Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Vulvar Verruciform Xanthoma: A Comprehensive Literature Review
Authors Wu W ![]() , Sun L, Lu J
, Sun L, Lu J ![]() , Yang X, Liu Q, Wang J
, Yang X, Liu Q, Wang J
Received 11 May 2022
Accepted for publication 2 August 2022
Published 18 August 2022 Volume 2022:15 Pages 1675—1680
DOI https://doi.org/10.2147/CCID.S371979
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Weiwei Wu,1,* Lengbing Sun,2,3,* Jiejie Lu,2 Xianxu Yang,2 Qiao Liu,3,4 Junzhi Wang5
1Department of Plastic and Dermatological Surgery, The Fifth People’s Hospital of Hainan Province, Haikou, People’s Republic of China; 2Department of Dermatology, The Fifth People’s Hospital of Hainan Province, Haikou, People’s Republic of China; 3School of Clinical Medicine, Jiangxi University of Chinese Medicine, Nanchang, People’s Republic of China; 4Department of Dermatology,The Second Affiliated Hospital of Jiangxi University of Chinese Medicine, Nanchang, People’s Republic of China; 5First Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine, Harbin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiao Liu; Junzhi Wang, Email [email protected]; [email protected]
Abstract: Verruciform xanthoma (VX) is a rare, benign, mucocutaneous, verrucous, papillary lesion. This paper retrospectively summarizes clinical and pathologic features of 32 vulvar verruciform xanthoma reported from China and abroad. The skin lesions are generally single, mainly in labia minora, clitoris and fourchette with partly extending to the groin, buttocks and anus. The possible inducing factors include long-term scratching, local itching, severe lymphedema or lymphangioma circumscriptum. Severe cutaneous trauma and chronic inflammation may be the main causes. Clinically, it can easily be misdiagnosed as condylomata acuminata, squamous cell carcinoma, bowenoid papulosis, etc. It is reported to be related to underlying disorders. The main treatment is complete resection.
Keywords: verruciform xanthoma, vulvar, clinical features, immunohistochemistry, treatment, etiology
Introduction
Verruciform xanthoma (VX) is a rare, benign, mucocutaneous, verrucous, papillary lesion characterized by collections of foamy histiocytes in the papillary dermis, lipid-laden macrophages (xanthoma cells), epidermal hyperplasia with hyperkeratosis and parakeratosis.1 It was first described in 1971 on the oral mucosa.2 Since then, the extraoral cases have also been reported, especially cases with lesions on anogenital area,2 thumb,3 esophagus4 and other areas, which are usually presented as painless polypoid or sessile papules with a verrucous or pebbly surface and pink-yellowish hue.1
Among them, vulvar verruciform xanthoma can easily be misdiagnosed as a genital wart and HPV-independent TP53-independent vulvar intraepithelial neoplasia,5 etc. The diagnostic test of this disease is mainly through biopsy and pathological examination.6 Herein, we retrospectively summarized clinical and pathologic features of vulvar verruciform xanthoma reported from China and abroad through searches of PubMed (http://www.ncbi.nlm.nih.gov/pubmed/) and China National Knowledge Infrastructure (http://www.cnki.net/).
Clinical Features
To our knowledge, only thirty-two cases have been reported so far6–26 (Table 1). In the review of previously reported 32 vulval VX cases, the mean age was 46 years (range from 1.5 to 84 years), the mean duration was 72 months (range from 1 to 300 months), and the main place of occurrence was labia minora, clitoris and fourchette with partly extending to the groin, buttocks and anus.
