Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Update on Erythrodermic Psoriasis: Proposal of a Management Algorithm by an Innovative Severity Evaluation Approach
Authors Xu JM ![]() , Wu C, Feng H, Jin HZ
, Wu C, Feng H, Jin HZ
Received 2 April 2025
Accepted for publication 8 July 2025
Published 19 July 2025 Volume 2025:15 Pages 301—320
DOI https://doi.org/10.2147/PTT.S532062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Enzo Errichetti
Jia-Ming Xu,* Chao Wu,* Hao Feng, Hong-Zhong Jin
Department of Dermatology, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, National Clinical Research Center for Dermatologic and Immunologic Diseases, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong-Zhong Jin, Email [email protected]
Abstract: Erythrodermic psoriasis (EP) is an uncommon and severe form of psoriasis, which exhibits a Th1/Th17/TNF inflammatory pattern. Most patients with EP experience systemic symptoms that necessitate systemic treatments. These treatments include conventional systemic drugs (such as acitretin, cyclosporin A, and methotrexate), biologics (including IL-17, IL-12/23, and TNF-α inhibitors), and small molecule drugs (such as apremilast and JAK inhibitors). Evaluating the severity of EP is critical for determining appropriate treatment strategies. According to an innovative EP severity evaluation approach, patients exhibiting two or more clinical features—fever, exudation, or lymphadenopathy—are classified as having moderate-to-severe EP, while those with one or none of these symptoms are categorized as having mild EP. Mild EP can often be managed with monotherapy using acitretin, methotrexate, or biologics, such as IL-17 or IL-12/23 inhibitors, excluding TNF-α inhibitors. For moderate-to-severe EP, cyclosporine A and biologics, particularly IL-17 or IL-12/23 inhibitors, are recommended. Combination therapies are considered when monotherapies prove ineffective. These may involve combining a biologic with a conventional systemic drug or using two to three conventional systemic drugs together to enhance efficacy. Supportive care plays a critical role in alleviating the discomfort associated with skin lesions and other complications. Additionally, treatments should be tailored to address specific comorbidities, often requiring multidisciplinary collaboration. In our comprehensive review, we summarized the current evidence on therapeutic options for EP, including details on dosages, treatment durations, efficacy, and adverse events. Additionally, we incorporated new evidence on the use of acitretin, biologics, and JAK inhibitors for EP. We also introduced, for the first time, a practical management algorithm based on severity evaluation to guide the appropriate treatment of EP.
Keywords: erythrodermic psoriasis, treatment, conventional systemic drugs, biologics, small molecule drugs
Introduction
Erythrodermic psoriasis (EP) is a severe variant of psoriasis, characterized by generalized erythema and scaling throughout the body. Previous studies suggested two clinical subtypes of EP: one was gradually developed from the primary plaque lesions of psoriasis vulgaris, and the patients had a relatively stable disease condition and less systemic symptoms (Figure 1A–D); the other was rapidly developed from previous normal skin or lesions of severe plaque psoriasis or generalized pustular psoriasis (GPP), and patients tended to have severe systemic symptoms or abnormal laboratory test results (Figure 2A–D).1,2 The definition of the diffuse erythema in EP differs among countries. Some dermatologists adopt a 75% or 80% percent of body surface area (BSA) of skin lesions in the diagnosis of EP, while the most commonly used criterium is 90% BSA.2,3 The prevalence of EP among psoriatic patients varies among different countries and racial groups, ranging from 1% to 6.1% worldwide.1,4 The difference in diagnostic criteria of BSA might influence the prevalence of EP among countries because patients with severe plaque psoriasis whose BSA >75% might be occasionally categorized as EP according to the aforementioned criterium.
 |
Figure 1 The clinical subtype of EP developed from previous lesions of plaque psoriasis. The photos were taken from 4 EP patients with previous plaque psoriasis and without systemic symptoms. (A) 41-year old male. (B) 55-year old male. (C) 53-year old male. (D) 38-year old male. |
 |
Figure 2 The clinical subtype of EP rapidly developed from previous normal skin or severe psoriasis lesions. The photos were taken from a 45-year old male patient with an 11-year history of plaque psoriasis, which progressed to EP over 2 months. The patient experienced hyperthermia, lower extremity edema, exudation, electrolyte imbalance, and hypoalbuminemia. (A and B) Severe swelling of hands and left foot. (C and D) Diffuse erythema and scaling on the trunk and upper limbs. |
The development of EP can result from exacerbation of previous psoriatic lesions, but it can also grow spontaneously with certain triggering factors. Various triggering factors were suggested to induce EP development in previous studies, with the most reported being medications.1 Various systemic agents were reported to induce EP, including antihypertensive drugs (β-blockers, enalapril), biologics (tremelimumab, durvalumab, rituximab, adalimumab, and efalizumab), antibiotics (trimethoprim-sulfamethoxazole), antiviral drugs (sofosbuvir and daclatasvir), bupropion, COVID-19 vaccination, and iodine-containing radiographic contrast media.5–16 The exacerbation of plaque psoriasis to EP is sometimes observed during withdrawal of systemic treatments, such as systemic corticosteroids and immunosuppressants (eg, cyclosporin).17–19 Systemic infections, incluing β hemolytic streptococcus, COVID-19 virus, and HIV, can also induce the development of EP.20–22 Rarely, the abrupt appearance of EP might suggest an underlying malignancy, such as B-cell chronic lymphocytic leukemia.23 As an immune-mediated disease, previous studies had indicated that the interleukin (IL)-17 signaling pathway dominated in the inflammatory responses of EP, with an increase level of serum IgE, a Th2 cell pattern, an increase in vascular formation, and an overexpression of intercellular adhesion molecules.24–27 Compared to psoriasis vulgaris, the vascular endothelial cells in EP patients upregulated gene expressions relative to angiogenesis, leukocyte adhesion and antigen presentation.28 A previous proteomics study also revealed that the serum of EP patients exhibited a Th1/Th17/TNF inflammatory pattern with mild Th2 upregulation, along with significant increases in epidermal-development markers. Among the cellular markers, the Th17 markers strongly associated with disease severity in EP.29 Several genes were also suggested to associate with EP pedigrees, such as HLA-Cw1, CARD14, and TNF-308 G/A genotypes.30–32 Through metabolomics analysis, a lower serum level of L-tryptophan was observed in EP than psoriasis vulgaris, which was also negatively associated with the PASI scores. The amino acid and glycerophospholipid metabolism were also dysregulated in EP.33 However, the exact pathogenesis of EP, as well as its difference from psoriasis vulgaris, requires more elucidation, and the potential causes of two EP subtypes might differ.
Apart from the severe skin manifestations, the systemic involvement of EP are also evident. The laboratory examinations had showed a higher total white blood cell (WBC), neutrophil, and platelet counts, but lower hemoglobin levels in EP patients than healthy controls, which suggested a high systemic inflammatory state in EP patients.34 Retrospective studies had reported various systemic comorbidities in EP patients, including hypertension, dyslipidemia, diabetes mellitus, thyroid dysfunction, and depression.35,36 More severe comorbidities, such as acute respiratory distress syndrome (ARDS), nephrotic syndrome, were also reported in individual cases.37,38 The severe skin manifestations and the involvement of multiple organs significantly increase the difficulty of EP treatment. Various complications have been reported during the treatment of EP, including infection, electrolyte imbalance, multiple organ failure, even death.39,40 The severe complications further complicate the management of EP. Compared to patients with psoriasis vulgaris, patients with EP tend to have longer hospital length of stay and higher mortality.41,42 Therefore, the disease burden of EP is substantial, appealing for better management of EP. In 2010, the National Psoriasis Foundation had established a consensus for therapeutic options of EP.3 However, the consensus was based on few high-quality studies, and it also lacked the data of the newly emerging biologics and other targeted agents. This narrative review elaborates on the therapeutic options and adds the latest developed drugs for EP. We aimed to compare different therapies’ effectiveness and adverse events and propose our recommendations for EP treatment from evidence-based medicine and real-world clinical practices.
Evaluation of EP Severity
The severity of EP is usually assessed using BSA and the Psoriasis Area and Severity Index (PASI) that describe the overall condition of the skin lesions, especially in treatment-related individual cases or clinical trials.43,44 However, for patients with the more acute subtype of EP, it is insufficient to evaluate the disease severity based merely on their skin manifestations, because their systemic involvement might be more serious and even life-threatening. Therefore, the evaluation of systemic involvement of EP might assist in the stratification of EP. Ye et al analyzed the clinical characteristics of EP patients with different severity and proposed three characteristics associated with more severe diseases: fever (>37.3°C) at admission; swelling and exudation of at least 50% skin lesions, or lower extremity edema; superficial lymphadenopathy. Patients who have two or more of these characteristics are classified under moderate-to-severe EP. In comparison, patients who have one or none of these characteristics are classified under mild EP. Based on the criteria, patients with moderate-to-severe EP have a higher systemic inflammatory state and a higher risk of developing anemia, hypoalbuminemia, and hypocalcemia than patients with mild EP.45 However, the current use of this evaluation method of EP severity is limited. From our aspect, the combination of the PASI and systemic evaluation may provide a more accurate assessment of disease severity in each EP patient. In the future, new evaluating tools combining both methods may aid in the treatment selection and the customized patient care for EP patients.
Systemic Treatments
Conventional Systemic Treatments
Before the application of biologics and other targeted therapies, several conventional systemic agents have already been used in EP, including retinoids, immunosuppressants, and systemic corticosteroids. Nowadays, the retinoids and immunosuppressants are still commonly applied in EP treatment. Their efficacy and safety profiles are summarized in Table 1.
