Back to Journals » Biologics: Targets and Therapy » Volume 17
Why and How Should Ethiopia Establish a Stem Cell Transplant Service? A Review Article
Authors Mekonnen S ![]() , Farris H
, Farris H ![]()
Received 13 December 2022
Accepted for publication 8 March 2023
Published 20 March 2023 Volume 2023:17 Pages 33—40
DOI https://doi.org/10.2147/BTT.S401289
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Doris Benbrook
Sintayehu Mekonnen,1 Hawi Farris2
1Department of Internal Medicine, All Africa Leprosy, Tuberculosis and Rehabilitation Training Center, Addis Ababa, Ethiopia; 2Department of Radiology, Addis Ababa University College of Health Science, Addis Ababa, Ethiopia
Correspondence: Sintayehu Mekonnen, Email [email protected]
Abstract: Ethiopia is attempting to reduce cancer-related morbidity and mortality through a strategic national cancer control plan but according to Globocan 2020, hematologic malignancies particularly leukemia and non-Hodgkin’s lymphoma rank among the top five leading causes of new cancer incidence and cause of death among all age groups in both sexes. Hematopoietic stem-cell transplantation (HSCT) is an advanced treatment modality that makes the only effective treatment for cancer and non-cancer-related hematologic diseases unresponsive to conventional therapy. Patients who need stem cell transplants must travel to abroad countries to get the treatment. Meanwhile, the Ethiopian National Specialty and Subspecialty Roadmap sets the goal of establishing HSCT centers in 2020– 2029 GC, yet leaders and planners must start taking steps to put the setup in place. Setting up an HSCT facility is challenging for developing countries due to the high costs, limited infrastructure, and need for intensive medical staff training; however, several nations have been able to start successful stem cell transplant programs. This review summarizes the basic steps and requirements of the program in light of guidelines recommendations and lessons learned from other developing countries. It also highlights possible cost-effective opportunities, bottlenecks, and areas that will require work and investment to make the objective reality in Ethiopia. Provides key information to assist administrators and policymakers to set priorities in planning and making informed decisions to establish and maintain the service.
Keywords: Ethiopia, cancer, hematopoietic stem-cell transplantation, hematologic malignancy
Introduction
Hematopoietic stem cell transplant (HSCT) is the sole therapeutic option in various hematological malignant and nonmalignant illnesses nonresponsive to conventional treatment.1 To suppress the immune system and enable the engraftment of healthy stem cells, the patient goes through numerous cycles of high-dose chemotherapy or radiation treatment during the process. As a result, it requires a lot of resources because the patient may stay in the hospital for up to a month to receive urgent treatment if complications or adverse effects arise.2
Although Ethiopia is making progress in cancer treatment provision through expanding oncology centers and radiotherapy under the National Cancer Control Plan (2016–2020),3 hematologic malignancies particularly leukemia and non-Hodgkin lymphoma account for the third and fourth leading causes of new cancer incidence and mortality in the country according to Globocan 2020.4 In recent studies, leukemia is one of the top five reasons why people die from cancer,5 and an increased burden of hematologic malignancy predominantly affecting the productive age group has been reported in the northwest part of Ethiopia.6 This data highlights the demand for the HSCT center to improve cancer mortality and the patient’s quality of life. It also increases the credibility of the tertiary care level, circumvents the need for abroad referral, and becomes an asset for medical tourism.
In the meantime, setting up a stem cell transplant facility is among the prioritized subspecialty programs which are planned to be provided at certain tertiary institutions under the national specialty and subspecialty service roadmap of Ethiopia (2020–2029 GC).7 However, establishing HSCT service is a high-profile endeavor and continues to be difficult for developing countries due to the expensive investment needed in specialized infrastructure, substantial healthcare professional training, and competing health priorities.8–10 Meanwhile, there are several works of literature from resource-constrained nations that detail how they launched prosperous, self-sustaining HSCT programs.8,11–13 To achieve the goal of launching the HSCT facility, it is essential to examine the experience of developing nations and guideline recommendations of open-access journals.
This paper intends to provide crucial elements of the program, such as the infrastructure needs, the role of a cooperative partnership, the development of human resources, and financial considerations. It will also be a useful evidence-based tool for decision-making for the Ministry of Health’s goal to beat cancer in Ethiopia3 and its commitment to investing in advanced therapeutic services.7
The Burden of Hematological Disorders and Rationale of HSCT in Ethiopia
The prevalence of leukemia in patients with deranged hematological characteristics was reported to be 9.6% at Jimma university and 11.4% at Wollo university.14,15 Hematologic malignancy is the leading cause of pediatric cancer in the country.16,17 According to Globocan 2020 report in both sexes and across all age groups, leukemia is the third most common cause of new cancer incidence and mortality with 4364 new cases and 3182 fatalities, non-Hodgkin’s lymphoma is the fourth most common cancer with 3824 new cases and 2514 fatalities. There were 764 new cases and 345 deaths from Hodgkin lymphoma and 357 new cases and 304 deaths from multiple myeloma.4 The overall impact of hematologic malignancy calls for an evaluation of the current treatment modalities and possible future actions to reduce mortality in Ethiopia.
