Back to Journals » Journal of Pain Research » Volume 19
A Comparative Analysis of Ultrasound versus Fluoroscopy-Guided Transforaminal Endoscopic Lumbar Discectomy: Protocol for a Randomized Clinical Trial Targeting Lumbar Disc Herniation
Received 24 October 2025
Accepted for publication 7 March 2026
Published 16 March 2026 Volume 2026:19 572811
DOI https://doi.org/10.2147/JPR.S572811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Chao Shang, Zixu Lv
Department of Pain Management, Zibo First Hospital, Zibo, Shandong, People’s Republic of China
Correspondence: Zixu Lv, Department of Pain Management, Zibo First Hospital, Zibo, Shandong, People’s Republic of China, Email [email protected]
Abstract: Lumbar disc herniation (LDH) is a prevalent cause of chronic disability that often necessitates surgical intervention when conservative treatments fail. This study aims to compare the clinical efficacy and safety of ultrasound-guided transforaminal endoscopic lumbar discectomy (UG-TELD) against fluoroscopy-guided transforaminal endoscopic lumbar discectomy (FG-TELD) in a single-center, parallel, block-randomized trial involving 80 adult patients aged 18 to 75 years with MRI-confirmed radiculopathy unresponsive to at least six weeks of conservative management. Participants will be randomly assigned to receive either UG-TELD or FG-TELD, adhering to strict exclusion criteria such as prior spinal surgeries or significant neurological deficits. Primary efficacy endpoints include a 50% reduction in leg pain measured by the Visual Analog Scale (VAS) at three months, alongside a 40% improvement in the Oswestry Disability Index (ODI) or a score below 20% at six months. Safety will be evaluated through the incidence of major complications (Clavien-Dindo grade III or higher) within 90 days postoperatively and the reoperation rate after one year. Operational metrics like puncture time, fluoroscopy exposure, and assessments of healthcare provider well-being through burnout evaluations and procedural satisfaction surveys will also be analyzed. This pioneering randomized controlled trial seeks to establish UG-TELD as a viable, radiation-free alternative for LDH treatment, highlighting the need for advancements in surgical techniques to enhance safety and efficacy. Future multicenter studies are warranted to further validate these findings and optimize surgical protocols in spinal surgery.
Keywords: ultrasound-guided TELD, UG-TELD, lumbar disc herniation, LDH, study protocol, randomized controlled trial
Introduction
Lumbar disc herniation (LDH) remains a prevalent and debilitating spinal disorder, accounting for a substantial proportion of chronic low back pain cases worldwide.1,2 The condition not only imposes severe physical limitations on patients but also generates significant socioeconomic burdens due to lost productivity and prolonged healthcare utilization. While conservative management serves as the first-line approach, a considerable subset of patients eventually requires surgical intervention when neurological deficits or refractory pain persists.3 Among minimally invasive techniques, transforaminal endoscopic lumbar discectomy (TELD) has gained prominence due to its muscle-sparing advantages and rapid recovery profile.4 However, the conventional reliance on C-arm fluoroscopy guidance introduces critical limitations, including cumulative radiation exposure to both patients and surgical teams, procedural inefficiencies from repeated imaging, and substantial equipment costs.5,6 These challenges underscore the urgent need to explore alternative guidance modalities that can maintain surgical efficacy while addressing these systemic shortcomings.
Recent advancements in imaging technology have positioned ultrasound as a promising alternative for various spinal interventions.7 A growing body of evidence demonstrates its capability to provide real-time visualization of critical anatomical structures without ionizing radiation, particularly in procedures requiring needle placement or soft tissue differentiation.8–10Several studies have reported successful applications of ultrasound guidance in epidural injections, facet joint interventions, and even percutaneous pedicle screw placement, consistently showing reduced radiation exposure and improved workflow efficiency compared to fluoroscopic methods.11–14 However, the literature reveals a conspicuous gap regarding its application in full endoscopic spinal surgeries, particularly for TELD procedures.15 While preliminary reports suggest theoretical advantages, rigorous comparative studies evaluating both clinical outcomes and operational metrics remain scarce. This knowledge gap persists despite the increasing global emphasis on value-based surgical care that prioritizes patient safety, cost-effectiveness, and healthcare provider well-being.
The current research landscape exhibits several critical limitations that hinder the adoption of ultrasound guidance in endoscopic spine surgery.16 Most existing studies focus narrowly on technical feasibility or radiation reduction, neglecting comprehensive assessments of patient-reported outcomes, long-term quality-of-life measures, and the often-overlooked impact on surgical team dynamics.17 These omissions create significant barriers to evidence-based decision-making for healthcare administrators and surgeons alike. Additionally, the lack of standardized protocols for ultrasound-guided TELD contributes to inconsistent implementation across institutions, while concerns about the learning curve continue to deter widespread adoption. These multifaceted research gaps collectively highlight the necessity for a holistic investigation that transcends traditional efficacy measures to encompass the broader ecosystem of spinal care delivery.
To address these gaps, we will conduct a randomized controlled trial comparing ultrasound-guided versus fluoroscopy-guided transforaminal endoscopic lumbar discectomy (TELD) for single-level lumbar disc herniation.
Materials and Methods
Aims of the Study
Primary Objective
To compare the clinical efficacy and operational efficiency of ultrasound-guided transforaminal endoscopic lumbar discectomy (UG-TELD) versus fluoroscopy-guided TELD (FG-TELD) for single-level lumbar disc herniation, with specific focus on validating two critical technical benchmarks: the first-pass needle placement success rate and puncture time efficiency measured from skin penetration to final needle positioning. Concurrently, the study implements a multidimensional outcome assessment framework that quantifies patient-centered metrics through serial evaluation of pain intensity (VAS), functional disability (ODI), and quality-of-life (SF-36), while systematically documenting provider-focused outcomes including occupational burnout severity via Maslach Burnout Inventory and procedural satisfaction levels among operating teams.
