Back to Journals » Orthopedic Research and Reviews » Volume 15
Management of Acromioclavicular Injuries – Current Concepts
Authors de Groot C, Verstift DE, Heisen J, van Deurzen DFP, van den Bekerom MPJ
Received 3 August 2022
Accepted for publication 23 January 2023
Published 16 February 2023 Volume 2023:15 Pages 1—12
DOI https://doi.org/10.2147/ORR.S340531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Charlotte de Groot,1 Daniel E Verstift,2 Jelle Heisen,3 Derek FP van Deurzen,2 Michel PJ van den Bekerom2,4
1Department of Orthopaedic Surgery and Trauma Surgery, OLVG, Amsterdam, the Netherlands; 2Shoulder and Elbow Unit, Joint Research, Department of Orthopaedic Surgery and Trauma Surgery, OLVG, Amsterdam, the Netherlands; 3Movamento, Amsterdam, the Netherlands; 4Department of Human Movement Sciences, Faculty of Behavioural and Movement Sciences, Vrije Universiteit Amsterdam, Amsterdam Movement Sciences, Amsterdam, the Netherlands
Correspondence: Charlotte de Groot, Department of Orthopaedic Surgery and Trauma Surgery, OLVG, P.O. Box 95500, Amsterdam, 1090 HM, the Netherlands, Email [email protected]
Introduction: Treatment of a patient with acromioclavicular joint (ACJ) injury remains challenging for orthopedic surgeons. To date, there is debate over the optimal management of ACJ injuries. This review provides an overview of assessment, treatment, and future perspectives for the treatment of and research into ACJ.
Material and Methods: A scoping literature review was performed. The search was built including the following terms: acromioclavicular joint injuries or dislocation, and pathophysiology, etiology, anatomy, treatment, and trauma mechanism. The papers with evidence levels 1– 3 were included in the current narrative review.
Results: A total of 2242 potential relevant studies were identified in the searches. After removal of duplicates, 432 studies were screened on their titles and abstracts, resulting in 35 studies being included in the review, based on the eligibility criteria.
Conclusion: The management of acute and chronic ACJ injuries is not clarified in the current literature. However, there is currently insufficient high-level evidence for the overall treatment options for ACJ injuries. If surgical intervention is decided upon in consultation with the patient, the complications may not outweigh the benefits. The multitude of existing techniques is indicative of the uncertainty surrounding this issue, and no gold standard has yet been established for treatment methods. An ideal classification would include not only vertical and horizontal instability, but also the severity of kinematic alterations of the shoulder complex. This indicates the need for a new and improved diagnostic tool for the classification of ACJ injuries.
Keywords: acromioclavicular joint injury, rehabilitation, operative treatment, Rockwood classification, instability, semitendinosus graft
Introduction
Shoulder injuries are especially common among athletes and young individuals. More than 40% of these shoulder injuries are acromioclavicular joint (ACJ) injuries, with an incidence of 9.2 per 1000 people a year. There is an increase in the prevalence of ACJ injury between the ages of 20 and 40, with men having a 5–10 times higher risk of suffering an ACJ injury in comparison to women.1 Low-grade injuries are usually not associated with significant long-term morbidity,2 but other grades can lead to significant loss of strength and function of the shoulder. The weighted mean time to return to sport in operated high-grade injuries is 4 months.3 The objectives of the evaluation of a patient with ACJ injury are to identify the severity of the injuries, identify factors that can guide treatment, and choose the optimal treatment to achieve pain-free functioning of the shoulder. To date, there is debate about the optimal treatment of ACJ injuries, including the need for surgery and the best surgical method. These uncertainties raise questions about diagnosing and classifying ACJ injuries. This review aims to provide an overview of the current treatment strategies in ACJ dislocations, based on the best available evidence. In addition, this review highlights potential undervalued aspects of the diagnostic and treatment process that may change future perspectives.
Material and Methods
A scoping literature review was performed. A systematic search in PubMed and the Cochrane Database of Systematic Reviews was carried out on 24 February 2022. The search was built including the following terms: “acromioclavicular joint injuries or dislocation”, and (“pathophysiology”), or (“etiology” or “aetiology”) or (“anatomy” or (“biomechanics”) or (“treatment” or “operative treatment” or “conservative treatment” or “physiotherapy”) or (“trauma and mechanism”). Publications had to be original papers published in English. Articles were eligible for inclusion if there was a focus on ACJ dislocation. Only papers with levels of evidence 1–3 were included in the current narrative review. Exclusion criteria were case reports, editorials, articles that included fractures, and papers about specific operation techniques without reporting the results. After the selection of the eligible studies, we grouped the search into five main categories: acute grade I–II ACJ injuries, acute grade III–IV ACJ injuries, chronic injuries, ACJ revision surgery, and return to sport/work after an ACJ injury. Informed consent was provided for using the photographs in the article before participation in the study.
Results
A total of 2242 potential relevant studies were identified in the search. We used 35 studies for this review. A PRISMA flowchart of the review process is presented in Figure 1. The results from the literature search were grouped into five main categories, as follows:
- Studies relating to acute grade I–II ACJ injuries (n=4).
- Studies relating to acute grade III–VI ACJ injuries (n=16).
- Studies relating to chronic ACJ injuries (n=8).
- Studies relating to revision after ACJ surgery (n=4).
- Studies relating to return to sport/work after an ACJ injury (n=3).
