Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Serum Derivatives of Reactive Oxygen Metabolites are Associated with Severity of Chronic Obstructive Pulmonary Disease and Affected by a p53 Gene Polymorphism
Authors Yamamura K, Nojiri M, Nishiki K, Kato R, Shinomiya S, Takahara Y, Oikawa T, Ishizaki T, Toga H, Mizuno S
Received 17 March 2022
Accepted for publication 4 July 2022
Published 13 July 2022 Volume 2022:17 Pages 1589—1600
DOI https://doi.org/10.2147/COPD.S366792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Koichi Yamamura,* Masafumi Nojiri,* Kazuaki Nishiki, Ryo Kato, Shohei Shinomiya, Yutaka Takahara, Taku Oikawa, Takeshi Ishizaki, Hirohisa Toga, Shiro Mizuno
Department of Respiratory Medicine, Kanazawa Medical University, Ishikawa, Japan
*These authors contributed equally to this work
Correspondence: Shiro Mizuno, Department of Respiratory Medicine, Kanazawa Medical University, 1-1 Daigaku, Uchinada, Kahoku-gun, Ishikawa, 920-0293, Japan, Tel +81-76-218-8157, Fax +81-76-286-0980, Email [email protected]
Purpose: Oxidative stress is known to activate tumor suppressor p53, which inhibits cell cycle progression and induces apoptosis. Levels of p53 in lung tissues from patients with chronic obstructive pulmonary disease (COPD) are increased compared with levels in nonsmokers or smokers without emphysema. A polymorphism in p53 codon 72 (rs1042522) is associated with emphysematous changes in patients with COPD. However, whether oxidative stress in the serum is associated with the p53 polymorphism and disease severity in COPD patients is unclear.
Patients and Methods: A total of 251 patients with a history of smoking more than 10 pack-years were enrolled in this study, and serum levels of derivatives of reactive oxygen metabolites (d-ROMs), biological antioxidant potential (BAP), and d-ROMs/BAP ratio (oxidative stress index; OSI) were measured. The percent low-attenuation area (LAA%) and cross-sectional area of the erector spinae muscles (ESMCSA) at the Th12 level were calculated from chest high-resolution computed tomography images. p53 codon 72 C/G genotyping was performed using polymerase chain reaction–restriction fragment length polymorphism analysis.
Results: In patients carrying the p53 GG genotype, LAA% was significantly higher than in those carrying the CC genotype. d-ROM levels and OSI were associated with COPD severity and correlated with airflow limitation and markers of muscle atrophy (ESMCSA and creatinine/cystatin C ratio). Associations between markers of oxidative stress and COPD severity were observed primarily in patients carrying the p53 codon 72 GG genotype.
Conclusion: Susceptibility to pulmonary emphysema and responses to oxidative stress may be affected by the p53 gene polymorphism.
Keywords: oxidative stress, low attenuation area, sarcopenia, smoking status
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory disease caused primarily by inhalation of cigarette smoke. In patients with COPD, long-term cigarette smoking generates large amounts of free radicals.1 Even after cessation of smoking, oxidative stress derived from activated macrophages and neutrophils persists in the lungs.2,3 Oxidative stress is known to activate tumor suppressor p53, which inhibits cell cycle progression and induces apoptosis of cells with irreparable genetic damage,4 and the levels of p53 in lung tissues of patients with COPD are increased compared with those of nonsmokers or smokers without emphysema.5–7 A previous study showed that polymorphisms in p53 are associated with the occurrence of smoking-related COPD in Taiwan Chinese patients.8 Similarly, we previously reported that a polymorphism in p53 codon 72 (rs1042522) was associated with emphysematous changes in patients with COPD.9 The p53 gene polymorphism in codon 72 is the most frequently studied single-nucleotide polymorphism in the p53 pathway and plays an important role in inducing apoptosis and stress-induced senescence pathways10–12 involved in the pathophysiologic changes associated with pulmonary emphysema and COPD.13
Oxidative stress can be assessed by measuring a variety of factors, such as serum thiobarbituric acid–reactive substances, serum oxidized low-density lipoprotein, and urinary oxidized nucleosides of DNA.14–16 In contrast, measurements of intracellular levels of superoxide dismutase and glutathione peroxidase have been studied as indicators of antioxidant potential.17,18 However, these assay methods are too complex for the analysis of large numbers of samples. An increasing number of studies have examined assay methods to measure levels of derivatives of reactive oxygen metabolites (d-ROMs) and biological antioxidant potential (BAP) as a simpler means of detecting reactive oxygen species (ROS).18–22 The d-ROMs test does not directly measure active oxygen and free radicals but rather peroxides such as hydroperoxide, which is an oxidative metabolite. The BAP test measures antioxidant power via the reduction of ferric ions to ferrous ions. Both assays use serum samples and can be easily performed simultaneously in a short time.19 Therefore, in the present study, we measured d-ROM levels and BAP in serum samples obtained from COPD patients as biomarkers of oxidative stress.
Measurements of various markers of oxidative stress in blood samples from COPD patients have revealed increased lung oxidative stress,20–24 and it has been postulated that this oxidative stress leads to enhanced expression of p53 in the lungs of COPD patients.5,24,25 However, whether the levels of oxidative stress markers in serum are associated with the p53 polymorphism and disease severity in COPD patients is unclear. In the present study, we characterized the p53 codon 72 polymorphism and measured d-ROM levels and BAP in serum from smokers and COPD patients in order to determine whether the p53 polymorphism affects the oxidative stress response and clinical parameters of COPD such as pulmonary function and disease severity.
Patients and Methods
Patients
From December 2015 to November 2017, a total of 264 patients were recruited from the outpatient department of the Department of Respiratory Medicine, Kanazawa Medical University Hospital. The inclusion criteria for enrollment were as follows: age >40 years; at least a 10 pack-year history of tobacco smoking; and meeting the Global Initiative for Obstructive Lung Disease (GOLD) stage criteria for COPD based on post-bronchodilator spirometry. Two patients on hemodialysis for chronic renal failure were excluded. Sixteen patients were also excluded due to increased high-sensitivity C-reactive protein (HsCRP) levels (>1 mg/dL). Consequently, 246 patients participated in the present study. The study was approved by the Research Ethics Committee of Kanazawa Medical University (protocol: no. G102, I100), and all subjects gave written informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Pulmonary Function Tests
Pulmonary function tests were performed to determine forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1). The predicted pulmonary function values were calculated according to Japanese Respiratory Society guidelines. The diagnosis of COPD and classification of airflow limitation severity in COPD were based on clinical history, physical examination, and spirometry data, following the GOLD classification.26 The study included 151 patients with COPD and 95 smokers without COPD. The COPD patients were classified into 3 subcategories (mild, GOLD I; moderate, GOLD II; and severe, GOLD III and IV) based on spirometry data (Table 1).
