Back to Journals » Journal of Pain Research » Volume 19
Effect of Electroacupuncture for Trigeminal Neuralgia: Study Protocol for a Multicenter Randomized Controlled Trial
Authors Chen N, Xu M ![]() , Wang J, Wang D, Luo K, Hao YB, Chen K, Yang X, Ren H, Fang J, Wu Y
, Wang J, Wang D, Luo K, Hao YB, Chen K, Yang X, Ren H, Fang J, Wu Y ![]()
Received 14 April 2026
Accepted for publication 22 May 2026
Published 3 June 2026 Volume 2026:19 616735
DOI https://doi.org/10.2147/JPR.S616735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Nisang Chen,1,* Moran Xu,1,* Junyi Wang,1 Dong Wang,2 Kaitao Luo,3 Ya-Bo Hao,3 Kun Chen,4 Xibing Yang,3 Hongbin Ren,3 Jianqiao Fang,1,5 Yuanyuan Wu1,5
1The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Zhejiang Greentown Cardiovascular Hospital, Hangzhou, Zhejiang, People’s Republic of China; 3Jiaxing Hospital of Traditional Chinese Medicine, Jiaxing, Zhejiang, People’s Republic of China; 4Pingyang Research Institute, Zhejiang Chinese Medical University, Wenzhou, Zhejiang, People’s Republic of China; 5The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuanyuan Wu, Email [email protected] Jianqiao Fang, Email [email protected]
Introduction: Trigeminal neuralgia (TN) is a severe neuropathic pain disorder characterized by unpredictable pain paroxysms, significantly impairing patients’ quality of life through associated anxiety and depression. Electroacupuncture (EA) has demonstrated clinical value in managing chronic neuropathic pain. However, its specific efficacy as a pharmacotherapy-sparing strategy for TN remains to be systematically evaluated. This study aims to evaluate the short-term effectiveness and safety of an EA regimen for TN, and to examine changes in exploratory neuro-immune biomarkers, including IL-6 and 5-HT, related to pain and affective symptoms.
Methods and Analysis: This is a multicenter, randomized, double-simulation, placebo-controlled trial designed to compare the efficacy of EA plus placebo with sham EA plus carbamazepine (CBZ) for TN. A total of 126 adults with TN, maintained on a stable, low-to-moderate CBZ dose (200– 400 mg/day) to control for baseline medication-masking effects, will be randomly allocated to the EA plus placebo group or the sham EA plus CBZ group at a 1:1 ratio. Participants in the EA plus placebo group will receive EA plus placebo for 2 weeks, while those in the sham EA plus CBZ group will receive sham EA plus active CBZ on the same schedule, followed by a 6-week follow-up. The primary outcome will be the proportion of participants achieving a ≥ 50% reduction in visual analog scale (VAS) score at week 2. Secondary outcomes will include daily pain diary metrics (attack frequency, intensity, rescue medication use), Patient Global Impression of Change, Brief Pain Inventory-Facial, Short-Form McGill Pain Questionnaire, and psychological assessments (Self-Rating Anxiety and Depression Scales). Furthermore, plasma biomarkers (interleukin-6 and serotonin) and safety profiles (hepatic and renal functions) will be evaluated at baseline and week 2. All analyses will be conducted in accordance with the intention-to-treat principle.
Trial Registration: ClinicalTrials.gov Identifier: NCT06977932 (March 2, 2026).
Keywords: trigeminal neuralgia, TN, electroacupuncture, EA, carbamazepine, CBZ, biomarkers, randomized controlled trial, study protocol
Introduction
Trigeminal neuralgia (TN) is a chronic neuropathic pain disorder characterized by sudden, severe paroxysms of pain within the distribution of the trigeminal nerve. Clinically, TN presents with highly distinctive features: the pain is typically unilateral, described as electric shock-like, stabbing, or burning, and is often precipitated by innocuous stimuli such as speaking, chewing, or washing the face.1 The global lifetime prevalence of TN ranges from 0.16% to 0.3%, with a 1-year prevalence of 0.5% to 1%, and a significantly higher prevalence in women than in men.2,3 The unpredictability and severity of attacks frequently lead to patient psychological comorbidities, including anxiety and depression, which in turn impair social functioning and markedly reduce quality of life.4
Currently, therapeutic strategies for TN primarily comprise pharmacological and surgical approaches. Carbamazepine (CBZ) remains the first-line pharmacological agent,2 effectively reducing the frequency and severity of paroxysmal pain. However, managing TN remains challenging. Current medications often fail to simultaneously address refractory pain and its emotional burden. Furthermore, long-term administration is frequently limited by drug tolerance and severe adverse effects, including sedation, ataxia, hepatic and renal impairment, hyponatremia, and bone marrow suppression.5 Moreover, complex drug–drug interactions require careful consideration.6 Consequently, patients who are refractory to or intolerant of these medications often require surgical management, such as microvascular decompression, stereotactic radiosurgery, or percutaneous procedures.7 However, advanced age and significant medical comorbidities render many patients ineligible for these procedures.1,8 Even when surgery is performed, postoperative recurrence, along with complications such as facial numbness, masticatory weakness, and olfactory disturbances, remains prevalent.9 Additionally, psychological factors, including fear of surgery, further limit the widespread adoption of surgical treatments as first-line strategies.
Due to the risks of surgical interventions and cumulative toxicities of long-term pharmacotherapy, effective non-pharmacological treatments are required. To objectively evaluate how these alternative therapies alleviate both physical pain and psychological comorbidities, recent studies have targeted biomarkers within their shared neurobiological pathways. Consequently, the neuro-immune axis and neurotransmitter networks have emerged as critical evaluative targets.10,11 Specifically, interleukin-6 (IL-6) acts as a key mediator of neuroinflammation; elevated serum levels strongly correlate with pain severity, making it a reliable biomarker for assessing therapeutic response.12 Concurrently, serotonin (5-HT) plays a pivotal, dual role in this pathology. While peripheral 5-HT directly enhances trigeminal nociceptor activity and genetic polymorphisms in its transporter are linked to TN susceptibility,13 central 5-HT dysregulation is also widely recognized as a primary driver of the associated anxiety and depression.
Acupuncture, a Traditional Chinese Medicine technique widely utilized for pain management, is increasingly recognized for its clear efficacy in alleviating neuropathic pain.14,15 Electroacupuncture (EA), developed by integrating traditional acupuncture with electrical stimulation, is extensively applied in clinical practice owing to its favorable safety profile and sustained analgesic effects.16–18 Building on our prior research in the symptom management of TN,19 we have previously demonstrated the efficacy of EA through a randomized controlled trial. However, previous studies mainly focused on the analgesic effect of EA itself, and direct comparisons with guideline-recommended first-line medications under individualized treatment regimens remain limited. In addition, the effectiveness of a short-term intensive EA regimen for rapid pain relief in TN has not been fully clarified. Accordingly, we designed this multicenter randomized controlled trial to evaluate a short-term EA regimen within a double-simulation design comparing the EA plus placebo group with the sham EA plus CBZ group.
