Back to Journals » Cancer Management and Research » Volume 17

Unveiling Psychological Capital Profiles and Their Impact on Quality of Life in Breast Cancer Patients: A Latent Profile Analysis
Received 18 May 2025
Accepted for publication 8 October 2025
Published 22 October 2025 Volume 2025:17 Pages 2429—2440
DOI https://doi.org/10.2147/CMAR.S537692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Bilikere Dwarakanath
Chunying Cui,1 Hairong Liu,1 Lie Wang2
1Department of Management, School of Humanities and Management, Wannan Medical College, Wuhu, Anhui, People’s Republic of China; 2Department of Social Medicine, School of Public Health, China Medical University, Shenyang, Liaoning, People’s Republic of China
Correspondence: Chunying Cui, Email [email protected]
Purpose: Our study aimed to identify the profiles of psychological capital (PsyCap), explore its influencing factors, and examine the association between PsyCap and quality of life (QoL) among breast cancer (BC) patients.
Methods: A total of 229 BC patients completed our survey questionnaire. The questionnaire package included general sociodemographic and clinical information, the Psychological Capital Questionnaire for patients with Cancer (PCQ-C), and the Functional Assessment of Cancer Therapy-Breast (FACT-B). Latent profile analysis was adopted to identify PsyCap profiles. Multivariate logistic regression was used to analyze each profile’s sociodemographic and clinical characteristics, and ANOVA was used to explore the relationships between PsyCap profiles and QoL.
Results: Three profiles of PsyCap were identified, including the low PsyCap, moderate PsyCap, and high PsyCap groups, which comprised 23.1, 48.1, and 28.8% of the sample, respectively. K-means clustering further supported the categorization of PsyCap into three distinct profiles. Regression results showed that the low PsyCap group was more likely to be unemployed, a risk factor affecting BC patients’ PsyCap. Compared with the low PsyCap group, the moderate PsyCap (Beta=0.209, P=0.002) and high PsyCap (Beta=0.664, P< 0.001) groups possessed better QoL.
Conclusion: PsyCap is classifiably heterogeneous among patients with BC, which suggests that healthcare professionals should give full consideration to the impact of unemployment on the PsyCap groups. The PsyCap profiles affected BC patients’ QoL, so healthcare professionals can identify BC patients with poor QoL based on their PsyCap and provide them with psychological counseling services and psychological healing groups to help them improve their mental and physical health.
Keywords: psychological capital, quality of life, latent profile analysis, breast cancer
Introduction
Female breast cancer is the second leading cause of global cancer incidence in 2022, with an estimated 2.3 million new cases, and is the fourth leading cause of cancer mortality in the world, with 666,000 deaths.1 Studies estimated that the burden of BC would grow to over 3 million new cases and 1 million deaths per year by 2040, with the population expanding and aging worldwide.2 BC diagnosis is not only accompanied by physical symptoms (eg, chronic pain, fatigue, and functional limitations), but it also causes adverse psychological effects.3,4 Quality of life (QoL) has become essential in evaluating cancer patients’ health status, including an individual’s physical, functional, psychological, and social well-being.5–7 Studies have shown that BC patients with similar disease severity and treatment status tend to have significant differences in QoL, most likely due to differences in positive psychological resources.8–10
According to the Conservation of Resources (COR) theory,11 a resource is an object or personal characteristic valuable to the individual. The theory emphasizes that losing resources is critical in developing stress; thus, protecting the available resources or acquiring resources is essential in motivation and adaptation.12,13 PsyCap is an individual attribute representing an individual’s psychological strength and, therefore, a resource for adapting and coping with stressful situations, enabling people to thrive.14–17 PsyCap included the dimensions of hope (persevering towards goals, and when necessary, redirecting paths to reach those goals), optimism (making a positive attribution about reaching goals), resilience (withstanding problems and adversity, and rebounding), and self-efficacy (having confidence to take on and succeed at challenging tasks).18 Due to the cultural differences, for a Chinese BC patient, PsyCap is not an individual’s internal asset but a relational and shared resource cultivated within the family system, expressed through endurance and compliance, and directed toward collective well-being rather than individual recovery, compared with Western individualism. Therefore, Chinese therapy or support programs based on PsyCap should engage the family unit, not just the patient. According to the Multiple Resource theory proposed by Hobfoll SE,19 PsyCap is a higher-order internal resource where the core dimensions are related and work together synergistically. Therefore, Luthans et al thought PsyCap had a relatively stronger association with positive effects than individual dimensions.
PsyCap is vital for individuals’ physical and psychological health.20 A longitudinal study presented that some cancer patients had better psychological adaptation in the high-risk cancer treatment. In contrast, others had not, and psychological resources intervention reduced the risk of adjustment problems and improved the positive health outcomes.21 According to Sen’s theory,22 individual resources and capabilities are critical positive factors affecting QoL. Increasing personal resources and improving personal capabilities can significantly enhance QoL. PsyCap is generally considered a positive personal resource that is the foundation for personal development and physical and mental health. Studies found that PsyCap and four dimensions were positively associated with mental health and QoL among cancer patients.23–25 Therefore, our study suggests that positive psychological variables probably could contribute to explaining individual variation in quality of life in BC patients.
Several studies thought the impact of PsyCap facets tends to be more significant when combined than separately.26,27 Previous research on PsyCap has generally employed variable-focused analytic techniques that presuppose an even distribution of patients’ psychological profiles, which ignores individual differences. However, other studies have shown that this distribution is heterogeneous after cancer diagnosis, suggesting that research using variable-focused analytic techniques may not reflect the psychological responses associated with patient heterogeneity.28–30 Research on individual differences helps us understand how different PsyCap classes combine in different BC patients and whether these combinations are associated with individual psychological development. Therefore, a more ideal technique was needed to explore the patterns of PsyCap in BC patients.
Latent profile analysis (LPA) and k-means clustering have commonly been used as grouping methods. LPA is a model-based latent variable approach based on person-focused that identifies unobserved subpopulations where individuals within a profile are similar to each other and distinct from individuals in other profiles based on their pattern of responses across multiple variables. The focus is on classifying people, not variables. These are variable-centered approaches compared to conventional methods (eg, regression analysis and factor analysis). They assume the population is homogeneous and examine how variables relate to one another across the entire population, ignoring the possibility that different subgroups might exist. These approaches lack specificity and may contribute to the poor results.31 Therefore, LPA acknowledges population heterogeneity and is an ideal method to explore social relationship profiles.32 Increasingly, studies based on LPA claim significant individual differences were found in social constraints, social support, and resilience among cancer patients.30,33,34 In addition, K-means clustering is a non-model-based method that is not grounded on an underlying statistical model and typically corresponds to discrete optimization algorithms to optimize across a diverse range of objective criteria.31 Given the markedly different principles underlying these two grouping methods, their results could be mutually verified. Consistent results provide an opportunity to confirm the accuracy and stability of the results.