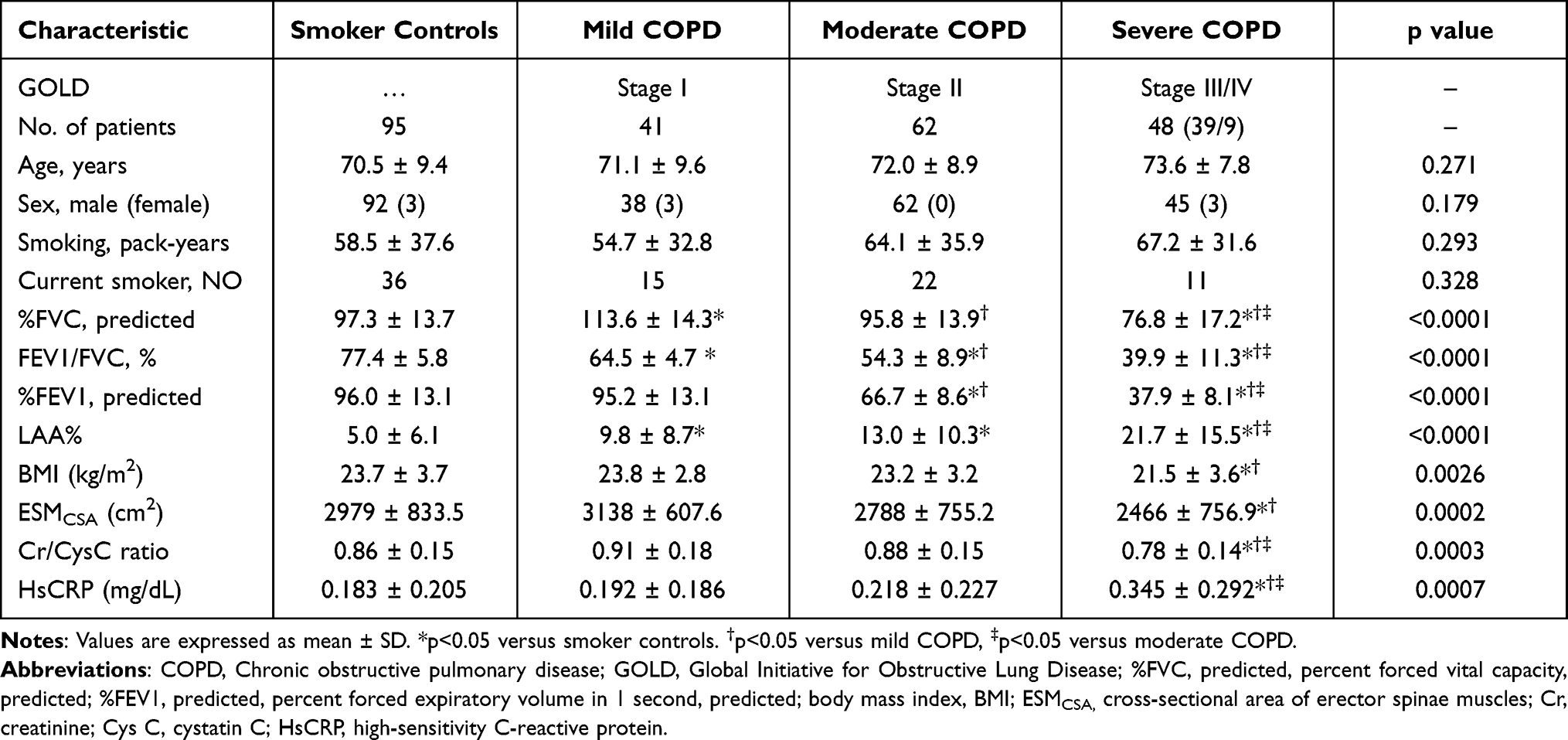 |
Table 1 Patient Characteristics |
Measurement of Percent Low-Attenuation Area (LAA%)
LAA% was measured as previously reported.25,27,28 Briefly, high-resolution computed tomography (CT) scans were acquired using a 128-multidetector CT scanner (Somatom Definition FLASH; Siemens Medical Solutions, Erlangen, Germany) with a slice thickness of 2 mm. LAA% was calculated using a threshold of −960 Hounsfield units (HU) to assess emphysematous changes and total lung volume using the computer software LungVisionTM, version 2.1 (Cybernet Systems Co., Ltd., Tokyo, Japan).
Quantitative Analysis of Cross-Sectional Area (CSA) of Erector Spinae Muscles (ESMs)
The CSA of ESMs (ESMCSA) was measured based on our previous study.28 Briefly, ESMCSA was measured on a single-slice, axial chest CT image at the level of the lower margin of the 12th thoracic vertebra using ImageJ software (National Institutes of Health, Bethesda, MD, USA). The left and right ESMs were manually selected, the areas of both ESMs were selected, and the CSAs of both ESMs were calculated.
Measurement of Creatinine and Cystatin C (CysC), Hs-CRP, d-ROMs, and BAP Levels
Whole blood was collected from each patient into anticoagulant-treated tubes. The serum was separated from the whole blood by centrifugation for 10 min at 1000 x g using a refrigerated centrifuge. The serum samples were stored in a deep freezer at −80°C until analyzed. Aliquots of serum samples were sent to SRL Inc. (Shinjuku-ku, Tokyo, Japan), a clinical laboratory testing company, for measurement of serum creatinine, CysC, and Hs-CRP levels.
d-ROM levels and BAP were measured using a free radical elective evaluator system (FREE Carpe Duo, Wismerll Co. Ltd., Tokyo, Japan) with a kit for d-ROM and BAP testing (Wismerll Co., Ltd.). Briefly, each serum sample (20 μL) was placed in a cuvette filled with buffer (pH 4.8). The cuvette was then turned upside down and agitated. Fe2+ and Fe3+ served as catalysts, resulting in the degradation of blood hydroperoxide into alkoxy and peroxy radicals. A color-developing chromogen was then added in a volume of 20 μL, resulting in oxidation of the chromogen substrate by the free radicals to yield a red-colored radical cation. The cuvette was once again turned upside down and agitated and then placed in a photometer for optical measurement of d-ROMs. A chromogen for BAP (a reagent containing trivalent iron, 50 μL) was added to the cuvette to induce red coloration. The cuvette was turned upside down, and the color intensity was measured using a photometer. Each serum sample (10 μL) was then placed into a cuvette and agitated. The cuvette was then placed in a thermostatically controlled chamber for 5 min. Finally, the cuvette was placed into the photometer for optical measurement of BAP.
p53 Genotyping
Genomic DNA was extracted from peripheral blood using a PAXgene blood DNA kit (Qiagen, Valencia, CA, USA) and stored in PAX gene collection tubes (Qiagen) at −20°C. Genotyping of p53 codon 72 was performed by polymerase chain reaction (PCR)–restriction fragment length polymorphism. Briefly, PCR was performed with 100 ng of genomic DNA and specific oligonucleotide primers using a Type-it Mutation Detect PCR kit (Qiagen) and GeneAmpTM PCR System thermocycler (Applied Biosystems). The sequence of the forward primer for p53 was 5’-CATGGGACTGACTTTCTGCT-3’, and the sequence of the reverse primer was 5’-GGTGTGATGGGATGGATAAA-3’. The polymorphism in codon 72 of the p53 gene was analyzed by BstUI (New England Biolab; Beverly, MA, USA) digestion of PCR products for 4 h at 60°C. The G allele (but not the C allele) has a single BstUI site within the amplified fragment; the fragments were resolved by electrophoresis on a 1.5% agarose gel with ethidium bromide staining (Figure 1). In order to clarify the effect of the p53 polymorphism on the expression of oxidative stress and systemic inflammation markers, we evaluated d-ROM levels, BAP, and oxidative stress index (OSI) in serum samples from COPD patients categorized by p53 genotype and disease severity.