Most of the hematological malignancies in Ethiopia are treated in tertiary hospitals, among which Tikur Anbessa Specialized Hospital is the first to provide treatment for all kinds of hematological disorders and offers an adult hematology fellowship and postgraduate oncology nursing training programs. Another hospital that handles hematological conditions other than acute leukemia is St. Paul’s Hospital Millennium Medical College. Recently, Mekelle University, Jimma University Hospital, and Gondar University Hospital started providing pediatric oncology care.18
Available treatment modalities are chemotherapy, immunotherapy, and radiotherapy. Data from Addis Ababa university institutional repository showed that treatment response and survival are very low in patients diagnosed with acute leukemia and non-Hodgkin’s lymphoma and relapse is a common condition that is also independently associated with mortality.19–21 In a similar vein, the median survival rate for multiple myeloma is extremely low compared to other nations.22 Thus, stem cell transplantation is a valuable intervention to reduce hematological malignancy-related mortality in Ethiopia. Aplastic anemia, which is a non-hematologic malignant illness that usually requires HSCT, is also not infrequent, with an incidence of 10.5% observed in the northeastern part of Ethiopia.15
Currently, six African countries are offering stem cell transplant services.23 Ethiopia is the second largest populated country in Africa where the government envisioned establishing an HSCT facility7 So, it is important to comprehend the key requirements, as well as the opportunities, sociopolitical obstacles, and financial challenges of the service. Table 1 presents the author’s perspectives on the internal and external factors (SWOT analysis) associated with setting up an HSCT center in Ethiopia.
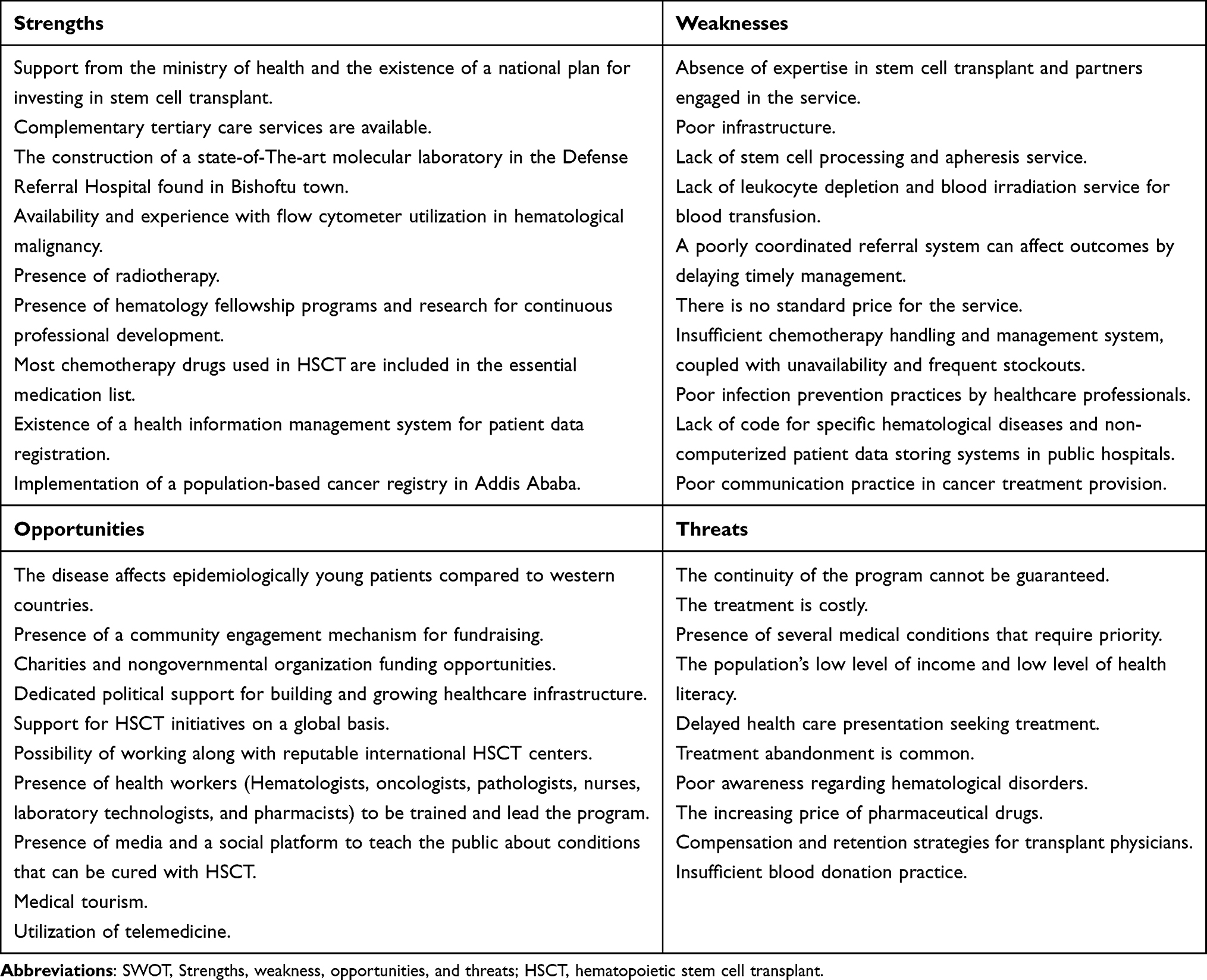 |
Table 1 SWOT Analysis for the Establishment of HSCT Service in Ethiopia |
The Role of Understanding the Types of Transplants for Establishing the HSCT Facility
Planning to establish HSCT facilities for the first time necessitates a substantial investment in human resource development, inpatient and outpatient rooms, equipment, blood banks, and laboratories, depending on the kind of transplant—autologous vs allogeneic.24
In an autologous transplant, the patient’s stem cells are harvested and frozen for later use before radiation or chemotherapy. Following chemotherapy or radiation therapy, the collected stem cells are given back to the patient. In an allogeneic transplant, stem cells are obtained from a donor, ideally a sibling with a comparable genetic profile. In the absence of a sibling, an unrelated person with a similar genetic makeup is employed. It is also possible in some situations to employ a parent or child who is only partially matched and this operation is known as a haploidentical transplant. Under specific circumstances, it is also possible to use umbilical cord blood.1,25