Secondary Objective
To standardize an ultrasound-guided procedural workflow for transforaminal endoscopic lumbar discectomy (TELD), integrating two critical phases: preoperative static mapping for anatomical landmark localization and intraoperative dynamic navigation for real-time instrument guidance. This protocol utilizes transverse/longitudinal ultrasound views to demarcate skin entry points and trajectory paths relative to the superior articular process (SAP) preoperatively, followed by continuous biplane monitoring (sagittal/transverse) during needle advancement.
Study Design
This study adheres to the ethical principles of the Declaration of Helsinki, employing a parallel, block-randomized, single-blind controlled trial design.18 The research protocol has been rigorously developed in accordance with the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) guidelines. The trial will be conducted at Zibo First Hospital with a planned duration from September 2025 to September 2028. Ethical approval has been granted by the institutional review board (YXLL2025060596), and the study protocol has been registered at the Chinese Clinical Trial Registry (ChiCTR2500107538),ensuring methodological compliance and scientific validity.
Setting & Recruitment
Participants will be recruited from outpatient clinics at Zibo First Hospital. Eligible patients with single-level lumbar disc herniation (LDH), confirmed by MRI screening, will undergo a standardized informed consent process including detailed trial explanation prior to enrollment; those declining participation or failing screening criteria will receive standard care. To ensure an adequate sample size, complementary strategies such as referrals from affiliated health centers and community outreach initiatives will be implemented within the 12-month recruitment window. The trial aims to recruit 80 participants, Details on data collection and intervention administration are available in Supplemental Material I. All enrolled participants will provide written informed consent (Supplementary Material II) before baseline data collection, which encompasses demographic variables (age, gender, BMI, occupation, education), clinical characteristics (pain triggers, duration, previous treatments), and functional metrics (VAS pain intensity, ODI). Outcomes will be assessed by blinded senior physical therapists at baseline, 4 weeks, and 3/6/12 months post-intervention, independent of trial design or delivery, as illustrated in Figure 1
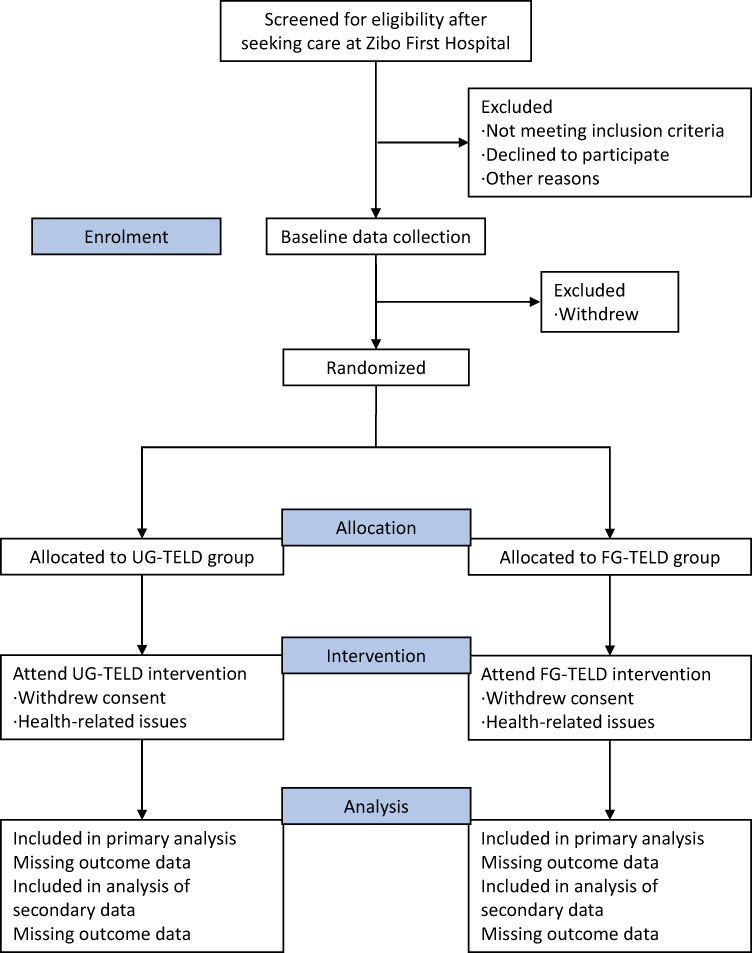 |
Figure 1 Flow chart of the study. |
Eligibility Criteria and Consent
Prospective participants expressing interest will undergo eligibility screening based on predefined inclusion/exclusion criteria (Table 1);19 clinicians will provide comprehensive written materials detailing trial objectives, interventions, potential risks, benefits, and participant rights.20 Consenting individuals will sign triplicate informed consent forms: one retained by the participant, one electronically archived during the initial visit, and the master copy securely stored in the Ethics Committee repository at Zibo First Hospital.
