Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Emergency Department Visits Due to Dyspnea: Association with Inhalation Therapy in COPD and Cases with Adverse Drug Reactions
Authors Bergs I ![]() , Just KS, Müller A, Stingl JC
, Just KS, Müller A, Stingl JC ![]() , Dreher M
, Dreher M
Received 19 March 2022
Accepted for publication 21 July 2022
Published 11 August 2022 Volume 2022:17 Pages 1827—1834
DOI https://doi.org/10.2147/COPD.S367062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Ingmar Bergs,1 Katja S Just,2 Annegret Müller,1 Julia C Stingl,2,* Michael Dreher1,*
1Department of Pneumology and Internal Intensive Care Medicine, University Hospital RWTH Aachen, Aachen, Germany; 2Institute of Clinical Pharmacology, University Hospital RWTH Aachen, Aachen, Germany
*These authors contributed equally to this work
Correspondence: Ingmar Bergs, Department of Pneumology and Internal Intensive Care Medicine, University Hospital RWTH Aachen, Pauwelsstr. 30, Aachen, 52074, Germany, Tel +49 241/80 35443, Email [email protected]
Purpose: Dyspnea is a leading symptom of COPD that causes presentations in emergency departments or negatively impacts on them. Guideline-based inhalation therapies are intended to reduce dyspnea in COPD patients. This study analyzed how common guideline recommended inhalation therapy regimens are occurring in clinical practice among COPD patients presenting to emergency departments due to adverse drug reactions in polytherapy using data of the German ADRED database.
Patients and Methods: In total, 269 COPD cases were identified. In a further analysis, all cases were analyzed for documented GOLD stage and guideline-recommended inhalation therapy for COPD. Dyspnea and other symptoms identified during ED presentation were analyzed and compared between patients who did and did not receive the guideline’s recommended inhalation therapy.
Results: In this observation, 41% (n = 46) of all 112 cases with a documented COPD and GOLD stage received an underdosed therapy according to current guidelines. Dyspnea was the most common identified symptom (32%, n = 36) in this cohort and occurred more often in patients who received an underdosage of inhalation therapy (p < 0.01).
Conclusion: Patients with COPD presenting to ED with ADRs show a high rate of non-guideline-recommended inhalation therapy and present more often with dyspnea compared to those COPD patients who received an adequate dosing of inhalation therapy.
Keywords: emergency department, dyspnea, guideline therapy, chronic obstructive pulmonary disease, adverse drug events
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most common pulmonary diseases, with an increasing prevalence worldwide.1 Chronic progression and limitations due to the symptoms of COPD present challenges to both patients and health-care systems.2 Leading symptoms of COPD are dyspnea and cough. In acute cases, patients may primarily present to emergency departments. In Germany, hospital admission rates as a result of COPD are significantly higher than in other countries, up to 200 admissions per 100.000 people.3 Various risk factors, such as age, severity of COPD and poor lung function influence patient outcomes.4 Recurrent hospital admissions and emergency presentations, coupled with disease progression, also lead to increased personnel and financial burdens in the healthcare system.5
Inhalation therapies that use bronchodilators have been established for decades. Long-acting beta-2 agonists (LABA) and long-acting muscarinic antagonists (LAMA) improve lung function, COPD symptoms and health status6–9 whilst short-acting beta-2 agonists and anticholinergics can reduce dyspnea.3 Inhaled glucocorticoids, in combination with bronchodilatators, can reduce the frequency of acute exacerbations.10 Current scientific data on optimal therapy for COPD, such as combination therapies of different drug classes, have been collated and summarized into guideline recommendations to improve patient care. Guideline recommendations provide guidance to physicians concerning optimal therapy in clinical practice. In Germany, the established guideline recommendations for the treatment of COPD have been based on the GOLD report which requires the inhaled therapy to be adjusted according to COPD severity and symptoms. Depending on the severity, monotherapy (LABA, LAMA) is extended to combination therapy (LABA+LAMA) or triple therapy (LABA+LAMA+ICS).11,12 The more severe the pulmonary obstruction is, the sooner patients become symptomatic and an adjustment of the anti-obstructive therapy takes place.
We used patient data from the observational ADRED cohort study on emergency admissions due to adverse drug reactions,13 to analyze how common guideline-based inhalation therapy regimens are applied in clinical practice for COPD patients who present to emergency departments with adverse drug reactions from polytherapy treatments.
