Back to Journals » Biologics: Targets and Therapy » Volume 16
Is Tofacitinib Effectiveness in Patients with Rheumatoid Arthritis Better After Conventional Than After Biological Therapy? – A Cohort Study in a Colombian Population
Authors Santos-Moreno P ![]() , Martinez S, Ibata L, Villarreal L, Rodríguez-Florido F
, Martinez S, Ibata L, Villarreal L, Rodríguez-Florido F ![]() , Rivero M, Rojas-Villarraga A, Galarza-Maldonado C
, Rivero M, Rojas-Villarraga A, Galarza-Maldonado C
Received 11 February 2022
Accepted for publication 28 June 2022
Published 13 July 2022 Volume 2022:16 Pages 107—117
DOI https://doi.org/10.2147/BTT.S361164
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Pedro Santos-Moreno,1 Susan Martinez,1 Linda Ibata,1 Laura Villarreal,1 Fernando Rodríguez-Florido,1 Manuel Rivero,1 Adriana Rojas-Villarraga,2 Claudio Galarza-Maldonado3
1Scientific Department, Biomab IPS SAS, Bogotá, Colombia; 2Research Institute, Fundación Universitaria de Ciencias de la Salud–FUCS, Bogotá, Colombia; 3Unit of Rheumatic and Autoimmune Diseases UNERA, Mont Sinai Hospital, Cuenca, Ecuador
Correspondence: Pedro Santos-Moreno, Scientific and Research Director, Rheumatology, Scientific department, Biomab IPS SAS, Calle 48 #13– 86, Bogotá, Colombia, Tel +57 320 8094232, Email [email protected]
Purpose: Tofacitinib is recommended for treatment of rheumatoid arthritis (RA) in patients with moderate to severe disease activity, but there is not enough evidence on its effectiveness after conventional DMARDs vs its use after biologics. The aim was evaluating the effectiveness of tofacitinib in RA as first-line treatment (after conventional DMARDs) in a real-life setting in Colombian (Latin-American) patients.
Patients and Methods: Retrospective cohort study conducted at a specialized center for RA management. A complete statistical analysis was performed to compare the values of the change in the DAS28 at months 3, 6, and 12 in both treatment groups.
Results: A total of 152 RA patients who received tofacitinib: first-line 85 patients (55.9%) after failure on conventional DMARDs or second-line 67 patients (44.1%) after failure on biologic DMARDs. Comparative analysis of response to treatment showed a reduction in DAS28 at 3, 6, and 12 months in both study groups without statistical differences, but a higher proportion of first-line patients achieved remission (45% vs 23%). Nonresponse at three months were associated with no response at six months of follow-up. Baseline DAS28 was significantly associated with response at 12 months (OR: 1.87, 95%CI: 1.06– 3.30, p-value 0.028). In second-line patients, response to tofacitinib was not related to number of biologic DMARDs previously used.
Conclusion: Tofacitinib is an effective treatment option for patients with RA, maybe better after conventional DMARDs than after biologic therapy failure. Further studies are required to determine the role of tofacitinib in different lines of RA treatment and in other groups of patients.
Keywords: tofacitinib, rheumatoid arthritis, treatment, biologics
Introduction
Rheumatoid arthritis (RA) is an autoimmune and disabling disease with a chronic course and increasing morbidity and mortality rate around the world. Estimations indicate that up to 1% of the world’s population is affected.1 Both the clinical burden of the disease and its economic impact require research into the therapy effectiveness to maximize clinical outcomes in affected patients. Studies have shown that a significant proportion of patients may have inadequate responses to conventional management, and up to half of patients, undergoing biologic therapy, may not achieve expected clinical improvement, according to the American College of Rheumatology (ACR) criteria.2
Tofacitinib is the first oral Janus kinase inhibitor approved to treat RA.3 The efficacy and safety of tofacitinib 5 mg and 10 mg twice daily (BID), administered as monotherapy or in combination with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), in patients with moderate to severe active RA, has been demonstrated in randomized controlled trials (RCTs) phase 24,5 and Phase 36–10 for up to 24 months, and in long-term studies for up to nine years of observation.11,12 According to this evidence, this small-molecule is currently recommended by American College of Rheumatology (ACR) as well as the European Alliance of Associations for Rheumatology (EULAR) like an alternative to biologic DMARDs (bDMARDs) when a patient remains with moderate or high disease activity after the use of csDMARD, usually methotrexate, in patients with established RA.13–15
Early identification of nonresponse is required in the context of optimal direct treatment in RA; however, few real-life studies examine the therapeutic results of tofacitinib in biologic-naïve patients and those who have received biological therapy, considering factors that may be related to treatment response. Therefore, evaluating effectiveness of specific RA medications in a different population is relevant.
