Back to Journals » Infection and Drug Resistance » Volume 16
Brucella Infectious Aneurysm: A Retrospective Study of 14 Cases and Review of the Literature – Case Report and Literature Review
Authors Wang L, Wang Y, Ma T, Yuan J ![]() , Wang H
, Wang H ![]() , Ren Y, Zhang J
, Ren Y, Zhang J
Received 19 October 2022
Accepted for publication 16 December 2022
Published 5 January 2023 Volume 2023:16 Pages 87—104
DOI https://doi.org/10.2147/IDR.S393060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Lin Wang,1 Yan Wang,1 Tongqiang Ma,2 Jianwei Yuan,1 Hongxia Wang,1 Yuan Ren,3 Jianwei Zhang1
1Department of Infection, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, People’s Republic of China; 2Department of Vascular Surgery, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, People’s Republic of China; 3School of Public Health, Shanxi Medical University, Taiyuan, People’s Republic of China
Correspondence: Yan Wang, Department of Infection, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, People’s Republic of China, Tel +8613513635015, Email [email protected]
Objective: To analyze the clinical characteristics and treatment process of 14 patients with aneurysm due to brucellosis, summarize the morbidity characteristics, and improve the knowledge and diagnosis of the disease.
Methods: The clinical data of patients with aneurysms who were diagnosed to have brucellosis through Rose Bengal Test (RBT), Serum Agglutination Test (SAT), blood culture, and computed tomography angiography from January 2012 to November 2022 in Bethune Hospital, Shanxi Province, China, were retrospectively analyzed, and their clinical characteristics and disease regression findings were summarized.
Results: Of the 14 patients, 13 were men, and 1 was a woman; the youngest patient was 48-year-old, and the oldest patient was of 74 years. All had a history of smoking. The sites of lesion occurrence included the abdominal aorta (5 patients), abdominal aorta +iliac artery (5 patients), iliac artery (2 patients), thoracic aorta and brachial artery were less common (1 case each). Symptoms in the patients mostly began with abdominal pain, which was accompanied by fever, nausea, and vomiting. Six patients had a clear history of livestock exposure. Fourteen patients showed elevated D-dimer and C-reactive protein levels and decreased hemoglobin and albumin levels. Thirteen of the 14 cases were treated surgically, there were no complications of surgery, and 3 patients were readmitted with recurrence of brucellosis, it is related to the treatment that did not reach the early stage, combination, full dose and full course of treatment, with a mean recurrence time of 8 months. In the telephone follow-up, the patient’s recovery proceeded well.
Conclusion: The present study revealed that the recurrence in male gender, advanced age, smoking and irregular treatment is higher. On the contrast, early intervention, a combination of adequate course of anti-infection treatment and timely surgery can improve the prognosis.
Keywords: Brucella, brucellosis-related aneurysm, clinical features, retrospective analysis, case series
Introduction
Brucellosis is a zoonotic bacterial disease of natural origin caused by Brucella species and belongs to the national statutory category B infectious disease. Humans are mainly infected through contact with infected animals such as cattle and sheep or by eating meat and dairy products contaminated with the causative bacteria. In China, brucellosis is mainly prevalent in Xinjiang Uygur Autonomous Region, Inner Mongolia Autonomous Region, Shanxi Province, and Heilongjiang Province, which are located in the north. The reported cases in Shanxi Province are mainly concentrated in Datong, Shuozhou, Jinzhong, and Xinzhou.1
Brucellosis can be multisystemic, with osteoarticular disease and genitourinary disease being the most common forms of brucellosis2 and cardiovascular disease such as endocarditis, myocarditis, pericarditis, or endarteritis being rare (3%).3 Infected aortic aneurysm (IAAA) is much rarer in brucellosis,4 and the risk of death from arterial dissection is extremely high, with 71 cases identified in the last 70 years and a global mortality rate of 22%.5 Open surgery and long-term antibiotics are usually required to complete treatment and monitor postoperative complications such as graft infection, recurrent (pseudo) aneurysms, and abscess formation.6 The early symptoms of this disease are similar to those of many other diseases and lack specificity, especially in noninfected areas where the disease is disseminated. Hence, early and accurate diagnosis is the key to treat aneurysms due to brucellosis. To raise clinicians’ awareness of this complication, a retrospective analysis was conducted using the clinical data of 14 patients with aneurysms due to brucellosis who were treated in our hospital.
Patients and Methods
Data and Methods
General Data
Fourteen patients with aneurysms due to brucellosis who were admitted to Bethune Hospital in Shanxi Province from January 2012 to November 2022 were selected for inclusion in the study. All patients signed consent form. All the recruited patients were confirmed to have brucellosis on the basis of a positive result for the Rose Bengal Test (RBT) or Serum Agglutination Test (SAT) in accordance with the WS269–2007 Diagnostic Criteria for Brucellosis.7 Among them, 14 cases were positive for RBT and SAT, 5 cases were positive for blood culture, and 5 cases were positive for all three. All patients underwent computed tomography angiography (CTA) or vascular Doppler ultrasonography, and the aneurysm was detected in the following locations: abdominal aorta (5 patients), abdominal aorta + iliac artery (5 patients), iliac artery (2 patients), thoracic aorta and brachial artery were less common (1 case each). Exclusion criteria were as follows: symptoms and signs similar to brucellosis but having aneurysms because of other causes. The following steps were taken for treatment: (1) restoring normal temperature and ensuring disappearance of clinical symptoms and signs; (2) recovery of physical strength and work capacity; and (3) negative bacterial culture on two occasions (30 days to 1 month interval) for those with positive brucellosis culture; normal function of all organs in clinical laboratory examination (brucellosis serological reaction does not necessarily show a negative reaction). The following conditions were considered for improvement: 2 of the above 3 indicators or 1 or 2 indicators are better than that before treatment. The following patients were considered to show ineffective recovery: (1) those with no significant change or no change before or after treatment and (2) those with short-term symptomatic improvement after treatment but with relapse 2 weeks after stopping the drug. The first episode was considered as the first instance of brucellosis, while recurrence was considered as recurrent or repeated brucellosis after the cure of the first episode.
Study Method
A retrospective study was conducted to collect general information, underlying diseases, clinical manifestations, laboratory tests, imaging manifestations, treatment medication, surgical methods, and disease regression of the selected cases for analysis.
Statistical Methods
SPSS 26.0 software was used for statistical analysis. Normally distributed variables were expressed as mean ± standard deviation ( ), while non-normally distributed variables were expressed as median M(P25, P75). Count data were expressed as cases (%).
), while non-normally distributed variables were expressed as median M(P25, P75). Count data were expressed as cases (%).
Results
Epidemiological Characteristics
Gender Distribution
Of the 14 patients with aneurysms due to brucellosis, 13 (92.9%) were male patients, and 1 (7.1%) was female.