Materials and Methods
Study Population
Participants of the multicentre prospective observational study trial named Adverse Drug Reactions in Emergency Departments (“ADRED”; DRKS-ID: DRKS00008979) were analyzed. The ADRED study draws on adverse drug reaction (ADR) cases in four large hospital EDs of tertiary care and academic teaching hospitals in Germany. These cases are classified as possible, probable or certainly related to drug intake. The recruitment of participants in the study followed the guidelines of the World Health Organization–Uppsala Monitoring Centre system for causality assessment by a trained physician or pharmacist.14 Data collection in ADRED draws on medical records (eg, diagnoses) of COPD cases, current medication plans and participant interviews. All medications taken by patients (including dosage) before presentation in the emergency department were recorded and analyzed. Further information of the ADRED study design has been published elsewhere.13,15 The ADRED database contained 2939 cases at the time of the study, with patients enrolled in the trial between 2015 and 2018. The ADRED study was approved by the responsible ethical committee of the University of Bonn (202/15), with all participants providing informed consent in accordance with the World Medical Association’s Declaration of Helsinki.
Data Collection and Classification of Cases
Cases with a co-diagnosis of COPD (according to ICD-10 codes) were selected from the ADRED cohort regardless of the reason for presentation to the emergency department. Demographic and clinical data including current drug intake, pre-existing diagnoses and reported symptoms were recorded. Symptoms were classified according to the “medical terminology for drug regulatory authorities” (MedDRA) and were analyzed on the “preferred term” level (PT).16
In total, 309 cases with a diagnosed COPD were identified. Subsequently, cases with multiple presentations during case recruitment or with incorrect documentation were excluded (40 cases). The remaining cases were analyzed against the international COPD classification of GOLD3 using documented ICD codes (ICD-10 codes). Cases with an undefined GOLD classification were excluded from further analysis, resulting in the enrollment of 112 cases. Two pneumologists analyzed and assessed the cases prescribed inhalation therapy against the graduated GOLD stage. Both pneumologists independently assessed whether the drug prescription met the current standard of COPD treatment according to the German COPD guideline.11 Each case’s drug prescription was examined for anti-obstructive drug classes (long-acting β-agonists (LABA), long-acting muscarinic-antagonists (LAMA), short-acting β-agonists (SABA), short-acting muscarinic-antagonists (SAMA) and inhaled corticosteroids (ICS)) and prescription errors. Prescription errors were classified as errors in dosage, in frequency of use and/or in the appropriateness of the combination of the prescription. Identified inappropriate prescriptions for COPD patients using inhaled therapies included, eg, single shot use of olodaterol/tiotropium respimat or multiple uses of salbutamol (SABA) per day without using a LABA or LAMA in basic therapy. The expert assessments were then compared and where assessments differed, cases were discussed and a common consensus was reached.
Following this work, patients with adequate therapy were compared to the group of patients with inadequate therapy. This comparative analysis examined typical symptoms of COPD including dyspnea and cough, which are treated by inhalation drug classes, reporting by patients in the emergency department. Further analysis examined whether the cause of presentation to the emergency department was also associated with dyspnea or worsening of COPD. For this purpose, the cases were bundled for the admission diagnoses dyspnea (R06) and COPD (J44) according to the common ICD-10 classification, which were then compared.
Statistical Analysis
Descriptive statistics were calculated for the study population. Continuous parameters were tested for normal distribution using the Kolmogorov–Smirnov test. Where results were not normally distributed, continuous parameters were presented as median and interquartile range (IQR) and compared using Mann–Whitney test. Categorical parameters were presented in absolute numbers and percentages. The frequency of symptoms and main diagnoses was compared between the two groups using the chi-squared test.
Results
A total of 112 cases (42%) were found with a defined GOLD stage3 with 19 cases (17%) classified as GOLD I, 40 cases (36%) as Gold II, 29 cases (26%) as GOLD III and 24 cases (21%) as GOLD IV. The median age of the study’s participants was 74 years old, with 61% of the cases male and 39% female. The study also identified that the median for drugs taken was 11 different drugs. Further characteristics of the study population are shown in Table 1.