This study presents an analysis of a cohort of Colombian RA patients with the aim of evaluating the effectiveness of tofacitinib, both in the first-line (after using csDMARD) and at the second-line, after biologic therapy failure in a real-life setting. It also aims to explore factors related to the achievement of decreased activity disease or control/remission of the disease, when using tofacitinib up to one year of follow-up.
Materials and Methods
Study Design and Population
This is a retrospective cohort study conducted at a specialized center or RA in Colombia. Institutional databases from 2017 to 2019 were used to choose and study patients with RA and a recent indication of tofacitinib, regardless of their previous treatment or disease status. Indication and initiation of tofacitinib was an independent medical decision made as part of the individualized management of the patient. The decision was based on the disease activity assessment, considering the indications and contraindications of the medicine. Patients who did not start the treatment and those who did not complete three months of follow-up were excluded from this study. Effectiveness was evaluated in those patients who met the high adherence criteria (at least three visits with a rheumatologist per year), without increasing the dose or frequency of the index drug and without a new dose or dose increased of oral glucocorticoids.
Concerning the use of the medicine, tofacitinib was administered 5 mg BID or 11 mg once daily as a monotherapy or in combination with some csDMARDs. The drug was also administered as first-line treatment after failure with csDMARDs or as a second-line treatment after one or more biological drugs with inadequate response including: ineffectiveness, efficacy loss, or adverse events. Medicines used as treatment against RA in the cohort included: csDMARD (methotrexate, sulfasalazine, leflunomide, hydroxychloroquine, and chloroquine), TNFi (adalimumab, etanercept, infliximab, certolizumab, and golimumab) with or without csDMARD, non-TNF biologicals like (abatacept, rituximab, and tocilizumab) with or without csDMARD, and tofacitinib, as the subject matter of this study, with or without csDMARD.
Discontinuation of drug, defined as withdrawal of tofacitinib due to an adverse event, lack or loss efficacy, or loss of follow-up prior to the end of the 12-month follow-up period, was recorded. Patients may also be receiving other drugs to control their symptoms (including non-steroidal anti-inflammatory drugs, COX-2 inhibitors and/or opioids) and corticosteroids (≤10 mg prednisone or equivalent/day).
For each patient, sociodemographic characteristics and aspects related to RA, such as duration, stage and activity of disease and concomitant medicine use, were recorded.
Endpoint
Therapy effectiveness was assessed by estimating the change in disease activity through DAS28 at an initial measurement and at 3, 6, and 12 months of treatment. According to DAS28 scores, patients were classified as remission (DAS28 <2.6), low disease activity (DAS28 between 2.6 and 3.2), moderate activity (DAS28 >3.2 and ≤5.1), or high activity (DAS28 >5.1.)16 Response analyses were performed according to the change in DAS28: a reduction in activity level or to remain in low activity or remission was considered effective therapy. A DAS28 ≤3.2 was considered an indicator of disease control.
Therapeutic outcomes at follow-up were compared between the first-line tofacitinib group (no experience with biologicals) and the second-line tofacitinib group (after biologic therapy failure). For the analysis, each patient contributed to therapy event.
Analysis Methods
Frequencies and proportions in baseline characteristics were calculated in each group of treatment and in the total population. Differences in disease activity between the first- and second-line tofacitinib treatment groups were also estimated. Comparisons of continuous variable data between the two patient groups were made using the t-test of independent measurements (Mann–Whitney U-test was used for independent samples when presenting non-normal distribution). The chi-squared test and Fisher’s exact test were used for statistical analysis of categorical variables. To compare the values of the change in the DAS28 in months 3, 6, and 12, the missing data on patients without continuity in follow-up were replaced by the last observed values. A subgroup analysis was performed for those who had received tofacitinib after a biological vs two or more biologicals.
For all tests, a p-value <0.05 was considered to indicate statistical significance. Variables with statistical significance in the analysis or those of great clinical interest or plausibility in relation to response to therapy were included in multivariate analyses. Logistic regressions were performed to analyze the influence of individual, clinical, and pharmacological factors with therapeutic response outcomes at 6 and 12 months in patients with moderate to high disease activity. All calculations were performed using PASW statistics software version 25.
Ethical Aspects
According to Resolution 8430 of 1993 from the Ministry of Health of Colombia, this research presents no risks to patients; therefore, this study does not need approval from the ethics committee. The authors adhered to the Declaration of Helsinki in all aspects of ethics in investigation. This study was approved by the Institutional Review Board of BIOMAB IPS – Center for Rheumatoid Arthritis, record number 006–20, October 29, 2020 (code GC.IN.01.FR.03). All patients had previously signed informed consent for data use; the database was anonymized to protect the confidentiality and privacy of patients.
