Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Validation and Application of the Simplified Chinese Version of the Dyspnea-12 Questionnaire: An Independent Predictor for Hospitalization Risk in Chronic Obstructive Pulmonary Disease
Authors Chen X, Du L ![]() , Xiao W, Liu M, Miao T, Xiong C, Liao L, Li Y, Hu Y, Fu J
, Xiao W, Liu M, Miao T, Xiong C, Liao L, Li Y, Hu Y, Fu J ![]()
Received 17 June 2025
Accepted for publication 11 October 2025
Published 31 October 2025 Volume 2025:20 Pages 3559—3574
DOI https://doi.org/10.2147/COPD.S547507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Xugui Chen,1,2 Longyi Du,1 Wei Xiao,1 Meilu Liu,1 Tiwei Miao,1 Chan Xiong,2 Li Liao,2 Yu Li,2 Yonggang Hu,3 Juanjuan Fu1
1Division of Pulmonary Medicine, Department of Internal Medicine, Institute of Integrated Traditional Chinese and Western Medicine, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2Department of Respiratory Medicine, No. 3 Affiliated Hospital of Chengdu University of Traditional Chinese Medicine (West District)/Chengdu Pidu District Hospital of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 3Chengdu Xinjin District Hospital of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China
Correspondence: Juanjuan Fu, Email [email protected]
Introduction: The Dyspnea-12 is a brief patient reported tool assessing physical and emotional components of breathlessness. However, the reliability and effectiveness of the Chinese version of Dyspnea-12 (D-12-C) needs to be verified.
Purpose: This study aimed to assess the reliability and validity of D-12-C in patients with chronic obstructive pulmonary disease (COPD) and investigate its associations with clinical outcomes of COPD.
Patients and Methods: Patients from three centers completed baseline assessments (pulmonary function test, the COPD Assessment Test (CAT), the Modified Medical Research Council Dyspnea Scale (mMRC), the Hospital Anxiety and Depression Scale (HADS), St George’s Respiratory Questionnaire (SGRQ), Borg dyspnea scale, 6-minute walking distance (6MWD) and the history of exacerbations. The internal consistency, construct validity, convergent validity and reliability of the D-12-C were evaluated. The binary multivariate logistic regression analysis was performed to explore the influencing factors for hospitalization during follow-up.
Results: A total of 279 patients were recruited. Exploratory factor analysis divided the D-12-C into physical and affective dimensions. A high level of internal consistency was manifested by the Cronbach’s alpha values of the D-12-C with total scores, physical, and affective dimensions of 0.94, 0.96, and 0.92, respectively. The score of D-12-C increased as the GOLD or mMRC grade rose, and patients suffering from anxiety or depression had more severe dyspnea. The score of D-12-C was significantly correlated with CAT, mMRC, HADS, SGRQ and hospitalization during follow-up. Additionally, baseline D-12-C was an independent predictor of hospitalization during the one year follow-up (OR=1.086, 95% CI: 1.035– 1.139, p < 0.001).
Conclusion: The D-12-C demonstrated good internal consistency and validity in COPD. The score of D-12-C correlates with the clinical parameters of disease severity and predicts severe exacerbations of hospitalization, supporting its use in risk stratification and management planning to prevent adverse outcomes.
Keywords: dyspnea-12 questionnaire, dyspnea, chronic obstructive pulmonary disease, exacerbation
Introduction
Dyspnea is defined as a subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity by the American Thoracic Society (ATS).1 Dyspnea is a hallmark symptom of chronic obstructive pulmonary disease (COPD) which not only limit the daily activities and affect emotions of patients with COPD but is also associated with increased risk of acute exacerbation of COPD (AECOPD) and mortality.2–6 Importantly, psychologic, social, and environmental factors contribute to the severity of dyspnea beyond physiologic abnormality.1,7–9 Clinical instruments assessing breathlessness need to address these multiple dimensions.
Spirometry represented by FEV₁ measures airflow limitation, but it is a poor surrogate for the symptom burden and overall disease impact experienced by the patient.10 Several patient-reported questionnaires have been designed and used in COPD clinically and in research assessing the severity of dyspnea. The modified Medical Research Council (mMRC) dyspnea scale, though valuable for assessing functional limitation, represents a unidimensional assessment that evaluate only the physical intensity of dyspnea and may lack sensitivity to the full symptomatic experience.2,11 The Visual Analogue Scale (VAS) and the Borg Dyspnea Scale are used to measure the severity of patients’ perception of dyspnea. Nonetheless, these methods cannot capture the complex nature of dyspnea.12,13 The COPD Assessment Test (CAT) is often used to assess the physical health status of patients with COPD, including coughing, expectoration, chest tightness, etc., beyond a single assessment of breathlessness.14 In addition, the Hospital Anxiety and Depression Scale (HADS), a questionnaire designed to detect potential psychological comorbidities of diseases, has been used to evaluate the affective dimension of diseases in previous studies. However, it cannot specifically evaluate anxiety or depression in relation to dyspnea.15–17 Finally, The St George’s Respiratory Questionnaire (SGRQ) is not explicitly applied to assess dyspnea but includes other symptoms and their repercussions.18
The Dyspnea-12 questionnaire (D-12) is a simple, convenient, and effective tool that patients can complete quickly on their own that is more comprehensive in assessing breathlessness. The process of developing the D-12 involves gathering dyspnea descriptors from a variety of patients with different cardiorespiratory diseases and reducing them from 81 to 34 items using hierarchical methods and principal component analysis.19 D-12 directly provides descriptions of the severity of dyspnea and emotions related to dyspnea through words or sentences. It has been confirmed that D-12 can be used to evaluate both physical and affective dimensions of dyspnea in various diseases.20–22 The D-12 has been translated into several languages, and the internal consistency and validity of each version have been confirmed.23–34 A prior study by Choi et al from Hong Kong has developed the traditional Chinese version of D-12, which was translated into Cantonese,35 However, our work has addressed several critical gaps that distinguish it from the prior research. First, although the Cantonese version has been validated, its applicability is limited to specific regions and it can hardly be integrated into healthcare systems.36 In contrast, Mandarin is the official language used in mainland China’s healthcare and public health systems, our study provides a validated instrument for the vastly larger population using Simplified Chinese. This fulfills a significant national need for linguistically and culturally appropriate tools. Furthermore, our multicenter design enhances the generalizability of the findings across diverse clinical settings within China. Most importantly, our study conduct assessment for predictive validity of D-12-C with exacerbation frequency by multivariate regression analysis controlling for confounding factors, aiming to uncover its accurate and powerful relationship with clinical outcomes, which has not been explored in previous studies. Various patient-reported tools have been demonstrated to be associated with exacerbation and mortality.37,38 A large retrospective cohort study (n=67,362 hospitalized patients) which demonstrated that even mild dyspnea (scores 1–3 on a 0–10 scale) was associated with significantly increased hospital mortality (adjusted OR=2.1, 95% CI: 1.7–2.6), with higher dyspnea scores showing even greater risk (scores ≥4: adjusted OR=3.1, 95% CI: 2.4–3.9).39 And a recent multinational study across 25 countries (n=19,714 adults) which found that dyspnea was significantly associated with both physical (coefficient = −7.59; 95% CI −8.60, −6.58; I2 = 78.5%) and mental (coefficient = −3.50; 95% CI −4.36, −2.63; I2 = 71.4%) health-related quality of life impairments, with particularly pronounced effects on physical health dimensions.40 Whether D-12 is related to clinical outcomes of COPD especially the future risk of exacerbation is unknown.
In view of the results of earlier research, as well as the necessity and potential advantages of utilizing multidimensional dyspnea assessment tools, this study attempted to bridge the gap in the simplified Chinese version (D-12-C) and verify its reliability and effectiveness.