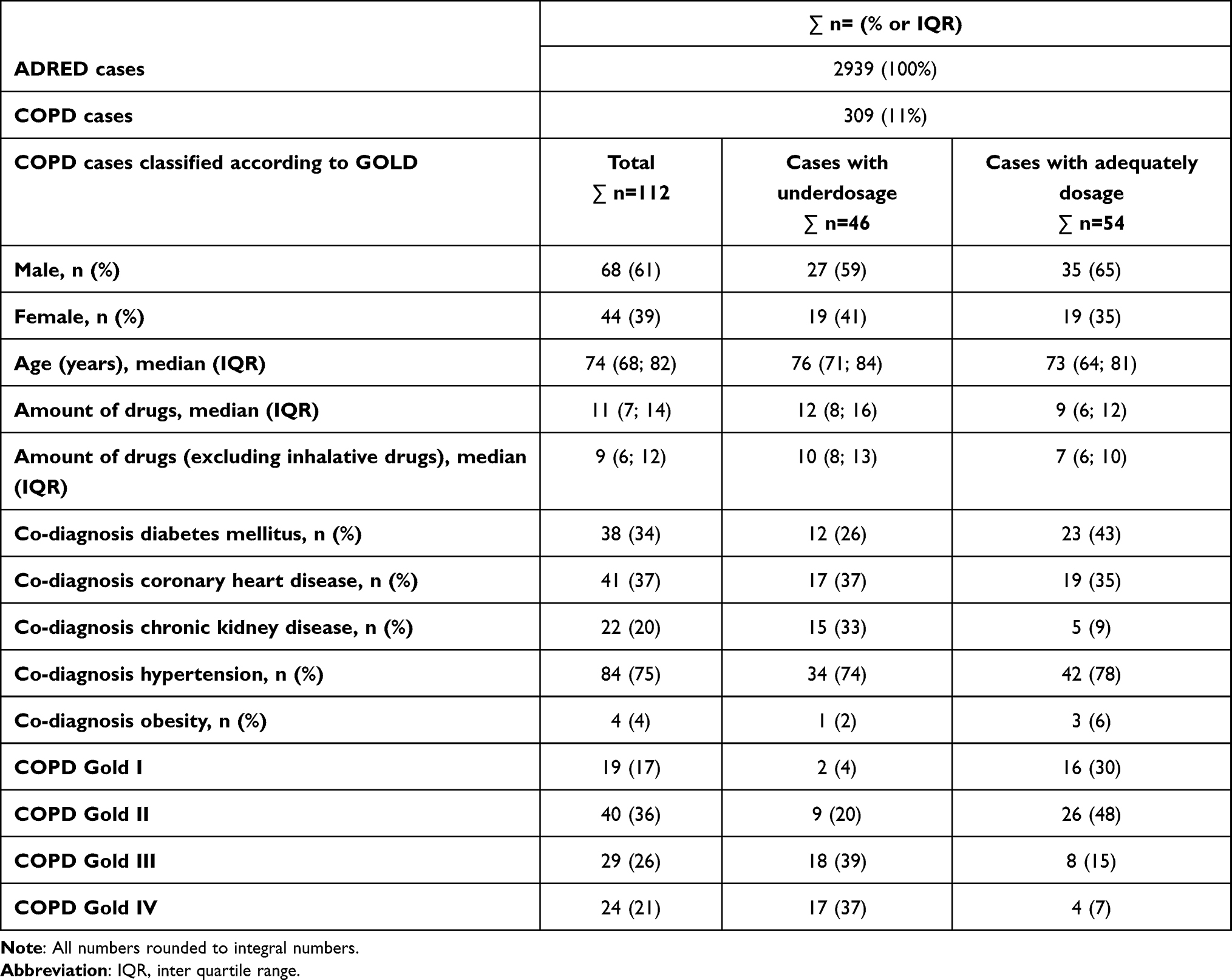 |
Table 1 Characteristics of the COPD-Cases in ADRED in General and Compared Between Cases with Adequately Dosage and Underdosage of Inhalation Therapy |
Inhalation therapy regimes were prescribed in 76 (68%) of all cases with a known Gold classification. A minimum of one long acting bronchodilatator was prescribed in 56 cases (74%) and a minimum of one short acting bronchodilatator was taken in 44 cases (58%). For cases with a documented inhalation therapy, LABA were prescribed in 49 cases (65%), LAMA in 45 cases (59%), ICS in 34 cases (45%), SABA in 41 cases (54%) and SAMA in 31 cases (41%). A LABA/LAMA combination therapy was taken in 15 cases (20%), a triple therapy including LABA/LAMA/ICS in 23 cases (30%) and a LABA/ICS combination in 6 cases (8%). The study also identified that single therapy was used in 5 cases (6%) for LABA, 7 cases (9%) for LAMA and in 5 cases (6%) for ICS. The study also found that 20 patients (26%) took both SABA and SAMA (Figure 1).