Results
A total of 152 patients with RA who received tofacitinib were included, they had a previous inadequate response including primary failure or loss of efficacy. Eighty-five (55.9%) patients received first-line treatment (T1) and 67 (44.1%) received second-line treatment (T2). Women were predominant in both groups (78.6% of the total). Patients were between 25 and 83 years old, but T1 group was younger than patients in T2 group (53±12.8 years old and 59±11.4 years old, respectively, p-value 0.01). The most frequent concomitant pathology at diagnosis time of RA was hypertension affecting a quarter of the individuals.
In patients who received first-line tofacitinib, an average of 11.8 years of disease (from onset of symptoms) was reported and 15.5 years in those who received tofacitinib as second-line (p-value 0.003).
Table 1. describes patients characteristics at diagnosis according to the treatment line. Patients who were in moderate or high disease activity according to DAS28 level were 77%. There were no statistically significant differences in baseline disease characteristics between treatment groups; including disease activity measured with DAS28, hand and foot radiography, and baseline values for C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), rheumatoid factor (RF), and anticitrullinated antibodies (anti-CCP). Patients in each treatment line received two different doses of tofacitinib, as first-line 50.6% of patients received 5 mg twice daily and 49.4% received 11 mg once daily doses; as a second-line 65.7% of patients received 5 mg twice daily, and 34.3% of patients the 11 mg once daily doses.
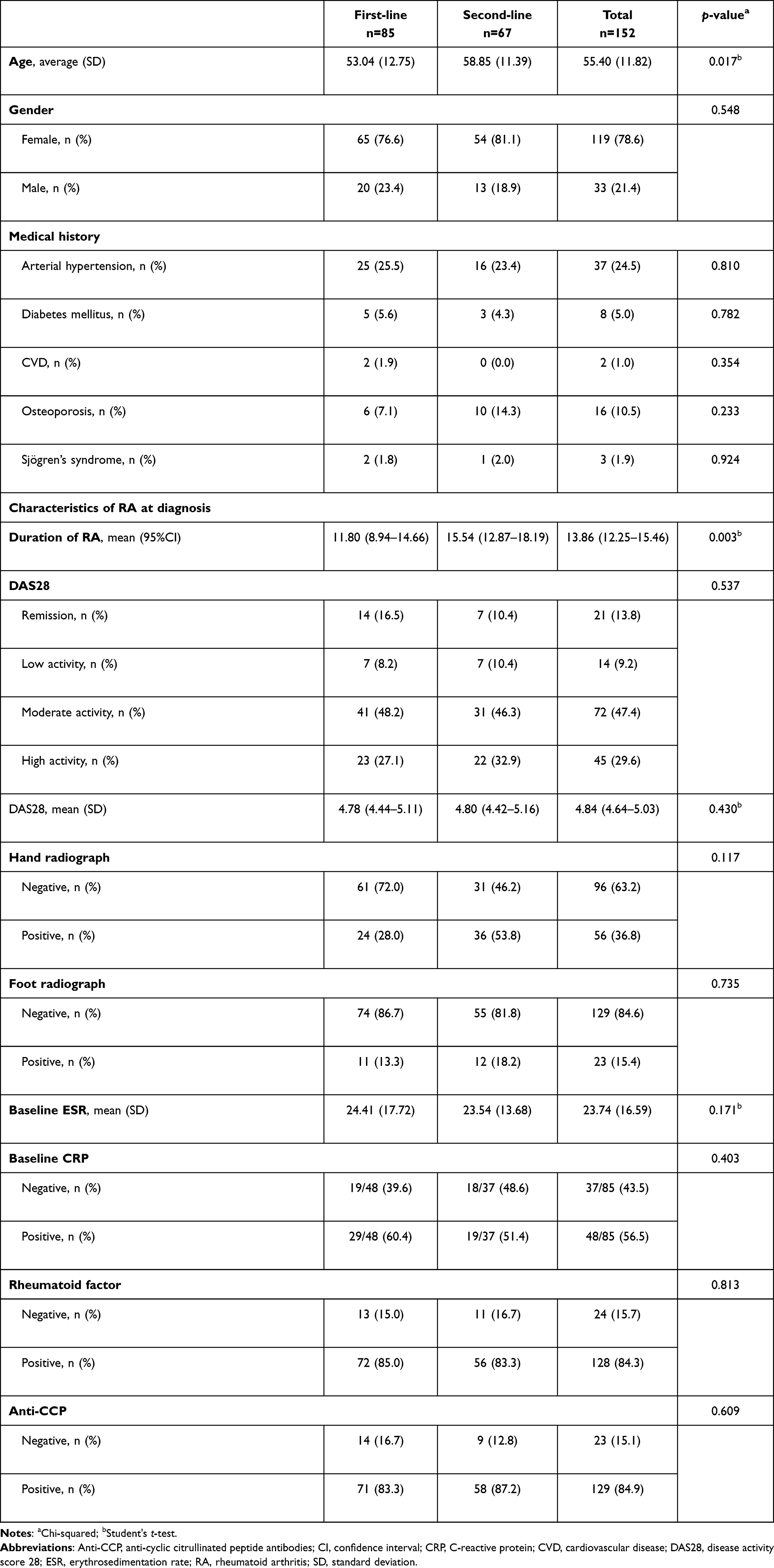 |
Table 1 Baseline Characteristics of Patients by Treatment Line |
Treatment response was assessment in patients who were initially classified with moderate or high disease activity at 3, 6, and 12 months with the change in DAS28 (Table 2.) The comparative analysis of treatment response showed a reduction in DAS28 at three and six months of treatment in both study groups, with no statistically significant differences