Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Treatment Patterns, Socioeconomic Status and Clinical Burden in Mild COPD: A Swedish Real-World, Retrospective Cohort Study, the ARCTIC Study
Authors Larsson K ![]() , Lisspers K
, Lisspers K ![]() , Ställberg B
, Ställberg B ![]() , Johansson G, Gutzwiller FS
, Johansson G, Gutzwiller FS ![]() , Mezzi K, Bjerregaard BK, Jorgensen L, Koo H, Janson C
, Mezzi K, Bjerregaard BK, Jorgensen L, Koo H, Janson C ![]()
Received 3 March 2022
Accepted for publication 9 June 2022
Published 21 June 2022 Volume 2022:17 Pages 1409—1421
DOI https://doi.org/10.2147/COPD.S364932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Kjell Larsson,1 Karin Lisspers,2 Björn Ställberg,2 Gunnar Johansson,2 Florian S Gutzwiller,3 Karen Mezzi,3 Bine Kjoeller Bjerregaard,4 Leif Jorgensen,4 Hyewon Koo,5 Christer Janson6
1Integrative Toxicology, The National Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden; 2Department of Public Health and Caring Sciences, Family Medicine and Preventive Medicine, Uppsala University, Uppsala, Sweden; 3Novartis Pharma AG, Basel, Switzerland; 4IQVIA Solutions, Copenhagen, Denmark; 5IQVIA Solutions, Solna, Sweden; 6Department of Medical Sciences: Respiratory, Allergy and Sleep Research, Uppsala University, Uppsala, Sweden
Correspondence: Kjell Larsson, Integrative Toxicology, The National Institute of Environmental Medicine, Karolinska Institutet, Stockholm, SE-171 77, Sweden, Tel +467 0582 0763, Email [email protected]
Background: Patients with mild chronic obstructive pulmonary disease (COPD) account for more than half of the total COPD population but are often undiagnosed and sparsely studied. This real-world, longitudinal study compared the socioeconomic burden, clinical characteristics and treatment patterns in patients with mild COPD and age- and gender-matched controls.
Patients and methods: Our population included mild COPD patients (forced expiratory volume in one second ≥ 80% of predicted value) and reference controls from 52 Swedish primary care centres over 15 years (2000– 2014). We linked electronic medical record (EMR) data to Sweden’s National Health Registries. The outcomes analyzed were socioeconomic status including annual income from work, presence of comorbidities and the use of medications.
Results: 844 patients with mild COPD were included in this study and matched with 844 reference controls. Compared with the reference controls, mild COPD patients had a significantly lower annual income from work (mean difference, men: 12,559€ and women: 7143€) and were significantly less likely to be married or employed. The presence of comorbidities, including cardiovascular disease, anxiety and depression (only women) was significantly higher in mild COPD patients. The use of medications, such as proton pump inhibitors, antidepressants, central painkillers and sleep medications, was significantly higher in the mild COPD group.
Conclusion: Mild COPD presents a considerable socioeconomic and clinical burden compared with reference controls The findings suggest that COPD constitutes a condition that influences health status even in mild disease clearly demanding an increased need for early detection and treatment.
Keywords: chronic obstructive pulmonary disease, socioeconomic status, comorbidities, co-medications, annual income, exacerbation, Sweden
Background
Chronic obstructive pulmonary disease (COPD) is a progressive disorder characterized by chronic airflow limitation and persistent respiratory symptoms including breathing difficulties, shortness of breath and wheezing, chronic cough, sputum production, reduced exercise capacity and poor quality of life.1 It is a major cause of chronic morbidity and the third leading cause of death worldwide. However, due to multiple reasons, COPD remains underdiagnosed, misdiagnosed or diagnosed too late, preventing patients from receiving optimal treatment early. In Sweden, COPD diagnosis is often missed due to low awareness of COPD among physicians and focus on other diagnostic concomitant conditions.2 Another reason of COPD underdiagnosis might be attributed to the fact that many patients with chronic airflow limitation are conscious of symptoms for a number of years before seeking medical help.1,3 Given the progressive nature of COPD, early diagnosis and treatment may be beneficial for reducing the disease burden for patients and healthcare systems. In a previous study, more than half of the individuals with chronic airflow limitation had mild COPD.4
Little research has been done on mild COPD, as patients with preserved lung function (forced expiratory volume in one second [FEV1] ≥80% of predicted value) do not often seek medical care and are generally excluded from clinical studies.5,6 In a literature review, it was suggested that mild COPD patients are at a high risk of disease progression leading to substantial disease burden. Hence, identifying these patients offers the opportunity to determine the most appropriate patients who could benefit from early treatment resulting in improved health outcomes.7 Previous studies on COPD have mainly focused on severe and moderate disease, whereas less is known about disease burden and costs for COPD patients with mild disease. Therefore, there is a need for increased knowledge about the socioeconomic consequences and the impact of mild COPD on health status and to what extent these patients are undertreated. This study aimed to compare socioeconomic status, clinical characteristics, and treatment patterns in patients with mild COPD with age- and gender-matched controls without COPD from the same primary care centres.