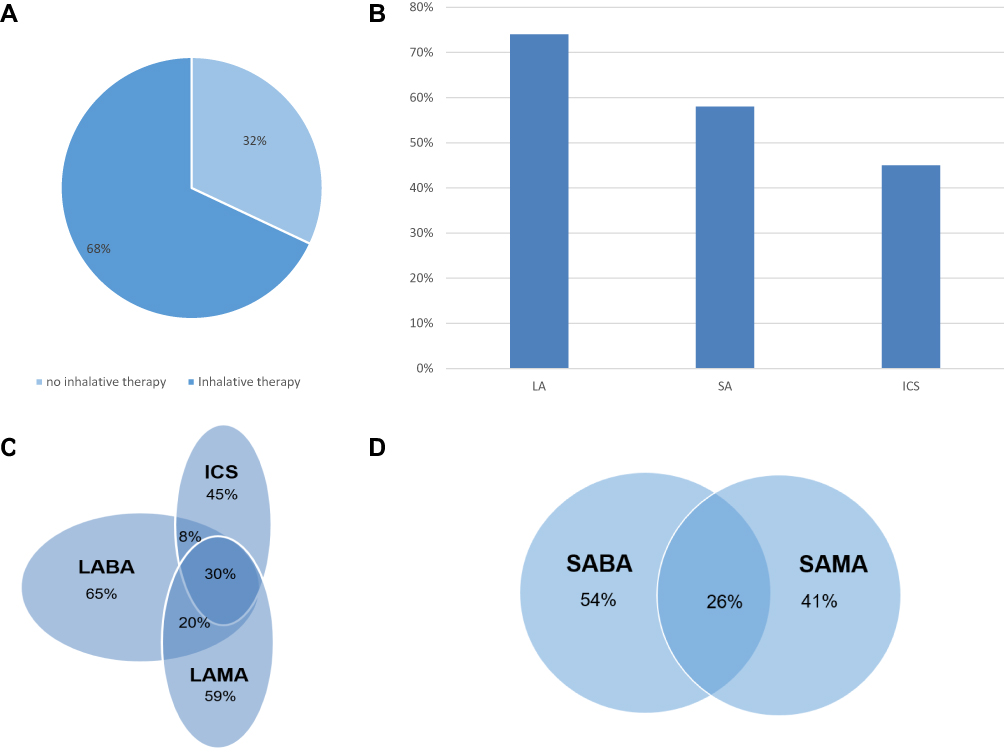 |
Figure 1 Therapy in the COPD Gold group (n=112); (A) inhalative therapy, (B) inhalative drug classes, (C) Venn chart of long-acting bronchodilatators and ICS, (D) Venn chart of short-acting bronchodilatators, All numbers rounded to integral numbers. Abbreviations: LA, long-acting bronchodilatator; SA, short-acting bronchodilatator; ICS, inhalative glucocorticoid; LABA, long-acting β-agonists; LAMA, long-acting muscarinic-antagonists; SABA, short-acting β-agonists; SAMA, short-acting muscarinic-antagonists. |
A total of 46 patients (41%) were classified as underdosed according to their GOLD stage and current guidelines,3 while there were 9 cases (8%) where the therapy was overdosed and 3 cases that had to be excluded due to insufficient documentation. The most commonly reported symptom at presentation to the emergency department in all COPD patients was “dyspnea” with 32% (n = 36); however, this diagnose was more often reported in the group of patients with underdosed therapy than in patients who were not underdosed (n = 24, p < 0.01). There was no significant difference between the two groups for the symptom “cough” (p = 0.23) and, except for dyspnea, there were no significant differences among the 10 most frequently complained ADR symptoms resulting in emergency admission between the groups (Table 2). COPD patients with underdosed therapy were more likely to be admitted to the emergency department due to worsening COPD (J44) and dyspnea (R06) (p = 0.03). Other ADR symptoms such as anemia, falling and dizziness did not differ between the adequately dosed versus underdosed COPD groups (Table 2). The most frequent diagnoses leading to the ED admission were “acute renal failure” (N17), “heart failure” (I50), “volume depletion” (E86) or “lung cancer” (C34), where each diagnosis represented 7% (n = 3) of the cases and was not more frequent compared to the other group with adequate inhaled therapy (p = 0.51).