Materials and Methods
Participants
This is a multicenter prospective study of patients with stable COPD who were consecutively recruited from outpatient service of three centers in China: West China Hospital of Sichuan University, No. 3 Affiliated Hospital of Chengdu University of Traditional Chinese Medicine (West District)/Pidu District Traditional Chinese Medicine Hospital of Chengdu, and Xinjin District Traditional Chinese Medicine Hospital of Chengdu. All eligible patients meeting inclusion and exclusion criteria were included. This study was approved by the Clinical Trial and Biomedical Ethics Committee of West China Hospital of Sichuan University (approval number: 2021(1394)), Medical Ethics Committee of Pidu District Hospital of Traditional Chinese Medicine (approval number: 2020027), and Medical Ethics Committee of Xinjin District Traditional Chinese Medicine Hospital of Chengdu (approval number: 2021–08-20-01) and was registered (https://www.chictr.org.cn/, identifier: ChiCTR2300071725). All participants were informed of the purpose and process and signed informed consent forms.
Patients must meet the following criteria to be included in the study: (1) diagnosed with COPD according to the Global Initiative for Obstructive Lung Disease (GOLD) guidelines,2 and did not use antibiotics/corticosteroids or hospitalization due to worsening respiratory symptoms in the past four weeks (2) ages between 40 and 85 years without limitation of gender; (3) willing to cooperate with lung function test and able to fill out questionnaires independently.
The exclusion criteria were as follows: (1) suffering from another chronic respiratory disease; (2) with severe comorbidities such as cardiovascular diseases, malignant tumors, or other organic diseases often accompanied by dyspnea; (3) suffering from neurological disorders or inability to understand Mandarin that might affect communication.
Measurements
Dyspnea-12 Questionnaire
The Dyspnea-12, consisting of 12 items, is a tool designed for evaluating the severity of dyspnea from two components (physical component: seven items; affective component: five items).19 Each item has four options for options: none (0); mild (1); moderate (2); severe (3). The total score, physical score and affective score in the dyspnea-12 questionnaire ranges from 0 to 36, 0 to 21, and 0 to 15, respectively.21,22,41 The reconciliation process translated the initial English version of dyspnea-12 into Chinese (spoken in Mandarin, written in simplified Chinese) according to the “forward-backward” translation standard which including two independent forward and backward translations.42,43 Forward translation was independently conducted by two bilingual researchers with medical translation expertise. Synthesis of translations was achieved through meetings of research group to resolve minor discrepancies. Back translation was performed by a professor with an Australian educational background blinded to the original version of dyspnea-12. Then, a multidisciplinary expert committee composed of translation experts, respiratory clinicians, and linguists conducted a comprehensive review of the translation results. Differences between translations were discussed and resolved within the research group where the researchers were located. Following the completion of the questionnaire, a trained researcher conducted one-on-one, semi-structured interviews with 15 patients. All patients confirmed that the questionnaire was quick to complete (approximately 3–5 minutes). There were six patients had difficulty in understanding “catching up breath” (item 4), we therefore added detailed explanation after this question. Nine patients struggled to differentiate “make me feel miserable” (item 9) and “distressing” (item 10), and the descriptions in Chinese were refined correspondingly. After revision, patients were required to complete two assessments of D-12-C with an interval of eight weeks. After each assessment, they were interviewed to confirmed comprehensibility of the final version, and the intra group correlation coefficient (ICC) before and after 8 weeks will be calculated to evaluate test-retest reliability.
The COPD Assessment Test (CAT)
In addition to the assessing dyspnea, the CAT also contains seven other questions related to COPD symptoms, including cough, sputum, exercise ability, etc. and patients need to score each symptom based on its severity in the range of 0 to 5 points, with higher scores indicating more severe symptoms.14,44
The Modified Medical Research Council Dyspnea Scale (mMRC)
The mMRC is a five-point (0–4) questionnaire developed to measure breathlessness, with scores closely related to other multidimensional health status indicators and patients need to conduct self-assessments based on their actual situation.11,45
The Hospital Anxiety and Depression Scale (HADS)
The HADS, a questionnaire consisting of 14 items, was designed to evaluate anxiety and depression. Not only emotional disorder, it is also used in clinical or research to measure the emotional state of patients with COPD.46,47
The St George’s Respiratory Questionnaire (SGRQ)
The SGRQ is a comprehensive measurement that includes 50 items to measure three dimensions (symptoms, activity, and impacts), and the scores for each dimension are calculated by weighting.18,48 Patients need to complete the questionnaire based on their situation in the past month, and higher scores mean poorer health status and quality of life.
All patient-reported outcome measures used in this study were the officially validated and widely used Chinese versions. This was done to ensure linguistic and cultural appropriateness for our participant population.
The Six-Minute Walking Test (6MWT)
The 6MWT is commonly developed to assess exercise tolerance. According to the guideline published by the ATS,49 subjects will be asked to walk back and forth for 6 minutes on a 30-meter-long corridor. Heart rate, oxygen saturation, and blood pressure will be recorded to monitor vital signs, and breathlessness will be measured by the Borg score at the end of the test.
Pulmonary Function Tests (PFTs)
PFT will be conducted strictly by trained professionals who have received standard training according to the guideline published by the ATS in 2019.50 Patients are required to perform the test in a sitting position as much as possible and use nasal clips or manually occlude the nostrils. For better completion, operators can guide the patients through detailed explanations, vivid presentation and continuous encouragement. A complete test requires at least three repeatable operations and the post-bronchodilator forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) will be recorded.
Follow-Up of Exacerbation
History of exacerbations was recorded for the one year preceding enrollment. Telephone follow-ups were conducted every three months after enrollment. Data on exacerbations, medication use, unplanned outpatient visits, emergency department visits, and hospitalizations for exacerbations were recorded. An exacerbation of COPD is defined as the worsening of respiratory symptoms that results in additional therapy, such as short acting bronchodilators, antibiotic, oral corticosteroids, or hospitalization according to GOLD 2021.2 The severity of exacerbation is classified as mild, moderate and severe according to the following GOLD guidelines: (1) mild: only short-acting bronchodilators (SABDs) are needed to alleviate the worsening symptoms; (2) moderate: except SABDs, oral corticosteroids or antibiotics are required; (3) severe: hospitalization or visiting emergency because of exacerbations.2 Patients who have two or more exacerbations per year are considered as frequent exacerbator phenotype.51,52 High exacerbation risk is defined as a patient who experienced at least two exacerbations or one hospitalization within one year.52
Statistical Analysis
The descriptive analysis was applied to demographic characteristics and each measurement tool. The use of mean [standard deviation (SD)], median [interquartile range (IQR) (25–75%)], and numbers (percentage) depended on the type of data and whether the data distribution satisfied normality.
The missing values for all items were calculated, as was the proportion of the highest score (36) and lowest score (0) for D-12-C to evaluate the ceiling and floor effects.
The internal consistency of D-12-C was estimated by Cronbach’s alpha coefficients for all items as well as items 1 to 7 (physical component) and items 8 to 12 (affective component). Generally, Cronbach’s alpha coefficient greater than 0.7 is considered good internal consistency on the scale, while the higher the score, the stronger the internal consistency. Fifteen subjects were asked to complete the D-12-C questionnaires again after 8 weeks and the ICC was calculated to evaluate the test-retest reliability.
The exploratory factor analysis was used to assess construct validity. Using Kaiser–Meyer–Olkin (KMO) and Bartlett’s Test of Sphericity to determine whether factor analysis can be performed. Choose to extract common factors using the principal component method and then rotate using the maximum variance to test the structural effectiveness of D-12-C. The construct validity was estimated by examining the associations between items within the same scale. The confirmatory factor analysis was used to confirm assess construct validity. Acceptable or good model fit was assessed by the χ2 / Df (acceptable fit if < 3), root mean square error of approximation (RMSEA, acceptable fit if < 0.08), comparative fit index (CFI, acceptable fit if > 0.90), tucker-lewis index (TLI, acceptable fit if > 0.90), standardized root mean square residual (SRMR, acceptable fit if < 0.08).
