Back to Journals » Cancer Management and Research » Volume 18

A Real-Time Online Nomogram Integrating Systemic Inflammatory Response Index and Lactate Dehydrogenase to Predict Pathological Response in Gastric Cancer Patients Receiving Neoadjuvant Chemoimmunotherapy
Authors Li L ![]() , Cai W, Han H, Chen S, Long B, Zhang G, Jiang X
, Cai W, Han H, Chen S, Long B, Zhang G, Jiang X ![]() , Zhou H, Qin L, Yu Z, Jiao Z
, Zhou H, Qin L, Yu Z, Jiao Z ![]()
Received 8 August 2025
Accepted for publication 9 January 2026
Published 21 January 2026 Volume 2026:18 559532
DOI https://doi.org/10.2147/CMAR.S559532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Javier-David Benitez-Fuentes
Long Li,1,2 Weiwen Cai,1,2 Haobo Han,1,2 Shigong Chen,1,2 Bo Long,1,2 Gengyuan Zhang,1,2 Xiangyan Jiang,1,2 Huinian Zhou,1,2 Long Qin,2,3 Zeyuan Yu,1,2 Zuoyi Jiao1,2
1Department of General Surgery, The Second Hospital of Lanzhou University, Lanzhou, People’s Republic of China; 2The Second Clinical Medical School, Lanzhou University, Lanzhou, People’s Republic of China; 3Cuiying Biomedical Research Center, Lanzhou University Second Hospital, Lanzhou, People’s Republic of China
Correspondence: Zuoyi Jiao, Department of General Surgery, The Second Hospital of Lanzhou University, Lanzhou, People’s Republic of China, Email [email protected]
Background: Globally, gastric cancer is a significant health burden. Neoadjuvant chemoimmunotherapy (NACI) has emerged as a promising strategy for locally advanced gastric cancer, but responses vary substantially among patients. Predicting major pathological response (MPR) is crucial for treatment personalization.
Objective: To develop and validate a web-based nomogram that integrates readily available clinical and serological markers to predict MPR in gastric cancer patients receiving NACI.
Methods: This retrospective study analyzed 325 gastric cancer patients who underwent NACI and radical resection. A nomogram was constructed using R software and validated with metrics including receiver operating characteristic curve (ROC), area under curve (AUC), calibration curves, and decision curve analysis (DCA), compared to the use of a single biomarker.
Results: The MPR was 53.5%. Multivariate analysis identified lower stomach location (odds ratio (OR) = 2.90; 95% confidence interval (CI): 1.35– 6.22; P = 0.006), histological differentiation grade (OR = 3.43; 95% CI: 1.77– 6.63; P < 0.001), systemic inflammatory response index (SIRI) (OR = 2.02; 95% CI: 1.02– 3.97; P = 0.043) and lactate dehydrogenase (LDH) (OR = 1.02; 95% CI: 1.01– 1.03; P < 0.001) as independent predictors of MPR. The nomogram demonstrated robust discriminative ability, with AUC values of 0.807 (95% CI: 0.751– 0.863) and 0.799 (95% CI: 0.711– 0.888) in the training and testing sets, respectively. Furthermore, DCA further confirmed its significant clinical utility.
Conclusion: We developed and internally validated a nomogram that accurately predicts MPR after NACI. Implemented as a user-friendly web-based calculator, this model enables real-time, individualized estimation of MPR probability and may assist clinicians in tailoring treatment strategies for patients with gastric cancer. Further external and prospective validation is warranted.
Keywords: gastric cancer, systemic inflammatory response index, lactate dehydrogenase, nomogram, major pathological response, web calculator
Introduction
Globally, gastric cancer ranks fifth in both incidence and mortality among malignant tumors.1 In China, the burden of gastric cancer is especially severe, with incidence and mortality rates remaining high, potentially due to factors such as later stage at diagnosis and regional disparities in access to optimal care.2 The advent of immune checkpoint inhibitors (ICIs) has transformed the therapeutic landscape. Combining neoadjuvant chemotherapy (NAC) with ICIs (NACI) for locally advanced gastric cancer shows promising efficacy.3,4 However, responses to NACI are heterogeneous, creating a pressing need for practical tools to identify patients most likely to benefit.
Major pathological response (MPR) is a well-established surrogate endpoint that correlates with improved long-term survival after neoadjuvant therapy, making its prediction clinically valuable.5,6 For patients with a reduced probability of achieving MPR, the treatment strategy should be modified by immediately stopping NACI and considering surgical or other options instead. Current approaches to predict treatment response, including repeated histopathological evaluations,7–9 advanced molecular profiling,10 specialized imaging techniques,11,12 and gene expression profiling13 are often costly, invasive, technically complex, and not universally accessible. Furthermore, machine learning has demonstrated substantial potential in data processing. On this basis, numerous clinical models integrating machine learning algorithms and large-scale medical datasets have been established for practical application in clinical practice.14 While machine learning (ML) models offer potential, they can be “black boxes” with limited interpretability and require significant computational expertise, hindering their practical adoption in routine clinical practice.15 In contrast, nomograms provide a transparent, intuitive, and user-friendly graphical interface that quantifies individual risk by integrating multiple variables, making them highly suitable for point-of-care clinical decision-making.16 In recent years, researchers have investigated the potential of routine serological markers to predict pCR in breast cancer patients receiving NAC.17 There is a growing recognition of the value of routine serological markers as cost-effective and minimally invasive proxies of the tumor microenvironment. Among these, the systemic inflammatory response index (SIRI), which integrates neutrophil, monocyte, and lymphocyte counts, has emerged as a robust prognostic indicator in gastric cancer, reflecting the critical interplay between systemic inflammation and cancer progression.18 Similarly, lactate dehydrogenase (LDH), a key enzyme in tumor glycolysis, serves as a valuable marker of tumor metabolic activity.19
Despite the established prognostic value of SIRI and LDH, their combined role in predicting pathological response to NACI has not been systematically explored. Critically, the predictive role of SIRI may be context-dependent. While prior research in patients receiving direct surgery or surgery combined with neoadjuvant chemotherapy without immunotherapy consistently links elevated SIRI to poorer survival, reflecting a pro-tumor inflammatory milieu,18 the immunomodulatory action of ICIs within NACI may fundamentally alter this relationship. Our preliminary data intriguingly suggest that in the unique context of NACI, a comparatively higher SIRI may, in fact, be associated with a better pathological response. This indicates that the biological implications of systemic inflammation may shift when immunotherapy is introduced, potentially signifying a more robust, pre-activated immune state poised for synergy with chemoimmunotherapy. The development of an integrative model that leverages these dynamic, readily available biomarkers is therefore critical to address a clear unmet need in clinical oncology. Although risk stratification models are valuable, existing approaches that rely on single conventional laboratory indicators suffer from limited predictive accuracy. To date, few studies have systematically explored which combinations of routine laboratory tests can effectively predict MPR in gastric cancer patients receiving NACI, and the efficacy of such integrated models requires further validation.