Age Distribution
The age range of the 14 patients was 48–74 years, including 2 patients (14.3%) in the age group 48–50 years, 2 patients (14.3%) in the age group 51–60 years, 7 patients (50.0%) in the age group 61–70 years, and 3 patients (21.4%) in the age group >70 years. The age group of 61–70 years showed the highest incidence of aneurysms due to brucellosis.
Regional Distribution
All 14 patients were from Shanxi Province, including 4 patients (28.6%) from Lvliang, 3 patients (21.4%) from Datong, 3 patients (21.4%) from Xinzhou, 2 patients (14.3%) each from Taiyuan and Jinzhong.
Time Distribution
Aneurysms due to brucellosis occurred throughout the year, with a higher number of cases (7, 50.0%) observed from March to August.
Admissions
According to the departmental distribution, 6 patients (42.9%) were admitted to the interventional medicine department and 8 patients (57.1%) to the vascular surgery department.
Past and Personal History
All 14 patients had a history of smoking (100%), and 9 patients had a history of alcohol consumption (64.3%), 5 patients had combined hypertension (42.9%).
Epidemiological History
Seven of the 14 patients had a clear history of animal contact, including contact with sheep in 5 patients (35.7%) and dogs in 2 patients (14.3%). Drinking fresh milk was the cause of infection in 1 case (7.1%), while the route of infection was unclear in 6 patients (42.9%). The patient characteristics are provided in Table 1.
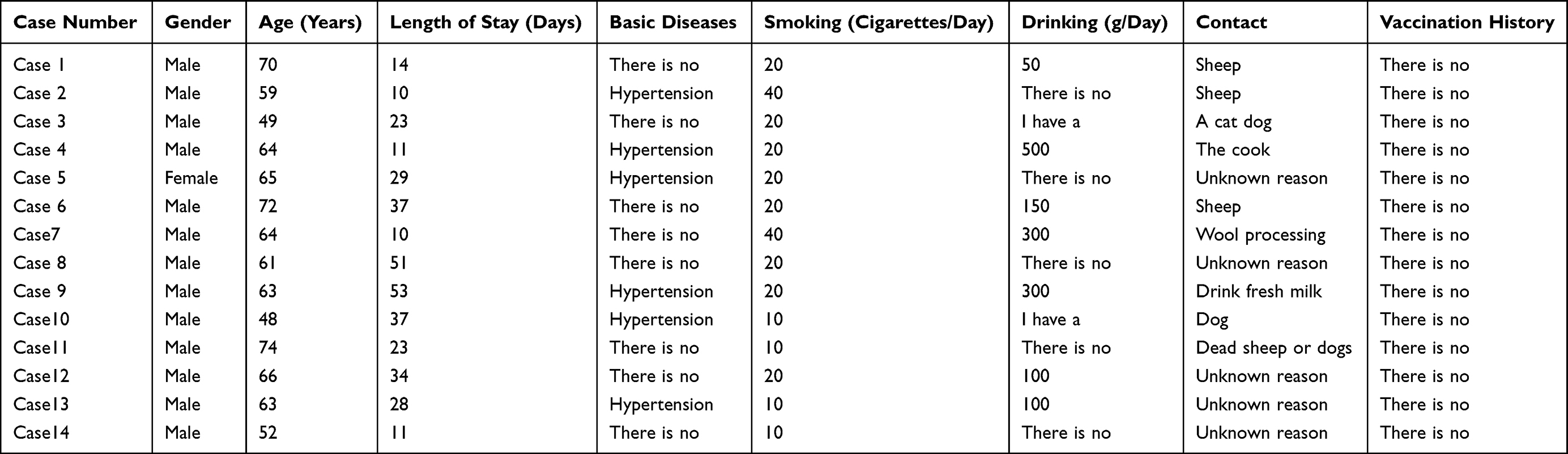 |
Table 1 Basic Information of 14 Patients with Aneurysms Due to Brucellosis |
Clinical Presentation and Laboratory Investigations
In 9 (64.3%) of the 14 patients, symptoms of the infection began with abdominal pain. Eleven (78.6%) patients had fever during the course of the disease, and the remaining comorbidities included hypoproteinemia in 14 patients (100%), coagulation abnormalities in 10 patients (71.4%), anemia in 8 patients (57.1%), renal involvement [hematuria (defined as >3 red blood cells per high magnification field), and/or at least two 3-month test paper urinalyses ≥ +1 proteinuria, and/or eGFR <60 mL/min]8 in 1 patient (7.1%), and infective endocarditis in 1 patient (7.1%). All 14 patients (100%) had elevated D-dimer with a median value of 432 ng/mL (normal value 0–243) and had elevated C-reactive protein level with a mean value of 70.59 ± 41.28 mg/L (normal value 0.00–8.00). Ten patients had elevated international normalized ratio, median 1.21 (normal value 0.8–1.1); 7 patients (50.0%) had elevated prothrombin time, median 12.5 s (normal value 9.9–12.8); 5 patients (35.7%) showed elevated neutrophil ratio, mean 70.83% ± 12.24% (normal value 40.0–75.0); 2 patients (14.3%) had elevated platelet count, mean 251.12 ± 95.57mg/L (normal value 123–350); 1 patient (7.1%) had elevated glutamate transaminase, mean 25.96 ± 8.64mg/L (normal value 15–40); 14 patients (100%) showed decreased albumin, mean 32.54 ±5.20g/L (normal value 40–55); 7 patients (50.0%) exhibited decreased lymphocyte percentage, mean 20.26 ±9.75% (normal value 20.0–50.0); 6 patients (42.9%) showed decreased hemoglobin level, median 116.5 g/L (normal value 115–150); and 5 patients (35.7%) showed decreased red blood cell count, mean value 3.81 ± 0.83 × 1012/L (normal value 3.8–5.1). White blood cell count and glutathione transaminase level were in the normal range in all patients. Details are provided in Table 2.