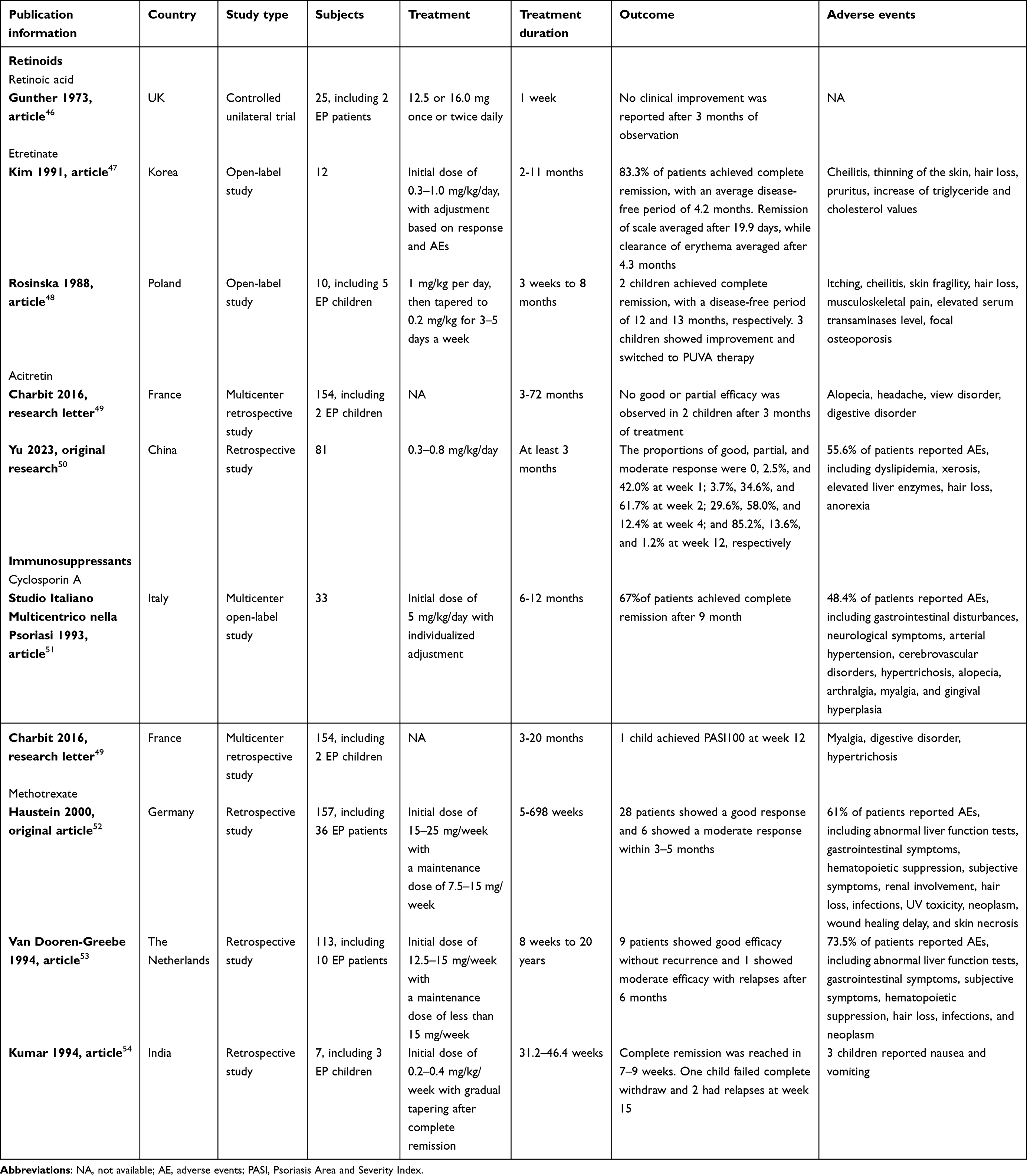 |
Table 1 Current Reports on the Effectiveness and Safety Profile of Conventional Systemic Therapies |
Retinoids
The retinoids are a group of molecules derived from vitamin A. Before taking effects in human bodies, these compounds are converted into the active metabolite all-trans-retinoic acid (ATRA). The ATRA binds to a retinoic acid receptor (RAR) in the cell nucleus, promoting heterodimerization of the RAR with a retinoid X receptor (RXR), resulting in initiation of transcription. ATRA can also directly regulate several signaling pathways by activating cellular kinases, including the p38-mitogen-activated protein kinase (p38MAPK), phosphatidylinositol-3-kinase (PI3K), and extracellular signal-regulated kinases 1/2 (ERK1/2). Therefore, the retinoids can regulate various physiological functions, including differentiation, apoptosis, and growth arrest.55,56 The retinoic acid was the first retinoid reported to treat a patient with EP in 1973. However, the systemic retinoic acid was applied only for 1 week, and no clinical response was observed after 3 months of observation.46 In comparison, the other retinoid agents, etretinate and its metabolite acitretin, have shown a high efficacy in EP, with no severe adverse events in the follow-up to 10 years.57 Case series have reported the use of etretinate in both adult and pediatric EP patients. With the initial dose of 20–60 mg/day, patients had a satisfactory response to etretinate treatment, and the average time to scale and remission was 19.9 (15–28) days and 4.3 (2–11) months, respectively.47,48 In a recent retrospective study involving 81 EP patients, the dose of 20–60 mg/day of acitretin, the majority of participants achieved a good or partial clinical response after treatment.50 However, acitretin seemed less effective in pediatric patients.49 The most common adverse events of retinoids were dyslipidemia, xerosis, and elevated liver enzymes. In addition, the potential teratogenic effect of retinoids must be addressed.50 Due to its relative short half-life of 2 days, acitretin is currently the most commonly applied retinoid, as well as the first-line treatment for EP.3,58
Immunosuppressants
As an immune-mediated disease, EP is associated with an abnormal T-cell pattern, leading to the up-regulation of many inflammatory cytokines, with the domination of the Th1 cytokines and IL-17 signaling pathway, as well as a slight shift toward Th2 inflammatory response.25,26 Therefore, the inhibition of the immune system is a therapeutic target for EP. The immunosuppressants like cyclosporin A (CSA), methotrexate (MTX), and mycophenolate mofetil (MMF) are candidates for EP treatment (Table 1).
CSA is a member of the calcineurin inhibitor family. The inhibition of calcineurin results in a decrease of inflammatory cytokines as well as T cells. Considering its immune-modulatory effects, CSA was first approved to treat psoriasis in 1997.59 Studies have shown a good response to CSA in severe EP patients, including one pediatric patient. Using the maximum initial dose of 5 mg/kg/day and individualized tapering strategy, 67% of EP patients achieved complete remission after a 9-month follow-up.49,51 The adverse events of CSA included gastrointestinal disturbances, hypertension, and neurological symptoms, and most of them were reversible after dose adjustment.51 However, the nephrotoxicity of CSA must be noted and monitored during treatment, as it can lead to acute kidney injury.60
MTX is a folate analog that inhibits dihydrofolate reductase and subsequently inhibits the proliferation of immune cells by promoting the release of adenosine and suppressing transmethylation reactions.61 Three retrospective studies evaluated the application of MTX in a total of 49 EP patients, including 3 pediatric patients. With the initial dose of 12.5–25 mg/week (or 0.2–0.4 mg/kg in children), 40 patients showed good efficacy, and the long-term use of MTX was tolerable.52–54 The most reported adverse events of MTX treatment included abnormal liver function, gastrointestinal symptoms, a hematopoietic suppression. However, with careful evaluation and regular monitoring, the long-term application of low-dose MTX was generally considered an effective and safe therapeutic option.52 MMF was reported only in individual cases before the 2000s, and its efficacy and safety data in EP need more investigation.62,63
Systemic Glucocorticoids (GCs)
GCs are mainly involved in the metabolism of carbohydrate, fat and protein. Through interacting with the cytosolic GC receptor, GCs alter gene transcription, increasing the transcription of anti-inflammatory genes but reducing the transcription of inflammatory genes. Therefore, GCs have anti-inflammatory and immunosuppressive effects when applied systemically or topically.64 Systemic corticosteroids were prescribed to EP patients in the 1950s, when Pascher et al reported the efficacy of prednisone in 2 case of childhood EP. According to the patients’ conditions, the doses were adjusted to 25–100mg per day, and a “breakthrough” effect was observed after 2–4 weeks of treatment. However, both patients soon suffered exacerbation of skin manifestations during dose reduction.65 A 10-year retrospective study in the 1980s suggested that systemic GCs are possibly a precipitating factor of EP, especially after the abrupt discontinuation of the therapy.17,66 Previous studies also found an association between systemic GC exposure and an increased risk of psoriasis flare or psoriatic arthritis.67 Therefore, systemic GCs are no longer recommended for EP treatment. However, some patients with severe EP are refractory to other drugs, which requires short-term application of systemic GCs. Therefore, it is important to emphasize the risk of systemic GCs in EP, and their adverse events should be monitored during application. Long-term use of systemic GCs should be avoided. Once the disease is controlled, the dose of systemic GCs should be gradually reduced, with careful monitoring of the patient. Relapses of EP and the development of GPP should be closely observed.
Biologics
The approval of biologics has greatly changed the treatment pattern and treatment outcomes of psoriasis. However, the evidence of biologics in EP is limited. A multicenter retrospective study in Japan reported the application of different types of biologics in 28 patients with 42 EP flares, indicating a good short-term efficacy but an unsatisfying long-term efficacy.68 The biologics used in EP treatment includes IL-17 inhibitors, TNF-α inhibitors, and IL-12/23 inhibitors. Their efficacy and safety profiles are summarized in Table 2.