Methods and Analysis
Study Design
In this multicenter randomized controlled trial, eligible participants will be randomly assigned in a 1:1 ratio to receive either EA plus placebo or sham EA plus CBZ. Figure 1 presents the study flow diagram, and Table 1 summarizes the schedule of enrollment, interventions, and assessments. The protocol has been prepared in accordance with the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) statement.20 Furthermore, the final trial results will be reported in adherence to the CONSORT21 (Consolidated Standards of Reporting Trials) guidelines and its STRICTA (Standards for Reporting Interventions in Clinical Trials of Acupuncture) extension to ensure standardized reporting.22
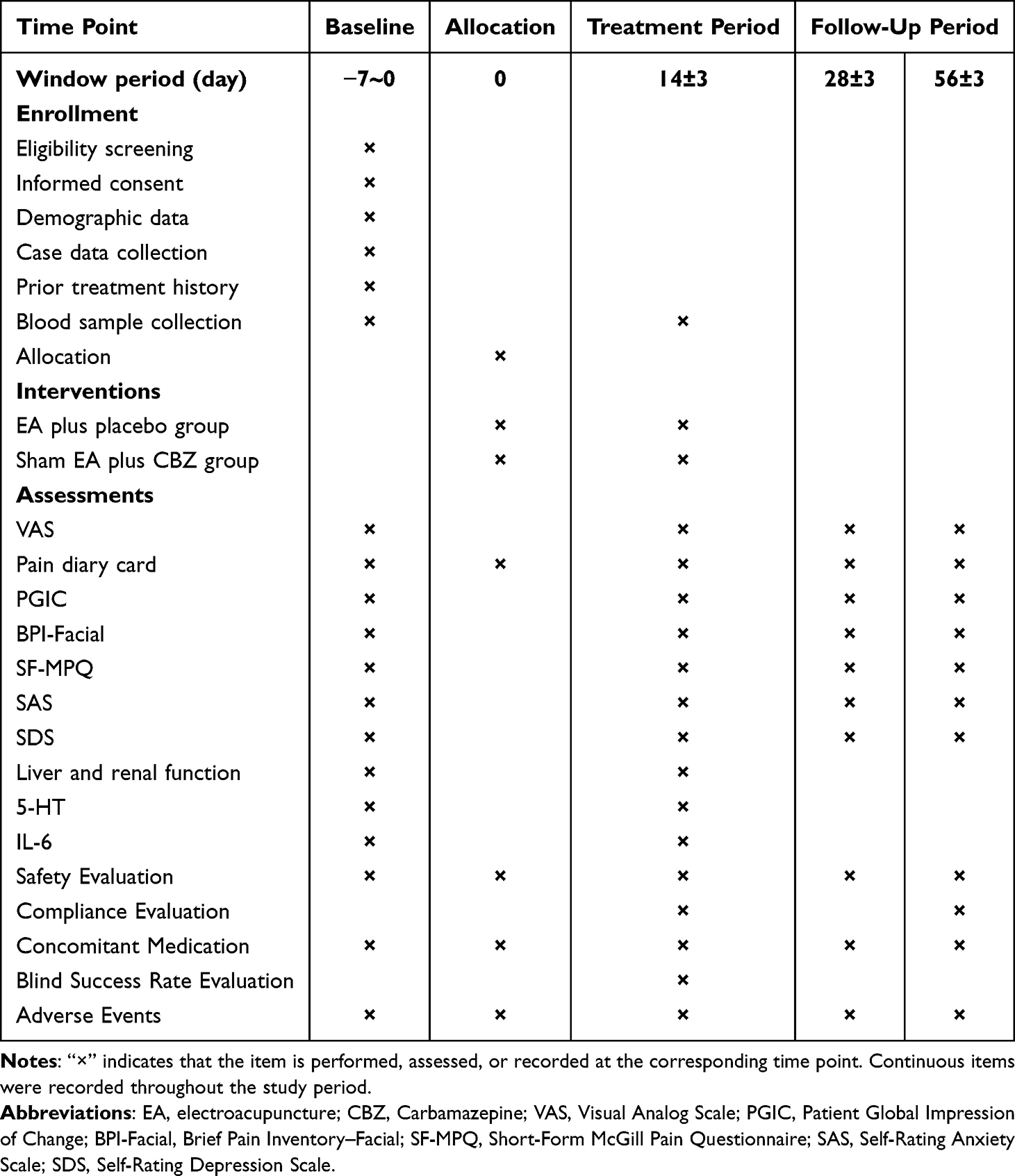 |
Table 1 Schedule of the Trial Based on the SPIRIT Standard Protocol Items for Interventional Trials |
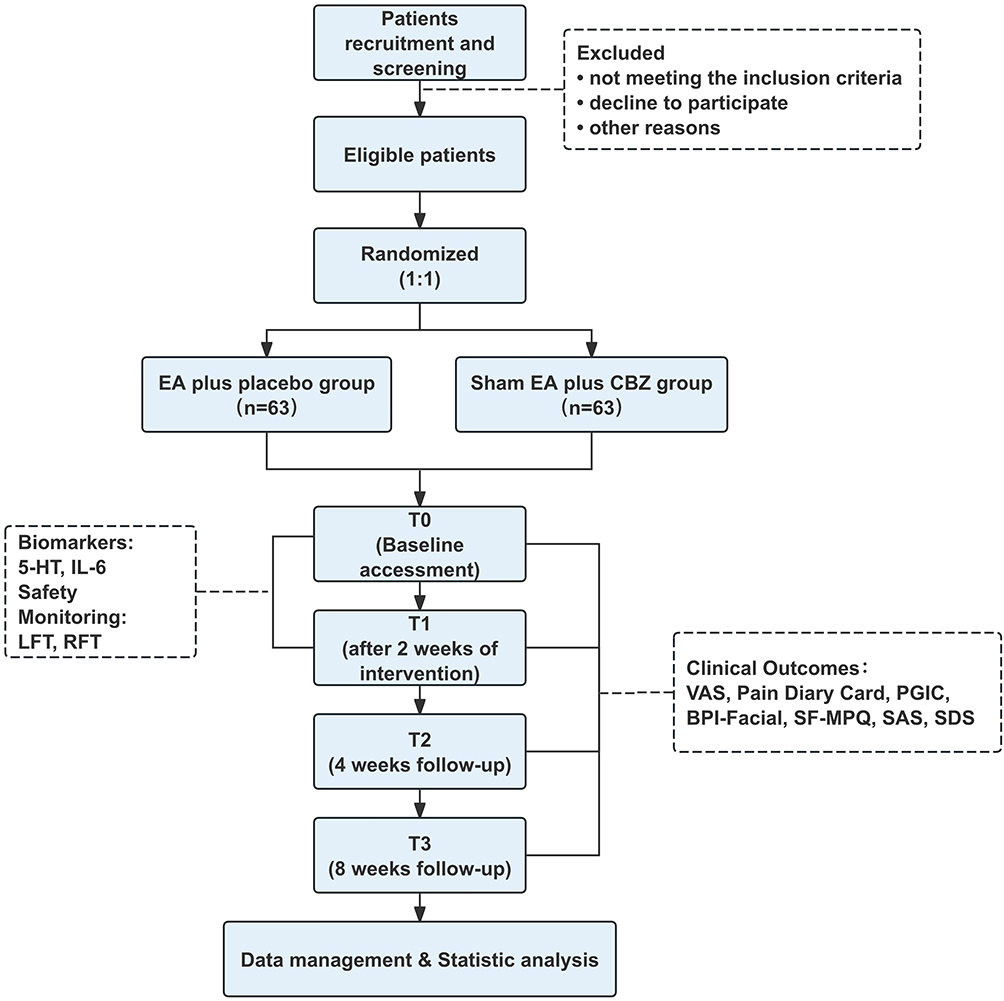 |
Figure 1 Flow chart of the study process. |
Ethical Standards and Registration
This multicenter trial was approved by the ethics committee of the Third Affiliated Hospital of Zhejiang Chinese Medical University (lead committee; approval No. ZSLL-KY-2025-040-05) and by each participating site: Pingyang County Hospital of Traditional Chinese Medicine (approval No. I2026-011-01) and Jiaxing Hospital of Traditional Chinese Medicine (approval No. S1-2025-0024-4). The trial was prospectively registered with ClinicalTrials.gov (NCT06977932), consistent with international standards for clinical trial transparency.