between them. At 12 months of treatment, although both groups showed disease response and control according to the DAS28 from baseline, a higher proportion of T1 patients achieved remission (45% vs 23%). A subgroup analysis to evaluate second-line tofacitinib therapy showed no statistically significant differences in any response criteria according to the number of previously received biologicals.
 |
Table 2 Response at 3, 6, and 12 Months Depending on Treatment Line |
A logistic regression analysis was performed to evaluate the relationship of different factors with the disease response measured by the DAS28 at 6 and 12 months (Table 3.) At the multivariate analysis, the use of tofacitinib as first-line of treatment showed a tendency toward a lower response at six months (OR: 0.21, 95%CI: 0.06–0.76, p-value 0.018) but not at 12 months. The response in disease activity at three months was a major factor related to six-month response (OR: 15.63, 95%CI: 4.38–55.74, p-value 0.000), while the initial DAS28 was significantly associated with response at 12 months of treatment. (Table 3).
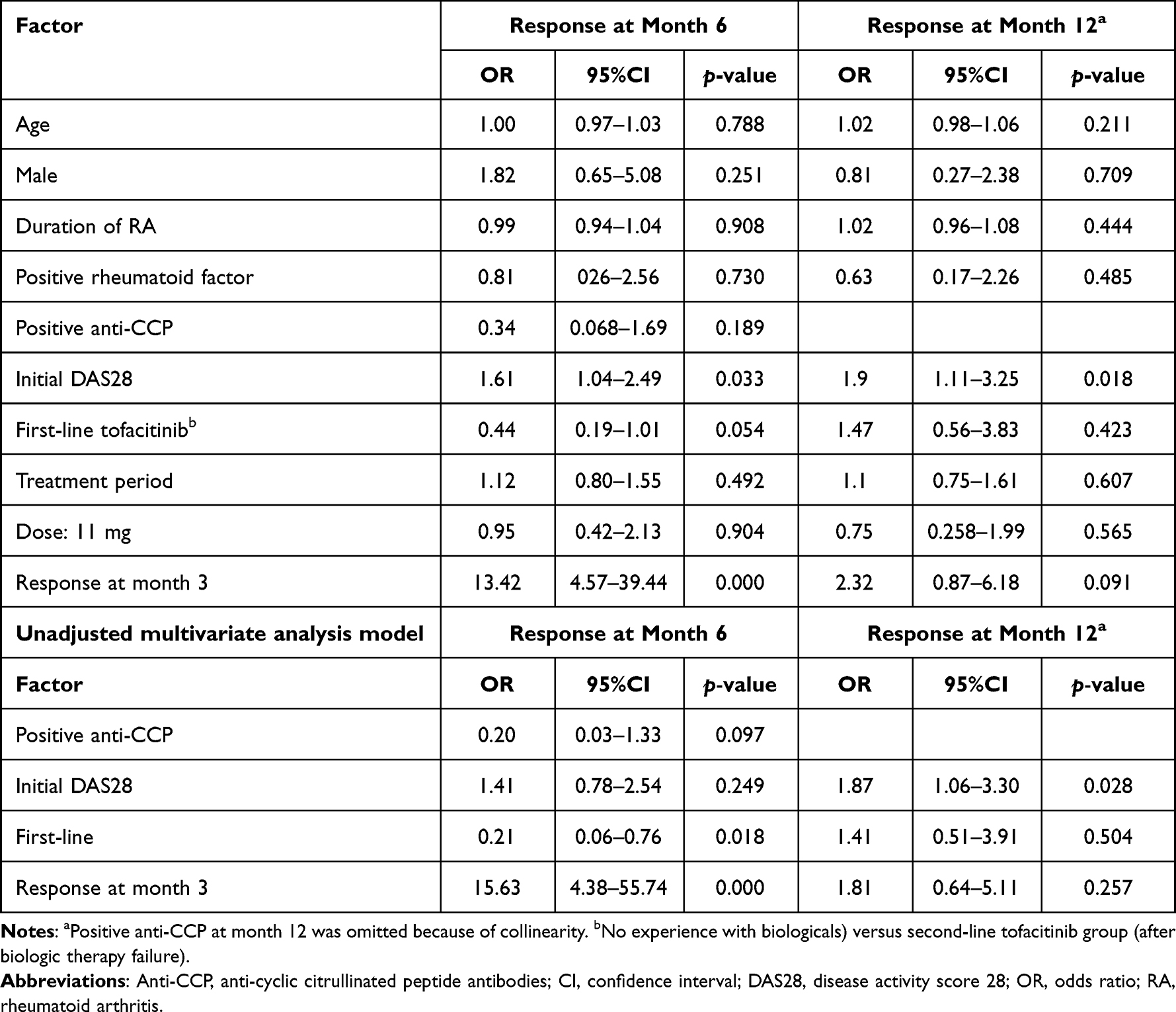 |
Table 3 Regression Analysis to Estimate the Risk of Response of the Disease at 6 and 12 Months of Treatment with Tofacitinib (Adjusted Model) |
Discussion
This study shows outcomes of one-year follow-up on patients with RA who received tofacitinib treatment. The frequency of established monitoring was determined accordingly by clinical guidelines that recommend frequent follow-up on patients with active disease to closely monitor disease activity and adjust treatment accordingly.13,14 The guidelines of the EULAR14 specify follow-up every one to three months with more frequent monitoring on patients with high disease activity and suggest that if no improvement is observed within three months or if the treatment target is not reached within six months, treatment should be changed.