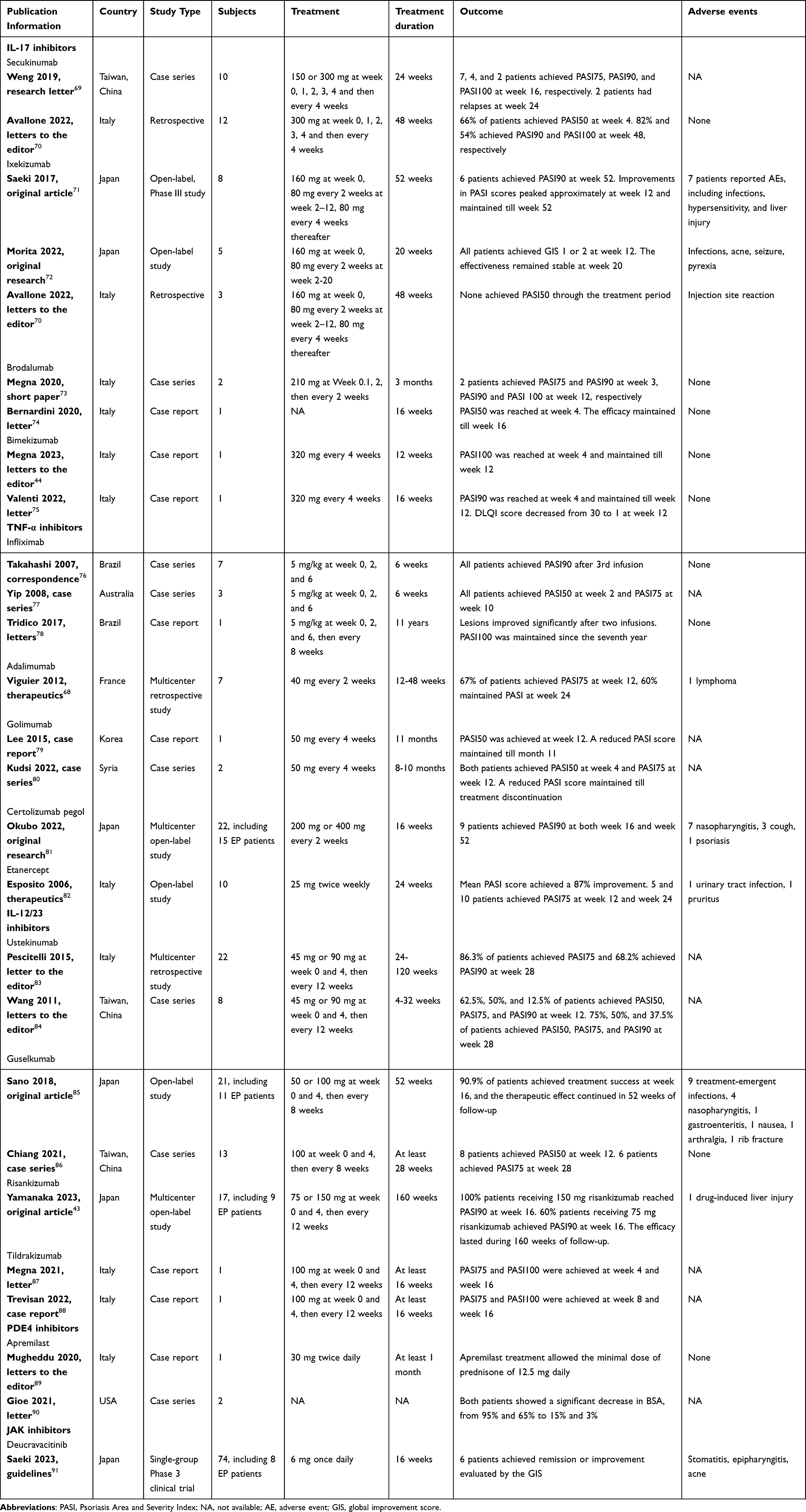 |
Table 2 Current Case Series or Clinical Trials on the Effectiveness and Safety Profile of Biologics and Small Molecule Drugs |
IL-17 Inhibitors
The IL-17 inhibitors are the most reported biologics in EP. Considering their different pharmacological mechanisms, there are four IL-17 inhibitors reported in EP treatment: secukinumab, ixekizumab, brodalumab, and bimekizumab.
Both secukinumab and ixekizumab have affinity for IL-17A, the dominant cytokine in EP development.70 A case series of 10 EP patients reported the use of 150 or 300 mg secukinumab after the treatment failure of systemic agents or other biologics. Secukinumab was injected subcutaneously once a week at a 5-week initiation and then every 4 weeks. A suboptimal effectiveness was observed, with 7 patients achieving PASI75 at week 12.69 Two studies reported the use of long-term and short-term efficacy of ixekizumab in 8 and 5 EP patients, respectively. Ixekizumab was administered subcutaneously at the dose of 160 mg at baseline, then 80 mg every other week for 12 weeks, followed by 80 mg monthly. Patients achieved significant remission in disease severity up to week 52, with improvements in different evaluation scales.71,72 Compared to patients with plaque psoriasis, the adverse events (AEs) of ixekizumab were more common in patients with EP, with infections being the most common AEs.71,72,92 A retrospective study compared the treatment pattern of secukinumab and ixekizumab in EP patients, suggesting that secukinumab had a faster PASI reduction as well as a higher drug survival rate.70
Brodalumab and bimekizumab act differently from secukinumab and ixekizumab. Brodalumab blocks both the IL-17A and the IL-17 receptor, while bimekizumab inhibits both IL-17A and IL-17F.44,74 Only individual cases reported the effectiveness of brodalumab and bimekizumab. The labeled dosage of brodalumab was 210 mg at week 0, 1, 2, and then every 2 weeks. Reports on the efficacy of brodalumab in EP seemed controversial.73,74 In comparison, bimekizumab has shown a fast efficacy in two EP patients.44,75
TNF-α Inhibitors
Five TNF-α inhibitors were used to treat EP in previous studies: infliximab, adalimumab, golimumab, certolizumab pegol (CZP), and etanercept (Table 2). Most TNF-α inhibitors specifically bind to TNF-α molecules and block their interaction with the receptors, therefore neutralize the inflammatory cytokines. These TNF-α inhibitors include infliximab, adalimumab, golimumab, and CZP.93–96 In comparison, etanercept can link to the TNF-α receptor through its p75 Fc region, therefore competitively inhibits TNF-α.82 Distinct from other TNF-α inhibitors, CZP is unable to bind to fetal Fc receptor, which prevents CZP from placental transfer from mother to fetus.97
Infliximab was the first as well as the most reported TNF-α inhibitor in EP treatment.98 Two case series reported the use of infliximab in a total of 10 patients with EP. Infliximab was administered intravenously at a dose of 5 mg/kg at week 0, 2, and 6. All patients achieved PASI75 after 3 doses of infliximab.76,77 The long-term effectiveness of infliximab for 11 years was also observed in one patient.78 However, a new increase in ANA and anti-dsDNA-ab IgM was observed in EP patients treated by infliximab, implying that infliximab might induce autoimmunity.99 The efficacy of adalimumab was reported in 7 EP patients. After 12 weeks of adalimumab therapy, 67% of patients achieved PASI75. Notably, the severe adverse event of T-cell lymphoma was recognized in one patient during the follow-up period.68 Three EP patients received 50 mg golimumab monthly, and they all reached PASI75 at week 12. The efficacy of golimumab lasted at least 11 months with the AE of pruritus and burning sensations in one patient.79,80 Both treatment of CZP 400 mg and CZP 200 mg every two weeks showed satisfactory efficacy in 15 EP patients, with 9 patients reaching PASI90 at both week 16 and week 52. However, the severe AE of erythema multiforme was reported in one patient with generalized pustular psoriasis who received 400 mg CZP treatment.81 Etanercept was given 25 mg subcutaneously twice a week in 10 EP patients. After 24 weeks, the mean PASI decreased from 39.1 to 5.1, with AEs of urinary tract infection and intense itching.82 Notably, previous studies suggested that TNF-α inhibitors might also induce paradoxical erythrodermic or pustular psoriasis during the treatment of psoriasis or other immune-mediated systemic diseases.77,100
IL-12/23 Inhibitors and IL-23 Inhibitors
Four IL-12/23 inhibitors or IL-23 inhibitors were applied in the treatment of EP: ustekinumab, guselkumab, risankizumab, and tildrakizumab (Table 2).
Ustekinumab is a human monoclonal antibody that inhibits the interaction of both IL-12 and IL-23 with their receptors. Two studies showed different efficacy of 45 and 90 mg ustekinumab among racial groups. In 22 Italian EP patients, 86.3% of patients reaching PASI75 and 68.2% reaching PASI90 at week 28. However, only 50% and 37.5% of 8 Asian patients achieved PASI75 and PASI90 at week 28.83,84 The difference in efficacy perhaps lay in different numbers of treatments or different responses among racial groups. Notably, ustekinumab may benefit refractory EP patients carrying certain gene mutations, such as CARD14.31
Guselkumab is a human monoclonal antibody that specifically inhibits the activity of IL-23. It was given 50 or 100 mg subcutaneously at week 0, 4, and then every 8 weeks. In two studies involving 24 EP patients receiving guselkumab, treatment success was achieved by most patients at week 16, and 46.2% patients reached PASI75 at week 28. The most common AE was infection.85,86
Risankizumab and tildrakizumab are IL-23 inhibitors which bind to the p19 subunit of IL-23 and blocks its activity.101,102 In a recent study involving 9 Japanese EP patients, risankizumab was given 75 or 150 mg at week 0, 4, and then every 12 weeks until week 160. All four patients who received 150 mg risankizumab and 60% (3/5) of the patients who received 75 mg reached PASI90 at week 16, and the efficacy continued through week 160. Notably, the approval dosage of risankizumab in Japan is 150 mg. One AE of drug-induced liver injury was reported in the 150 mg treatment group.43 The labeled dose of tildrakizumab is 100 mg at week 0, 4, and then every 12 weeks. Two Italian EP patients who received 100 mg tildrakizumab achieved PASI100 after 16 weeks, with substantial improvement in pruritus and fatigue.87,88 But the AE of tildrakizumab was unavailable from both cases.
Anti-Th2 Treatments
Previous studies suggested that EP patients present a Th1/Th17/TNF inflammatory pattern, but mild Th2 upregulation was also observed in EP.26,29 Therefore, anti-Th2 treatments may benefit EP patients. We conducted a literature search of anti-Th2 agents, including dupilumab, in EP treatments. However, no report was found till now.