Therefore, the present study adopted LPA to explore, 1) define distinct BC patients’ PsyCap profiles through LPA and to verify its stability by the k-means clustering method, 2) determine the characteristics of each subgroup by using a range of sociodemographic and clinical variables, and 3) examine the association of these profiles with QoL among BC patients.
Methods
Study Design and Participants
This cross-sectional design study was conducted in Shenyang, Liaoning Province, China, from June 2021 to April 2022. Participants were recruited from the Affiliated Hospital of China Medical University. The inclusion criteria of this study included patients 1) diagnosed with BC, 2) able to understand and communicate in Chinese, and 3) at least 18 years old. The exclusion criteria of this study included that the patients 1) had other severe diseases (such as severe cardiovascular disease), 2) had a history of psychiatry, and 3) had cognitive and intellectual disorders. Each eligible patient will be distributed self-reported questionnaires after signing the informed consent form for this study. Finally, 229 patients effectively completed the survey among 265 BC participants, and the effective response rate of this study was 86.4%. Twenty patients refused this study, and sixteen questionnaires were excluded due to invalid data (missing data > 30%). Therefore, our study had 229 Chinese BC patients. The study was approved by the Committee on Human Experimentation of the First Affiliated Hospital of China Medical University (NO. 2021–430-2).
Measurement of PsyCap
The level of PsyCap was measured using the Chinese version of the Psychological Capital Questionnaire for patients with Cancer (PCQ-C)35 in the present study. The scale contains 24 items and is divided into four dimensions: resilience, self-efficacy, optimism, and hope. Each item of the PCQ-C adopts a 5-point Likert-type scale varying from “1=very strongly disagree” to “5=very strongly agree”, and higher scores mean a higher level of PsyCap. The Cronbach’s coefficient for the PCQ-C was 0.911 in the present study.
Measurement of QoL
The present study adopted the Chinese version of Functional Assessment of Cancer Therapy-Breast (FACT-B)36 to evaluate QoL among patients with BC. The scale contains 38 items and is divided into five dimensions, including physical well-being (PWB), emotional well-being (EWB), social/family well-being (SFWB), functional well-being (FWB), and concerns about BC (BCS).37 It is rated on a five-point scale from 0 (not at all) to 4 (extremely). The FACT-B total score = PWB + SWB + EWB + FWB + BCS, with higher scores indicating better QoL.38 The Cronbach’s coefficient for the FACT-B was 0.902 in this study.
Demographic and Clinical Information
The present study also included demographic information, including age, marital status, educational background, employment status, monthly income, and smoking status. Clinical information included distant metastasis and the final stage of cancer.
Statistical Analysis
First, descriptive statistics were used to describe participants’ demographic and clinical variables using frequency, percentage, mean, and SD.
Second, a PLA was performed to identify the specific patterns of PsyCap among BC patients in Mplus 8.0 software. To evaluate model fit and determine the optimal class solution, two- to five class groups were developed and compared according to a series of statistical indicators: (a) Lower Akaike information criterion (AIC), Bayesian information criterion (BIC), adjusted Bayesian information criterion (aBIC), with lower values indicating better model fit; (b) higher entropy values;39 (c) significant Lo-Mendell-Rubin (LMR) and the Bootstrap Likelihood Ratio Test (BLRT).40
Third, k-means clustering was used to validate the reliability of the LPA classification method. The optimal cluster number solution was determined by the elbow test. The elbow test determined the optimal cluster number solution. The elbow method ran k-means clustering on the dataset for a range of values for k, and for each value of k, the sum of squared errors (SSE) was calculated. The optimal number is the elbow position.41
Fourth, the chi-square test was used to analyze demographic and clinical characteristics of PsyCap among BC patients. Fifth, our study performed multivariable logistic regression analysis to examine the influence of sociodemographic and clinical characteristics on different profiles of PsyCap among patients with BC. Sixth, the Kruskal–Wallis test was used to explore the relationship between the profiles of PsyCap and QoL. Finally, multiple linear regression was conducted to analyze the relationship between the profiles of PsyCap and QoL.
Results
Descriptive Statistics
Table 1 displays the sociodemographic and clinical information among 229 patients with BC. The mean age of participants was 47.62 years (SD=10.65). Out of these patients, 79.5% were married or cohabited. 64.6% of patients were senior middle school or above, and 40.2% of participants had a monthly income of <3000 yuan (CNY). More than 50% of patients had distant metastasis. BC patients were diagnosed at stage I (36.7%), and stage II/III (63.3%) in the final stages.