Methods
Study Design
ARCTIC is a large, real-world, retrospective Swedish cohort study of 18,586 eligible, primary care, COPD patients.8–12 It was conducted in accordance with the principles of the Declaration of Helsinki. Ethics approval was obtained from the local Ethical Regional Board in Uppsala, Sweden, on 11 December 2014 (number: 2014–397), to access the National Health Register and recruit primary care centres for the study. An amendment specifying additional analysis was approved by the Ethical Regional Board in Uppsala on 6 October 2017. All records were de-identified and, therefore, the Ethics committee did not require patient consent.
Electronic medical record (EMR) data were collected for all eligible patients at 52 primary care centres across Sweden between the years 2000 and 2014 using an established software system (Customized eXtraction Program, CXP 3.0). Data included age, gender, prescriptions (classified by the World Health Organization Anatomical Therapeutic Chemical [ATC] codes), clinical diagnoses (coded using the International Classification of Diseases, 10th Revision [ICD-10]), spirometry measurements, laboratory tests, healthcare professional visits and referrals. Participating centres covered urban and rural areas of varying sizes across Sweden. These EMR data were linked to National Health Register data sources by the Swedish National Board of Health and Welfare using unique patient identification (ID) numbers. Patient IDs were pseudonymised. The registry data sources included: (i) the Longitudinal Integration Database for Health Insurance and Labour Market Studies (LISA),10 which provided socio-demographic data, including educational level, marital status and family situation, occupational status, retirement and economic compensation, and social benefits; (ii) the National Patient Register,13 which contains data related to diagnosis (ICD-10 codes and associated positions) from secondary care, including gender, age, region, hospital visits, specialty visits, inpatient stays as well as all medical procedures and surgeries performed, regardless of clinical setting; (iii) the National Prescription Register (2005–2014),13 which tracks comprehensive information for all medications dispensed from pharmacies (ATC codes), including brand name, prescription date, dose, strength, pack size, prescriber specialty and prescription costs; and (iv) the Cause of Death Register,13 which stores data including sex, date of death and cause of death.
Study Patients
The study population consisted of all patients aged ≥40 years who had an ICD-10 diagnosis of COPD (ICD-10: J44) in either a primary care (EMR database) or hospital setting (National Patient Register) between 1 January 2002 and 31 December 2012. The study index date corresponded to the date of the first recorded physician’s diagnosis of COPD during the enrolment time frame. Patients were included if diagnosed with mild COPD (post-bronchodilator FEV1 ≥80% of predicted value) based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria.1 Patients with FEV1 <80% of predicted value and those with a concomitant diagnosis of asthma (ICD-10: J45/J46) at index date (date of COPD diagnosis) were excluded from the study. Lung function was used to assess the degree of airflow limitation based on data collected from spirometry and recorded in the EMRs. Comorbidities were defined by recorded ICD-10 diagnoses from the study index date.
An age- and gender-matched reference population was included among patients selected from the same primary care centres, excluding those who had a diagnosis of COPD and/or asthma. A random date between the start and end of the observation period was selected as the index date for the reference population. In the COPD group age at index was calculated by the difference in days between the date of birth and date of diagnosis of COPD. Afterwards, a reference patient having the closest age at index date to the age at index date of a mild COPD patient was selected. If there were multiple reference patients satisfying the criteria, one was randomly selected among these candidates. Patients without FEV1 values, socioeconomic information, and who died or were lost to follow-up were excluded from the analysis.
Outcomes
The primary objective of this analysis was to assess the annual income from work among the mild COPD cohort compared with an age- and gender-matched reference population. Annual income (€) was extracted and stratified by gender. As the income reported was from work, only non-retired patients at that particular time point in the follow-up period were included for the analysis.