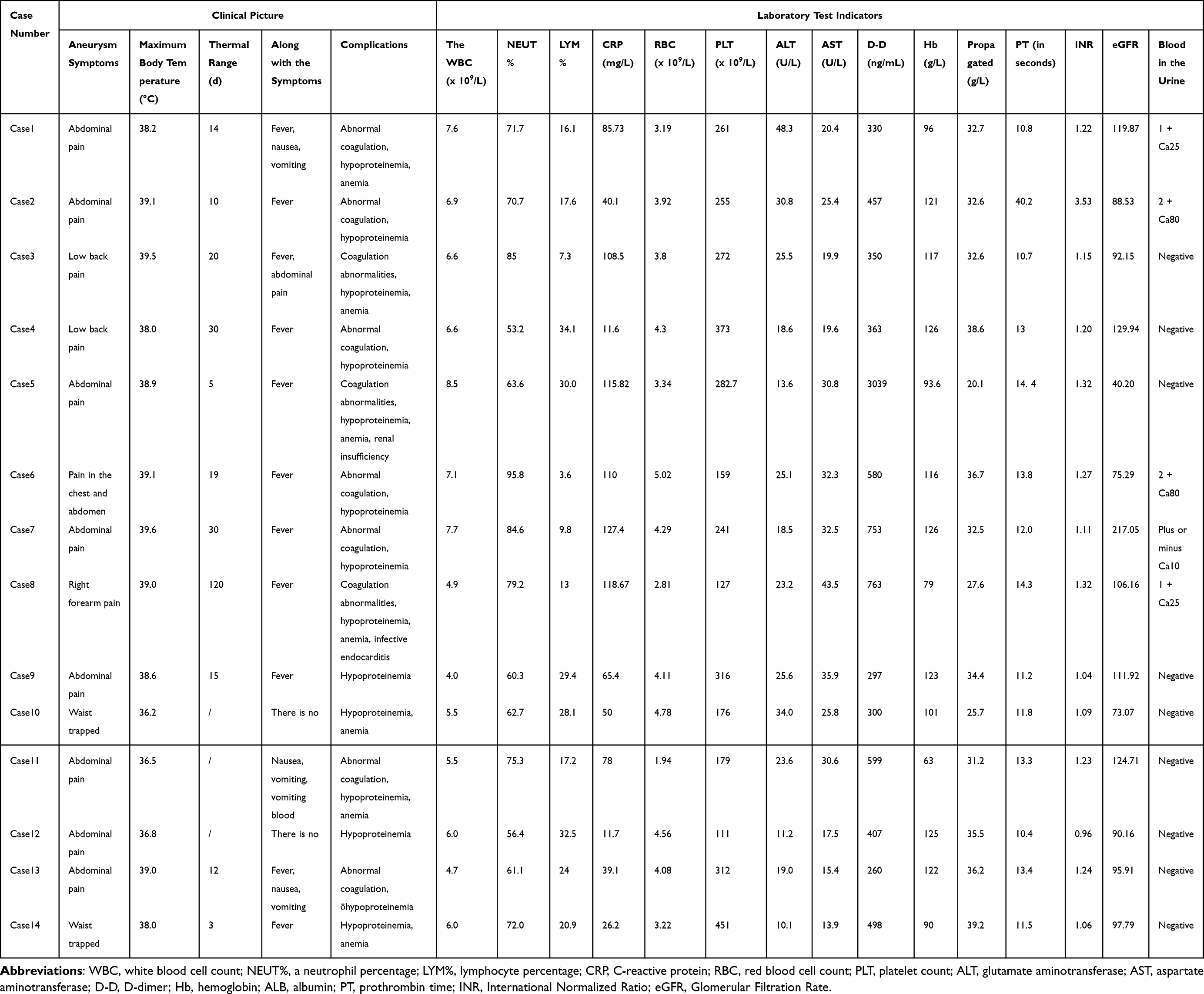 |
Table 2 Clinical Manifestations and Laboratory Test Results of 14 Patients with Aneurysms Due to Brucellosis |
Imaging Presentation
All 14 patients underwent vascular CT/CTA. All cases are presented with cystic tumor. As for the location of the lesions, the lesions were detected mainly in the abdominal aorta (5 patients), abdominal aorta + iliac artery (5 patients), iliac artery (2 patients), thoracic aorta and brachial artery were less common (1 case each). Vascular plaque and occlusion was presented in 10 cases. The details are provided in Table 3 and Figure 1 (Case 1–Case 14).
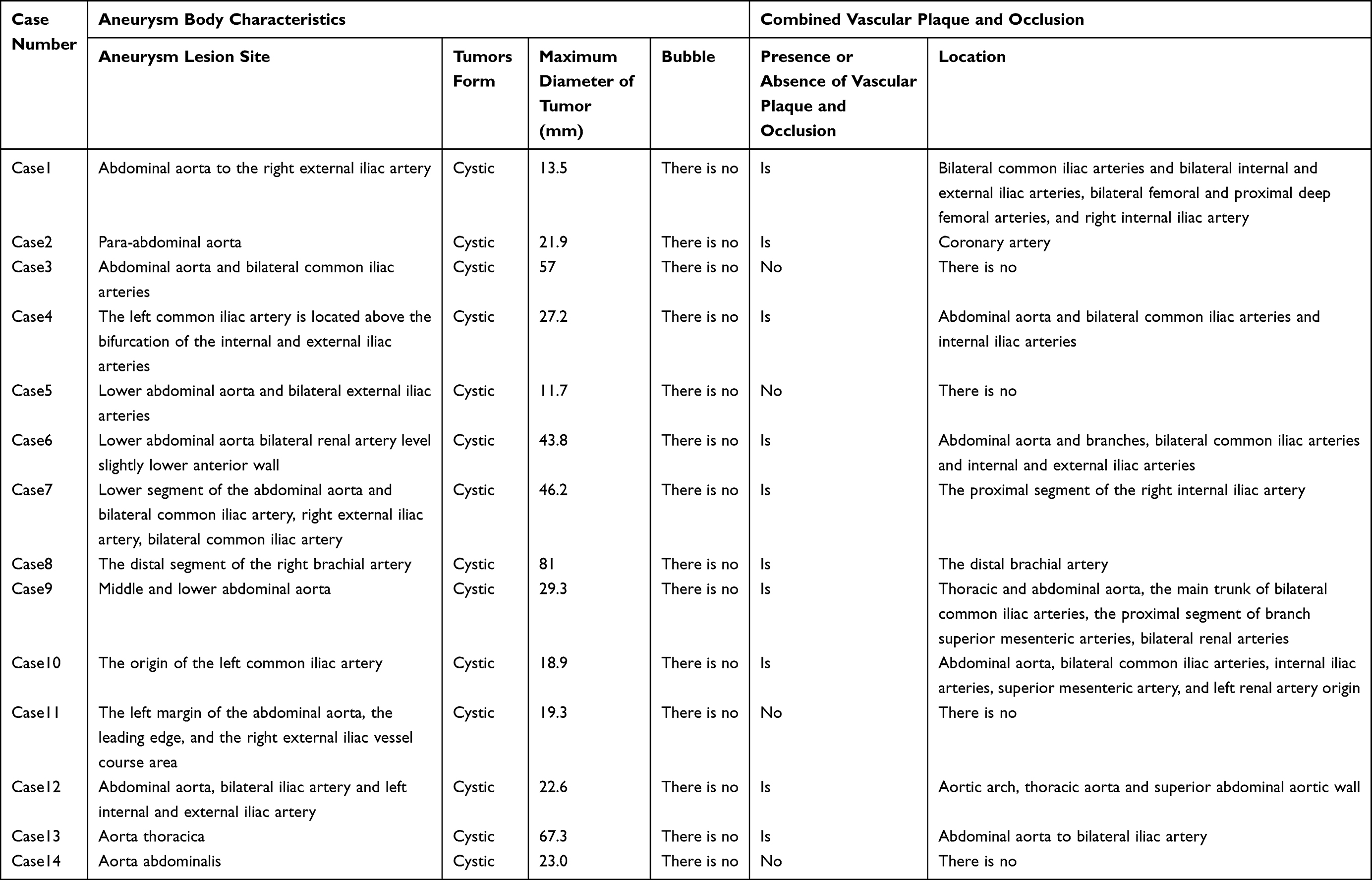 |
Table 3 CT/CTA Imaging of 14 Patients with Aneurysm Due to Brucellosis |
 |
Figure 1 CT/CTA imaging findings in 14 patients with aneurysm due to brucellosis. Case 1: Moderate luminal stenosis from the bilateral common iliac arteries to the proximal femoral arteries and occlusion of the proximal right internal iliac artery; Case 2: High-density changes in the para-abdominal aorta; Case 3: Hypointense shadow around the bifurcation of the lower abdominal aorta near the common iliac artery; Case 4: Wall notch and posterior aneurysmal contrast filling of the posterior wall of the left common iliac artery proximal to the opening of the left internal iliac artery; Case 5: Longitudinal cystic inclusion in the right retroperitoneum; Case 6: Progressive enlargement of the distal abdominal aorta; Case 7: A low-density mass shadow visible between the common iliac arteries bilaterally and occlusion of the right proximal internal iliac artery; Case 8: Contrast ectasia with irregular morphology outside the distal brachial artery of the right upper limb, with no visualization of the distal brachial artery; Case 9: Limited aneurysmal dilatation of the lower abdominal aorta and limited moderate-severe stenosis of the proximal internal iliac arteries bilaterally; Case 10: Limited aneurysmal protrusion of the lumen at the beginning of the left common iliac artery, mild stenosis of the lumen at the beginning of the superior mesenteric artery and the left renal artery; Case 11: Oval cystic lesion in the right external iliac vessel travel area; Case 12: Localized thickening of the left common iliac artery at the lower branch of the abdominal aorta, High density shadows can be seen in the lumen of the upper abdominal aorta; Case 13: An annular low-density shadow can be seen next to the lower thoracic aorta stent; Case 14: Multiple exudations and soft tissue density shadows around the bilateral iliac artery and abdominal aorta. |