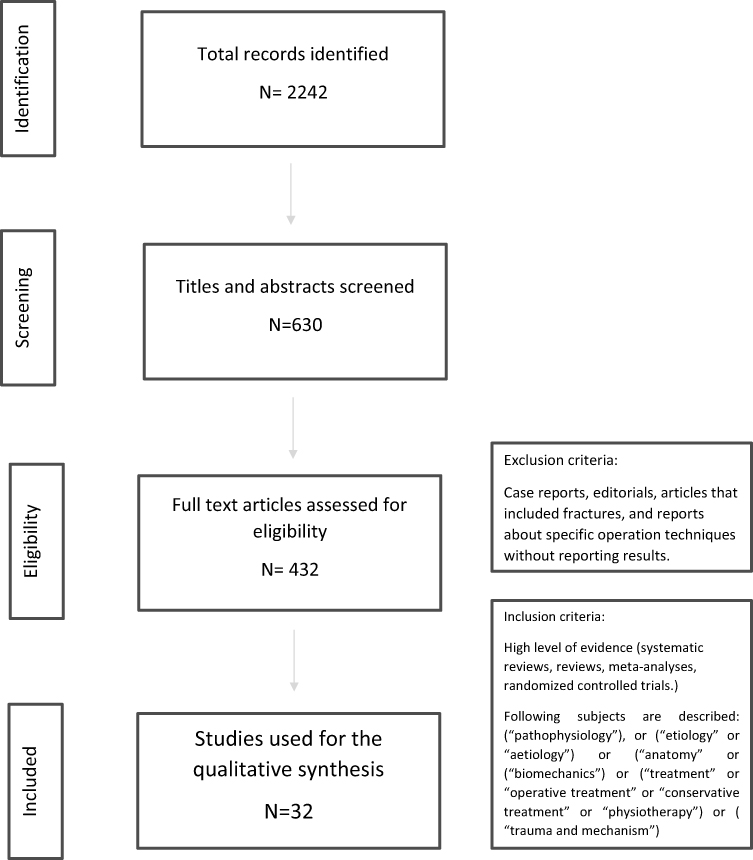 |
Figure 1 Flowchart of study selection. |
Anatomy and Biomechanics
The ACJ is one of the four joints of the shoulder complex. The normal anatomy is shown in Figure 2. The ACJ is a complex diarthrodial articulation connecting the lateral clavicle with the acromion process of the scapula, and is a plane-style synovial joint. The primary function of the ACJ is to give the scapula an additional range of scapulothoracic rotation and to allow adjustments of the scapula in order to follow the shape of the thorax as arm movement occurs. It also allows the transmission of forces from the upper extremity to the clavicle. The joint is stabilized by three ligaments and its joint capsule: the acromioclavicular ligament; the coracoclavicular ligament, which consists of two fasciculi, the trapezoid ligament and the conoid ligament; and the coracoacromial ligament. The extracapsular ligaments primarily provide vertical and compressive stability and are commonly disrupted in high-grade ACJ injuries. The capsular ligaments provide stability in the anteroposterior direction as well as vertical stability with physiological loads. Also, rotational stability is greatly affected when the capsular ligaments are injured, especially the anterior segments.4 Biomechanically, motion at the ACJ is a combination of translation, elevation, and rotational motions influenced by the complex interaction of scapulothoracic motion and guided by ligamentous restraints and dynamic muscular support. Normal biomechanics can be affected when the normal ACJ anatomy or stability is disrupted.5 Reconstructive surgery of ACJ injuries has focused for years on reducing the ACJ in the vertical plane; however, in recent years, the importance of horizontal-plane stability has been recognized.6 The cadaver study by Lee et al concluded that the conoid ligament is the primary stabilizer of superior displacement of the clavicle.7 The ACJ capsular ligament is the primary stabilizer of inferior displacement of the clavicle. The capsular ligament and conoid ligament contribute equally to anterior stability. The capsular ligament is the primary contributor to posterior stability.7 The contributions of the capsular and extracapsular ligaments to ACJ stability are synergistic, and this supports the need for anatomic reconstruction.4 The resection of the lateral clavicle affects the stability, especially increased horizontal translation, and careful consideration is necessary before choosing such an intervention.8
 |
Figure 2 Anatomy of the shoulder (courtesy of shoulder and elbow expertise center). |
Trauma Mechanism
An ACJ injury can occur as a result of either direct or indirect trauma, although a major cause of ACJ separation is a direct blow to the lateral acromion with the arm in an adducted position.9 Indirect injury is generally position related and can occur after a fall onto the ipsilateral extremity in either an adducted or outstretched position, which makes the acromioclavicular and coracoclavicular ligaments more vulnerable to injury.10 These injuries are most common in contact sports such as hockey, wrestling, and rugby.11 A 2013 study found that almost 30% of injuries in American professional football players of the National Football League are ACJ related.11
Physical Examination
Physical examination of the patient’s shoulder after an ACJ injury may reveal swelling, hematoma, and a deformity of the ACJ, combined with restriction in the active and passive range of motion secondary to pain. The “piano key sign” may be seen, with an elevation of the clavicle relative to the acromion, which rebounds after inferior compression. To test horizontal instability, the distal clavicle is shifted posteriorly while the acromion is fixed with the other hand. An increased posterior translation in comparison to the unaffected side indicates a horizontal component to the ACJ instability.12 Finally, it is essential to evaluate the entire clavicle for possible fractures or sternoclavicular injuries, as well as performing a full neurovascular examination on the affected extremity.
The diagnostic values of three commonly used physical tests have been reported for chronic ACJ injuries.13 The cross-body adduction stress test showed the greatest sensitivity (77%) and the active compression test had the greatest specificity (95%). All tests had a negative predictive value of greater than 94%, but the positive predictive value was less than 30% for all tests. The active compression test had the highest overall accuracy (92%), followed by the acromioclavicular resisted extension test (84%) and the cross-arm adduction stress test (79%). Combinations of the tests increased the diagnostic values for chronic ACJ lesions.13 There is increasing evidence that scapulothoracic kinematics should be assessed in patients with ACJ injuries. Several studies have reported on scapulothoracic dyskinesia following ACJ dislocation, ranging from abnormalities in scapular motor control to “winging” of the inferomedial angle to the medial border, and prominence of the angulus superior.14–16 Kinematic changes in the shoulder complex have been described in a cadaveric study of ACJ injuries, in which alterations were seen in both the ACJ and movements of the scapula.17 Physical examination not only involves the ACJ; it is important to examine the entire chain of motion of the shoulder complex to identify ACJ injuries more clearly.