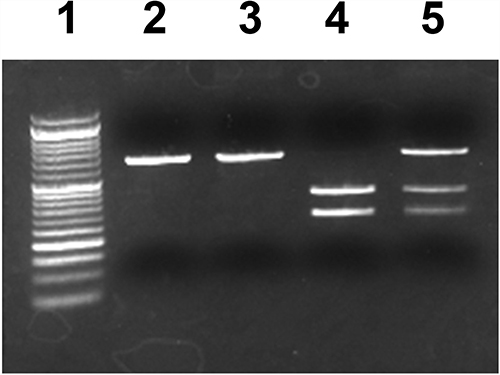 |
Figure 1 Representative photograph of PCR-RFLP analysis of p53 gene codon 72 polymorphisms. PCR-amplified genomic DNA corresponding to the p53 gene was digested with BstUI, which distinguishes among p53 genotypes. Lane 1 shows the DNA ladder marker, lane 2 shows the PCR product without restriction digestion, lane 3 shows the p53 codon 72 CC genotype, lane 4 shows the GG genotype, and lane 5 shows the CG genotype. |
Statistical Analysis
Age, smoking index (expressed as pack-years), pulmonary function parameters, ESMCSA, and LAA%, HsCRP, d-ROM levels, and BAP were compared between groups using analysis of variance with Bonferroni correction for multiple comparisons. Comparisons of d-ROMs, BAP, OSI and HsCRP values between current smoker and ex-smoker were performed using the Student’s t-test. Correlations were analyzed using Pearson’s correlation coefficient. The significance of differences in the distributions of sex and smoking status between the groups was determined using the chi-squared test and the chi-squared test for trends. Comparisons were considered significant at p<0.05.
Results
Patient Characteristics
Age, sex, smoking history, pulmonary function data, LAA%, body mass index (BMI), ESMCSA, serum creatinine/cystatin C (Cr/CysC) ratio, and HsCRP levels of COPD patients classified by disease severity are summarized in Table 1. No significant differences between the groups were observed in terms of age, sex, or smoking history. As expected, LAA% was significantly higher in association with impairment of pulmonary function. BMI, ESMCSA, and Cr/CysC ratio, which is an indicator of sarcopenia in COPD patients,28–30 were decreased in patients with severe COPD compared with smoker controls. HsCRP levels were significantly increased in patients with severe COPD compared with smoker controls and patients with moderate and mild COPD (Table 1).
Associations of d-ROMs, BAP, and OSI with Pulmonary Function and Indicators of Sarcopenia
d-ROM levels were significantly increased in patients with severe COPD compared with smoker controls and those with moderate COPD (Figure 2A). No significant differences were observed in terms of BAP between the groups (Figure 2B); however, the d-ROMs/BAP ratio (OSI) was significantly increased in patients with severe COPD compared with smoker controls and those with moderate COPD (Figure 2C). Because smoking can affect oxidative stress and systemic inflammation, d-ROM levels, BAP, and HsCRP levels were compared between current and ex-smokers among the whole patient population (Figure 3). Although there were no significant differences in d-ROM and HsCRP levels between current and ex-smokers, the BAP was increased and OSI decreased in ex-smokers compared with current smokers.
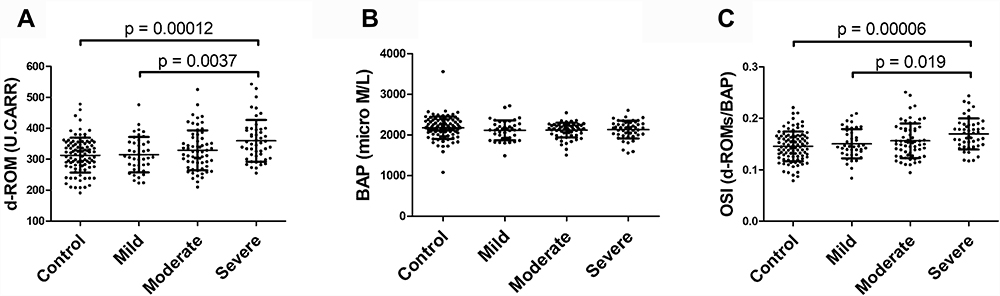 |
Figure 2 Derivatives of reactive oxygen metabolites (d-ROMs) (A), biological antioxidant potential (BAP) (B), and oxidative stress index (OSI) (C) in serum from smoker controls (control) and patients with moderate chronic obstructive pulmonary disease (COPD) (moderate), mild COPD (mild), and severe COPD (severe). d-ROM levels and OSI were significantly higher in patients with severe COPD compared with the control and moderate COPD patient groups. No significant differences were observed in BAP between the groups. Data are expressed as mean ± SD. |
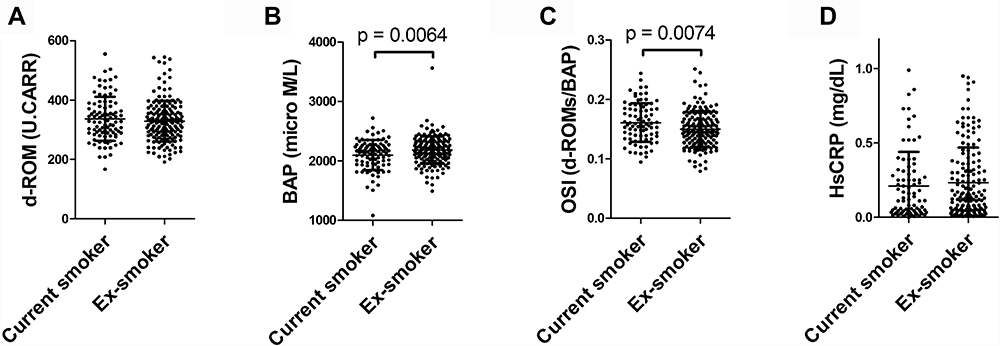 |
Figure 3 D-ROM levels (A), BAP (B), OSI (C), and high-sensitivity C-reactive protein (HsCRP) levels (D) in serum from current and ex-smokers. Data are expressed as mean ± SD. BAP was significantly increased and OSI significantly decreased in ex-smokers compared with current smokers. |
d-ROMs and OSI exhibited a small inverse correlation with the percent forced expiratory volume in 1 second, predicted (%FEV1) but not with the percent predicted forced vital capacity (%FVC) and LAA% (Figure 4A–F). In the context of markers of sarcopenia, d-ROMs exhibited a small inverse correlation with Cr/CysC ratio and ESMCSA, but not with BMI. The OSI exhibited a small inverse correlation with Cr/CysC ratio, but not with BMI and ESMCSA (Figure 5A–F).