The secondary objective was to assess the socioeconomic status, comorbidities and the use of medications for non-respiratory conditions among mild COPD patients compared with the reference population. In addition to annual income from work (primary objective), socioeconomic status included employment status, marital status, any absenteeism due to sickness, sickness benefit, number of inpatient visits, number of outpatient clinic visits, length of hospitalization and the number of primary care visits.
All results are presented graphically for men and women, separately. If multiple FEV1 values were recorded for a patient during the year, then the lowest FEV1 value was chosen for that particular year. For example, if a patient was registered as both mild COPD and non-mild COPD in the same year, that patient was categorised as non-mild. As FEV1 values were not recorded for each year of follow-up, certain rules were created to assign an FEV1 value for each patient from baseline through the entire follow-up period. If a patient was categorised with mild COPD at a particular year during follow-up, then this severity level was carried five years forward and five years backwards, only if there was no overwriting of existing severity. If a patient was categorised as non-mild COPD at a particular year during follow-up, then this severity level was only carried five years forward if there was no overwriting of existing severity. After applying the above rules, years with no assigned severity level were left as severity missing.
‘Moderate exacerbations’ were defined as treatment with oral corticosteroids (H02AB) or antibiotics (J01AA, J01CA) or both (but no hospitalization). ‘Severe exacerbations’ were defined as COPD-related hospitalizations (J44 in the primary position or J44.0/J44.1 in a secondary position) or emergency visits (J44.0/J44.1 in outpatient hospital care). Recurrent exacerbations occurring within 14 days were considered as one unique event.
Statistical Analysis
In the original ARCTIC publication, approximately 18,000 COPD patients were compared with more than 84,000 subjects in the reference population.10 This large sample size allowed for a valid analysis of our defined subpopulations. The statistical analysis software used for this analysis was SAS version 9.4 (SAS Institute, Cary, NC). Baseline was defined as two years prior to the index date. Patient demographics at baseline were described for both mild COPD patients and the reference population. Continuous variables at baseline were compared between mild COPD patients and the reference group using analysis of covariance. Categorical variables at baseline were compared between mild COPD patients and subjects in the reference group using a chi-square test, and the proportions (gender, body mass index [BMI], smoking, education levels, employment status, marital status, any absenteeism due to sickness (yes/no), presence of individual comorbidities) in both populations were analyzed.
For our primary objective, median income levels for both the mild COPD and reference populations were calculated and stratified by gender. The secondary objective used generalized estimating equations (GEE) to estimate the regression parameters in the marginal model. GEE models with binary distribution and logit link function were used for comparative analyses of binary variables of socioeconomic status, healthcare utilization, comorbidities and co-medications. For each GEE model, the predictor variable was the “group” (mild COPD vs reference population). GEE model results were stratified by gender.
Results
Of the 202,397 patients identified from EMRs, FEV1 values were available for 5883 COPD patients, of which 844 patients with mild COPD at index date and 844 age- and gender-matched reference controls were included in this study (Figure 1). Patient demographics and socioeconomic status of the mild COPD patients and the reference population are summarized in Tables 1 and 2, respectively.
