Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 18
A Cross-Sectional Study of the Relationship Between Disease Activity and Fatigue in Rheumatoid Arthritis Patients at King Abdulaziz University Hospital, Saudi Arabia
Authors Bawazir Y ![]() , Mustafa MA
, Mustafa MA ![]()
Received 23 November 2025
Accepted for publication 17 February 2026
Published 5 March 2026 Volume 2026:18 583296
DOI https://doi.org/10.2147/OARRR.S583296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Yasser M Bawazir,1 Mohammad A Mustafa2
1Department of Medicine, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia; 2Department of Medicine, University of Jeddah, Jeddah, Kingdom of Saudi Arabia
Correspondence: Yasser M Bawazir, Department of Medicine, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia, Email [email protected]
Background: Fatigue is one of the most prevalent and disabling symptoms in patients with rheumatoid arthritis (RA), yet its relationship with disease activity remains complex and underexplored in many populations.
Objective: To evaluate the association between disease activity and fatigue in RA patients at King Abdulaziz University Hospital using validated clinical measures.
Methods: A cross-sectional study was conducted among 253 RA patients fulfilling the ACR/EULAR 2010 classification criteria. Disease activity was assessed using the Clinical Disease Activity Index (CDAI), and fatigue was measured with the Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) scale. Relationships between fatigue (FACIT-F scores) and CDAI were examined using Pearson correlation with continuous CDAI scores. Descriptive statistics (mean ± SD) of FACIT-F scores across CDAI categories were provided for illustration. Multivariate linear regression adjusted for age, sex, disease duration, body mass index, employment status, serological markers, and treatment type. ANOVA was applied to assess differences in mean FACIT-F scores across disease activity categories. Statistical significance was set at p < 0.05.
Results: Fatigue was reported by 80% of patients, with 10% experiencing severe fatigue (FACIT-F ≤ 13). Mean FACIT-F scores decreased as disease activity increased: remission 40.1 ± 8.2, low disease activity 35.7 ± 10.4, moderate disease activity 25.6 ± 9.8, and high disease activity 15.4 ± 7.3 (p < 0.001, ANOVA). Pearson correlation demonstrated a strong inverse relationship between CDAI and FACIT-F scores (r = – 0.68, 95% CI: – 0.83 to – 0.45 in the high disease activity group). Multivariate analysis confirmed that disease activity remained a key determinant of fatigue after adjusting for potential confounders, with female sex, obesity, and longer disease duration also independently associated with lower FACIT-F scores.
Conclusion: Fatigue in RA is strongly associated with disease activity but persists in patients with well-controlled inflammation, reflecting multifactorial origins. Routine fatigue assessment and holistic management strategies addressing both inflammatory and non-inflammatory contributors are essential to improve patient quality of life and treatment outcomes.
Keywords: rheumatoid arthritis, fatigue, disease activity, CDAI, FACIT-F, multivariate analysis
Background
Rheumatoid arthritis (RA) is a chronic autoimmune disorder characterized by persistent synovial inflammation, leading to joint damage, pain, and functional disability.1 Affecting approximately 1% of the global population, RA predominantly targets the small joints of the hands and feet, though larger joints can also be involved.2 The disease is systemic, with extra-articular manifestations such as cardiovascular, pulmonary, and dermatologic complications contributing significantly to morbidity and mortality. The progressive nature of RA and its impact on patients’ quality of life make it a significant public health concern.3 Despite advances in understanding the pathophysiology of RA and the introduction of disease-modifying therapies, managing the disease’s physical and psychological symptoms remains a considerable challenge.4,5
One of the most debilitating symptoms experienced by patients with RA is fatigue, which affects nearly 40–80% of individuals with the disease. Fatigue in RA is multidimensional, encompassing physical, cognitive, and emotional components, and it often does not correlate directly with disease activity or the severity of joint damage.6,7 The unpredictability of fatigue, along with its chronic nature, complicates its management and severely impacts patients’ quality of life, work productivity, and social functioning.8 Despite the high prevalence of fatigue between 40–80% in RA populations, the underlying mechanisms are not fully understood, and there is no standardized approach to its assessment and treatment.9–12
Fatigue in RA can be influenced by a wide range of factors, including disease activity, pain, depression, sleep disturbances, and medication side effects. These factors may act independently or interactively, exacerbating the patient’s sense of fatigue.13 Disease activity itself, typically measured using composite indices such as the Disease Activity Score (DAS) or the Clinical Disease Activity Index (CDAI), is often considered a primary driver of fatigue.14 However, studies have shown that fatigue can persist even in patients with well-controlled disease, suggesting that other, non-inflammatory mechanisms may contribute to this symptom.15–17 Understanding the complex relationship between disease activity and fatigue is critical for developing effective management strategies aimed at improving patient outcomes.18
King Abdulaziz University Hospital in Saudi Arabia, a tertiary care center in Saudi Arabia, provides specialized care to a large cohort of RA patients. This setting offers a unique opportunity to assess the relationship between fatigue and disease activity in a Middle Eastern population, where sociocultural factors may influence the experience and reporting of fatigue. While numerous studies have explored fatigue in RA in Western populations,19,20 there is a relative paucity of research in the Middle East, particularly in Saudi Arabia. Given the potential differences in patient perceptions of fatigue, disease burden, and healthcare access in this region, it is essential to investigate these aspects in local contexts.