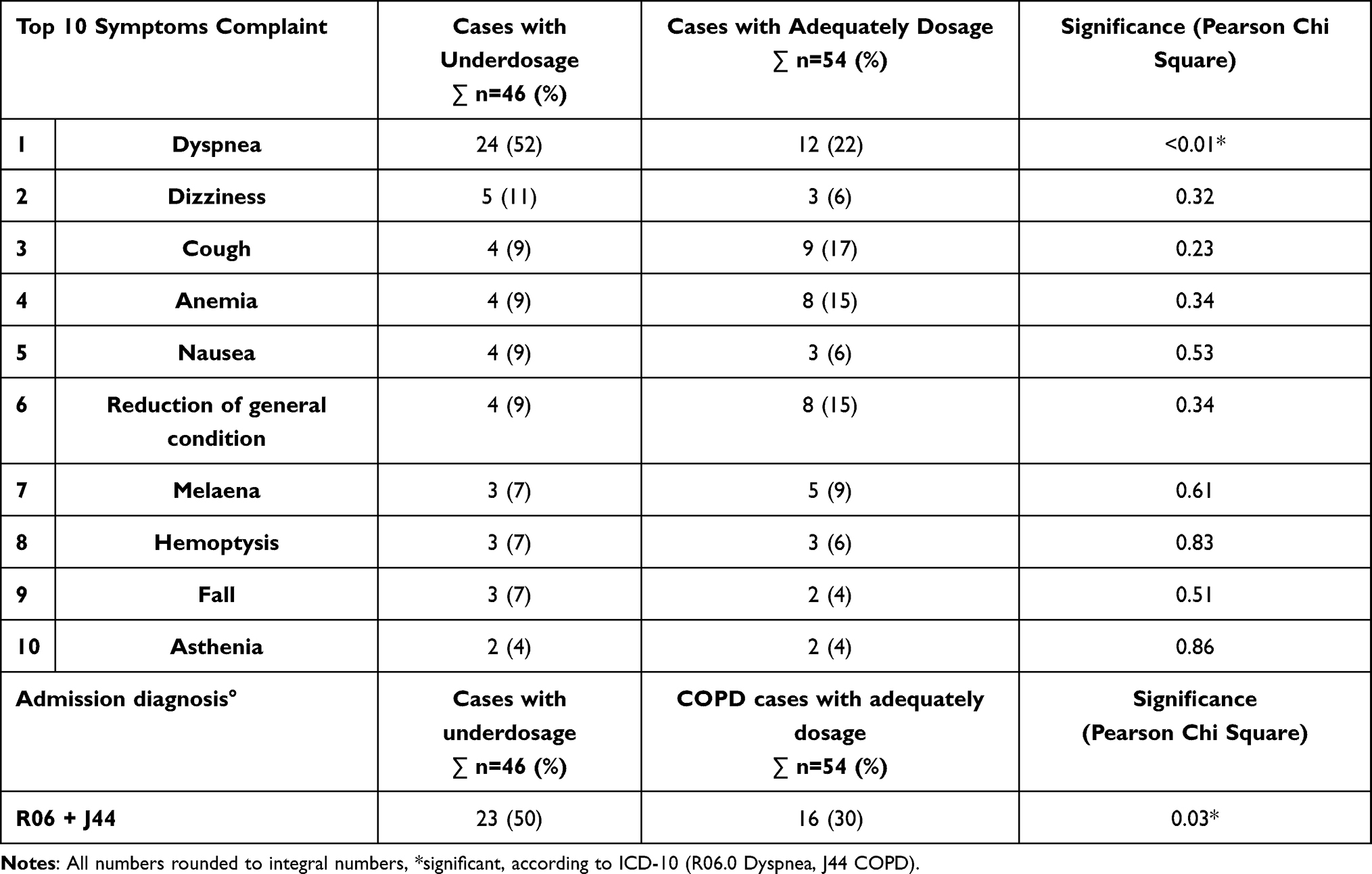 |
Table 2 Analysis of the Inhalation Therapy, Top 10 Symptoms Complaint and Admission Diagnosis “Dyspnea” |
The characteristics of the different groups are compared in Table 1. Patients with underdosed therapy regimes tended to be older and differed in comorbidities including chronic kidney disease, or diabetes. Cases with underdosed inhalation therapy were more often assigned to advanced Gold stages (COPD Gold III 39%, COPD Gold IV 37%) while cases with underdosed inhalation therapy regimes classified as Gold Stage II, III and IV complained more often of dyspnea during ED presentation compared to cases with adequate inhalation therapy regimes and advanced Gold stages (Table 3).
