Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
A Brief and Effective Questionnaire for COPD Screening in High-Altitude Areas
Authors Cui J, Wang Y, Tong Y, Liao Y ![]() , Liu Y, Chai D, Xing Z, Long H
, Liu Y, Chai D, Xing Z, Long H ![]() , Guo Y
, Guo Y
Received 11 November 2024
Accepted for publication 31 March 2025
Published 26 April 2025 Volume 2025:20 Pages 1239—1248
DOI https://doi.org/10.2147/COPD.S505941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Jia Cui,1 Yuxia Wang,1 Yaqi Tong,1 Yixuan Liao,1 Yan Liu,1 Di Chai,1 Zhenzhen Xing,2 Huanyu Long,3 Yanfei Guo1
1Department of Respiratory and Critical Care Medicine, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing Hospital, Beijing, 100730, People’s Republic of China; 2Research Center of Occupational Medicine, Peking University Third Hospital, Beijing, 100191, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, Peking University Third Hospital, Beijing, 100191, People’s Republic of China
Correspondence: Yanfei Guo, Department of Respiratory and Critical Care Medicine, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing Hospital, Beijing, 100730, People’s Republic of China, Tel +86-13601173230, Email [email protected]
Purpose: To develop a reliable screening questionnaire for chronic obstructive pulmonary disease (COPD) for primary health care institutions in high-altitude areas.
Patients and Methods: This was a large cross-sectional study. The study included individuals who resided at an altitude of more than 2100 meters, were aged 35 years or older. The data were randomly divided into a development set and a validation set at a ratio of 7:3. Single-factor and multifactor logistic regression equations were employed to identify pertinent variables and construct a scoring system. The receiver operating characteristic (ROC) curve, area under the curve (AUC), positive predictive value (PPV) and negative predictive value (NPV) were used to evaluate the discriminative ability of the questionnaire.
Results: A total of 2909 individuals were included in this study, including 1304 males (44.83%), with a median age of 47.00 (41.00– 55.00) years. A multivariate analysis of the development set revealed that five variables (age, history of pulmonary tuberculosis, smoking status, household air pollution exposure and CPOD Assessment Test (CAT) score) were significantly correlated with COPD. A scoring system was constructed on the basis of these findings. The AUC for the model in the development set was 0.714, whereas that for the validation set was 0.726. ROC analysis indicated that the optimal diagnostic cutoff value for the score was 22 points, with a sensitivity of 85.0% and a specificity of 48.4%. The results indicated that the sensitivity of the model was the highest (87.3%) at altitudes between 2100 and 3000 meters, whereas the specificity was the highest (80.9%) at altitudes > 4000 meters. The conclusions were essentially consistent when the lower limit of normal (LLN) was used to verify the values in different altitude areas.
Conclusion: The COPD screening questionnaire effectively screens COPD in high-altitude primary healthcare settings.
Keywords: chronic obstructive pulmonary disease, screening, questionnaire, primary care, high-altitude
Introduction
Chronic obstructive pulmonary disease (COPD) is a common disease that is characterized by persistent respiratory symptoms and airflow limitation.1 The prevalence of COPD was reported to be 13.7% in adults aged 40 years and older according to the China Pulmonary Health (CPH) study, although only 2.6% were aware of their condition.2 COPD is the third leading cause of death globally.3 Early diagnosis is key to managing COPD.4 Many international guidelines emphasize the importance of case identification in primary care settings.1,5
Although spirometry is recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) for the diagnosis of COPD, spirometers are often inaccessible in most primary care units in low- to middle-income areas. The Chinese Guidelines for COPD recommend that questionnaire screening should first be conducted in primary healthcare facilities to identify high-risk individuals. Numerous COPD screening questionnaires have been developed on the basis of symptoms and risk factors, such as the Self-Scored COPD Population Screener Questionnaire (COPD-PS)6 and COPD Screening Questionnaire (COPD-SQ).7 The majority of questionnaires have been designed for populations residing at sea level. Consequently, these questionnaires may not be suitable for high-altitude areas because of the presence of different risk factors (eg, biomass smoke exposure and tuberculosis (TB) are significant risk factors for COPD in Tibet) and cultural variations.8
More than 400 million people worldwide reside at elevations above 1,500 meters.9 COPD is also prevalent in high-altitude regions, with a reported prevalence rate of 6.1% to 15.6%.8,10–13 Low-pressure hypoxia is associated with rapid disease progression and a high mortality rate among patients with COPD in high-altitude areas. China has many high-altitude areas with large populations and poor economic conditions. These areas have low rates of spirometry use owing to environmental and medical limitations. It is thus crucial to facilitate early diagnosis and treatment for patients with COPD.