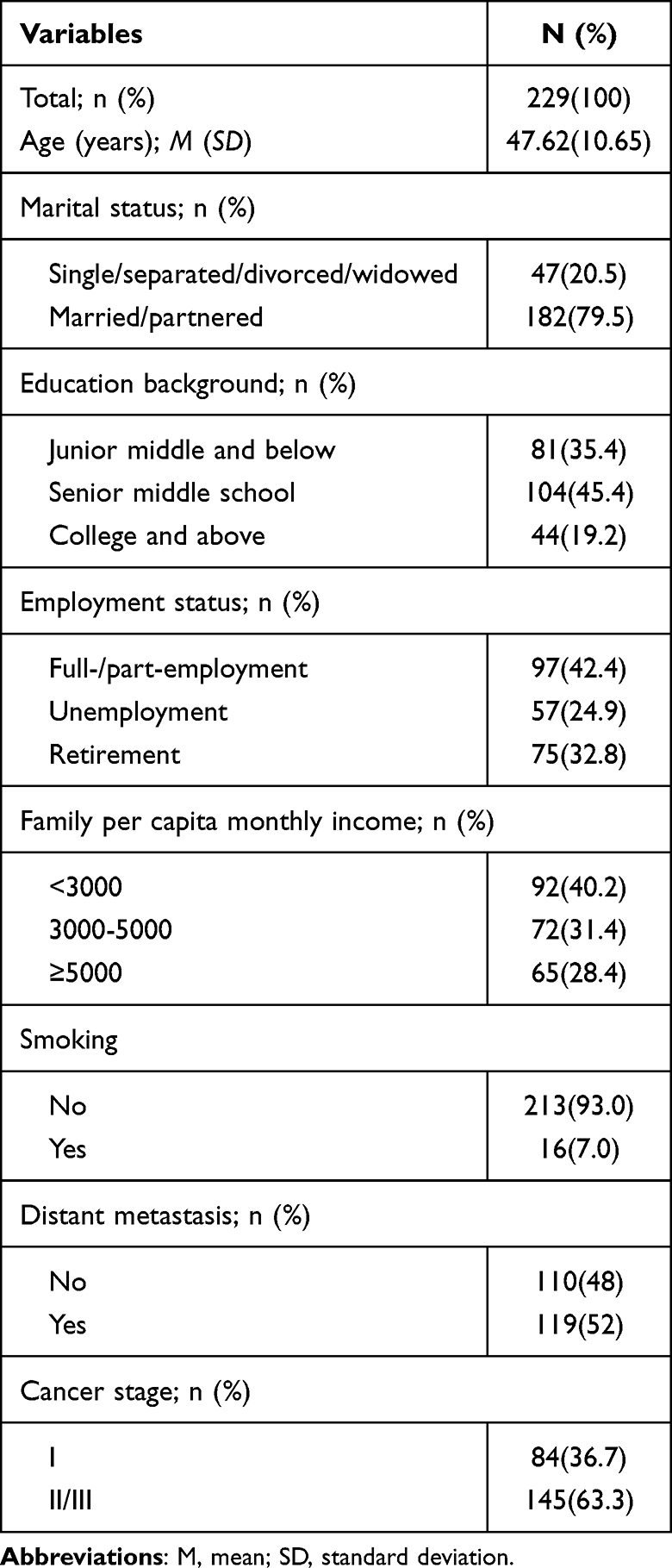 |
Table 1 BC Patients’ Demographic and Clinical Characteristics |
Latent Profile Analysis
Table 2 presents the latent class solution of PsyCap in BC patients. The four- and five-class models had lower AIC, BIC, and aBIC values than the two- and three-class models. However, the two- and three-class had significant LMR values compared with the four- and five-class models. The three classes had lower AIC, BIC, and BIC values. The entropy value was >0.7 in all classes, suggesting a relatively accurate classification. In addition, BLRT values in all classes were significant. Therefore, our study chose the three-class patterns model as the optimal solution.
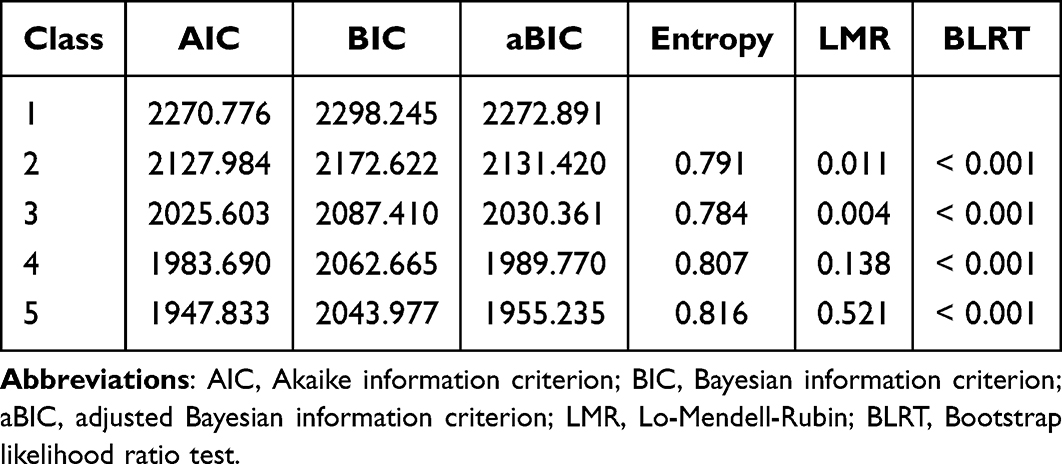 |
Table 2 Model Fit Information for Latent Profile Analysis for the Study Sample |
The three profiles of PsyCap are depicted in Figure 1. In Figure 1, the Y-axis represents the mean value of each dimension of PsyCap, and the X-axis represents the four dimensions of PsyCap. Profile 1 represented 23.1% of the sample (n=53) and had a lower probability of PsyCap. Hence, this subgroup was named the “low PsyCap group”. Profile 2 represented 48.1% of the sample (n=110) and had a moderate probability of PsyCap. Consistently, profile 2 was labelled the “moderate PsyCap group”. Profile 3 represented 28.8% of the sample (n=66) and had a higher probability of PsyCap. Thus, the subgroup was named the “high PsyCap group”. Profile 2 accounted for the majority of subjects.
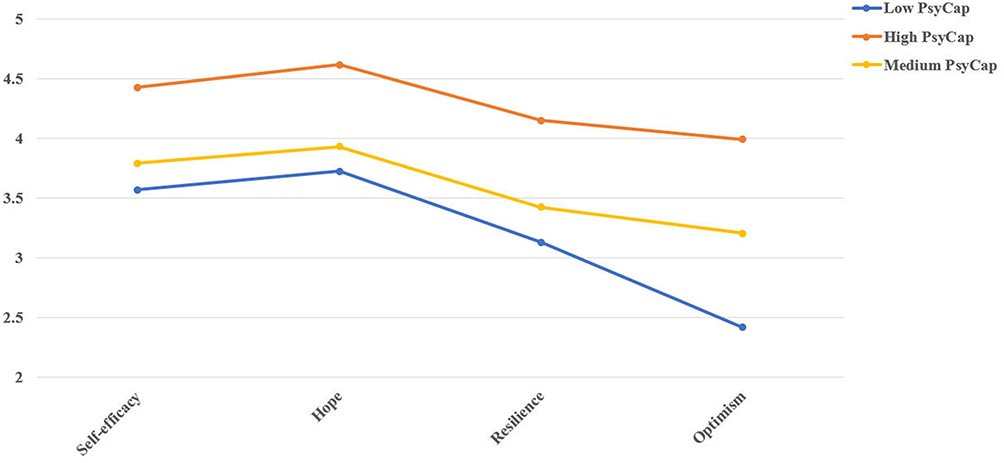 |
Figure 1 Latent profiles of psychological capital (PsyCap) among breast cancer patients. The Y axis represents the mean value of each dimension of PsyCap, and x axis represents the 4 dimensions of PsyCap. |
K‑means Clustering Analysis
The elbow test depicted in Figure 2A showed that the most significant decrease in slope for SSE across sequential clusters was from k=2–3 to k=3–4. Therefore, k=3 was considered the optimal number of categories suited for our data, and then k-means clustering was used to cluster the data into 3 clusters. As illustrated in Figure 2B, Cluster 1 included 123 BC patients, accounting for 53.7% of the total 229, and was characterized by a moderate level of PsyCap. Cluster 2, consisting of 63 (27.5%) BC patients, was characterized by a high level of PsyCap. Cluster 3, with 43 (18.8%), was characterized by a low level of PsyCap. The results obtained from the k-means clustering further supported the rationale behind categorizing PsyCap into these three distinct profiles.