Therefore, the primary objective of this study was to develop and validate a practical, web-based nomogram that integrates pretreatment SIRI and LDH with key clinical variables to predict the probability of MPR in gastric cancer patients undergoing NACI. The ultimate goal is to provide clinicians with an accessible and actionable tool to facilitate personalized treatment planning at the point of care.
Materials and Methods
Study Participants
This retrospective study consecutively enrolled raw data from the medical record system at the Second Hospital of Lanzhou University, a major tertiary care center in Gansu Province. The study period was from June 1, 2020, to May 31, 2025. The study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of the Second Hospital of Lanzhou University (Project Number: 2024 A-1281). The need for informed consent was waived due to the retrospective nature of the study and the protection of patient privacy and identity information. Data integrity was assessed through manual curation. Inclusion criteria: (1) patients who underwent radical resection after NACI; (2) pathological confirmation of gastric cancer; (3) availability of complete clinicopathological. Exclusion criteria: (1) coexistence of other malignant tumors; (2) a history of hematological, autoimmune, or chronic inflammatory diseases prior to enrollment.
Data Collection
Clinical variables were retrieved from the hospital’s electronic medical records, including: demographic details (sex, age and Eastern Cooperative Oncology Group Score), body mass index, pretreatment laboratory parameters before NACI (blood cell counts, carcinoembryonic antigen (CEA), cancerantigen19-9 (CA19-9) and lactate dehydrogenase (LDH)), and detailed pathological information. The latter included overall TNM stage (tumors staged according to the eighth version of the American Joint Committee on Cancer (AJCC) tumor-node-metastasis classification), primary tumor location (classified as upper (cardia/fundus), middle (gastric body), or lower (antrum/pylorus) based on AJCC criteria) and MSI status.
Systemic inflammatory response index (SIRI)= (neutrophil count × monocyte count)/lymphocyte count,20 Monocyte lymphocyte ratio (MLR)= monocyte count/lymphocyte count, Platelet lymphocyte ratio (PLR)= platelet count/lymphocyte count.21
The primary endpoint of the study was MPR. MPR was defined as ≤10% residual viable tumor cells using Becker’s tumor regression grading (TRG) criteria.22
Statistical Analysis
Analyses used SPSS 26.0 and R 4.5.1. Continuous variables were compared with Student’s t-test (normally distributed) or Mann–Whitney U-test (non-normal distributions). Categorical variables were analyzed with χ2 or Fisher’s exact tests. Variables with a P-value < 0.05 in univariate logistic regression were included in the multivariate logistic regression model to identify independent predictors. Gender was included as a covariate in the multivariate model to adjust for potential confounding. A nomogram incorporating independent predictors was developed by using the rms package in R. Model performance was assessed by receiver operating characteristic curve (ROC), area under curve (AUC), sensitivity, specificity, accuracy, positive predictive value (PPV), negative predictive value (NPV), calibration curves (Bootstrap resampling, 1000 replicates), and decision curve analysis (DCA). Data were partitioned into training (70%) and testing (30%) sets using the caret package. Internal validation employed 1000 bootstrap iterations in the training and testing set. Two-tailed P<0.05 indicated statistical significance.
Results
Characteristics of the Study Cohort
A total of 378 patients were enrolled in primary analysis. Following manual data integrity assessment, 53 patients were excluded for varying degrees of missing data, resulting in a final cohort of 325 patients for analysis and model development, of whom 280 were men and 45 were women, 174 patients attained MPR and 151 did not, the MPR rate is 53.5% in this study. The screening diagram is shown in Figure 1. These patients were randomly allocated to training and testing sets at a 7:3 ratio, resulting in 227 and 98 subjects in each set, respectively. Baseline characteristics showed no significant intergroup differences (all P>0.05), with complete comparative data presented in Table 1.