In the case of tofacitinib, the documentation of real-world experiences in its use against RA is relatively recent,17 derived from use in countries where tofacitinib has been available in clinical practice for several years. The analysis derived from this data has been aimed at understanding treatment patterns and patient outcomes and characterizing the safety profile of tofacitinib.9,12,17,18 Similarly, reviews of 6 or 12-month studies on the use of biologics or tofacitinib, in monotherapy or in combination, have shown their efficacy (functionality and remission of the disease) in persons with RA who had previously experienced and failed treatment with methotrexate or other DMARDs,19 and in persons with RA who had previously experienced failure with biological treatment.19 In this context, this study provides useful information on cohort results considering the use of tofacitinib in patients who have not received biological therapy, as in those who have previously received biologicals in the management of their RA.
The findings of this study show disease response in both treatment groups. In 2018, Mori et al20 published a study that directly compared the results of tofacitinib therapy in methotrexate-refractory RA between patients without biologic treatment (36 subjects) and patients who had experienced inadequate response to biological agents (77 patients). There, clinical disease activity evaluated at six months with the Clinical Disease Activity Index (CDAI) found an association of previous use of biological agents with failure to achieve therapeutic response (OR: 4.48, p=0.002) and the number of previous biological agents was twice as large in nonresponders as in responders (p<0.001); patients without biological experience achieved remission more quickly and in greater proportion (41.7% vs 11.7%, p=0.001). In contrast, our study showed no statistically significant differences in patients with moderate and high disease activity with the use of second-line tofacitinib, or in relation to the number of previous biological agents. These dissimilar results can be attributed to differences in scales and estimation of response between studies, indicating in both cases the efficacy of tofacitinib in patients with difficult-to-manage RA.