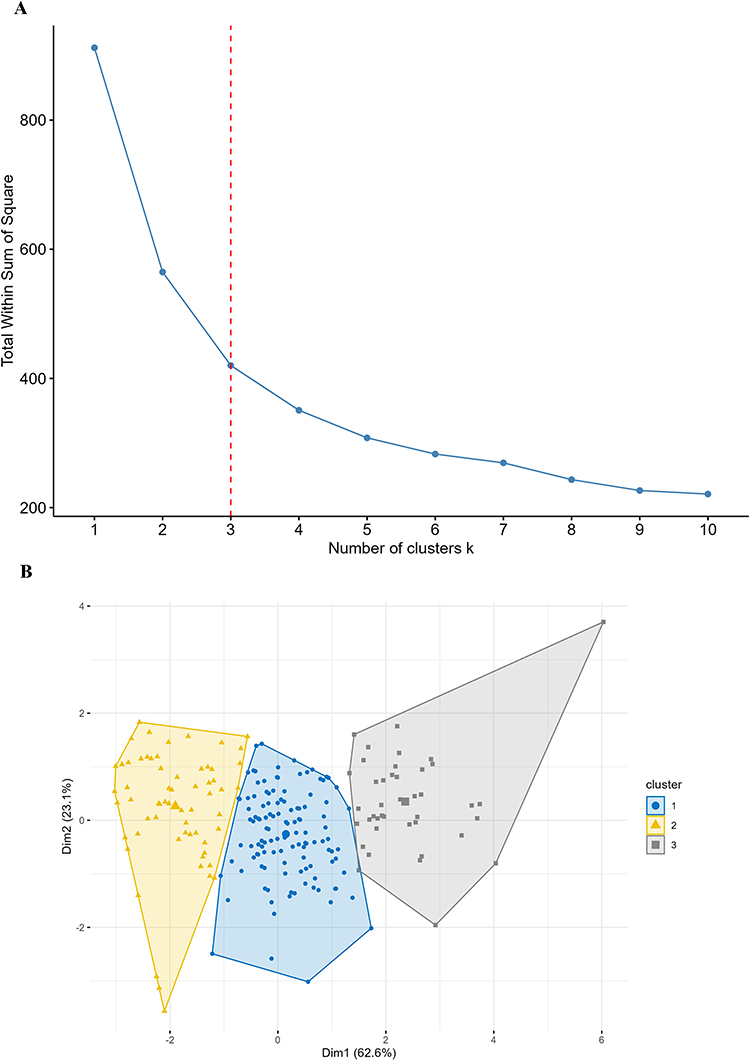 |
Figure 2 Elbow test for k-means analysis (A) and k-means clustering results (B). (A) the “elbow” on the graph indicates that the ideal number of clusters is “k=3”. (B) Since clustering is generated on 4 axes, these axes are dimensionally reduced to “Dim1” and “Dim 2”, representing the greatest consistency between the data.). |
Influencing Factors of PsyCap
As shown in Table 3, our study used the multivariate logistic regression analysis to determine the factors influencing PsyCap in BC patients. The low PsyCap group (profile 1) was considered the control group in the regression model. The analysis found that only employment status had a significant effect on PsyCap. Specifically, unemployment was a risk factor (OR=0.213, 95% CI=0.073~0.627, P=0.005) for profile 3, compared to baseline profile 1, and appears likely to be categorized in the low PsyCap group.
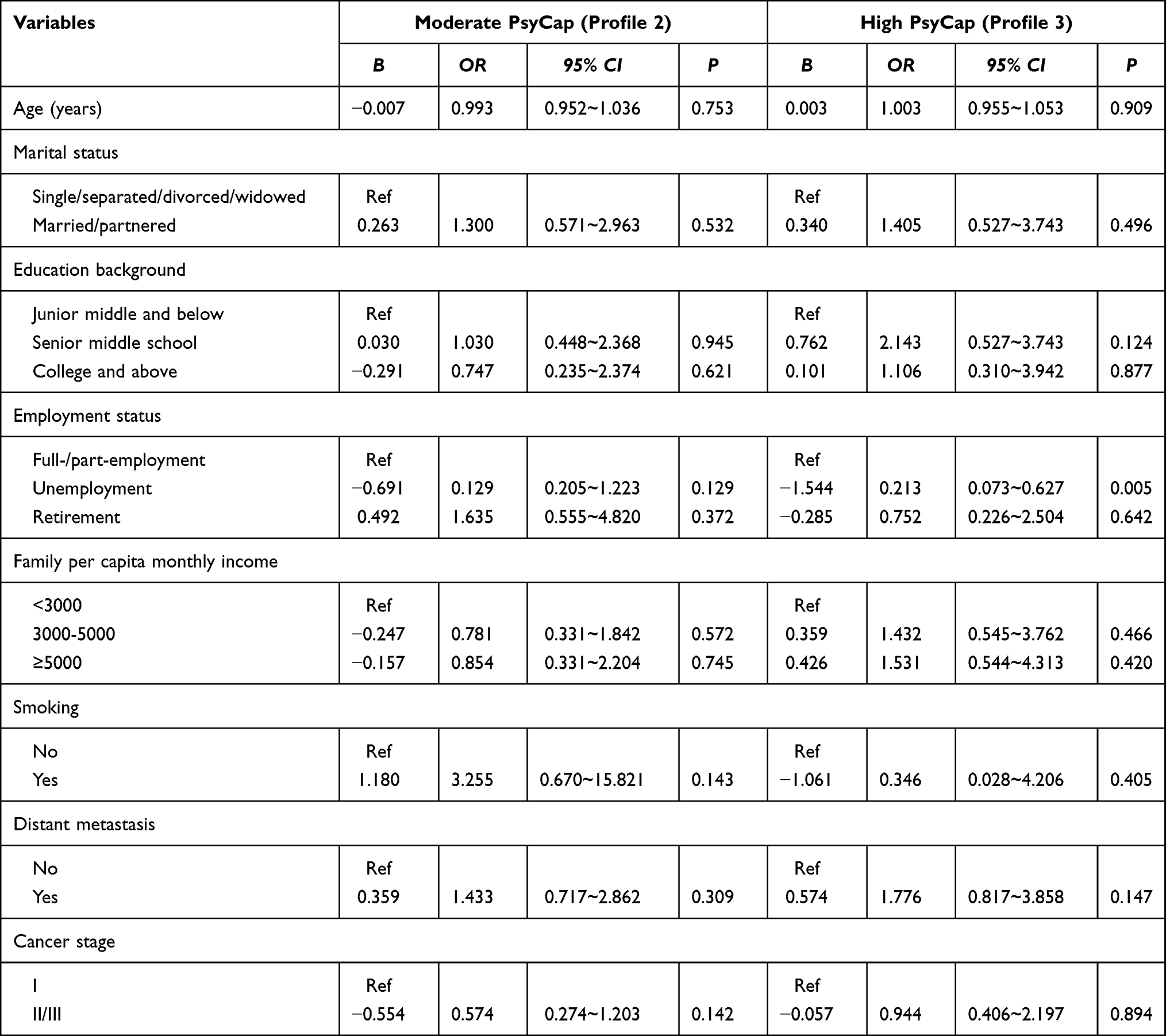 |