To examine convergent validity, we calculated Spearman correlations between D-12-C and FEV1%pred, FEV1/FVC, CAT, mMRC, HADS, SGRQ, Borg score, 6MWD and the history of exacerbations.
To test for differences in D-12-C levels between two or more groups, independent sample t-tests, Mann Whitney U-tests, or Kruskal–Wallis test were applied based on the normality test results, and the Bonferroni was used for pairwise comparisons. The influencing factors of hospitalization during the follow-up period will be explored through the binary multivariate logistic regression analysis, and univariate analysis will screen out noteworthy factors as the independent variables to be included in the regression analysis.
All the statistical analyses were undertaken using the SPSS Statistics 27.0 (IBM Corporation, Armonk, NY) and GraphPad Prism 9 software. All statistical tests were two-tailed, and statistical significance required P-values<0.05.
Results
A total of 279 patients with an average age of 65.78±7.88 were recruited in this study and 227 (81.4%) were males. There were 56 (20.1%) non-smokers, 184 (65.9%) ex-smokers and 39 (14.0%) current-smokers, and 158 (56.6%) patients with mMRC≥2.
The median D-12-C total score was 8 (3–14), the scores for the physical and affective components of D-12-C were 6 (2–10) and 2 (1–6), respectively. Two patients (0.72%) had the highest total score of 36, while 44 patients (15.77%) had the lowest score of 0 in D-12-C. The results of demographic characteristics and clinical measurements are shown in Table 1.
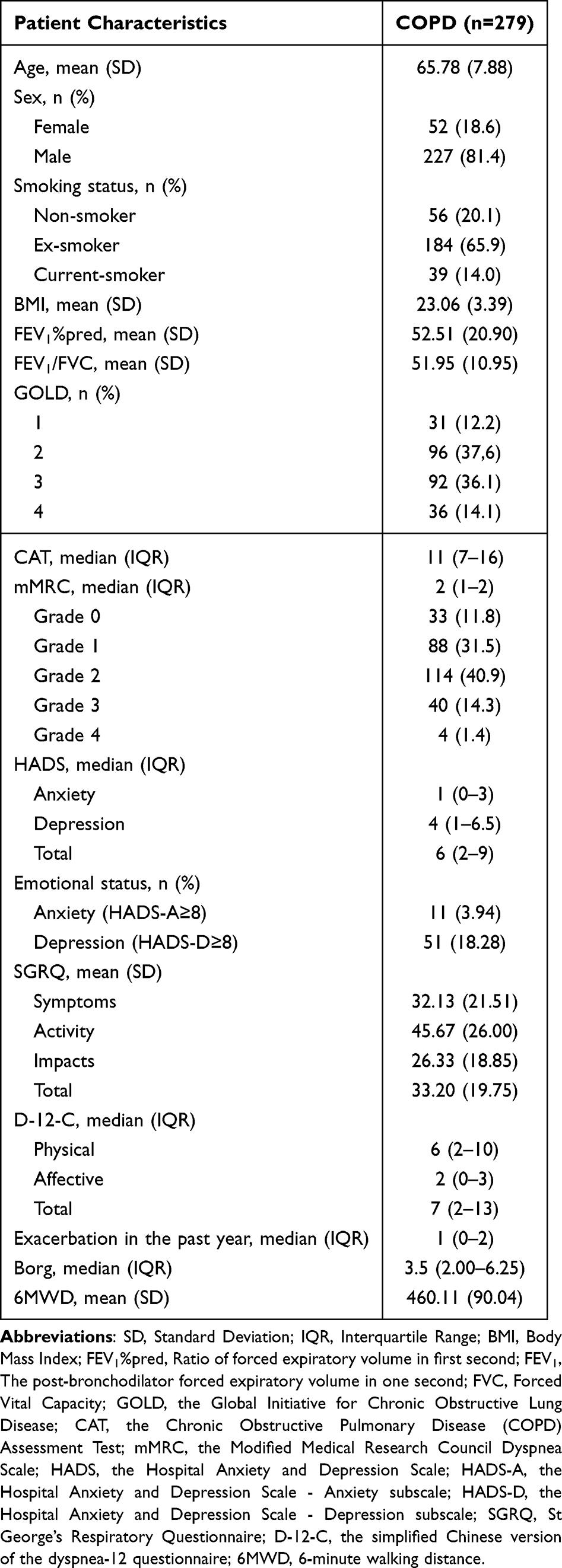 |
Table 1 Demographic Characteristics and Clinical Measurements |
Reliability
As shown in Table 2, Cronbach’s Alpha (0.94, 0.96, 0.92) for the total, physical, and affective components of D-12-C have shown a high level of internal consistency. The high level of test–retest reliability was also found in D-12-C (ICC = 0.843, P<0.001), showing its good time stability and consistency.
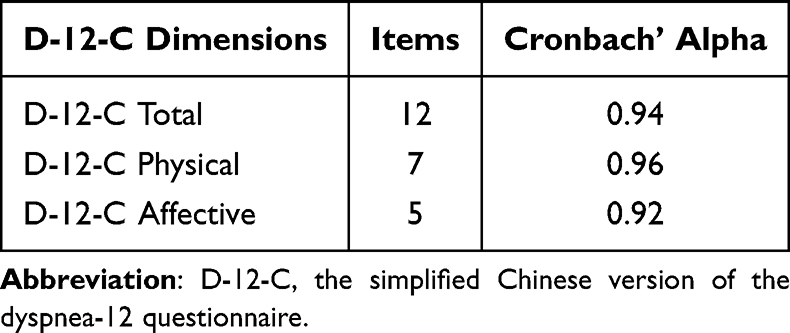 |
Table 2 Internal Consistency of D-12-C |
Construct Validity
The exploratory factor analysis was conducted on the data. The Kaiser–Meyer–Olkin value of 0.929 and the result of Bartlett’s sphericity test (χ2=3285.747; P<0.001) indicated the feasibility of factor analysis.53 And then, the principal component analysis and varimax rotation were used to extract common factors. Factor loadings exceeding 0.5 were classified as a common factor. Thus, the 12 items within D-12-C can be divided into the physical and affective factors (Table 3). Items 1 to 7 had the higher factor loadings on factor 1 (factor loadings>0.5) representing physical components, which mainly evaluate physical perception of dyspnea, and items 8 to 12 had high factor loadings in factor 2 (factor loadings>0.5) representing affective components which reflect the emotional dimension of dyspnea.
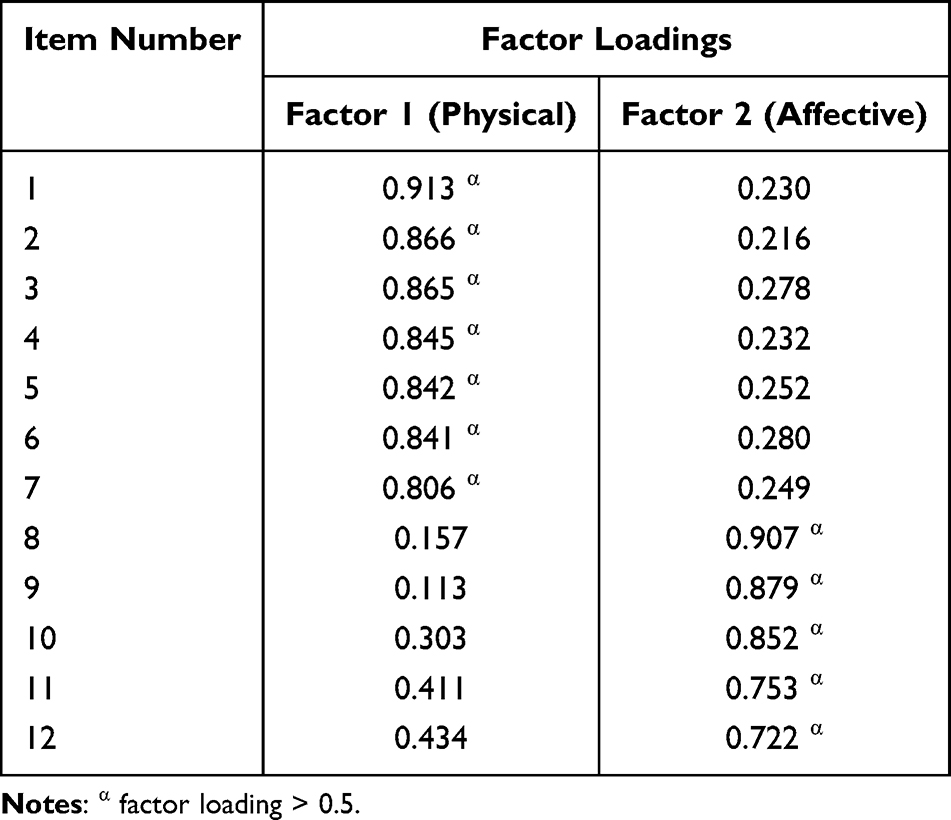 |
Table 3 Exploratory Factor Analysis for D-12-C Items |
The model of the confirmatory factor analysis is shown in Figure 1. After adding a connection between item 11 (“My breathing makes me agitated”) and item 12 (“My breathing is irritating”), the D-12-C model had good model fit (χ2/DF=2.992 < 3, RMSEA = 0.075 < 0.08, CFI = 0.968 > 0.90, TLI = 0.921 > 0.90, SRMR = 0.0432 < 0.05).