Radiology and Classification
Proper radiographic evaluation of the ACJ requires an anteroposterior, lateral and axial view. However, a Zanca view is the most accurate view for examining the ACJ for the assessment of subtle deformities.18 The axial view of the shoulder is important in differentiating a type III ACJ injury from a type IV injury. A type IV lesion will show the scapula anterior to the clavicle. The configuration of the ACJ on anteroposterior radiographs varies substantially. The ACJ width is normally between 1 and 3 mm.6 It is difficult to diagnose horizontal ACJ instability using plain radiographs; dynamic views, compared with static views and sonography, were shown in some cases to better detect horizontal instability.19,20 Weighted bilateral comparative views can be required for an accurate classification of the ACJ, as the addition of weights may differentiate a type V injury from a type III.21 The radiographic classification of ACJ injuries was initially described by Rockwood et al22 (Figure 3). A type I injury is where only the acromioclavicular (AC) ligaments are sprained, but the joint is intact. Radiographically, there is no widening, separation, or deformity at the ACJ. In type II injuries, the AC ligaments are torn, but the coracoclavicular (CC) ligaments are intact. Radiography demonstrates that the distal clavicle is slightly elevated, but there is no enlargement of the CC interspace. In type III injuries, both the AC and the CC ligaments are torn. X-rays reveal that the distal clavicle is totally displaced in relation to the acromion, but there is no more than 100% increase of the CC interspace. Type IV injuries are characterized by complete dislocation with posterior displacement of the distal clavicle into or through the fascia of the trapezius. Type V injuries are characterized by a greater superior dislocation. On bilateral X-ray, there is a 100–300% increase in the CC interspace. Type VI injuries are inferior ACJ dislocations into a subacromial or subcoracoid position.
 |
Figure 3 Rockwood classification (courtesy of shoulder and elbow expertise center). |
The Upper Extremity Committee of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) proposed a subclassification of the original Rockwood type III dislocation into stable (type IIIA) and unstable (type IIIB) variants.23 Grade IIIA injuries are defined by a stable ACJ without overriding of the clavicle on the cross-body adduction view and without significant scapular dysfunction. Unstable grade IIIB injuries are defined by therapy-resistant scapular dysfunction and an overriding clavicle on the cross-body adduction view. Karargyris et al described the acromial centerline to dorsal clavicle (AC-DC) radiographic measurement to improve the identification of unstable ACJ injuries.24 The authors concluded that use of the AC-DC measurement on an Alexander view provides the clinician with a more realistic appreciation of true ACJ displacement, particularly in the presence of posterior horizontal displacement such as that seen in Rockwood IV injuries.25 The systematic review by Pogorzelski et al reported that the interobserver and intraobserver reliability for diagnosing vertical instabilities of the clavicle using bilateral projections showed a high level of reproducibility in acute ACJ injuries26 The results for horizontal instabilities were more heterogeneous. They concluded that there is currently no clear consensus on a protocol for the image-based diagnosis and classification of acute ACJ injuries. This lack of consensus may be related to the non-optimal reliability and clinical utility of the current classifications.
Acute Injuries – Low Grade
By consensus, a non-operative strategy has been identified as the first choice of treatment for low-grade ACJ dislocations.27 The current literature is consistent about the treatment strategies for the initial acute phase, which include the use of a sling, analgesics, and anti-inflammatory modalities, followed by a rehabilitation program.27 Some of the exercise programs were recommended from 4–6 weeks post-injury, and included strengthening and coordination exercises for the scapula stabilizers and rotator cuff. But none of these exercise programs can be reported as “evidence-based care”. Long-term complaints are widely reported, such as modifications in work or sport, ACJ-related symptoms and deficit of function, and the need for surgery for ongoing symptoms.27 LeVasseur et al claim that standardized rehabilitation protocols do not allow for constructive modification of treatment, resulting in a lesser degree of recovery for the patient. The quality of patient care can be improved with guidelines for exercise or rehabilitation programs, which should focus on the management of pain, anxiety, and (anterior chest wall) stiffness, and be more appropriate to the needs of the individual patient.28 Verstift et al reported outcomes after non-operative therapy for low-grade ACJ injuries, regarding functional and radiological outcomes. Compared to the contralateral, non-injured shoulder, the outcomes of the injured shoulder were not clinically different after a follow-up of 85 months. Radiological changes were seen; patient had similar rates of degeneration, more frequent osteolysis and deformity of the distal clavicle, and more ossification of the ligaments. However, the need for subsequent surgery was low.2 In conclusion, low-grade injuries can be treated conservatively, and full rehabilitation should be achieved within 6–12 weeks.23
Acute Injuries – High Grade
High-grade ACJ dislocations are all injuries classified as Rockwood type IIIB and higher. In 2019, a panel of European Shoulder Associates–European Society of Sport, Traumatology, Knee Surgery and Arthroscopy (ESA-ESSKA) members achieved consensus regarding the treatment of ACJ injuries.29 In cases where surgical treatment is deemed necessary, arthroscopically assisted (no minimally invasive surgery) anatomic reconstruction, using a suspensory device with no need for a biological augmentation, is thought to be the right method in acute injuries. Consensus was reached on the Rockwood classification plus the ISAKOS statement on type III injuries.29 To our knowledge, no randomized trial or prospective study has identified the superiority of surgical treatment over non-operative treatment.