The present study aims to assess fatigue and its association with disease activity in RA patients at King Abdulaziz University Hospital. Specifically, it seeks to explore the prevalence and severity of fatigue among RA patients, identify factors that contribute to fatigue, and evaluate the correlation between fatigue and standard measures of disease activity. By doing so, this study will contribute to a better understanding of how fatigue manifests in RA patients in this setting and may inform tailored interventions to address this often-overlooked aspect of RA management.
Materials and Methods
Study Design, Setting, and Period
This cross-sectional study was conducted at King Abdulaziz University Hospital to assess the relationship between fatigue and disease activity in patients with rheumatoid arthritis (RA). King Abdulaziz University Hospital is a major tertiary referral center in Jeddah, Saudi Arabia, providing specialist rheumatology services to patients from the western and central regions of the country. The rheumatology clinic receives referrals from primary and secondary care facilities, resulting in a cohort that reflects a diverse RA population with varying disease severities and sociodemographic backgrounds.
Data collection occurred over several months, with each participant assessed at a single point in time, consistent with the cross-sectional study design. Patients were eligible if they had a confirmed clinical diagnosis of RA and also fulfilled the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) 2010 classification criteria.21 All participants were aged 18 years or older and provided written informed consent prior to participation.
Study Population, Sampling, and Sample Size
Patients were recruited consecutively from the Rheumatology Clinic at King Abdulaziz University Hospital. Eligible participants were adults with a confirmed clinical diagnosis of rheumatoid arthritis (RA) who also fulfilled the ACR/EULAR 2010 classification criteria. Patients with comorbidities that could interfere with the assessment of fatigue (eg, severe anemia, uncontrolled thyroid disease, or major psychiatric disorders) were excluded. Written informed consent was obtained from all participants prior to enrollment.
The sample size calculation was based on detecting a moderate correlation between fatigue and disease activity (effect size r = 0.30), guided by prior studies examining this relationship in RA populations. Using a two-tailed significance level of 0.05 and 80% power, the minimum required sample size was determined. Consecutive recruitment continued until this target was met, resulting in the final study cohort.
Data Collection
Participants underwent a comprehensive clinical evaluation by a rheumatologist to assess disease activity using the Clinical Disease Activity Index (CDAI). Immediately following the clinical evaluation, trained research assistants administered the Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) questionnaire, version 4,22 to assess fatigue levels 22. The FACIT-F is a validated instrument for evaluating fatigue in chronic illnesses, including RA. It consists of 13 items scored on a 0–4 scale, where higher scores indicate less fatigue. The total score is calculated by summing the item responses, multiplying by 13, and dividing by the number of items answered, with higher scores reflecting better functioning and lower fatigue severity.
Serological and laboratory data, including anti-cyclic citrullinated peptide (anti-CCP) and antinuclear antibody (ANA) status, were retrospectively retrieved from patient medical records. Blood samples were collected during the same clinical visit or within a short period relative to the CDAI and FACIT-F assessments to maintain temporal relevance. ANA status was determined using indirect immunofluorescence (IIF) on HEp-2 cells, according to standard hospital laboratory protocols. Missing data were minimal (<5%) and were handled using complete case analysis, excluding only those participants with missing values from specific analyses.
Clinical Disease Activity Index (CDAI)
RA disease activity was assessed using the Clinical Disease Activity Index (CDAI), which includes counts of tender and swollen joints (28 joints), patient global assessment, and physician global assessment. CDAI scores range from 0 to 76 and were categorized as follows: remission (<2.8), low disease activity (2.8–10), moderate disease activity (11–22), and high disease activity (>22). In all analyses, the term “disease activity” refers specifically to CDAI scores.23 Although the Disease Activity Score using 28 joint counts (DAS28) is a widely used measure of RA disease activity, this study focused on the Clinical Disease Activity Index (CDAI) as the primary measure. Therefore, DAS28 was not analyzed in relation to fatigue, and all analyses presented are based on CDAI scores.
FACIT-F Fatigue Categorization and Measurement
Fatigue was assessed using the 13-item Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) scale, which has been validated and shown to be reliable in Arabic-speaking populations.24,25 Based on FACIT-F scores, patients were categorized into four levels of fatigue: severe (0–13), moderate (14–26), mild (27–39), and no fatigue (40–52). This stratification enabled a detailed assessment of fatigue severity and facilitated analysis of its relationship with rheumatoid arthritis disease activity. This scoring classification has been applied in prior studies utilizing the FACIT-F instrument.24,26,27
Data Analysis
Normality of continuous variables was assessed using the Shapiro–Wilk test. Differences in FACIT-F scores across CDAI categories (remission, low, moderate, and high disease activity) were analyzed using one-way analysis of variance (ANOVA), followed by post-hoc comparisons with Bonferroni correction to identify significant group differences. Pearson correlation was used to evaluate the relationship between continuous CDAI scores and FACIT-F scores.