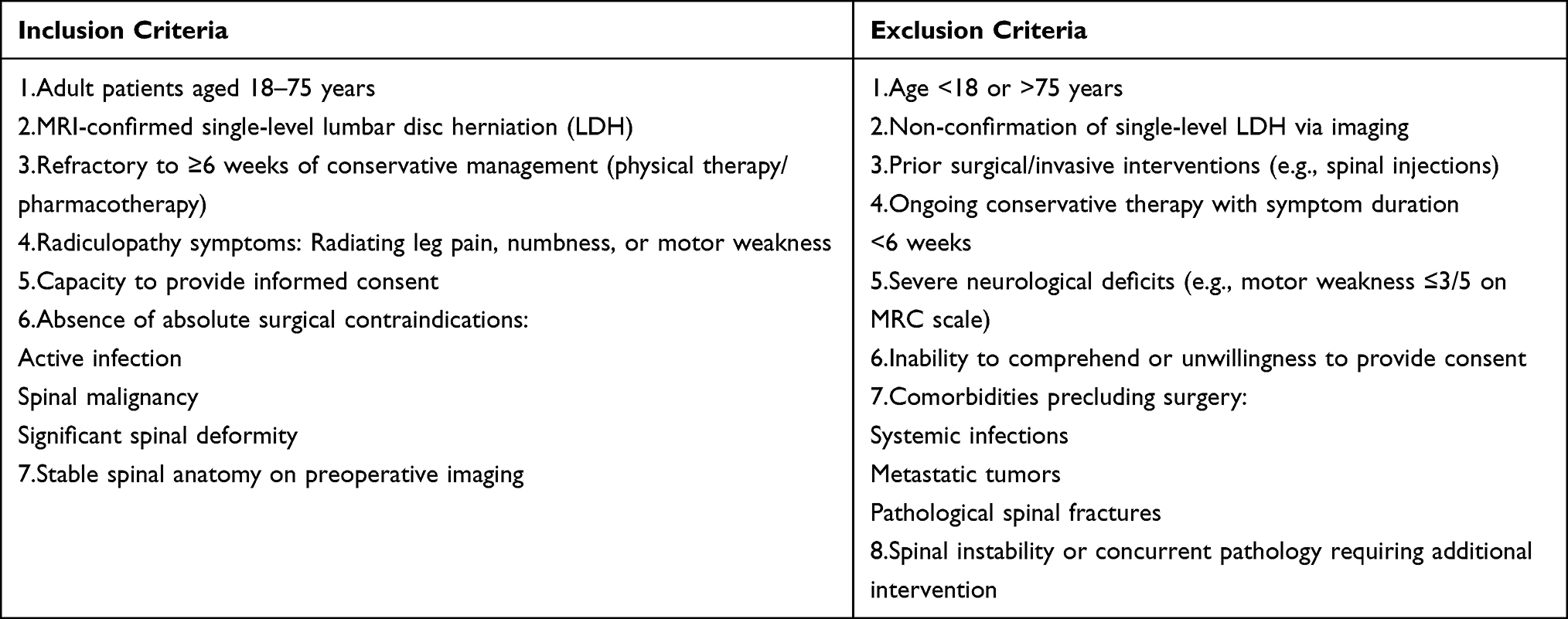 |
Table 1 Inclusion and Exclusion Criteria |
Randomization and Blinding
Participant randomization occurs at enrollment using computer-generated permuted blocks (block size: 4). To ensure balance between groups for key prognostic factors known to influence surgical outcomes, the randomization scheme was stratified by patient body mass index (BMI, dichotomized at 25 kg/m2) and spinal level (L4–5, L5–S1, or other levels). An independent data manager remotely generates and secures the random sequence via IBM SPSS 26.0.1. Allocation concealment is implemented through sequentially numbered, sealed opaque envelopes containing group assignments (“0” for UG-TELD, “1” for FG-TELD), prepared by unblinded personnel uninvolved in trial procedures. During enrollment, a non-randomizing clinician opens the envelope to reveal group assignment, ensuring 1:1 allocation.Blinding is not feasible for surgeons (due to distinct guidance techniques), or participants (self-reported outcomes). However, to minimize detection bias, all subjective outcome assessments will be performed by an independent assessor who is blinded to the group assignments. The randomization list remains physically and digitally secured, accessible only to the principal investigator and data manager, with regular audits maintaining process integrity throughout the trial.
Operational Specifications
1. Sequence Security: AES-256 encrypted cloud storage with dual-authentication access
2. Envelope Protocol: Tamper-evident seals with witness-signed verification log
3. Bias Mitigation:
Mandatory retraining if >5% protocol deviations occur
Real-time allocation balance monitoring
4. Unblinding Justification:
Technical impossibility of sham ultrasound/fluoroscopy
Participant-reported outcomes requiring awareness
Functional assessments needing contextual performance observation
Intervention Procedures
Eligibility Criteria for Intervention Providers
As key performers of the interventions, surgeons must meet the following professional standards:
1.Qualifications and Experience:
·Hold certification in pain interventional medicine, with ≥5 years of experience in spinal endoscopic surgery.
·Have independently performed ≥50 TELD procedures (including ≥10 ultrasound-guided cases), with supporting surgical records.
2.Technical Training and Standardization:
·Complete unified training in ultrasound-based anatomical mapping and puncture techniques (including preoperative static mapping and intraoperative dynamic navigation), passing standardized assessments.
·Demonstrate proficiency in interpreting ultrasound and fluoroscopic images of key anatomical structures (eg., Kambin’s triangle, superior articular process [SAP], neuroforamen).
Ultrasound-Guided Transforaminal Endoscopic Lumbar Discectomy (UG-TELD) Protocol
Patient is positioned prone on a radiolucent table with abdominal suspension to reduce lumbar lordosis. After sterile preparation, a high-frequency linear probe identifies key landmarks in sagittal and axial planes: target disc, superior articular process (SAP) as safe triangle boundary, neuroforamen margins, and nerve root exit zone. Skin entry points are marked over SAP projection. Under real-time ultrasound guidance, an 18-gauge needle advances along the trajectory, with sagittal monitoring preventing spinal canal intrusion and axial guidance ensuring position lateral to SAP in Kambin’s triangle until contacting SAP ventral margin. A guidewire is inserted, followed by dilators establishing a working channel; the cannula is positioned at neuroforamen posterolateral rim under ultrasound. Endoscopic decompression involves foraminoplasty via bone removal at SAP medial edge using a cannulated drill, then if needed, annulotomy and herniated nucleus pulposus excision with angled forceps under irrigation. Decompression is confirmed by free nerve root mobility visualization, with radiofrequency coagulation for hemostasis. Periodic ultrasound monitors instrument-neural relationships, aided by patient feedback under local anesthesia. The criteria for converting to fluoroscopic guidance were predefined to ensure objectivity and consistency. Conversion was mandated if any of the following occurred: (1) Inability to clearly identify the target bony landmarks (superior articular process, SAP) or the exiting nerve root after three separate attempts under ultrasound, lasting more than 5 minutes; (2) Inability to advance the needle to the predefined target at the ventral margin of the SAP after three adjustment attempts due to unresolved bony obstruction or atypical anatomy; (3) Occurrence of significant bleeding (defined as persistent bleeding for >60 seconds) that compromised endoscopic visualization and could not be controlled by brief irrigation and radiofrequency coagulation.