There is an ongoing debate regarding the indication for surgery for type III injuries in young (overhead) active patients. To date, the literature has reported no differences in stable or unstable Rockwood type III ACJ dislocations. To our knowledge, no high-level evidence study has selectively focused on Rockwood type IIIB ACJ dislocations. Kim and Koh reported that there is no difference in clinical outcomes between operative and non-operative treatment of type III ACJ dislocation.30 The systematic review by Longo et al reported that there were several advantages associated with non-operative treatment, including the shorter period of rehabilitation, no hospitalization, and satisfactory functional results in most patients. In contrast, a moderate rate of persistent pain, instability, and limitation of motion were described as disadvantages of non-operative treatment. Non-operative treatment results in a lower incidence of complications, such as ossification of the CC ligament and osteolysis of the lateral clavicle, compared with surgical treatment.31 No difference is seen in terms of clinical outcomes, and the study by Windhamre et al reported even better patient-reported outcomes (Constant score, Subjective Shoulder Value, QuickDASH [Quick Disabilities of the Arm, Shoulder and Hand]) and less pain at rest and during movement, compared to operative treatment.32–35,53 Furthermore, 18% of non-operatively treated patients converted within 19 months to the surgery group. Non-operative treatment failure is more likely when patients presented more than 30 days after the initial injury.33
Although high-level evidence is lacking, there is consensus that in type V ACJ dislocations there may be an indication for surgery. Numerous operative techniques have been described. In 2019, Gowd et al reported a systematic review and meta-analysis of the following techniques; suture or button fixation, synthetic artificial ligament, tendon graft, and Weaver–Dunn coracoacromial ligament transfer.36 Comparison of open and arthroscopic ACJ reconstruction techniques revealed no differences in loss of reduction, complication rate, or revision rate. The (modified) Weaver–Dunn procedure has long been regarded as one of the most effective techniques to treat complete ACJ dislocation. However, new anatomic reconstructions have demonstrated superior results.37–39 The hook-plate technique demonstrates inferior results (significantly longer hospitalization time, higher estimated blood loss, lower Constant and higher VAS scores, and higher incidence of failure) compared to other techniques, and should be removed as an option.40–42 The systematic review by Saccomanno et al described the surgical treatment of high-grade ACJ dislocations (Rockwood type III–V). Suture buttons seemed to be the favored choice in the acute setting.43
Complications were reported by Marsalli et al in patients with Rockwood type V ACJ dislocation who were undergoing arthroscopic coracoclavicular fixation. The most commonly described complication was loss of reduction of >1 mm. Patient older than 55 years and woman were more likely to develop a secondary ACJ disease. ACJ pain was more often seen in patients with osteolysis and loss of reduction of more than 5 mm.44 In conclusion, there is no consensus that surgical intervention is necessary for acute high-grade lesions classified through a radiological classification system. If a surgical treatment is performed, suture buttons seem to be the favored choice in the acute setting.
Chronic Injuries
The definition of chronic injuries varies in the literature. The majority of authors do not define this term explicitly. The systematic review by Flint et al concluded that ACJ dislocations are acute if the sustained trauma was less than 6 weeks ago and chronic when the trauma was more than 6 months ago.45 Rapid operative management may not be necessary for high-grade injuries, as most patients may still benefit from surgery at a later stage.46 Song et al, however, found that early surgical treatment is superior to delayed surgical treatment in terms of functional outcome and reduction.47 Optimal timing is not clear, and some of the studies were performed with older techniques. There is no gold standard for operative techniques in chronic injuries. Sircana et al systematically reviewed the different surgical techniques and reported superior outcome of arthroscopic techniques over open procedures. Anatomic–biological non-augmented graft reconstruction showed better patient-reported outcomes and better shoulder function compared to augmented techniques. Combined CC and AC ligament reconstruction showed better Constant and American Shoulder and Elbow Surgeons (ASES) scores compared to isolated CC ligament reconstruction.48 However, conclusions were drawn based on studies with low levels of evidence. The systematic review by Borbas et al compared a non-biological fixation between the coracoid and clavicle, a biological reconstruction of the CC ligament, and ligament and/or tendon transfer. No differences were seen for any of their groups, including the Constant score and the overall complication rate.39 Recent cadaveric studies showed that native stability in the horizontal and vertical planes can be restored in anterior, posterior, superior, and inferior stability measures when performing suture or button reconstruction that passed directly through tunnels in the clavicle and coracoid, compared to tape implants wrapped around the bones.49 The only level 2 study that was described in this review showed superior results when ACJ reconstruction was performed with a tendon graft.50 This prospective randomized comparative study showed that chronic dislocation using a semitendinosus allograft, compared to synthetic stabilization (Ligament Augmentation and Reconstruction System), had better clinical scores on one- and four-year follow-up. A limitation of this study is that no comparison was made between allograft and autograft reconstruction. Figure 4 shows a reconstruction of a chronic luxation with a semitendinosus graft. Eigenschink et al reported, in a recent systematic review, that there are no significant differences in clinical outcomes, risk of revision surgery, and overall complications between allograft and autograft reconstruction.51 There may be an increased risk of loss of reduction with allografts versus autografts. However, they reported that the published studies are generally of low quality with low levels of evidence. Late symptomatic ACJ osteoarthritis is reported in patients with chronic ACJ injuries, and can be treated conservatively or with a distal clavicle resection. If a distal clavicle resection is performed, a higher risk of superior capsule damage and bone loss can commonly result in ACJ instability.8,52 It may be concluded that, despite the lack of high-level research, there is some evidence that a graft may be the best surgical option for chronic ACJ reconstruction.