To account for potential confounding factors, a multiple linear regression analysis was conducted with FACIT-F score as the dependent variable and CDAI (continuous), age, gender, body mass index (BMI), disease duration, employment status, biologic therapy, and serological markers (anti-CCP and ANA) as independent variables. Multicollinearity was assessed using variance inflation factors (VIF), and residuals were examined to confirm model assumptions. All statistical tests were two-tailed, with a p-value < 0.05 considered statistically significant. Analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA).
Results
A total of 253 patients met the inclusion criteria and were enrolled in the study. The cohort had a mean age of 55.3 years, and 60% were female. Most patients were married and had children, and a substantial proportion were unemployed. Obesity was common in the study population, and serological markers showed moderate positivity for CCP and ANA. Disease duration varied widely, with over one-third of patients living with RA for more than six years. In our cohort, 38.7% of patients were positive for anti-CCP antibodies, which is lower than rates reported in some international RA cohorts. This difference may reflect population-specific characteristics, variations in disease duration at diagnosis, referral patterns to the tertiary care center, or differences in assay methods. ANA positivity was observed in 35.2% of patients. These serological findings were included as independent variables in the multivariate regression analysis. Of the 253 patients, 72 (28.5%) were undergoing biologic or JAK inhibitor therapy, while 173 (68.4%) were treated with conventional synthetic DMARDs (csDMARDs) (Table 1). Medications reported in Table 1 include those available and prescribed in the study setting. Abatacept and tocilizumab were not used by patients as these agents are not routinely available locally.
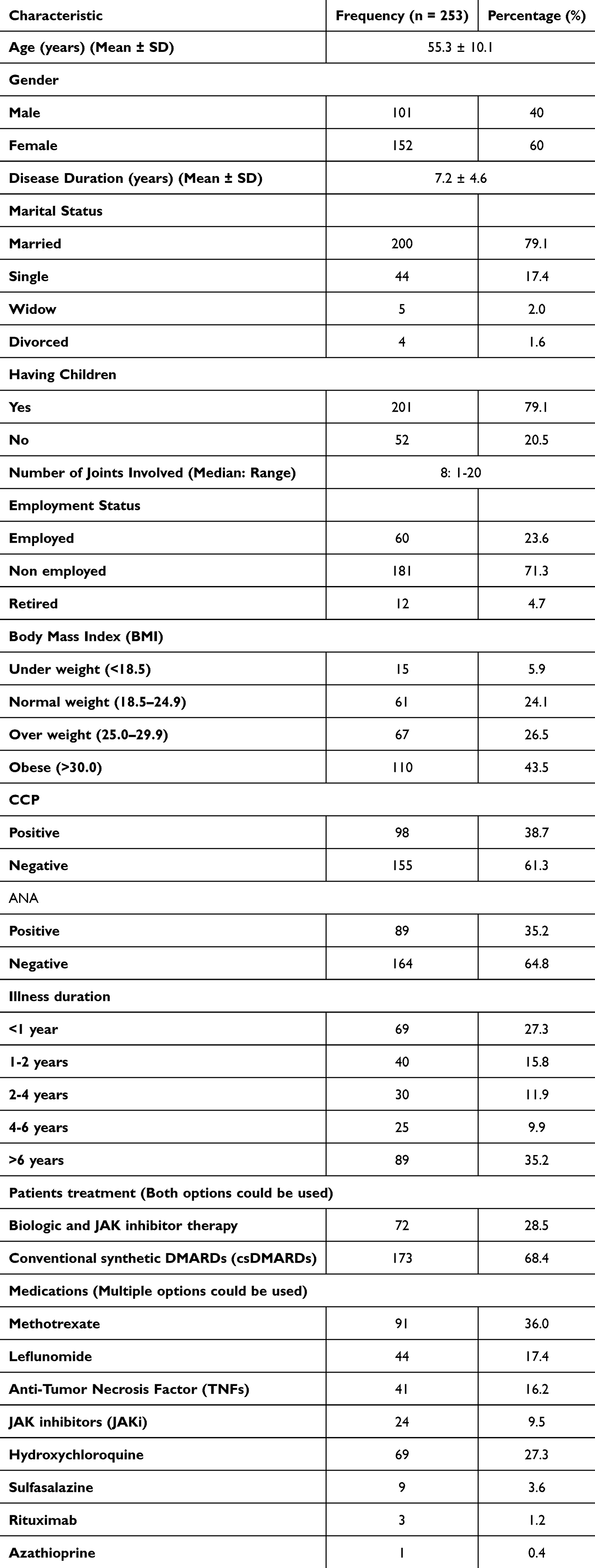 |
Table 1 Demographic and Clinical Characteristics of RA Patients |
Analysis of disease activity using the Clinical Disease Activity Index (CDAI) showed that the majority of patients had low to moderate disease activity, with smaller proportions in remission or high disease activity. Fatigue levels, as measured by the FACIT-F, were inversely associated with disease activity. Patients in remission exhibited the lowest fatigue, while those with high disease activity experienced the most severe fatigue. Moderate disease activity was associated with substantial fatigue, and even some patients with low disease activity continued to report moderate fatigue. Among the 253 RA patients, fatigue was highly prevalent, with 80% reporting at least mild fatigue. Higher disease activity, as measured by CDAI, was associated with greater fatigue severity. Pearson correlation analysis showed moderate-to-strong inverse relationships between CDAI and FACIT-F scores across disease activity categories. In multivariate regression, CDAI, female sex, and obesity were independently associated with fatigue severity. Serological markers (CCP and ANA) and biologic therapy use were not significant predictors (Table 2).