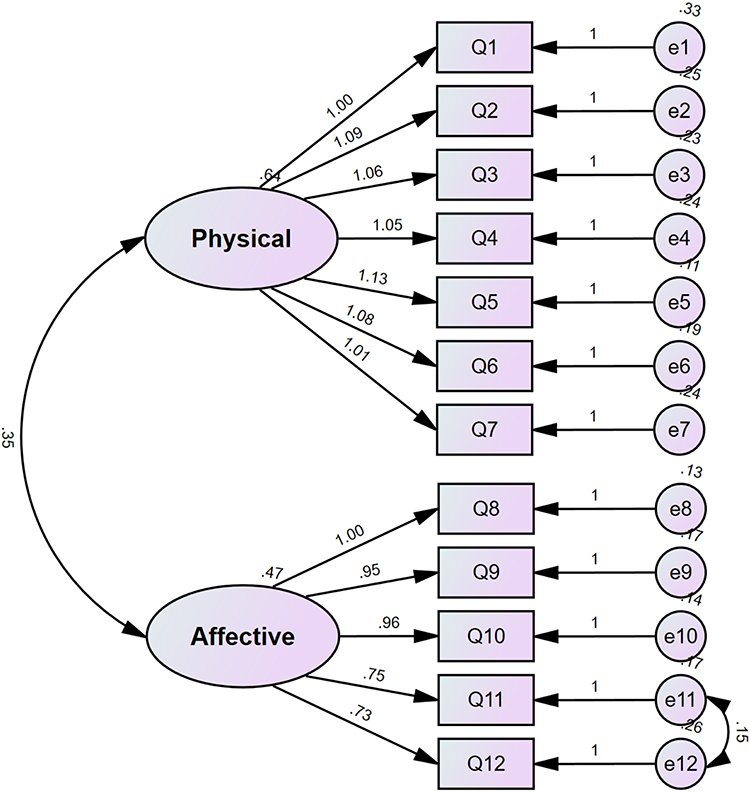 |
Figure 1 Confirmatory Factor Analysis for D-12-C Items. |
Convergent Validity
The D-12-C scores were significantly correlated with CAT, mMRC, HADS, SGRQ and hospitalization during follow-up. The D-12-C physical and total scores were correlated with FEV1%pred and FEV1/FVC. The Borg dyspnea score was related to the D-12-C affective and total scores (rs=0.310, P=0.007, rs=0.233, P=0.046). Weak correlations were found between the total score of D-12-C and exacerbations in the past year (rs=0.159, P=0.008) (Table 4). The highest correlation was found between the total D-12-C score and the SGRQ total score (rs=0.768, P<0.001) (Table 4).
 |
Table 4 Correlation Between D-12-C and Clinical Measurements |
Discriminant Performance
Patients with anxiety or depression (HADS anxiety score or HADS depression score ≥ 854) exhibited more severe breathlessness ((non-anxiety vs anxiety: D-12-C-Physical: 5(2–10) vs 17(9–21), P<0.001; D-12-C-Affective: 0(0–3) vs 8(3–12), P<0.001; D-12-C-Total: 6(2–12) vs 24(12–33), P<0.001), non-depression vs depression: D-12-C-Physical: 5(1–9) vs 7(3–17.25), P=0.011; D-12-C-Affective: 0(0–3) vs 3(0–5.5), P<0.001; D-12-C-Total: 6(2–12) vs 8.5(4–23.25), P=0.004)) (Table 5). The results in Figure 2 showed that the D-12-C score of patients with mMRC grade 3 significantly increased compared to patients with mMRC grade 2 (P<0.001). The results in Figure 3 showed that the score of D-12-C (both physical and total score) increased as the GOLD stage rose (P<0.001). There was no significant difference in the D-12-C affective score across GOLD stage (P=0.826).
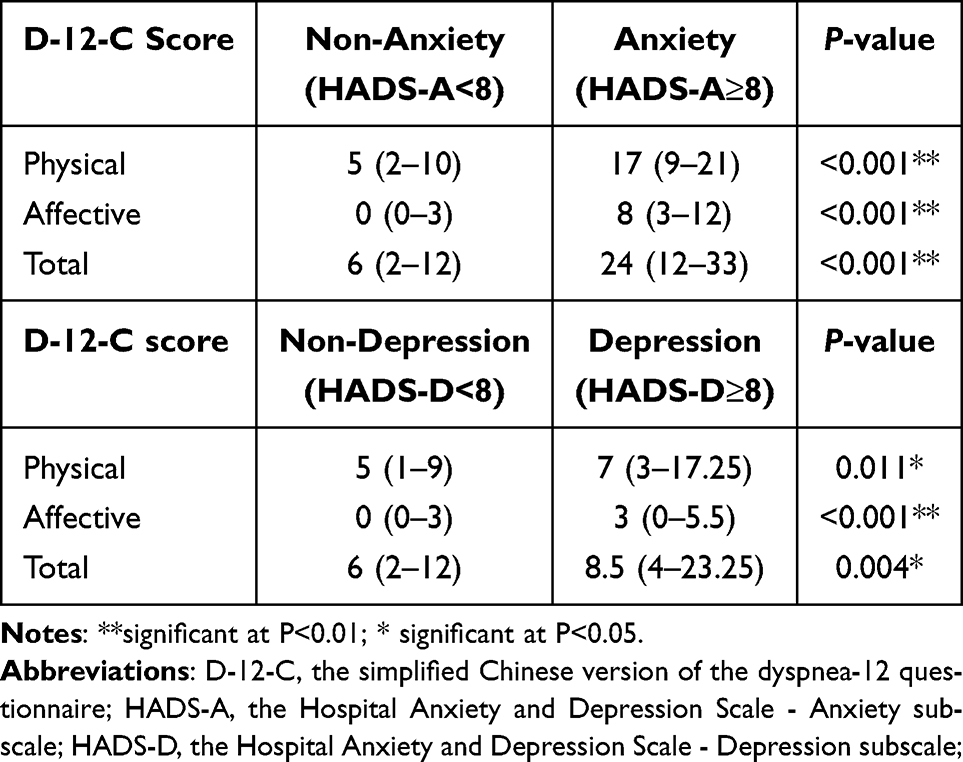 |
Table 5 The Difference in D-12-C Score Between Patients with Anxiety and Depression |
 |
Figure 2 The differences in D-12-C across mMRC grade. Abbreviation: D-12-C-Physical, the physical dimension score of simplified Chinese version of the dyspnea-12 questionnaire; D-12-C-Affective, the affective dimension score of simplified Chinese version of the dyspnea-12 questionnaire; D-12-C-Total, the total score of simplified Chinese version of the dyspnea-12 questionnaire. |
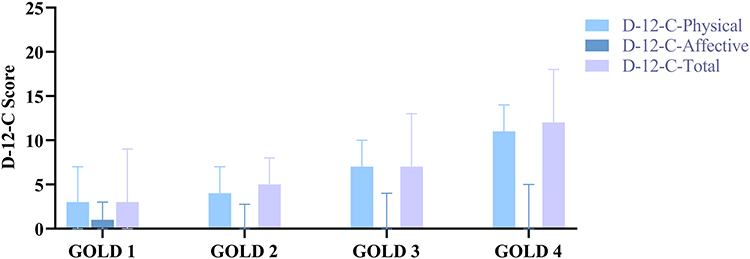 |
Figure 3 The D-12-C score across GOLD stage. Abbreviation: D-12-C, the simplified Chinese version of the dyspnea-12 questionnaire; GOLD, the Global Initiative for Obstructive Lung Disease D-12-C-Physical, the physical dimension score of simplified Chinese version of the dyspnea-12 questionnaire; D-12-C-Affective, the affective dimension score of simplified Chinese version of the dyspnea-12 questionnaire; D-12-C-Total, the total score of simplified Chinese version of the dyspnea-12 questionnaire. |
Exacerbation in the Past Year
Patients with high exacerbation risk had the higher total score of D-12-C (6 (1–11) vs 6 (2–13), P=0.035). However, there was no statistically significant difference between the two groups in the single dimension (Figure 4A). The frequent exacerbators had more severe dyspnea (D-12-C-Physical: 5 (1–8) vs 7 (3–14), P=0.007; D-12-C-Affective: 0 (0–3) vs 1 (0–5), P=0.018; D-12-C-Total: 6 (2–12) vs 9 (3–18), P=0.002) (Figure 4B).