Small Molecule Drugs
Apremilast
Apremilast is an inhibitor of the phosphodiesterase 4 (PDE4) that has been approved for plaque psoriasis and psoriatic arthritis by the U.S. Food and Drug Administration (FDA). With its immunoregulation ability and anti-inflammatory effects, apremilast was also a promising therapeutic option in other subtypes of psoriasis, such as GPP and palmoplantar pustulosis (PPP).103–105 Apremilast given at the dose of 30 mg orally had successfully controlled the erythema and scaling in a 45-year-old Italian EP patient with comorbid oligodendroglioma, allowing the minimal dose of prednisone of 12.5 mg daily. The apremilast therapy continued when the patient suffered from COVID-19, suggesting a good safety profile of apremilast.89 Another 2 American EP patients with multiple comorbidities received apremilast therapy. After one month of treatment, both patients reported a significant decrease in BSA, from 95% and 65% to 15% and 3%, respectively.90 Therefore, apremilast shows promising efficacy and safety in EP patients, especially those with multiple comorbidities or contradictions for other therapy. However, larger-scale cohorts are needed to prove the efficacy of apremilast in EP.
Janus Kinase (JAK) Inhibitors
JAK inhibitors target specific subtypes of Janus kinases (JAK1, JAK2, JAK3 and TYK2), thus regulate a wide range of cytokines.91 Therefore, JAK inhibitors may be an ideal therapeutic option for various immune-mediated diseases, including EP. A single-group phase 3 clinical trial investigated the efficacy of the TYK2 inhibitor deucravacitinib in plaque psoriasis, pustular psoriasis, and EP. Patients received 6 mg deucravacitinib daily until week 52. At week 16, 75% (6/8) of EP patients achieved remission or improvement evaluated by the GIS. The adverse events were reported in 25.7% (19/74) of all participants, and acne was reported in one EP patient. Actually, the Japanese guidance for JAK inhibitors has listed refractory EP as an indication for deucravacitinib.91 However, more substantial evidence in other populations is needed to evaluate the efficacy and safety of JAK inhibitors. Other JAK inhibitors, including tofacitinib, upadacitinib, and abrocitinib, require further investigation to determine their efficacy in EP.
Other Systemic Treatments
In 1988, Venier et al reported the use of somatostatin infusion in 20 patients with severe forms of psoriasis, including EP and sub-erythrodermic psoriasis. Somatostatin was administered by 96 hours of continuous intravenous infusion at a speed of 250 mg/h. The erythrodermic lesions had a nearly complete remission at 2–3 weeks after treatment, and 13 patients had no relapse in 4 years of follow-up. Seven patients who had an EP relapse received another somatostatin therapy with satisfying skin remission.106
A prospective study explored the efficacy of hydroxyurea in 34 patients with chronic plaque psoriasis, EP, or GPP. Hydroxyurea was administered orally at a dose of 1 g or 1.5 g daily. The mean PASI score was reduced by 76% in all patients at 10–12 weeks. The efficacy duration lasted from 6 months to 1 year, and 5 patients suffered a disease relapse. In addition, leukopenia was observed in 3 patients, resulting in termination of hydroxyurea therapy.107
In a case report, a 38-year-old female EP patient with an initial PASI score of 48, who refused to take any immunosuppressants, was prescribed low-dose naltrexone (LDN) of 4.5 mg every night. A remarkable clinical improvement was observed after 10 days of LDN therapy, and the patient reached complete remission after 3 months of treatment without adverse events.108
A prospective, double-blind, placebo-controlled clinical study investigated the effects of supplementation with antioxidants in EP and psoriatic arthritis. Patients who received intravenous prednisolone with the antioxidants coenzyme Q10, vitamin E, and selenium showed a better and faster improvement in disease severity, as well as a faster normalization of the oxidative stress markers, compared to patients who received prednisolone alone.109
Furthermore, a 50-year-old EP patient with comorbid HIV and HCV infection, who were unresponsive to different antipsoriatic drugs like acitretin, cyclosporin, and systemic GCs, showed a dramatic improvement in EP after the beginning of antiviral therapy, even without other antipsoriatic agents.110 The case highlighted the potential of managing comorbidities in EP treatment.
Topical Treatments
Emollients, moisturizers, topical vitamin D derivatives, topical GCs are widely used in the treatment of psoriasis. Emollients and moisturizers are products that limit the skin water evaporation and aid in skin rehydration.111 Their effect takes gently, seldom inducing skin irritation. These products are applied in general management of psoriasis vulgaris as well as GPP.112 Although there is no report on application of emollients and moisturizers in EP, it is possible that patients may receive these products to relieve the skin symptoms.
In a single-center double-blind clinical trial, patients with EP or plaque psoriasis involving >10% BSA were recruited. They received either 1.5 μg calcitriol with 0.1 g Vaseline or 0.1 g of Vaseline alone every night. After 2.4±0.1 months, the global severity score of patients treated by calcitriol decreased by 60.8±3.0%, with clinical improvements in erythema, plaque thickness and scaling. In comparison, patients treated by emollients (Vaseline) alone showed a decrease of 4.7±1.0% in global severity score. After 12 months of treatment, patients receiving calcitriol reported the decrease of erythema, plaque thickness, and scaling by 94.4±4.9%, 86.2±5.5%, and 75.0±4.1%, respectively. In comparison, patients receiving Vaseline alone had the improvements of 1.6±1.0%, 3.9±2.7%, 7.1±3.3% in erythema, plaque thickness, and scaling, respectively. No adverse event was reported during calcitriol treatment. However, the specific data of calcitriol on EP were not available.113 Notably, calcitriol monotherapy may induce skin irritation and EP deterioration. Thus, topical use or dilution before calcitriol application is recommended.
Although a series of clinical trials have investigated the efficacy and safety profile of topical GCs in severe plaque psoriasis, the data of these agents on EP are currently limited.114–116 Interestingly, two patients who received super potent topical corticosteroids under total body occlusion had a rapid clinical response, with significant improvements of erythema and scaling after 3–4 days of treatment.117 The side-effects of corticosteroids must be addressed during application, as iatrogenic Cushing’s syndrome has been reported in an EP patient self-treated by topical corticosteroid.118 Furthermore, large amounts of topical GCs may also induce EP flares. Therefore, patients are suggested to avoid large areas of topical GC use to reduce the recurrence of EP.
Topical aryl hydrocarbon receptor (AHR) is a newly recognized target for immune regulation, which participates in autoimmunity, cancer, and infection.119 Topical tapinarof is the first AHR agonist approved in plaque psoriasis. However, evidence on the use of tapinarof in EP is still lacking.
Phototherapy
Phototherapy is an effective therapeutic option for plaque psoriasis. Both psoralen plus ultraviolet light A (PUVA) and ultraviolet B (UVB) were reported in EP management. A multicenter clinical trial investigated the efficacy and safety profile of PUVA in different types of psoriasis, including 30 patients with EP. Compared with guttate and plaque psoriasis, EP needed a higher energy and more treatment counts to clear the skin lesions. Patients required an average of 16.4 weeks to achieve remission under the treatment of a mean total 368 J/cm2. The drop-out proportion was 29%, higher than the other two types of psoriasis. In addition, severe complications of cardiovascular disease and EP flares were observed during the PUVA treatment period.120 Another study concluded that only patients with plaque psoriasis reported clinical improvements after PUVA therapy. Instead, patients with other types of psoriasis showed worsening skin conditions after PUVA application, including 2 patients with EP.121 Therefore, it seemed that PUVA was not suitable for the management of EP.
Recently, Myers et al explored the value of the old-school Goeckerman therapy (UVB and crude coal tar) in the treatment of EP. A 46-year-old male with refractory EP was applied the Goeckerman regimen for 6 hours, 5 days a week. After application, he received a gradual increasing energy from 30 mJ of NB-UVB, as well as 2–10% crude coal tar. After 12 weeks of the Goeckerman therapy, a significant improvement was observed. The authors also emphasized the importance of a cool-down period using topical corticosteroids to reduce the skin inflammation prior to the initiation of phototherapy.122 After this case, the cool-down period perhaps will widen the application of phototherapy in EP.
Combination Therapy
The combination of different therapeutic options points to a new way to treat EP, especially when monotherapy loses effectiveness. As reported by individual cases and case series, different conventional systemic drugs are combined with biologics, other systemic agents, or topical agents.
Acitretin and secukinumab have been combined to treat 3 Turkish patients with severe psoriasis, including one with EP. The patient was first treated by 300 mg secukinumab every 4 weeks, which led to the achievement of PASI50 after 16 weeks. However, residual plaques remained uncleared even when secukinumab was increased to 300 mg every 2 weeks. Thus, acitretin with a dose of 0.1 mg/kg every two days was added, which resulted in almost complete skin clearance after another 6 weeks. No relapse of disease nor adverse event was observed during 1 year of follow-up.123
A case series presented the application of CSA combined with etretinate in 3 EP patients. All patients were unresponsive to monotherapy of CSA or etretinate. However, the combination of CSA and etretinate at an initial dose of 3.5 mg/kg and 0.5–0.6 mg/kg daily, respectively, has enabled the patients to reach a complete remission in 11–18 days. The doses of CSA and etretinate were then tapered and finally suspended. The patients reported no adverse events.124 In comparison, the clinical response to the combination of CSA and acitretin in 3 EP patients was unsatisfactory. All patients stopped treatment due to adverse events, including xerosis, elevated blood pressure, and increased serum creatinine. Interestingly, in one patient, the therapy was adjusted to the combination of CSA and topical calcipotriol, which resulted in significant clinical improvements after 6 weeks.125 The combination of CSA and calcipotriol has also successfully improved the skin condition of a 83-year-old male EP patient. However, CSA was discontinued due to the suspected adverse events of tremor and increased serum creatinine. Then, a low dose UVB was applied combined with calcipotriol, which also induced a satisfactory remission without side effects after 6 months of follow-up.126
Four patients with recalcitrant EP and comorbid psoriatic arthritis who had failed previous systemic treatment received the combination therapy of infliximab and MTX. In a dose of MTX 5–7.5 mg/week and infliximab 2.7–4.4 mg/kg every 6–8 weeks, significant clinical improvements were observed after 2–3 infusions of infliximab. The efficacy of this combination therapy maintained from 9 months to 5 years, respectively. During the maintenance treatment period, one case of severe skin bacterial infection was reported.127 MTX was also combined with adalimumab in a 36-year-old female EP patient, but no clinical response was seen after 4 weeks of treatment. Therefore, the efficacy of combination therapy seemed limited when systemic agent was started after the biologic failed.128
Management of Systemic Complications and Comorbidities of EP
Severe skin lesions associated with EP can lead to various systemic symptoms, including fever, skin exudation, lower extremity edema, and lymphadenopathy. These symptoms may progress to serious systemic complications, such as infections, electrolyte imbalances, anemia, and multiple organ failure—including renal impairment and heart failure—which pose a life-threatening risk to patients.39,40 Therefore, supportive medical care is indispensable. Patients without systemic involvement can be treated and regularly followed in the outpatient department. However, patients with systemic involvement may require hospitalization for general management including temperature regulation, fluid control, treatment of electrolyte imbalances, nutritional supports, and management of secondary infections.3 For skin lesions, emollients and cooling wet dressings may help relieve the uncomfortable feelings. For various comorbidities, patients may require multi-disciplinary treatment (MDT) so that they can receive specific treatments according to their comorbidities (Figure 3).