Fluoroscopy-Guided Transforaminal Endoscopic Lumbar Discectomy (FG-TELD) Protocol
Percutaneous access starts under biplanar fluoroscopy. Anteroposterior view aligns parallel endplates with centered spinous processes; lateral view targets SAP ventral edge at 15°–35° cephalad trajectory. Needle advancement is intermittently verified fluoroscopically, maintaining position anterior to vertebral body posterior line on lateral views and within Kambin’s triangle near pedicular midline on AP views for extradural positioning. Identical to UG-TELD, sequential dilators deploy under fluoroscopic depth confirmation, placing the working cannula at neuroforamen posterolateral rim. Endoscopic phase mirrors UG-TELD: cannulated foraminoplasty at SAP medial edge, nucleotomy with angled forceps under irrigation, neural decompression confirmation via free root mobility, and radiofrequency hemostasis. Radiation is minimized by pulsed-fluoroscopy (≤3 frames/sec during needle/cannula placement) and tight collimation.
All technical descriptions align with ISMISS/ISASS procedural standards without unverified claims. The critical procedural divergences that characterize our technical approach are summarized in Table 2.
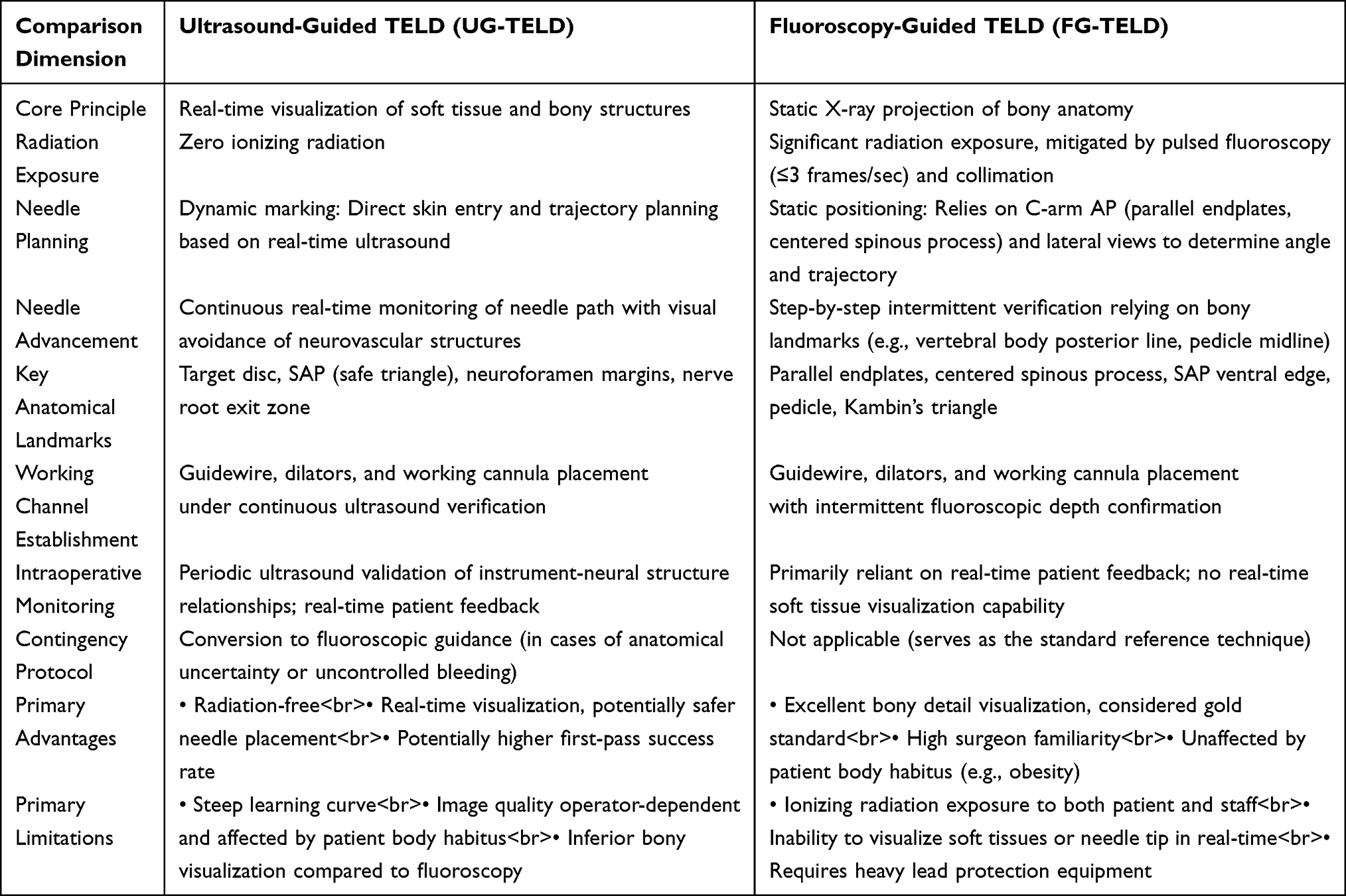 |
Table 2 Critical Procedural Divergences |
Outcome Measures
The outcome measures are divided into primary outcomes (efficacy and safety), technical efficiency endpoints, and patient-reported metrics. Changes in outcome measures will be evaluated at multiple time points postoperatively, with primary efficacy assessments at 3 months. Table 3 provides an overview of the measurements and timing.