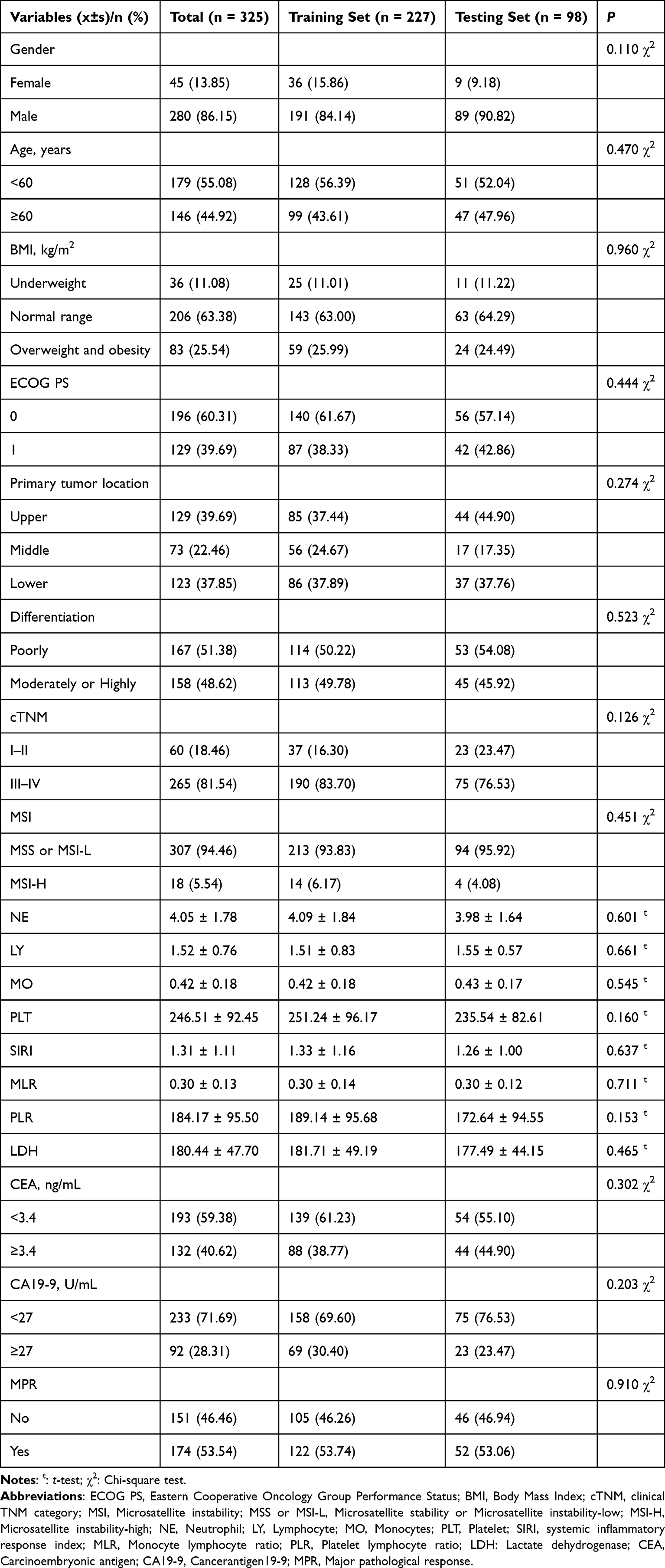 |
Table 1 Baseline Characteristics of the Training and Testing Sets |
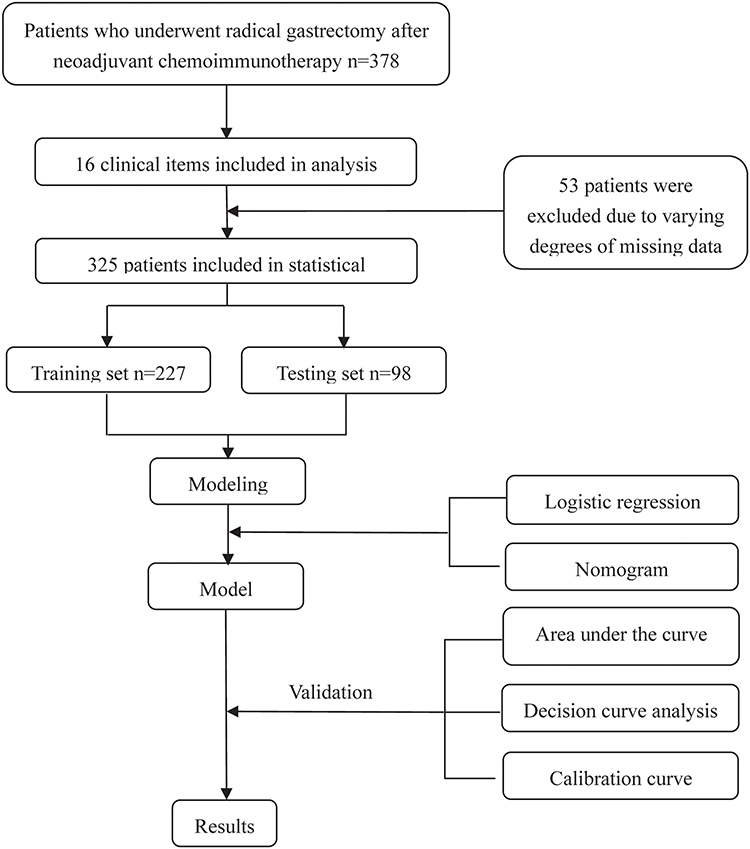 |
Figure 1 Flow diagram of study design. |
Univariate and Multivariate Logistic Regression Analyses
Table 2 presents the outcomes of both univariate and multivariate Logistic regression analyses, elucidating the relationship of various clinical and biochemical parameters with MPR in gastric cancer patients. Univariate analysis revealed that primary tumor location, MSI status, histological differentiation grade, SIRI, LDH and MLR were significantly correlated with MPR (all P<0.05). The independent prognostic role of these variables was further examined through multivariate regression analysis. Multivariate analysis results showed that SIRI (Odds Ratio (OR)=2.02, 95% Confidence Interval (CI)=1.02–3.97, P=0.043), LDH (OR=1.02, 95% CI=1.01–1.03, P<0.001), primary tumor location in the lower stomach (OR=2.90, 95% CI=1.35–6.22, P=0.006), and histological differentiation grade (OR=3.43, 95% CI=1.77–6.63, P<0.001) emerged as independent predictors of MPR.