 |
Figure 3 Recommendations for the management of EP. Abbreviations: MDT, multi-disciplinary treatment. |
Recommendations for Therapeutic Options of EP
Several previous studies have examined the therapeutic options for EP and evaluated the quality of evidence. Unfortunately, the quality of evidence was unsatisfactory.3,129,130 These studies recommended the management of EP be based on the disease severity, the comorbidities, or the disease phases.3,129,130 However, the definition of disease severity was not clearly elucidated in these studies, limiting the popularization of the recommendations.
Based on the currently available evidence of this review, we suggest the application of different therapeutic options by disease severity (Figure 3). Moderate-to-severe EP patients fulfill two or three of the criteria: fever (>37.3°C) at admission; swelling and exudation of at least 50% skin lesions, or lower extremity edema; superficial lymphadenopathy.45 For conventional systemic drugs, acitretin and methotrexate are recommended for patients with mild EP, while cyclosporin A is recommended for moderate-to-severe EP patients.50–52 If available, biologics, particularly IL-17 and IL-12/23 inhibitors, are recommended for EP patients of any severity.69,83,86 Combination therapies should be considered for patients with refractory EP.127 Besides, topical treatments may help reduce localized symptoms.113,117 However, it is important to note that skin irritation can occur after applying topical vitamin D derivatives, and sudden withdrawal of topical GCs may induce EP flares. Therefore, the application of these agents should be avoided over large areas. Generally, systemic GC and phototherapy are not recommended for EP management.17,120
Treatment-associated complications are adverse events or side effects of long-term treatment of EP. Different therapies entail diverse complications requiring monitoring. For CSA and MTX, routine blood tests every 1–3 months, including complete blood counts (CBC) and comprehensive metabolic panel (CMP), are recommended.59,131 Acitretin requires monthly monitoring of blood lipid levels, with strict avoidance of pregnancy during therapy.132 Biologics may reactivate latent systemic infections, especially tuberculosis (TB) and viral hepatitis. Prior to biological therapy, TB and viral hepatitis examinations are essential. The T-SPOT TB test and serum hepatitis B (HBV) DNA detection via real-time polymerase chain reaction (PCR) are recommended before biologic initiation and annually thereafter. Positive results necessitate careful evaluation of the infection activity and the necessity of biologic treatment. Biologics are contraindicated in active TB and viral hepatitis. For latent infections, anti-TB or anti-HBV therapies are recommended before biologic initiation.133 For patients receiving apremilast treatment, regular blood tests and screening for TB and HBV are unnecessary.134 For patients receiving JAK inhibitors, CBC, CMZ, and blood lipid level should be monitored. Risks of reactivating latent infections and malignancy are also noted.135
Conclusion
Erythrodermic psoriasis is a rare disease with substantial disease burden, which is beyond solely a severe form of psoriasis vulgaris from both clinical presentations and pathogenesis. Compared to previous review articles and clinical guidelines, our review offers updates in three key areas.3,129,130 First, it incorporates new evidence on the use of acitretin, biologics, and JAK inhibitors for EP. Second, we propose practical criteria for evaluating EP severity, developed in alignment with our prior research. Third, using these newly proposed evaluation criteria, we present a practical management algorithm for the first time, providing guidance for the optimal treatment of EP. For conventional systemic treatments, acitretin and MTX are suggested for mild EP, while cyclosporin A is recommended for moderate-to-severe EP. For biologics, IL-17 and IL-12/23 inhibitors have shown benefits for EP patients, regardless of disease severity, when compared with TNF-α inhibitors. Combination therapies are considered when monotherapy proves ineffective. These approaches may involve combining a biologic agent with a conventional systemic drug or using two to three conventional systemic drugs together to improve efficacy. Supportive medical care and management of comorbidities are also crucial. However, it is important to note that the quality of the current evidence remains suboptimal. In the future, clinical trials involving more EP patients can investigate the efficacy and safety of mainstream therapies for EP and compare the effectiveness among various therapeutic options.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Beijing Natural Science Foundation (7242109), National High Level Hospital Clinical Research Funding (2022-PUMCH-B-092, 2022-PUMCH-A-066), Beijing Key Clinical Specialty Construction Project, National Key Clinical Specialty Project of China, and Peking Union Medical College Hospital Talent Cultivation Program Category D (UHB11983).
Disclosure
The authors have no competing interests to declare that are relevant to the content of this article.
References
1. Singh RK, Lee KM, Ucmak D, et al. Erythrodermic psoriasis: pathophysiology and current treatment perspectives. Psoriasis. 2016;6:93–104. doi:10.2147/PTT.S101232
2. Stinco G, Errichetti E. Erythrodermic psoriasis: current and future role of biologicals. BioDrugs. 2015;29(2):91–101. doi:10.1007/s40259-015-0119-4
3. Rosenbach M, Hsu S, Korman NJ, et al. Treatment of erythrodermic psoriasis: from the medical board of the national psoriasis foundation. J Am Acad Dermatol. 2010;62(4):655–662. doi:10.1016/j.jaad.2009.05.048
4. Morrone A, Dell’anna ML, Cristaudo A, et al. Psoriasis in Tigray, Ethiopia: focusing on available treatments. Dermatol Ther. 2022;35(3):e14718. doi:10.1111/dth.14718
5. Voloshyna D, Ehsan Ullah S, Jahan N, et al. Beta-blocker-induced erythrodermic psoriasis: a case report. Cureus. 2022;14(10):e29809. doi:10.7759/cureus.29809
6. Pinto-Pulido EL, Polo-Rodriguez I, Gonzalez-Canete M, et al. Ixekizumab treatment for drug-induced erythrodermic psoriasis. Dermatol Ther. 2022;35(11):e15863. doi:10.1111/dth.15863
7. Vinaixa Aranzazu A, Morillas-Lahuerta V, Blanco De Tord M, et al. Ixekizumab for the treatment of erythrodermic psoriasis triggered by durvalumab-tremelimumab in a cancer patient. Eur J Dermatol. 2021;31(4):564–565. doi:10.1684/ejd.2021.4087
8. Koumaki D, Koumaki V, Haniotis V, et al. Erythrodermic psoriasis after rituximab treatment in a patient with autoimmune hemolytic anemia. Indian J Dermatol. 2021;66(1):108–112. doi:10.4103/ijd.IJD_336_19
9. Tichy M. Arthropathic psoriasis complicated by a paradoxical reaction in the form of erythrodermic psoriasis following Adalimumab and by an allergic reaction following infliximab which was successfully managed with secukinumab. Postepy Dermatol Alergol. 2019;36(4):495–497. doi:10.5114/ada.2019.87454
10. Nowsheen S, Kohorst JJ, El-Azhary RA. Adalimumab-induced erythrodermic reactions. Int J Dermatol. 2019;58(10):e204–e6. doi:10.1111/ijd.14503
11. Hernandez Garcia I. Severe erythroderma in a patient under intermittent therapy with efalizumab. J Drugs Dermatol. 2008;7(10):987–989.