 |
Table 1 Patient Demographics of the Mild COPD and Reference Groups |
 | 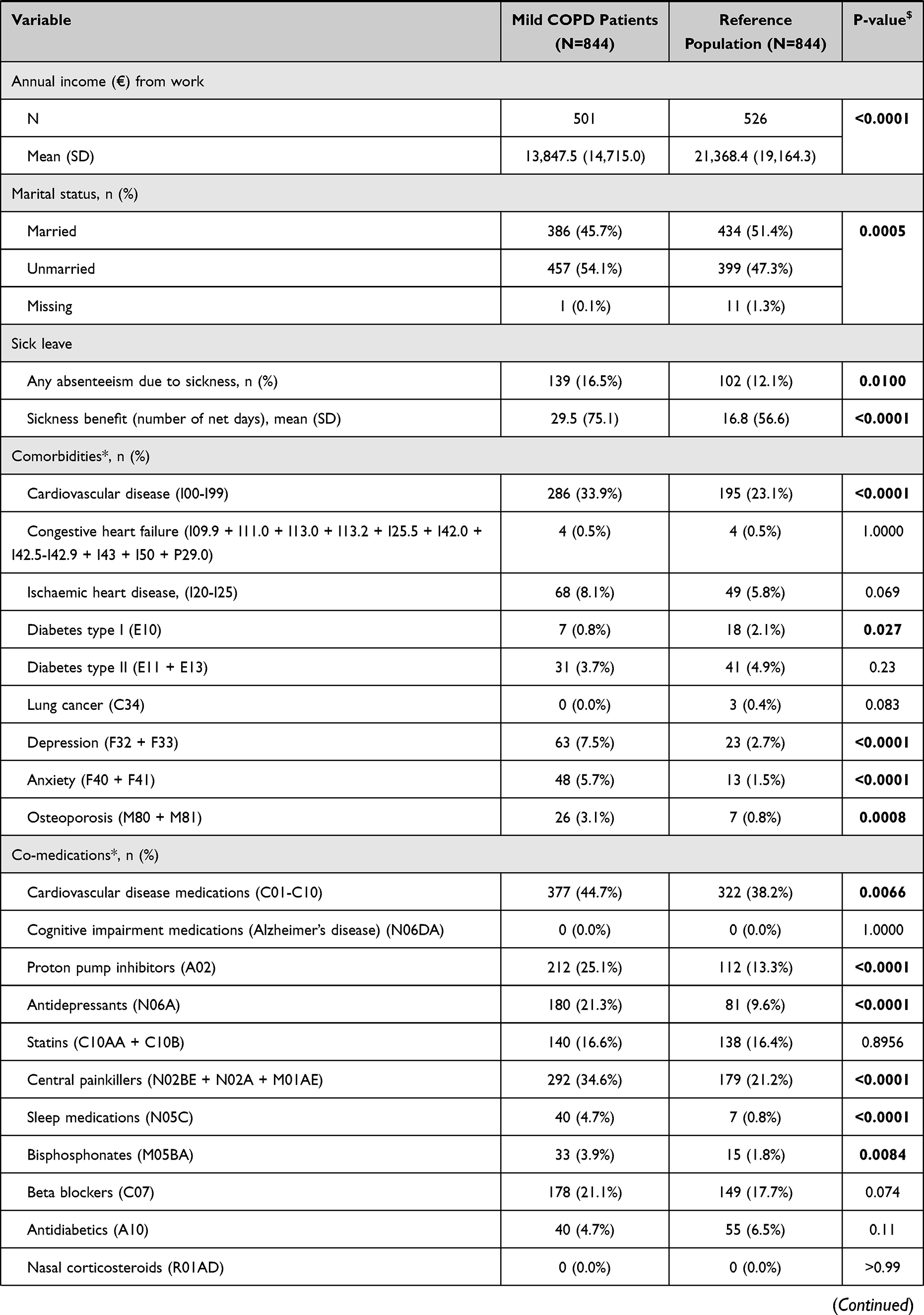 |  |
Table 2 Socioeconomic Status of the Mild COPD and Reference Groups |
 |
Figure 1 Flowchart of patient inclusion and exclusion criteria. |
Baseline Assessments
In the mild COPD group, 28.4% of patients were overweight or obese and 1.5% were underweight. Data on BMI and smoking status were missing for most patients in the reference group, which precluded comparisons between groups.
Relative to socioeconomic status, unemployment and mean days on sickness benefit were significantly higher in the mild COPD group than in the reference controls. A high proportion of mild COPD patients had less than nine years of elementary school education. There was also a significant difference in marital status with more unmarried patients among the COPD population than in the controls.
The proportion of patients with various comorbidities and the use of medications for conditions other than COPD was higher in the COPD group than in the control group. Although they had a lower number of outpatient clinic visits, COPD patients had a higher number of primary care visits compared with subjects in the control group.
Characteristics of Patients with Mild COPD
Lung function values were recorded either before, at, or after the index date for patients with mild COPD. The closest value to the index date is given in Table 3. During the follow-up period, the mean annual moderate exacerbation rate was 0.64 in patients with mild COPD, but 0.0% patients experienced severe exacerbation. The use of long-acting beta-agonists, long-acting antimuscarinics and short-acting beta-agonists was reported in approximately 46%, 40% and 48% of mild COPD patients, respectively. The combination of inhaled corticosteroids and long-acting beta-agonists was used by 34% of patients (Table 3).
 |
Table 3 Post-Bronchodilator Lung Function, Exacerbations and Respiratory Medications in Patients with Mild COPD |
Follow-Up Assessments
The mean length of follow-up was 6.9 ± 3.2 and 6.3 ± 3.3 years (p=0.0009) in the mild COPD and reference populations, respectively.