Table 3 Multiple Logistic Regression of Sociodemographic and Clinical Variables on Different Profiles of PsyCap |
Disparity Between the Latent Profiles of PsyCap and QoL
As shown in Table 4, the dimensions and total scores of FACT-B showed significant differences in the latent profiles of PsyCap among BC patients (P<0.001). Specifically, post hoc analysis showed that the high PsyCap group scored significantly higher on FACT-B than the low and moderate PsyCap groups. Similar findings were observed in PWB, EWB, SFWB, FWB, and BCS.
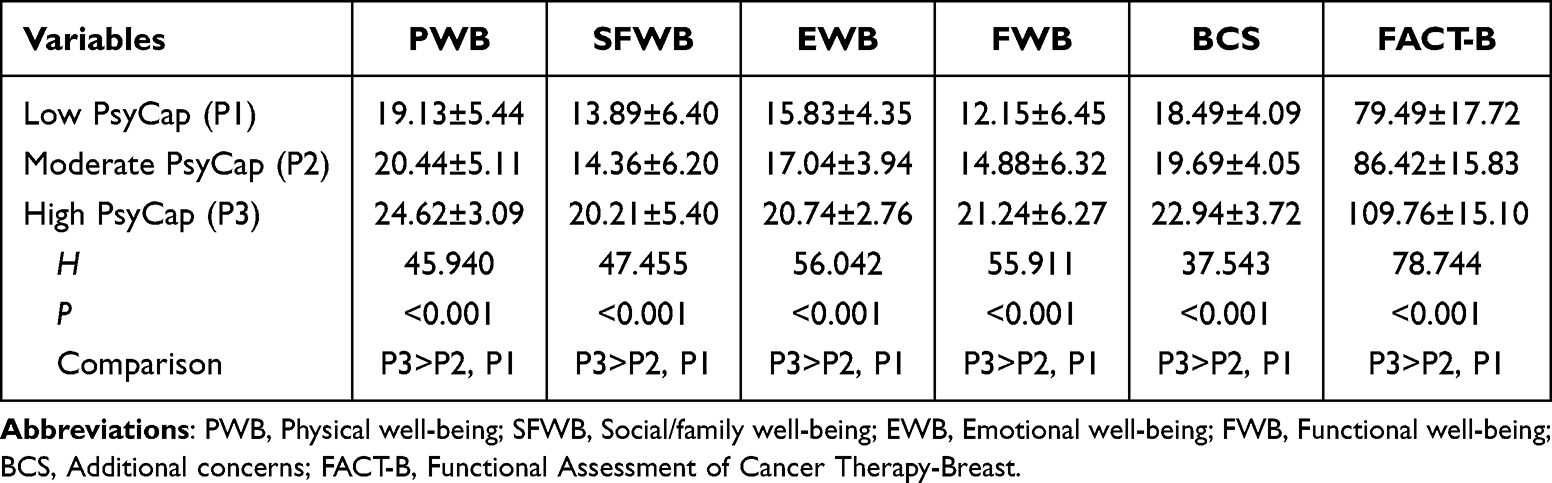 |
Table 4 Disparity Between the Profiles of PsyCap and QoL Among BC Patients |
Multiple Linear Regression Between the Latent Profiles of PsyCap and QoL
Multiple linear regression analysis showed that after controlling for demographics and clinical characteristics, compared with the low PsyCap group, the moderate PsyCap group (Beta=0.209, P=0.002) and the high PsyCap group (Beta=0.664, P<0.001) reported higher levels of QoL among BC patients (Table 5).