This study aimed to develop a simple and reliable questionnaire for the screening of COPD in primary health care settings in high-altitude areas.
Methods
Design and Population
This was a large cross-sectional, population-based study of cardiac and pulmonary health among adults in Tibet and the Xinjiang Uygur Autonomous Region. Details have been reported elsewhere.8 In brief, a multistage stratified sampling procedure was employed to select a representative sample of individuals residing at altitudes between 2,100 and 4,700 meters. A more comprehensive investigation of cardiopulmonary disease was conducted among individuals aged 35 years and older. Moreover, similar studies have been conducted. This analysis included permanent residents (those living in their current residence for a period exceeding one year) aged 35 years or older (Supplemental Figure 1). The exclusion criteria were defined as follows: 1) current tuberculosis therapy; 2) resting blood pressure exceeding 180/120 mmHg or heart rate greater than 120 beats per minute; 3) history of myocardial infarction or cerebrovascular events within three months preceding enrollment; 4) pregnancy; and 5) any contraindications to spirometry performance, including but not limited to recent thoracic/abdominal surgical procedures, ocular surgery, or diagnosed retinal detachment.
The study involved human participants and was approved by the Institutional Review Board and Ethics Committee of Beijing Hospital (2013BJYYEC-042C-01). The participants provided informed consent to participate before taking part in the study.
A standardized questionnaire was administered by experienced interviewers to obtain data regarding demographic characteristics, living conditions, respiratory symptoms, medical history, and potential risk factors for COPD. The questionnaire was developed by the project expert group, and all the interviewers received unified training in Mandarin and the local languages. The mean altitudes were obtained from the local government.
Pulmonary function tests were performed by trained technicians in all the included study participants by using a MasterScreenTM Pneumo PC spirometer (CareFusion, Yorba Linda, California) in accordance with the American Thoracic Society/European Respiratory Society (ATS/ERS) recommendations.14 Each participant underwent the same procedure twice, before and after receiving a bronchodilator (BD) (400 µg of salbutamol through a 500 mL spacer). Forced expiratory maneuvers were performed three to eight times until the forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) were reproducible within 150 mL.15 The acceptability of FVC and FEV1 values was evaluated according to the grading system proposed by Enright et al (A-F).15 Grades of A, B or C were considered acceptable for analysis.
COPD was defined as a postbronchodilator FEV1/FVC ratio <0.70, on the basis of the GOLD guidelines.1 For sensitivity and specificity analysis, the lower limit of normal (LLN) of the reference value was also utilized.16
The detailed definitions have been previously reported.8,17 In brief, post-TB lung disease was defined as the presence of pulmonary TB sequalae on chest radiographs and/or a positive medical history of TB. Exposure to household air pollution was defined as the use of wood, animal waste, or coal for cooking or heating during the previous 6 months or longer. Occupational exposure history was defined as working in a workplace with dust or harmful gases for more than 3 months.
Statistical Analysis
The characteristics of the two sets are described as the number (proportion) or the mean ± standard deviation (M (1/4, 3/4)) where appropriate, and a chi-square test or T/rank-sum test was used for comparisons. The observed difference was considered statistically significant at P < 0.05.
In this study, the data were divided into a training set and a verification set at a 7:3 ratio. The factors with the best predictive efficiency were determined via stepwise multivariate logistic regression on the basis of the Akaike information criterion (AIC). The Youden index was then employed to determine the optimal cutoff point of the model scoring system. The discrimination of the scoring system was evaluated through the presentation of the receiver operating characteristic (ROC) curve and area under the curve (AUC), as well as the calculation of the accuracy, positive predictive value, and negative predictive value for the development set and validation set.
Results
Characteristics of the Study Population
A total of 2909 individuals who had information on key variables, were older than 35 years and were permanent residents were included in this study. A total of 294 (10.11%) participants were identified as having COPD via spirometry, 150 (51.02%) participants were male, and the mean age was 52.00 (44.00–61.75) years (supplemental table 1).