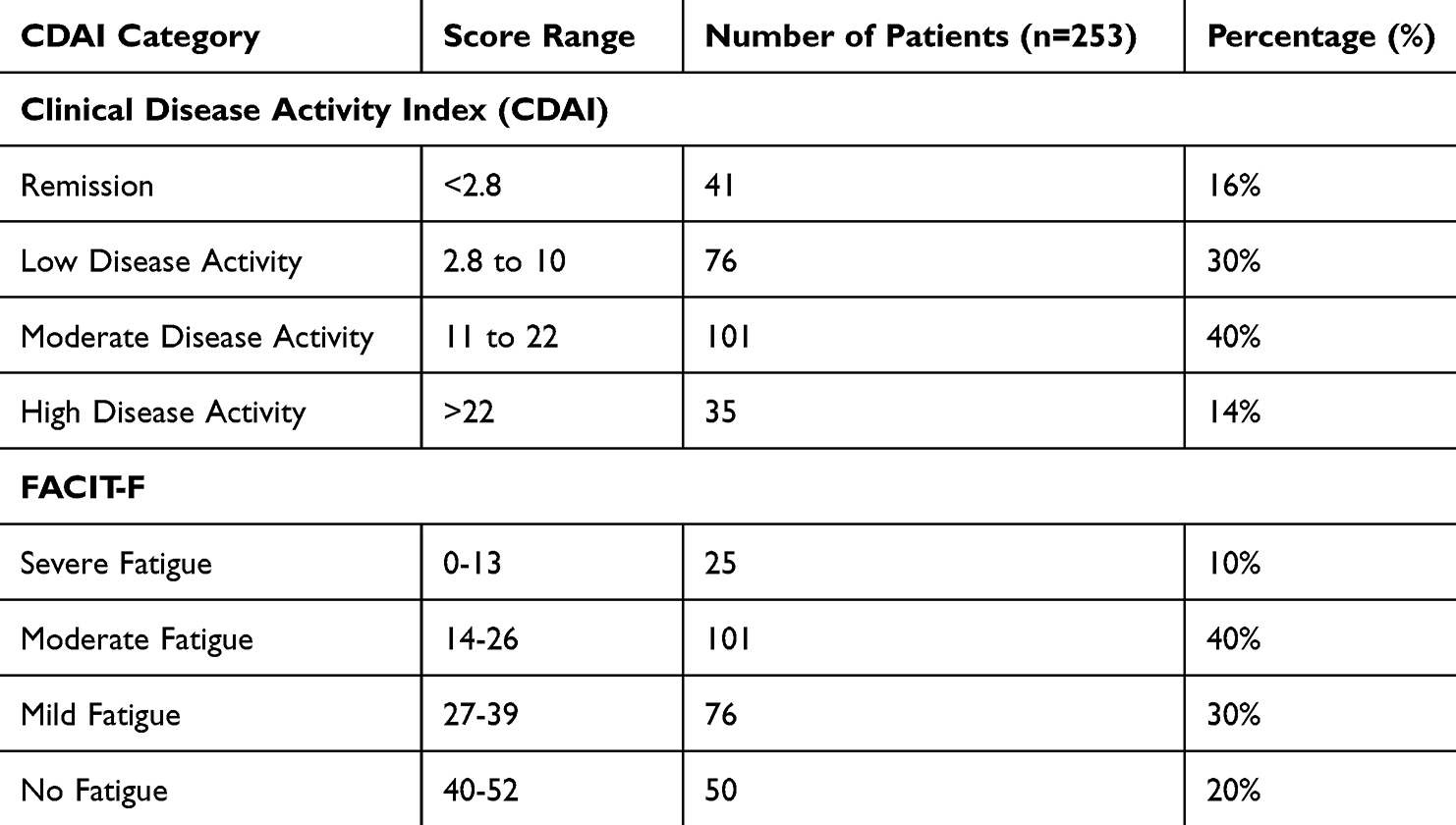 |
Table 2 Distribution of CDAI and FACIT-F Scores |
FACIT-F scores were negatively correlated with continuous CDAI scores, indicating that higher disease activity was associated with greater fatigue (r = –0.56, 95% CI: –0.67 to –0.43, p < 0.001). For descriptive purposes, mean ± SD FACIT-F scores across CDAI categories were as follows: remission 40.1 ± 8.2, low disease activity 35.7 ± 10.4, moderate disease activity 25.6 ± 9.8, and high disease activity 15.4 ± 7.3. These results demonstrate that fatigue severity increases with increasing disease activity (Table 3) (Figure 1).