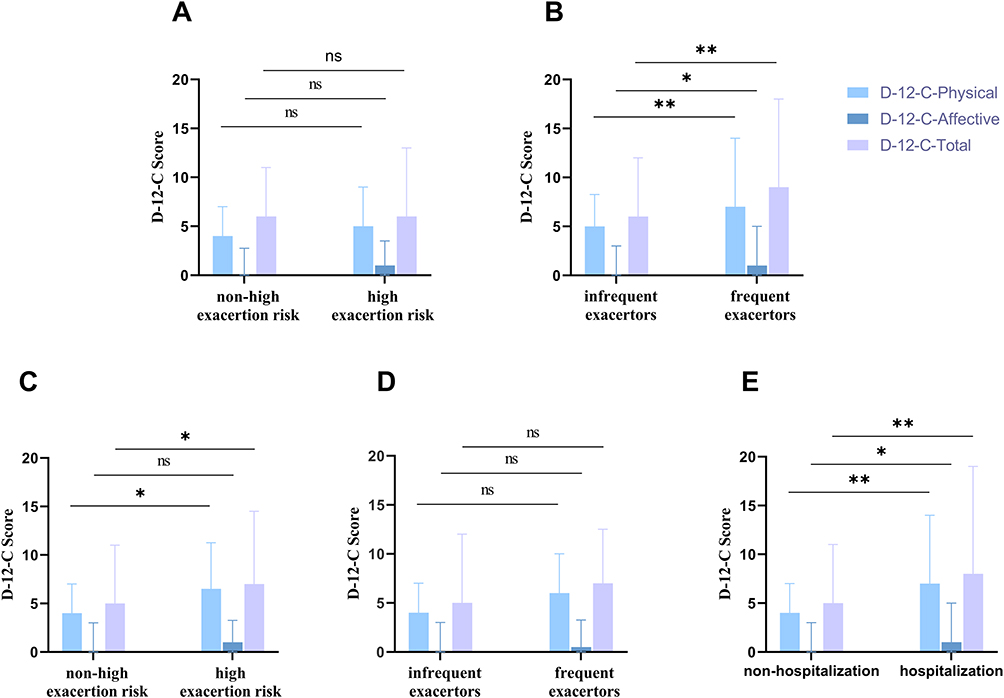 |
Figure 4 (A) Comparison of the D-12-C scores between patients with high exacerbation risk or not over the past year; (B) Comparison of the D-12-C scores between the group of frequent exacerbator or infrequent exacerbators over the past year; (C) Comparison of the D-12-C scores between patients with high exacerbation risk or not during a one-year follow-up; (D) Comparison of the D-12-C scores between the group of frequent exacerbator or infrequent exacerbators during a one-year follow-up; (E) Comparison of the D-12-C scores between patients with and without hospitalization during a one-year follow-up. Abbreviation: D-12-C-Physical, the physical dimension score of simplified Chinese version of the dyspnea-12 questionnaire; D-12-C-Affective, the affective dimension score of simplified Chinese version of the dyspnea-12 questionnaire; D-12-C-Total, the total score of simplified Chinese version of the dyspnea-12 questionnaire. Notes: nsnot significant as P>0.05; *significant at P<0.05; **significant at P<0.01. |
Exacerbation During Follow-Up
Patients with high exacerbation risk had the higher physical score and total score of D-12-C (D-12-C-Physical: 5 (1–8) vs 7 (3–14), P=0.013; D-12-C-Affective: 0 (0–3) vs 1 (0–5), P=0.268; D-12-C-Total: 6 (2–12) vs 9 (3–18), P=0.018) (Figure 4C). There was no statistically significant difference in the baseline D-12-C score between the frequent exacerbators and infrequent exacerbators during 1-year follow-up (Figure 4D). However, as shown in Figure 4E, patients who had at least one hospitalization during follow-up had more serious dyspnea at baseline as measured by D-12-C than those without hospitalization (D-12-C-Physical: 4(1–7) vs 7(3–14), P=0.002; D-12-C-Affective: 0(0–3) vs 1(0–5), P=0.039; D-12-C-Total: 5(1–11) vs 8(5–19), P=0.002).
Through binary multivariate logistic regression after stepwise selection, we found that baseline D-12-C total score was an independent influencing factor for hospitalization during follow-up after adjusting for age, gender and the exacerbations in the past year (OR=1.086, 95% CI: 1.035–1.139, p < 0.001) (Table 6).
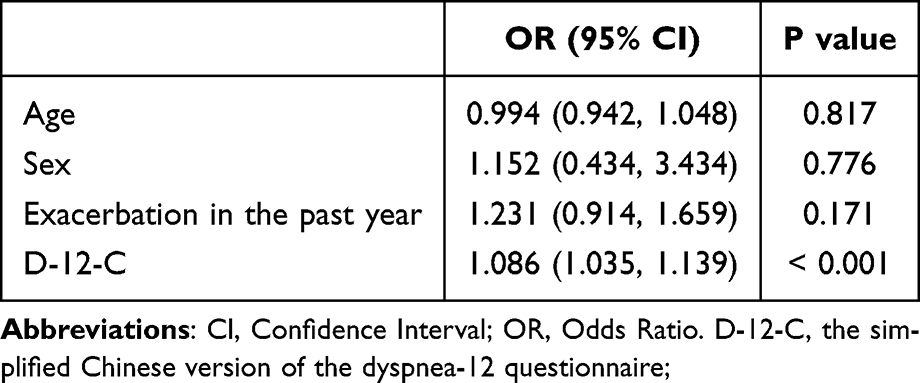 |
Table 6 Binary Logistic Regression of Hospitalization Due to Exacerbation of COPD |
Discussion
This is the first study that developed and validated a simplified Chinese version of D-12 (D-12-C) for the multidimensional assessment of breathlessness in patients with stable COPD, in which we found that it is valid and reliable in terms of internal consistency, structural validity and convergent validity. The D-12-C score was significantly correlated with multiple patient-reported outcome measures, and frequent exacerbators demonstrated higher D-12-C scores compared to infrequent exacerbators over the past year. Importantly, the baseline D-12-C score was an independent predictor of hospitalization during the one-year follow-up period. A traditional Chinese version of D-12 has been designed and verified but it may only apply to a limited region of China because of the regional differences of Chinese.35 Actually, Simplified Chinese is the standardized written form of the Chinese language used predominantly in Mainland China. Therefore, the D-12-C has a broad range of applicability and promotion that can be applied in all parts of China and other Mandarin speaking areas of the world. Secondly, compared to this study which included 155 participants in a single center,35 our study included a total of 279 participants from three centers, which increased the credibility and reliability of the results. Lastly, we identified the role of D-12-C in predicting hospitalization by using prospective and longitudinal clinical data.