Participant Recruitment
Participants will be recruited from three clinical sites: the Third Affiliated Hospital of Zhejiang Chinese Medical University (coordinating center), Pingyang County Hospital of Traditional Chinese Medicine, and Jiaxing Hospital of Traditional Chinese Medicine. Recruitment strategies include WeChat advertisements and posters placed in participating hospitals and surrounding communities. All eligible participants must provide written informed consent prior to undergoing baseline assessments.
Eligibility Criteria
Diagnostic Criteria
Diagnostic criteria for TN will be defined according to the International Classification of Headache Disorders, 3rd edition (ICHD-3), published by the International Headache Society (IHS) in 2018:23 (1) Recurrent paroxysms of unilateral facial pain localized to the distribution of one or more divisions of the trigeminal nerve, with no radiation beyond the trigeminal territory, and fulfilling criteria (2) and (3); (2) Pain characterized by all of the following: ① Paroxysms lasting from a fraction of a second to 2 minutes; ② Severe intensity; ③ Electric shock‑like, stabbing, or sharp quality; (3) Paroxysms may be provoked by innocuous stimuli within the affected trigeminal distribution; (4) Not better accounted for by another ICHD‑3 diagnosis of facial pain.
Inclusion Criteria
Participants will be eligible for inclusion if they met all of the following criteria: (1) Meet the diagnostic criteria for TN; (2) Aged 18 to 80 years, inclusive, of any sex; (3) Receiving CBZ at a stable dose of 200–400 mg/day; (4) Conscious, able to perceive and discriminate pain, and capable of basic communication; (5) Willing to participate voluntarily and provided written informed consent, either personally or through a legal guardian/authorized representative.
Exclusion Criteria
Participants will be excluded if they met any of the following criteria: (1) Comorbid epilepsy, head injury, or other relevant neurological disorders; (2) Severe cardiac, hepatic, or renal impairment; (3) Cognitive impairment, aphasia, psychiatric illness, or inability to adhere to study procedures; (4) Poorly controlled hypertension or hyperglycemia; (5) Recent diagnosis of severe anxiety or depression; (6) Pregnancy or breastfeeding; (7) Cardiac pacemaker or other contraindications to EA;(8) Concurrent enrollment in another clinical trial.
Randomization and Allocation Concealment
Eligible participants will be randomly assigned to the treatment or control group in a 1:1 ratio. Randomization will be performed using a computer-generated permuted block randomization with a block size of 4. To ensure strict allocation concealment, investigators or designated study personnel at each site will enroll participants and then log into a centralized randomization system to obtain group assignments. The randomization sequence generation and data management will be overseen by an independent third party, Sluxin (Shanghai) Information Technology Co., Ltd.
Blinding
Given the nature of the acupuncture intervention, the acupuncturist will be necessarily aware of group assignment and could not be blinded. However, blinding will be maintained for all other parties, including patients, outcome assessors, data entry personnel, and statisticians. The success of patient blinding will also be evaluated. To preserve blinding integrity, each patient will be treated individually whenever possible to minimize opportunities for discussion of treatment procedures, needling sensations, or therapeutic responses among participants.
Emergency unblinding: Emergency unblinding procedures will only be permitted in cases of severe medical emergencies where knowing the group assignment is crucial for the participant’s immediate clinical management. The principal investigator must be notified within 24 hours of any unblinding event.
Intervention
Eligible participants will be randomly assigned to receive either EA plus placebo or sham EA plus CBZ. Both groups will undergo a 2‑week treatment period followed by a 6‑week follow‑up. Participants in the EA plus placebo group will receive EA administered for 5 consecutive days per cycle, with a 2‑day interval between cycles, for a total of 2 cycles (2 weeks). Placebo will be taken daily throughout the 2‑week treatment period. Those in the sham EA plus CBZ group will receive an identical schedule of sham EA sessions, along with daily CBZ for 2 weeks.
All acupuncture procedures will be performed using disposable stainless steel needles (Hwato), Suzhou Medical Supplies Co., Ltd., Suzhou, China; specifications: φ0.18 × 25 mm and φ0.25 × 40 mm; both NMPA‑approved). Electrical stimulation will be delivered using a transcutaneous and acupoint electrical stimulator (FANGS-100, Hangzhou Dalishen Medical Devices Co., Ltd., Hangzhou, China). All treatment procedures will be administered by 10 licensed Traditional Chinese Medicine practitioners with 5 years or more of clinical experience in acupuncture. These practitioners hold nationally recognized Traditional Chinese Medicine (TCM) practitioner licenses and have undergone standardized training in point localization, acupuncture manipulation techniques, and EA procedures.
EA Plus Placebo Group
Patients will be treated in a supine position. Local point selection includes Siba (ST2), Xiaguan (ST7), and Dicang (ST4) on the affected side, supplemented by branch‑specific points: Tongziliao (GB1) for the ophthalmic branch, Quanliao (SI18) for the maxillary branch, and Jiache (ST6) for the mandibular branch. Distal points Hegu (LI4) and Waiguan (TE5) will be selected bilaterally. At local sites, 0.18×25 mm needles will be inserted superficially using a cluster needling technique along the affected trigeminal nerve branches; deqi sensation will not be required, and manipulation will be kept gentle to avoid triggering points—hypersensitive areas identified through prior patient communication. At distal points, 0.25×40 mm needles will be inserted perpendicularly to a depth of 20–30 mm to achieve deqi, followed by the reducing method (10 repetitions of rotating and lifting‑thrusting). During acute pain episodes, distal acupoints will be needled first, using reducing manipulation to achieve initial pain relief, followed by needling of the local acupoints.
For EA stimulation, pairs of local points (ST7 + GB1, ST7 + SI18, or ST7 + ST6) and distal points (LI4 + TE5) will be connected to an electrical stimulator (FANGS-100), which will deliver dense-and-sparse waves at 2/100 Hz for 60 minutes, with the current intensity adjusted within a range of 0.1–0.6 mA according to patient tolerance.
CBZ placebo (manufactured by Zhejiang CONBA Pharmaceutical Co., Ltd., 100 mg/tablet), identical in appearance to active CBZ but without therapeutic effect, will be administered to participants in the placebo group. Patients will continue their pre‑enrollment CBZ dosage using placebo tablets, with doses individually packaged, vacuum‑sealed by study personnel, and dispensed accordingly. No separate CBZ tapering phase will be performed before randomization.
Sham EA Plus CBZ Group
Participants assigned to the sham EA plus CBZ group will not receive active EA, although they will be informed of this after trial completion and will be offered 2 weeks of complimentary active EA as compensation. For sham acupuncture, needles will be superficially inserted (0.5–1 mm) at non-acupoints located 1 cm lateral to the acupoints used in the active EA group (avoiding trigger points). No manual needle manipulation will be performed. Electrodes will be attached to pairs of local points (sham ST7 + sham GB1, sham ST7 + sham SI18, or sham ST7 + sham ST6) and distal points (sham LI4 + sham TE5) in the same manner as in the active EA group; however, the electrical stimulator will remain off throughout the 60-minute treatment session, delivering no current. The treatment frequency and session duration will be identical to those in the active EA group. Regarding medication, participants continue their pre-enrollment CBZ dosage using active CBZ tablets, with doses individually packaged, vacuum-sealed by study personnel, and dispensed accordingly.