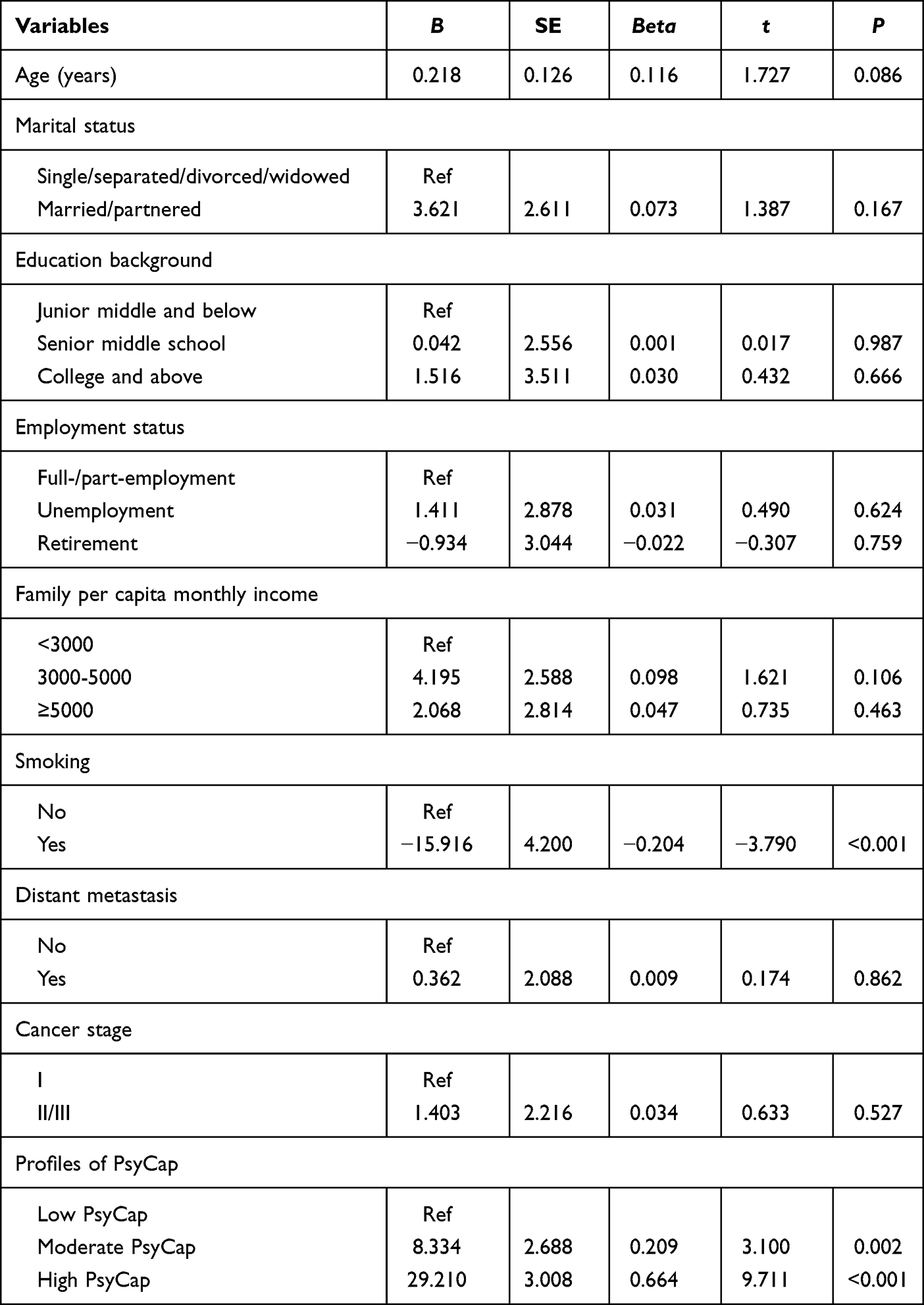 |
Table 5 Relationship Between Latent Profiles of PsyCap and QoL Among BC Patients |
Discussion
According to the PLA results, our findings indicated significant individual differences in PsyCap in BC patients. Our study further substantiated the reliability of three profiles through k-means clustering. Specifically, three profiles of PsyCap were identified, including the low PsyCap group, the moderate PsyCap group, and the high PsyCap group. Less than 30% BC patients possessed a high level of PsyCap, which suggested that the overall psychological capital of BC patients in our sample was low to medium. Other studies had similar latent classes based on teachers,42 students,43 and workers’ PsyCap.44 Existing studies about the PsyCap profiles mainly focused on the healthy population, which ignores the significance of PsyCap on BC patients’ physical and psychological health.
As shown in Figure 1, the development direction of four dimensions (self-efficacy, hope, resilience, and optimism) in PsyCap’s three profiles was characterized by “equally high” or “equally low”. Specifically, the high PsyCap group had significantly higher levels of each dimension than the moderate PsyCap group, and the moderate PsyCap group had substantially higher levels of each dimension than the low PsyCap group. Wu et al45 also reported similar findings based on the LPA of PsyCap. Our results were supported by the Multiple Resource theory.19 This theory views PsyCap as a higher-order internal resource where the core dimensions are related and work together synergistically. Therefore, our findings indicated that all dimensions of PsyCap play an essential role in their physical and psychological health. Notably, the level of optimism dimension in each profile was lower than the other three dimensions. The level of optimism decreased because BC patients were dissatisfied with the results of their disease treatment or because the disease was progressing more rapidly. Increasing studies demonstrated that optimism was associated with better psychological well-being and mental health among cancer patients.46–49 That means reinforcing optimism may be an effective tool to support patients in adapting to their illness.
In the present study, we found that BC patients in profile 1 were mainly unemployed, while more patients in profile three were employed. Results of the regression model also indicated that unemployment status is a risk factor for the high PsyCap group. BC surgery is associated with unemployment.50 A longitudinal study displayed that unemployed BC patients were more prone to negative emotions than those employed.51 This may be because unemployment is highly predictive of experiencing a range of financial problems, such as a lack of savings and difficulties paying bills, consumer debt, and mortgage loans. In turn, financial distress leads to a higher prevalence of poor well-being and mental health deterioration.52 A meta-analysis53 displayed that BC patients were more likely to be unemployed than healthy control participants. Occupation as a social attribute, employed patients can divert their attention, can alleviate the negative emotions caused by the disease, and are associated with better social functioning, greater financial security, improved health, and higher self-esteem,50,54,55 thus contributing to the generation and development of PsyCap.
Furthermore, our findings reported that all the profiles of PsyCap were significantly associated with BC patients’ QoL. Specifically, the high PsyCap profile had better QoL than the other profiles. These results were supported by previous studies demonstrating that PsyCap was significantly and positively associated with QoL in patients with systemic lupus erythematosus.56 In addition, other studies found that PsyCap dimensions positively affected QoL in cancer patients.57,58 PsyCap enables BC patients to behave proactively and have a more optimistic evaluation of the future despite suffering from cancer, thus promoting well-being and QoL. Moreover, emerging research indicated that patients with greater PsyCap were prone to less stress, fatigue, depression, and anxiety.23,35,56 Therefore, strengthening PsyCap enables BC patients to look at the positives in cancer diagnosis and treatment and enables coping, thereby facilitating their flourishing and minimizing the likelihood that they will experience a deterioration in their mental health and QoL.