Allogeneic stem cell transplant is a resource-intensive procedure, associated with several complications, which requires a multidisciplinary supportive system.26 This makes autologous transplant the better cost-effective move for starting HSCT for the first time in adults;27 however, it is quite the reverse in pediatrics due to technical difficulties with autologous transplant processing and its less frequent indication.28 Although allogeneic transplantation is resource intensive, it has a curative potential thanks to its property of inducing graft versus leukemia effect while the role of autologous transplant is to facilitate the administration of high-dose chemotherapy and act as a lifeboat for recovering hematopoiesis but primary tumor relapses are the concern.25
Recently WBMT (worldwide network for blood and marrow transplantation) recommendations classified the requirements of autologous and allogeneic programs as a minimum to the preferable and ideal in a graded manner, which can assist the developing country to prioritize and use resources efficiently to start the program and reach the ideal (full accreditation) level subsequently (Annex 1).24
Infrastructure and Equipment
Hospitals place their HSCT rooms on the upper floors, away from wet areas, infectious wards, and construction zones.12 A team made up of a hospital administrator, project manager, architect, engineer, information technology (IT), finance, nurse, and a doctor is necessary for efficient renovation or infrastructure design.27 Site visit by existing HSCT center experts to assess the planned hospital’s suitability and viability has been mentioned as an important initial step in the developing nation’s experience.11,12 Therefore, this must be considered when a potential tertiary hospital in Ethiopia seeks to adopt the HSCT program.
Planning the infrastructure must leave enough area for the following: outpatient, nurse corridor, nurses’ offices, doctors’ offices, apheresis rooms, waiting rooms, infusion rooms, pretransplant admission rooms, on-site pharmacy, and drug preparation rooms, and soiled and clean utility rooms.24 In a study from Tikur Anbessa Specialized Hospital, the lack of a designated area for the preparation of medications was linked to dose-related mistakes that can result in inappropriate treatment and toxicities.29 To deliver safe and effective treatments, proper infrastructure design must be a top priority.