Multivariate logistic regression analysis, which explored the relationships of several possible factors with disease response, found that three-month response is an indicator of six-month response, similar to previous study findings. A post hoc analysis of two randomized, double-blind, Phase III studies explored early changes in disease activity and achievement of low activity and remission goals with tofacitinib.21 In patients with an inadequate response to methotrexate, the lack of response to tofacitinib after one or three months predicted a low probability of achieving low disease activity by month six.21 These results are important in guiding decision-making for continued treatment with tofacitinib in the face of a lack of early response, and stress the need to include this measurement early in the therapeutic evaluation of patients with RA. Also, the multivariate analysis showed that the use of tofacitinib as first-line of treatment had a tendency toward significancy a lower response at six months but not at 12 months, showing that the use of tofacitinib achieves responses per year of treatment regardless of its use after conventional or biological therapy, as shown in other studies.17
Considering that ancestry is one of the factors that define autoimmune tautology,22,23 evaluating the effectiveness of RA medications, according to ancestry, is relevant, since different responses may occur depending on the population in question. Indeed, the tofacitinib dose-response or effectiveness between patients of different ancestries has been evaluated (ie Japanese, Chinese, Western among others)24–26 in addition to the evaluation of security profile according to ancestry.27 This is one of the first studies analyzing the tofacitinib effectiveness in RA patients after conventional or biological therapy in Colombian patients (Latino population). Although the information regarding this topic is scarce in the Latino population, there are studies that evaluate the effectiveness and safety of tofacitinib in the Latin-American population compared with the rest of the world.28 This is important because of the particular RA outcomes in this population when compared with different populations.
In the present study, patients who received first-line tofacitinib had a shorter duration of disease than patients who received tofacitinib as second-line therapy. This result was similar to the outcomes described in the Corrona registry, they showed that patients that start tofacitinib had longer disease duration.17 Fleischmann et al compared efficacy and safety of tofacitinib in patients with early disease (defined as a disease duration less than one year) versus established disease (defined as a disease duration more than one year), they found that ACR response rates, were higher in patients with tofacitinib use versus methotrexate, and at 12 months there were higher response rates in patients with early established disease that used tofacitinib.29 In this study, patients in the T1 group (that had fewer years with the disease) showed a slight decrease in the number of those with moderate disease activity, 42 (50%) to 30 (35%) at 6 and 12 months, respectively compared with the T2 group, 30 (45.8%) to 38 (45.8%) at 6 and 12 months, respectively, that had lower DAS28 response. Therefore, the duration of the disease becomes important not only at the response under tofacitinib treatment measured by the activity of the disease, but also in how well the patient preserves their functionality and how radiographic compromise progresses.29
This study is subject to some limitations such as sample size, those inherent in the measurement instruments used and others inherent in observational studies, including channeling bias or confounding by indication bias. Regarding those biases, although we performed multivariate logistic regression analysis to adjust for confounding variables, we did not include a propensity score in those analyses, so the results should be interpreted in the light of these limitations. In conclusion, tofacitinib alone or in combination is an effective treatment option for patients with RA after csDMARD and in patients who have failed prior treatment with biologic therapy. The findings in monitoring the response measured by the DAS28 highlight the importance of early response in the predictability of medium- and long-term response. Further studies will help determine the role of tofacitinib in the treatment of patients with RA in the different treatment lines and expand the exploration of factors related to therapeutic success.
Conclusion
In conclusion, the present research shows that tofacitinib is not only effective after conventional DMARDs, but also after biological therapy, this regardless of the number of prior biologics used. In addition, the comparative analysis of treatment response showed a reduction in DAS28 at 3, 6, and 12 months of treatment in both study groups under tofacitinib treatment (after csDMARDs and after biologics), without statistically significant differences between them, but a higher proportion of patients after csDMARDs achieved remission in disease activity. Finally, the response in disease activity at three months was a major factor related to consecutive months (six-month response, and maybe also to 12-month response); therefore, it could be suggested that there is predictability in the response to tofacitinib at three months in this population.
Data Sharing Statement
The authors declare that the database and other study materials are available for review at any time. All files, databases and other documents related to the study are available on a computer in our research office and with access only to the team of researchers. In any case, please contact PSM.
Acknowledgments
We thank Anggie Aza, Fernando Rodriguez-Florido, and Biomab IPS for the administrative data provided for this study. An abstract of this work/paper was presented and published as an abstract at EULAR2021 (Annual European Congress of Rheumatology), with interim findings. The poster’s abstract was published in: Ann Rheum Dis, volume 80, supplement 1, year 2021, page 1163 – Tofacitinib effectiveness in patients with rheumatoid arthritis after conventional or biological therapy – it real role in different lines of treatment http://dx.doi.org/10.1136/annrheumdis-2021-eular.3770. We thank Gabriel-Santiago Rodríguez-Vargas for the final review of the paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
PSM has received fees for conferences, counseling, advisory boards, and also travel to academic meetings expenses and research grants in the last five years from: Abbvie, Abbott, Biopas-UCB, Bristol, Janssen, Lilly, Pfizer, Roche, Sanofi. ARV has received fees for conferences, counseling or advisory boards in the last five years from: Abbvie, Amgen, Biopas-UCB, Bristol, Glaxo, Janssen, Pfizer. The authors report no other conflicts of interest in this work.