The Position and Function of Acupoints
Acupuncture points will be selected and localized in accordance with the National Standard of the People’s Republic of China (GB/T 12346–2021). Figure 2 depicts the precise anatomical locations of the acupoints, and Table 2 summarizes the acupoints, their anatomical landmarks, and positioning guidelines used in this study.
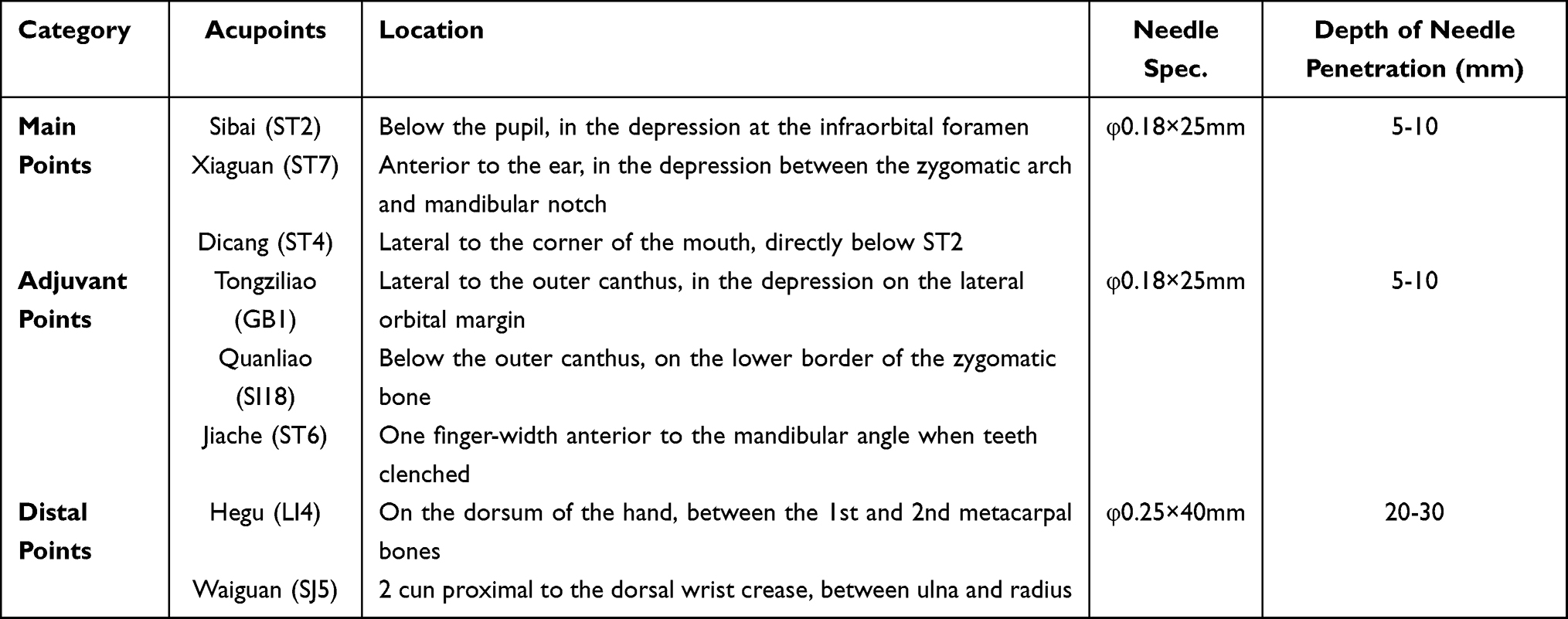 |
Table 2 Categories of Acupoint Selection, Acupoint Localization, Needle Selection, and Depth of Insertion in Electroacupuncture Therapy |
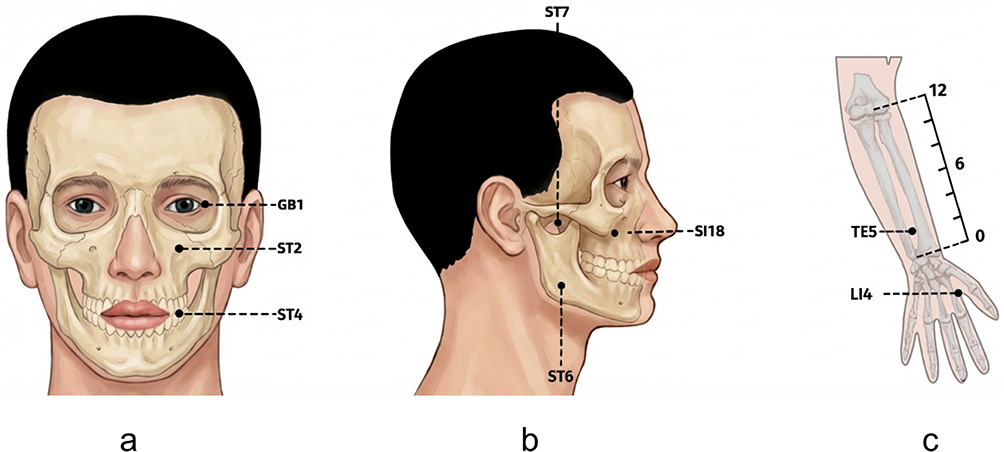 |
Figure 2 Acupoints and locations. Notes: (a) Anterior view of the face illustrating the anatomical locations of acupoints GB1, ST2, and ST4. (b) Lateral view of the face indicating the positions of ST7, SI18, and ST6. (c) Lateral view of the upper limb showing TE5 and LI4. |
Emergency Treatment
Concomitant analgesic therapy is prohibited throughout the trial period. Rescue medication (including but not limited to CBZ) may be permitted only in cases of severe, intolerable pain that significantly impairs daily functioning; if CBZ is administered, the maximum total daily dose must not exceed 1200 mg. All rescue medication use, including drug name, administration date, time, and dosage, must be accurately documented by the patient.
Outcomes
Primary Outcome
VAS Responder Rate
The primary outcome is the VAS responder rate,24 defined as the proportion of participants achieving a ≥50% reduction in the VAS score from baseline to the end of week 2. Week 2 was selected as the primary endpoint because it corresponds to the end of the short-term intensive intervention and is intended to capture the immediate analgesic response to the assigned treatment strategy. The VAS will be used to assess the average pain intensity experienced over the preceding 24 hours on a continuous 10-cm scale, ranging from 0 (“no pain”) to 10 (“worst imaginable pain”).25 Higher scores indicate more severe pain. At each assessment time point, patients will rate their average pain intensity over the preceding 24 hours, and investigators will record the specific values.
Secondary Outcome
Changes in VAS Scores
Changes in VAS scores from baseline will be evaluated to assess the specific trend of pain reduction. The VAS score will reflect the average pain intensity experienced over the preceding 24 hours, ranging from 0 to 10, with higher scores reflecting worse pain outcomes. Assessments will be conducted at baseline and weeks 2, 4, and 8.