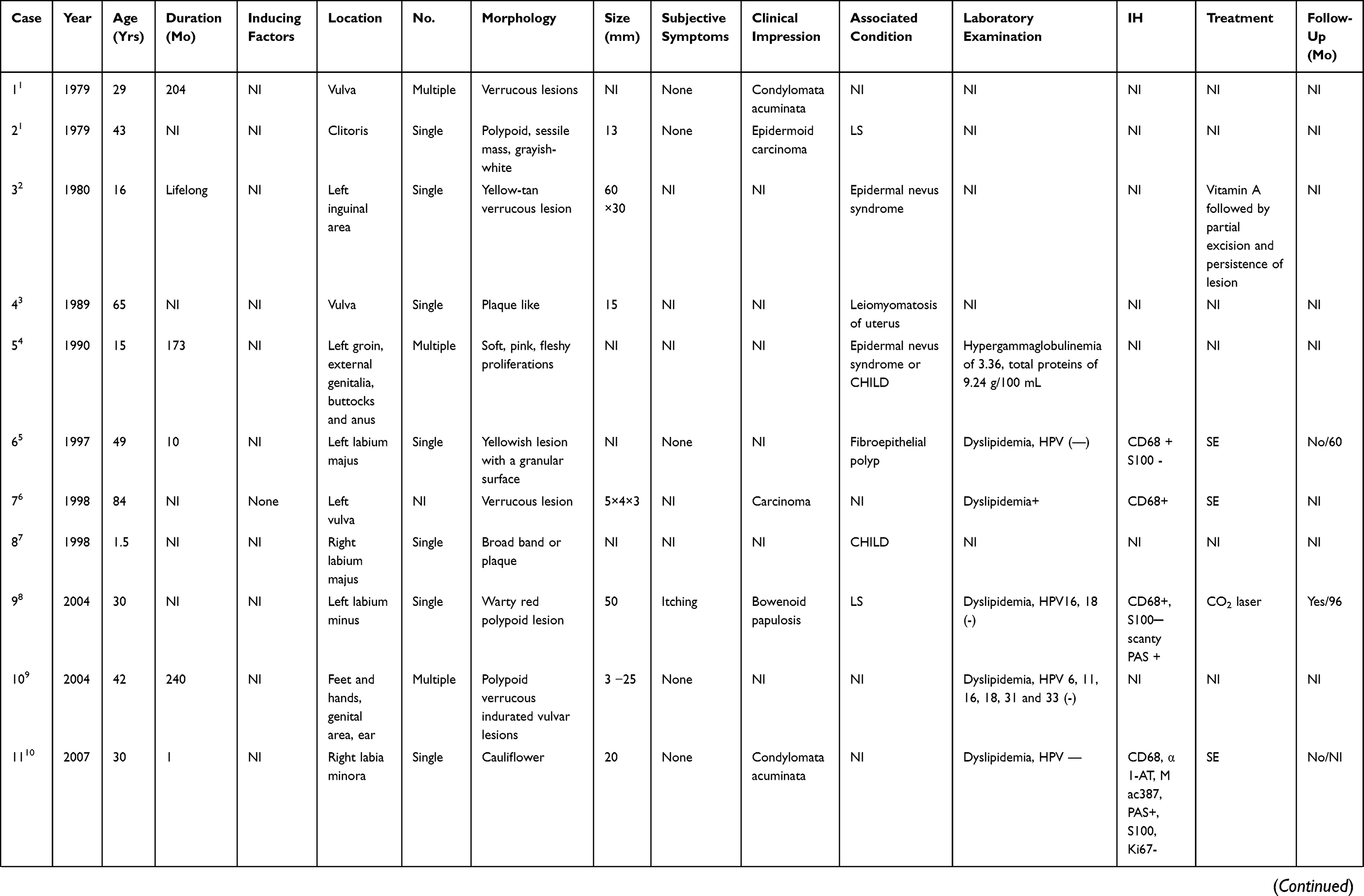 | 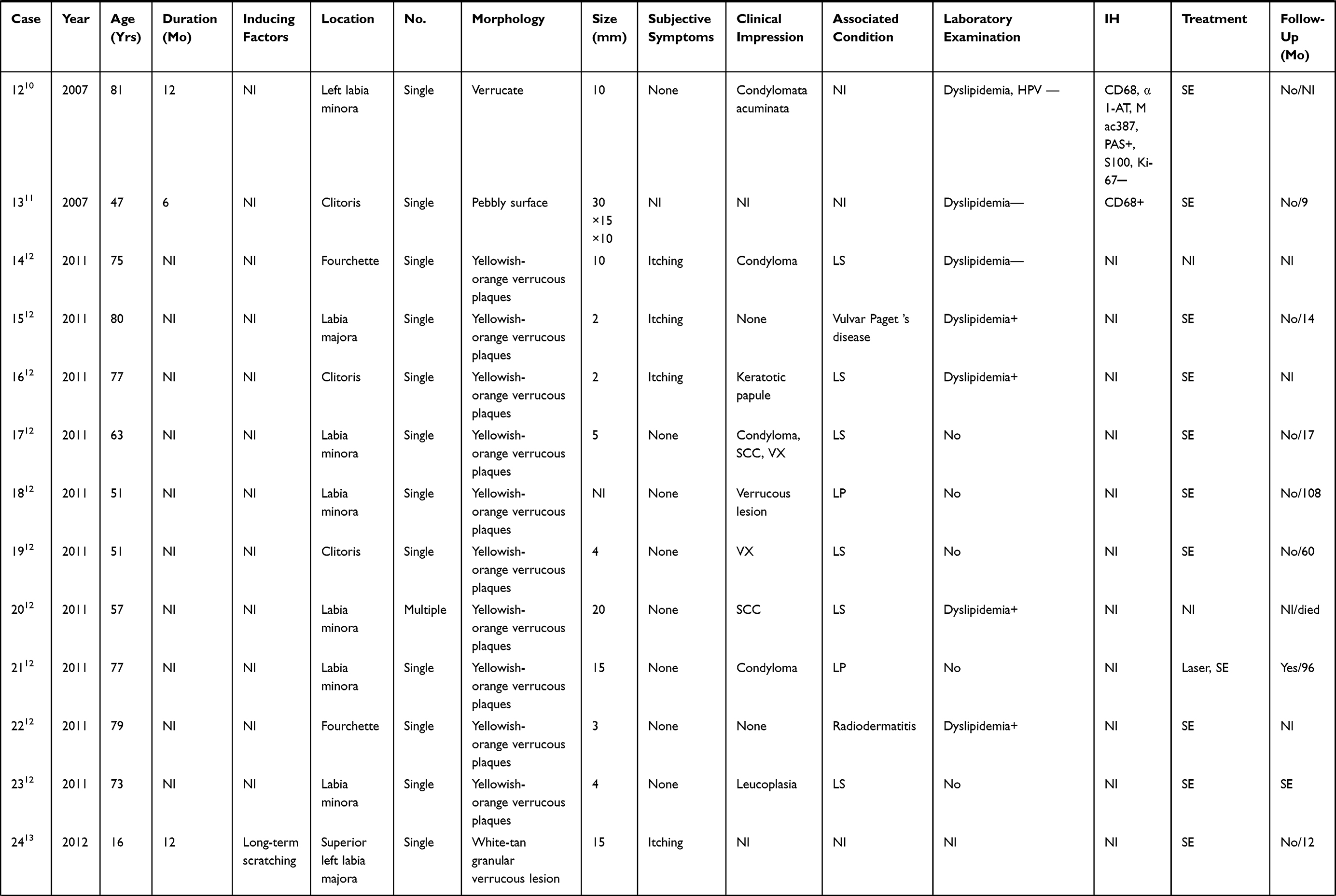 | 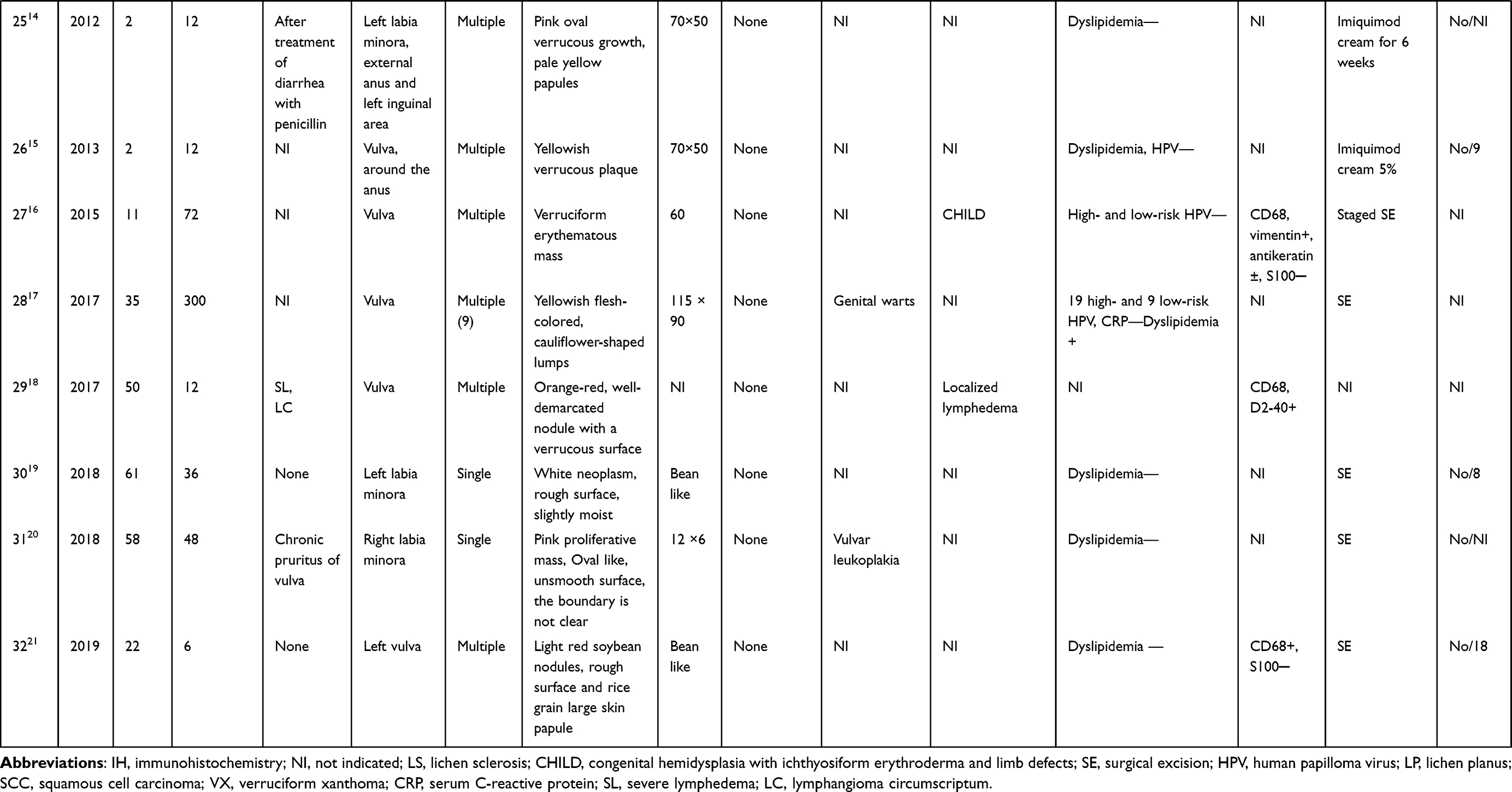 |
Table 1 Vulvar Verruciform Xanthoma Cases Reported to Date |
Among the 32 patients, 21 cases showed single skin lesions, 10 cases showed multiple skin lesions, and 1 case did not mention single or multiple skin lesions. Seven of 32 cases presented as mild itching, excluding 5 cases not mentioned, and the skin lesions ranged in size from 2 to 115 mm. Clinically, it can easily be misdiagnosed as condylomata acuminata, squamous cell carcinoma, bowenoid papulosis, etc. And it was reported to be related to underlying disorders, such as lichen sclerosis (8 patients), congenital hemidysplasia with ichthyosiform erythroderma and limb defects (3 patients), lichen planus (2 patients), epidermal nevus syndrome (2 patients), Paget’s disease (1 patients), radiodermatitis (1 patient), fibroepithelial polyp (1 patient), leiomyomatosis of uterus (1 patient) or localized lymphedema (1 patient).