After random splitting at a 7:3 ratio, 2037 individuals were assigned to the development set, and 872 were assigned to the validation set. There were 900 (44.18%) males, and the mean age was 47.00 (41.00–55.00) years, with 10.51% of the participants in the development cohort having COPD. A total of 404 (46.33%) males were included, and the mean age was 47.00 (41.00–54.00) years, with 9.17% of the participants in the validation cohort having COPD. No significant difference was observed in any risk factor between the two sets (Table 1).
 |
Table 1 Comparison of Characteristics Between the Development and Validation Datasets |
Item Selection and Scoring
The results of univariate logistic regression analysis demonstrated that sex, age, body mass index (BMI), history of tuberculosis, household air pollution exposure, smoking status, CAT score, and history of asthma were risk factors for the diagnosis of COPD (P < 0.1). After excluding collinearity among the factors, the above factors were included in the multivariate logistic regression equation. Five variables, including age, a history of TB, household air pollution exposure, smoking history and the CAT score, were significantly independently associated with COPD in the development set after stepwise selection via a multivariate logistic model. These variables were used to develop the predictive score according to their odds ratios. After the minimum score was determined, a score was assigned for each variable (Table 2).
 |
Table 2 Results of Logistic Regression and Scores in the Development Set |
When the questionnaire was used to screen for COPD according to the GOLD diagnostic criteria, the corresponding AUC was 0.714 (95% CI 0.68–0.748) in the development set and 0.726 (95% CI 0.667–0.784) in the validation set (Figure 1). The sensitivity, specificity, PPV and NPV were 0.85, 0.48, 0.162 and 0.965, respectively (Table 3), at the cutoff score of 22, which yielded the largest AUC and a balance between sensitivity and specificity.
 |
Table 3 Accuracy and Positive and Negative Predictive Values for COPD Across Different Score Thresholds |
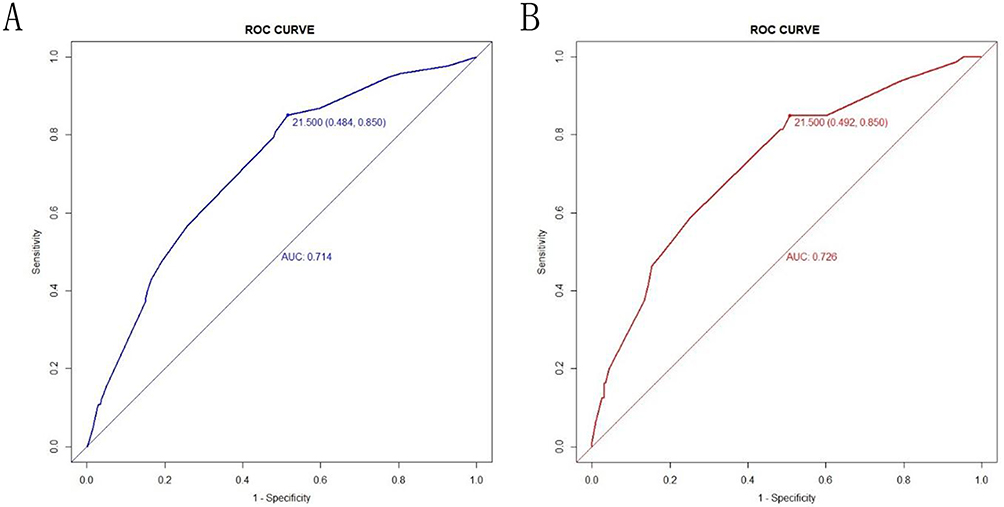 |
Figure 1 ROC curve for screening questionnaires in the development set (A) (AUC = 0.714) and validation set (B) (AUC = 0.726). Abbreviation: AUC, area under the curve. |
In addition, we tried to verify the efficacy of the model in regions at different altitude and reported that the model had the highest sensitivity of 0.873 in regions with altitudes of 2100–3000 meters, whereas the specificity was the highest in regions at altitudes >4000 meters, with a value of 0.809. The results of the screening questionnaire using the LLN as an alternative diagnostic criterion for COPD are shown in Figure 2.