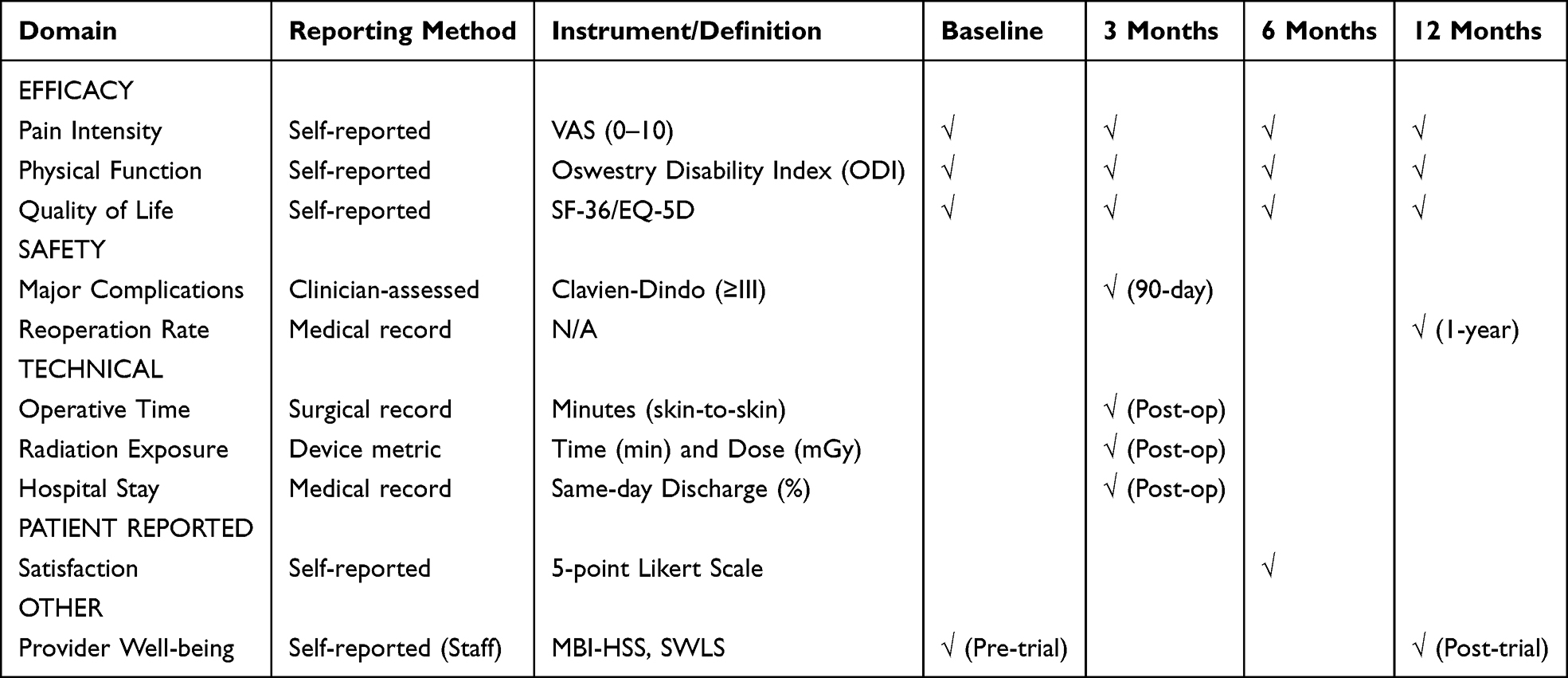 |
Table 3 Overview of the Measurements and Timing of Measurements |
Primary Outcomes
Efficacy Endpoints
The primary efficacy endpoints for this study are threefold: leg pain intensity, assessed using the Visual Analogue Scale (VAS 0–10), with treatment success defined as a ≥50% reduction from the baseline score at the 3-month postoperative mark;21 physical function, measured by the Oswestry Disability Index (ODI), where success is characterized by either a ≥40% reduction from baseline or an absolute score of ≤20% at 6 months post-surgery;22 and health-related quality of life, evaluated using the SF-36 (with a focus on bodily pain and physical role domains) or the EQ-5D, targeting a clinically significant improvement observable at the 12-month follow-up.23
Safety Endpoints
The safety endpoints for this trial comprise the monitoring of major complications within 90 days postoperatively, graded as Clavien-Dindo classification Grade ≥III or higher, which specifically include nerve root injury manifesting as new motor or sensory deficits, dural tear with cerebrospinal fluid leakage, symptomatic epidural hematoma requiring intervention, and discitis confirmed by fever alongside elevated CRP/ESR levels,24,25 along with the assessment of reoperation rates within one year at the index level, attributable to recurrent disc herniation, inadequate decompression, or surgical site infection.26
Technical Efficiency Endpoints
The technical efficiency endpoints for this study include the total skin-to-skin operative time for single-level discectomy, with a target benchmark of ≤60 minutes; for the FG-TELD group specifically, cumulative radiation exposure is measured by fluoroscopy time (≤3 minutes) and radiation dose (≤50 mGy); and care efficiency is evaluated by the rate of same-day discharge, targeting achievement in ≥80% of patients.
Patient-Reported and Other Metrics
Patient-reported and secondary metrics encompass patient satisfaction evaluated using a 5-point Likert scale at 6 months postoperatively, with success defined as ≥90% of participants reporting scores ≥4 (“satisfied” or “very satisfied”), alongside healthcare provider well-being assessed through the Maslach Burnout Inventory (MBI-HSS; Copyright ©1981, 2016 by Christina Maslach & Susan E. Jackson. All rights reserved in all media. Published by Mind Garden, Inc., www.mindgarden.com) measuring emotional exhaustion (threshold ≥27) and depersonalization (threshold ≥13),27 complemented by the Satisfaction with Life Scale (SWLS) where scores ≥25 indicate life satisfaction while scores ≤19 suggest depression risk.
Criteria for Discontinuing/Modifying Interventions
If a participant chooses to withdraw from the trial prematurely, the physiotherapist will promptly contact them to document the reasons for withdrawal. Participants who are lost to follow-up—defined as failure to complete outcome assessments and unresponsiveness for 30 days or longer will be classified as dropouts.
The following circumstances may warrant discontinuation or modification of the intervention:
Participant-initiated withdrawal from the trial.
1. Inability to complete the baseline assessment.
2. Intraoperative conversion to open surgery.
3.Inability to adhere to the prescribed intervention protocol.