Socioeconomic Status
The annual income (primary objective) from work was lower in mild COPD patients compared with the reference population irrespective of gender (Figure 2). On average, patients with mild COPD had a lower annual income from work (mean difference, men: 12,559 €, p=0.0001 and women: 7143€, p<0.0001) than subjects in the reference group.
 |
Figure 2 Annual income from work, in Euros. |
Overall, socioeconomic status was lower in mild COPD patients compared with the reference population irrespective of gender. Compared with the reference population, mild COPD patients were significantly less likely to be married or employed. These patients were significantly more likely to have sick days and absenteeism due to sickness (Table 4).
 |
Table 4 Comparative Analysis Between Mild COPD Patients vs the Reference Population Over Time Stratified by Gender |
Comorbidities
The likelihood of having comorbidities, specifically cardiovascular disease and anxiety, was significantly higher in patients with mild COPD compared with the reference population. For congestive heart failure, ischaemic heart disease, diabetes mellitus (both type I and II) and lung cancer, no significant differences were observed between the mild COPD group and the reference group irrespective of gender. The likelihood of having depression was significantly higher in women with mild COPD; however, no significant differences were observed in men with mild COPD compared with those in the reference group (Table 4).
Co-Medications
The likelihood of using co-medications, such as proton pump inhibitors, antidepressants, central painkillers and sleep medications, was significantly higher in the mild COPD group for both men and women compared with their reference controls (Table 4).
Healthcare Resource Utilization
Compared with that in the reference group, the number of primary care visits was significantly higher in women with mild COPD (Table 4). The number of outpatient visits were very rare in both groups to conduct any meaningful comparisons.
Discussion
The present study clearly highlighted that patients with mild COPD, ie patients who have normal FEV1 (≥80% of predicted value), are worse off both in socioeconomic and medical outcomes when compared with age-and gender-matched controls without COPD or asthma from the same healthcare centres. The findings are interesting considering patients with mild COPD have normal lung function as assessed based on FEV1. Usually these patients do not seek medical care until the disease has progressed to an advanced stage. The delay in seeking medical care results in delayed diagnosis of COPD, a statement that is corroborated by other studies.2,14 Prior results of the ARCTIC study demonstrate that late COPD diagnosis is associated with a higher exacerbation rate, increased comorbidities and higher costs compared with early diagnosis.9 Our results demonstrated a lower socioeconomic status, including annual income from work and a higher prevalence of both comorbidities and co-medications in patients with mild COPD, when compared with the matched controls.
It is known that low socioeconomic status, irrespective of other risk factors, is associated with a higher prevalence of COPD;15,16 however, it is unknown if this is the case only for individuals with more advanced disease or if it also occurs in mild COPD. It is intriguing that our study suggests a clear association between low socioeconomic status and mild COPD. The lower annual income of patients with mild COPD compared with the controls might be associated with a higher unemployment rate and more absenteeism due to sickness.
Our study clearly showed that many patients with mild COPD use drugs for their respiratory condition and that they experience moderate, but not severe, exacerbations. These results are consistent with previous results showing that COPD exacerbations also occur in patients with preserved lung function, who are thus regarded as having mild COPD.17 A considerable number of studies have demonstrated that exacerbations contribute to higher utilization of healthcare services, imposing a financial burden on the healthcare system.11,18 Patients with mild COPD also likely contribute to this burden as reported in this study. We found that one out of three patients with mild COPD experienced moderate exacerbations.
Previous studies have reported that the prevalence of comorbidities in patients with COPD is higher compared with control subjects without COPD.12,19 Earlier studies also demonstrate that comorbidities are associated with increased levels of unemployment and more time off from work among COPD patients compared with those without the disease.20,21 In a previous ARCTIC study, it was shown that healthcare costs in COPD are driven by healthcare utilization due to comorbidities.11 Our results suggest similar trends for mild COPD. There was a higher prevalence of cardiovascular diseases and depression/anxiety in the mild COPD group compared with the controls both at the index date and during follow-up. Hence, the difference in daily life, social status and healthcare utilization between our two cohorts may not only be explained by mild COPD but also by the increased prevalence of cardiovascular disease, depression and anxiety. Additionally, the increased use of co-medications among mild COPD patients is associated with a significant economic burden, as increased medication use is a key contributor for higher direct costs of COPD.11
The healthcare utilization with respect to primary care visits was higher (significant only in women) in patients with mild COPD compared with the control population. This result supports the findings from the previous studies.12,22 A few outliers in the reference population (3 patients with more than 100 visits) resulted in a significantly higher number of outpatient clinic visits in the reference group compared to the mild COPD patients. It is interesting to note that heart failure, ischaemic heart disease, lung cancer and diabetes (ie conditions that previously have been shown to co-variate with COPD)12,23 were not overrepresented in patients with mild COPD during follow-up. Thus, these important comorbid conditions in moderate and severe COPD do not appear to contribute much to the impaired socioeconomic and medical outcomes observed in mild COPD.