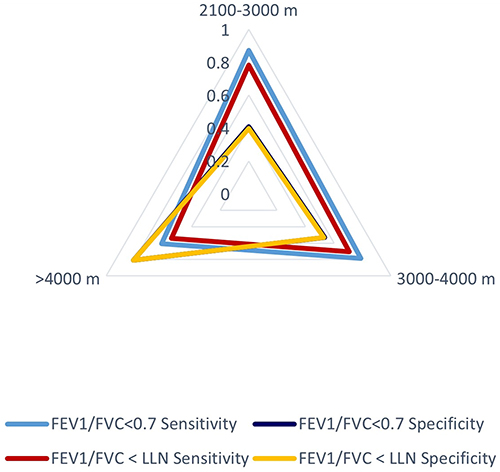 |
Figure 2 Validity of the performance of the screening questionnaire at the cutoff score of 22 in screening for airflow obstruction according to different diagnostic criteria and different altitudes. |
The predicted individual COPD probabilities according to the screening questionnaire score were estimated and are shown in Figure 3. The population was divided into two probability levels according to the probability of COPD occurrence: low probability and high probability.
 |
Figure 3 Individual COPD probabilities according to the screening questionnaire score with 95% confidence intervals. |
Discussion
In this study, a screening questionnaire was developed and validated as a COPD screening tool for residents living in high-altitude regions on the basis of a large cross-sectional spirometry dataset. The five-item scoring system is an effective and simplified method for identifying individuals at risk of COPD, with a recommendation for further lung function testing. The scoring system demonstrated acceptable validity, reliability, and a correct classification ratio for quick clinical or online COPD screening.
The early diagnosis and treatment of COPD has been shown to significantly improve symptoms and slow the annual decline in FEV1.18 Population-based screening for COPD has the potential to be cost effective in China. It is estimated that COPD screening could prevent 0.39–8.10% of COPD-related deaths and 0.58–2.70% of COPD exacerbations.19 Unfortunately, our previous study indicated that only 1.1% of patients diagnosed with COPD were previously aware of their diagnosis.8 The COPD screening questionnaire is an economical tool that plays an important role in the screening of COPD in primary care settings. Numerous questionnaires have been developed on the basis of symptoms and risk factors, with sensitivities ranging from 54% to 86% and specificities ranging from 40% to 85.2%.6,7,20–24 However, the results of their external verification were suboptimal.25 The sensitivity of the CAPTURE tool, which was developed on the basis of the American population, for the screening of clinically significant COPD in the primary health care population in the United States was found to be only 48.2%.26 Otherwise, the development of these questionnaires did not include individuals residing at high altitudes. Our present study was the only spirometry-defined COPD research among residents living in high-altitude regions using a rigorous sampling design and quality control, and for the first time, residents living over 4,000 meters above sea level were included. A previous study revealed that the risk factors and clinical characteristics of COPD differ between high-altitude regions and low-altitude regions.8 The development of a user-friendly screening questionnaire with high-altitude characteristics for COPD in primary health care settings is highly important.
Exposure to indoor air pollution is associated with an increased risk of COPD.27,28 An important source of indoor air pollution in domestic settings is biomass fuel used for cooking and heating in enclosed spaces.29 Approximately 2.6 billion people worldwide are exposed to polluting energy sources.28 More than half of the households in Xinjiang and Tibet rely on solid fuels for cooking and heating.30 In our study, 70.4% of the individuals were exposed to biomass fuel, whereas 28.22% were smokers, suggesting that indoor air pollution may be an important item for COPD screening.
TB is a major health problem in low- and middle-income countries. China is the third largest contributor to this global epidemic.31 Xinjiang and Tibet have the highest incidence rates of tuberculosis, with spatial clustering of cases observed in these areas.32 Previous research has demonstrated a correlation between a history of TB and the development of airflow obstruction, which is a defining characteristic of COPD. The prevalence of airflow obstruction in individuals with a history of TB is 1–3 times greater than that in those without a history of TB.33–36 Our research in Xinjiang and Xizang also revealed that 21.3% of patients with post-TB lung disease had airflow obstruction, an OR of airflow obstruction was found to be significantly associated with post-TB lung disease, following adjustment for other potential confounding factors (OR 1.31, 95% CI 1.05 to 1.62).17 Post-TB lung disease should be considered a potentially important cause of airflow obstruction, and the presence of this disease should be considered a high-risk factor for COPD in settings with a high TB burden.