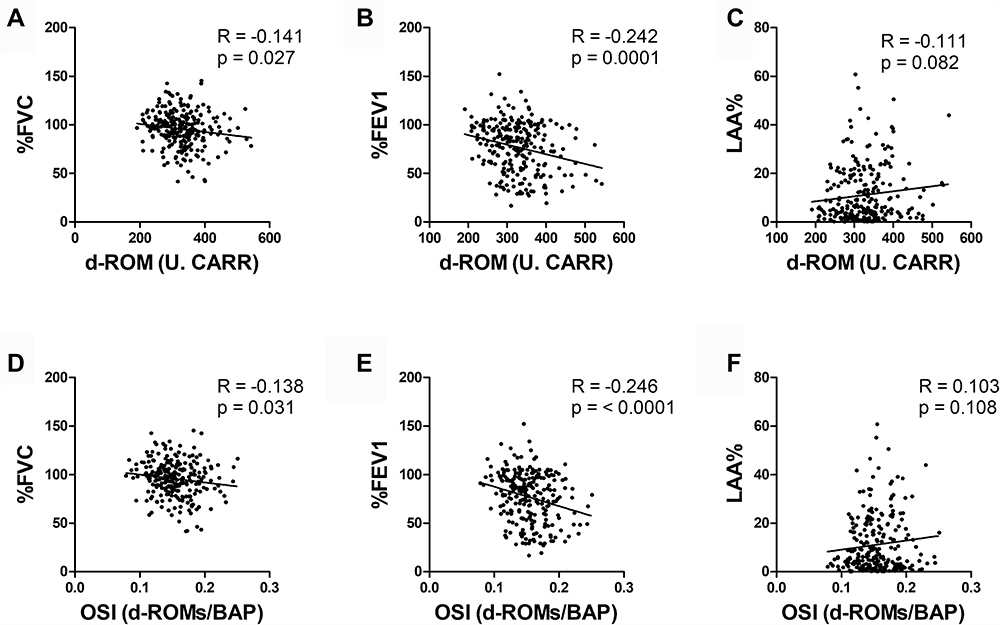 |
Figure 4 Results of correlation analyses between d-ROM levels and percent forced vital capacity, predicted (%FVC) (A), percent forced expiratory volume in 1 second, predicted (%FEV1) (B), percent low-attenuation area (LAA%) (C), and between OSI and %FVC (D), %FEV1 (E), and LAA% (F). d-ROM levels were weakly correlated with %FVC and %FEV1. |
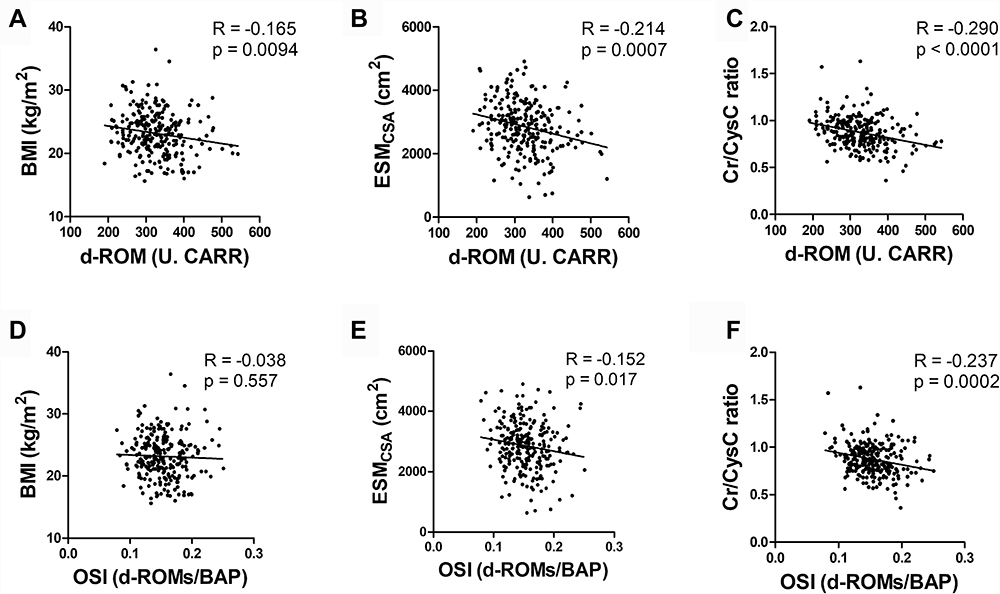 |
Figure 5 Results of correlation analyses between d-ROM levels and body mass index (BMI) (A), cross-sectional area of the erector spinae muscles (ESMCSA) (B), creatinine/cystatin C ratio (Cr/CysC ratio) (C), and between OSI and BMI (D), ESMCSA (E), and Cr/CysC ratio (F). d-ROM levels and OSI were weakly correlated with ESMCSA and Cr/CysC ratio. |
Effect of the p53 Polymorphism on d-ROMs, BAP, and OSI
Age, sex, smoking history, pulmonary function data, LAA%, BMI, ESMCSA, serum Cr/CysC ratio, d-ROM levels, BAP, OSI, and HsCRP levels among all patients classified by p53 codon 72 genotype are summarized in Table 2. With the exception of LAA% and %FEV1, no significant differences were observed in the other parameters among the p53 genotypes. LAA% was significantly higher in patients carrying the GG genotype than in patients carrying the CC genotype, and %FEV1 was significantly decreased in patients carrying the CG genotype and tended to decrease