According to the Indian guideline, the HSCT facility room should feature positive pressure ventilation as a standard.8 However, the most recent WBMT recommendation and EBMT (European Society for Blood and Bone Marrow Transplantation) suggest the inpatient and outpatient rooms need to be at least clean and single bedded and HEPA (high-efficiency particulate air) filter is not strictly necessary for newly establishing centers. The HEPA filter must be considered through time or for high-risk transplants (allogeneic transplants).24,30
The HSCT center needs a stem cell processing laboratory, which can be built either in a new area or as an extension of the existing laboratory. A successful stem cell laboratory needs to be well designed, have the right tools, have a staff that is properly trained, and have standard operating procedures that cover every step of the facility’s stem cell processing. For the freezing of autologous stem cell products, controlled cryopreservation using liquid nitrogen is necessary. Flow cytometry must be available for counting CD34 cells.31 The availability and experience of using flow cytometry for hematological malignancies in Ethiopia32 will partially reduce the investment costs required to purchase equipment and train manpower.
For allogeneic transplants, advanced testing such as polymerase chain reaction (PCR), human leukocyte antigen (HLA) typing, donor-specific antibody screen, fluorescence in situ hybridization, chimerism, and medication levels are required in addition to conventional diagnostics.24,30 This requires an expensive investment in an advanced laboratory but, as Bangladesh did, these sophisticated tests can be sent to a foreign country.12 Fortunately, Ethiopia is building a cutting-edge molecular laboratory in the defense military hospital located at Bishoftu. This hospital has the advantage of becoming a cost-effective innovation area, or it will help other hospitals by lowering the time needed for shipping and receiving laboratory tests to other nations. This is a great opportunity for the establishment of HSCT by lowering redundant capital expenditure.8
Depending on the type of transplant, several support systems are required, including emergency access, a critical care unit, hemodialysis, endoscopy, bronchoscopy, and radiology services at the same facility. Consequently, the country’s tertiary healthcare facilities especially those who are offering oncology services, are potential areas for the expansion of HSCT services. In addition, a 24-hour blood bank with the necessary licenses for apheresis, stem cell collection, and storage, irradiation, leukocyte depletion of blood products, blood cross-matching, and transfusion is necessary.24,30 Apheresis, leukocyte depletion, and blood irradiation services are not available in Ethiopia and need investment. Furthermore, blood products are in short supply due to inadequate blood donation practices, and raising public awareness is critical.33 In the course of providing the service, a registry of unrelated stem cell donors needs to be established. For details on the standards, see the World Marrow Donor Society Guidelines.34
Human Resource Development
A successful transplantation program’s foundation is built on the experience of medical, nursing, and laboratory staff, hospital support, and effective leadership.10,35 The biggest challenge to establishing the HSCT program in Ethiopia is the lack of transplant doctors, except for a few hematologists, and an abundant middle-level workforce; internists, lab technicians, nurses, and pharmacists.
Developing countries addressed poor human resources by establishing a collaborative partnership with an existing HSCT facility. The significance of twining or pairing with established HSCT centers overseas is mentioned in nearly all types of work investigating the opening of new HSCT services in poor nations. To give example, Bangladesh launched the HSCT center in Dhaka with assistance from the Massachusetts General Hospital.12 In Iraqi Kurdistan, the HSCT unit at the Hiwa Cancer Hospital was established with assistance from the Italian Agency for Development Cooperation.11 With assistance from the Italian nongovernmental organization (NGO) Cure 2 Children, several HSCT facilities have been built in South-East Asia, the Middle East, and Africa.13
Collaboration with an established institution helps to get the required expertise. This enables efficient on-site staff training and offers continuing support for administering the service, which is an innovative and cost-effective strategy as opposed to sending workers abroad for training.12 In addition, online tools like telemedicine can also allow case discussions with local physicians to fill the gap while regional medical professionals get the necessary proficiency and assurance.
A capacity-building partnership has made it possible to train four pediatric hematology-oncology subspecialists in Ethiopia through on-site training and rotating fellows overseas. Two of the trainees stayed at Tikur Anbessa Specialized Hospital, and one went to Jimma University.36 This experience serves as a model to train transplant hematologists, nurses, laboratory technicians, and pharmacy staff. In addition, the hematology fellowship and oncology nursing training program at Tikur Anbessa Specialized Hospital will ensure the propensity for continuous professional development, which is essential for the sustainability of HSCT services.