12. Esposito M, Saraceno R, Schipani C, et al. Trimethoprim-sulfamethoxazole induced erythrodermic psoriasis. J Infect. 2008;57(1):90–92. doi:10.1016/j.jinf.2008.04.005
13. Wang Y, Liu P. A case of erythema multiforme drug eruption associated with erythrodermic psoriasis induced by sofosbuvir and daclatasvir. J Clin Pharm Ther. 2017;42(1):108–110. doi:10.1111/jcpt.12467
14. Matos-Pires E, Campos S, Mendes-Bastos P, et al. Erythrodermic psoriasis induced by bupropion. J Eur Acad Dermatol Venereol. 2017;31(2):e129–e30. doi:10.1111/jdv.13876
15. Trepanowski N, Coleman EL, Melson G, et al. Erythrodermic psoriasis after COVID-19 vaccination. JAAD Case Rep. 2022;28:123–126. doi:10.1016/j.jdcr.2022.07.041
16. Evans AV, Parker JC, Russell-Jones R. Erythrodermic psoriasis precipitated by radiologic contrast media. J Am Acad Dermatol. 2002;46(6):960–961. doi:10.1067/mjd.2002.120570
17. Heinrich M, Cook E, Roach J, et al. Erythrodermic psoriasis secondary to systemic corticosteroids. Proc Bayl Univ Med Cent. 2020;33(1):113–114. doi:10.1080/08998280.2019.1686911
18. Papadavid E, Kokkalis G, Polyderas G, et al. Rapid clearance of erythrodermic psoriasis with apremilast. J Dermatol Case Rep. 2017;11(2):29–31. doi:10.3315/jdcr.2017.1246
19. Potter KA, Motaparthi K, Schzoch JJ. Erythrodermic psoriasis after discontinuation of ixekizumab. JAAD Case Rep. 2018;4(1):22–23. doi:10.1016/j.jdcr.2017.06.026
20. Chen W, Peng C, Zheng J, et al. Bullous pemphigoid associated with erythrodermic psoriasis: a case report. Clin Cosmet Invest Dermatol. 2022;15:1805–1808. doi:10.2147/CCID.S374556
21. Ali Khan Q, Khan T, Anthony MR, et al. An erythrodermic psoriasis flare-up with staphylococcus bacteremia secondary to COVID-19 infection: a case report. Cureus. 2023;15(3):e36418. doi:10.7759/cureus.36418
22. Kassi K, Mienwoley OA, Kouyate M, et al. Severe skin forms of psoriasis in black Africans: epidemiological, clinical, and histological aspects related to 56 cases. Autoimmune Dis. 2013;2013:561032. doi:10.1155/2013/561032
23. Li Y, Wen Y, You R, et al. Erythrodermic psoriasis precipitated by B-cell chronic lymphocytic leukemia. Dermatol Ther. 2021;34(3):e14904. doi:10.1111/dth.14904
24. Li LF, Sujan SA, Yang H, et al. Serum immunoglobulins in psoriatic erythroderma. Clin Exp Dermatol. 2005;30(2):125–127. doi:10.1111/j.1365-2230.2004.01717.x
25. Xing X, Liang Y, Sarkar MK, et al. IL-17 responses are the dominant inflammatory signal linking inverse, erythrodermic, and chronic plaque psoriasis. J Invest Dermatol. 2016;136(12):2498–2501. doi:10.1016/j.jid.2016.07.008
26. Zhang P, Chen HX, Duan YQ, et al. Analysis of Th1/Th2 response pattern for erythrodermic psoriasis. J Huazhong Univ Sci Technolog Med Sci. 2014;34(4):596–601. doi:10.1007/s11596-014-1322-0
27. Bressan AL, Picciani BLS, Azulay-Abulafia L, et al. Evaluation of ICAM-1 expression and vascular changes in the skin of patients with plaque, pustular, and erythrodermic psoriasis. Int J Dermatol. 2018;57(2):209–216. doi:10.1111/ijd.13883
28. Wu X, Luo Y, Liu L, et al. Single-cell RNA-seq reveals increased and activated post-capillary venule endothelial cells in erythrodermic psoriasis. Inflammation. 2025.
29. Song B, Ning X, Guo L, et al. Comparative proteomics analysis reveals distinct molecular phenotype and biomarkers in patients with erythrodermic atopic dermatitis and erythrodermic psoriasis. Inflammation. 2024;48(1):331–345. doi:10.1007/s10753-024-02078-3
30. Huang YW, Tsai TF. HLA-Cw1 and Psoriasis. Am J Clin Dermatol. 2021;22(3):339–347. doi:10.1007/s40257-020-00585-1
31. Signa S, Campione E, Rusmini M, et al. Whole exome sequencing approach to childhood onset familial erythrodermic psoriasis unravels a novel mutation of CARD14 requiring unusual high doses of ustekinumab. Pediatr Rheumatol Online J. 2019;17(1):38. doi:10.1186/s12969-019-0336-3
32. Cardili RN, Deghaide NS, Mendes-Junior CT, et al. HLA-C and TNF gene polymorphisms are associated with psoriasis in B razilian patients. Int J Dermatol. 2016;55(1):e16–22. doi:10.1111/ijd.12894
33. Guo L, Wu C, Song B, et al. Exploration of circulating metabolic signature of erythrodermic psoriasis based on LC-MS metabolomics. Exp Dermatol. 2024;33(5):e15103. doi:10.1111/exd.15103
34. Wang WM, Wu C, Gao YM, et al. Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and other hematological parameters in psoriasis patients. BMC Immunol. 2021;22(1):64. doi:10.1186/s12865-021-00454-4
35. Kampe T, Dorko E, Rimarova K, et al. Prevalence of cardiovascular risk factors in patients with psoriasis. Cent Eur J Public Health. 2022;30(Supplement):S05–S10. doi:10.21101/cejph.a6806
36. Zheng J, Gao Y, Liu N, et al. Higher prevalence of thyroid dysfunction in patients with erythrodermic psoriasis. J Dermatol. 2020;47(9):1007–1012. doi:10.1111/1346-8138.15427
37. Al-Niaimi F, Lyon CC. Erythrodermic psoriasis complicated by acute respiratory distress syndrome. Eur J Dermatol. 2011;21(3):429–430. doi:10.1684/ejd.2011.1303
38. Kagan A, Husza’r M, Frumkin A, et al. Reversal of nephrotic syndrome due to AA amyloidosis in psoriatic patients on long-term colchicine treatment. Case report and review of the literature. Nephron. 1999;82(4):348–353. doi:10.1159/000045450
39. Zhao Z, Zhang X, Wang R, et al. Vaccine-induced erythrodermic psoriasis in a child successfully treated with secukinumab: a case report and brief literature review. Dermatol Ther. 2022;35(9):e15684. doi:10.1111/dth.15684
40. Karimi M, Zaher A, Bressler M, et al. Distributive shock in erythrodermic psoriasis treated with norepinephrine and vasopressin: a case report. Cureus. 2023;15(4):e37728. doi:10.7759/cureus.37728
41. Schaefer C, Mamolo C, Cappelleri JC, et al. Treatment patterns and outcomes among adults admitted to hospital in the U.K. due to plaque or erythrodermic psoriasis. Br J Dermatol. 2017;177(3):e52–e4. doi:10.1111/bjd.15270
42. Egeberg A, Thyssen JP, Gislason GH, et al. Prognosis after hospitalization for erythroderma. Acta Derm Venereol. 2016;96(7):959–962. doi:10.2340/00015555-2445
43. Yamanaka K, Okubo Y, Yasuda I, et al. Efficacy and safety of risankizumab in Japanese patients with generalized pustular psoriasis or erythrodermic psoriasis: primary analysis and 180-week follow-up results from the phase 3, multicenter IMMspire study. J Dermatol. 2023;50(2):195–202. doi:10.1111/1346-8138.16667
44. Megna M, Battista T, Potestio L, et al. A case of erythrodermic psoriasis rapidly and successfully treated with Bimekizumab. J Cosmet Dermatol. 2023;22(3):1146–1148. doi:10.1111/jocd.15543
45. Ye F, Gui X, Wu C, et al. Severity evaluation and prognostic factors in erythrodermic psoriasis. Eur J Dermatol. 2018;28(6):851–853. doi:10.1684/ejd.2018.3437
46. Gunther S. The therapeutic value of retinoic acid in chronic discoid, acute guttate, and erythrodermic psoriasis: clinical observations on twenty-five patients. Br J Dermatol. 1973;89(5):515–517. doi:10.1111/j.1365-2133.1973.tb03014.x
47. Kim BS, Shin KS, Youn JI, et al. Treatment of erythrodermic psoriasis with etretinate. Ann Dermatol. 1991;3(2):107–111. doi:10.5021/ad.1991.3.2.107
48. Rosinska D, Wolska H, Jablonska S, et al. Etretinate in severe psoriasis of children. Pediatr Dermatol. 1988;5(4):266–272. doi:10.1111/j.1525-1470.1988.tb00902.x
49. Charbit L, Mahe E, Phan A, et al. Systemic treatments in childhood psoriasis: a French multicentre study on 154 children. Br J Dermatol. 2016;174(5):1118–1121. doi:10.1111/bjd.14326
50. Yu C, Wu C, Yang Y, et al. Systemic monotherapy with Acitretin for erythrodermic psoriasis: results of a retrospective study of 81 patients. Ther Adv Chronic Dis. 2023;14:20406223231178412. doi:10.1177/20406223231178412
51. Multicentrico SI. Management of erythrodermic psoriasis with low-dose cyclosporin. Studio Italiano Multicentrico nella Psoriasi (SIMPSO). Dermatology. 1993;187(Suppl 1):30–37. doi:10.1159/000247289
52. Haustein UF, Rytter M. Methotrexate in psoriasis: 26 years’ experience with low-dose long-term treatment. J Eur Acad Dermatol Venereol. 2000;14(5):382–388. doi:10.1046/j.1468-3083.2000.00058.x
53. Van Dooren-Greebe RJ, Kuijpers AL, Mulder J, et al. Methotrexate revisited: effects of long-term treatment in psoriasis. Br J Dermatol. 1994;130(2):204–210. doi:10.1111/j.1365-2133.1994.tb02901.x
54. Kumar B, Dhar S, Handa S, et al. Methotrexate in childhood psoriasis. Pediatr Dermatol. 1994;11(3):271–273. doi:10.1111/j.1525-1470.1994.tb00602.x
55. Szymanski L, Skopek R, Palusinska M, et al. Retinoic acid and its derivatives in skin. Cells. 2020;9(12):2660. doi:10.3390/cells9122660
56. Das BC, Thapa P, Karki R, et al. Retinoic acid signaling pathways in development and diseases. Bioorg Med Chem. 2014;22(2):673–683. doi:10.1016/j.bmc.2013.11.025
57. Magis NL, Blummel JJ, Kerkhof PC, et al. The treatment of psoriasis with etretinate and Acitretin: a follow up of actual use. Eur J Dermatol. 2000;10(7):517–521.