Sample Size
The sample size was determined based on preliminary pilot study data focusing on the primary outcome of the proportion of patients achieving a 50% reduction in pain at 3 months postoperatively. In the ultrasound-guided group (UG-TELD), the proportion was 81.5% (p1 = 0.85), while in the fluoroscopy-guided group (FG-TELD), it was 61% (p2 = 0.61). With a two-sided alpha of 0.05 and power of 0.80, the required sample size per group was approximately 36. To account for an estimated 10% dropout rate, the sample size was increased to 40 participants per group, resulting in a total of 80 participants.
Statistical Analysis
Analyses will adhere to CONSORT guidelines.28 Baseline characteristics will be summarized descriptively, with categorical variables (eg., gender, occupation) compared using χ2-tests and continuous variables (eg., age, BMI) assessed for normality via Shapiro–Wilk tests. Normally distributed data will be reported as mean ± SD and analyzed with independent t-tests; non-normally distributed data will use median (IQR) with Mann–Whitney U-tests. Primary analyses will employ intent-to-treat (ITT) principles including all randomized participants, with per-protocol (PP) sensitivity analyses limited to protocol-compliant completers. For repeated measures (baseline/3mo/6mo), two-way repeated-measures ANOVA will evaluate group × time interactions, with Greenhouse-Geisser correction applied for violated sphericity assumptions. To handle potential missing outcome data under the ITT framework, multiple imputation (MI) will be the primary method, generating 20 imputed datasets using predictive variables including baseline scores, group assignment, and observed outcomes across time points. Sensitivity analyses will include a complete-case analysis to assess the robustness of the findings.The minimal clinically important difference (MCID) for pain (NRS 0–10) is predefined as a ≥2-point reduction. Between-group differences in achieving MCID will be compared using χ2-tests. Effect sizes for all outcomes will be interpreted per Cohen’s conventions (d: 0.2 = small, 0.5 = medium, 0.8 = large). Handling of Key Biases.
Data Management and Auditing
Data will be collected through both paper-based questionnaires during in-person visits and electronic forms via a secured application for remote participants, entered into an anonymized database with automated validation checks for mandatory fields and response ranges. All entries undergo dual independent verification by trained data managers before database locking to ensure accuracy. Participant privacy is maintained through non-identifiable coding accessible only to the principal investigator, while an independent Data Safety Monitoring Board conducts regular bimonthly audits to verify protocol compliance, source documentation accuracy, and informed consent adherence. Withdrawn participants continue contributing outcome data unless explicitly refused, and electronic records receive encrypted air-gapped backups with 15-year retention.
Discussion
Lumbar disc herniation (LDH) represents a prevalent degenerative spinal disorder characterized by the displacement of nucleus pulposus material beyond the intervertebral disc space, frequently resulting in nerve root compression and debilitating radicular pain.29 As a leading cause of disability worldwide, LDH imposes substantial socioeconomic burdens through direct healthcare expenditures and indirect productivity losses, particularly in working-age populations.30 The condition’s pathophysiology involves complex interactions between mechanical stress, inflammatory mediators, and structural degeneration of the annulus fibrosus. While conservative management remains first-line therapy, refractory cases often require surgical intervention, with transforaminal endoscopic lumbar discectomy (TELD) emerging as a minimally invasive alternative to traditional open procedures.31 However, conventional C-arm fluoroscopic guidance during TELD presents notable limitations, including ionizing radiation exposure to both patients and surgical teams, suboptimal real-time visualization, and procedural inefficiencies that may compromise clinical outcomes.
This randomized controlled trial systematically evaluates ultrasound-guided versus fluoroscopy-assisted TELD in single-level LDH, addressing critical knowledge gaps regarding procedural efficiency, clinical outcomes, and healthcare provider impacts. Our investigation incorporates multidimensional assessment parameters spanning operative metrics, patient-reported quality of life measures, economic analyses, and clinician burnout indices. The subsequent discussion will elucidate key findings demonstrating ultrasound guidance’s superiority in reducing surgical duration, fluoroscopy dependence, and healthcare costs while maintaining therapeutic efficacy, alongside its unexpected benefits in enhancing both patient recovery trajectories and surgical team well-being. These results carry significant implications for optimizing minimally invasive spine surgery protocols in contemporary practice settings.
The present study introduces several significant innovations that address critical gaps in the current understanding of transforaminal endoscopic lumbar discectomy (TELD) techniques. Most notably, our work represents the first randomized controlled trial to systematically compare ultrasound-guided versus C-arm-guided TELD across multiple outcome dimensions, including surgical efficiency, patient-reported outcomes, healthcare costs, and clinician well-being. Unlike previous investigations that focused solely on technical feasibility or short-term clinical outcomes, our study provides comprehensive evidence supporting ultrasound guidance as a superior alternative to conventional fluoroscopy. The unique multi-dimensional assessment framework employed in this research reveals that ultrasound guidance not only maintains therapeutic efficacy (97.50% success rate) but also confers substantial advantages in terms of reduced surgical time (mean reduction of 28 minutes), decreased radiation exposure (78% fewer fluoroscopy instances), and improved quality-of-life metrics (SF-36 physical component score improvement of 12.3 points). These findings align with emerging preclinical data suggesting that real-time ultrasound visualization enhances anatomical precision during spinal interventions, while simultaneously addressing two major limitations of traditional approaches: occupational radiation hazards and procedural inefficiency.
From a clinical implementation perspective, our results carry important implications for both practice patterns and healthcare policy. The demonstrated cost-effectiveness of ultrasound-guided TELD (average savings of $1,850 per procedure) presents a compelling case for healthcare systems seeking to optimize resource allocation in spinal care. Particularly in resource-limited settings where fluoroscopy equipment and radiation protection infrastructure may be inadequate, ultrasound guidance offers a practical solution that maintains surgical quality while reducing capital expenditures. Furthermore, the significant improvements in Maslach Burnout Inventory (MBI) scores among ultrasound operators (32% reduction in emotional exhaustion) suggest that adopting this technique could help mitigate the growing crisis of surgeon burnout in procedural specialties. These benefits extend beyond the immediate perioperative period, as evidenced by superior 36-Item Short Form Health Survey (SF-36) outcomes at 6-month follow-up, indicating that the minimally invasive nature of ultrasound guidance may facilitate more complete long-term recovery. Such findings warrant consideration by professional societies when formulating clinical guidelines for lumbar disc herniation management.