Histologic Examination
We note that histopathology plays a key role in the recognition and diagnosis of VX. The major pathognomonic feature is the collections of foamy histiocytes in the papillary dermis, lipid-laden macrophages (xanthoma cells), epidermal hyperplasia with hyperkeratosis and parakeratosis.1 The second main feature is the papillomatous appearance, including plaque-like configurations, more polypoid papular proliferations to lesions, discrete frondular papillae overlying ectatic basal vessels and variable chronic inflammation.27
Immunohistochemistry
In retrospective cases, immunohistochemistry revealed the foam cells were positive for the histiocytic marker CD68 (9 patients), α1-AT (2 patients), Mac387 (2 patients), vimentin (1 patient), PAS (2 patients); Weak positive for CK (AE1/AE3) (2 patients), antikeratin (1 patient); and negative for antibodies to S-100 (5 patients) and Ki67 (1 patient).
Treatment
Two patients were treated with laser, and both recurred; two patients were treated with imiquimod cream and satisfactory results have been obtained; the lesions of the other patients were typically managed successfully with surgical excision and no recurrence.
Etiology
The possible inducing factors include long-term scratching (1 patient), local itching (1 patient), severe lymphedema (1 patient) or lymphangioma circumscriptum (1 patient). The exact etiology of VX is unclear, and several main hypotheses have been proposed. ① Most studies deny the association between HPV and VX.28 Although HPV was found in several studies,29,30 others failed to confirm this association. ② It may be related to hyperlipidemia, but the majority of patients with VX do not have associated hyperlipidemia.28 ③ Severe cutaneous trauma and chronic inflammation seem to be a more plausible theory. First, rapid proliferation and release of chemokines that attract neutrophils may be stimulated by damaged keratinocytes. Then, the recruitment of neutrophils may accelerate the keratinolysis, when parakeratotic cells caused by the rapid proliferation of keratinocytes accumulate on the surface of the VX lesions. Finally, as keratinocytes degrade and degenerate toward the dermis, the necrotic keratinocyte debris is phagocytized by dermal macrophages and transformed into lipid-laden macrophages (foam cells).31
Conclusion
When verrucous plaques occur in vulva or anus, the diagnosis of VX should be considered, which can be confirmed by histopathology, and the other tests are performed to rule out other entities on the differential diagnosis. Clinically, vulvar VX should be differentiated with condyloma acuminatum, verrucous carcinoma, squamous cell carcinoma and intraepithelial neoplasia. Therefore, the correct diagnosis requires histopathologic examination. The typical pathological feature is the dense accumulation of macrophage foam cells in papillary dermis. It is generally believed that xanthoma cells were positive for CD68, indicating monocyte/macrophage participation in the disease. The main treatment was complete resection.
Funding
This work was supported by the Construction Project of Hainan Province Clinical Medical Center.
Disclosure
The authors declare no conflicts of interest.