Similar to the original version of D-12,19 the internal consistency of D-12-C (total, physical, affective) are all greater than 0.9. We found a strong association between the total D-12-C score and the SGRQ total score, and a similar result was reported in the English version of D-12 (rs=0.79).19 The correlation indicated that patients who have experienced severe dyspnea also had more negative impacts on the quality of life. Furthermore, compared to previous research,19,25,27,33 D-12-C was moderately associated with mMRC and CAT, indicating that the D-12-C score correlated to other instrument for dyspnea assessment and symptoms of COPD. While the mMRC scale excellently evaluates functional limitation and the CAT score offers a broad overview of health status, the D-12-C is uniquely positioned to quantify the often-overlooked affective dimension of dyspnea (such as fear, anxiety, and distress). This affective response is a potent driver of maladaptive behaviors and poor outcomes. Therefore, a composite assessment strategy could be highly powerful: for instance, using the mMRC for initial functional screening and then applying the D-12-C to further risk-stratify. This would allow clinicians to pinpoint patients who are particularly vulnerable due to the psychological impact of their breathlessness – a group that may be missed by conventional tools.
The initial purpose for the design of D-12 questionnaire was to describe dyspnea not only related to physical but also affective components. There was a significant correlation between D-12-C affective score and HADS (rs=0.549), and the result was similar to other studies.24,35,55 Both the affective component of D-12-C and HADS involve the assessment of anxiety and depression. The D-12-C measures the emotional changes caused by dyspnea and HADS focuses more on conventional anxiety or depression. Additionally, we found that patients with anxiety or depression had more severe dyspnea. Previous studies have shown that dyspnea is a predictor of depression in patients with COPD,56 and anxiety or depression is associated with more severe dyspnea conversely.3 Therefore, the interrelationship between dyspnea and anxiety or depression emphasizes the necessity of evaluating affective component in the assessment and treatment of dyspnea. A weak correlation was revealed between the total score of D-12-C and FEV1%pred, which also indicates the necessity of using multidimensional measurement tools to quantify breathlessness rather than functional abnormality only.
Interestingly, we found that D-12-C was correlated with frequent exacerbations over the past year and hospitalization during one year of follow-up. The results of binary logistic regression analysis showed that after adjusting for age and gender, baseline D-12-C score was an independent factor predicting future risk of hospitalization. As the D-12-C score increases by one unit, the probability of hospitalization for patients increases by 1.086 times. Hospitalization for AECOPD results in a rapid decline in health status with a high risk of mortality or other negative outcomes such as need for endotracheal intubation or intensive care unit admission. A recent clinical study used the univariate Cox proportional hazards model to explore the predictive properties of patient-reported outcomes for mortality and the time to first exacerbation of COPD. It had found that D-12 total score and its physical score were significant predictors for the time to the first exacerbation.57 We demonstrated that the D-12-C was significant related to health status (SGRQ) and, crucially, the future hospitalizations, suggesting its potential predictive utility for identifying patients at high risk of exacerbations. The predictive characteristics position of the D-12-C not merely as an assessment tool, but as a practical instrument for risk stratification. Furthermore, the D-12-C can quantify the distressing affective experience of breathlessness, and the multidimensional and predictive characteristics could be integrated into clinical care: Firstly, the D-12-C is brief, typically requiring less than five minutes for a patient to complete, making it a low-cost, high-yield strategy for assessing the physical and affective dimensions of dyspnea and optimizing resource allocation. Secondly, a high baseline D-12-C score, particularly on the affective subscale, could flag patients who may benefit from early referral to pulmonary rehabilitation programs that incorporate psychological support. Finally, in the context of hospital discharge planning, the D-12-C could aid in risk stratification, identifying patients who require more intensive follow-up to prevent readmission. The future prospective studies are needed to define specific cutoff scores for clinical decision-making and to validate its predictive power in longitudinal cohorts. Nonetheless, the present study provides the essential foundation for these next steps by delivering a validated tool ready for implementation in both clinical and research settings.
The main advantage of this study is that we firstly developed the simplified Chinese version of the Dyspnea-12 questionnaire, which is suitable for all Chinese populations, and validated this instrument in patients with stable COPD at multiple centers which indicated high external efficacy. Furthermore, we also discovered the clinical utility of D-12-C whose baseline score was associated with hospitalization during the follow-up, and the D-12-C was an independent predictor for hospitalization of COPD. Limitations also should be considered that two items in the affective dimension lack independence, indicating a correlation between the two items, similar results were found in the Norwegian version of D-12,25 and further validation is needed in different disease populations. Additionally, the affective score of D-12-C in our study is lower than other versions of D-12 (Swedish version: 6.1 (4.4); Norwegian version: 7.2 (4.5)),25,27 it may be related to under‐report psychological distress because of the social stigma in Chinese people. Actually, the Cantonese version of D-12 also found similar results, and the authors explained that this may be due to the underestimation of physical symptoms and psychological distress in their study population.35 A cross-sectional study of Chinese patients with COPD demonstrated that the prevalence of alexithymia symptoms in patients with COPD was 23.63%, and the male patients are more likely to suffer from alexithymia than female patients.9 Furthermore, Chinese people are more reserved than Westerners, and are unwilling to directly express their inner emotions and feelings.58 Furthermore, Chinese people are more reserved than Westerners, and are unwilling to directly express their inner emotions and feelings.59 Patients may be more inclined to express emotional distress through physical symptoms (such as emphasizing “chest tightness” or “fatigue”) rather than directly reporting feelings of fear or distress. Our findings require further validation in an independent external cohort to confirm the generalizability of the predictive model derived from the D-12-C. Although our multicenter design enhances the internal diversity of our sample, explicit external validation would strengthen confidence in our results. We did not assess the association between D-12-C scores and long-term hard endpoints, such as mortality or accelerated lung function decline. Future studies involving longer follow-up durations and diverse, independent populations are warranted to confirm the prognostic utility of the D-12-C for these critical endpoints and to establish its robustness across different healthcare settings. Furthermore, a proportion of patients with a score of zero suggests that the D-12-C may have a ceiling effect in populations with mild COPD or early COPD, potentially limiting its ability to detect subtle changes in this specific subgroup. Future studies focusing on earlier stages of disease should consider this. Lastly, the study finding needs to be validated in broader populations in China, and further studies for patients with other respiratory and cardiovascular disease are also needed. Additionally, the D-12-C could be integrated into digital health tools.
Conclusion
This study confirms the reliability, construct validity and convergent validity of D-12-C in patients with stable COPD in multiple centers. D-12-C can raisely evaluate dyspnea from both affective and physical dimensions and measure its changes. The score of D-12-C was strongly associated with SGRQ and increased as the GOLD stage or mMRC grade rose, and patients with anxiety or depression had worse dyspnea in COPD. Importantly, our findings establish the clinical application of D-12-C as an independent predictor for the risk of severe exacerbation in terms of hospitalization in COPD. This underscores its potential role not only in symptom assessment but also in risk stratification and guiding the management of high-risk patients. The D-12-C is a comprehensive multidimensional measurement tool used in clinical or research to evaluate dyspnea in COPD. This study also filled a national gap in Mandarin-speaking populations, especially for healthcare systems using Simplified Chinese. D-12-C has the potential to serve as a clinical instrument to assess severity of dyspnea clinically and for research in Mandarin-speaking areas with large population.