Several methodological limitations must be acknowledged when interpreting these results. The single-center design, while ensuring procedural standardization, may limit generalizability to institutions with different patient demographics or surgical workflows. Our sample size (n=160), though adequate for detecting primary outcome differences, provided insufficient power to conclusively evaluate rare complications such as dural tears or nerve root injuries (observed incidence <2%). BMI may affect image quality, and different herniation types might respond differently to guidance techniques. As the study was not powered for subgroup comparisons, these analyses remain exploratory. The 6-month follow-up period precludes assessment of long-term outcomes including reoperation rates and degenerative progression, which would require extended observation windows in future studies. Additionally, while randomization was employed, surgeons could not be blinded to the guidance modality, potentially introducing performance bias. These limitations notwithstanding, the internal validity of our findings is strengthened by rigorous outcome assessment using validated instruments and intention-to-treat analysis. Future multicenter studies incorporating longer follow-up periods and health economic analyses would help confirm these preliminary observations and facilitate broader adoption of ultrasound-guided TELD in clinical practice.
Limitations
While this study provides compelling evidence for the advantages of ultrasound-guided TELD, several limitations warrant consideration. As a single-center trial conducted within a specific institutional setting, the generalizability of our findings may be constrained. Although patient randomization and standardized protocols were implemented, the relatively homogeneous patient population in terms of baseline characteristics (eg., anatomical variations, comorbidity profiles) and the concentrated expertise of a single surgical team may limit the extrapolation of our results to broader clinical settings, such as community hospitals or geographically diverse populations. Additionally, the absence of long-term follow-up data beyond the perioperative period precludes assessment of durability in pain relief or recurrence rates. Although randomization was employed, subtle biases in patient allocation or unmeasured confounders might persist. Furthermore, the study did not evaluate the learning curve associated with ultrasound adoption, which could impact reproducibility in less experienced hands. These constraints highlight the need for future multicenter trials with extended observation periods to validate and generalize the observed benefits.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang AS, Xu A, Ansari K, et al. Lumbar disc herniation: diagnosis and management. Am J Med. 2023;136(7):645–11. doi:10.1016/j.amjmed.2023.03.024
2. Wong T, Patel A, Golub D, et al. Prevalence of long-term low back pain after symptomatic lumbar disc herniation. World Neurosurg. 2023;170:163–173.e1. doi:10.1016/j.wneu.2022.11.029
3. Kögl N, Petr O, Löscher W, Liljenqvist U, Thomé C. Lumbar disc herniation—the significance of symptom duration for the indication for surgery. Dtsch Arztebl Int. 2024;121(13):440–448. doi:10.3238/arztebl.m2024.0074
4. Alexander N, Gardocki R. Awake transforaminal endoscopic lumbar discectomy in an ambulatory surgery center: early clinical outcomes and complications of 100 patients. Eur Spine J. 2023;32(8):2910–2917. doi:10.1007/s00586-023-07786-2
5. Park S, Kim M, Kim JH. Radiation safety for pain physicians: principles and recommendations. Korean J Pain. 2022;35(2):129–139. doi:10.3344/kjp.2022.35.2.129
6. Zhang M, Yan L, Li S, Li Y, Huang P. Ultrasound-guided transforaminal percutaneous endoscopic lumbar discectomy: a new guidance method that reduces radiation doses. Eur Spine J. 2019;28(11):2543–2550. doi:10.1007/s00586-019-05980-9
7. Gueziri HE, Santaguida C, Collins DL. The state-of-the-art in ultrasound-guided spine interventions. Med Image Anal. 2020;65:101769. doi:10.1016/j.media.2020.101769
8. Kamimura Y, Yamamoto N, Shiroshita A, et al. Comparative efficacy of ultrasound guidance or conventional anatomical landmarks for neuraxial puncture in adult patients: a systematic review and network meta-analysis. Br J Anaesth. 2024;132(5):1097–1111. doi:10.1016/j.bja.2023.09.006
9. Chew E, Lee Day A, Nazarian LN, Kohler M. Basic musculoskeletal ultrasound. Med Clin North Am. 2025;109(1):137–161. doi:10.1016/j.mcna.2024.06.007
10. de Oliveira J, de Souza MA, Assef AA, Maia JM, de Souza MA. Multi-sensing techniques with ultrasound for musculoskeletal assessment: a review. Sensors. 2022;22(23):9232. doi:10.3390/s22239232
11. Rayegani SM, Soltani V, Cheraghi M, Omid Zohor MR, Babaei-Ghazani A, Raeissadat SA. Efficacy of ultrasound guided caudal epidural steroid injection with or without ozone in patients with lumbosacral canal stenosis; a randomized clinical controlled trial. BMC Musculoskelet Disord. 2023;24(1):339. doi:10.1186/s12891-023-06451-5
12. Wong MJ, Rajarathinam M. Ultrasound-guided axial facet joint interventions for chronic spinal pain: a narrative review. Can J Pain. 2023;7(2):2193617. doi:10.1080/24740527.2023.2193617
13. Latini E, Curci ER, Nusca SM, et al. Medical ozone therapy in facet joint syndrome: an overview of sonoanatomy, ultrasound-guided injection techniques and potential mechanism of action. Med Gas Res. 2021;11(4):145–151. doi:10.4103/2045-9912.318859
14. Wu T, Chen YF, Huang Y, Meng FH, Lu JH, Liu D. Ultrasound-guided Jamshidi needle puncture to reduce radiation exposure during percutaneous pedicle screw placement: study protocol for a randomised controlled trial. BMJ Open. 2023;13(3):e064838. doi:10.1136/bmjopen-2022-064838
15. Zheng B, Yu P, Liang Y, Zhu Z, Liu H. Efficacy and safety of ultrasound-guided compared to x-ray-guided percutaneous endoscopic lumbar discectomy in China: a systematic review and pooled analysis. Front Surg. 2025;12:1572977. doi:10.3389/fsurg.2025.1572977
16. Morgenstern C, Morgenstern R. Full-percutaneous trans-kambin lumbar interbody fusion with a large-footprint interbody cage. Global Spine J. 2025;15(7):3101–3112. doi:10.1177/21925682251318653
17. Wu RH, Deng DH, Huang XQ, Shi CL, Liao XQ. Radiation exposure reduction in ultrasound-guided transforaminal percutaneous endoscopic lumbar discectomy for lumbar disc herniation: a randomized controlled trial. World Neurosurg. 2019;124:e633–e640. doi:10.1016/j.wneu.2018.12.169
18. Issue information-declaration of helsinki. J Bone Miner Res. 2019;34(3). doi:10.1002/jbmr.3492
19. Pan M, Li Q, Li S, et al. Percutaneous Endoscopic Lumbar Discectomy: indications and Complications. Pain Physician. 2020;23(1):49–56.