in patients carrying the GG genotype compared with patients carrying the CC genotype (Table 2). The results of analyses of the frequencies of p53 codon 72 polymorphisms are summarized in Tables 3 and 4. Although the LAA% was significantly higher in patients carrying the p53 codon 72 GG genotype, the frequency of the p53 genotype and allele were not significantly different between COPD groups and smoker control subject.
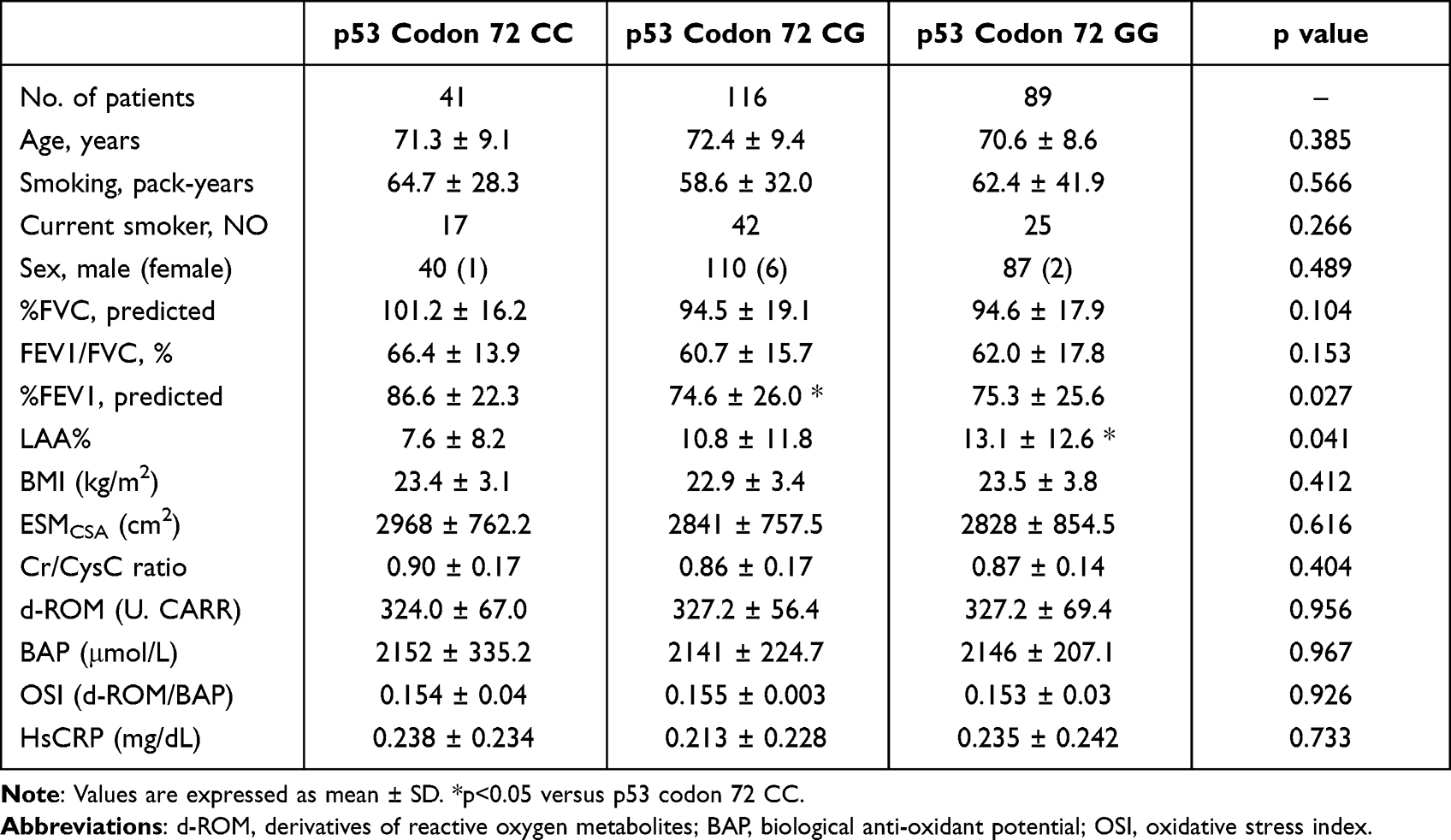 |
Table 2 Characteristics of Patients Categorized by p53 Codon 72 Genotype |
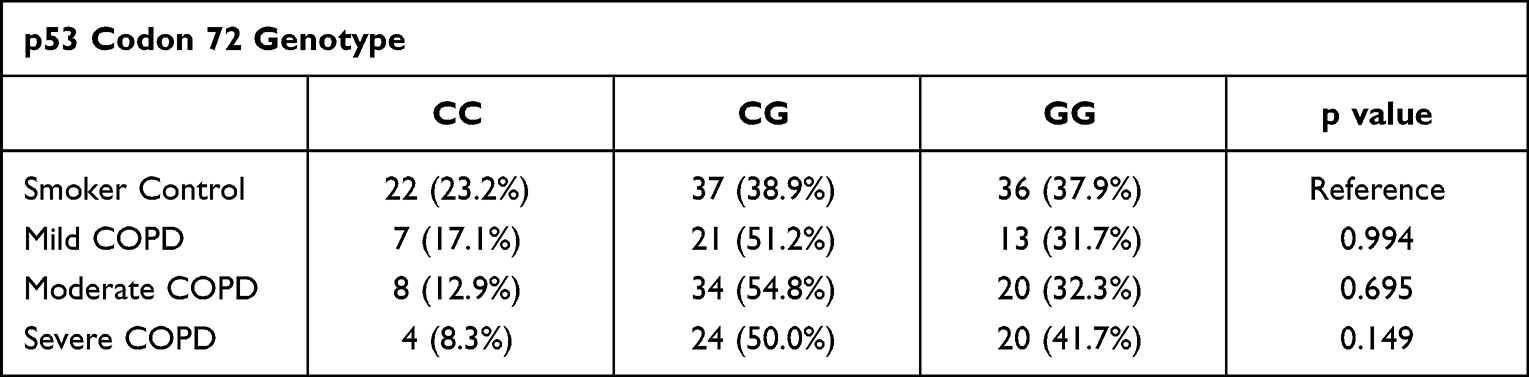 |
Table 3 p53 Genotype Frequencies in COPD Patients |
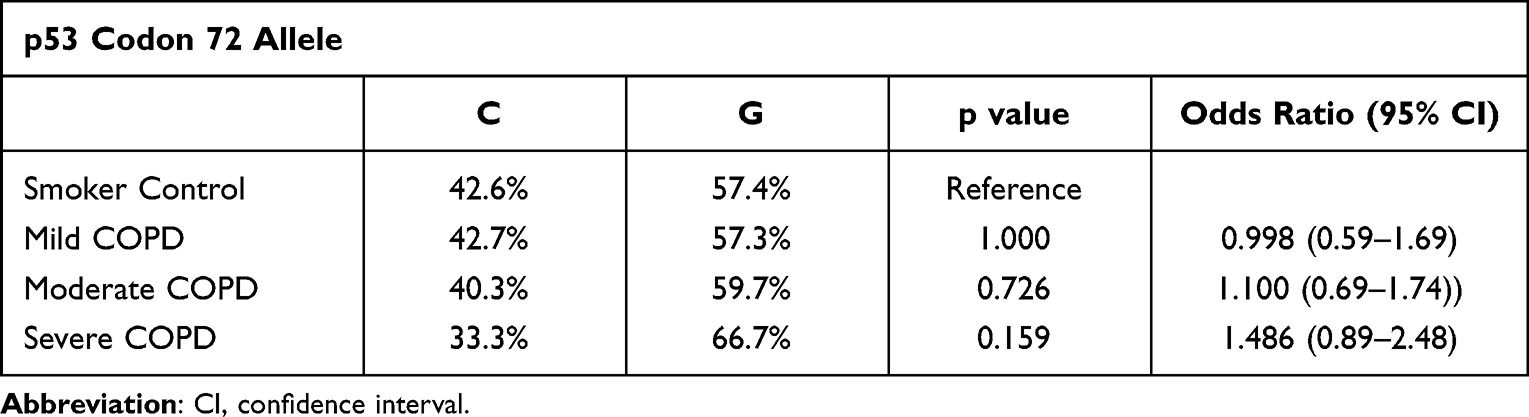 |
Table 4 p53 Allele Frequencies in COPD Patients |
In patients carrying the p53 codon 72 CG genotype, there were no significant changes in d-ROMs and OSI, but a significant change was observed in d-ROM levels of patients carrying the p53 codon 72 CC genotype. In patients carrying the p53 codon 72 GG genotype, d-ROM levels and OSI were significantly increased in the severe COPD group compared with patients in the smoking control and moderate and mild COPD groups (Figure 6). d-ROMs exhibited a small correlation with LAA% only in patients carrying the p53 GG genotype; however, there was no significant correlation between d-ROMs and LAA% in patients carrying the p53 CC or CG genotype (Figure 7).