Implications
Given that PsyCap is considered a modifiable domain, characterization of a patient’s PsyCap profile using tools evaluated in this study may identify potentially actionable risk factors ripe for clinician intervention. Therefore, we recommended that PsyCap be included in routine psychological assessments to screen for the three PsyCap profiles and develop early prevention interventions among Chinese BC patients. The PsyCap Intervention (PCI) is a structured, micro-intervention that targets each PsyCap component sequentially. According to the Chinese collectivist culture, the therapy or support programs based on PsyCap should engage the family unit, not just the patient. Studies have confirmed that PCI can effectively improve the PsyCap of BC patients.59 Unemployment BC patients should be paid more attention to. Knowledge of the unemployment risk factors could help determine the most appropriate treatment to facilitate the return to work. Studies revealed that a high level of hope is positively associated with work ability and work engagement, and that a high level of hope or resilience is negatively associated with burnout complaints among employed cancer patients.60 Clinical psycho-oncological practice may benefit from these insights, which guide this vulnerable group of employed BC patients. In addition, the PsyCap profiles affected BC patients’ QoL, so healthcare professionals can identify BC patients who have poor QoL based on their PsyCap and provide them with psychological counseling services and psychological healing groups to help them improve their mental and physical health.
Limitations
Nevertheless, some limitations should be noted in our study. First, our study adopted a cross-sectional design, which limited our ability to investigate the trajectory of PsyCap and the association between QoL in BC patients over time. Therefore, a longitudinal study based on latent transition analysis should be performed to track the changes in the three profiles of PsyCap, and examine the causal relationships between PsyCap and QoL. Second, the LPA analysis in this study did not fully account for the effect of covariates, and the following studies should include theoretically sound covariates. In addition, our study did not explore the potential moderation/mediation effect of PsyCap due to insufficient data. Therefore, the subsequent research will collect other variables (eg, anxiety and depression) to explore the impact of PsyCap. Finally, our study’s participants were recruited from the three Grade-A hospitals in Shenyang, China, which limited the representativeness of the samples due to many regional differences. Hence, to increase the diversity of the sample, future research should include a multi-regional, multi-center clinical study.
Conclusion
Our study identified three profiles of PsyCap based on LPA, which were named “low PsyCap group”, “moderate PsyCap group”, and “high PsyCap group”. PsyCap is classifiably heterogeneous among patients with BC, which suggests that healthcare professionals should give full consideration to the impact of unemployment on the PsyCap groups. The PsyCap profiles affected BC patients’ QoL, so healthcare professionals can identify BC patients with poor QoL based on their PsyCap and provide them with psychological counseling services and psychological healing groups to help them improve their physical and psychological health. A longitudinal study should be conducted to track the changes in the profiles of PsyCap and examine the causal claims.
Data Sharing Statement
The dataset in this study is available from the corresponding author on reasonable request.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the First affiliated Hospital of China Medical University (NO. 2021-430-2).
Consent to Participate
All patients provided their written informed consent prior to responding to the survey.
Acknowledgments
All authors would like to express their gratitude to patients who completed our questionnaires in the present study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Doctoral Research Initiation Fund of Wannan Medical College (No. X600100117) and Anhui Province University Research Project (No. 2024AH053457).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca A Cancer J Clinicians. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Arnold M, Morgan E, Rumgay H, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. 2022;66:15–23. doi:10.1016/j.breast.2022.08.010
3. Shrestha A, Martin C, Burton M, Walters S, Collins K, Wyld L. Quality of life versus length of life considerations in cancer patients: a systematic literature review. Psychooncology. 2019;28(7):1367–1380. doi:10.1002/pon.5054
4. Wang X, Wang N, Zhong L, et al. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: a systematic review and meta-analysis of 282,203 patients. Mol Psychiatry. 2020;25(12):3186–3197. doi:10.1038/s41380-020-00865-6
5. Aune D, Markozannes G, Abar L, et al. Physical activity and health-related quality of life in women with breast cancer: a meta-analysis. JNCI Cancer Spectr. 2022;6(6). doi:10.1093/jncics/pkac072
6. AlFayyad I, Al-Tannir M, Howaidi J, AlTannir D, Abu-Shaheen A. Health-related quality of life of breast and colorectal cancer patients undergoing active chemotherapy treatment: patient-reported outcomes. Qual Life Res. 2022;31(9):2673–2680. doi:10.1007/s11136-022-03145-8
7. Shao Z, Zhu T, Zhang P, Wen Q, Li D, Wang S. Association of financial status and the quality of life in Chinese women with recurrent ovarian cancer. Health Qual Life Outcomes. 2017;15(1):144. doi:10.1186/s12955-017-0714-9
8. Boškailo E, Franjić D, Jurić I, Kiseljaković E, Marijanović I, Babić D. Resilience and quality of life of patients with breast cancer. Psychiatry Danub. 2021;33(Suppl 4):572–579.
9. Ejder ZB, Sanlier N. The relationship between loneliness, psychological resilience, quality of life and taste change in cancer patients receiving chemotherapy. Support Care Cancer. 2023;31(12):683. doi:10.1007/s00520-023-08156-w
10. Zhao X, Tong S, Yang Y. The correlation between quality of life and positive psychological resources in cancer patients: a meta-analysis. Front Psychol. 2022;13:883157. doi:10.3389/fpsyg.2022.883157
11. Hobfoll S. The ecology of stress. Choice Rev Online. 1989;26(07).
12. Hobfoll SE. Social and psychological resources and adaptation. Rev General Psychol. 2002;6(4):307–324.
13. Halbesleben JRB, Neveu JP, Paustian-Underdahl SC, Westman M. Getting to the \”COR\”: understanding the role of resources in conservation of resources theory. J Manage. 2014;40(5):1334–1364.
14. Chen DJQ, Lim VKG. Strength in adversity: the influence of psychological capital on job search. J Organizational Behav. 2012;33(6):811–839. doi:10.1002/job.1814
15. Luthans F, Youssef-Morgan CM. Psychological capital: an evidence-based positive approach. Ann Rev Organization Psychol Organization Behav. 2017;4(1):339–366. doi:10.1146/annurev-orgpsych-032516-113324
16. Newman A, Ucbasaran D, Zhu F, Hirst G. Psychological capital: a review and synthesis. J Organizational Behav. 2014;35(S1):S120–S138.
17. Avey JB, Luthans F, Jensen SM. Psychological capital: a positive resource for combating employee stress and turnover. Human Resour Manag. 2010;48(5):677–693.