Treatment and Regression
All patients were treated with more than 2 empirical antibiotics on admission, including 2 patients on quadruple dosing, 7 patients on triple dosing, and 5 patients on double dosing. Thirteen of the 14 patients were treated surgically. Stent implantation was performed in 12 patients, including cases 1, 3, 4, 5, 6, 7, 9, 10, 11, 12, 13 and 14. Balloon dilation was performed in 14 patients, case 4,6,11 and 12. Case 8 received Right brachial artery pseudoaneurysm resection plus VSD placement. Three patients were readmitted with recurrence of brucellosis, and it is related to the treatment that did not reach the early stage, combination, full dose and full course of treatment. Case 3 presented with abdominal pain and pain in lower back. Case 6 presented with pain and intermittent fever in the chest and abdomen at recurrence. The manifestation of case 7 at recurrence was abdominal pain. The mean time to recurrence in this patient group was 8 months. Of these 14 patients, 2 were more than 2 years postoperative, 1 was more than 3 years postoperative, 3 were more than 4 years postoperative, and 1 was more than 5 years postoperative, with zero short-term (within 30 days) postoperative mortality, zero intermediate (up to 4 years after randomization grouping) postoperative mortality, and zero long-term (more than 4 years) postoperative morbidity and mortality. Moreover, there were no graft-related complications, such as endoleaks and reintervention (defined as initial repair or any secondary intervention after initial repair-EVAR). In the telephone follow-up in December 2022, the patient’s recovery proceeded well. The details are provided in Tables 4 and 5.
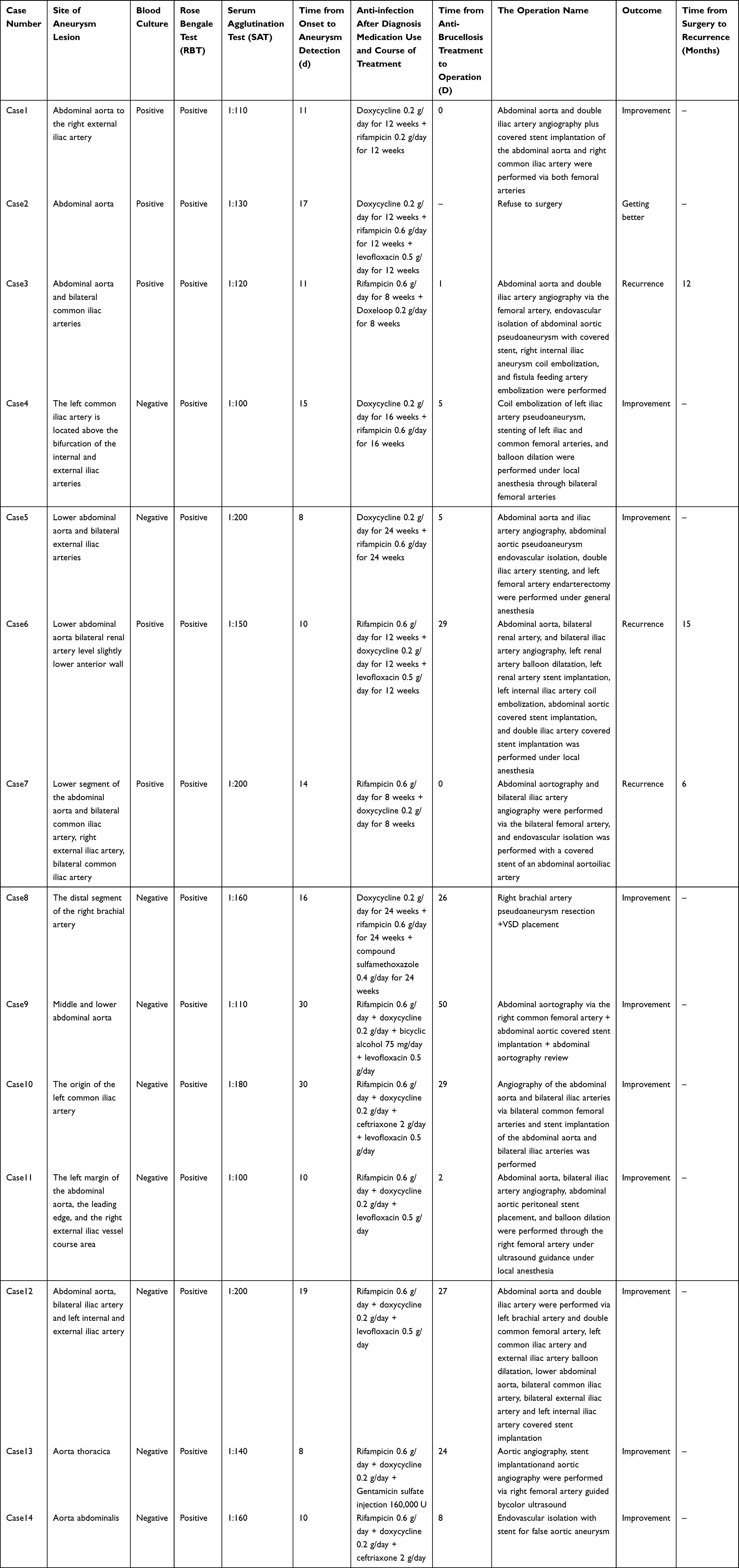 |
Table 4 Treatment and Recurrence in 14 Patients with Aneurysm Due to Brucellosis |
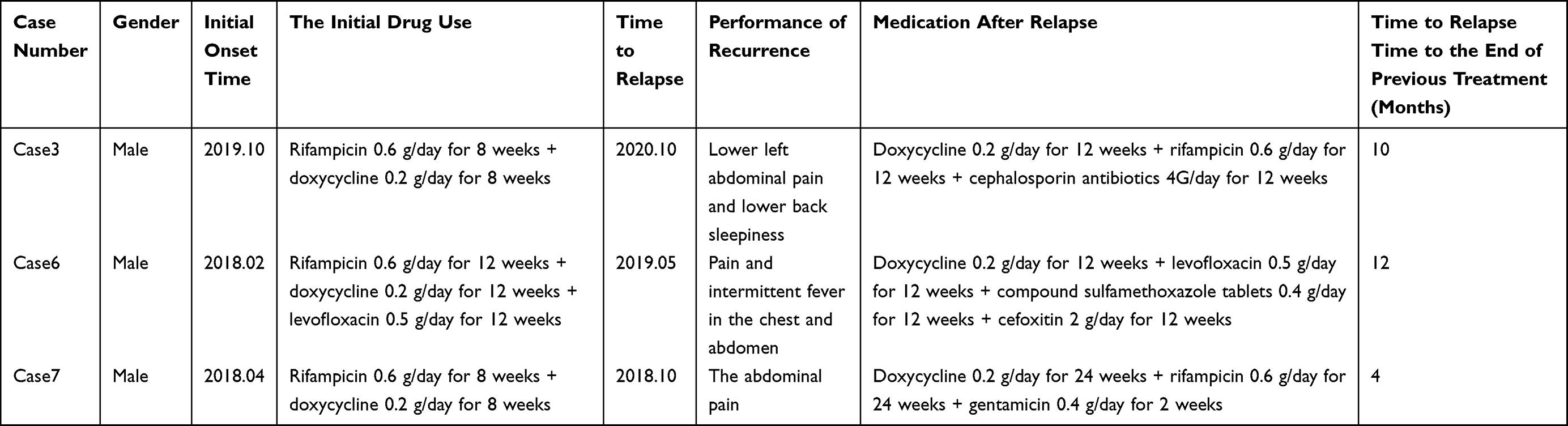 |
Table 5 Morbidity and Treatment of 3 Patients with Aneurysm Due to Recurrent Brucellosis |
Discussion