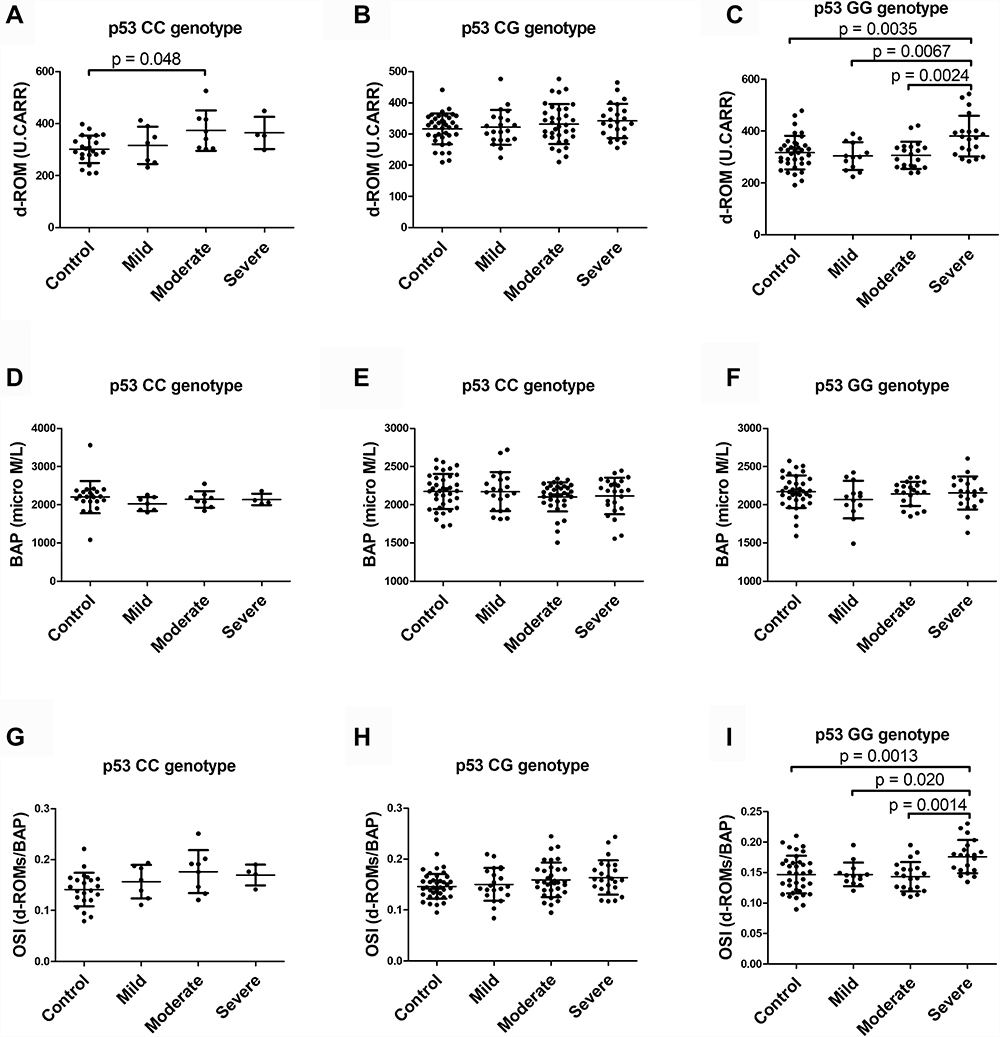 |
Figure 6 D-ROM levels in serum from smoker controls (control) and patients with moderate COPD (moderate), mild COPD (mild), and severe COPD (severe) carrying the p53 codon 72 CC genotype (A), CG genotype (B), and GG genotype (C). BAP of serum from controls and patients with moderate, mild, and severe COPD carrying the p53 codon 72 CC genotype (D), CG genotype (E), and GG genotype (F). OSI in serum from patients carrying p53 codon 72 CC genotype (G), CG genotype (H), and GG genotype (I). Data are expressed as mean ± SD. d-ROM levels and OSI in patients with severe COPD were significantly increased among those carrying the GG genotype compared with control subjects and patients with moderate and mild COPD. Only among patients with mild COPD carrying the CC genotype were d-ROM levels increased compared with control subjects. |
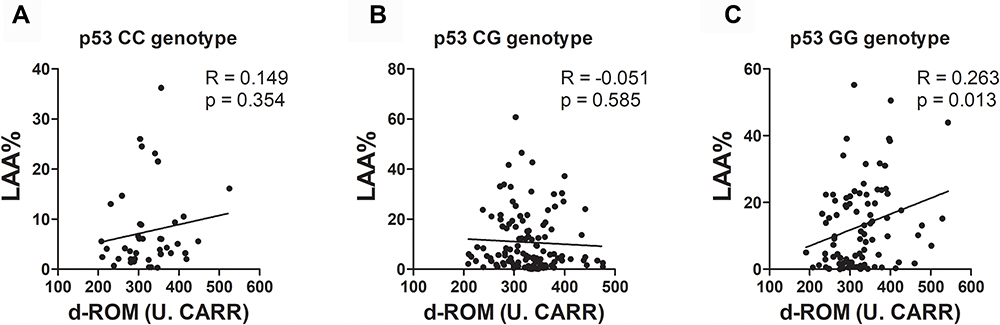 |
Figure 7 Results of correlation analyses between d-ROM levels and LAA% in patients carrying the p53 codon 72 CC genotype (A), CG genotype (B) and GG genotype (C). d-ROM levels were weakly correlated with LAA% in patients carrying the GG genotype. |
Discussion
In the present study, we demonstrated that the oxidative stress markers d-ROMs and OSI can be easily measured in serum and that these markers are associated with airflow limitations and markers of muscle atrophy and sarcopenia in COPD patients. In contrast to patients carrying the p53 codon CC and CG genotypes, associations between oxidative stress markers and COPD severity were clearer in COPD patients carrying the p53 codon 72 GG genotype, which is related to susceptibility to pulmonary emphysema.
Cigarette smoking is a major risk factor for developing COPD and also a major source of oxidative stress in the lungs. Chronic exposure to oxidative stress and persistent inflammation can lead to lung cell apoptosis and pulmonary emphysema.31 In addition, cigarette smoking depletes antioxidants associated with defense against damage to lung cells from oxidative stress.32,33 Oxidative stress can be evaluated based on the balance between ROS production and antioxidant capacity. The serum d-ROM level is an indicator of ROS production, and serum BAP represents antioxidant potential.19,34,35 Our results showing increased d-ROM levels and OSI in patients with severe COPD and the correlation between these oxidative stress markers and airflow limitation are in line with those of previous studies in COPD patients using serum malondialdehyde and iron levels,36 serum thiobarbituric acid–reactive substances, superoxide dismutase, catalase, glutathione, homocysteine,37 and serum d-ROM levels as markers of oxidative stress.22
With regard to antioxidant potential, we found no significant differences in BAP between the disease severity groups, and smoking cessation increased BAP and decreased OSI, despite the fact that severity of airflow limitation did not affect the BAP levels in the present study. These results could be explained in part by smoking-related depletion of antioxidants. Smoking is significantly associated with decreased antioxidant levels.38,39 Although it has been reported that ROS markers improve after smoking cessation, improvement in antioxidant markers is less common in COPD patients,40 probably due to sarcopenia resulting from disease progression.41 Our results showing a relatively higher ratio of ex-smokers among patients with severe COPD compared with smoking controls could have been related to BAP and OSI levels. We speculate that the improvement in antioxidants in the high proportion of former smokers was counteracted by the depletion of antioxidants due to the effect on BAP of sarcopenia associated with advanced-stage COPD in patients with severe COPD.
Previous studies reported that cells carrying the GG genotype of p53 codon 72 are more susceptible to apoptosis in response to cellular damage from various sources, including oxidative stress, compared with cells carrying the CC genotype,10,11,25 in association with enhanced activation of transcriptional apoptosis effectors.42 In the present study, we confirmed the results of our previous study showing an association between the p53 codon 72 polymorphism and severity of pulmonary emphysema.25 Furthermore, associations between the markers of oxidative stress and severity of airflow limitation and pulmonary emphysema were observed primarily in patients carrying the p53 codon 72 GG genotype. These results suggest that the p53 polymorphism plays a role in not only susceptibility of lung cells to apoptosis but also in determining different responses to oxidative stress. It is possible that patients carrying the p53 GG genotype have impaired antioxidant defense compared with patients carrying the p53 CC or CG genotype, which may be associated with lung cell apoptosis and changes in emphysema. However, the precise mechanisms underlying the different responses to oxidative stress induced by the p53 polymorphism could not be elucidated in the present study. Further studies evaluating the expression of p53-related transcriptional effector genes and/or circulating microRNAs are necessary to clarify the differences in signal transduction associated with p53 polymorphisms.
Although a previous report showed an association between the occurrence of smoking-related COPD in patients with the p53 codon 72 polymorphism,8 we did not observe any significant differences in pulmonary function between the p53 genotypes or significant differences in the frequency of the p53 genotype between the COPD groups and smoker control subjects in the present study. This discrepancy could be explained by the heterogeneous and multi-component nature of the combination of small airway disease and parenchyma destruction characterized by airflow limitation. Airflow limitation develops due to both bronchial stenosis and emphysematous changes. Airway narrowing in COPD patients may also be affected by the p53 pathway through the induction of bronchial cell apoptosis in response to the oxidative stress associated with smoking.43 The susceptibility to smoking-related airflow limitation–associated p53 polymorphisms may depend on the structural features of COPD, such as chronic bronchitis and emphysema.