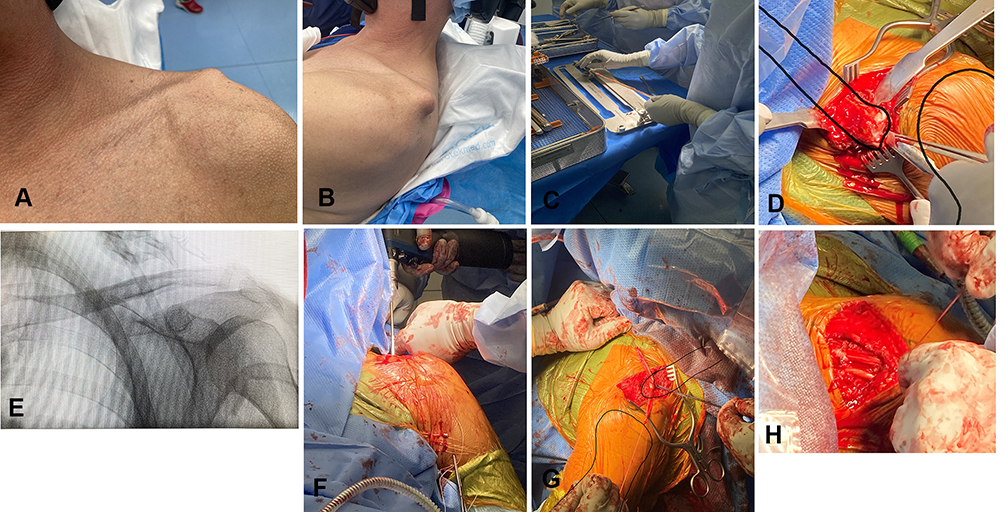 |
Figure 4 Reconstruction of chronic ACJ injury with semitendinosus graft. (A) Pre-operation luxation. (B) Pre-operation luxation. (C) Preparation of semitendinosus graft. (D) Preparation of clavicle. (E) Positioning of clavicle. (F) Bone tunnels. (G) Ligament reconstruction. (H) Ligament reconstruction. |
Revision and Complications
Complications are described for low-grade and high-grade ACJ injuries. Non-operative treatment shows a lower incidence of complications but is associated with poorer cosmetic outcome.34,53 Surgical treatment of ACJ instability is associated with a variable rate of postoperative radiographic and clinical complications, which have been reported to vary between 5% and 88.9% of patients.54 The systematic review by Woodmass et al described the five most commonly documented complications after arthroscopic fixation of acromioclavicular separations: superficial infection, with a pooled rate of 3.8%; shoulder pain, with a pooled rate of 26.7%; CC calcification, with a pooled rate of 31.6%; fracture, with a pooled rate of 5.3%; and loss of reduction, with a pooled rate with 26.8%.55 In revision surgery, the initial treatment technique is not always possible because of fracture or bone loss, and applying an alternative surgical technique can be difficult because of the complicated anatomy of the joint. Dyrna et al described treatment options for revision for three different reasons: when failure is because of new trauma or insufficient primary fixation, an anatomic stabilization of the CC and AC ligaments using a tendon graft is suggested; if clinically and/or radiographically noticeable horizontal instability is the reason for failure, anatomic reconstruction is preferred, with the focus on the acromioclavicular capsule during the repair; and, in case of fractures or massive bone loss, open reduction and internal fixation of the clavicle in combination with a biological tendon graft is preferred.54 Restoring the native joint biomechanics will translate into long-term stabilization and patient contentment.54 Not all complications require revision surgery, but if it is performed, similar operative management as in chronic ACJ injury is preferred.
Return to Sport/Work
Most ACJ injuries occur in young and active individuals. A fast recovery and return to sport or work is desirable. Kay et al systematically described that the rate of return to any sporting activities ranged from 94% to 100%.56 Return to the preinjury level of sport ranges from 62% to 100%.56 The time to return to sport was reported as being from 2.3 to 6 months postoperatively for acute and chronic ACJ injuries after surgical treatment.54 Verstift et al reported similar rates of return to sport of 94%, with the mean rate of return to sport ranging from 76% to 100%. Patients who were surgically treated for high-grade ACJ injuries were allowed to return to sport after 3 months, with a mean time ranging from 2.5 to 5.3 months. Moreover, 84% of patients returned to the same level of preinjury sports, ranging from 62% to 100%. Adequate rehabilitation to return to work is also important.3 To our knowledge, fewer high-quality articles have described return to work. Porschke et al conclude, in a retrospective case study, that 94% of patients returned to work, while 76% became temporarily incapacitated to work after surgery. Most of the patients who became temporarily incapacitated to work, 88.2%, did manual labor, and needed more than twice as long to return to work compared to non-manual workers; 15.5 weeks versus 6 weeks.57
Discussion
The current literature has too low a level of evidence to allow definitive conclusions to be drawn. There is no consensus that surgical intervention leads to superior results for acute high-grade lesions, and the lack of high-level evidence makes decision making difficult. Patients with chronic ACJ lesions are probably more suitable for surgery because the patient is still symptomatic and more motivated to undergo surgery. The current literature cannot give a good indication of which patients will continue to have symptoms, and the Rockwood classification cannot differentiate between patients who will benefit from surgery and those who will not. Clinical observation, a physical examination of the entire shoulder complex, the patient’s symptoms, and differentiation between patients with low and high demands will be more important and may provide more insight into the severity of the injury and the risk of long-term symptoms. To better understand the role of the stabilizing ligaments of the ACJ, Lee et al conducted a cadaver study. They concluded that the conoid ligament is the primary stabilizer of the superior displacement of the clavicle at the ACJ and contributes considerably to anterior–posterior stability. Reconstruction of the ACJ capsular ligament should be considered in high-grade and horizontally unstable injuries.7 Also, the cadaver study of Dyrna et al showed that native translational stability could be restored by the addition of AC capsule augmentation. Rotational instability partially remained.4 All ligaments play an important role in the stabilization of the ACJ. However this does not give a direct indication of the appropriate treatment.
In order to make a connection between complaints and anatomic changes, physical examination seems to be increasingly important, encompassing not only the function of the ACJ, but the function of the entire shoulder complex. This is confirmed by a cadaver study focusing not only on the kinematic alterations during humerothoracic movements but also on the alterations during scapulothoracic movements in patients with a Rockwood type V injury.17 The literature described the relationship of scapular dyskinesis and scapular inferior coracoid dyskinesis (SICK) syndrome to ACJ dislocation. Gumina et al reported that patients affected by type III chronic ACJ injury develop scapular dyskinesis and SICK syndrome in 70% and 58% of cases, respectively.16 A rehabilitation program for patients with chronic type III ACJ injuries and SICK syndrome was studied by Carbone et al; after 12 months, in 78% of the patients the scapular dyskinesis was no longer present, and significantly better Constant scores and infraspinatus strength were achieved.58 This study shows that there are more factors at play when examining shoulder function after acromioclavicular injuries. Taking into account the entirety of the shoulder complex may provide insight into which patients will benefit from surgery and who will benefit from individualized rehabilitation or physiotherapy. The biomechanical function and all anatomic structures of the ACJ can potentially provide information about the patient’s symptoms and link them to the severity of the injury.