References
1. van der Woude D, van der Helm-van Mil AHM. Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2018;32(2):174–187. doi:10.1016/j.berh.2018.10.005
2. Romão VC, Vital EM, Fonseca JE, Buch MH. Right drug, right patient, right time: aspiration or future promise for biologics in rheumatoid arthritis? Arthritis Res Ther. 2017;19(1):239. doi:10.1186/s13075-017-1445-3
3. Rocha CM, Alves AM, Bettanin BF, et al. Current jakinibs for the treatment of rheumatoid arthritis: a systematic review. Inflammopharmacology. 2021;29(3):595–615. doi:10.1007/s10787-021-00822-x
4. Fleischmann R, Cutolo M, Genovese MC, et al. Phase IIb dose-ranging study of the oral JAK inhibitor tofacitinib (CP-690,550) or Adalimumab monotherapy versus placebo in patients with active rheumatoid arthritis with an inadequate response to disease-modifying antirheumatic drugs. Arthritis Rheum. 2012;64(3):617–629. doi:10.1002/art.33383
5. Kremer JM, Cohen S, Wilkinson BE, et al. A phase IIb dose-ranging study of the oral JAK inhibitor tofacitinib (CP-690,550) versus placebo in combination with background methotrexate in patients with active rheumatoid arthritis and an inadequate response to methotrexate alone. Arthritis Rheum. 2012;64(4):970–981. doi:10.1002/art.33419
6. Burmester GR, Blanco R, Charles-Schoeman C, et al. Tofacitinib (CP-690,550) in combination with methotrexate in patients with active rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitors: a randomised phase 3 trial. Lancet. 2013;381(9865):451–460. doi:10.1016/S0140-6736(12)61424-X
7. Van Der Heijde D, Tanaka Y, Fleischmann R, et al. Tofacitinib (CP-690,550) in patients with rheumatoid arthritis receiving methotrexate: twelve-month data from a twenty-four-month phase III randomized radiographic study. Arthritis Rheum. 2013;65(3):559–570. doi:10.1002/art.37816
8. Cohen SB, Pope J, Haraoui B, et al. Efficacy and safety of tofacitinib modified-release 11 mg once daily plus methotrexate in adult patients with rheumatoid arthritis: 24-week open-label phase results from a phase 3b/4 methotrexate withdrawal non-inferiority study (ORAL Shift). RMD Open. 2021;7(2):e001673. doi:10.1136/rmdopen-2021-001673
9. Burgos-Vargas R, Cardiel M, Xibillé D, et al. Tofacitinib, an oral Janus kinase inhibitor, in patients from Mexico with rheumatoid arthritis: pooled efficacy and safety analyses from Phase 3 and LTE studies. Reumatol Clin. 2019;15(1):43–53. doi:10.1016/j.reuma.2017.04.006
10. Radominski SC, Cardiel MH, Citera G, et al. Tofacitinib, un inhibidor oral de la quinasa Janus, para el tratamiento de artritis reumatoide en pacientes de Latinoamérica: eficacia y seguridad de estudios fase 3 y de extensión a largo plazo. Reumatol Clin. 2017;13(4):201–209. doi:10.1016/j.reuma.2016.04.010
11. Wollenhaupt J, Silverfield J, Lee Prof EB, et al. Safety and efficacy of tofacitinib, an oral janus kinase inhibitor, for the treatment of rheumatoid arthritis in open-Label, long term extension studies. J Rheumatol. 2014;41(5):837–852. doi:10.3899/jrheum.130683
12. Cohen SB, Tanaka Y, Mariette X, et al. Long-term safety of tofacitinib up to 9.5 years: a comprehensive integrated analysis of the rheumatoid arthritis clinical development programme. RMD Open. 2020;6(3):e001395. doi:10.1136/rmdopen-2020-001395
13. Singh JA, Saag KG, Bridges SL, et al. 2015 American College of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res. 2016;68(1):1–25. doi:10.1002/acr.22783
14. Smolen JS, Landewé RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):S685–S699. doi:10.1136/annrheumdis-2019-216655
15. Fraenkel L, Bathon JM, England BR, et al. 2021 American College of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res. 2021;2021:1–16. doi:10.1002/acr.24596
16. England BR, Tiong BK, Bergman MJ, et al. 2019 update of the American College of rheumatology recommended rheumatoid arthritis disease activity measures. Arthritis Care Res. 2019;71(12):1540–1555. doi:10.1002/acr.24042