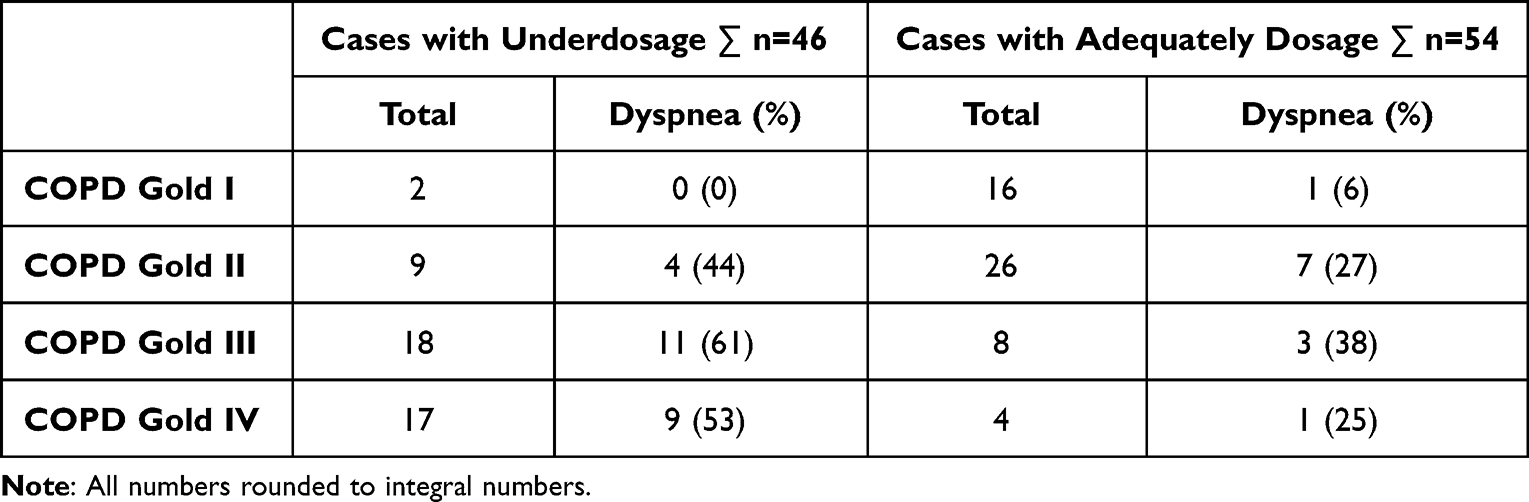 |
Table 3 Dyspnea in COPD-Cases Compared to GOLD and Therapy Assessment |
Discussion
This observational study shows that within a cohort of patients who present to emergency departments due to an ADR, dyspnea is the major symptom for COPD patients. However, dyspnea is more often observed in patients with underdosed inhalation therapy than COPD patients who are prescribed according to the guideline’s recommended inhalation therapy.
Analysis of the patient’s treatment when compared to the guideline’s derived dose found 41% of patients did not receive the recommended dosage of the inhalation therapy. This high number could be due to an accumulation of patient vulnerability factors as the ADRED cohort includes cases of severe ADRs presenting to the ED with severe symptoms. However, the evaluation of dosing shows that in 41% of ADRED patients with COPD, the recommended dose was not given and dyspnea was a common symptom which lead to ED admission. This finding suggests that a guideline-appropriate dose might have avoided the ED admissions.
The study shows real-world data of the treatment of COPD in Germany, irrespective of current national or international recommendations.1,3,17 It is interesting to note that 45% of cases took an ICS despite sufficient control of symptoms under a LABA/LAMA combination therapy. Only 58% of the patients on inhaled therapy reported using a short-acting bronchodilator even though these treatments recommended for dyspnea.18
Dyspnea is a common reason for presentation in EDs. Studies from the USA showed that dyspnea was the main reason for presentation in 12% of cases and that in 13% of these cases COPD was the cause of dyspnea.19 Similar data from Australia and Southeast Asia support these observations. There, COPD was estimated to be the cause of complained dyspnea in the ED at 19.7% and the incidence of acute exacerbated COPD was estimated at 13.6%.20,21 There was no investigation whether the presentation was also associated with insufficient adherence to the different classes of inhaled substance taken before presentation at the ED.
Causes of dyspnea, including exacerbation as a reason for presentation in ED, have been studied and discussed for years. In particular, classic risk factors identified in several studies4 found that age, comorbidities, the severity of COPD according to GOLD classification, lung function, or scores such as the Bode Index played a role in identifying causes of dyspnea.22–25 In addition, our study has shown that inadequate inhalation therapy in COPD patients resulted in dyspnea once patients were admitted to the ED following an ADR episode. Chavez et al found that only 55% of patients with COPD received the guideline’s recommended therapy;26 however, the data referred to general presentations and not explicit presentations to EDs. However, respecting a potentially less quality in medication documentation in EDs due to the urgency of cases, with a total of 49% of inadequate treated patients in our sample seem to be comparable to Chavez et al’s results despite the different health-care environments.