The current Rockwood classification, despite the addition of the ISAKOS committee, does not seem to be able to accurately predict patients in need of surgery. An ideal classification would include not only vertical and horizontal instability, but also the severity of kinematic alterations of the shoulder complex. If it were possible to create a classification that could better indicate high-grade lesions, there would be a better selection of those patients who have a high level of long-term symptoms and require surgical treatment.
Conclusion
The management of acute and chronic ACJ injuries is not clarified in the current literature. If surgical intervention is decided upon in consultation with the patient, the complications may not outweigh the benefits. The multitude of existing techniques is indicative of the uncertainty surrounding this issue, and no gold standard has yet been established. However, we aim for low-grade injuries to be treated conservatively and there is no consensus that surgical intervention is necessary for acute high-grade lesions. There is some evidence that a graft may be the best choice for chronic injuries and revision surgery. Biomechanical studies on the function of the shoulder complex and ACJ can be helpful to better understand the complexity of the ACJ in relation to the shoulder complex, and may give answers to better differentiate the severity of acromioclavicular injuries. In Figure 5, we present a flowchart with our opinion of the current literature and management of ACJ dislocations. There is a need for a new and improved diagnostic tool for the classification of ACJ injuries.
 |
Figure 5 Flowchart of our opinion of the current literature and management of ACJ dislocations. |
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
Dr Derek FP van Deurzen reports personal fees and grants from Wright Medical and reports fellowship funding from Smith and Nephew. The authors report no other conflicts of interest in this work.
References
1. Pallis M, Cameron KL, Svoboda SJ, Owens BD. Epidemiology of acromioclavicular joint injury in young athletes. Am J Sports Med. 2012;40(9):2072. PMID: 22707749. doi:10.1177/0363546512450162.
2. Verstift Daniël E, Kilsdonk ID, van Wier MF, et al. Long-term outcome after nonoperative treatment for Rockwood I and II acromioclavicular joint injuries. Am J Sports Med. 2021;49:757–763. doi:10.1177/0363546520981993
3. Verstift DE, Welsink CL, Spaans AJ, et al. Return to sport after surgical treatment for high-grade (Rockwood III-VI) acromioclavicular dislocation. Knee Surg Sports Traumatol Arthrosc. 2019;27:3803–3812. doi:10.1007/s00167-019-05528-w
4. Dyrna F, Imhoff FB, Haller B, et al. Primary stability of an acromioclavicular joint repair is affected by the type of additional reconstruction of the acromioclavicular capsule. Am J Sports Med. 2018;46(14):3471–3479. PMID: 30419178. doi:10.1177/0363546518807908
5. Keener JD. Acromioclavicular joint anatomy and biomechanics. Oper Tech Sports Med. 2014;22(3):210–213. doi:10.1053/j.otsm.2014.02.018
6. Maristella F, De Ieso C, Milano G, et al.; Biomechanica extra: Saccomanno. Acromioclavicular joint instability: anatomy, biomechanics and evaluation. Joints. 2014;2:87–92. doi:10.11138/jts/2014.2.2.087
7. Lee J, El-Daou H, Alkoheji M, et al. Ligamentous and capsular restraints to anterior-posterior and superior-inferior laxity of the acromioclavicular joint: a biomechanical study. J Shoulder Elbow Surg. 2021;30:1251–1256. doi:10.1016/j.jse.2020.09.006
8. Beitzel K, Sablan N, Chowaniec DM, et al. Sequential resection of the distal clavicle and its effects on horizontal acromioclavicular joint translation. Am J Sports Med. 2012;40(3):681–685. PMID: 22156172. doi:10.1177/0363546511428880.
9. Warth RJ, Martetschlager F, Gaskill TR, Millett PJ. Acromioclavicular joint separations. Curr Rev Musculoskelet Med. 2013;6(1):71–78. doi:10.1007/s12178-012-9144-9
10. Johansen JA, Grutter PW, McFarland EG, Petersen SA. Acromioclavicular joint injuries: indications for treatment and treatment options. J Shoulder Elbow Surg. 2011;20:S70–S82. doi:10.1016/j.jse.2010.10.030
11. Lynch TS, Saltzman MD, Ghodasra JH, Bilimoria KY, Bowen MK, Nuber GW. Acromioclavicular joint injuries in the National Football League: epidemiology and management. Am J Sports Med. 2013;41(12):2904–2908. doi:10.1177/0363546513504284
12. Tauber M. Management of acute acromioclavicular joint dislocations: current concepts. Arch Orthop Trauma Surg. 2013;133(7):985–995. PMID: 23632779. doi:10.1007/s00402-013-1748-z.
13. Chronopoulos E, Kim TK, Park HB, Ashenbrenner D, McFarland EG. Diagnostic value of physical tests for isolated chronic acromioclavicular lesions. Am J Sports Med. 2004;32(3):655–661. PMID: 15090381. doi:10.1177/0363546503261723.
14. Taft TN, Wilson FC, Oglesby JW. Dislocation of the acromioclavicular joint. An end-result study. J Bone Joint Surg Am. 1987;69:1045–1051. doi:10.2106/00004623-198769070-00013
15. Walsh WM, Peterson DA, Shelton G, et al. Shoulder strength following acromioclavicular injury. Am J Sports Med. 1985;13:153–158. doi:10.1177/036354658501300302
16. Gumina S, Carbone S, Postacchini F. Scapular dyskinesis & SICK scapula syndrome in patients with chronic type III acromioclavicular dislocation. J Arthroscopy. 2009;25(1):40–45. doi:10.1016/j.arthro.2008.08.019
17. Peeters I, Braeckevelt T, Herregodts S, et al. Kinematic alterations in the shoulder complex in Rockwood V acromioclavicular injuries during humerothoracic and scapulothoracic movements: a whole-cadaver study. Am J Sports Med. 2021;49:3988–4000. doi:10.1177/03635465211053016
18. Zanca P. Shoulder pain: involvement of the acromioclavicular joint. (Analysis of 1000 cases). Am J Roentgenol Radium Ther Nucl Med. 1971;112(3):493–506. PMID: 5570359. doi:10.2214/ajr.112.3.493.