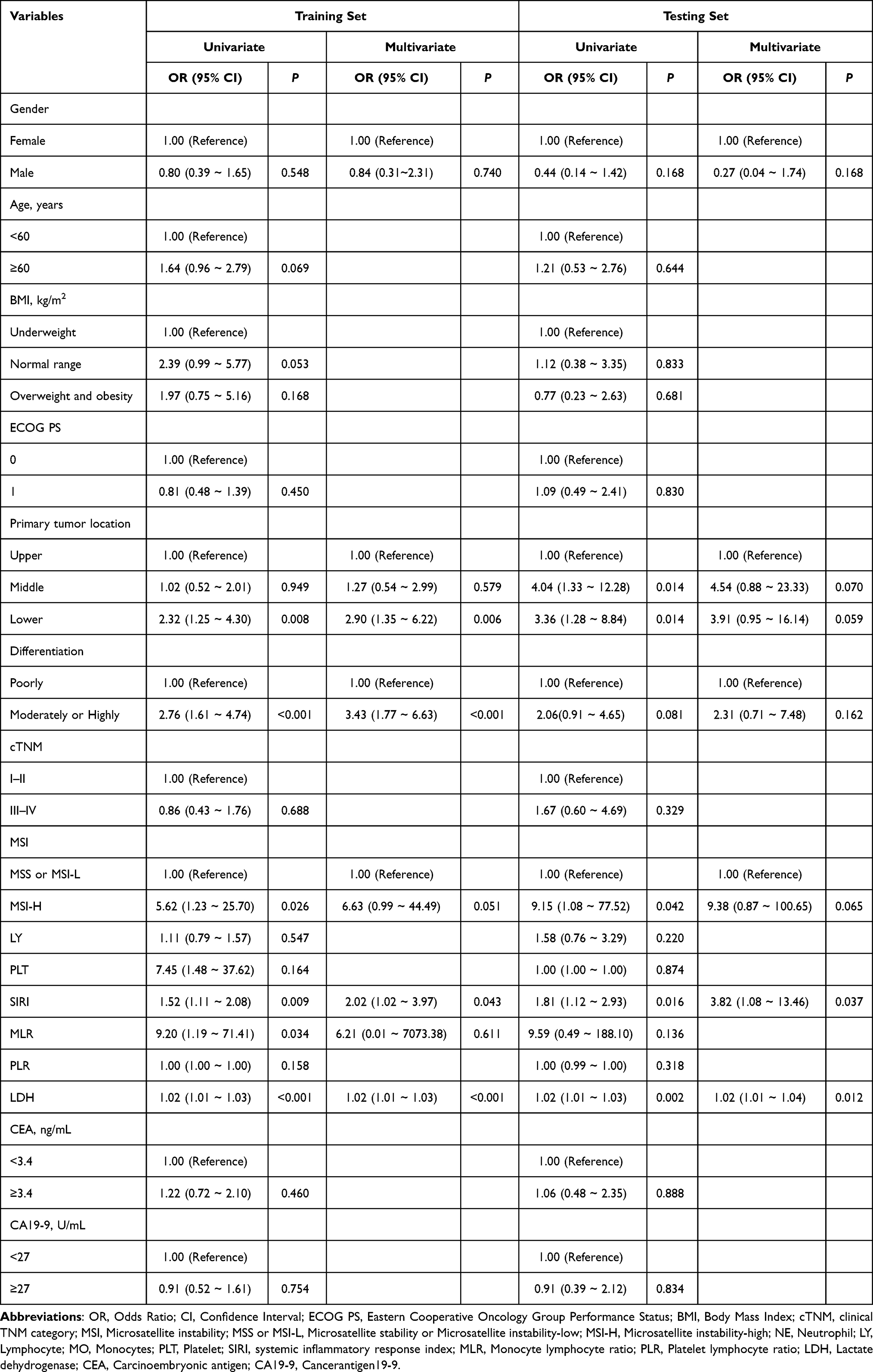 |
Table 2 Univariate and Multivariate Analysis of Variables Related to MPR in Training and Validation Sets |
Development and Validation of the Nomogram Model
Utilizing independent prognostic factors identified through univariate and multivariate Logistic regression analyses, a nomogram model was constructed to predict MPR in gastric cancer patients (Figure 2). Comparative analysis comparing the predictive efficacy of each independent risk factor individually to that of the nomogram model demonstrated the superiority of the latter in predicting MPR. Through bootstrap validation (resampling=1000), the developed nomogram model demonstrated robust predictive performance, achieving an AUC value of 0.807 (95% CI: 0.751–0.863) in the training set and 0.799 (95% CI: 0.711–0.888) in the independent testing set (Figure 3). Calibration curves for MPR probabilities demonstrated a high level of agreement between predicted and observed outcomes, attesting to the model’s credibility (Figure 4). Additionally, the DCA further confirmed the significant clinical efficacy of this nomogram model in predicting MPR probabilities (Figure 5).
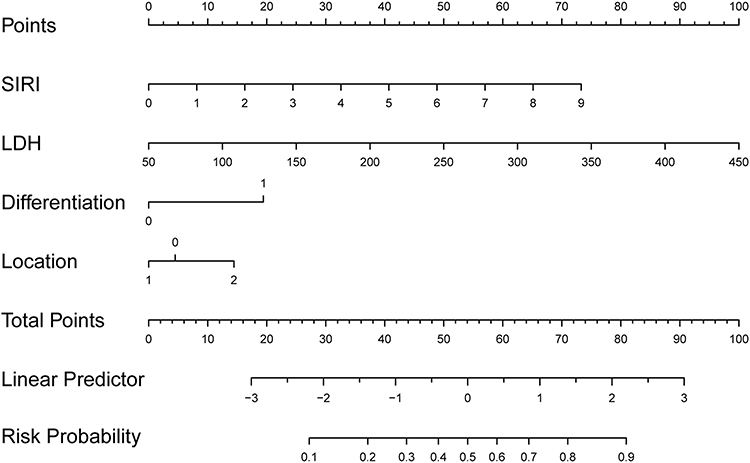 |
Figure 2 Nomogram model based on the variables selected by Logistic regression. |
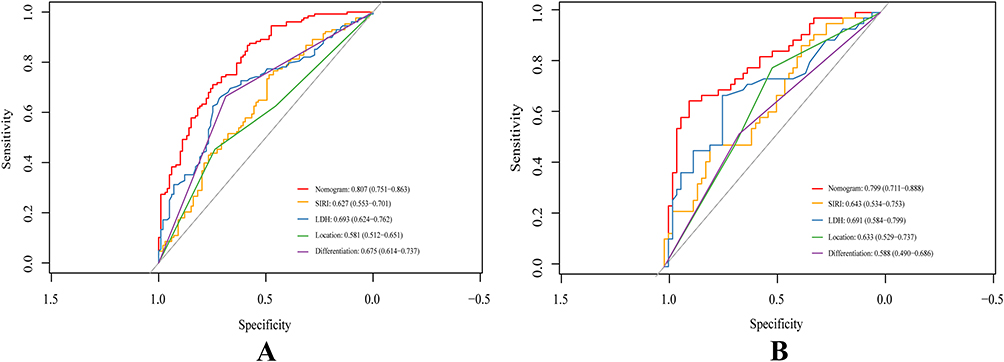 |
Figure 3 Performance of the predictive model by receiver operating characteristic (ROC) curves. (A) The training set. (B) The testing set. |
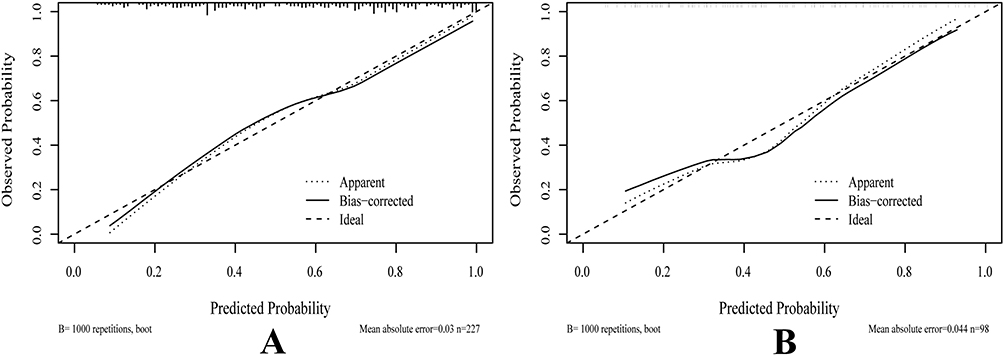 |
Figure 4 The calibration curve of the nomogram. (A) The training set. (B) The testing set. |
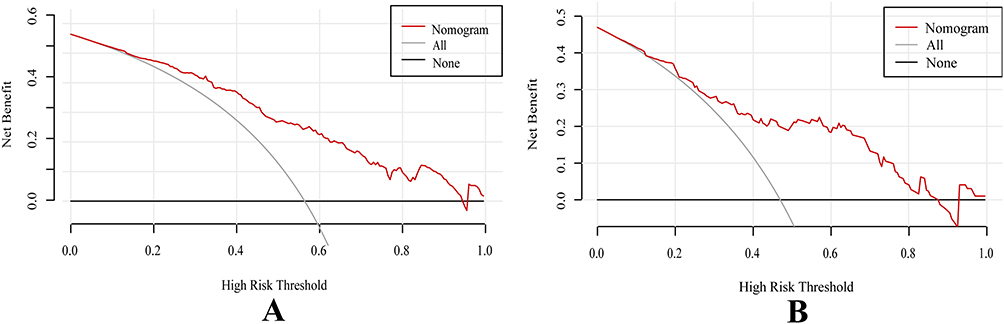 |
Figure 5 The validation of the decision curve analysis (DCA) for the nomogram. (A) The training set. (B) The testing set. |
Comprehensive Model Performance Evaluation
The predictive performance of the nomogram was further evaluated using a comprehensive set of classification metrics at the optimal probability threshold, which was determined to be 0.576 by maximizing Youden’s Index. As summarized in Table 3, in the training set, the model demonstrated a sensitivity of 67.2%, a specificity of 80.2%, and an overall accuracy of 73.2%. The PPV and NPV were 79.6% and 68.0%, respectively, resulting in an F1-score of 0.729. When applied to the independent testing set, the model maintained robust performance with a sensitivity of 59.6%, a specificity of 75.6%, and an accuracy of 67.0%. The corresponding PPV, NPV, and F1-score in the testing set were 0.738, 0.618, and 0.660, respectively. The observed consistency in performance across both sets, with a predictable and minor decrease in metrics in the testing set, indicates a good generalizability of the nomogram without substantial overfitting.
 |
Table 3 Comprehensive Performance Metrics of the Nomogram in the Training and Testing Sets |
Discussion