References
1. Joo J, Fung MA, Jagdeo J. Successful treatment of scrotal verruciform xanthoma with shave debulking and fractionated carbon dioxide laser therapy. Dermatol Surg. 2014;40(2):214–217. doi:10.1111/dsu.12382
2. Shafer WG. Verruciform xanthoma. Oral Surg Oral Med Oral Pathol. 1971;31(6):784–789. doi:10.1016/0030-4220(71)90134-4
3. Li Z, Wang Y. Verruciform xanthoma of the thumb. Indian J Dermatol Venereol Leprol. 2018;84(1):67–69. doi:10.4103/ijdvl.IJDVL_10_17
4. Noguchi H, Kitazono I, Hamada K, et al. Verruciform xanthoma of the esophagus: two case reports with review of the literature. Int J Surg Pathol. 2020;28(3):302–305. doi:10.1177/1066896919879495
5. Roy SF, Wong J, Rahimi K. Verruciform xanthoma of the vulva in the context of lichen sclerosus: a mimicker of HPV and p53-independent intraepithelial neoplasia. Hum Pathol Rep. 2021;26:300556. doi:10.1016/j.hpr.2021.300555
6. Lee SR, Jeon JH, Jeong K, et al. Giant vulvar verruciform xanthoma can mimic a common vulvar mass, genital warts. Am J Obstet Gynecol. 2017;216(4):421–422. doi:10.1016/j.ajog.2016.11.1041
7. Santa Cruz DJ, Martin SA. Verruciform xanthoma of the vulva. Report of two cases. Am J Clin Pathol. 1979;71(2):224–228. doi:10.1093/ajcp/71.2.224
8. Barr RJ, Plank CJ. Verruciform xanthoma of the skin. J Cutan Pathol. 1980;7(6):422–428. doi:10.1111/j.1600-0560.1980.tb01216.x
9. de Rosa G, Barra E, Gentile R, et al. Verruciform xanthoma of the vulva: case report. Genitourin Med. 1989;65(4):252–254. doi:10.1136/sti.65.4.252
10. Zamora-Martinez E, Martin-Moreno L, Barat-Cascante A, et al. Another CHILD syndrome with xanthomatous pattern. Dermatologica. 1990;180(4):263–266. doi:10.1159/000248044
11. Kishimoto S, Takenaka H, Shibagaki R, et al. Verruciform xanthoma in association with a vulval fibroepithelial polyp. Br J Dermatol. 1997;137(5):816–820. doi:10.1111/j.1365-2133.1997.tb01126.x
12. Leong FJ, Meredith DJ. Verruciform xanthoma of the vulva. A case report. Pathol Res Pract. 1998;194(9):661–667. doi:10.1016/S0344-0338(98)80106-4
13. Hashimoto K, Prada S, Lopez AP, et al. CHILD syndrome with linear eruptions, hypopigmented bands, and verruciform xanthoma. Pediatr Dermatol. 1998;15(5):360–366. doi:10.1046/j.1525-1470.1998.1998015360.x
14. Reich O, Regauer S. Recurrent verruciform xanthoma of the vulva. Int J Gynecol Pathol. 2004;23(1):75–77. doi:10.1097/01.pgp.0000101143.79462.f7
15. Sopena J, Gamo R, Iglesias L, et al. Disseminated verruciform xanthoma. Br J Dermatol. 2004;151(3):717–719. doi:10.1111/j.1365-2133.2004.06164.x
16. Jingjing X, Rujun X, Nengding W, et al. Vulval and scrotal verruciform xanthoma: a report of three cases and review of literatures. J Clin Exp Pathol. 2007;23(2):163–166. Chinese.
17. Song W, Liuqing C, Hongying C, et al. Vulva verruciform xanthoma: a case report. J Clin Dermatol. 2007;65(04):231–232. Chinese.
18. Charlotte F, Françoise P, Nicolas D, et al. Vulvar verruciform xanthoma: ten cases associated with lichen sclerosus, lichen planus, or other conditions. Arch Dermatol. 2011;147(9):1087–1092.