The incidence of IAAA is relatively rare in the general population, and its incidence ranges from approximately 0.85% to 1.30% of all abdominal aortic aneurysms.9 Risk factors for IAAA include immunocompromised status, smoking, hypertension, diabetes, alcohol consumption, steroid treatment or chemotherapy, and atherosclerotic plaques. Brucellosis is a zoonotic disease caused by small intracellular gram-negative bacteria of the genus Brucella. Brucella shows strong tissue tropism and replicates within the vesicles of macrophages, dendritic cells (DCs), and placental trophoblast cells. Brucella can replicate in various mammalian cell types, including microglia, fibroblasts, epithelial cells, and endothelial cells,10 resulting in multisystemic infections. Although the arterial vasculature is a rare site of Brucella invasion, aneurysms due to Brucella infection have been reported from time to time. However, there were few studies focusing on the features of aneurysm due to brucellosis and the recurrence. In this study, we recruited 14 cases of aneurysm due to brucellosis to compare the clinical characteristics as well as analyze the recurrence. The findings in the current study provide novel information for differential diagnosis and predict the prognosis of patients with aneurysm due to brucellosis.
According to the data from our hospital over the last 10 years, the incidence of aneurysms in patients with brucellosis was 2.32%, and it accounted for 2.73% of the total patients with infected aneurysms who were admitted to our hospital over the same period, thus showing an annually increasing trend. According to previous studies, male gender, age, smoking, white race, family history of abdominal aortic aneurysm, and atherosclerotic disease are the main factors with a positive association with aneurysms, while female gender and black race are the main factors with a negative association.11 In our study, we found that more than 90% patients recruited in our study were male. Moreover, our results revealed a higher incidence rate in patients with advanced age. Their findings were in agreement with previous studies. Previous observational studies have shown that smoking is associated with the rate of aneurysm enlargement and that smoking cessation reduced the rate of aneurysm growth by approximately 20% and the risk of aneurysm rupture by approximately 50%.12 In consistent with these previous studies, among the 14 patients reported in this study, 13 (92.9%) were male patients; 10 (71.4%) were elderly patients over the age of 60 years; and all patients had a long history of smoking, including 20 cigarettes per day in 8 patients, 40 cigarettes per day in 2 patients, and 10 cigarettes per day in 4 patients. Our findings also showed that the recurrent rate in smoking patients was higher than in non-smokers.
