients with acute exacerbation of COPD, which is often complicated with pneumonia, pleural effusion, pleural changes, etc. Therefore, future studies need to pay attention to the influence of these factors.
Our study revealed that LUS was correlated with commonly used scores that reflect the pathophysiology of COPD (mMRC score, CAT score), which suggests that LUS can be used as a new tool in daily medical practice to assist medical staff (doctors, nurses, etc.) in assessing patients’ dyspnoea and comprehensive symptoms. Compared with relevant questionnaires,41 lung ultrasound can reduce the subjective influence of patients and evaluate the condition of COPD patients more objectively, which has certain advantages. In the future, medical staff will be able to evaluate the effect of pulmonary rehabilitation in COPD patients under the guidance of lung ultrasound, which is helpful for improving the relevant nursing work, accelerating the rehabilitation process and improving the prognosis.
There are some limitations to our study. First, this is a single-center study that lacks longitudinal comparison. Second, ultrasound examination is limited to respiratory muscle, pleura, and subpleural lung parenchyma and cannot involve deep lung tissue. CT examination has advantages in this field, and the combination of these two examinations might be better for the evaluation of COPD.
In summary, the LUS constructed from pleural slip in different regions and PSD can be used to evaluate LH in stable COPD patients. We expect this score to be an effective auxiliary tool for evaluating LH in COPD patients.
Conclusion
This clinical study showed that the LUS, based on pleural slip in different regions and PSD, was increased in stable COPD patients, which was correlated with pulmonary function indicators reflecting LH. Its correlations were stronger than those of DE at maximal deep inspiration. The diagnostic efficacy of pulmonary ultrasound scoring in the diagnosis of severe LH is better than that of DE at maximal deep inspiration, so it can be used to evaluate LH in stable COPD patients.
Abbreviations
COPD, chronic obstructive pulmonary disease; LH, lung hyperinflation; FRC, functional residual capacity; IC, inspiratory capacity; sLH, static lung hyperinflation; dLH, dynamic lung hyperinflation; TLC, total lung capacity; RV, residual volumetotal; AreaFE, area under the forced expiratory flow-volume loop; AreaFE%, AreaFE expressed as a percentage of reference value; MPT, manually/metronome paced tachypnea; MPIH, metronome-paced incremental hyperventilation; IOS, impulse oscillometry system; DE, diaphragm excursion; FEV1, forced expiratory volume; FVC, forced vital capacity; mMRC, modified Medical Research Council; CAT, COPD Assessment Test; PSD, pleura sliding displacement; ROC, receiver operator characteristic; LUS, lung ultrasound score; AUC, area under curve.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Fujian Medical University (reference number: 2019-223). This study was conducted in accordance with the Declaration of Helsinki and all participants gave informed consent.
Acknowledgments
We are grateful for the support of the Department of Respiratory Medicine of the Second Affiliated Hospital of Fujian Medical University.
Funding
This project was financially supported by Natural Science Foundation of Fujian Province, China (NO:2022J01783).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Cross SH, Ely EW, Kavalieratos D., et al. Place of Death for Individuals With Chronic Lung Disease: trends and Associated Factors From 2003 to 2017 in the United States. Chest. 2020;15:25–31.
2. Marçôa R, Rodrigues DM, Dias M, et al. Classification of Chronic Obstructive Pulmonary Disease (COPD) according to the new Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017: comparison with GOLD 2011. COPD. 2018;15(1):21–26. doi:10.1080/15412555.2017.1394285
3. Gagnon P, Guenette JA, Langer D, et al. Pathogenesis of hyperinflation in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9(1):187–201. doi:10.2147/COPD.S38934
4. O’Donnell DE, Elbehairy AF, Webb KA, et al. The link between reduced inspiratory capacity and exercise intolerance in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2017;14(Supplement_1):S30–S39. doi:10.1513/AnnalsATS.201610-834FR
5. Rossi A, Aisanov Z, Avdeev S, et al. Mechanisms, assessment and therapeutic implications of lung hyperinflation in COPD. Respir Med. 2015;109(7):785–802. doi:10.1016/j.rmed.2015.03.010
6. O’Donnell DE, Laveneziana P. Physiology and consequences of lung hyperinflation in COPD. Eur Respir Rev. 2006;15(100):61–67. doi:10.1183/09059180.00010002
7. Casanova C, Cote C, de Torres JP, et al. Inspiratory-to-total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(6):591–597. doi:10.1164/rccm.200407-867OC
8. Park J, Lee CH, Lee YJ, et al. Longitudinal changes in lung hyperinflation in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:501–508. doi:10.2147/COPD.S122909