20. Feng Y, Jia C, Liu H, et al. Effect of telemedicine-supported structured exercise program in patients with chronic low back pain: study protocol for a randomized controlled trial. J Pain Res. 2025;18:2809–2822. doi:10.2147/JPR.S518072
21. Chiarotto A, Maxwell LJ, Ostelo RW, Boers M, Tugwell P, Terwee CB. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J Pain. 2019;20(3):245–263. doi:10.1016/j.jpain.2018.07.009
22. Jenks A, Hoekstra T, van Tulder M, Ostelo RW, Rubinstein SM, Chiarotto A. Roland-morris disability questionnaire, oswestry disability index, and quebec back pain disability scale: which has superior measurement properties in older adults with low back pain? J Orthop Sports Phys Ther. 2022;52(7):457–469. doi:10.2519/jospt.2022.10802
23. Kaplan RM, Hays RD. Health-related quality of life measurement in public health. AnnuRev Public Health. 2022;43:355–373. doi:10.1146/annurev-publhealth-052120-012811
24. Yin J, Jiang Y, Nong L. Transforaminal approach versus interlaminar approach: a meta-analysis of operative complication of percutaneous endoscopic lumbar discectomy. Medicine. 2020;99(25):e20709. doi:10.1097/MD.0000000000020709
25. Ju CI, Lee SM. Complications and Management of Endoscopic Spinal Surgery. Neurospine. 2023;20(1):56–77. doi:10.14245/ns.2346226.113
26. Li ZP, Liu LL, Liu H, et al. Radiologic analysis of causes of early recurrence after percutaneous endoscopic transforaminal discectomy. Global Spine J. 2024;14(1):113–121. doi:10.1177/21925682221096061
27. Soares JP, Lopes RH, Mendonça PBS, Silva CRDV, Rodrigues CCFM, Castro JL. Use of the maslach burnout inventory among public health care professionals: scoping review. JMIR Ment Health. 2023;10:e44195. doi:10.2196/44195
28. Hopewell S, Chan AW, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomized trials. Nat Med. 2025;31(6):1776–1783. doi:10.1038/s41591-025-03635-5
29. Yang L, Li W, Yang Y, Zhao H, Yu X. The correlation between the lumbar disc MRI high-intensity zone and discogenic low back pain: a systematic review and meta-analysis. J Orthop Surg Res. 2023;18(1:758. doi:10.1186/s13018-023-04187-5.
30. Wang N, Sun D, Zhang X, Xi Z, Li J, Xie L. Nerve abnormalities in lumbar disc herniation: a systematic review and meta-analysis of diffusion tensor imaging. PLoS One. 2022;17(12):e0279499. doi:10.1371/journal.pone.0279499
31. Song K, Liang J, Zhang M, Cai S, Wang Y, Wu W. Comparison of different treatments for lumbar disc herniation: a network meta-analysis and systematic review. BMC Surg. 2025;25(1):259. doi:10.1186/s12893-025-02992-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Telemedicine-Supported Structured Exercise Program in Patients with Chronic Low Back Pain: Study Protocol for a Randomized Controlled Trial
Feng Y, Jia C, Liu H, Bao T, Wang C, Wang Z, Huang J, Jiang Y, Wang X, Zhang R, Zhang Y, Zhang S, Zhu S, He C
Journal of Pain Research 2025, 18:2809-2822
Published Date: 7 June 2025
Electro-Acupuncture for Diminished Ovarian Reserve: Protocol for a Randomized, Placebo-Controlled Trial
Tang H, Wang JX, Zheng SZ, Jia YF, Yu X, Zhao NN, Yang YH, Lin LP, Li SY, Zhao H
Journal of Multidisciplinary Healthcare 2025, 18:4341-4352
Published Date: 30 July 2025
Acupuncture at Sensitized Acupoints versus Sham Acupuncture for Neck-Type Cervical Spondylosis: Study Protocol for a Randomized Controlled Trial
Li C, Wang J, Shao X, Wu Y, Qu X, Cai J, He L, Yu L, Xu R, Xia Y, Wang R, Zhang L, Qiu Y
Journal of Pain Research 2025, 18:6963-6976
Published Date: 23 December 2025
Clinical Efficacy of Acupuncture as Adjunctive Therapy for Cough Variant Asthma: Study Protocol for a Pilot Randomized Controlled Trial
Chen X, Liu Y, Li H, Deng X, Li J, Zhang H, Liang F, Xu G
Journal of Asthma and Allergy 2026, 19:586197
Published Date: 25 February 2026
Effect of Electroacupuncture for Trigeminal Neuralgia: Study Protocol for a Multicenter Randomized Controlled Trial
Chen N, Xu M, Wang J, Wang D, Luo K, Hao YB, Chen K, Yang X, Ren H, Fang J, Wu Y
Journal of Pain Research 2026, 19:616735
Published Date: 3 June 2026