There were several limitations in present study. First, there was a relatively small number of stage IV COPD patients in our cohort, which made it difficult to assess the usefulness of biomarkers of oxidative stress in severe COPD patients. In this study, there were no significant differences in d-ROM and OSI levels between patients with severe COPD or mild COPD. However, it is possible that a study with a larger number of patients with stage IV COPD could detect significant differences in d-ROMs and OSI between mild and severe COPD patients. In turn, this could reveal additional characteristics of these biomarkers that are affected by differences in the severity of airflow limitation and by p53 polymorphisms. Second, as this was a single-center retrospective study conducted in Japan, the patients were all Japanese, and thus, regional and racial differences were not considered. Because the principle of the d-ROMs test involves the release of iron from serum proteins at low pH, leading to degradation of hydroperoxides into free radicals via the Fenton reaction,44 the d-ROMs test is easily affected by lifestyle and dietary habits.45 As lifestyle varies by region and race, a multi-lateral prospective validation study involving a large cohort to exclude the effects of lifestyle on the d-ROMs test conducted in multiple facilities is needed.
Conclusion
Oxidative stress is involved in the development of COPD. In patients with COPD, systemic oxidative stress is reflected in lung cell inflammation and influenced by genetic factors.21 In the present study, d-ROMs and OSI were associated with severity of emphysema and airflow limitation, and this association was observed primarily in patients carrying the p53 codon 72 GG genotype. Susceptibility to pulmonary emphysema and responses to oxidative stress could be affected by the p53 gene polymorphism. In COPD patients carrying the p53 GG genotype, measuring d-ROMs and OSI could be a prognostic factor for increased response to oxidative stress and progression of pulmonary emphysema and deterioration of pulmonary function. In addition, measurement of d-ROM levels and BAP is an inexpensive, rapid, and easy method for evaluating oxidative stress using serum samples. If serum samples are properly stored, this method is useful in a variety of settings, including retrospective cohort analyses of COPD patients. Future long-term observational studies should be conducted to determine if measurement of d-ROM levels and BAP could be useful in predicting the outcome of patients with COPD.
Acknowledgments
This study was supported by Grants-in-Aid for Scientific Research of Japan (nos. 24591144 and 16K09593). The authors thank Makoto Kobayashi, MS, for expert technical assistance.
Disclosure
The authors report no conflicts of interest in this work. The authors confirm that the data supporting the findings of this study are available within the article.
References
1. Pryor WA. Cigarette smoke radicals and the role of free radicals in chemical carcinogenicity. Environ Health Persp. 1997;105(Suppl 4):875–882. doi:10.1289/ehp.97105s4875
2. Gwinn MR, Vallyathan V. Respiratory burst: role in signal transduction in alveolar macrophages. J Toxicol Environ Heal Part B. 2007;9(1):27–39. doi:10.1080/15287390500196081
3. Almkvist J, Dahlgren C, Leffler H, Karlsson A. Activation of the neutrophil nicotinamide adenine dinucleotide phosphate oxidase by galectin-1. J Immunol. 2002;168(8):4034–4041. doi:10.4049/jimmunol.168.8.4034
4. Roos WP, Kaina B. DNA damage-induced cell death: from specific DNA lesions to the DNA damage response and apoptosis. Cancer Lett. 2013;332(2):237–248. doi:10.1016/j.canlet.2012.01.007
5. Mizuno S, Bogaard HJ, Gomez-Arroyo J, et al. MicroRNA-199a-5p Is associated with hypoxia-inducible factor-1α expression in lungs from patients with COPD. Chest. 2012;142(3):663–672. doi:10.1378/chest.11-2746
6. Siganaki M, Koutsopoulos AV, Neofytou E, et al. Deregulation of apoptosis mediators’ p53 and bcl2 in lung tissue of COPD patients. Respir Res. 2010;11(1):46. doi:10.1186/1465-9921-11-46
7. Morissette MC, Vachon-Beaudoin G, Parent J, Chakir J, Milot J. Increased p53 Level, Bax/Bcl-x L Ratio, and TRAIL receptor expression in human emphysema. Am J Resp Crit Care. 2008;178(3):240–247. doi:10.1164/rccm.200710-1486oc
8. Lee YL, Chen W, Tsai WK, et al. Polymorphisms of p53 and p21 genes in chronic obstructive pulmonary disease. J Lab Clin Med. 2006;147(5):228–233. doi:10.1016/j.lab.2005.12.008
9. Mizuno S, Bogaard HJ, Kraskauskas D, et al. p53 Gene deficiency promotes hypoxia-induced pulmonary hypertension and vascular remodeling in mice. Am J Physiol-Lung C. 2011;300(5):L753–L761. doi:10.1152/ajplung.00286.2010
10. Walker KK, Levine AJ. Identification of a novel p53 functional domain that is necessary for efficient growth suppression. Proc National Acad Sci. 1996;93(26):15335–15340. doi:10.1073/pnas.93.26.15335
11. Sakamuro D, Sabbatini P, White E, Prendergast GC. The polyproline region of p53 is required to activate apoptosis but not growth arrest. Oncogene. 1997;15(8):887–898. doi:10.1038/sj.onc.1201263
12. Birch J, Barnes PJ, Passos JF. Mitochondria, telomeres and cell senescence: implications for lung ageing and disease. Pharmacol Therapeut. 2018;183:34–49. doi:10.1016/j.pharmthera.2017.10.005
13. Taraseviciene-Stewart L, Voelkel NF. Molecular pathogenesis of emphysema. J Clin Invest. 2008;118(2):394–402. doi:10.1172/jci31811
14. Walter MF, Jacob RF, Jeffers B, et al. Serum levels of thiobarbituric acid reactive substances predict cardiovascular events in patients with stable coronary artery disease A longitudinal analysis of the PREVENT study. J Am Coll Cardiol. 2004;44(10):1996–2002. doi:10.1016/j.jacc.2004.08.029
15. El-Bassiouni EA, Helmy MH, El-Zoghby SM, Kamel EN, Hosny RM. Relationship between level of circulating modified LDL and the extent of coronary artery disease in type 2 diabetic patients. Brit J Biomed Sci. 2016;64(3):109–116. doi:10.1080/09674845.2007.11732768
16. Wu LL, Chiou CC, Chang PY, Wu JT. Urinary 8-OHdG: a marker of oxidative stress to DNA and a risk factor for cancer, atherosclerosis and diabetics. Clin Chim Acta. 2004;339(1–2):1–9. doi:10.1016/j.cccn.2003.09.010
17. Faraci FM, Didion SP. Vascular protection: superoxide dismutase isoforms in the vessel wall. Arterioscler Thromb Vasc Biol. 2004;24(8):1367–1373. doi:10.1161/01.atv.0000133604.20182.cf
18. Pyne-Geithman GJ, Caudell DN, Prakash P, Clark JF. Glutathione peroxidase and subarachnoid hemorrhage: implications for the role of oxidative stress in cerebral vasospasm. Neurol Res. 2013;31(2):195–199. doi:10.1179/174313209x393906
19. Pasquini A, Luchetti E, Marchetti V, Cardini G, Iorio EL. Analytical performances of d-ROMs test and BAP test in canine plasma. Definition of the normal range in healthy Labrador dogs. Vet Res Commun. 2008;32(2):137–143. doi:10.1007/s11259-007-9014-x
20. Barnes PJ. Oxidative stress-based therapeutics in COPD. Redox Biol. 2020;33:101544. doi:10.1016/j.redox.2020.101544
21. Taniguchi A, Tsuge M, Miyahara N, Tsukahara H. Reactive oxygen species and antioxidative defense in chronic obstructive pulmonary disease. Antioxidants. 2021;10(10):1537. doi:10.3390/antiox10101537
22. Markoulis N, Gourgoulianis KI, Moulas A, Gerogianni E, Molyvdas AP. Reactive oxygen metabolites as an index of chronic obstructive pulmonary disease severity. Panminerva Med. 2006;48(4):209–213.