9. Fishman A, Martinez F, Naunheim K, et al. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003;348(21):2059–2073.
10. Caviezel C. Lung volume reduction surgery in selected patients with severe emphysema: significant benefit with low peri-operative risk. J Xiangya Med. 2017;2(6):48. doi:10.21037/jxym.2017.05.04
11. Casanova C, Cote C, de Torres JP, et al. Inspiratory-to-total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(6):591–597.
12. Lee J, Lee CT, Lee JH, et al. Graphic analysis of flow-volume curves: a pilot study. BMC Pulm Med. 2016;16(1):115. doi:10.1186/s12890-016-0277-2
13. Das N, Topalovic M, Aerts JM, et al. Area under the forced expiratory flow-volume loop in spirometry indicates severe hyperinflation in COPD patients. Int J Chron Obstruct Pulmon Dis. 2019;14:409–418. doi:10.2147/COPD.S185931
14. Mannée D, Vis E, Hoekstra-Kuik A, et al. Is the metronome-paced tachypnea test (MPT) ready for clinical use? Accuracy of the MPT in a prospective and clinical study. Respiration. 2019;97(6):569–575. doi:10.1159/000496290
15. Kawachi S, Fujimoto K. Metronome-paced incremental hyperventilation may predict exercise tolerance and dyspnea as a surrogate for dynamic lung hyperinflation during exercise. Int J Chron Obstruct Pulmon Dis. 2020;15:1061–1069. doi:10.2147/COPD.S246850
16. Milne S, Hammans C, Watson S, et al. Bronchodilator responses in respiratory impedance, hyperinflation and gas trapping in COPD. COPD. 2018;15(4):341–349. doi:10.1080/15412555.2018.1458217
17. D’Ascanio M, Viccaro F, Calabrò N, et al. Assessing static lung hyperinflation by whole-body plethysmography, helium dilution, and impulse oscillometry system (ios) in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:2583–2589. doi:10.2147/COPD.S264261
18. Jat KR, Agarwal S. Lung Function Tests in Infants and Children. Indian J Pediatr. 2023;90(8):790–797. doi:10.1007/s12098-023-04588-8
19. Jia YH, Zhang QX. Research Progress on Diaphragm Ultrasound in Chronic Obstructive Pulmonary Disease: a Narrative Review. Ultrasound Med Biol. 2022;48(4):587–597. doi:10.1016/j.ultrasmedbio.2021.10.019
20. Polkey MI, Kyroussis D, Hamnegard CH, et al. Diaphragm strength in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1996;154:1310–1317. doi:10.1164/ajrccm.154.5.8912741
21. Shiraishi M, Higashimoto Y, Sugiya R, et al. Diaphragmatic excursion is correlated with the improvement in exercise tolerance after pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Respir Res. 2021;22(1):271. doi:10.1186/s12931-021-01870-1
22. Zhao HT, Liu YL, Liu Y, et al. Study on Characteristics of Different Lung Diseases by Lung Ultrasound. Chinese J Ultrasound Med. 2023;39(1):12–16.
23. Global strategy for the diagnosis, management, and prevention of COPD; 2020. Available from: http://www.goldcopd.org.