Dyspnea is a characteristic symptom of COPD. However, the objective level of dyspnea is not correlated with patients’ perceptions of disease severity.37 Patients often adjust their activity levels to avoid reaching their tolerance limits and experiencing dyspnea. Furthermore, the specificity of exertional dyspnea is significantly reduced in high-altitude regions due to hypoxia. Patients are more likely to visit their physician when they experience fluctuations in respiratory symptoms or a decline in their quality of life.38 The CAT is a globally accepted measure of health status impairment in COPD patients.1,39 In addition to the typical symptoms of COPD, the CAT also encompasses aspects related to activity limitations. Therefore, the CAT is a more appropriate tool for identifying COPD-related symptoms in individuals living at high altitudes.
Smoking is a key environmental risk factor for COPD. Compared with nonsmokers, smokers present a greater prevalence of lung function abnormalities, a greater annual rate of decline in FEV1, and a greater COPD mortality rate.40 The prevalence of COPD is significantly increased in individuals who smoke more than 20 packs per year.2 Most screening questionnaires use the smoking index to evaluate smoking status.7,41, However, owing to the specific environment, living habits, and economic conditions, the use of pipes, cigars, water pipes, and other types of tobacco was common in this study. The use of types of tobacco has also been identified as risk factors for COPD.1 There are no quantitative indicators available to quantify the extent of this risk. Consequently, the questionnaire did not use the smoking index as a measure; rather, it utilized whether a participant had smoked as a screening item.
Some limitations should be acknowledged. First, the diagnosis of COPD was based on spirometry criteria alone, with no consideration of the patient’s clinical presentation or risk factors. Consequently, individuals with other obstructive pulmonary diseases, such as severe asthma, could have been misclassified. Second, the participants were required to self-report their risk factors (eg, smoking status and exposure to household air pollution), which may lead to recall bias. Third, only internal validation was performed, and external validation was also needed. However, it is uncommon to obtain such a substantial quantity of data in high-altitude regions. This study presents a simple method for identifying groups at high risk of COPD.
Conclusion
In conclusion, the screening questionnaire, which incorporates age, history of tuberculosis, household air pollution exposure, smoking status, and the CAT score, demonstrated has high discriminatory power and can be utilized for the preliminary screening of patients in primary health care institutions situated in high-altitude areas.
Ethics Approval and Informed Consent
The study involved human participants and was approved by the Institutional Review Board and Ethics Committee of Beijing Hospital (2013BJYYEC-042C-01). The participants provided informed consent to participate before taking part in the study. This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
National High Level Hospital Clinical Research Funding (BJ-2021-189).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Disease G I F C. Global strategy for prevention, diagnosis and management of COPD: 2024 report [EB/OL]. 2024. Available from: https://goldcopd.org/2024-gold-report/.
2. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China pulmonary health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
3. WHO. The top 10 causes of death [EB/OL]. 2020. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/the-top-10-causes-of-death.
4. Stolz D, Mkorombindo T, Schumann DM, et al. Towards the elimination of chronic obstructive pulmonary disease: a lancet commission. Lancet. 2022;400(10356):921–972. doi:10.1016/S0140-6736(22)01273-9
5. Hopkinson NS, Molyneux A, Pink J, Harrisingh MC. Chronic obstructive pulmonary disease: diagnosis and management: summary of updated NICE guidance. BMJ. 2019;366:14486.