In addition, our study showed that when inhaled therapy guideline recommendations are not followed, there are more frequent presentations of dyspnea and patients presenting with worsening of COPD to EDs. This conclusion is supported by COPD treatment adherence data where27 less adherence to guidance leads to more hospitalizations and less adherence medication guidance leads to worsening of COPD symptoms.28,29 While we cannot make assumptions concerning medication adherence in our sample, the study shows comparable associations due to inadequately prescribed inhalation therapy. The results of this study draw on patients suffering from COPD who have been impacted by ADR and explicitly excludes patients with COPD admitted to the ED who have not been impacted by an ADR event which is a limitation of this study. However, COPD patient data that includes ADR are rare, so this study increases knowledge within this field. Another limitation of the study is the increased allocation of cases with underdosage of inhalation therapy in advanced stages of COPD compared to the group with adequate inhalation therapy. This is due to the fact that, according to the guidelines, inhaled therapy is not mandatory in early stages and is primarily administered on an as needed basis. Despite these limitations, the available data support the finding that dyspnea tends to be more frequent in the undertreated group with advanced COPD compared to patients with adequate dosing and advanced COPD. Additionally, the impact of comorbidities such as diabetes or chronic kidney disease on the main results of this study needs further critical examination.
The available data does not enable the drawing of conclusions as to why the patients in the study received inadequate care and cannot rule out other factors such as incorrect medication use by the patient or an incorrectly prescribed medication according to the guidelines. This study finds that poor adherence to therapy not only leads to a deterioration in the health status of patients but also results in increased costs for the healthcare system.
Conclusion
In a cohort of COPD patients presenting to EDs with ADRs, dyspnea is the most commonly presented symptom and was found significantly more in cases whose treatment did not follow the guideline’s recommended therapy compared to those COPD patients with an adequate dosing of inhaled therapy that complied with the guidelines.
Further studies should investigate ways to improve monitoring of therapy and education of COPD patients which would be expected to lead to better care outcomes and a reduction of unnecessary emergency department presentations.
Disclosure
Prof. Dr. Michael Dreher reports fees for speaking from Astra Zeneca, Berlin Chemie, Boehringer, Chiesi, GSK, and Novartis, received fees for consulting from Astra Zeneca, Boehringer, Chiesi, GSK, and Novartis. The authors report no other conflicts of interest in this work.
References
1. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease – 2022 report. Available from: https://goldcopd.org/wp-content/uploads/2021/11/GOLD-REPORT-2022-v1.1-22Nov2021_WMV.pdf.
2. Murray CJ, Atkinson C, Bhalla K, et al. The state of US health, 1990–2010: burden of diseases, injuries, and risk factors. JAMA. 2013;310:591–608. doi:10.1001/jama.2013.13805
3. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582.
4. Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
5. López-Campos JL, Tan W, Soriano JB. Global burden of COPD. Respirology. 2016;21(1):14–23. doi:10.1111/resp.12660
6. Chrystyn H, Mulley BA, Peake MD. Dose response relation to oral theophylline in severe chronic obstructive airways disease. BMJ. 1988;297:1506–1510. doi:10.1136/bmj.297.6662.1506
7. Gross NJ, Petty TL, Friedman M, et al. Dose response to ipratropium as a nebulized solution in patients with chronic obstructive pulmonary disease. A three-center study. Am Rev Respir Dis. 1989;139:1188–1191. doi:10.1164/ajrccm/139.5.1188
8. Ulrik CS. Efficacy of inhaled salmeterol in the management of smokers with chronic obstructive pulmonary disease: a single centre randomised, double blind, placebo controlled, crossover study. Thorax. 1995;50:750–754. doi:10.1136/thx.50.7.750
9. Tashkin DP, Fabbri LM. Long-acting beta-agonists in the management of chronic obstructive pulmonary disease: current and future agents. Respir Res. 2010;11:149. doi:10.1186/1465-9921-11-149
10. Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, randomised controlled trial. Lancet. 2016;388:9. doi:10.1016/S0140-6736(16)31354-X
11. Vogelmeier C, Buhl R, Burghuber O, et al. unter Mitwirkung der folgenden wissenschaftlichen Fachgesellschaften: deutsche Gesellschaft für Arbeitsmedizin und Umweltmedizin e.V.; Deutsche Gesellschaft für Rehabilitationswissenschaften e.V. Leitlinie zur Diagnostik und Therapie von Patienten mit chronisch obstruktiver Bronchitis und Lungenemphysem (COPD) [Guideline for the Diagnosis and Treatment of COPD Patients - Issued by the German Respiratory Society and the German Atemwegsliga in Cooperation with the Austrian Society of Pneumology]. Pneumologie. 2018. 72(4):253–308. German. PMID: 29523017. doi:10.1055/s-0043-125031
12. Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie COPD – teilpublikation der Langfassung, 2. Auflage. Version 1; 2021. [National Health Care Guideline COPD - Partial publication of the long version, 2nd edition. Version 1; 2021]. German.
13. Schurig AM, Bohme M, Just KS, et al. Adverse drug reactions (ADR) and emergencies. Dtsch Arztebl Int. 2018;115(15):251–258.