24. Dos RIMM, Ohara DG, Januário LB, et al. Surface electromyography in inspiratory muscles in adults and elderly individuals: a systematic review. J Electromyogr Kinesiol. 2019;44:139–155. doi:10.1016/j.jelekin.2019.01.002
25. Turato G, Zuin R, Miniati M, et al. Airway inflammation in severe chronic obstructive pulmonary disease: relationship with lung function and radiologic emphysema. Am J Respir Crit Care Med. 2002;166(1):105–110. doi:10.1164/rccm.2111084
26. Gibson GJ. Pulmonary hyperinflation a clinical overview. Eur Respir J. 1996;9(12):2640–2649. doi:10.1183/09031936.96.09122640
27. Singh S, Maltais F, Tombs L, et al. Relationship between exercise endurance and static hyperinflation in a post hoc analysis of two clinical trials in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:203–215. doi:10.2147/COPD.S145285
28. Tantucci C, Donati P, Nicosia F, et al. Inspiratory capacity predicts mortality in patients with chronic obstructive pulmonary disease. Respir Med. 2008;102(4):613–619. doi:10.1016/j.rmed.2007.11.004
29. Celli BR, Decramer M, Lystig T, et al. Longitudinal inspiratory capacity changes in chronic obstructive pulmonary disease. Respir Res. 2012;13(1):66. doi:10.1186/1465-9921-13-66
30. O’Donnell DE, Guenette JA, Maltais F, et al. Decline of resting inspiratory capacity in COPD: the impact on breathing pattern, dyspnea, and ventilatory capacity during exercise. Chest. 2012;141(3):753–762. doi:10.1378/chest.11-0787
31. Albuquerque ALP, Nery LE, Villaça DS, et al. Inspiratory fraction and exercise impairment in COPD patients GOLD stages II-III. Eur Respir J. 2006;28(5):939–944. doi:10.1183/09031936.06.00040506
32. Lichtenstein DA, Mezière GA. Relevance of Lung Ultrasound in the Diagnosis of Acute Respiratory Failure*: the BLUE Protocol. Chest. 2008;134(1):117–125. doi:10.1378/chest.07-2800
33. Scioscia G, Lacedonia D, Quarato CMI, et al. Could transthoracic ultrasound be useful to suggest a small airways disease in severe uncontrolled asthma? Ann Allergy Asthma Immunol. 2022;129(4):461–466. doi:10.1016/j.anai.2022.05.024
34. Lichtenstein D, Rialp G. Lung ultrasound in a dyspneic patient with giant bullae. Intensive Care Med. 2019;45:690–691. doi:10.1007/s00134-018-5317-3
35. Zhang Y, Lian XH, Huang SF, et al. A study of the diagnostic value of a modified transthoracic lung ultrasound scoring method in interstitial lung disease. Quant Imaging Med Surg. 2023;13(2):946–956. doi:10.21037/qims-22-153
36. Aziz SG, Patel BB, Ie SR, et al. The Lung Point Sign, not Pathognomonic of a Pneumothorax. Ultrasound Q. 2016;32:277–279. doi:10.1097/RUQ.0000000000000199
37. Zhao HT, Liu Y, Xue HY. Pulmonary ultrasound findings of a case of Sjogren’s syndrome associated interstitial lung disease with pulmonary bullae. Chinese J Ultrasound Med. 2022;38(2):241. doi:10.1142/S0192415X10007816
38. Travaline JM, Addonizio VP, Criner GJ. Effect of bullectomy on diaphragm strength. Am J Respir Crit Care Med. 1995;152:1697–1701. doi:10.1164/ajrccm.152.5.7582315
39. Kilburn KH, Warshaw RH, Thornton JC. Do radiographic criteria for emphysema predict physiologic impairment? Chest. 1995;107(5):1225–1231. doi:10.1378/chest.107.5.1225
40. Similowski T, Yan S, Gauthier AP, et al. Contractile properties of the human diaphragm during chronic hyperinflation. N Engl J Med. 1991;325(13):917–923. doi:10.1056/NEJM199109263251304
41. Yamaji Y, Hirano T, Ogawa H, et al. Utility of the Shortness of Breath in Daily Activities Questionnaire (SOBDA-Q) to Detect Sedentary Behavior in Patients with Chronic Obstructive Pulmonary Disease (COPD). J Clin Med. 2023;12(12):4105. doi:10.3390/jcm12124105
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.