19. Bockmann B, Venjakob AJ, Thrasyvoulidis G, Holschen M, Schulte TL, Nebelung W. Sonographic measurement of dynamic horizontal instability in acromioclavicular joint instability: description of a simple technique and correlation to radiographic parameters. J Ultrasound Med. 2022;41(2):409–415. PMID: 33955022. doi:10.1002/jum.15719.
20. Aliberti GM, Kraeutler MJ, Trojan JD, Mulcahey MK. Horizontal Instability Of The Acromioclavicular Joint: A Systematic Review. Am J Sports Med. 2020;48(2):504–510. PMID: 31013137. doi:10.1177/0363546519831013.
21. Ibrahim EF, Forrest NP, Forester A. Bilateral weighted radiographs are required for accurate classification of acromioclavicular separation: an observational study of 59 cases. Injury. 2015;46(10):19005. PMID: 26194267. doi:10.1016/j.injury.2015.06.028.
22. Rockwood CA
23. Beitzel K, Mazzocca AD, Bak K, et al. ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy. 2014;30:271–278. doi:10.1016/j.arthro.2013.11.005
24. Karargyris O, Murphy RJ, Arenas A, Bolliger L, Zumstein MA. Improved identification of unstable acromioclavicular joint injuries in a clinical population using the acromial center line to dorsal clavicle radiographic measurement. J Shoulder Elbow Surg. 2020;29(8):1599–1605. PMID: 32147334. doi:10.1016/j.jse.2019.12.014.
25. Alexander OM. Radiography of the acromioclavicular articulation. Med Radiogr Photogr. 1954;30(2):34–39.
26. Pogorzelski J, Beitzel K, Ranuccio F, et al. The acutely injured acromioclavicular joint - which imaging modalities should be used for accurate diagnosis? A systematic review. BMC Musculoskelet Disord. 2017;18(1):515. PMID: 29216919; PMCID: PMC5721483. doi:10.1186/s12891-017-1864-y
27. Reid D, Polson K, Johnson L, et al. Acromioclavicular joint separations grades I-III: a review of the literature and development of best practice guidelines. Sports Med. 2012;42:681–696. doi:10.2165/11633460-000000000-00000
28. LeVasseur MR, Mancini MR, Berthold DP, et al. Acromioclavicular joint injuries: effective rehabilitation. Open Access J Sports Med. 2021;12:73–85. doi:10.2147/OAJSM.S244283
29. Rosso C, Martetschläger F, Saccomanno MF, et al. High degree of consensus achieved regarding diagnosis and treatment of acromioclavicular joint instability among ESA-ESSKA members. Knee Surg Sports Traumatol Arthrosc. 2021;29:2325–2332. doi:10.1007/s00167-020-06286-w
30. Kim S-H, Koh K-H. Treatment of Rockwood type III acromioclavicular joint dislocation. Clin Shoulder Elb. 2018;21:48–55. doi:10.5397/cise.2018.21.1.48
31. Longo UG, Ciuffreda M, Rizzello G, et al. Surgical versus conservative management of Type III acromioclavicular dislocation: a systematic review. Br Med Bull. 2017;122:31–49. doi:10.1093/bmb/ldx003
32. Tang G, Zhang Y, Liu Y, et al. Comparison of surgical and conservative treatment of Rockwood type-III acromioclavicular dislocation: a meta-analysis. Medicine. 2018;97:e9690. doi:10.1097/MD.0000000000009690
33. Windhamre H. No difference in clinical outcome at two-year follow-up in patients with acromioclavicular joint dislocation type III and V treated with hook plate or physiotherapy: a randomized controlled trial. J Shoulder Elbow Surg. 2022. doi:10.1016/j.jse.2021.12.003
34. Chang N, Furey A, Kurdin A, et al. Operative versus nonoperative management of acute high-grade acromioclavicular dislocations: a systematic review and meta-analysis. J Orthop Trauma. 2018;32:1–9. doi:10.1097/BOT.0000000000001004
35. Petri M, Warth RJ, Greenspoon JA, et al. Clinical results after conservative management for grade III acromioclavicular joint injuries: does eventual surgery affect overall outcomes? Arthroscopy. 2016;32:740–746. doi:10.1016/j.arthro.2015.11.024
36. Gowd AK, Liu JN, Cabarcas BC, et al. Current concepts in the operative management of acromioclavicular dislocations: a systematic review and meta-analysis of operative techniques. Am J Sports Med. 2019;47:2745–2758. doi:10.1177/0363546518795147
37. Xará-Leite F, Andrade R, Moreira PS, et al. Anatomic and non-anatomic reconstruction improves post-operative outcomes in chronic acromio-clavicular instability: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2019;27(12):3779–3796. PMID: 30806755. doi:10.1007/s00167-019-05408-3
38. Moatshe G, Kruckeberg BM, Chahla J, et al. Acromioclavicular and coracoclavicular ligament reconstruction for acromioclavicular joint instability: a systematic review of clinical and radiographic outcomes. Arthroscopy. 2018;34(6):
39. Borbas P, Churchill J, Ek ET. Surgical management of chronic high-grade acromioclavicular joint dislocations: a systematic review. J Shoulder Elbow Surg. 2019;28(10):2031. PMID: 31350107. doi:10.1016/j.jse.2019.03.005
40. Nie S, Lan M. Comparison of clinical efficacy between arthroscopically assisted Tight-Rope technique and clavicular hook plate fixation in treating acute high-grade acromioclavicular joint separations. J Orthop Surg. 2021;29:23094990211010562. doi:10.1177/23094990211010562