Pain Diary–Derived Outcome Measures
Participants will complete a 24-hour pain diary26 on a daily basis from baseline to week 8. The diary will record the frequency of pain episodes, average pain intensity over the preceding 24 hours, highest pain intensity over the preceding 24 hours, and rescue medication use. These daily records will be used to derive the following outcome measures: average daily frequency of pain episodes, average daily pain intensity, highest daily pain intensity, and total number of days of rescue medication use.27
Changes Value in the Patient Global Impression of Change (PGIC)
The PGIC scale evaluates the patient’s perceived change in overall health status. The scale uses a 7-point Likert format (1 = “very much worse” to 7 = “very much better”).28 Scores of 1–3 indicate disease progression, 4 indicates functional stability, and 5–7 represents clinical improvement. Because it assesses changes relative to pre-treatment, assessments will be conducted only at weeks 2, 4, and 8.
Changes Value in the Brief Pain Inventory-Facial Scale (BPI-Facial)
The BPI-Facial is a validated multidimensional instrument for facial pain assessment. It evaluates both pain intensity and pain-related interference, including the impact of pain on general daily activities and face-specific function. Given that TN often affects facial activities such as eating, chewing, talking, and oral hygiene, the BPI-Facial is useful for assessing the functional burden associated with pain. Higher scores indicate greater pain severity and functional impairment. This instrument has shown sound psychometric performance in patients with TN.29 Assessments will be conducted at baseline and weeks 2, 4, and 8.
Changes Value in the Short-Form McGill Pain Questionnaire (SF-MPQ)
The SF-MPQ is a well-established multidimensional pain questionnaire used to assess the sensory and affective dimensions of pain.30 It includes 11 sensory descriptors and 4 affective descriptors, each rated from 0 to 3, yielding a total Pain Rating Index ranging from 0 to 45. Higher scores reflect more severe pain and greater affective distress. This questionnaire is particularly useful for characterizing the qualitative features of pain and the subjective pain experience in patients with trigeminal neuralgia. It has previously been used in the assessment of TN and related facial pain conditions.31 Assessments will be conducted at baseline and weeks 2, 4, and 8.
Changes Value in the Self-Rating Anxiety Scale (SAS)
The SAS is a self-report instrument used to assess the severity of anxiety symptoms. The raw score is multiplied by 1.25 to obtain a standard score ranging from 25 to 100. According to commonly used Chinese criteria, a standard score of ≥50 indicates clinically significant anxiety. Higher scores reflect more severe symptoms.32 Assessments will be conducted at baseline and weeks 2, 4, and 8.
Changes Value in the Self-Rating Depression Scale (SDS)
The SDS evaluates the severity of depressive symptoms. Similar to the SAS, the raw score is multiplied by 1.25 to derive a standard score ranging from 25 to 100. Based on Chinese normative data, a standard score of ≥53 indicates clinically significant depression. Higher scores reflect more severe symptoms.33 Assessments will be conducted at baseline and weeks 2, 4, and 8.
Biochemical Outcomes
Venous blood samples will be collected to explore the potential neuroimmunological mechanisms underlying the intervention. Specifically, 5 mL of venous blood will be obtained from each participant in the morning at baseline and at the end of week 2. The samples will then be processed according to standard operating procedures, stored at −80°C, and assayed in duplicate by investigators blinded to group allocation.
- IL-6: Plasma IL-6 concentrations (pg/mL) will be measured using enzyme-linked immunosorbent assay (ELISA) to assess neuroinflammation.
- 5-HT: Plasma 5-HT levels (ng/mL) will be measured using ELISA to evaluate neurotransmitter regulation.
Safety Evaluation
Incidence of Treatment-Related Adverse Events (AEs)
Safety will be rigorously evaluated by continuously monitoring the incidence of treatment-related AEs from baseline up to week 8. Comprehensive safety profiling will encompass three main domains: (1) acupuncture-related events, including severe needling pain, subcutaneous hematoma, syncope, and needle-site complications; (2) CBZ-associated adverse reactions, encompassing neurological/cognitive symptoms, gastrointestinal distress, visual disturbances, and systemic reactions; and (3) laboratory abnormalities. Specifically, clinically significant alterations in liver function tests (LFT) and renal function tests (RFT), assessed at baseline and the end of week 2, will be documented as AEs. All untoward events will be systematically recorded in the case report forms, categorized by severity, and managed according to standard clinical practice. In addition, whether the participant continues in the trial, discontinues the intervention, or withdraws from the study because of the AE will be documented in detail.
Assessment of Treatment Expectancy and Adherence
Prior to the initial acupuncture session, participants’ treatment expectancy will be evaluated using a 6-point Likert scale (ranging from 0 to 5), with higher scores indicating greater confidence in therapeutic efficacy. Participants reporting no belief in acupuncture will be requested to provide written justification for their skepticism. At the end of week 2, upon completion of the acupuncture intervention, treatment adherence will be evaluated based on session attendance and calculated as: Adherence Rate = (number of completed sessions / total prescribed sessions) × 100%.
Blinding Evaluation
Regarding blinding integrity assessment, participants will be queried at the conclusion of the second week following acupuncture intervention to identify their group allocation perception (true acupuncture, sham acupuncture, or uncertain), with comparative analysis of the distribution percentages between study arms.
Data Collection and Management
Data will be collected and recorded using standardized case report forms (CRFs) by trained assessors who are blinded to group allocation. Follow-up assessments will be conducted through an internet-based follow-up platform. Trained data management staff, who are also blinded to treatment allocation, will subsequently enter the data from the CRFs for statistical analysis.
Quality Control
A standardized operating procedure for acupuncture will be established prior to trial initiation. All treatments will be delivered by practitioners with at least three years of independent clinical experience. Investigators from the three sites attended a centralized training session to ensure consistency in intervention delivery and outcome assessment. Data collection and verification will be performed by trained study personnel and overseen by an independent data management company. To control inter-site variability, monthly on-site monitoring and quarterly multicenter audits will be conducted throughout the trial. An independent Data and Safety Monitoring Board, comprising a neurologist, an acupuncturist, and a statistician unassociated with the trial, will be established to periodically review cumulative safety data and ensure the ongoing validity and integrity of the trial.
Statistical Methods
Sample Size
Based on response rates observed in our prior study19—40% (2/5) in the sham EA plus CBZ group and 67% (2/3) in the EA plus placebo group—we estimated that approximately 105 participants in total would provide 80% power to detect a between-group difference of 27 percentage points at a two-sided α of 0.05. The sample size calculation was performed using PASS software (version 15.0, NCSS, LLC). After increasing the estimated sample size by 20% to account for potential dropout, the final target sample size will be 126 participants in total, with 63 participants in each group. These response estimates were obtained from our previous randomized trial;19 however, the small preliminary sample may introduce uncertainty in the assumed effect size.
Statistical Analysis
De-identified outcome data will be analyzed by an independent statistician blinded to group assignments using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Efficacy analyses will be conducted on both the intention-to-treat (ITT) population and the per-protocol (PP) population (participants completing ≥ 8 of 10 acupuncture sessions and the week-2 primary assessment).
Continuous data will be presented as the mean (standard deviation, SD) or median (interquartile range, IQR), and categorical data as frequencies and percentages. Baseline characteristics and independent continuous outcomes will be compared between groups using the Student’s t-test or Mann–Whitney U-test, as appropriate. Categorical variables will be analyzed using the Chi-square test or Fisher’s exact test. For continuous outcomes measured repeatedly over time, linear mixed-effects models (LMM) will be utilized to assess fixed effects (treatment group, time, and group-by-time interaction) while adjusting for baseline covariates and within-subject correlations. Generalized estimating equations (GEE) or appropriate nonparametric tests will be applied for repeated non-continuous or ordinal data. Missing data will be addressed using multiple imputation methods. All statistical tests will be two-sided, with a pre-specified significance level of p < 0.05. Exploratory analyses will not be adjusted for multiple comparisons and will be interpreted as hypothesis-generating.