Financing HSCT
Although HSCT facilities are associated with government healthcare spending and GDP per capita, there is little information available on the HSCT center’s price.37 Renovating and outfitting the units for use within an existing healthcare facility will cost between $50,000 and $100,000.28,38 The median cost of HSCT varies by transplant type and ranges between $12,500 to $290,000 per patient worldwide (India, Mexico, and the United States).39–41 In Bangladesh, the government provided funds for the first transplants and the building of the transplant unit,12 But other countries used a combination of government and charitable funds.38
Ethiopia’s health sector transformation plan allocated high-cost budgeting for medicines and supply procurement, followed by infrastructure and manpower development.42 The recent GDP per capita is 925 dollars and the government covers around one-third of the cost of healthcare, with the remaining costs coming from individual out-of-pocket expenses, donations, and others.43 However, government expenditure on health care is extremely low, according to the Abuja Declaration, so possible ways to finance HSCT facilities may include reallocating additional cash from other budgets, improving the governance of donor funding, and efficient resource management. Medical tourism is another potential opportunity for financial support but for good quality control, the poor infection prevention practice by health care professionals in Ethiopia44 remains to be addressed.
In terms of the cost of the service consumables, supporting medications, and chemotherapy make up a sizable amount of beginning and maintenance costs in addition to the labor cost.9 The drugs Busulfan, Cyclophosphamide, Fludarabine, and Melphalan are frequently used in conditioning programs. Granulocyte colony-stimulating factor for stem cell mobilization, anti-thymocyte globulin (ATG) in aplastic anemia and for immunosuppressive in graft versus host disease (GVHD) prophylaxis in addition to Cyclosporine A, Methotrexate, and Tacrolimus are necessary for allogeneic transplantation. The accessibility of antiviral, antifungal, and broad-spectrum antibiotics is also crucial.
Although almost all of the medications mentioned above are authorized by the Ethiopian Essential Medication List,22 crucial medications for HSCT such as busulfan, ATG, and intravenous cyclosporine are not on the list. Given its frequent use in conditioning regimens, busulfan must be prioritized and supplied,45,46 while ATG is an ideal requirement when the service evolves.24 Intravenous cyclosporine can be optional as an alternative calcineurin inhibitor (tacrolimus) is available for the prevention of GVHD.47 Unfortunately, access to chemotherapy drugs in the country is limited and unaffordable, some drugs are not available at all pharmacies,48 and drug stock-outs are common.49 To sustain the viability of HSCT service continuous medication supply and effective utilization are fundamental.
Recently, WBMT provided several technical strategies to help countries with limited resources to lower the cost of the service, including outsourcing inaccessible tests like HLA typing, choosing the intensity of conditioning regimens based on the patient and illness parameters, using peripheral blood stem cell sources in autologous HSCT, and employing biosimilar medications. Using non-cryopreserved stem cells in autologous transplantation and giving young patients priority for new HSCT facilities.9
The patients’ demographics in Ethiopia can make the program cost-effective since they are often younger, which increases the curative and longer survival chance.6,14,15 However, patients frequently arrive late in health care facilities with advanced diseases,50 thus, it is necessary to raise community awareness through the media and social platforms to increase the cost-effectiveness of the service. Forgoing cancer treatment is also common,18 which may be exacerbated by a longer HSCT treatment period and costs, so financial support mechanisms and precise communication of the necessity to finish therapy are critical. Indeed, communication is substantially impeded in cancer treatment provision in Ethiopia due to several reasons51 and needs to be tackled.
In some circumstances, radiotherapy is necessary for conditioning regimens30,46 but for newly opening HSCT facilities, it is not required because non-radiation conditioning regimens are applicable for the majority of disorders.24 Nevertheless, given that Ethiopia recently expanded and opened two oncology facilities with the capacity to provide radiotherapy services, which made the service already available in three tertiary hospitals, the cost and availability concerns will not be a barrier.52,53
Conclusion
The ability to forge connections with established transplant centers, devoted local staff, and capable leadership is essential for success. Achieving a collaborative partnership is the first step in the process; after that, experts will determine the project’s suitability in the proposed hospital and provide training for effective local human resource development and ongoing support. Charity may spur the partnership, but for it to endure there need to be mutual benefits like opportunities for joint research and training. For a twinning initiative to be successful, a dedicated local oncologist or hematologist who can foster the relationship is mandatory. It is more cost-effective, to begin with, autologous and expand to allogeneic transplants since the latter is associated with a major cost driver of the service. Establishing and maintaining an HSCT facility demands substantial investment so setting priorities, and recognizing the requirements and the challenges are critical. To secure funding, it is essential to explore assistance from international initiatives and to pursue innovative government budgetary mechanisms. Considering the therapy is unavailable in 89% of African countries and patients from developed countries are increasingly seeking treatment in developing countries at a reduced cost, can help to generate revenue through medical tourism, however, its effectiveness is uncertain.