This single-center retrospective cohort study evaluated SIRI, LDH, primary tumor location, and histological differentiation grade as predictors of treatment efficacy in gastric cancer patients receiving NACI. In this study, we established correlations between these biomarkers and therapeutic response, developing a visualized nomogram to assist clinicians in personalizing treatment strategies.
Inflammation plays a multifaceted role in oncogenesis, actively contributing to tumor initiation and progression across all stages.23 Neutrophils can either synergize with immune networks to suppress tumors or be co-opted to facilitate immune escape and progression. Additionally, their granular components can promote proliferation, metastasis, and angiogenesis.24 Lymphocytes form the foundation of tumor immunosurveillance through antigen-specific recognition and cytotoxic elimination.25 Monocytes and their derivatives, such as tumor-associated macrophages, paradoxically regulate both immune tolerance and anti-tumor responses. Peripheral blood monocytes differentiate into tumor-associated macrophages, dendritic cells, and myeloid-derived suppressor cells, critically regulating progression and therapy outcomes by modulating immune responses.26 This link between systemic inflammation and the tumor immune milieu underpins the value of accessible peripheral blood parameters as cost-effective prognostic biomarkers, despite their inherent variability due to non-specific confounders like infection or medication.
SIRI, calculated from neutrophil, lymphocyte, and monocyte counts, serves as an inflammatory biomarker and prognostic indicator for OS and PFS in various cancers, such as gastric cancer,27 breast cancer,28 rectal cancer,29 hepatoblastoma,30 lung adenocarcinoma,31 and pancreatic cancer.32 SIRI integrates these three cell levels to holistically assess systemic inflammatory activity and immune state, providing a comprehensive biomarker for disease monitoring. Contrary to expectations, our study showed gastric cancer patients with high pretherapeutic SIRI exhibited better therapeutic responses than those with low SIRI. Interestingly, Zuo et al31 found that SIRI values declined in lung adenocarcinoma patients who had the best response to first-line therapy and increased again as the disease progressed. Real-time tracking of systemic inflammatory dynamics serves as a predictive tool for therapeutic response, providing early warning signals of resistance while guiding precise treatment. Elevated SIRI may signify enhanced myeloid regenerative capacity facilitating post-chemoimmunotherapy immune reconstitution. Our cohort identifies a distinctive SIRI cutoff (0.765) below conventional thresholds, potentially indicating an immunologically primed state. Preliminarily, we use the upper limit of normal (ULN) for monocytes and neutrophils and the lower limit of normal for lymphocytes to calculate the maximum normal threshold of SIRI (3.436), serving as its prognostic high-risk threshold. Dynamic SIRI patterns post-treatment showed predictive value: decreases may correlate with immune activation, progressive elevations with hyperactivation, while sustained surges beyond high-risk thresholds signal pathological inflammation.