23. Yasuo M, Droma Y, Kitaguchi Y, et al. The relationship between acrolein and oxidative stress in COPD: in systemic plasma and in local lung tissue. Int J Chronic Obstr. 2019;14:1527–1537. doi:10.2147/copd.s208633
24. Kato R, Mizuno S, Kadowaki M, et al. Sirt1 expression is associated with CD31 expression in blood cells from patients with chronic obstructive pulmonary disease. Respir Res. 2016;17(1):139. doi:10.1186/s12931-016-0452-2
25. Mizuno S, Ishizaki T, Kadowaki M, et al. p53 signaling pathway polymorphisms associated with emphysematous changes in COPD patients. Chest. 2017;152(1):58–69. doi:10.1016/j.chest.2017.03.012
26. Agusti A, Vogelmeier C, Papi A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: 2021 report. Available from: https://goldcopd.org/2022-gold-reports-2/.
27. Nojiri M, Mizuno S, Nishiki K, et al. ADRB2 gene polymorphism and emphysema heterogeneity can modulate bronchodilator response in patients with emphysema. Pulm Pharmacol Ther. 2018;48:80–87. doi:10.1016/j.pupt.2017.09.004
28. Nishiki K, Nojiri M, Kato R, et al. Serum Creatinine/Cystatin C ratio associated with cross-sectional area of erector spinae muscles and pulmonary function in patients with chronic obstructive pulmonary disease. Int J Chronic Obstr. 2021;16:3513–3524. doi:10.2147/copd.s339243
29. Tanimura K, Sato S, Fuseya Y, et al. Quantitative assessment of erector spinae muscles in patients with chronic obstructive pulmonary disease. novel chest computed tomography–derived index for prognosis. Ann Am Thorac Soc. 2016;13(3):334–341. doi:10.1513/annalsats.201507-446oc
30. Hirai K, Tanaka A, Homma T, et al. Serum creatinine/cystatin C ratio as a surrogate marker for sarcopenia in patients with chronic obstructive pulmonary disease. Clin Nutr. 2021;40(3):1274–1280. doi:10.1016/j.clnu.2020.08.010
31. Fischer BM, Voynow JA, Ghio AJ. COPD: balancing oxidants and antioxidants. Int J Chronic Obstr. 2015;10:261–276. doi:10.2147/copd.s42414
32. Antwerpen VLV, Theron AJ, Richards GA, et al. Vitamin E, pulmonary functions, and phagocyte-mediated oxidative stress in smokers and nonsmokers. Free Radical Bio Med. 1995;18(5):935–941. doi:10.1016/0891-5849(94)00225-9
33. Halliwell B. Antioxidants in human health and disease. Annu Rev Nutr. 1996;16(1):33–50. doi:10.1146/annurev.nu.16.070196.000341
34. Kamezaki F, Yamashita K, Kubara T, et al. Derivatives of reactive oxygen metabolites correlates with high-sensitivity C-reactive protein. J Atheroscler Thromb. 2008;15(4):206–212. doi:10.5551/jat.e538
35. Hirose H, Kawabe H, Komiya N, Saito I. Relations between Serum Reactive Oxygen Metabolites (ROMs) and various inflammatory and metabolic parameters in a Japanese population. J Atheroscler Thromb. 2009;16(2):77–82. doi:10.5551/jat.e265
36. Bajpai J, Prakash V, Kant S, et al. Study of oxidative stress biomarkers in chronic obstructive pulmonary disease and their correlation with disease severity in north Indian population cohort. Lung India Official Organ Indian Chest Soc. 2017;34(4):324–329. doi:10.4103/lungindia.lungindia_205_16
37. Folchini F, Nonato N, Feofiloff E, D’Almeida V, Nascimento O, Jardim J. Association of oxidative stress markers and C-reactive protein with multidimensional indexes in COPD. Chron Resp Dis. 2011;8(2):101–108. doi:10.1177/1479972310391284
38. Ishizaka Y, Yamakado M, Toda A, Tani M, Ishizaka N. Relationship between coffee consumption, oxidant status, and antioxidant potential in the Japanese general population. Clin Chem Laboratory Medicine Cclm. 2013;51(10):1951–1959. doi:10.1515/cclm-2013-0146
39. Waseem SMA, Mobarak MH, Islam N, Ahmad Z. Comparative study of pulmonary functions and oxidative stress in smokers and non-smokers. Indian J Physiology Pharmacol. 2012;56(4):345–352.
40. Aydemir Y, Aydemir Ö, Şengül A, et al. Comparison of oxidant/antioxidant balance in COPD and non-COPD smokers. Heart Lung. 2019;48(6):566–569. doi:10.1016/j.hrtlng.2019.07.005
41. Sepúlveda-Loyola W, De Castro LA, Matsumoto AK, et al. NOVEL antioxidant and oxidant biomarkers related to sarcopenia in COPD. Heart Lung. 2021;50(1):184–191. doi:10.1016/j.hrtlng.2020.06.001
42. Grochola LF, Zeron-Medina J, Mériaux S, Bond GL. Single-nucleotide polymorphisms in the p53 signaling pathway. Csh Perspect Biol. 2010;2(5):a001032. doi:10.1101/cshperspect.a001032
43. Shenberger JS, Dixon PS. Oxygen induces S-phase growth arrest and increases p53 and p21(WAF1/CIP1) expression in human bronchial smooth-muscle cells. Am J Resp Cell Mol. 1999;21(3):395–402. doi:10.1165/ajrcmb.21.3.3604
44. Kilk K, Meitern R, Härmson O, Soomets U, Hõrak P. Assessment of oxidative stress in serum by d-ROMs test. Free Radical Res. 2014;48(8):883–889. doi:10.3109/10715762.2014.919390
45. Komatsu F, Kagawa Y, Sakuma M, et al. Investigation of oxidative stress and dietary habits in Mongolian people, compared to Japanese people. Nutr Metabolism. 2006;3(1):21. doi:10.1186/1743-7075-3-21
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Polymorphisms in Antioxidant Enzyme-Encoding Genes with Diabetic Nephropathy in a Group of Saudi Arabian Patients with Type II Diabetes Mellitus
Albeladi FI, Mostafa MM, Zayed MA, Atta H
International Journal of General Medicine 2022, 15:5919-5928
Published Date: 1 July 2022
Dental Pulp Stem Cells Ameliorate Elastase-Induced Pulmonary Emphysema by Regulating Inflammation and Oxidative Stress
Gao X, Liu Z, Wang Z
Journal of Inflammation Research 2023, 16:1497-1508
Published Date: 8 April 2023
Identification of Oxidative Stress-Associated Biomarkers in Chronic Obstructive Pulmonary Disease: An Integrated Bioinformatics Analysis
Jiang X, Wang M, Li H, Liu Y, Dong X
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:841-855
Published Date: 26 March 2025
Exercise Prescription Training in Chronic Obstructive Pulmonary Disease: Benefits and Mechanisms
Liu S, Yang A, Yu Y, Xu B, Yu G, Wang H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1071-1082
Published Date: 15 April 2025
Impact of Low Hand Grip Strength on Quality of Life, Utilization of Healthcare, and Mental Health in Individuals with Airflow Limitation
Kim SH, Zo S, Kong SA, Cho JH, Do JG, Shin SH, Park HY
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2199-2210
Published Date: 4 July 2025