Discussion
TN is a debilitating neuropathic pain disorder in which recurrent paroxysmal attacks not only cause severe physical suffering but also trigger a cascade of psychological consequences.34 Unlike many other chronic pain conditions, TN is uniquely characterized by the unpredictable, stimulus-evoked nature of its attacks, which generates persistent anticipatory fear and avoidance behavior, progressively restricting patients’ daily activities such as eating, speaking, and facial hygiene.35 This behavioral withdrawal, compounded by ongoing pain, contributes to a high prevalence of comorbid anxiety and depression, and these negative emotional states often intensify as pain progresses, while in turn aggravating pain symptoms and perpetuating a vicious cycle.36 Current pharmacological management with CBZ, though often effective initially, is frequently limited by poor long-term tolerability. Real-world data indicate that adverse effects occur in approximately 43.6% of CBZ-treated patients, and cohort studies suggest that side effects may necessitate dose reduction or treatment withdrawal in a substantial minority of cases.37 Surgical approaches, while offering sustained relief for selected patients, are constrained by strict eligibility criteria and procedure-related morbidity.38 This therapeutic gap—particularly for patients maintained on suboptimal medication doses due to tolerability constraints—provided the primary motivation for the current trial, which was designed to evaluate a short-term EA regimen within a double-simulation comparison with CBZ-based treatment for TN.
The rationale for investigating EA in this context is grounded in accumulating clinical and mechanistic evidence. A large-scale individual patient data meta-analysis including over 20,000 patients established that acupuncture produces clinically meaningful analgesic effects in chronic pain that persist beyond the treatment period.39 In TN, several meta-analyses have suggested that acupuncture or EA may reduce pain intensity compared with CBZ alone, although the quality of included trials was generally rated low.40 Mechanistically, EA exerts analgesic effects through promotion of endogenous opioid release, suppression of glial cell-mediated neuroinflammation, and modulation of descending inhibitory pathways.41 Building on this evidence base, our group previously conducted a randomized controlled trial demonstrating that a 4-week EA regimen was efficacious for TN compared to fixed-dose CBZ.19 However, that trial employed a standardized CBZ dose (300 mg/day) that does not reflect individualized dose titration in clinical practice, and did not comprehensively assess psychological outcomes or explore underlying biomarker changes. The current trial was specifically designed to address these limitations by comparing the EA plus placebo group with the sham EA plus CBZ group under patients’pre-existing individualized CBZ dosing schedules, while incorporating psychological assessments and measuring neuro-immune biomarkers.
The acupoint selection in this trial was designed to reflect the neuroanatomical specificity of TN. The core local points—ST2, ST7, and ST4—are all located within the trigeminal nerve distribution territory on the affected side, enabling direct stimulation of the peripheral branches involved in nociceptive transmission. Notably, a branch-specific supplementation strategy was adopted: GB1 for the ophthalmic branch, SI18 for the maxillary branch, and ST6 for the mandibular branch. This individualized approach allows the intervention to target the specific trigeminal division responsible for each patient’s pain, which is clinically important given that the maxillary and mandibular branches are affected in the vast majority of TN cases, while isolated ophthalmic involvement is rare.34 Among the local points, ST7 deserves particular attention: it is anatomically situated at the depression anterior to the mandibular condyle, in close proximity to the mandibular nerve trunk as it exits the foramen ovale, and is one of the most frequently reported acupoints for TN treatment in published clinical trials.42,43 For distal points, LI4 and TE5 were selected bilaterally. LI4 is classically indicated for orofacial pain conditions and has been shown to modulate pain processing in the trigeminal system.44 TE5 is traditionally paired with local facial points to enhance analgesic effects in head and face disorders.45
The outcome measures were selected to capture the multidimensional burden of TN and to align with TN-specific clinical characteristics. The VAS-based primary endpoint was chosen not only for its established validity in neuropathic pain assessment,46 but also because the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) consensus identifies this threshold as representing clinically meaningful improvement.47 Critically, TN pain is paroxysmal and fluctuates substantially within and between days; a single cross-sectional pain rating may therefore fail to capture the true disease burden. For this reason, daily pain diaries recording attack frequency, intensity, and rescue medication consumption were incorporated to provide a longitudinal, ecologically valid representation of symptom control—an approach endorsed by current pain-trial methodology.25 The BPI-Facial was specifically selected over the generic BPI because TN-related functional interference concentrates on orofacial activities that are not adequately captured by generic pain interference scales; the BPI-Facial has been validated in TN populations with established clinically important difference thresholds.29 The SAS and SDS were included because, unlike generic quality-of-life instruments, they specifically quantify affective symptom severity and have demonstrated sensitivity to change in pain intervention studies.48,49 Plasma IL-6 and 5-HT were selected as exploratory biomarkers based on their specific relevance to TN pathophysiology rather than as generic inflammatory markers. IL-6 upregulation has been directly demonstrated in trigeminal ganglia in TN animal models,50 contributing to nociceptive sensitization, while 5-HTTLPR polymorphisms have been specifically associated with TN susceptibility.13 This biomarker strategy was designed to generate preliminary mechanistic hypotheses linking pain relief with affective symptom changes, acknowledging that peripheral markers provide indirect evidence of central processes.
Several additional methodological considerations merit discussion. First, the dose-anchored eligibility criterion (CBZ 200–400 mg/day) was adopted to address a design limitation specific to TN trials: because observed pain intensity is inherently conditioned on concurrent anticonvulsant exposure, conventional pain-cutoff enrollment may inadvertently select patients at heterogeneous points on their dose-response curves. Anchoring eligibility to a defined dose range reduces this confounding and ensures a clinically homogeneous population of patients with ongoing tolerability constraints. Second, the double-simulation design (EA plus placebo medication versus sham EA plus active CBZ) was implemented to maintain blinding integrity while enabling a direct comparison between two active treatment strategies. Third, rescue medication is permitted to reflect real-world practice; accordingly, the primary estimate represents the effectiveness of each assigned strategy under pragmatic conditions. Fourth, blinding will be formally evaluated using a blinding assessment index, with expectancy assessment incorporated to contextualize subjective outcomes, as complete blinding remains a recognized methodological challenge in acupuncture trials. Because active EA may generate perceptible needling and electrical sensations that are difficult to fully mimic, the blinding assessment and treatment expectancy ratings will be used to contextualize the interpretation of subjective outcomes.
This study has several limitations. First, although this is a multicenter trial, all three participating centers are located within Zhejiang Province, which may introduce geographic bias and limit the generalizability of the findings. Future studies should expand the trial network to more diverse regions. Second, the assessment of treatment efficacy relies predominantly on patient-reported outcomes. While plasma biomarkers were incorporated to provide objective biological evidence, the sensitivity of these peripheral markers in reflecting central neuropathological changes requires further validation. Future research should consider integrating neuroimaging modalities such as functional MRI to enable evaluation across neural circuit levels, thereby strengthening the mechanistic interpretability of treatment effects. In addition, the relatively short 2-week intervention period may limit the evaluation of longer-term durability, although follow-up assessments at weeks 4 and 8 are included. Moreover, the double-simulation design involves temporary CBZ placebo substitution in the EA plus placebo group, which may introduce potential bias related to medication manipulation; therefore, rescue medication use and pain diary data will be considered when interpreting pain-related outcomes. Despite these limitations, this trial is expected to provide clinical evidence for the application of EA in TN management and inform the design of future confirmatory trials.