LDH, a key metabolic enzyme, functions as a prognostic biomarker for multiple cancers.33 Research indicates that LDH enhances tumor cell survival, migration, and proliferation while driving angiogenesis and metastasis in gastric cancer.19 Previous clinical studies have confirmed that high LDH levels are associated with worse OS and PFS prognoses in various cancers, including gastric cancer,34 urothelial carcinoma35 and renal cell carcinoma.36 Contrary to conventional paradigms, lactate-mediated augmentation of CD8+ T cell stemness was found to potentiate anti-tumor immunity in multiple tumor models, a protective mechanism historically overshadowed by its immunosuppressive dominance.37 Interestingly, our study revealed enhanced NACI responses in patients with elevated pretherapeutic LDH compared to those with low baseline LDH. Whereas prior investigations employed the institutional ULN (typically <250 U/L) as the OS and PFS prognostic cutoff, our cohort established a substantially lower threshold (171 U/L). Elevated LDH may signify enhanced immunometabolic fitness for processing chemotherapy-released tumor antigens. However, sustained elevation beyond ULN serves as a harbinger of disease progression. Therefore, serial LDH assessment is imperative for therapeutic monitoring during chemoimmunotherapy.
Our analysis of 325 gastric cancer patients who underwent NACI and radical surgery identified that low pretherapeutic levels of LDH and SIRI were associated with a poorer therapeutic response. Both LDH and SIRI emerged as independent risk factors for MPR, underscoring the impact of inflammation, glycolysis, and hypoxia on treatment outcomes and their utility in effective prognosis prediction. While the findings underscore the necessity for in-depth exploration of potential molecular mechanisms that may underlie the current discoveries, the precise biological basis for these observations remains unclear. The ROC curve analysis demonstrated that the nomogram model exhibited significantly better predictive performance than any single indicator alone. By integrating inflammation- and glycolysis-related markers with conventional clinical factors, the nomogram enables refined risk stratification, enhances prediction precision, and supports personalized treatment strategies. The nomogram serves as a valuable tool to identify high-risk patients requiring intensive regimens, closer monitoring, or targeted therapies, improving outcomes. Monitoring SIRI or LDH dynamics may prompt clinicians to reassess and adjust therapeutic strategies. For patients with persistently low SIRI & LDH or sustained elevation exceeding conventional high-risk thresholds, early NACI discontinuation, followed by timely surgery or alternative strategies, is recommended to enhance prognosis and minimize unnecessary treatment. Consequently, protocol-mandated serial assessment of SIRI and LDH dynamics at baseline and during treatment is essential for precision management of these patients.
To our knowledge, this is the first study combining inflammatory markers reflecting inflammation, immunity, glycolysis, and hypoxia to explore their relationship with chemoimmunotherapeutic response in gastric cancer. Our nomogram visualizes their impact on therapeutic outcomes. To enhance accessibility and clinical utility, we developed and deployed a web-based computational prediction tool using R Shiny (URL: https://prediction-123.shinyapps.io/Gastric_MPR_Predictor/). This tool enables rapid risk-level determination through simple interpretation of test indices or results and accurate identification of high-risk patients. By providing a holistic assessment, this readily accessible nomogram and its online implementation serve as invaluable resources for informing therapeutic strategies. Readily available at the point of care via the web interface, our nomogram offers clinicians a robust basis for informed decisions and tailored management, holding substantial clinical importance.
Our study has some limitations. Primarily, the single-institution retrospective design constrains generalizability due to limited sample diversity (n=325) and absence of external validation. Secondly, optimal cut-offs for SIRI and LDH determined through ROC analysis lack standardized reference thresholds, introducing inter-method variability that may compromise comparability.38 Thirdly, given that SIRI levels exhibit dynamic fluctuations during tumor progression and demonstrate significant correlations with therapeutic response, longitudinal multimodal data collection throughout the treatment course is imperative. Finally, due to the uncertainty of the critical value of SIRI and LDH, our web calculator also needs further improvement. Consequently, these limitations highlight the need for multicenter prospective trials with standardized protocols and external validation to enhance reproducibility and clinical applicability. Furthermore, the male-predominant cohort (86%) may limit the generalizability of our findings, and future validation is necessary not only in more balanced populations but also through comparisons with more complex machine learning models to determine the optimal predictive approach.
Despite these limitations, our nomogram provides a valuable, cost-effective strategy for initial risk stratification. It can help clinicians identify patients with a high probability of response, who may optimally benefit from NACI, and those with a low probability, for whom alternative treatment strategies or early surgical intervention could be considered. Meanwhile, our findings provide the necessary foundation for prospective clinical validation of this model, and plan to conduct an external validation study in the future.
Conclusion
In conclusion, we developed and validated a nomogram that effectively predicts the probability of MPR following NACI in gastric cancer patients by integrating four key variables: histological differentiation grade, tumor location, SIRI, and LDH. This model has been translated into an accessible web-based calculator to facilitate point-of-care risk assessment. While this represents a significant step towards personalized therapy, the model’s definitive generalizability awaits external validation in multi-center, prospective cohorts, including assessments across key patient subgroups. Future work should also focus on evaluating the tool’s real-world utility in optimizing clinical decision-making, such as stratifying patients for treatment escalation or de-escalation, which could inform future clinical policy.