The most important pathophysiological mechanism of IAAA is necrosis and rupture of the atherosclerotic vessel wall, leading to bacterial adhesion. Therefore, atherosclerosis is the most common and important cause of IAAA.13 In almost all cases in our study patients, plaques at varying stages were detected. These plaques have an irregular surface and provide potential attachment sites for microbes.14 Previous studies have found that the presence of atheromatous plaques in the abdominal aorta, carotid artery, and femoral artery doubles the risk of aneurysm.15 It has been reported that 75% of patients with IAAA are associated with thrombosis. Moreover, open surgery also found that most IAAA are associated with thrombosis, suggesting that atherosclerosis and thrombosis are closely related to the development and progression of IAAA.16 IAAA can be caused by a variety of pathogenic bacteria. Among the bacteria, the most common causative agents are Salmonella spp., Streptococcus spp., and Staphylococcus aureus, as they have a strong affinity for the arterial wall. Salmonella is the most common pathogen infecting aortic aneurysms, with a reported incidence of up to 75%.17 Brucella is less common. As an endoparasitic bacterium, Brucella can attach to vascular branches or small trophoblastic vessels through blood circulation to invade the arterial wall, become encapsulated in peripheral soft tissues, and form a hematoma linked to the aorta, which gradually develops into an aneurysm. In our study, brucellosis-related IAAAs occurred mainly in the abdominal aorta (5 patients), abdominal aorta + iliac artery (5 patients), iliac artery (2 patients), thoracic aorta and brachial artery were less common (1 case each). The most frequent site of aneurysm is the abdominal aorta, followed by the ascending aorta, the descending aorta, and the iliac artery.18 Patients with abdominal aortic involvement show severe abdominal pain and low back pain, particularly with spinal involvement. These findings supported the previous findings that aorta is more susceptible for brucellosis-related IAAA. Cystic tumor was presented in all cases. Vascular plaque and occlusion was presented in 10 cases. Patients with thoracic aortic involvement show chest pain and hypotension.19 Because of the progression of infection in the arterial wall and surrounding tissues, aneurysms can expand rapidly and lead to rupture; furthermore, patients often have a combination of sepsis and multiple serious underlying diseases, thereby making such aneurysms difficult to cure and highly fatal. According to previous studies, special locations such as the neck of the aneurysm, the posterior inferior part of the aneurysm cavity, and the side of the iliac branch at the bifurcation of the main iliac artery at a greater angle to the long axis of the abdominal aorta are the areas of overlapping flow disturbances, high flow velocities, high wall pressure, and high wall shear stress, thus indicating that abnormal local hemodynamic parameters in these locations are an important cause of aneurysm development and progression. Attention to hemodynamic alterations in these specific locations is beneficial to prevent and treat aneurysms and optimize treatment plans.20
Treatment of aneurysms due to brucellosis involves thorough surgical debridement of the infected area, hematological reconstruction, and prolonged antibiotic therapy. Hematological reconstruction can be safely performed by in situ repair or extra-dissecting bypass, followed by aggressive long-term antibiotic therapy. As the rate of arterial rupture within 1 week is as high as 53% in patients with conservative treatment alone,21 surgical treatment is almost always the mainstay of treatment for infected aneurysms. Endovascular aneurysm repair (EVAR) is currently the primary treatment for aneurysms,22 and the IAAA diameter is the primary factor in the decision to conduct the operation. The rate of IAAA growth, symptoms, and embolism due to dislodgement of the aneurysm are also important factors in the decision to operate. Regardless of the size of the aneurysm, prompt surgery is recommended if pain due to the aneurysm is present and rupture cannot be ruled out. Elective IAAA repair should be avoided in patients with uncontrolled active infection or sepsis, active bleeding (non-aneurysm related) or coagulation disorders, acute myocardial infarction, acute cerebral infarction, acute liver or renal failure, and life expectancy <6 months (eg, advanced malignancy).23 The Society for Vascular Surgery (SVS) guidelines recommend open surgery for IAAA patients with poor vascular anatomy, and the European Society for Vascular Surgery (ESVS) guidelines recommend open surgical repair for patients with a life expectancy of 10 to 15 years.24 According to the National Institute for Health and Clinical Excellence (NICE) guidelines, open surgery is recommended as the first-line surgical treatment for patients with unruptured IAAA, with EVAR or conservative treatment being considered for patients at risk of anesthesia or in whom open repair is contraindicated. Although EVAR surgery has a lower perioperative mortality rate and shorter hospital stay, it has a higher long-term mortality rate and more complications than open surgery;25 moreover, endoleaks are common complications after EVAR.26 Both open surgery and endoluminal repair may result in endothelial damage, thereby providing an opportunity for bacteria in the circulation to invade the arterial wall;27 hence, antibiotics must be administered throughout the preoperative preparation and long-term postoperative follow-up. In China, the actual situation in each center needs to be assessed to give patients the most appropriate treatment.
When dealing with the treatment of Brucella in the cardiovascular system in the absence of specific data, we adopt the recommendation of widespread infection. The World Health Organization recommends doxycycline (100 mg twice daily) and rifampicin (600–900 mg once daily) as standard therapy for brucellosis for 6 weeks,28 and 6 weeks of doxycycline and an initial 3 weeks of streptomycin are acceptable alternatives.29,30 The regimen is also recommended by Ioannina.31 On the contrary, fluoroquinolones are less effective in the treatment of brucellosis and are not recommended.32 The Sanford guidelines for antimicrobial therapy suggest that the preferred regimen in the absence of localized lesions is doxycycline 100 mg twice daily × 6w + gentamicin 5 mg/kg once daily for 1 week.33 According to the recommendations of Harrison Infectious Diseases, the gold standard of treatment for adult brucellosis is intramuscular streptomycin (0.75–1 g daily for 14–21 days) combined with doxycycline (100 mg twice daily for 6 weeks).34 A common alternative, according to the WHO recommendation, is rifampicin (600–900 mg/d) combined with doxycycline (100 mg twice daily) for 6 weeks. The relapse/failure rate under experimental conditions is approximately 10%. In contrast, the recurrence rate of an aneurysm due to brucellosis in the present patient group was 37.5%, which was higher than the recurrence/failure rate of the common type of brucellosis. A meta-analysis showed that a triple combination of doxycycline, rifampicin, and initial therapy with aminoglycosides was superior to a two-combination regimen and should be considered for all patients with the complex disease, where treatment adherence may be problematic. According to the Expert Consensus on the Treatment of Brucellosis developed in China in 2017,35 in the presence of comorbidities, treatment is recommended to last for at least 3–6 months. A change to another triple antibiotic regimen may be considered for patients readmitted to the hospital, and the course of antibiotics may be extended appropriately to avoid drug resistance and relapse.
Regarding the criteria for relapse, it has been proposed that relapses and new-onset patients should be distinguished according to the time of disappearance of protective antibodies after the disease; patients who develop the disease within 1 year after cure of the first disease should be considered as relapse patients, and those who develop the disease again more than 1 year after cure of the first disease should be considered as new-onset patients.36 In Practical Clinical Brucellosis, it is suggested that relapse generally occurs within 10 months of completion of treatment. In the follow-up of patients with aneurysms due to brucellosis, the observation period should be extended appropriately. Harrison Infectious Diseases suggests that patients should be ideally followed up clinically for up to 2 years to detect recurrence and that peripheral blood PCR has great potential to detect bacteremia, predict recurrence, and rule out “chronic brucellosis”. In the present patient group, the longest follow-up period was 5 years, and the shortest was 6 months. One study showed a recurrence rate of 5% to 15% in patients with brucellosis. Our studies also indicated that the location of lesion was associated with recurrence: patients with lesion located in the abdominal aorta showed higher chance of recurrence. However, the presence of vascular plaque and occlusion did not correlate with recurrence based on our findings in this current study. Previous studies suggest that Brucella causes infection through nutrient acquisition, pathogen replication, or intercellular transmission of the pathogen by disrupting the host IRE1 (signaling cascade to ensure intracellular ecological niches).37 To date, there are no valid and reliable data on risk factors for the recurrence of brucellosis and on the epidemiology of recurrence. Positive blood cultures, temperature >38.3°C, disease progression in the short time before treatment, males and low platelet counts are the major risk factors for recurrence of brucellosis,38,39 Host characteristics such as advanced age, immune status, the severity of the infection, and delayed treatment are potential risk factors for recurrence, and elderly populations and cold months may be triggers for the recurrence of brucellosis in humans.40 In the present study, there were three cases of recurrence, all of which occurred during cold months. Two patients were elderly men in a high-risk environment of sheep grazing. Furthermore, there were two cases of multisite recurrence in the abdominal aorta + iliac artery. Avoidance of environmental exposure is recommended to prevent reinfection. Brucella mainly multiplies in the cells of the human reticuloendothelial system, and it is difficult for many drugs to enter the cells; consequently, Brucella cannot be easily eradicated, and the patients are prone to recurrent infections. Hence, early, combined, adequate, and full-course treatment is emphasized for patients with brucellosis. One study found that aminoglycosides (gentamicin or streptomycin versus doxycycline) were associated with a lower rate of recurrence of brucellosis.41 The present findings suggest a high recurrence rate of aneurysms due to brucellosis. It is recommended that close contact be established between surgery and internal medicine that professional guidance is given by the internal medicine department and that clinicians be made more aware of the need to perform blood cultures. Brucella is an exclusively aerobic bacterium and grows slowly; therefore, blood culture should be extended to obtain a higher positive rate. If no bacteria are detected, then the culture time should be extended, or the sample should be present for blood culture. Because of the low positive culture rate, a negative result does not exclude Brucella infection, and treatment decisions should not be influenced by a negative result but should consider all aspects of clinical, epidemiological history, and serology to give an appropriate diagnosis and treatment.