17. Caporali R, Zavaglia D. Real-world experience with tofacitinib in RA. Clin Exp Rheumatol. 2019;37(37):485–495.
18. Álvaro-Gracia JM, García-Llorente JF, Valderrama M, Gomez S, Montoro M. Update on the safety profile of tofacitinib in rheumatoid arthritis from clinical trials to real-World studies: a narrative review. Rheumatol Ther. 2021;8(1):17–40. doi:10.1007/s40744-020-00258-9
19. Singh JA, Hossain A, Mudano AS, et al. Biologics or tofacitinib for people with rheumatoid arthritis naive to methotrexate: a systematic review and network meta-analysis. Cochrane Database Syst Rev. 2017;2017(5). doi:10.1002/14651858.CD012657
20. Mori S, Yoshitama T, Ueki Y. Tofacitinib therapy for rheumatoid arthritis: a direct comparison study between biologic-naïve and experienced patients. Intern Med. 2018;57(5):663–670. doi:10.2169/internalmedicine.9341-17
21. van Vollenhoven RF, Lee EB, Fallon L, et al. Tofacitinib in rheumatoid arthritis: lack of early change in disease activity and the probability of achieving low disease activity at month 6. Arthritis Care Res. 2019;71(1):71–79. doi:10.1002/acr.23585
22. Anaya JM. The autoimmune tautology. A summary of evidence. Jt Bone Spine. 2017;84(3):251–253. doi:10.1016/j.jbspin.2016.11.012
23. Anaya J-M. Common mechanisms of autoimmune diseases (the autoimmune tautology). Autoimmun Rev. 2012;11(11):781–784. doi:10.1016/j.autrev.2012.02.002
24. Suzuki M, Shoji S, Miyoshi S, Krishnaswami S. Model-based comparison of dose-response profiles of tofacitinib in Japanese versus Western rheumatoid arthritis patients. J Clin Pharmacol. 2020;60(2):198–208. doi:10.1002/jcph.1514
25. Li Z-G, Liu Y, Xu H-J, et al. Efficacy and safety of tofacitinib in chinese patients with rheumatoid arthritis. Chin Med J. 2018;131(22):2683–2692. doi:10.4103/0366-6999.245157
26. Suzuki M, Tse S, Hirai M, Kurebayashi Y. Application of physiologically-based pharmacokinetic modeling for the prediction of tofacitinib exposure in Japanese. Kobe J Med Sci. 2016;62(6):E150–E161.
27. Bing N, Zhou H, Chen X, et al. Contribution of a European-prevalent variant near CD83 and an East Asian–Prevalent Variant near IL17RB to Herpes Zoster Risk in tofacitinib treatment: results of genome-wide association study meta-analyses. Arthritis Rheumatol. 2021;73(7):1155–1166. doi:10.1002/art.41655
28. Castañeda OM, Romero FJ, Salinas A, et al. Safety of tofacitinib in the treatment of rheumatoid arthritis in Latin America compared with the rest of the world population. J Clin Rheumatol. 2017;23(4):193–199. doi:10.1097/RHU.0000000000000498
29. Fleischmann RM, Huizinga TWJ, Kavanaugh AF, et al. Efficacy of tofacitinib monotherapy in methotrexate-naive patients with early or established rheumatoid arthritis. RMD Open. 2016;2(2):1–10. doi:10.1136/rmdopen-2016-000262
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Demographic, Physical, and Psychological Determinants of Patient Experience with Subcutaneous Self-Injection in Patients with Rheumatoid Arthritis: Structural Equation Modeling Approach
Onishi A, Kaizu M, Shirasugi I, Yagyu T, Ueda Y, Sakai Y, Miura Y, Saegusa J
Patient Preference and Adherence 2023, 17:1551-1559
Published Date: 3 July 2023
Nail Psoriasis: An Updated Review of Currently Available Systemic Treatments
Battista T, Scalvenzi M, Martora F, Potestio L, Megna M
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1899-1932
Published Date: 24 July 2023
Management Strategies for Pediatric Moderate-to-Severe Plaque Psoriasis: Spotlight on Biologics
Ruggiero A, Portarapillo A, Megna M, Patruno C, Napolitano M
Pediatric Health, Medicine and Therapeutics 2023, 14:435-451
Published Date: 14 November 2023
JAK-Inhibitors – A Story of Success and Adverse Events
Wlassits R, Müller M, Fenzl KH, Lamprecht T, Erlacher L
Open Access Rheumatology: Research and Reviews 2024, 16:43-53
Published Date: 26 February 2024
Update on Erythrodermic Psoriasis: Proposal of a Management Algorithm by an Innovative Severity Evaluation Approach
Xu JM, Wu C, Feng H, Jin HZ
Psoriasis: Targets and Therapy 2025, 15:301-320
Published Date: 19 July 2025