Acknowledgment
We thank the Ethiopian Ministry of Health for opening the chance to learn more about HSCT through the mission of service initiation of the defense referral hospital found at Bishoftu.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Copelan EA. Hematopoietic stem-cell transplantation. N Eng J Med. 2006;354(17):1813–1826. doi:10.1056/NEJMra052638
2. Canonica CM. An overview of hematopoietic stem cell transplantation. Physician Assist Clin. 2016;1(3):409–418. doi:10.1016/j.cpha.2016.03.006
3. MOHE. Federal ministry health Ethiopia. Int J Equity Health. 2020;84(9):936–943.
4. World Health Organization. Global cancer observatory Ethiopia fact sheet. Int Agency Res Cancer. 2021;133:2020–2021.
5. Awedew AF, Asefa Z, Belay WB. National Burden and Trend of Cancer in Ethiopia, 2010–2019: a systemic analysis for Global burden of disease study. Sci Rep. 2022;12(1):12736. doi:10.1038/s41598-022-17128-9
6. Enawgaw B, Aynalem M, Melku M, et al. Hematological malignancies in the Northwest Ethiopia. PLoS One. 2021;16(12):1–10. doi:10.1371/journal.pone.0260639
7. Duguma D. National specialty and sub-specialty service roadmap, ministry of health 2020–2029; 2020.
8. Das K, Khanna T, Agrawal N. Establishing hematopoietic stem cell transplant unit in resource limited setting: a critical analysis of Indian Council of medical research 2017 guidelines. J Transplant. 2018;2018:1–4. doi:10.1155/2018/1292307
9. Aljurf M, Weisdorf D, Hashmi S, et al. Worldwide network for blood and marrow transplantation recommendations for establishing a hematopoietic stem cell transplantation program in countries with limited resources, part II: clinical, technical, and socioeconomic considerations. Biol Blood Marrow Transplant. 2019;25(12):2330–2337. doi:10.1016/j.bbmt.2019.04.012
10. Mtenga J, Orf K, Zheng J, et al. Haematopoietic stem cell transplantation in Tanzania. Br J Haematol. 2021;192(1):17–21. doi:10.1111/bjh.17106
11. Majolino I, Othman D, Rovelli A, et al. The start-up of the first hematopoietic stem cell transplantation center in the Iraqi Kurdistan: a capacity building cooperative project by the Hiwa Cancer Hospital, Sulaymaniyah, and the Italian Agency for Development Cooperation: an innovative approach. Mediterr J Hematol Infect Dis. 2017;9(1):1–10. doi:10.4084/mjhid.2017.031
12. Barron AM, Moran J, Nina SS, et al. Building specialized nursing practice capacity in Bangladesh: an educational program to prepare nurses to care for oncology and bone marrow transplant patients in Dhaka, Bangladesh. J Global Oncol. 2018;2018(4):1–6. doi:10.1200/JGO.2016.006486
13. Faulkner L. How to setup a successful transplant program for hemoglobinopathies in developing countries: the Cure2Children approach. Hematol Oncol Stem Cell Ther. 2020;13(2):71–75. doi:10.1016/j.hemonc.2019.12.010
14. Kassahun W, Tesfaye G, Bimerew LG, Fufa D, Adissu W, Yemane T. Prevalence of Leukemia and associated factors among patients with abnormal hematological parameters in Jimma medical center, Southwest Ethiopia: a Cross-Sectional Study. Adv Hematol. 2020;2020:3–9. doi:10.1155/2020/2014152
15. Ebrahim H, Fisha T, Debash H, Bisetegn H. Patterns of bone marrow confirmed malignant and non-malignant hematological disorders in patients with abnormal hematological parameters in Northeast Ethiopia. J Blood Med. 2022;13:51–60. doi:10.2147/JBM.S346091
16. Memirie ST, Habtemariam MK, Asefa M, et al. Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data. J Glob Oncol. 2018;4:1–11. doi:10.1200/JGO.17.00175
17. Yifru S, Muluye D. Childhood cancer in Gondar University Hospital, Northwest Ethiopia. BMC Res Notes. 2015;8(1):1–5. doi:10.1186/s13104-015-1440-1
18. Mirutse MK, Tolla MT, Memirie ST, et al. The magnitude and perceived reasons for childhood cancer treatment abandonment in Ethiopia: from health care providers’ perspective. BMC Health Serv Res. 2022;22(1):1–13. doi:10.1186/s12913-022-08188-8
19. Survival status and predictors of mortality among acute leukemia patients attending adult hematology oncology ward at Tikur Anbessa Specialized hospital. Addis Abeba, Ethiopia; 2019. Available from: http://etd.aau.edu.et/handle/123456789/21353.
20. Outcome of patients with non Hodgkin’s Lymphoma and its predictors, at Tikur Anbessa specialized hospital: a retrospective chart review. Addis Abeba, Ethiopia; 2019. Available from: http://etd.aau.edu.et/handle/123456789/21357.