14. Uppsala Monitoring Centre. The WHO-UMC system. Available from: https://www.who-umc.org/media/2768/standardised-case-causality-assessment.pdf.
15. Just KS, Dormann H, Böhme M, et al. Personalising drug safety – results from the multi-Centre prospective observational study on adverse drug reactions in emergency departments (ADRED). Eur J Clin Pharmacol. 2019;76(3):439–448. doi:10.1007/s00228-019-02797-9
16. Wood K. The medical dictionary for drug regulatory affairs (MEDDRA) project. Pharmacoepidemiol Drug Saf. 1994;3:7–13. doi:10.1002/pds.2630030105
17. Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie COPD – leitlinienreport, 2. Auflage. Version 1; 2021. [National Health Care Guideline COPD - Guideline report, 2nd edition. Version 1; 2021]. German.
18. Vogelmeier C, Buhl R, Burghuber O, et al. Leitlinie zur Diagnostik und Therapie von Patienten mit chronisch obstruktiver Bronchitis und Lungenemphysem (COPD) [Guideline for the diagnosis and treatment of COPD patients - issued by the German Respiratory Society and the German Atemwegsliga in Cooperation with the Austrian Society of Pneumology]. Pneumologie. 2018;72(4):253–308. doi:10.1055/s-0043-125031
19. Prekker ME, Feemster LC, Hough CL, et al. The epidemiology and outcome of prehospital respiratory distress. Acad Emerg Med. 2014;21:543–550. doi:10.1111/acem.12380
20. Kelly AM, Holdgate A, Keijzers G, et al. Epidemiology, prehospital care and outcomes of patients arriving by ambulance with dyspnoea: an observational study. Scand J Trauma Resusc Emerg Med. 2016;24(1):113. doi:10.1186/s13049-016-0305-5
21. Kelly AM, Holdgate A, Keijzers G, et al. Epidemiology, treatment, disposition and outcome of patients with acute exacerbation of COPD presenting to emergency departments in Australia and South East Asia: an AANZDEM study. Respirology. 2018;23(7):681–686. doi:10.1111/resp.13259
22. Hurst JR, Vestbo J, Anzueto A, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. PMID: 20843247. doi:10.1056/NEJMoa0909883
23. Guerrero T, Mayordomo C, Sanchez-Agudo L, Nicolau F, Segu JL. Factors associated with increased risk of exacerbation and hospital admission in a cohort of ambulatory COPD patients: a multiple logistic regression analysis. Respiration. 2000;67(5):495–501. doi:10.1159/000067462
24. Alcazar B, Garcia-Polo C, Herrejon A, et al. Factors associated with hospital admission for exacerbation of chronic obstructive pulmonary disease. Arch Bronconeumol. 2012;48(3):70–76. doi:10.1016/j.arbr.2012.01.001
25. Niewoehner DE, Lokhnygina Y, Rice K, et al. Risk indexes for exacerbations and hospitalizations due to COPD. Chest. 2007;131(1):20–28. doi:10.1378/chest.06-1316
26. Chavez PC, Shokar NK. Diagnosis and management of chronic obstructive pulmonary disease (COPD) in a primary care clinic. COPD. 2009;6(6):446–451. doi:10.3109/15412550903341455
27. López-Campos JL, Quintana Gallego E, Carrasco Hernández L. Status of and strategies for improving adherence to COPD treatment. Int J Chron Obstruct Pulmon Dis. 2019;14:1503–1515. doi:10.2147/COPD.S170848
28. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
29. Wisniewski D, Porzezinska M, Gruchala-Niedoszytko M, Niedoszytko M, Slominski JM, Jassem E. Factors influencing adherence to treatment in COPD patients and its relationship with disease exacerbations. Pneumonol Alergol Pol. 2014;82(2):96–104. doi:10.5603/PiAP.2014.0015
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Obesity Impact on Dyspnea in COPD Patients
Dupuis A, Thierry A, Perotin JM, Ancel J, Dormoy V, Dury S, Deslée G, Launois C
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1695-1706
Published Date: 22 July 2024
Validation and Application of the Simplified Chinese Version of the Dyspnea-12 Questionnaire: An Independent Predictor for Hospitalization Risk in Chronic Obstructive Pulmonary Disease
Chen X, Du L, Xiao W, Liu M, Miao T, Xiong C, Liao L, Li Y, Hu Y, Fu J
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3559-3574
Published Date: 31 October 2025
Revisiting Acute Exacerbations of Chronic Obstructive Pulmonary Disease: Insights from Applying the Rome Proposal in a North American Academic Hospital
Saint-Pierre MD, Neder JA
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:614290
Published Date: 26 May 2026