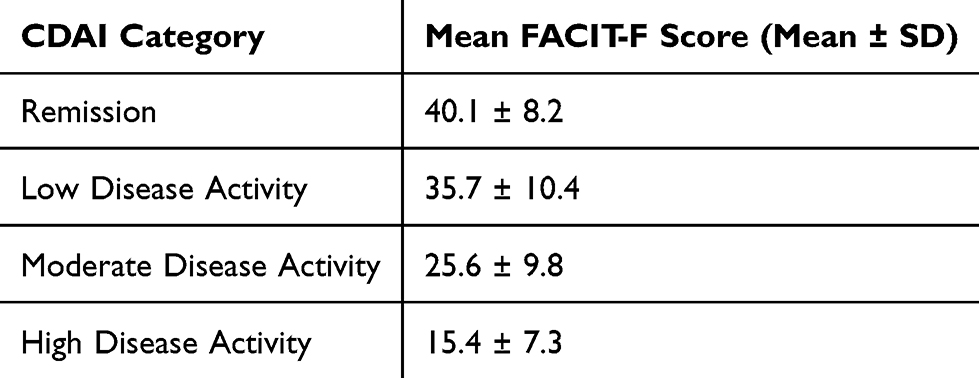 |
Table 3 Correlation Between Continuous CDAI Scores and FACIT-F Scores |
 |
Figure 1 Mean FACIT-F scores across CDAI categories in RA patients. Error bars represent standard deviations (Mean ± SD). Abbreviations: CDAI, Clinical Disease Activity Index; FACIT-F, Functional Assessment of Chronic Illness Therapy–Fatigue. |
In the multivariate linear regression analysis (Table 4), CDAI score, as a measure of disease activity, was a strong independent predictor of fatigue (FACIT-F score, β = –0.39, p < 0.001). In addition, female sex (β = –0.13, p = 0.021), obesity (β = –0.16, p = 0.008), and longer disease duration (β = –0.11, p = 0.050) were also independently associated with lower FACIT-F scores.
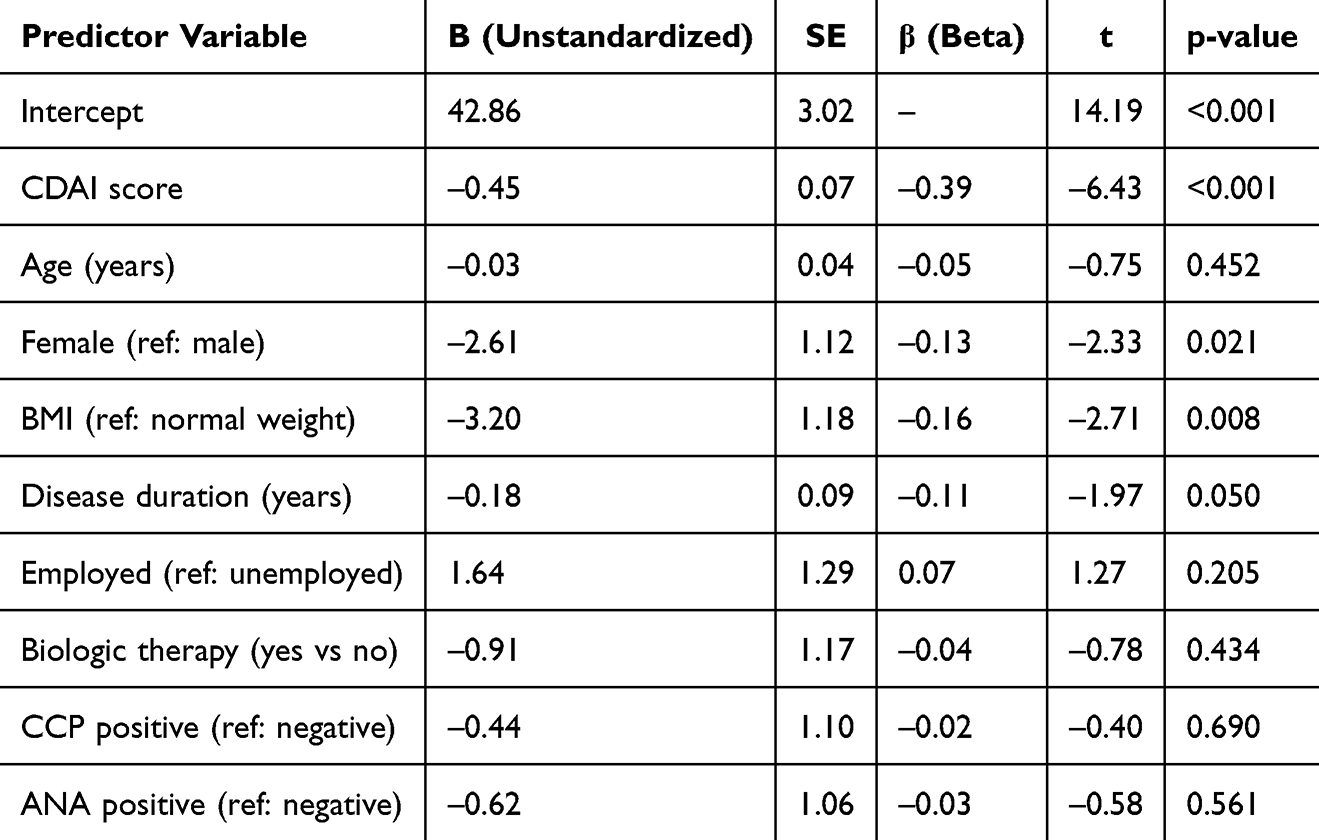 |
Table 4 Multiple Linear Regression Analysis of Predictors of Fatigue (FACIT-F Score) |
Discussion
This study investigated the relationship between disease activity and fatigue in patients with rheumatoid arthritis (RA) using the Clinical Disease Activity Index (CDAI) and the Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) scale. Our cohort exhibited a lower anti-CCP positivity rate (38.7%) than commonly reported in RA populations, where rates typically exceed 50–60%. This difference may reflect population-specific characteristics, earlier or milder disease presentations, selective referral patterns, or assay variability. Nevertheless, CDAI remained a strong determinant of fatigue, suggesting that inflammatory activity is an important contributor to fatigue regardless of serological status.
Overall, 80% of participants reported fatigue, with 10% classified as severe (FACIT-F ≤ 13), consistent with previous studies reporting prevalence estimates between 42% and 90%, highlighting fatigue as a core and disabling symptom of RA that often exceeds joint pain in impact on quality of life.28,29 Our data show that mean FACIT-F scores differed significantly across CDAI categories (ANOVA, p < 0.001), with patients in clinical remission scoring highest (40.1 ± 8.2) and those with high disease activity scoring lowest (15.4 ± 7.3) (Figure 1, Table 3). These findings indicate that higher disease activity is associated with greater fatigue severity, aligning with prior reports of moderate-to-strong inverse relationships between inflammatory activity and fatigue severity.11,19