Data Sharing Statement
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of the Second Hospital of Lanzhou University (Project Number:2024 A-1281). As this study is a retrospective and the privacy and personal identity information of the patients were protected, the need for informed consent was waived by the Medical Ethics Committee of the Second Hospital of Lanzhou University.
Acknowledgments
We are grateful for the financial support provided by the National Natural Science Foundation of China, Grant from Gansu Provincial Administration of Traditional Chinese Medicine, Basic Research Innovation Group of Lanzhou University, Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital and Lanzhou Science and Technology Plan Project. This previous version is available as a preprint on ResearchSquare at: https://www.researchsquare.com/article/rs-7001726/v1.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82371952), Grant from Gansu Provincial Administration of Traditional Chinese Medicine (No. GZKZ-2024-23), Basic Research Innovation Group of Lanzhou University (No. 25JRRA800), Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (No. CY2022-QN-A13) and Lanzhou Science and Technology Plan Project (No. 2023-4-26).
Disclosure
The authors declare no competing interests in this work.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–13. doi:10.3322/caac.21834
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Li S, Xu Q, Dai X, et al. Neoadjuvant therapy with immune checkpoint inhibitors in gastric cancer: a systematic review and meta-analysis. Ann Surg Oncol. 2023;30(6):3594–3602. doi:10.1245/s10434-023-13143-w
4. de Moraes FCA, Sano VKT, Silva BL, et al. PD-1/PD-L1 Inhibitors Increase Pathological Complete Response in Locally Advanced Gastric Cancer: a Meta-analysis and Trial Sequential Analysis. J Gastrointest Cancer. 2025;56(1):49. doi:10.1007/s12029-024-01141-4
5. Su S. Efficacy and safety of PD‑1/PD‑L1 inhibitors combined with chemotherapy in patients with advanced gastric or gastro‑esophageal junction cancer: a systematic review and meta‑analysis. Oncol Lett. 2023;26(3):373. doi:10.3892/ol.2023.13960
6. Formica V, Morelli C, Fornaro L, et al. PD-L1 thresholds predict efficacy of immune checkpoint inhibition in first-line treatment of advanced gastroesophageal adenocarcinoma. A systematic review and meta-analysis of seven Phase III randomized trials. ESMO Open. 2024;9(11):103967. doi:10.1016/j.esmoop.2024.103967
7. Zhou Z, Ren Y, Zhang Z, et al. Digital histopathological images of biopsy predict response to neoadjuvant chemotherapy for locally advanced gastric cancer. Gastric Cancer. 2023;26(5):734–742. doi:10.1007/s10120-023-01407-z
8. Hoang DT, Dinstag G, Shulman ED, et al. A deep-learning framework to predict cancer treatment response from histopathology images through imputed transcriptomics. Nat Cancer. 2024;5(9):1305–1317. doi:10.1038/s43018-024-00793-2
9. Han Z, Zhang Z, Yang X, et al. Development and interpretation of a pathomics-driven ensemble model for predicting the response to immunotherapy in gastric cancer. J Immunother Cancer. 2024;12(5):e008927. doi:10.1136/jitc-2024-008927
10. Matsuoka T, Yashiro M. Bioinformatics analysis and validation of potential markers associated with prediction and prognosis of gastric cancer. Int J Mol Sci. 2024;25(11):5880. doi:10.3390/ijms25115880
11. Huang W, Xiong W, Tang L, et al. Non-invasive CT imaging biomarker to predict immunotherapy response in gastric cancer: a multicenter study. J Immunother Cancer. 2023;11(11):e007807. doi:10.1136/jitc-2023-007807
12. Ma Y, Wang Z, Qiu C, et al. Nomogram based on CT imaging and clinical data to predict the efficacy of PD-1 inhibitors combined with chemotherapy in advanced gastric cancer. Front Immunol. 2025;16:1504387. doi:10.3389/fimmu.2025.1504387
13. Wang Q, Zhang B, Wang H, et al. Identification of a six-gene signature to predict survival and immunotherapy effectiveness of gastric cancer. Front Oncol. 2023;13:1210994. doi:10.3389/fonc.2023.1210994
14. Barat M, Pellat A, Hoeffel C, et al. CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence. Jpn J Radiol. 2024;42(3):246–260. doi:10.1007/s11604-023-01504-0
15. Lei H, Li X, Ma W, et al. Comparison of nomogram and machine-learning methods for predicting the survival of non-small cell lung cancer patients. Cancer Innov. 2022;1(2):135–145. doi:10.1002/cai2.24
16. Park SY. Nomogram: an analogue tool to deliver digital knowledge. J Thorac Cardiovasc Surg. 2018;155(4):1793. doi:10.1016/j.jtcvs.2017.12.107
17. Şahin AB, Cubukcu E, Ocak B, et al. Low pan-immune-inflammation-value predicts better chemotherapy response and survival in breast cancer patients treated with neoadjuvant chemotherapy. Sci Rep. 2021;11(1):14662. doi:10.1038/s41598-021-94184-7
18. Ren JY, Xu M, Niu XD, et al. Systemic inflammatory response index is a predictor of prognosis in gastric cancer patients: retrospective cohort and meta-analysis. World J Gastrointest Surg. 2024;16(2):382–395. doi:10.4240/wjgs.v16.i2.382
19. Mishra D, Banerjee D. Lactate dehydrogenases as metabolic links between tumor and stroma in the tumor microenvironment. Cancers. 2019;11(6):750. doi:10.3390/cancers11060750
20. Kanbur B, Unek IT, Uzun M, et al. Association of Systemic Inflammatory Response Index and Prognostic Nutritional Index Scores with Sarcopenia in Patients with Metastatic Gastric Cancer. Medicina. 2025;61(5):785. doi:10.3390/medicina61050785