Abbreviations
TN, Trigeminal neuralgia; EA, Electroacupuncture; CBZ, Carbamazepine; VAS, Visual Analog Scale; PGIC, Patient Global Impression of Change; BPI-Facial, Brief Pain Inventory–Facial; SF-MPQ, Short-Form McGill Pain Questionnaire; SAS, Self-Rating Anxiety Scale; SDS, Self-Rating Depression Scale; IL-6, Plasma Interleukin-6; 5-HT, Plasma Serotonin; CRFs, Case report forms; LMM, Linear mixed-effects models; GEE, Generalized estimating equations; mITT, modified Intention-To-Treat; PP, Per-Protocol.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the lead ethics committee at the Third Affiliated Hospital of Zhejiang Chinese Medical University (approval No. ZSLL-KY-2025-040-05) and from each participating site: Pingyang County Hospital of Traditional Chinese Medicine (approval No. I2026-011-01) and Jiaxing Hospital of Traditional Chinese Medicine (approval No. S1-2025-0024-4). The trial was prospectively registered with ClinicalTrials.gov (NCT06977932). Furthermore, the trial will be conducted in accordance with the Declaration of Helsinki and applicable Chinese regulations, with written informed consent obtained from all participants.
Acknowledgments
We thank all participants who will be involved in this trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received funding from several sources: the Major Project (Grant No. GZX-KJS-ZJ-2025-006) and its associated Sub-project (Grant No. 2025ZS043) under the 2025 Joint TCM Science & Technology Program of the National Demonstration Zones for Comprehensive TCM Reform, along with the Hangzhou Natural Science Foundation (Grant No. 2025SZRJJ0464) for the year 2026.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jiao Y, Wang X, Cai L, Ceccato GHW, Chen G. Combined application of arachnoid membrane and petrosal dura to transpose dual offending arteries in microvascular decompression for trigeminal neuralgia: two-dimensional operative video. World Neurosurg. 2020;137:415. doi:10.1016/j.wneu.2020.02.029
2. Ashina S, Robertson CE, Srikiatkhachorn A, et al. Trigeminal neuralgia. Nat Rev Dis Primers. 2024;10(1):39. doi:10.1038/s41572-024-00523-z
3. Cruccu G, Di Stefano G, Truini A. Trigeminal Neuralgia. N Engl J Med. 2020;383(8):754–14. doi:10.1056/NEJMra1914484
4. Martinelli R, Vannuccini S, Burattini B, et al. Psychological assessment in patients affected by trigeminal neuralgia. A systematic review. Neurosurg Rev. 2025;48(1):414. doi:10.1007/s10143-025-03556-4
5. Chisari CG, Sgarlata E, Arena S, D’Amico E, Toscano S, Patti F. An update on the pharmacological management of pain in patients with multiple sclerosis. Expert Opin Pharmacother. 2020;21(18):2249–2263. doi:10.1080/14656566.2020.1757649
6. Di Stefano G, Truini A, Cruccu G. Current and innovative pharmacological options to treat typical and atypical trigeminal neuralgia. Drugs. 2018;78(14):1433–1442. doi:10.1007/s40265-018-0964-9
7. Liu Y, Tanaka E. Pathogenesis, diagnosis, and management of trigeminal neuralgia: a narrative review. J Clin Med. 2025;14(2). doi:10.3390/jcm14020528
8. Bal W, Łabuz-Roszak B, Tarnawski R, Lasek-Bal A. Effectiveness and safety of CyberKnife radiosurgery in treatment of trigeminalgia - experiences of Polish neurological and oncological centres. Neurol Neurochir Pol. 2020;54(1):28–32. doi:10.5603/PJNNS.a2020.0009
9. Uhl C, Vajkoczy P. Contact-free transposition and interposition techniques for trigeminal neuralgia: a systematic review. J Neurosurg Sci. 2023;67(1):36–45. doi:10.23736/s0390-5616.22.05514-x
10. Vieira WF, Coelho DRA, Litwiler ST, et al. Neuropathic pain, mood, and stress-related disorders: a literature review of comorbidity and co-pathogenesis. Neurosci Biobehav Rev. 2024;161:105673. doi:10.1016/j.neubiorev.2024.105673
11. Li M, She K, Zhu P, et al. Chronic pain and comorbid emotional disorders: neural circuitry and neuroimmunity pathways. Int J Mol Sci. 2025;26(2). doi:10.3390/ijms26020436
12. Rapisarda A, Baroni S, Gentili V, et al. The role of biomarkers in drug-resistant trigeminal neuralgia: a prospective study in patients submitted to surgical treatment. Neurol Sci. 2022;43(7):4425–4430. doi:10.1007/s10072-022-05971-7
13. Cui W, Yu X, Zhang H. The serotonin transporter gene polymorphism is associated with the susceptibility and the pain severity in idiopathic trigeminal neuralgia patients. J Headache Pain. 2014;15(1):42. doi:10.1186/1129-2377-15-42
14. Zhang C, Wu Z, Fan W, et al. Comparison of the effects of acupuncture and drug treatment for central post-stroke pain: a systematic review and network meta-analysis of randomized trials. Behav Brain Res. 2026;499:115936. doi:10.1016/j.bbr.2025.115936
15. Lan L, Wang L, Sadeghirad B, et al. Acupuncture for the management of chronic diabetic peripheral neuropathy: a systematic review and meta-analysis of randomized controlled trials. Curr Pain Headache Rep. 2025;29(1):74. doi:10.1007/s11916-025-01386-z
16. Edwards JW, Shaw V. Acupuncture in the management of trigeminal neuralgia. Acupunct Med. 2021;39(3):192–199. doi:10.1177/0964528420924042
17. Hu X, Pan Y, Tang Y, et al. Efficacy and safety of electroacupuncture-based comprehensive treatment for post-stroke depression: a systematic review and meta-analysis of randomized controlled trials. Front Psychiatry. 2025;16:1610032. doi:10.3389/fpsyt.2025.1610032
18. Sator-Katzenschlager SM, Scharbert G, Kozek-Langenecker SA, et al. The short- and long-term benefit in chronic low back pain through adjuvant electrical versus manual auricular acupuncture. Anesth Analg. 2004;98(5):1359–1364. doi:10.1213/01.ane.0000107941.16173.f7
19. Li R, Sun J, Luo K, et al. Electroacupuncture and carbamazepine for patients with trigeminal neuralgia: a randomized, controlled, 2 × 2 factorial trial. J Neurol. 2024;271(8):5122–5136. doi:10.1007/s00415-024-12433-x
20. Chan AW, Boutron I, Hopewell S, et al. SPIRIT 2025 statement: updated guideline for protocols of randomised trials. BMJ. 2025;389:e081477. doi:10.1136/bmj-2024-081477
21. Hopewell S, Chan AW, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomized trials. JAMA. 2025;333(22):1998–2005. doi:10.1001/jama.2025.4347
22. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. PLoS Med. 2010;7(6):e1000261. doi:10.1371/journal.pmed.1000261
23. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
24. Wu CJ, Lian YJ, Zheng YK, et al. Botulinum toxin type A for the treatment of trigeminal neuralgia: results from a randomized, double-blind, placebo-controlled trial. Cephalalgia. 2012;32(6):443–450. doi:10.1177/0333102412441721