19. Ann FM. Verruciform xanthoma in an adolescent: a case report. J Low Genit Tract Dis. 2012;16(1):70–74.
20. Yuanyuan G, Songmei G. Multiple verrucous xanthoma of vulva. The 18th annual meeting of dermatology and venereology of Chinese Medical Association, Beijing China.2012. Chinese.
21. Guo Y, Dang Y, Toyohara JP, et al. Successful treatment of verruciform xanthoma with imiquimod. J Am Acad Dermatol. 2013;69(4):e184–e186. doi:10.1016/j.jaad.2013.04.026
22. Xu XL, Huang LM, Wang Q, et al. Multiple verruciform xanthomas in the setting of congenital hemidysplasia with ichthyosiform erythroderma and limb defects syndrome. Pediatr Dermatol. 2015;32(1):135–137. doi:10.1111/pde.12198
23. Ijichi A, Mitoma C, Yasukochi Y, et al. Vulvar verruciform xanthoma developing in acquired lymphangioma circumscriptum. J Dermatol. 2017;44(5):604–605. doi:10.1111/1346-8138.13490
24. Lin F, Yang L, Qin Z, et al. Vulva verruciform xanthoma: a report of two cases. Chin J Derm Venereol. 2018;32(9):1068–1069. Chinese.
25. Yajing C, Yan W, Ping T. A case of verruciform xanthoma on the labia minora. J Clin Dermatol. 2018;47(1):29–30. Chinese.
26. Shuangli Z, Wenwen Z, Xiaokang W, et al. Verrucous xanthoma of vulva: a case report. Chin J Lepr Skin Dis. 2019;35(1):42–43. Chinese.
27. Wang G, Mochel MC, Randall MB, et al. Genital verruciform xanthoma: lessons from a contemporary multi-institutional series. Histopathology. 2020;77(5):841–846. doi:10.1111/his.14198
28. An Q, Zhang L, Gao XH, et al. Images of the month: verruciform xanthoma: an easily confused disease. Clin Med. 2020;20(4):e123–e124. doi:10.7861/clinmed.2019-0477
29. Rohwedder A, Murphy M, Carlson JA. HPV in verruciform xanthoma – sensitivity and specificity of detection methods and multiplicity of HPV types affect results. J Cutan Pathol. 2003;30(3):219–221.
30. Khaskhely NM, Uezato H, Kamiyama T, et al. Association of human papillomavirus type 6 with a verruciform xanthoma. Am J Dermatopathol. 2000;22(5):447–452. doi:10.1097/00000372-200010000-00012
31. Cumberland L, Dana A, Resh B, et al. Verruciform xanthoma in the setting of cutaneous trauma and chronic inflammation: report of a patient and a brief review of the literature. J Cutan Pathol. 2010;37(8):895–900. doi:10.1111/j.1600-0560.2009.01470.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Brucella Infectious Aneurysm: A Retrospective Study of 14 Cases and Review of the Literature – Case Report and Literature Review
Wang L, Wang Y, Ma T, Yuan J, Wang H, Ren Y, Zhang J
Infection and Drug Resistance 2023, 16:87-104
Published Date: 5 January 2023
Management of Acromioclavicular Injuries – Current Concepts
de Groot C, Verstift DE, Heisen J, van Deurzen DFP, van den Bekerom MPJ
Orthopedic Research and Reviews 2023, 15:1-12
Published Date: 16 February 2023
Epidermal Cyst on the Scalp Induced by Forceps Injury During Delivery: A Case Report and Epidemiological Analysis of 3949 Patients
Liu M, Liu X, Wang Y, Wang Z, Tuo H, Feng Y, Zheng Y
Clinical, Cosmetic and Investigational Dermatology 2023, 16:593-601
Published Date: 8 March 2023
Clinical Characteristics and Treatment of Middle-Aged and Elderly Patients with IBD in Shanghai, China
Mi L, Wang K, Yao J, Ma J, Chen YW, Zeng Q, Liu K
International Journal of General Medicine 2024, 17:6053-6064
Published Date: 11 December 2024