However, fatigue in RA is a multidimensional construct influenced not only by inflammation but also by psychosocial, psychological, and treatment-related factors.15,30 The persistence of fatigue among patients with low CDAI scores underscores the role of non-inflammatory contributors, including female sex, obesity, longer disease duration, depression, sleep disturbances, physical deconditioning, comorbidities, and treatment-related effects (eg, glucocorticoids, biologics, JAK inhibitors, and recent therapy adjustments).12,13,31 In our multivariate analysis, female sex, obesity, and longer disease duration remained independently associated with lower FACIT-F scores, reinforcing the multifactorial etiology of fatigue. These results do not contradict our study hypotheses but rather emphasize that fatigue cannot be attributed solely to disease activity.
The clinical implications are significant. Patients with high disease activity exhibited profound fatigue (FACIT-F 15.4), which is associated with marked impairments in daily functioning, occupational performance, and social engagement.6,26 While controlling inflammation is essential, it may not fully restore quality of life without addressing fatigue directly through comprehensive strategies, including cognitive-behavioral interventions, structured exercise programs, and psychosocial support.6,8,18,32
Conclusion
Fatigue in patients with rheumatoid arthritis (RA) is closely associated with disease activity, yet it persists in a substantial proportion of patients with well-controlled inflammation. Female sex, longer disease duration, and obesity are additional independent contributors to fatigue. Comprehensive RA management should include routine assessment of fatigue and implement interventions targeting both inflammatory and non-inflammatory factors to enhance patient quality of life and overall functional outcomes.
Abbreviations
RA, Rheumatoid Arthritis; CDAI,Clinical Disease Activity Index; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue; DAS, Disease Activity Score; ACR/EULAR, American College of Rheumatology/European League Against Rheumatism; TNF, Anti-Tumor Necrosis Factor; JAKi, Janus Kinase inhibitors.