6. Martinez FJ, Raczek AE, Seifer FD, et al. Development and initial validation of a self-scored COPD population screener questionnaire (COPD-PS). Copd. 2008;5(2):85–95. doi:10.1080/15412550801940721
7. Zhou YM, Chen SY, Tian J, et al. Development and validation of a chronic obstructive pulmonary disease screening questionnaire in China. Int J Tuberc Lung Dis. 2013;17(12):1645–1651. doi:10.5588/ijtld.12.0995
8. Guo Y, Xing Z, Shan G, et al. Prevalence and risk factors for COPD at high altitude: a large cross-sectional survey of subjects living between 2100-4700m above sea level. Front Med Lausanne. 2020;7:581763. doi:10.3389/fmed.2020.581763
9. Cohen JE, Small C. Hypsographic demography: the distribution of human population by altitude. Proc Natl Acad Sci USA. 1998;95(24):14009–14014. doi:10.1073/pnas.95.24.14009
10. Jaganath D, Miranda JJ, Gilman RH, et al. Prevalence of chronic obstructive pulmonary disease and variation in risk factors across four geographically diverse resource-limited settings in Peru. Respir Res. 2015;16(1):40. doi:10.1186/s12931-015-0198-2
11. Menezes AM, Perez-Padilla R, Jardim JR, et al. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet. 2005;366(9500):1875–1881. doi:10.1016/S0140-6736(05)67632-5
12. Caballero A, Torres-Duque CA, Jaramillo C, et al. Prevalence of COPD in five Colombian cities situated at low, medium, and high altitude (PREPOCOL study). Chest. 2008;133(2):343–349. doi:10.1378/chest.07-1361
13. Laniado-Laborin R, Rendón A, Batiz F, Alcantar-Schramm JM, Bauerle O. High altitude and chronic obstructive pulmonary disease prevalence: a casual or causal correlation? Arch Bronconeumol. 2012;48(5):156–160. doi:10.1016/j.arbres.2011.12.004
14. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
15. Enright P. FEV1 and FVC repeatability goals when performing spirometry. Prim Care Respir J. 2010;19(2):194. doi:10.4104/pcrj.2010.00031
16. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
17. Xing Z, Sun T, Janssens JP, et al. Airflow obstruction and small airway dysfunction following pulmonary tuberculosis: a cross-sectional survey. Thorax. 2023;78(3):274–280. doi:10.1136/thoraxjnl-2021-218345
18. Zhou Y, Zhong NS, Li X, et al. Tiotropium in early-stage chronic obstructive pulmonary disease. N Engl J Med. 2017;377(10):923–935. doi:10.1056/NEJMoa1700228
19. Chen Q, Fan Y, Huang K, et al. Cost-effectiveness of population-based screening for chronic obstructive pulmonary disease in China: a simulation modeling study. Lancet Reg Health West Pac. 2024;46:101065. doi:10.1016/j.lanwpc.2024.101065
20. Yawn BP, Mapel DW, Mannino DM, et al. Development of the lung function questionnaire (LFQ) to identify airflow obstruction. Int J Chron Obstruct Pulmon Dis. 2010;5:1–10.
21. Bailey WC, Sciurba FC, Hanania NA, et al. Development and validation of the chronic obstructive pulmonary disease assessment questionnaire (COPD-AQ). Prim Care Respir J. 2009;18(3):198–207. doi:10.4104/pcrj.2009.00032
22. Price DB, Tinkelman DG, Halbert RJ, et al. Symptom-based questionnaire for identifying COPD in smokers. Respiration. 2006;73(3):285–295. doi:10.1159/000090142
23. Levy ML, Fletcher M, Price DB, et al. International primary care respiratory group (IPCRG) guidelines: diagnosis of respiratory diseases in primary care. Prim Care Respir J. 2006;15(1):20–34. doi:10.1016/j.pcrj.2005.10.004
24. Hanania NA, Mannino DM, Yawn BP, et al. Predicting risk of airflow obstruction in primary care: validation of the lung function questionnaire (LFQ). Respir Med. 2010;104(8):1160–1170. doi:10.1016/j.rmed.2010.02.009
25. Pan Z, Chi C, Zheng J. Review of screening methods for chronic obstructive pulmonary disease in primary care. Chin Gen Pract. 2020;23(3):257–266.
26. Martinez FJ, Han MK, Lopez C, et al. Discriminative accuracy of the CAPTURE tool for identifying chronic obstructive pulmonary disease in US primary care settings. JAMA. 2023;329(6):490–501. doi:10.1001/jama.2023.0128
27. Mortimer K, Montes de Oca M, Salvi S, et al. Household air pollution and COPD: cause and effect or confounding by other aspects of poverty? Int J Tuberc Lung Dis. 2022;26(3):206–216. doi:10.5588/ijtld.21.0570
28. Yang IA, Jenkins CR, Salvi SS. Chronic obstructive pulmonary disease in never-smokers: risk factors, pathogenesis, and implications for prevention and treatment. Lancet Respir Med. 2022;10(5):497–511.
29. Apte K, Salvi S. Household air pollution and its effects on health. F1000Res. 2016;5. doi:10.12688/f1000research.7552.1
30. Duan X, Jiang Y, Wang B. Household fuel use for cooking and heating in China: results from the first Chinese environmental exposure-related human activity patterns survey (CEERHAPS) – science direct. Appl Energy. 2014;136(1):692–703. doi:10.1016/j.apenergy.2014.09.066
31. Chakaya J, Khan M, Ntoumi F, et al. Global tuberculosis report 2020 - reflections on the global TB burden, treatment and prevention efforts. Int J Infect Dis. 2021;13(Suppl 1):S7–s12.