It is known that patients with GOLD COPD stage 1 (FEV1 ≥80% predicted) are less physically active than subjects in a matched control group.24 The lower level of physical activity in COPD patients is not only a marker of advanced disease but also has been found to start decreasing in the early stages and to be more strongly associated with comorbid conditions than lung function.25,26 Impaired levels of physical activity lead to adverse clinical outcomes including hospitalization and all-cause mortality.27 This suggests that increasing activity levels is crucial for the effective disease management of COPD patients across all severities, including mild disease. Despite this knowledge, physical activity for mild COPD patients has not yet been emphasised in current guidelines. The current Swedish guidelines (Swedish Medical Agency 2015)28 recommend physical training with a physiotherapist only for COPD patients with FEV1 <80% predicted value.
In agreement with previous analyses,9 our findings also emphasise the need to identify COPD patients as early as possible in primary care by carefully assessing the presence of airway symptoms, documenting any history of harmful exposure and performing lung function measurements. Our conclusions are in an agreement with a recently published study that emphasises both the lack of and the need for more studies specifically for early (disease which is near its onset) and mild COPD (disease associated with mild airflow limitation).29
The present study has several strengths. The primary care setting and the real-world study design adequately reflect the general population and clinical practice in Sweden. Additionally, we were able to validly perform a comprehensive, longitudinal (2000–2014) assessment on a range of outcomes generated from a robust data source and explore gender differences between mild COPD patients and non-COPD subjects. Data quantification in this study can allow clinical decision-makers to identify the burden associated with mild COPD, which may serve as a basis for the development of treatment strategies to achieve better outcomes in the millions of patients with mild COPD globally.
Nevertheless, this study also has certain limitations. As a retrospective study, the potential for bias and confounding factors cannot be excluded. As patients with missing FEV1 values were excluded from the study group, this might have led to exclusion of the patients with very mild COPD who have a good lung function and do not need to have their FEV1 values measured. The use of medications was based on prescription claims which may not accurately reflect the patients’ actual adherence to treatment. Moreover, this study enrolled only Swedish patients. It is, therefore, uncertain whether these findings can be extrapolated to a more diverse group of patients and to healthcare systems in other countries. In line with the objective and scope of this study, the present analyses focused on only mild COPD patients and other respiratory conditions were not assessed.
Conclusions
In conclusion, the present study highlighted that mild COPD presents a considerable socioeconomic and clinical burden compared with age- and gender-matched patients visiting healthcare centres for reasons other than COPD. We found that a substantial number of patients with mild COPD experience moderate exacerbations and an increased prevalence of cardiovascular disease, depression and anxiety. It is likely that the poor socioeconomic and medical outcomes in patients with mild COPD are caused both by mild COPD and comorbidities. The findings clearly show that COPD constitutes a condition that influences health status even at an early stage. As such, mild COPD clearly demands greater primary and secondary prevention and a need to increase early detection.
Abbreviations
ATC, Anatomical Therapeutic Chemical; BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; EMR, electronic medical record; FEV1, forced expiratory volume in one second; GEE, generalized estimating equations; GOLD, Global Initiative for Chronic Obstructive Lung Disease; LISA, Longitudinal Integration Database for Health Insurance and Labour Market Studies; SD, standard deviation.
Data Sharing Statement
The data for this study were obtained from primary care electronic medical records and the Swedish National Health Register. Restrictions apply to the availability of these data, which were used under licence for the current study, and are, therefore, not publicly available. Data are however available from IQVIA Solutions, Solna, Sweden, upon reasonable request and with the permission of the Swedish National Health Register.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the principles of the Declaration of Helsinki. Ethics approval was obtained from the local Ethical Regional Board in Uppsala, Sweden, on 11 December 2014 (number: 2014-397).