21. Clinical profile and treatment outcome of Acute leukemia patients at Tikur Anbessa Specialized Hospital. Addis Ababa, Ethiopia. Available from: http://etd.aau.edu.et/handle/123456789/24802.
22. Demographic, clinical characteristics, treatment outcome and determinant factors of patients with multiple myeloma at TASH from January 2015 to December 2019. Available from: http://etd.aau.edu.et/handle/123456789/24934.
23. Harif M, Weisdorf D, Novitzky N, et al. Special report: summary of the first meeting of African Blood and Marrow Transplantation (AfBMT) group, Casablanca, Morocco, April 19–21, 2018 held under the auspices of the Worldwide Network for Blood and Marrow Transplantation (WBMT). Hematol Oncol Stem Cell Ther. 2020;13(4):202–207. doi:10.1016/j.hemonc.2019.05.003
24. Pasquini MC, Srivastava A, Ahmed SO, et al. Worldwide Network for Blood and Marrow Transplantation (WBMT) recommendations for establishing a hematopoietic cell transplantation program (Part I): minimum requirements and beyond. Hematol Oncol Stem Cell Ther. 2020;13(3):131–142. doi:10.1016/j.hemonc.2019.08.001
25. Hatzimichael E, Tuthill M. Hematopoietic stem cell transplantation. Stem Cells Cloning. 2010;3(1):105–117. doi:10.2147/SCCAA.S6815
26. Shinohara A, Kurokawa M. Allogeneic hematopoietic stem cell transplantation. Otolaryngol Head Neck Surg. 2014;86(3):277–282.
27. John MJ, Chandy M. Setting up a hematopoietic stem cell transplantation unit; 2021:1–19.
28. Faulkner L, Verna M, Rovelli A, et al. Setting up and sustaining blood and marrow transplant services for children in middle-income economies: an experience-driven position paper on behalf of the EBMT PDWP. Bone Marrow Transplant. 2021;56(3):536–543. doi:10.1038/s41409-020-0983-5
29. Gessese YA, Fenta TG, Weldegiorgis MA. Assessment of medication use process in adult oncology unit of Tikur Anbesa Specialized Hospital: a cross-sectional study in Addis Ababa, Ethiopia. Eur J Oncol Pharm. 2018;1:3. doi:10.1097/OP9.0000000000000005
30. Polomeni A, Moreno E, Schulz-Kindermann F. Psychological morbidity and support. The EBMT Handbook: hematopoietic stem cell transplantation and cellular therapies; 2018:221–227.
31. Inamdar MS, Healy L, Sinha A, Stacey G. Global solutions to the challenges of setting up and managing a stem cell laboratory. Stem Cell Rev Report. 2012;8(3):830–843. doi:10.1007/s12015-011-9326-7
32. Tegegen M, Hassen F, Abubeker A, et al. Diagnostic utility of immunophenotyping by flow cytometry for diagnosis and classification of acute Leukemias in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. Indonesian J Cancer. 2021;15(3):129. doi:10.33371/ijoc.v15i3.796
33. Getie A, Wondmieneh A, Bimerew M, Gedefaw G, Demis A. Knowledge of blood donation and associated factors in Ethiopia: a systematic review and meta-analysis. BMJ Open. 2021;11:7. doi:10.1136/bmjopen-2020-044343
34. (WMDA) WMDA. International standards for unrelated hematopoietic stem cell donor registries; 2021.
35. Mahfuz H, Hossain ME, Uddin MM, et al. Overcoming the hurdles and establishing a haematopoietic stem cell transplant centre in a resource poor setting: an example from Dhaka, Bangladesh. Br J Haematol. 2021;194(2):e59–e60. doi:10.1111/bjh.17532
36. Hailu D, Adamu H, Fufa D, et al. Training pediatric hematologists / oncologists for capacity building in Ethiopia. Blood. 2019;134(Supplement_1):3423. doi:10.1182/blood-2019-121796
37. Hildreth CJ, Burke AE, Glass RM. Hematopoietic stem cell transplantation. JAMA. 2009;302(3):340. doi:10.1001/jama.302.3.340
38. Faulkner LB, Uderzo C, Masera G. International cooperation for the cure and prevention of severe hemoglobinopathies. J Pediatr Hematol Oncol. 2013;35(6):419–423. doi:10.1097/MPH.0b013e31829cd920
39. Sharma SK, Choudhary D, Gupta N, et al. Cost of hematopoietic stem cell transplantation in India. Mediterr J Hematol Infect Dis. 2014;6:1. doi:10.4084/mjhid.2014.046
40. Jaime-Pérez JC, Heredia-Salazar AC, Cantú-Rodríguez OG, et al. Cost structure and clinical outcome of a stem cell transplantation program in a developing country: the experience in Northeast Mexico. Oncologist. 2015;20(4):386–392. doi:10.1634/theoncologist.2014-0218
41. Broder MS, Quock TP, Chang E, et al. The cost of hematopoietic stem-cell transplantation in the United States. Am Health Drug Benefits. 2017;10(7):366–373.