Data Sharing Statement
The datasets produced and/or analyzed during this study are not publicly accessible but can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study received ethical approval from the Unit of Biomedical Ethics of the King Abdulaziz University, Jeddah, Saudi Arabia (Reference Number: 744-23). All participants provided written informed consent prior to enrollment. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Acknowledgment
The authors thank Dr. Samer Abuzerr for helping with data analysis, article screening, data extraction, and manuscript review. They also extend their gratitude to King Abdulaziz University for supplying the analysis program.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval for the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies. The article processing charges were covered by King Abdulaziz University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jahid M, Khan KU, Ahmed RS, Ahmed RS. Overview of rheumatoid arthritis and scientific understanding of the disease. Mediterranean J Rheumatol. 2023;34(3):284–10. doi:10.31138/mjr.20230801.oo
2. Fazal SA, Khan M, Nishi SE, et al. A clinical update and global economic burden of rheumatoid arthritis. Endocrine Metabo Disord. 2018;18(2):98–109.
3. Radu A-F, Bungau SG. Management of rheumatoid arthritis: an overview. Cells. 2021;10(11):2857. doi:10.3390/cells10112857
4. Davis JM III. Rheumatoid arthritis: a severe disease that preventive approaches would greatly benefit. Clin Ther. 2019;41(7):1240–1245. doi:10.1016/j.clinthera.2019.04.026
5. Smolen JS, Landewé RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheumatic Dise. 2020;79(6):685–699. doi:10.1136/annrheumdis-2019-216655
6. Dar WR, Mir IA, Siddiq S, Nadeem M, Singh G. The assessment of fatigue in rheumatoid arthritis patients and its impact on their quality of life. Clin Prac. 2022;12(4):591–598. doi:10.3390/clinpract12040062
7. Versteeg GA, Ten Klooster PM, van de Laar MAFJ. Fatigue is associated with disease activity in some, but not all, patients living with rheumatoid arthritis: disentangling “between-person” and “within-person” associations. BMC Rheumatol. 2022;6(1):1–9. doi:10.1186/s41927-021-00230-2
8. Katz P. Fatigue in rheumatoid arthritis. Curr Rheumatol Rep. 2017;19(5):1–10. doi:10.1007/s11926-017-0649-5
9. Zampeli E, Vlachoyiannopoulos PG, Tzioufas AG. Treatment of rheumatoid arthritis: unraveling the conundrum. J Autoimmun. 2015;65:1–18. doi:10.1016/j.jaut.2015.10.003
10. Nikolaus S, Bode C, Taal E, van de Laar MA. Fatigue and factors related to fatigue in rheumatoid arthritis: a systematic review. Arthritis Care Res. 2013;65(7):1128–1146. doi:10.1002/acr.21949
11. Pollard L, Choy E, Gonzalez J, Khoshaba B, Scott D. Fatigue in rheumatoid arthritis reflects pain, not disease activity. Rheumatology. 2006;45(7):885–889. doi:10.1093/rheumatology/kel021
12. Chauffier K, Salliot C, Berenbaum F, Sellam J. Effect of biotherapies on fatigue in rheumatoid arthritis: a systematic review of the literature and meta-analysis. Rheumatology. 2012;51(1):60–68. doi:10.1093/rheumatology/ker162
13. McInnis O. Factors Influencing Fatigue and Fatigue-Related Illnesses. Carleton University; 2011.
14. Nikiphorou E, Radner H, Chatzidionysiou K, et al. Patient global assessment in measuring disease activity in rheumatoid arthritis: a review of the literature. Arthritis Res Therapy. 2016;18(1):1–11. doi:10.1186/s13075-016-1151-6
15. Louati K, Berenbaum F. Fatigue in chronic inflammation - a link to pain pathways. Arthritis Res Therapy. 2015;17(1):1–10. doi:10.1186/s13075-015-0784-1
16. McGing JJ, Radford SJ, Francis ST, Serres S, Greenhaff PL, Moran GW. The aetiology of fatigue in inflammatory bowel disease and potential therapeutic management strategies. Aliment Pharmacol Ther. 2021;54(4):368–387. doi:10.1111/apt.16465
17. Boyden SD, Hossain IN, Wohlfahrt A, Lee YC. Non-inflammatory causes of pain in patients with rheumatoid arthritis. Curr Rheumatol Rep. 2016;18(6):1–8. doi:10.1007/s11926-016-0581-0
18. O’Boyle S, Nacul L, Nacul FE, et al. A natural history of disease framework for improving the prevention, management, and research on post-viral fatigue syndrome and other forms of myalgic encephalomyelitis/chronic fatigue syndrome. Front Med. 2022;8:688159. doi:10.3389/fmed.2021.688159
19. Rupp I, Boshuizen HC, Jacobi CE, Dinant HJ, van den Bos GA. Impact of fatigue on health‐related quality of life in rheumatoid arthritis. Arthritis Care Res. 2004;51(4):578–585. doi:10.1002/art.20539
20. Lihavainen K. Mobility limitation, balance impairment and musculoskeletal pain among people aged≥ 75 years: a study with a comprehensive geriatric intervention. Stud Sport Phys Educ Health. 2012;177.