Data Sharing Statement
The original contributions presented in the study are included in the article, and further inquiries can be directed to the corresponding author.
Ethical Approval and Informed Consent
This study has obtained ethical approval from the West China Hospital, Sichuan University (ethics approval number: 2021-1394), the No. 3 Affiliated Hospital of Chengdu University of Traditional Chinese Medicine (West District)/Chengdu Pidu District Hospital of Traditional Chinese Medicine (ethics approval number: 2020027), and Chengdu Xinjin District Hospital of Traditional Chinese Medicine (ethics approval number: 2021-08-20-01). All participants in this study were willing to attend the study and provided written informed consent.
This study have performed in accordance with the principles stated in the Declaration of Helsinki.
Acknowledgments
We thank all the participants and researchers who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by the National Natural Science Foundation of China (No.82174139), the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (No. 2018-119), and Sichuan Science and Technology Program of China (2023NSFSC1460). The funder will not be involved in the conduct or interpretation of this trial, or in any decision to publish the results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Parshall MB, Schwartzstein RM, Adams L. et al. An official American thoracic society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012;185(4):435–452. doi:10.1164/rccm.201111-2042ST
2. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. Global Initiative for Chronic Obstructive Lung Disease. 2021. Available from: https://goldcopd.org/.
3. Wu D, Zhao X, Huang D, et al. Outcomes associated with comorbid anxiety and depression among patients with stable COPD: a patient registry study in China. J Affect Disord. 2022;313:77–83. doi:10.1016/j.jad.2022.06.059
4. Crisafulli E, Ielpo A, Barbeta E, et al. Clinical variables predicting the risk of a hospital stay for longer than 7 days in patients with severe acute exacerbations of chronic obstructive pulmonary disease: a prospective study. Respir Res. 2018;19(1):261. doi:10.1186/s12931-018-0951-4
5. Figarska SM, Boezen HM, Vonk JM. Dyspnea severity, changes in dyspnea status and mortality in the general population: the Vlagtwedde/Vlaardingen study. Eur J Epidemiol. 2012;27(11):867–876. doi:10.1007/s10654-012-9736-0
6. Ho SF. Dyspnoea and quality of life in older people at home. Age Ageing. 2001;30(2):155–159. doi:10.1093/ageing/30.2.155
7. Hill K, Hug S, Smith A, O’Sullivan P. The role of illness perceptions in dyspnoea-related fear in chronic obstructive pulmonary disease. J Clin Med. 2023;13(1):200. doi:10.3390/jcm13010200
8. Hart JL, Summer AE, Ogunduyile L, et al. Accuracy of expected symptoms and subsequent quality of life measures among adults with COPD. JAMA Network Open. 2023;6(11):e2344030. doi:10.1001/jamanetworkopen.2023.44030
9. O’Donnell DE, Milne KM, James MD, de Torres JP, Neder JA. Dyspnea in COPD: new mechanistic insights and management implications. Adv Therapy. 2020;37(1):41–60. doi:10.1007/s12325-019-01128-9
10. Ding B, Judge D, Small M, Bent-Ennakhil N, Siddiqui S. Functional performance in patients with COPD: association with treatment regimen, GOLD group, lung function, and symptom burden in a cross-sectional study. Int J Chronic Obstr. 2018;13:2785–2796. doi:10.2147/COPD.S170391
11. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the medical research council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
12. Mahler DA, Rosiello RA, Harver A, Lentine T, McGovern JF, Daubenspeck JA. Comparison of clinical dyspnea ratings and psychophysical measurements of respiratory sensation in obstructive airway disease. Am Rev Respir Dis. 1987;135(6):1229–1233. doi:10.1164/arrd.1987.135.6.1229
13. Aitken RC. Measurement of feelings using visual analogue scales. Procee Royal Soc Med. 1969;62(10):989–993. doi:10.1177/003591576906201005
14. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Europ Resp J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
15. Yohannes AM, Murri MB, Hanania NA, et al. Depressive and anxiety symptoms in patients with COPD: a network analysis. Respir Med. 2022;198:106865. doi:10.1016/j.rmed.2022.106865
16. Stubbs MA, Clark VL, Gibson PG, Yorke J, McDonald VM. Associations of symptoms of anxiety and depression with health-status, asthma control, dyspnoea, dysfunction breathing and obesity in people with severe asthma. Respir Res. 2022;23(1):341. doi:10.1186/s12931-022-02266-5
17. Bottemanne H, Gouraud C, Hulot JS, et al. Do anxiety and depression predict persistent physical symptoms after a severe COVID-19 episode? A prospective study. Front Psychiatry. 2021;12:757685. doi:10.3389/fpsyt.2021.757685
18. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation. Am Rev Respir Dis. 1992;145(6):1321–1327. doi:10.1164/ajrccm/145.6.1321
19. Yorke J, Moosavi SH, Shuldham C, Jones PW. Quantification of dyspnoea using descriptors: development and initial testing of the Dyspnoea-12. Thorax. 2010;65(1):21–26. doi:10.1136/thx.2009.118521
20. Lemmers JMJ, Vonk MC, van den Ende CHM. Patient-reported outcomes to assess dyspnoea in interstitial lung disease and pulmonary hypertension: a systematic literature review of measurement properties. Euro Resp Rev. 2022;31(166):220091. doi:10.1183/16000617.0091-2022
21. Yorke J, Swigris J, Russell A-M, et al. Dyspnea-12 is a valid and reliable measure of breathlessness in patients with interstitial lung disease. Chest. 2011;139(1):159–164. doi:10.1378/chest.10-0693
22. Yorke J, Russell A-M, Swigris J, et al. Assessment of dyspnea in asthma: validation of The Dyspnea-12. J Asthma. 2011;48(6):602–608. doi:10.3109/02770903.2011.585412
23. Olsson M, Ekström M. Validation of the Dyspnoea-12 and multidimensional Dyspnea profile among older Swedish men in the population. BMC Geriatr. 2022;22(1):477. doi:10.1186/s12877-022-03166-5
24. Kako J, Kobayashi M, Kajiwara K, et al. Validity and reliability of the Japanese version of the Dyspnea-12 questionnaire in patients with lung cancer. J Pain Symptom Manage. 2022;64(2):e83–e89. doi:10.1016/j.jpainsymman.2022.04.171
25. Garratt AM, Nerheim EM, Einvik G, Stavem K, Edvardsen A. Evaluation of the Norwegian version of the Dyspnoea-12 questionnaire in patients with COPD. BMJ Open Respir Res. 2022;9(1):e001262. doi:10.1136/bmjresp-2022-001262
26. Nishimura K, Oga T, Nakayasu K, et al. Comparison between tools for measuring breathlessness: cross-sectional validation of the Japanese version of the Dyspnoea-12. Clin Resp J. 2021;15(11):1201–1209. doi:10.1111/crj.13427
27. Sundh J, Bornefalk H, Sköld CM, et al. Clinical validation of the Swedish version of Dyspnoea-12 instrument in outpatients with cardiorespiratory disease. BMJ Open Respir Res. 2019;6(1):e000418. doi:10.1136/bmjresp-2019-000418
28. Simsic AA, Yorke J, Regueiro EG, Di Lorenzo VP, Baddini-Martinez J. Validation of the dyspnoea-12 scale into Portuguese speaking COPD patients. Clin Respira J. 2018;12(5):1942–1948. doi:10.1111/crj.12762
29. Caruso R, Arrigoni C, Groppelli K, et al. Italian version of Dyspnoea-12: cultural-linguistic validation, quantitative and qualitative content validity study. Acta Bio-Medica. 2018;88(4):426–434. doi:10.23750/abm.v88i4.6341