42. FMoH. Health sector transformation plan II: HSTP II (2020/21–2024/25). Ethiopian Ministry Health. 2021;25:96.
43. Tilahun M, Mengistie B, Egata G, et al. Essential Health Services Package of Ethiopia. Vol. 397. Ministry of Health Ethiopia; 2019.
44. Sahiledengle B, Tekalegn Y, Woldeyohannes D. The critical role of infection prevention overlooked in Ethiopia, only one-half of health-care workers had safe practice: a systematic review and meta-analysis. PLoS One. 2021;16(1):1–18. doi:10.1371/journal.pone.0245469
45. Ciurea SO, Andersson BS. Busulfan in hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2009;15(5):523–536. doi:10.1016/j.bbmt.2008.12.489
46. Gyurkocza B, Sandmaier BM. Conditioning regimens for hematopoietic cell transplantation: one size does not fit all. Blood. 2014;124(3):344–353. doi:10.1182/blood-2014-02-514778
47. Huang B, Lin X, Zhang Z, et al. Comparison of tacrolimus and cyclosporine combined with methotrexate for graft versus host disease prophylaxis after allogeneic hematopoietic cell transplantation. Transplantation. 2020;104(2):428–436. doi:10.1097/TP.0000000000002836
48. Alemu BA, Hailemariam FH. Price, availability and affordability of anti-cancer medicines in Addis Ababa, Ethiopia. Risk Manag Healthc Policy. 2022;15:2421–2433. doi:10.2147/RMHP.S395456
49. Fentie AM, Mekonen ZT, Gizachew Z, et al. Chemotherapy supply chain management, safe-handling and disposal in Ethiopia: the case of Tikur Anbessa specialized hospital. Pediatr Hematol Oncol. 2022:1–9. doi:10.1080/08880018.2022.2139028
50. Haileselassie W, Mulugeta T, Tigeneh W, Kaba M, Labisso WL. The situation of cancer treatment in Ethiopia: challenges and opportunities. J Cancer Prev. 2019;24(1):33–42. doi:10.15430/JCP.2019.24.1.33
51. Kebede BG, Abraha A, Andersson R, et al. Communicative challenges among physicians, patients, and family caregivers in cancer care: an exploratory qualitative study in Ethiopia. PLoS One. 2020;15(3):1–16. doi:10.1371/journal.pone.0230309
52. Ministry of Health Ethiopia. Radiation therapy center inaugurated at Jimma University hospital. Available from: https://www.moh.gov.et/site/node/317.
53. Ethiopian Monitor. Officials inaugurate new cancer treatment center in Harar City. Available from: https://ethiopianmonitor.com/2022/02/25/officials-inaugurate-new-cancer-treatment-center-in-harar-city/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Causes and Risk Factors for Deaths Among Pediatric Oncology Patients: A 20-Year Observation
Mitura-Lesiuk M, Dubaj M, Drabko K, Zawitkowska J
Cancer Management and Research 2026, 18:604728
Published Date: 5 May 2026
Malignancy-Associated Hemophagocytic Lymphohistiocytosis: An Experience of 15 Years in Polish Pediatric Hematology Centers
Wolowiec M, Drabko K, Maciejka-Kemblowska L, Irga-Jaworska N, Smalisz K, Skoczen S, Tomaszewska R, Szczepanski T, Babol-Pokora K, Mlynarski W, Popko K, Demkow U, Furmanczyk K, Malinowska I
Journal of Blood Medicine 2026, 17:571561
Published Date: 27 May 2026
The Danish Lymphoid Cancer Research (DALY-CARE): Genetic Cohort Profile
Dietz JBN, Kadlec TF, Rotbain EC, Werling M, Vainer N, Katsimigas A, Ostrowski SR, Sørensen E, Pedersen OBV, Schwinn M, Nissen J, Magnusson MK, Elhussein HH, Agius R, Frederiksen CM, Rostgaard K, Hjalgrim H, Davidsson OB, Kristjánsson RP, Brieghel C, Niemann CU
Clinical Epidemiology 2026, 18:607221
Published Date: 15 July 2026