32. Yang LJ, Li T, Chen W. Study on spatial clustering characteristics of tuberculosis in China, 2013-2018. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(11):1843–1847. doi:10.3760/cma.j.cn112338-20200114-00029
33. Choi CJ, Choi WS, Lee SY, Kim KS. The definition of past tuberculosis affects the magnitude of association between pulmonary tuberculosis and respiratory dysfunction: Korea national health and nutrition examination survey, 2008-2012. J Korean Med Sci. 2017;32(5):789–795. doi:10.3346/jkms.2017.32.5.789
34. Amaral AF, Coton S, Kato B, et al. Tuberculosis associates with both airflow obstruction and low lung function: BOLD results. Eur Respir J. 2015;46(4):1104–1112. doi:10.1183/13993003.02325-2014
35. Lam KB, Jiang CQ, Jordan RE, et al. Prior TB, smoking, and airflow obstruction: a cross-sectional analysis of the Guangzhou Biobank Cohort study. Chest. 2010;137(3):593–600. doi:10.1378/chest.09-1435
36. Menezes AM, Hallal PC, Perez-Padilla R, et al. Tuberculosis and airflow obstruction: evidence from the PLATINO study in Latin America. Eur Respir J. 2007;30(6):1180–1185. doi:10.1183/09031936.00083507
37. Rennard S, Decramer M, Calverley PM, et al. Impact of COPD in North America and Europe in 2000: subjects’ perspective of confronting COPD international survey. Eur Respir J. 2002;20(4):799–805. doi:10.1183/09031936.02.03242002
38. van den Boom G, Rutten-van Mölken MP, Tirimanna PR, et al. Association between health-related quality of life and consultation for respiratory symptoms: results from the DIMCA programme. Eur Respir J. 1998;11(1):67–72. doi:10.1183/09031936.98.11010067
39. Jones PW, Harding G, Berry P, et al. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
40. Kohansal R, Martinez-Camblor P, Agustí A, et al. The natural history of chronic airflow obstruction revisited: an analysis of the Framingham offspring cohort. Am J Respir Crit Care Med. 2009;180(1):3–10. doi:10.1164/rccm.200901-0047OC
41. Price DB, Tinkelman DG, Nordyke RJ, Isonaka S, Halbert RJ. Scoring system and clinical application of COPD diagnostic questionnaires. Chest. 2006;129(6):1531–1539. doi:10.1378/chest.129.6.1531
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sex Differences in the International Primary Care Airways Group Questionnaire for Screening of Chronic Obstructive Pulmonary Disease: A Retrospective, Cross-Sectional Study
Machiguchi H, Arizono S, Tawara Y, Oomagari M, Yanagita Y, Tanaka T, Senjyu H, Kozu R
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1467-1476
Published Date: 22 June 2022
Prevalence and Risk Factors for COPD in an Urbanizing Rural Area in Western China: A Cross-Sectional Study
Zhang X, Lei Z, Wu Y, Song Y, Wu X, Yang B, Fan J, Feng S, Wu L, Li L, Dai Q, Zeng Z, Feng M, Zhang T
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:459-468
Published Date: 4 April 2023
A Long-Term Study of Adverse Outcomes Associated With Oral Corticosteroid Use in COPD

Tse G, Emmanuel B, Ariti C, Bafadhel M, Papi A, Carter V, Zhou J, Skinner D, Xu X, Müllerová H, Price D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2565-2580
Published Date: 15 November 2023
Patient Safety Climate in Danish Primary Care: Adaption and Validation of the Danish Safety Attitudes Questionnaire (SAQ-DK-PRIM)
Juhl MH, Olesen AE, Deilkås ET, Bruun NH, Obling KH, Rytter N, Larsen MD, Kristensen S
Clinical Epidemiology 2024, 16:533-547
Published Date: 27 August 2024
A Multi-Specialty Delphi Consensus on Assessing and Managing Cardiopulmonary Risk in Patients with COPD
Bhutani M, Bourbeau J, Goodman SG, Hawkins NM, Kaplan AG, Lin PJ, Penz ED, Verma S, Zieroth S
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:2051-2062
Published Date: 19 September 2024