58. Monfrecola G, Baldo A. Retinoids and phototherapy for psoriasis. J Rheumatol Suppl. 2009;83:71–72. doi:10.3899/jrheum.090231
59. Amber T, Tabassum S. Cyclosporin in dermatology: a practical compendium. Dermatol Ther. 2020;33(6):e13934. doi:10.1111/dth.13934
60. Rao S, Bernshteyn M, Sohal R, et al. The management of erythrodermic psoriasis complicated by cyclosporine. Case Reports in Dermatological Medicine. 2020;2020:5215478. doi:10.1155/2020/5215478
61. Cronstein BN. The mechanism of action of methotrexate. Rheum Dis Clin North Am. 1997;23(4):739–755. doi:10.1016/S0889-857X(05)70358-6
62. Geilen CC, Tebbe B, Garcia Bartels C, et al. Successful treatment of erythrodermic psoriasis with mycophenolate mofetil. Br J Dermatol. 1998;138(6):1101–1102. doi:10.1046/j.1365-2133.1998.02296.x
63. Marinari R, Fleischmajer R, Schragger AH, et al. Mycophenolic acid in the treatment of psoriasis: long-term administration. Arch Dermatol. 1977;113(7):930–932. doi:10.1001/archderm.1977.01640070064007
64. Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30. doi:10.1186/1710-1492-9-30
65. Pascher F, Wood WS. Erythrodermic psoriasis in children; a report of two cases. AMA Arch Derm. 1956;74(2):173–176. doi:10.1001/archderm.1956.01550080059009
66. Boyd AS, Menter A. Erythrodermic psoriasis. Precipitating factors, course, and prognosis in 50 patients. J Am Acad Dermatol. 1989;21(5 Pt 1):985–991. doi:10.1016/S0190-9622(89)70287-5
67. Kresch M, Weingarten M, Guenin S, et al. Risk of rebound psoriasis flare from systemic corticosteroid use in patients with psoriasis: a retrospective cohort study. J Am Acad Dermatol. 2023;88(5):1182–1183. doi:10.1016/j.jaad.2022.12.019
68. Viguier M, Pages C, Aubin F, et al. Efficacy and safety of biologics in erythrodermic psoriasis: a multicentre, retrospective study. Br J Dermatol. 2012;167(2):417–423. doi:10.1111/j.1365-2133.2012.10940.x
69. Weng HJ, Wang TS, Tsai TF. Clinical experience of secukinumab in the treatment of erythrodermic psoriasis: a case series [J]. Br J Dermatol. 2018;178(6):1439–1440. doi:10.1111/bjd.16252
70. Avallone G, Cariti C, Dapavo P, et al. Real-life comparison between secukinumab and ixekizumab in the treatment of pustular and erythrodermic psoriasis. J Eur Acad Dermatol Venereol. 2022;36(7):e574–e6. doi:10.1111/jdv.18069
71. Saeki H, Nakagawa H, Nakajo K, et al. Efficacy and safety of ixekizumab treatment for Japanese patients with moderate to severe plaque psoriasis, erythrodermic psoriasis and generalized pustular psoriasis: results from a 52-week, open-label, phase 3 study (UNCOVER-J). J Dermatol. 2017;44(4):355–362. doi:10.1111/1346-8138.13622
72. Morita A, Okubo Y, Morisaki Y, et al. Ixekizumab 80 mg every 2 weeks treatment beyond week 12 for Japanese patients with generalized pustular psoriasis and erythrodermic psoriasis. Dermatol Ther. 2022;12(2):481–494. doi:10.1007/s13555-021-00666-x
73. Megna M, Fabbrocini G, Ferrillo M, et al. Erythrodermic psoriasis successfully and rapidly treated with brodalumab: report of two cases. Dermatol Ther. 2020;33(6):e14351. doi:10.1111/dth.14351
74. Bernardini N, Skroza N, Tolino E, et al. Recurrent erythrodermic psoriasis and polycythemia successfully treated with brodalumab. Dermatol Ther. 2020;33(6):e14338. doi:10.1111/dth.14338
75. Valenti M, Gargiulo L, Ibba L, et al. Sub-erythrodermic psoriasis successfully treated with bimekizumab: a case report. Dermatol Ther. 2022;35(12):e15952. doi:10.1111/dth.15952
76. Takahashi MD, Castro LG, Romiti R. Infliximab, as sole or combined therapy, induces rapid clearing of erythrodermic psoriasis. Br J Dermatol. 2007;157(4):828–831. doi:10.1111/j.1365-2133.2007.08111.x
77. Yip L, Harrison S, Foley P. From biologic to biologic to biologic: lessons to learn for erythrodermic and recalcitrant chronic plaque psoriasis. Australas J Dermatol. 2008;49(3):152–155. doi:10.1111/j.1440-0960.2008.00463.x
78. Tridico LA, Antonio JR, Mathias CE, et al. Effectiveness and safety of infliximab for 11 years in a patient with erythrodermic psoriasis and psoriatic arthritis. An Bras Dermatol. 2017;92(5):743–745. doi:10.1590/abd1806-4841.20176565
79. Lee WK, Kim GW, Cho HH, et al. Erythrodermic psoriasis treated with golimumab: a case report. Ann Dermatol. 2015;27(4):446–449. doi:10.5021/ad.2015.27.4.446
80. Kudsi M, Alzabibi MA, Shibani M. Two cases of erythrodermic psoriasis treated with golimumab. Ann Med Surg Lond. 2022;78:103961. doi:10.1016/j.amsu.2022.103961
81. Okubo Y, Umezawa Y, Sakurai S, et al. Efficacy and safety of certolizumab pegol in Japanese patients with generalized pustular psoriasis and erythrodermic psoriasis: 52-week results. Dermatol Ther. 2022;12(6):1397–1415. doi:10.1007/s13555-022-00741-x
82. Esposito M, Mazzotta A, De Felice C, et al. Treatment of erythrodermic psoriasis with etanercept. Br J Dermatol. 2006;155(1):156–159. doi:10.1111/j.1365-2133.2006.07217.x
83. Pescitelli L, Dini V, Gisondi P, et al. Erythrodermic psoriasis treated with ustekinumab: an Italian multicenter retrospective analysis. J Dermatol Sci. 2015;78(2):149–151. doi:10.1016/j.jdermsci.2015.01.005
84. Wang TS, Tsai TF. Clinical experience of ustekinumab in the treatment of erythrodermic psoriasis: a case series. J Dermatol. 2011;38(11):1096–1099. doi:10.1111/j.1346-8138.2011.01224.x
85. Sano S, Kubo H, Morishima H, et al. Guselkumab, a human interleukin-23 monoclonal antibody in Japanese patients with generalized pustular psoriasis and erythrodermic psoriasis: efficacy and safety analyses of a 52-week, phase 3, multicenter, open-label study. J Dermatol. 2018;45(5):529–539. doi:10.1111/1346-8138.14294
86. Chiang CY, Tsai TF. Treatment response of patients with erythrodermic psoriasis after switching to guselkumab. Dermatol Ther. 2021;11(1):301–306. doi:10.1007/s13555-020-00480-x
87. Megna M, Potestio L, Fabbrocini G, et al. Tildrakizumab: a new therapeutic option for erythrodermic psoriasis? Dermatol Ther. 2021;34(5):e15030.
88. Trevisan G, Germi L, Naldi L. Erythrodermic psoriasis improved by Tildrakizumab. Dermatol Reports. 2022;14(4):9448. doi:10.4081/dr.2022.9448
89. Mugheddu C, Pizzatti L, Sanna S, et al. COVID-19 pulmonary infection in erythrodermic psoriatic patient with oligodendroglioma: safety and compatibility of apremilast with critical intensive care management. J Eur Acad Dermatol Venereol. 2020;34(8):e376–e8. doi:10.1111/jdv.16625
90. Gioe OA, Savoie C, Grieshaber EB, et al. Treatment of erythrodermic psoriasis with apremilast. JAAD Case Rep. 2021;11:36–37. doi:10.1016/j.jdcr.2021.03.011
91. Saeki H, Mabuchi T, Asahina A, et al. English version of Japanese guidance for the use of oral Janus kinase inhibitors (JAK1 and TYK2 inhibitors) in the treatments of psoriasis. J Dermatol. 2023;50(5):e138–e50. doi:10.1111/1346-8138.16797
92. Pruneda CC, Austin BA, Wallis DT, et al. Ixekizumab and herpes zoster in an erythrodermic patient. Proc Bayl Univ Med Cent. 2020;33(3):417–418. doi:10.1080/08998280.2020.1741756
93. Scallon BJ, Moore MA, Trinh H, et al. Chimeric anti-TNF-alpha monoclonal antibody cA2 binds recombinant transmembrane TNF-alpha and activates immune effector functions [J]. Cytokine. 1995;7(3):251–259. doi:10.1006/cyto.1995.0029
94. Croom KF, Mccormack PL. Adalimumab: in plaque psoriasis [J]. Am J Clin Dermatol. 2009;10(1):43–50. doi:10.2165/0128071-200910010-00008
95. Mazumdar S, Greenwald D. Golimumab. MAbs. 2009;1(5):422–431. doi:10.4161/mabs.1.5.9286
96. Lee A, Scott LJ. Certolizumab pegol: a review in moderate to severe plaque psoriasis. BioDrugs. 2020;34(2):235–244. doi:10.1007/s40259-020-00416-z
97. Mariette X, Forger F, Abraham B, et al. Lack of placental transfer of certolizumab pegol during pregnancy: results from CRIB, a prospective, postmarketing, pharmacokinetic study. Ann Rheum Dis. 2018;77(2):228–233. doi:10.1136/annrheumdis-2017-212196
98. Lisby S, Gniadecki R. Infliximab (Remicade) for acute, severe pustular and erythrodermic psoriasis. Acta Derm Venereol. 2004;84(3):247–248.