In summary, the present study provides a retrospective analysis of 14 patients with aneurysms due to brucellosis to fully understand their epidemiological features and clinical characteristics and to provide a scientific and reasonable basis for the correct diagnosis of an aneurysm due to brucellosis and for the formulation of effective prevention and control measures. The epidemic of brucellosis is still hidden and seriously endangers the healthy and sustainable development of cattle and sheep by causing large economic losses to farmers and threatening human health. Timely diagnosis and adequate treatment are the important factors that influence the effectiveness of brucellosis treatment; these factors should be supported by increasing public awareness, educating high-risk groups, increasing the vaccination rate, and improving the standard of treatment. The development and prognosis of aneurysms are significantly correlated with factors such as smoking, hypertension, and arterial plaque. We should strengthen research on factors that influence the development and prognosis of aneurysms and take comprehensive measures to curb smoking, control blood pressure, and prevent arterial plaque formation. We should also enhance the standardized treatment and follow-up management of patients to achieve dynamic assessment during the follow-up process, individualize the treatment course and timing of drug discontinuation, improve patient compliance, increase the cure rate, and reduce the chronicity and recurrence rate. Because brucellosis is a rare disease, there are still many unknown issues; for example, its pathogenesis and risk factors have not yet been fully elucidated; population epidemiological data and international diagnostic standards are lacking; the duration of preoperative antibiotic therapy, the timing of surgery, and the total course of antibiotic therapy are still controversial; and there is a lack of large-scale randomized controlled trial studies to compare the efficacy of various treatments due to insufficient sample size. Hence, further studies are warranted to overcome these limitations and gain comprehensive knowledge on treating brucellosis and its associated complications.
Conclusion
The present study revealed that the recurrence in male gender, advanced age, smoking, and irregular treatment is higher. On the contrast, early intervention, a combination of adequate course of anti-infection treatment and timely surgery can improve the prognosis. When the routine treatment for unexplained persistent fever or chest and abdominal pain is ineffective, especially for patients with epidemic history, brucellosis should be considered. Early blood culture, RBT and CTA should be performed to avoid missed diagnosis and misdiagnosis.
Ethics and Consent Statements
Informed consent to participate in this case study and to publish the findings was obtained from the patient. This case study was reviewed and approved by the Ethics Committee and Institutional Review Board of Shanxi Bethune Hospital (Approval notice number: YXLL-2022-116).
Consent for Publication
Telephone informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the telephone voice recording consent is available for review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work received no funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yongfei B, Ping T, Changfu Y, et al. Epidemiologic characteristics of human brucellosis in Shanxi Province, 2008–2017. China Trop Med. 2019;19(8):4.
2. Bosilkovski M, Krteva L, Caparoska S, Dimzova M. Osteoarticular involvement in brucellosis: study of 196 cases in the Republic of Macedonia. Croat Med J. 2004;45:727e33.
3. Li X, Wang T, Wang Y, et al. Short- and long-term follow-up outcomes of patients with Brucella endocarditis: a systematic review of 207 Brucella endocarditis cases. Bioeng. 2021;12(1):5162–5172. doi:10.1080/21655979.2021.1962683
4. Adaletli I, Albayram S, Gurses B, et al. Vasculopathic changes in the cerebral arterial system with neurobrucellosis. AJNR Am J Neuroradiol. 2006;27(2):384–386.
5. Willems SA, Brouwers JJWM, Eefting D. Aortic and iliac involvement in brucellosis - a rare but life threatening manifestation: a review of the literature. Eur J Vasc Endovasc Surg. 2022;63(5):743–750. PMID: 35282998. doi:10.1016/j.ejvs.2022.02.004
6. Willems S, Buntinx M, Gelinck L, et al. Ruptured aneurysm of the common iliac artery caused by Brucella melitensis: a case report. EJVES Vasc Forum. 2021;52:26–29. doi:10.1016/j.ejvsvf.2021.06.011
7. Gegenklonga. Diagnostic criteria for brucellosis. Dis Surveillance. 2009;24(10):781.
8. Shlipak MG, Tummalapalli SL, Boulware LE, et al.; Conference Participants. The case for early identification and intervention of chronic kidney disease: conclusions from a Kidney Disease: improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2021;99(1):34–47. PMID: 33127436. doi:10.1016/j.kint.2020.10.012
9. Goudard Y, Pierret C, de La Villéon B, et al. In situ repair of a primary Brucella-infected abdominal aortic aneurysm: long-term follow-up. Ann Vasc Surg. 2013;27(2):241.e1–241.e5. doi:10.1016/j.avsg.2012.02.028
10. Martirosyan A, Gorvel JP. Brucella evasion of adaptive immunity. Future Microbiol. 2013;8(2):147–154. PMID: 23374122. doi:10.2217/fmb.12.140
11. Lederle FA. The aneurysm detection and management study screening program. Arch Intern Med. 2000;160(10):1425. doi:10.1001/archinte.160.10.1425
12. Jahangir E, Lipworth L, Edwards TL, et al. Smoking, sex, risk factors and abdominal aortic aneurysms: a prospective study of 18 782 persons aged above 65 years in the southern community cohort study. J Epidemiol Community Health. 2015;69(5):481–488. PMID: 25563744; PMCID. doi:10.1136/jech-2014-204920
13. Golledge J. Abdominal aortic aneurysm: update on pathogenesis and medical treatments. Nat Rev Cardiol. 2019;16(4):225–242.
14. Betancourt MC, Mena R, Miguel C. Mycotic aneurysm: a rare complication of vertebral osteomyelitis. P R Health Sci J. 2007;26(3):233–236.