25. Nova CV, Zakrzewska JM, Baker SR, Riordain RN. Treatment outcomes in trigeminal neuralgia-a systematic review of domains, dimensions and measures. World Neurosurg X. 2020;6:100070. doi:10.1016/j.wnsx.2020.100070
26. Chong MS, Bahra A, Zakrzewska JM. Guidelines for the management of trigeminal neuralgia. Cleve Clin J Med. 2023;90(6):355–362. doi:10.3949/ccjm.90a.22052
27. Obermann M, Yoon MS, Sensen K, Maschke M, Diener HC, Katsarava Z. Efficacy of pregabalin in the treatment of trigeminal neuralgia. Cephalalgia. 2008;28(2):174–181. doi:10.1111/j.1468-2982.2007.01483.x
28. Wu S, Lian Y, Zhang H, et al. Botulinum Toxin Type A for refractory trigeminal neuralgia in older patients: a better therapeutic effect. J Pain Res. 2019;12:2177–2186. doi:10.2147/jpr.S205467
29. Lee JY, Chen HI, Urban C, et al. Development of and psychometric testing for the Brief Pain Inventory-Facial in patients with facial pain syndromes. J Neurosurg. 2010;113(3):516–523. doi:10.3171/2010.1.Jns09669
30. Melzack R. The short-form McGill pain questionnaire. Pain. 1987;30(2):191–197. doi:10.1016/0304-3959(87)91074-8
31. Melzack R, Terrence C, Fromm G, Amsel R. Trigeminal neuralgia and atypical facial pain: use of the McGill pain questionnaire for discrimination and diagnosis. Pain. 1986;27(3):297–302. doi:10.1016/0304-3959(86)90157-0
32. Yin W, Pang L, Cao X, et al. Factors associated with depression and anxiety among patients attending community-based methadone maintenance treatment in China. Addiction. 2015;110 Suppl 1:51–60. doi:10.1111/add.12780
33. Dunstan DA, Scott N. Clarification of the cut-off score for Zung’s self-rating depression scale. BMC Psychiatry. 2019;19(1):177. doi:10.1186/s12888-019-2161-0
34. Araya EI, Claudino RF, Piovesan EJ, Chichorro JG. Trigeminal neuralgia: basic and clinical aspects. Curr Neuropharmacol. 2020;18(2):109–119. doi:10.2174/1570159x17666191010094350
35. Zakrzewska JM, Wu J, Mon-Williams M, Phillips N, Pavitt SH. Evaluating the impact of trigeminal neuralgia. Pain. 2017;158(6):1166–1174. doi:10.1097/j.pain.0000000000000853
36. Melek LN, Devine M, Renton T. The psychosocial impact of orofacial pain in trigeminal neuralgia patients: a systematic review. Int J Oral Maxillofac Surg. 2018;47(7):869–878. doi:10.1016/j.ijom.2018.02.006
37. Di Stefano G, De Stefano G, Leone C, et al. Real-world effectiveness and tolerability of carbamazepine and oxcarbazepine in 354 patients with trigeminal neuralgia. Eur J Pain. 2021;25(5):1064–1071. doi:10.1002/ejp.1727
38. Henson CF, Goldman HW, Rosenwasser RH, et al. Glycerol rhizotomy versus gamma knife radiosurgery for the treatment of trigeminal neuralgia: an analysis of patients treated at one institution. Int J Radiat Oncol Biol Phys. 2005;63(1):82–90. doi:10.1016/j.ijrobp.2005.01.033
39. Vickers AJ, Vertosick EA, Lewith G, et al. Acupuncture for chronic pain: update of an individual patient data meta-analysis. J Pain. 2018;19(5):455–474. doi:10.1016/j.jpain.2017.11.005
40. Hu H, Chen L, Ma R, Gao H, Fang J. Acupuncture for primary trigeminal neuralgia: a systematic review and PRISMA-compliant meta-analysis. Complement Ther Clin Pract. 2019;34:254–267. doi:10.1016/j.ctcp.2018.12.013
41. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/aln.0000000000000101
42. Meltz L, Ortiz D, Chiang P. The anatomical relationship between acupoints of the face and the trigeminal nerve. Med Acupunct. 2020;32(4):181–193. doi:10.1089/acu.2020.1413
43. He Y, Li L, Zhou M, et al. Analysis of acupoint selection and combinations in acupuncture treatment of trigeminal neuralgia: a protocol for data mining. J Pain Res. 2025;18:3373–3381. doi:10.2147/jpr.S533617
44. Zhou M, Zhang Q, Huo M, et al. The mechanistic basis for the effects of electroacupuncture on neuropathic pain within the central nervous system. Biomed Pharmacother. 2023;161:114516. doi:10.1016/j.biopha.2023.114516
45. Sun J, Li R, Li X, et al. Electroacupuncture therapy for change of pain in classical trigeminal neuralgia. Medicine. 2020;99(16):e19710. doi:10.1097/md.0000000000019710
46. Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing numerical rating scales, verbal rating scales, and visual analogue scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011;41(6):1073–1093. doi:10.1016/j.jpainsymman.2010.08.016
47. Dworkin RH, Turk DC, Wyrwich KW, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;9(2):105–121. doi:10.1016/j.jpain.2007.09.005
48. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
49. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/s0033-3182(71)71479-0
50. Liu M, Li Y, Zhong J, Xia L, Dou N. The effect of IL-6/Piezo2 on the trigeminal neuropathic pain. Aging. 2021;13(10):13615–13625. doi:10.18632/aging.202887
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combination Treatment with Thread-Embedding Acupuncture and Electroacupuncture for Knee Osteoarthritis Patients with Postoperative Pain: A Randomized Controlled Feasibility Study
Lee YJ, Han CH, Jeon JH, Kim E, Park KH, Kim AR, Kim YI
Journal of Pain Research 2025, 18:89-103
Published Date: 8 January 2025
A Randomized, Sham-Controlled Trial on the Efficacy and Safety of Electroacupuncture for Lumbar Disc Herniation with Radiculopathy: Rationale and Study Protocol
Yang Y, Liu L, Yuan L, Liu X, Ding H, Zhou X, Cao Q
Journal of Pain Research 2025, 18:2307-2319
Published Date: 5 May 2025
The Clinical Effect of Electroacupuncture Combined with Surround Needling in the Treatment of Acute Lateral Ankle Sprain Based on Musculoskeletal Ultrasound Imaging Technology: A Protocol for a Single-Centre, Randomized, Controlled Trial
Chen L, Hu Q, Gao H, Tang D
Journal of Pain Research 2025, 18:2467-2478
Published Date: 15 May 2025
Effect of Telemedicine-Supported Structured Exercise Program in Patients with Chronic Low Back Pain: Study Protocol for a Randomized Controlled Trial
Feng Y, Jia C, Liu H, Bao T, Wang C, Wang Z, Huang J, Jiang Y, Wang X, Zhang R, Zhang Y, Zhang S, Zhu S, He C
Journal of Pain Research 2025, 18:2809-2822
Published Date: 7 June 2025
Electro-Acupuncture for Diminished Ovarian Reserve: Protocol for a Randomized, Placebo-Controlled Trial
Tang H, Wang JX, Zheng SZ, Jia YF, Yu X, Zhao NN, Yang YH, Lin LP, Li SY, Zhao H
Journal of Multidisciplinary Healthcare 2025, 18:4341-4352
Published Date: 30 July 2025