41. Qi W, Xu Y, Yan Z, et al. The tight-rope technique versus clavicular hook plate for treatment of acute acromioclavicular joint dislocation: a systematic review and meta-analysis. J Invest Surg. 2021;34:20–29. doi:10.1080/08941939.2019.1593558
42. Pan X, Lv RY, Lv MG, Zhang DG. TightRope vs clavicular hook plate for Rockwood III-V acromioclavicular dislocations: a meta-analysis. Orthop Surg. 2020;12:1045–1052. doi:10.1111/os.12724
43. Saccomanno MF, Sircana G, Cardona V, et al. Biologic and synthetic ligament reconstructions achieve better functional scores compared to osteosynthesis in the treatment of acute acromioclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2021;29(7):2175–2193. PMID: 32797247. doi:10.1007/s00167-020-06217-9
44. Marsalli M, Bistolfi G, Morán N, et al. High early-onset acromioclavicular secondary pathologies after acute arthroscopic joint reduction: a cohort study. Arch Orthop Trauma Surg. 2021;142:1623–1631. doi:10.1007/s00402-021-04123-4
45. Flint JH, Wade AM, Giuliani J, et al. Defining the terms acute and chronic in orthopaedic sports injuries. Am J Sports Med. 2014;42:235–241. doi:10.1177/0363546513490656
46. Lädermann A, Denard PJ, Collin P, Cau JB, Van Rooij F, Piotton S. Early and delayed acromioclavicular joint reconstruction provide equivalent outcomes. J Shoulder Elbow Surg. 2021;30:635–640. doi:10.1016/j.jse.2020.06.026
47. Song T, Yan X, Ye T, et al. Comparison of the outcome of early and delayed surgical treatment of complete acromioclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2016;24:194350. doi:10.1007/s00167-014-3225-9
48. Sircana G, Saccomanno MF, Mocini F, et al. Anatomic reconstruction of the acromioclavicular joint provides the best functional outcomes in the treatment of chronic instability. Knee Surg Sports Traumatol Arthrosc. 2021;29:2237–2248. doi:10.1007/s00167-020-06059-5
49. Alkoheji M, El-Daou H, Lee J, et al. Acromioclavicular joint reconstruction implants have differing ability to restore horizontal and vertical plane stability. Knee Surg Sports Traumatol Arthrosc. 2021;29:3902–3909. doi:10.1007/s00167-021-06700-x
50. Fauci F, Merolla G, Paladini P, et al. Surgical treatment of chronic acromioclavicular dislocation with biologic graft vs synthetic ligament: a prospective randomized comparative study. J Clin Orthop Trauma. 2013;14:283–290. doi:10.1007/s10195-013-0242-2
51. Eigenschink M, Heuberer PR, Pauzenberger L, et al. Allo- and autografts show comparable outcomes in chronic acromioclavicular joint reconstruction: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2021;29:2202–2211. doi:10.1007/s00167-021-06445-7
52. Soler F, Mocini F, Djemeto DT, Cattaneo S, Saccomanno MF, Milano G. No differences between conservative and surgical management of acromioclavicular joint osteoarthritis: a scoping review. Knee Surg Sports Traumatol Arthrosc. 2021;29(7):2194–2201. PMID: 33386878. doi:10.1007/s00167-020-06377-8
53. Korsten K, Gunning AC, Leenen LP. Operative or conservative treatment in patients with Rockwood type III acromioclavicular dislocation: a systematic review and update of current literature. Int Orthop. 2014;38(4):831–838. PMID: 24178060; PMCID: PMC3971277. doi:10.1007/s00264-013-2143-7
54. Dyrna F, Berthold DP, Feucht MJ, et al. The importance of biomechanical properties in revision acromioclavicular joint stabilization: a scoping review. Knee Surg Sports Traumatol Arthrosc. 2019;27:3844–3855. doi:10.1007/s00167-019-05742-6
55. Woodmass JM, Esposito JG, Ono Y, et al. Complications following arthroscopic fixation of acromioclavicular separations: a systematic review of the literature. Open Access J Sports Med. 2015;6:97–107. PMID: 25914562; PMCID: PMC4401206. doi:10.2147/OAJSM.S73211
56. Kay J, Memon M, Alolabi B. Return to sport and clinical outcomes after surgical management of acromioclavicular joint dislocation: a systematic review. Arthroscopy. 2018;34:2910–2924.e1. doi:10.1016/j.arthro.2018.04.027
57. Porschke F, Schnetzke M, Studier-Fischer S, et al. Return to work after acromioclavicular joint stabilization: a retrospective case control study. J Orthop Surg Res. 2019;14:45. doi:10.1186/s13018-019-1071-7
58. Carbone S, Postacchini R, Gumina S. Scapular dyskinesis and SICK syndrome in patients with a chronic type III acromioclavicular dislocation. Results of rehabilitation. Knee Surg Sports Traumatol Arthrosc. 2015;23(5):1473–1480. PMID: 24458335. doi:10.1007/s00167-014-2844-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Vulvar Verruciform Xanthoma: A Comprehensive Literature Review
Wu W, Sun L, Lu J, Yang X, Liu Q, Wang J
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1675-1680
Published Date: 18 August 2022
Epidermal Cyst on the Scalp Induced by Forceps Injury During Delivery: A Case Report and Epidemiological Analysis of 3949 Patients
Liu M, Liu X, Wang Y, Wang Z, Tuo H, Feng Y, Zheng Y
Clinical, Cosmetic and Investigational Dermatology 2023, 16:593-601
Published Date: 8 March 2023
Guillain-Barré Syndrome: Progress in Diagnosis, Biomarkers, Neuroimaging and Management
Freiha J, Min YG, Osman C, Rajabally YA
ImmunoTargets and Therapy 2026, 15:390161
Published Date: 2 April 2026