21. Kasturi S, Goldstein BL, Malspeis S, Karlson EW, Costenbader KH. Comparison of the 1987 American college of rheumatology and the 2010 American college of rheumatology/European league against rheumatism criteria for classification of rheumatoid arthritis in the nurses’ health study cohorts. Rheumatol Int. 2014;34(3):407–411. doi:10.1007/s00296-013-2865-2
22. Cella D, Lenderking WR, Chongpinitchai P, et al. Functional assessment of chronic illness therapy-fatigue is a reliable and valid measure in patients with active ankylosing spondylitis. J Patient-Reported Outcomes. 2022;6(1):100. doi:10.1186/s41687-022-00508-0
23. Aletaha D, Smolen JS. The simplified disease activity index (SDAI) and clinical disease activity index (CDAI) to monitor patients in standard clinical care. Best Prac Res Clin Rheumatol. 2007;21(4):663–675. doi:10.1016/j.berh.2007.02.004
24. Cella D, Yount S, Sorensen M, Chartash E, Sengupta N, Grober J. Validation of the functional assessment of chronic illness therapy fatigue scale relative to other instrumentation in patients with rheumatoid arthritis. J Rheumatol. 2005;32(5):811–819.
25. Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E. Measuring fatigue and other anemia-related symptoms with the functional assessment of cancer therapy (FACT) measurement system. J Pain Sympt Manage. 1997;13(2):63–74. doi:10.1016/S0885-3924(96)00274-6
26. Tinsley A, Macklin E, Korzenik J, Sands B. Validation of the functional assessment of chronic illness therapy‐fatigue (FACIT‐F) in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2011;34(11‐12):1328–1336. doi:10.1111/j.1365-2036.2011.04871.x
27. Alvarez Santana R, Garcia D, Santana Peralta J, et al. AB0216 fatigue assessment in rheumatoid arthritis, santo domingo, dominican republic. BMJ Publishing Group Ltd Euro League Against Rheumatism. 2022.
28. Matcham F, Ali S, Hotopf M, Chalder T. Psychological correlates of fatigue in rheumatoid arthritis: a systematic review. Clin Psycholog Rev. 2015;39:16–29. doi:10.1016/j.cpr.2015.03.004
29. Davies K, Dures E, Ng W-F. Fatigue in inflammatory rheumatic diseases: current knowledge and areas for future research. Nat RevRheumatol. 2021;17(11):651–664. doi:10.1038/s41584-021-00692-1
30. Zampeli E, Protogerou A, Stamatelopoulos K, et al. Predictors of new atherosclerotic carotid plaque development in patients with rheumatoid arthritis: a longitudinal study. Arthritis Res Therapy. 2012;14(2):1–10. doi:10.1186/ar3757
31. Wolfe F, Häuser W, Hassett AL, Katz RS, Walitt BT. The development of fibromyalgia – i: examination of rates and predictors in patients with rheumatoid arthritis (RA). Pain®. 2011;152(2):291–299. doi:10.1016/j.pain.2010.09.027
32. Hewlett S, Chalder T, Choy E, et al. Fatigue in Rheumatoid Arthritis: Time for a Conceptual Model. Oxford University Press; 2011:1004–1006.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adiponectin and Leptin as Biomarkers of Disease Activity and Metabolic Disorders in Rheumatoid Arthritis Patients
Targońska-Stępniak B, Grzechnik K
Journal of Inflammation Research 2022, 15:5845-5855
Published Date: 13 October 2022
Correlation Between Total Bilirubin, Total Bilirubin/Albumin Ratio with Disease Activity in Patients with Rheumatoid Arthritis
Zhang H, Yang G, Jiang R, Feng D, Li Y, Chen Y, Yuan G
International Journal of General Medicine 2023, 16:273-280
Published Date: 24 January 2023
Risk Factors Analysis for the Development of Hypocomplementemia in Rheumatoid Arthritis Patients: A Single-Center Retrospective Study
Chen Y, Xiao C, Liao Y, Tan L
International Journal of General Medicine 2023, 16:3583-3592
Published Date: 18 August 2023
Is Serum Uric Acid Level Associated with Disease Activity in Rheumatoid Arthritis Patients
Alkhudir D, Al-Herz A, Saleh K, Alawadhi A, Al-Kandari W, Hasan E, Mokaddem K, Ghanem A, Bartella YA, Hussain M, AlHadhood N, Ali Y, Nahar E, Alenizi A, Aldei A, Abutiban F, Hayat S, Behbehani H, Baron F, Alhajeri H, Alkadi A, Alsaber A
Open Access Rheumatology: Research and Reviews 2023, 15:223-230
Published Date: 14 November 2023
A Comparative Analysis of Cognitive Deficits in Rheumatoid Arthritis and Fibromyalgia: Impact of Symptoms Severity and Its Clinical Implications
Galvez-Sánchez CM, Duschek S, Reyes del Paso GA
Psychology Research and Behavior Management 2024, 17:1399-1415
Published Date: 28 March 2024