30. Beaumont M, Couturaud F, Jego F, et al. Validation of the French version of the London chest activity of daily living scale and the Dyspnea-12 questionnaire. Int J Chronic Obstr. 2018;13:1399–1405. doi:10.2147/COPD.S145048
31. Amado Diago CA, Puente Maestu L, Abascal Bolado B, et al. Translation and validation of the multidimensional Dyspnea-12 questionnaire. Archivos de Bronconeumología. 2018;54(2):74–78. doi:10.1016/j.arbr.2017.08.015
32. Sundh J, Ekström M. Dyspnoea-12: a translation and linguistic validation study in a Swedish setting. BMJ Open. 2017;7(5):e014490. doi:10.1136/bmjopen-2016-014490
33. Alyami MM, Jenkins SC, Lababidi H, Hill K. Reliability and validity of an arabic version of the dyspnea-12 questionnaire for Saudi nationals with chronic obstructive pulmonary disease. Ann Thoracic Med. 2015;10(2):112–117. doi:10.4103/1817-1737.150730
34. Al-Gamal E, Yorke J, Al-Shwaiyat MKEA. Dyspnea-12-Arabic: testing of an instrument to measure breathlessness in Arabic patients with chronic obstructive pulmonary disease. Heart Lung. 2014;43(3):244–248. doi:10.1016/j.hrtlng.2014.02.003
35. Choi TCM, Chan LLY, Tsang HC, et al. Adaptation and validation of the Chinese version of Dyspnoea-12 scale in individuals with chronic obstructive pulmonary disease. Clin Respir J. 2021;15(10):1081–1087. doi:10.1111/crj.13411
36. Pothirat C, Chaiwong W, Phetsuk N, et al. Dialectal influence on chronic pulmonary disease assessment test: the reliability and validity study. Int J Chronic Obstr. 2015;10:541–548. doi:10.2147/COPD.S79041
37. Lee S-D, Huang M-S, Kang J, et al. The COPD assessment test (CAT) assists prediction of COPD exacerbations in high-risk patients. Respir Med. 2014;108(4):600–608. doi:10.1016/j.rmed.2013.12.014
38. Martin AL, Marvel J, Fahrbach K, Cadarette SM, Wilcox TK, Donohue JF. The association of lung function and St. George’s respiratory questionnaire with exacerbations in COPD: a systematic literature review and regression analysis. Respir Res. 2016;17(1):40. doi:10.1186/s12931-016-0356-1
39. Stevens JP, Dechen T, Schwartzstein RM, O’Donnell CR, Baker K, Banzett RB. Association of dyspnoea, mortality and resource use in hospitalised patients. Europ resp J. 2021;58(3):1902107. doi:10.1183/13993003.02107-2019
40. Müller A, Wouters EFM, Burney P, et al. Quality of life associated with breathlessness in the multinational burden of obstructive lung disease (BOLD) study: a cross-sectional analysis. Pulmonology. 2025;31(1):2470566. doi:10.1080/25310429.2025.2470566
41. Yorke J, Armstrong I. The assessment of breathlessness in pulmonary arterial hypertension: reliability and validity of the Dyspnoea-12. Eur J Cardiovasc Nurs. 2014;13(6):506–514. doi:10.1177/1474515113514891
42. Koller M, Kantzer V, Mear I, et al. The process of reconciliation: evaluation of guidelines for translating quality-of-life questionnaires. Expert Rev Pharmacoecon Outcomes Res. 2012;12(2):189–197. doi:10.1586/erp.11.102
43. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value in Health. 2005;8(2):94–104. doi:10.1111/j.1524-4733.2005.04054.x
44. Wiklund I, Berry P, Lu KX, Fang J, Fu C. The Chinese translation of COPD assessment testTM (CAT) provides a valid and reliable measurement of COPD health status in Chinese COPD patients. Am J Respir Crit Care Med. 2010;181:A3575.
45. Xian-ling M, Yu-ting H, Ruo-lin M, Zhi-hong C. Application of St George’s respiratory questionnaire, CAT and mMRC in chronic obstructive pulmonary disease. Fudan Univ J Med Sci. 2022;49(06):862–868+876.
46. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
47. Yang Y, Ding R, Hu D, Zhang F, Sheng L. Reliability and validity of a Chinese version of the Hads for screening depression and anxiety in psycho-cardiological outpatients. Comprehen Psychiatry. 2014;55(1):215–220. doi:10.1016/j.comppsych.2013.08.012
48. Xu W, Collet JP, Shapiro S, et al. Validation and clinical interpretation of the St George’s respiratory questionnaire among COPD patients, China. Interl J Tuberculos Lung Dis. 2009;13(2):181–189.
49. Pulmonary ACo PSfC, Laboratories F. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
50. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. An official American thoracic society and European respiratory society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
51. Le Rouzic O, Roche N, Cortot AB, et al. Defining the “frequent exacerbator” phenotype in COPD. Chest. 2018;153(5):1106–1115. doi:10.1016/j.chest.2017.10.009
52. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. Global Initiative for Chronic Obstructive Lung Disease. 2022. Available from: https://goldcopd.org/.
53. Kaplan RM, Ries AL, Reilly J, Mohsenifar Z. Measurement of health-related quality of life in the national emphysema treatment trial. Chest. 2004;126(3):781–789. doi:10.1378/chest.126.3.781
54. Snaith RP. The Hospital Anxiety and Depression Scale. Health Qual Life Outcomes. 2003;1(1):29. doi:10.1186/1477-7525-1-29
55. Tan J-Y, Yorke J, Harle A, et al. Assessment of breathlessness in lung cancer: psychometric properties of the Dyspnea-12 questionnaire. J Pain Symptom Manage. 2017;53(2):208–215. doi:10.1016/j.jpainsymman.2016.08.009
56. Miravitlles M, Molina J, Quintano JA, Campuzano A, Pérez J, Roncero C. Factors associated with depression and severe depression in patients with COPD. Respir Med. 2014;108(11):1615–1625. doi:10.1016/j.rmed.2014.08.010
57. Nishimura K, Kusunose M, Sanda R, Mori M, Shibayama A, Nakayasu K. Comparison of predictive properties between tools of patient-reported outcomes: risk prediction for three future events in subjects with COPD. Diagnostics. 2023;13(13):2269. doi:10.3390/diagnostics13132269
58. Zhang H, Wang Y, Lou H, et al. Prevalence of and factors associated with alexithymia among patients with chronic obstructive pulmonary disease in China: a cross-sectional study. BMC Pulm Med. 2023;23(1):40. doi:10.1186/s12890-023-02335-5
59. Dion KL. Ethnolinguistic correlates of alexithymia: toward a cultural perspective. J Psychosom Res. 1996;41(6):531–539. doi:10.1016/s0022-3999(96)00295-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Patterns, Socioeconomic Status and Clinical Burden in Mild COPD: A Swedish Real-World, Retrospective Cohort Study, the ARCTIC Study
Larsson K, Lisspers K, Ställberg B, Johansson G, Gutzwiller FS, Mezzi K, Bjerregaard BK, Jorgensen L, Koo H, Janson C
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1409-1421
Published Date: 21 June 2022
Emergency Department Visits Due to Dyspnea: Association with Inhalation Therapy in COPD and Cases with Adverse Drug Reactions
Bergs I, Just KS, Müller A, Stingl JC, Dreher M
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1827-1834
Published Date: 11 August 2022
Automated Oxygen Administration Alleviates Dyspnea in Patients Admitted with Acute Exacerbation of COPD: A Randomized Controlled Trial
Sandau C, Hansen EF, Ringbæk TJ, Kallemose T, Bove DG, Poulsen I, Nørholm V, Pedersen L, Jensen JUS, Ulrik CS
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:599-614
Published Date: 18 April 2023
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023
Real-World Disease Burden and Healthcare Resource Utilization Among Patients with COPD and Asthma Using Triple Therapy (FF/UMEC/VI) in the United States
Igboekwe E, Verma S, Paczkowski R
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:281-296
Published Date: 25 January 2024