Acknowledgments
The authors would like to thank Harneet Kaur (Novartis) for managing and providing writing assistance in the development of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Novartis Pharma AG, Basel, Switzerland.
Disclosure
KLa has, during the last 5 years, on one or more occasions, served on an advisory board, served as a speaker, and/or participated in education activities arranged by AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Takeda, Novartis, Chiesi, Orion and Teva. CJ reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis and Teva, outside the submitted work. KLi reports personal fees from AstraZeneca, Novartis, Boehringer Ingelheim, GlaxoSmithKline and Chiesi, outside the submitted work. BS reports personal fees from AstraZeneca, Novartis, Boehringer Ingelheim, GlaxoSmithKline, Meda, Teva and Chiesi, outside the submitted work. GJ has participated on the steering committee organised by Novartis for this study and served on advisory boards arranged by AstraZeneca, Novo Nordisk and Takeda. FSG and KM are employees of Novartis Pharma AG. BKB, LJ and HK are employees of IQVIA and received remuneration in relation to statistical analyses. The authors report no other conflicts of interest in this work.
References
1. Global strategy for the diagnosis M, and prevention of chronic obstructive pulmonary disease, global initiative for chronic obstructive lung disease 2021 report. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
2. Sundblad BM, Larsson K, Nathell L. Low awareness of COPD among physicians. Clin Respir J. 2008;2(1):11–16. doi:10.1111/j.1752-699X.2007.00020.x
3. Welte T, Vogelmeier C, Papi A. COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract. 2015;69(3):336–349. doi:10.1111/ijcp.12522
4. Lindberg A, Bjerg A, Ronmark E, Larsson LG, Lundback B. Prevalence and underdiagnosis of COPD by disease severity and the attributable fraction of smoking Report from the Obstructive Lung Disease in Northern Sweden Studies. Respir Med. 2006;100(2):264–272. doi:10.1016/j.rmed.2005.04.029
5. Barrecheguren M, Gonzalez C, Miravitlles M. What have we learned from observational studies and clinical trials of mild to moderate COPD? Respir Res. 2018;19(1):177. doi:10.1186/s12931-018-0882-0
6. Kruis AL, Stallberg B, Jones RC, et al. Primary care COPD patients compared with large pharmaceutically-sponsored COPD studies: an UNLOCK validation study. PLoS One. 2014;9(3):e90145. doi:10.1371/journal.pone.0090145
7. Singh D, D’Urzo AD, Donohue JF, Kerwin EM. Weighing the evidence for pharmacological treatment interventions in mild COPD; a narrative perspective. Respir Res. 2019;20(1):141. doi:10.1186/s12931-019-1108-9
8. Janson C, Johansson G, Stallberg B, et al. Identifying the associated risks of pneumonia in COPD patients: arctic an observational study. Respir Res. 2018;19(1):172. doi:10.1186/s12931-018-0868-y
9. Larsson K, Janson C, Stallberg B, et al. Impact of COPD diagnosis timing on clinical and economic outcomes: the Arctic observational cohort study. Int J Chron Obstruct Pulmon Dis. 2019;14:995–1008. doi:10.2147/COPD.S195382
10. Lisspers K, Larsson K, Janson C, et al. Gender differences among Swedish COPD patients: results from the Arctic, a real-world retrospective cohort study. NPJ Prim Care Respir Med. 2019;29(1):45. doi:10.1038/s41533-019-0157-3
11. Lisspers K, Larsson K, Johansson G, et al. Economic burden of COPD in a Swedish cohort: the Arctic study. Int J Chron Obstruct Pulmon Dis. 2018;13:275–285. doi:10.2147/COPD.S149633
12. Stallberg B, Janson C, Larsson K, et al. Real-world retrospective cohort study Arctic shows burden of comorbidities in Swedish COPD versus non-COPD patients. NPJ Prim Care Respir Med. 2018;28(1):33. doi:10.1038/s41533-018-0101-y