99. Poulalhon N, Begon E, Lebbe C, et al. A follow-up study in 28 patients treated with infliximab for severe recalcitrant psoriasis: evidence for efficacy and high incidence of biological autoimmunity. Br J Dermatol. 2007;156(2):329–336. doi:10.1111/j.1365-2133.2006.07639.x
100. Goiriz R, Dauden E, Perez-Gala S, et al. Flare and change of psoriasis morphology during the course of treatment with tumour necrosis factor blockers. Clin Exp Dermatol. 2007;32(2):176–179. doi:10.1111/j.1365-2230.2006.02315.x
101. Singh S, Kroe-Barrett RR, Canada KA, et al. Selective targeting of the IL23 pathway: generation and characterization of a novel high-affinity humanized anti-IL23A antibody. MAbs. 2015;7(4):778–791. doi:10.1080/19420862.2015.1032491
102. Naslund-Koch C, Zachariae C, Skov L. Tildrakizumab: an evidence-based review of its use in the treatment of moderate-to-severe chronic plaque psoriasis. Ther Clin Risk Manag. 2020;16:903–916. doi:10.2147/TCRM.S227880
103. Krishnamoorthy G, Kotecha A, Pimentel J. Complete resolution of erythrodermic psoriasis with first-line apremilast monotherapy. BMJ Case Rep. 2019;12(1):e226959. doi:10.1136/bcr-2018-226959
104. Jeon C, Nakamura M, Sekhon S, et al. Generalized pustular psoriasis treated with apremilast in a patient with multiple medical comorbidities. JAAD Case Rep. 2017;3(6):495–497. doi:10.1016/j.jdcr.2017.07.007
105. Wilsmann-Theis D, Kromer C, Gerdes S, et al. A multicentre open-label study of apremilast in palmoplantar pustulosis (APLANTUS). J Eur Acad Dermatol Venereol. 2021;35(10):2045–2050. doi:10.1111/jdv.17441
106. Venier A, De Simone C, Forni L, et al. Treatment of severe psoriasis with somatostatin: four years of experience. Arch Dermatol Res. 1988;280:S51–4.
107. Sharma VK, Dutta B, Ramam M. Hydroxyurea as an alternative therapy for psoriasis. Indian J Dermatol Venereol Leprol. 2004;70(1):13–17.
108. Beltran Monasterio EP. Low-dose naltrexone: an alternative treatment for erythrodermic psoriasis. Cureus. 2019;11(1):e3943. doi:10.7759/cureus.3943
109. Kharaeva Z, Gostova E, De Luca C, et al. Clinical and biochemical effects of coenzyme Q(10), vitamin E, and selenium supplementation to psoriasis patients. Nutrition. 2009;25(3):295–302. doi:10.1016/j.nut.2008.08.015
110. Chiricozzi A, Saraceno R, Cannizzaro MV, et al. Complete resolution of erythrodermic psoriasis in an HIV and HCV patient unresponsive to antipsoriatic treatments after highly active antiretroviral therapy (ritonavir, atazanavir, emtricitabine, tenofovir). Dermatology. 2012;225(4):333–337. doi:10.1159/000345762
111. Peters BP, Weissman FG, Gill MA. Pathophysiology and treatment of psoriasis. Am J Health Syst Pharm. 2000;57(7):645–59;quiz60–1. doi:10.1093/ajhp/57.7.645
112. Wang HM, Xu JM, Jin HZ. Characteristics and burdens of disease in patients from Beijing with generalized pustular psoriasis and palmoplantar pustulosis: multicenter retrospective cohort study using a regional database. Am J Clin Dermatol. 2023;24(6):991–1002. doi:10.1007/s40257-023-00807-2
113. Perez A, Chen TC, Turner A, et al. Efficacy and safety of topical calcitriol (1,25-dihydroxyvitamin d3) for the treatment of psoriasis. Br J Dermatol. 1996;134(2):238–246. doi:10.1111/j.1365-2133.1996.tb07608.x
114. Sidgiddi S, Naqvi SMH, Shenoy M, et al. Efficacy and safety of novel formulation of clobetasol propionate 0.025% cream in Indian moderate-to-severe psoriasis patients: phase-2a, randomized 3-arm study. Dermatol Ther. 2021;11(5):1717–1732. doi:10.1007/s13555-021-00591-z
115. Lebwohl MG, Stein Gold L, Del Rosso JQ, et al. Posttreatment maintenance of therapeutic effect with fixed-combination halobetasol propionate 0.01%/tazarotene 0.045% lotion for moderate-to-severe plaque psoriasis. J DermatolTreat. 2022;33(4):2068–2074. doi:10.1080/09546634.2021.1914310
116. Castela E, Archier E, Devaux S, et al. Topical corticosteroids in plaque psoriasis: a systematic review of efficacy and treatment modalities. J Eur Acad Dermatol Venereol. 2012;26(3):36–46. doi:10.1111/j.1468-3083.2012.04522.x
117. Arbiser JL, Grossman K, Kaye E, et al. Use of short-course class 1 topical glucocorticoid under occlusion for the rapid control of erythrodermic psoriasis. Arch Dermatol. 1994;130(6):704–706. doi:10.1001/archderm.1994.01690060034003
118. Ohnishi T, Suzuki T, Watanabe S, et al. Erythrodermic psoriasis associated with hyperuricemia and Iatrogenic Cushing’s syndrome due to topical corticosteroid therapy. Int J Dermatol. 1996;35(5):379–380. doi:10.1111/j.1365-4362.1996.tb03647.x
119. Polonio CM, Mchale KA, Sherr DH, et al. The aryl hydrocarbon receptor: a rehabilitated target for therapeutic immune modulation. Nat Rev Drug Discov. 2025. doi:10.1038/s41573-025-01172-x
120. Melski JW, Tanenbaum L, Parrish JA, et al. Oral methoxsalen photochemotherapy for the treatment of psoriasis: a cooperative clinical trial. J Invest Dermatol. 1977;68(6):328–335. doi:10.1111/1523-1747.ep12496022
121. Desgroseilliers JP, Reilly SM, Cullen AE. The importance of patient selection for photochemotherapy in psoriasis. Can Med Assoc J. 1981;124(8):1016–1018.
122. Myers B, Reddy V, Brownstone N, et al. The use of Goeckerman therapy in managing erythrodermic psoriasis resistant to multiple medications. Dermatol Online J. 2021;27(2). doi:10.5070/D3272052387
123. Polat Ekinci A, Boluk KN, Babuna Kobaner KG. Secukinumab and acitretin as a combination therapy for three clinical forms of severe psoriasis in multi-drug refractory patients: a case series of high efficacy and safety profile. Dermatol Ther. 2021;34(1):e14704. doi:10.1111/dth.14704
124. Kokelj F, Plozzer C, Torsello P, et al. Efficacy of cyclosporine plus etretinate in the treatment of erythrodermic psoriasis (three case reports). J Eur Acad Dermatol Venereol. 1998;11(2):177–179.
125. Kuijpers AL, Van Dooren-Greebe JV, Van De Kerkhof PC. Failure of combination therapy with acitretin and cyclosporin A in 3 patients with erythrodermic psoriasis. Dermatology. 1997;194(1):88–90. doi:10.1159/000246070
126. Van Der Vleuten CJ, Gerritsen MJ, Steijlen PM, et al. A therapeutic approach to erythrodermic psoriasis: report of a case and a discussion of therapeutic options. Acta Derm Venereol. 1996;76(1):65–67. doi:10.2340/00015555766567
127. Heikkila H, Ranki A, Cajanus S, et al. Infliximab combined with methotrexate as long-term treatment for erythrodermic psoriasis. Arch Dermatol. 2005;141(12):1607–1610. doi:10.1001/archderm.141.12.1607
128. Kapoor DM, Tan KW. Erythrodermic psoriasis peculiarly sparing anti-TNF injection sites in a patient with secondary loss of efficacy. Dermatol Ther. 2017;30(6):e12551. doi:10.1111/dth.12551
129. Reynolds KA, Pithadia DJ, Lee EB, et al. A systematic review of treatment strategies for erythrodermic psoriasis. J Dermatol Treat. 2021;32(1):49–55. doi:10.1080/09546634.2019.1689228
130. Lo Y, Tsai TF. Updates on the Treatment of Erythrodermic Psoriasis. Psoriasis. 2021;11:59–73. doi:10.2147/PTT.S288345
131. Bangert CA, Costner MI. Methotrexate in dermatology. Dermatol Ther. 2007;20(4):216–228. doi:10.1111/j.1529-8019.2007.00135.x
132. Guenther LC, Kunynetz R, Lynde CW, et al. Acitretin use in dermatology. J Cutan Med Surg. 2017;21(3_suppl):2S–12S. doi:10.1177/1203475417733414
133. Xu JM, Wang HM, Jin HZ. An update on therapeutic options for palmoplantar pustulosis: a narrative review and expert recommendations. Expert Rev Clin Immunol. 2023;19(5):499–516. doi:10.1080/1744666X.2023.2185775
134. Shavit E, Shear NH. An update on the safety of apremilast for the treatment of plaque psoriasis. Expert Opin Drug Saf. 2020;19(4):403–408. doi:10.1080/14740338.2020.1744562
135. Mclornan DP, Pope JE, Gotlib J, et al. Current and future status of JAK inhibitors. Lancet. 2021;398(10302):803–816. doi:10.1016/S0140-6736(21)00438-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is Tofacitinib Effectiveness in Patients with Rheumatoid Arthritis Better After Conventional Than After Biological Therapy? – A Cohort Study in a Colombian Population
Santos-Moreno P, Martinez S, Ibata L, Villarreal L, Rodríguez-Florido F, Rivero M, Rojas-Villarraga A, Galarza-Maldonado C
Biologics: Targets and Therapy 2022, 16:107-117
Published Date: 13 July 2022
Nail Psoriasis: An Updated Review of Currently Available Systemic Treatments
Battista T, Scalvenzi M, Martora F, Potestio L, Megna M
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1899-1932
Published Date: 24 July 2023
Management Strategies for Pediatric Moderate-to-Severe Plaque Psoriasis: Spotlight on Biologics
Ruggiero A, Portarapillo A, Megna M, Patruno C, Napolitano M
Pediatric Health, Medicine and Therapeutics 2023, 14:435-451
Published Date: 14 November 2023
A Case of Erythrodermic Psoriasis Successfully Treated with Risankizumab
Megna M, Ruggiero A, Salsano A, Lauletta G, Portarapillo A, Torta G, Martora F, Potestio L
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3503-3507
Published Date: 5 December 2023