21. Kim SG, Eom BW, Yoon H, et al. Prognostic Value of Preoperative Systemic Inflammatory Parameters in Advanced Gastric Cancer. J Clin Med. 2022;11(18):5318. doi:10.3390/jcm11185318
22. Becker K, Mueller JD, Schulmacher C, et al. Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer. 2003;98(7):1521–1530. doi:10.1002/cncr.11660
23. Zavros Y, Merchant JL. The immune microenvironment in gastric adenocarcinoma. Nat Rev Gastroenterol Hepatol. 2022;19(7):451–467. doi:10.1038/s41575-022-00591-0
24. Huang X, Nepovimova E, Adam V, et al. Neutrophils in cancer immunotherapy: friends or foes? Mol Cancer. 2024;23(1):107. doi:10.1186/s12943-024-02004-z
25. Chen X, Wu P, Liu Z, et al. Tertiary lymphoid structures and their therapeutic implications in cancer. Cell Oncol Dordr. 2024;47(5):1579–1592. doi:10.1007/s13402-024-00975-1
26. Patysheva M, Frolova A, Larionova I, et al. Monocyte programming by cancer therapy. Front Immunol. 2022;13:994319. doi:10.3389/fimmu.2022.994319
27. Yazici H, Yegen SC. Is Systemic Inflammatory Response Index (SIRI) a Reliable Tool for Prognosis of Gastric Cancer Patients Without Neoadjuvant Therapy? Cureus. 2023;15(3):e36597. doi:10.7759/cureus.36597
28. Yamanouchi K, Maeda S. The Efficacy of Inflammatory and Immune Markers for Predicting the Prognosis of Patients with Stage IV Breast Cancer. Acta Med Okayama. 2023;77(1):37–43. doi:10.18926/AMO/64360
29. Ding Y, Liu Z, Li J, et al. Predictive effect of the systemic inflammation response index (SIRI) on the efficacy and prognosis of neoadjuvant chemoradiotherapy in patients with locally advanced rectal cancer. BMC Surg. 2024;24(1):89. doi:10.1186/s12893-024-02384-5
30. Zheng C, Ye S, Liu W, et al. Prognostic value of systemic inflammation response index in hepatoblastoma patients receiving preoperative neoadjuvant chemotherapy. Front Oncol. 2023;13:1276175. doi:10.3389/fonc.2023.1276175
31. Zuo R, Zhu F, Zhang C, et al. The response prediction and prognostic values of systemic inflammation response index in patients with advanced lung adenocarcinoma. Thorac Cancer. 2023;14(16):1500–1511. doi:10.1111/1759-7714.14893
32. Pacheco-Barcia V, Mondéjar Solís R, France T. A systemic inflammation response index (SIRI) correlates with survival and predicts oncological outcome for mFOLFIRINOX therapy in metastatic pancreatic cancer. Pancreatology. 2020;20(2):254–264. doi:10.1016/j.pan.2019.12.010
33. Sharma D, Singh M, Rani R. Role of LDH in tumor glycolysis: regulation of LDHA by small molecules for cancer therapeutics. Semin Cancer Biol. 2022;87:184–195. doi:10.1016/j.semcancer.2022.11.007
34. Chen J, Zou X. Prognostic significance of lactate dehydrogenase and its impact on the outcomes of gastric cancer: a systematic review and meta-analysis. Front Oncol. 2023;13:1247444. doi:10.3389/fonc.2023.1247444
35. Wakamiya T, Yamashita S, Kohjimoto Y, Hara I. Serum Lactate Dehydrogenase Level Prior to First-Line Chemotherapy for Metastatic Urothelial Carcinoma Is a Prognostic Factor for Avelumab Maintenance Therapy: a Multicenter Retrospective Study. Int J Urol. 2025;32(8):997–1004. doi:10.1111/iju.70086
36. Shen J, Chen Z, Zhuang Q, et al. Prognostic value of serum lactate dehydrogenase in renal cell carcinoma: a systematic review and meta-analysis. PLoS One. 2016;11(11):e0166482. doi:10.1371/journal.pone.0166482
37. Feng Q, Liu Z, Yu X, et al. Lactate increases stemness of CD8+T cells to augment anti-tumor immunity. Nat Commun. 2022;13(1):4981. doi:10.1038/s41467-022-32521-8
38. Naggara O, Raymond J, Guilbert F, et al. Analysis by categorizing or dichotomizing continuous variables is inadvisable: an example from the natural history of unruptured aneurysms. AJNR Am J Neuroradiol. 2011;32(3):437–440. doi:10.3174/ajnr.A2425
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Lactate Dehydrogenase and Alkaline Phosphatase as Predictive Biomarkers in the Prognosis of Hepatocellular Carcinoma and Development of a New Nomogram
Su K, Huang W, Li X, Xu K, Gu T, Liu Y, Song J, Qian K, Xu Y, Zeng H, Yang Y, Guo L, Han Y
Journal of Hepatocellular Carcinoma 2023, 10:69-79
Published Date: 14 January 2023
Nomogram Based on Preoperative Fibrinogen and Systemic Immune-Inflammation Index Predicting Recurrence and Prognosis of Patients with Borrmann Type III Advanced Gastric Cancer
Wang H, Yin X, Ma K, Wang Y, Fang T, Zhang Y, Xue Y
Journal of Inflammation Research 2023, 16:1059-1075
Published Date: 12 March 2023
Prognostic Model of D2 Radical Gastrectomy Combined with Neoadjuvant Chemotherapy for Gastric Cancer
Wang G, Tan Y, Jiang Y, Liu J, Su Y, Sun Z, Liu B
Risk Management and Healthcare Policy 2023, 16:1259-1271
Published Date: 10 July 2023
Development of Prognostic Nomogram Based on Lipid Metabolic Markers and Lactate Dehydrogenase in Non-Metastatic Nasopharyngeal Carcinoma
Huang R, Chen K, Jiang Y, Li L, Zhu X
Journal of Inflammation Research 2023, 16:3093-3107
Published Date: 24 July 2023
A Nomogram Based on Clinicopathological Characteristics for Estimating the Risk of Brain Metastasis from Advanced Gastric Cancer: A Multi-Center Retrospective Clinical Study
Zhang L, Yu Z, Zhang Y, Wang H, Cheng J, Shi C
Therapeutics and Clinical Risk Management 2024, 20:391-404
Published Date: 24 June 2024