15. Zhou X. Analysis of 80 cases of related factors in the pathogenesis and prognosis of abdominal aortic aneurysm. Lingnan J Emerg Med. 2012;17(3):221–223. doi:10.3969/j.issn.1671-301X.2012.03.029
16. Barrett HE, Cunnane EM, Hidayat H. On the influence of wall calcification and intraluminal thrombus on prediction of abdominal aortic aneurysm rupture. J Vasc Surg. 2018;67(4):1234–1246.e2. doi:10.1016/j.jvs.2017.05.086
17. Moneta GL, Taylor LM
18. Kakkos SK, Papadoulas S, Lampropoulos G, et al. Aorto-iliac aneurysm infected by Brucella: distinctive presentation patterns of a rare entity. Vascular. 2013;21(5):307–315. doi:10.1177/1708538113478777
19. Cascio A, De Caridi G, Lentini S, et al. Involvement of the aorta in brucellosis: the forgotten, life-threatening complication. A systematic review. Vector Borne Zoonotic Dis. 2012;12(10):827–840. doi:10.1089/vbz.2012.0965
20. Li G, Li L, Yu Z, Zhang H, Yang Y. Hemodynamic analysis based on numerical simulation of abdominal aortic aneurysm. J Vasc Endovasc Surg. 2021;7(10):8.
21. Youn JK, Kim SM, Han A, et al. Surgical treatment of infected aortoiliac aneurysm. Vasc Specialist Int. 2015;31(2):41–46.
22. Lili G, Jina M, Xiaoli B. Two cases of Brucella infectious abdominal aortic aneurysm. Chin J Infect Chemother. 2016;16(3):379–382. doi:10.16718/j.1009-7708.2016.03.024
23. Wei G, Zhong C, Tao Z; Vascular Surgery Group, Surgery Branch of Chinese Medical Association. Expert consensus on the diagnosis and treatment of abdominal aortic aneurysm in China (2022 edition). Chin J Pract Surg. 2022;42(4):8. doi:10.19538/j.cjps.issn1005-2208.2022.04.03
24. Beck AW, Sedrakyan A, Mao J, et al.; International Consortium of Vascular Registries. Variations in abdominal aortic aneurysm care: a report from the international consortium of vascular registries. Circulation. 2016;134(24):1948–1958. PMID: 27784712; PMCID: PMC5147037. doi:10.1161/CIRCULATIONAHA.116.024870
25. Paravastu SC, Jayarajasingam R, Cottam R, Palfreyman SJ, Michaels JA, Thomas SM. Endovascular repair of abdominal aortic aneurysm. Cochrane Database Syst Rev. 2014;1:CD004178. doi:10.1002/14651858.CD004178.pub2
26. Li ZY, Wang LX, Fu WG. The latest guidelines for the endovenous treatment of abdominal aortic aneurysms. Chin J Basic Clin Gener Surg. 2021;28(11):1414–1417.
27. Kaviani A, Ouriel K, Kashyap VS. Infected carotid pseudoaneurysm and carotid-cutaneous fistula as a late complication of carotid artery stenting. J Vasc Surg. 2006;43(2):379–382. PMID: 16476618. doi:10.1016/j.jvs.2005.10.058
28. Listed N. Joint FAO/WHO expert committee on brucellosis. World Health Organ Tech Rep Ser. 1986;740:1–132.
29. Herrick JA, Lederman RJ, Sullivan B, et al. Brucella arteritis: clinical manifestations, treatment, and prognosis. Lancet Infect Dis. 2014;14(6):520–526. doi:10.1016/S1473-3099(13)70270-6
30. Corbel MJ, Elberg SS, Cosivi O, editors. Brucellosis in Humans and Animals. Geneva: World Health Organization; 2006.
31. Ariza J, Bosilkovski M, Cascio A, et al. Perspectives for the treatment of brucellosis in the 21st century: the Ioannina recommendations. PLoS Med. 2007;4:e317. doi:10.1371/journal.pmed.0040317
32. Solís García Del Pozo J, Solera J, Biondi-Zoccai G. Systematic review and meta-analysis of randomized clinical trials in the treatment of human brucellosis. PLoS One. 2012;7(2):e32090. doi:10.1371/journal.pone.0032090
33. Gilbert D. Fever Sanford Guidelines for Antimicrobial Therapy New Translation 50 Edition. Beijing: Peking Union Medical College Press; 2021:11.
34. Kasper DL, Bijie H, Jue P, Xiaodong G. Harrison Infectious Disease. Shanghai: Shanghai Science and Technology Press; 2019:05.
35. Editorial Board of Chinese Journal of Infectious Diseases. Expert consensus on the diagnosis and treatment of brucellosis. Chin J Infect Dis. 2017;35(12):6. doi:10.3760/cma.j.issn.1000-6680.2017.12.001
36. Guo ZY, Lv JR, Hao ZY, et al. Epidemiological and clinical investigation of 71 cases of recurrent brucellosis. Dis Prev Control Bull. 2013;2:4.
37. Figueiredo PD, Ficht TA, Rice-Ficht A, et al. Pathogenesis and immunobiology of Brucellosis review of Brucella-host interactions. Am J Pathol. 2015;185(6):1505–1517. doi:10.1016/j.ajpath.2015.03.003
38. Solera J, Martínez-Alfaro E, Espinosa A, Castillejos ML, Geijo P, Rodríguez-Zapata M. Multivariate model for predicting relapse in human brucellosis. J Infect. 1998;36(1):85–92. doi:10.1016/S0163-4453(98)93342-4
39. Ariza J, Corredoira J, Pallares R, et al. Characteristics of and risk factors for relapse of brucellosis in humans. Clin Infect Dis. 1995;20(5):1241–1249. doi:10.1093/clinids/20.5.1241
40. Nematollahi S, Ayubi E, Karami M, et al. Epidemiological characteristics of human brucellosis in Hamadan Province during 2009–2015: results from the national notifiable diseases sur-veillanceSystem. Int J Infect Dis. 2017;61:56–61. doi:10.1016/j.ijid.2017.06.002
41. Roushan M, Moulana Z, Afshar ZM, et al. Risk factors for relapse of human brucellosis. Glob J Health Sci. 2016;8(7):77.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nanotechnology: A Promising Approach for Cancer Diagnosis, Therapeutics and Theragnosis
Dessale M, Mengistu G, Mengist HM
International Journal of Nanomedicine 2022, 17:3735-3749
Published Date: 26 August 2022
Updated Perspectives on the Diagnosis and Management of Onychomycosis
Falotico JM, Lipner SR
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1933-1957
Published Date: 15 September 2022
Nontuberculous Mycobacteria Lung Disease (NTM-LD): Current Recommendations on Diagnosis, Treatment, and Patient Management
Pathak K, Hart S, Lande L
International Journal of General Medicine 2022, 15:7619-7629
Published Date: 1 October 2022
Challenges in the Early Diagnosis and Treatment of Chronic Inflammatory Demyelinating Polyradiculoneuropathy in Adults: Current Perspectives
van Doorn IN, Eftimov F, Wieske L, van Schaik IN, Verhamme C
Therapeutics and Clinical Risk Management 2024, 20:111-126
Published Date: 14 February 2024
Managing Opioid Withdrawal Symptoms During the Fentanyl Crisis: A Review
Weber AN, Trebach J, Brenner MA, Thomas MM, Bormann NL
Substance Abuse and Rehabilitation 2024, 15:59-71
Published Date: 10 April 2024