13. Socialstyrelsen; 2017. Available from: http://www.socialstyrelsen.se/register.
14. Lamprecht B, Soriano JB, Studnicka M, et al. Determinants of underdiagnosis of COPD in national and international surveys. Chest. 2015;148(4):971–985. doi:10.1378/chest.14-2535
15. Cai L, Wang XM, Fan LM, Shen JR, Liu YN, Golden AR. Socioeconomic variations in chronic obstructive pulmonary disease prevalence, diagnosis, and treatment in rural Southwest China. BMC Public Health. 2020;20(1):536. doi:10.1186/s12889-020-08687-5
16. Sahni S, Talwar A, Khanijo S, Talwar A. Socioeconomic status and its relationship to chronic respiratory disease. Adv Respir Med. 2017;85(2):97–108. doi:10.5603/ARM.2017.0016
17. Hurst JR, Vestbo J, Anzueto A, et al. Evaluation of CLtIPSEI. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
18. Larsson K, Janson C, Lisspers K, et al. The impact of exacerbation frequency on clinical and economic outcomes in Swedish COPD patients: the Arctic study. Int J Chron Obstruct Pulmon Dis. 2021;16:701–713. doi:10.2147/COPD.S297943
19. Greulich T, Weist BJD, Koczulla AR, et al. Prevalence of comorbidities in COPD patients by disease severity in a German population. Respir Med. 2017;132:132–138. doi:10.1016/j.rmed.2017.10.007
20. Gronseth R, Erdal M, Tan WC, et al. Research teams at c. Unemployment in chronic airflow obstruction around the world: results from the BOLD study. Eur Respir J. 2017;50(3):1700499. doi:10.1183/13993003.00499-2017
21. Rai KK, Adab P, Ayres JG, Jordan RE. Systematic review: chronic obstructive pulmonary disease and work-related outcomes. Occup Med. 2018;68(2):99–108. doi:10.1093/occmed/kqy012
22. Schwab P, Dhamane AD, Hopson SD, et al. Impact of comorbid conditions in COPD patients on health care resource utilization and costs in a predominantly Medicare population. Int J Chron Obstruct Pulmon Dis. 2017;12:735–744. doi:10.2147/COPD.S112256
23. Stallberg B, Janson C, Johansson G, et al. Management, morbidity and mortality of COPD during an 11-year period: an observational retrospective epidemiological register study in Sweden (PATHOS). Prim Care Respir J. 2014;23(1):38–45. doi:10.4104/pcrj.2013.00106
24. Troosters T, Sciurba F, Battaglia S, et al. Physical inactivity in patients with COPD, a controlled multi-center pilot-study. Respir Med. 2010;104(7):1005–1011. doi:10.1016/j.rmed.2010.01.012
25. Van Remoortel H, Hornikx M, Demeyer H, et al. Daily physical activity in subjects with newly diagnosed COPD. Thorax. 2013;68(10):962–963. doi:10.1136/thoraxjnl-2013-203534
26. Van Remoortel H, Hornikx M, Langer D, et al. Risk factors and comorbidities in the preclinical stages of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;189(1):30–38. doi:10.1164/rccm.201307-1240OC
27. Shin KC. Physical activity in chronic obstructive pulmonary disease: clinical impact and risk factors. Korean J Intern Med. 2018;33(1):75–77. doi:10.3904/kjim.2017.387
28. Läkemedelsverket Medical Products Agency (Sweden). Läkemedelverkets expert panel. Farmakologisk behandling av kroniskt obstruktiv lungsjukdom (KOL) - behandlingsrekommendationer; 2015. Available from: https://www.lakemedelsverket.se/sv/.
29. Martinez FJ, Agusti A, Celli BR, et al. Treatment trials in young patients with COPD and pre-COPD patients: time to move forward. Am J Respir Crit Care Med. 2021;205:275–287.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optimal Management of Heart Failure and Chronic Obstructive Pulmonary Disease: Clinical Challenges
Cuthbert JJ, Pellicori P, Clark AL
International Journal of General Medicine 2022, 15:7961-7975
Published Date: 25 October 2022
A Prediction Scoring Model for the Effect of Withdrawal or Addition of Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease
Lee JH, Kim S, Oh YM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:113-127
Published Date: 15 February 2023
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023
Real-World Disease Burden and Healthcare Resource Utilization Among Patients with COPD and Asthma Using Triple Therapy (FF/UMEC/VI) in the United States
Igboekwe E, Verma S, Paczkowski R
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:281-296
Published Date: 25 January 2024
Dynamic Risk Status of OSA and Its Association with COPD Incidence and Progression to Oxygen Therapy: Insights from a US National Cohort

Wang Y, Luo J, Huang R, Xiao Y
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:753-766
Published Date: 21 March 2025