18. Luthans F, Avolio BJ, Avey JB, Norman SM. Positive psychological capital: measurement and relationship with performance and satisfaction. Personnel Psychol. 2010;60(3):541–572. doi:10.1111/j.1744-6570.2007.00083.x
19. Hobfoll SE. The influence of culture, community, and the nested‐self in the stress process: advancing conservation of resources theory. Applied Psychol. 2001;50(3):337–421. doi:10.1111/1464-0597.00062
20. Ren Y, Ji B. Correlation between perceived social support and loneliness among chinese adolescents: mediating effects of psychological capital. Psychiatry Danub. 2019;31(4):421–428. doi:10.24869/psyd.2019.421
21. Ye ZJ, Liang MZ, Qiu HZ, et al. Effect of a multidiscipline mentor-based program, be resilient to breast cancer (BRBC), on female breast cancer survivors in mainland China-A randomized, controlled, theoretically-derived intervention trial. Breast Cancer Res Treat. 2016;158(3):509–522. doi:10.1007/s10549-016-3881-1
22. Sugden R, Sen A. Commodities and capabilities. Econ J. 1986;96(383):820–822. doi:10.2307/2232999
23. Zhao D, Li Y, Zhou M, et al. The effect of mindfulness and psychological capital on mental health of breast cancer patients: based on polynomial regression and response surface analysis. J Psychosoc Oncol. 2024;42(2):190–207. doi:10.1080/07347332.2023.2233951
24. Harms CA, Cohen L, Pooley JA, Chambers SK, Galvão DA, Newton RU. Quality of life and psychological distress in cancer survivors: the role of psycho-social resources for resilience. Psychooncology. 2019;28(2):271–277. doi:10.1002/pon.4934
25. Wang JJ, Fang YC, Wang R, Huang YL, Xiao SQ, Li N. Mediating effect of psychological capital on the relationship between perceived stress and fear of cancer recurrence in breast cancer patients. J Nurs Sci. 2021;36(1):76–79.
26. Luthans F, Avolio BJ, Avey JB, Norman SM. Positive psychological capital: measurement and relationship with performance and satisfaction. Pers Psychol. 2007;60(3):541–547.
27. Nolzen N. The concept of psychological capital: a comprehensive review. Manag Rev Quarterly. 2018;68(3):1–41.
28. Bonanno GA, Mancini AD. Beyond resilience and PTSD: mapping the heterogeneity of responses to potential trauma. Psychol Trauma Theory Res Prac Policy. 2012;4(1):74–83.
29. Liu X, Zhang Q, Yu M, Xu W. Patterns of posttraumatic stress disorder and posttraumatic growth among breast cancer patients in China: a latent profile analysis. Psychooncology. 2020;29(4):743–750. doi:10.1002/pon.5332
30. Cui C, Wang L, Wang X. Profiles of social constraints and associated factors among breast cancer patients: a latent profile analysis. BMC Psychiatry. 2022;22(1):750. doi:10.1186/s12888-022-04407-y
31. Grant RW, McCloskey J, Hatfield M, et al. Use of latent class analysis and k-means clustering to identify complex patient profiles. JAMA Network Open. 2020;3(12):e2029068. doi:10.1001/jamanetworkopen.2020.29068
32. Lanza ST, Rhoades BL. Latent class analysis: an alternative perspective on subgroup analysis in prevention and treatment. Prev Sci. 2013;14(2):157–168. doi:10.1007/s11121-011-0201-1
33. Howard Sharp KM, Tillery Webster R, Cook J, Okado Y, Long A, Phipps S. Profiles of resilience, distress, and posttraumatic growth in parents of children with cancer and the relation to subsequent parenting and family functioning. J Pediatr Psychol. 2023;48(4):375–385. doi:10.1093/jpepsy/jsac097
34. Cai T, Huang Q, Yuan C. Profiles of instrumental, emotional, and informational support in Chinese breast cancer patients undergoing chemotherapy: a latent class analysis. BMC Womens Health. 2021;21(1):183. doi:10.1186/s12905-021-01307-3
35. Cui CY, Wang Y, Zhang Y, Chen S, Jiang N, Wang L. The development and validation of the psychological capital questionnaire for patients with Cancer the psychological capital questionnaire. BMC Cancer. 2021;21(1):1194. doi:10.1186/s12885-021-08960-9
36. Wan C, Zhang D, Yang Z, et al. Validation of the simplified Chinese version of the FACT-B for measuring quality of life for patients with breast cancer. Breast Cancer Res Treat. 2007;106(3):413–418. doi:10.1007/s10549-007-9511-1
37. Brady MJ, Cella DF, Mo F, et al. Reliability and validity of the functional assessment of cancer therapy-breast quality-of-life instrument. J Clin Oncol. 1997;15(3):974–986. doi:10.1200/JCO.1997.15.3.974
38. Lu Q, You J, Kavanagh A, et al. Differences in quality of life between American and Chinese breast cancer survivors. Support Care Cancer. 2016;24(9):3775–3782. doi:10.1007/s00520-016-3195-1
39. Vrieze SI. Model selection and psychological theory: a discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychol Methods. 2012;17(2):228–243. doi:10.1037/a0027127
40. Kim SY. Determining the number of latent classes in single- and multi-phase growth mixture models. Struct Equation Model. 2014;21(2):263–279. doi:10.1080/10705511.2014.882690
41. Liu F, Yang D, Liu Y, et al. Use of latent profile analysis and k-means clustering to identify student anxiety profiles. BMC Psychiatry. 2022;22(1):12. doi:10.1186/s12888-021-03648-7
42. Gou CM, Yang SH, Li JS. Relationship between psychological capital and occupational stress in elementary and secondary school principals: a potential profile study. China J Health Psychol. 2022;30(8):1202–1207.
43. Zhang YL, Dong XY, Ye Y, Fan XZ. Latent profile analysis of psychological capital of nursing graduates and its relationship with emotional well-being. Nurs J Chin PLA. 2021;38(12):1102–1108.
44. Chao L, Yang WJ, Zheng X. The psychological capital of small and medium-sized enterprise employees based on the potential profiles analysis. China J Health Psychol. 2017;25(1):54–60.
45. Wu M, Sun LP, Liang LC, Bian YF. Heterogeneity of psychological capital and its social adaptation among rural elementary boarding students: evidence based on latent profile analysis. Stud Psychol Behav. 2021;19(2):186–192.
46. Thieme M, Einenkel J, Zenger M, Hinz A. Optimism, pessimism and self-efficacy in female cancer patients. Jpn J Clin Oncol. 2017;47(9):849–855. doi:10.1093/jjco/hyx079
47. Faye-Schjøll HH, Schou-Bredal I. Pessimism predicts anxiety and depression in breast cancer survivors: a 5-year follow-up study. Psychooncology. 2019;28(6):1314–1320. doi:10.1002/pon.5084
48. Calderon C, Carmona-Bayonas A, Hernández R, et al. Effects of pessimism, depression, fatigue, and pain on functional health-related quality of life in patients with resected non-advanced breast cancer. Breast. 2019;44:108–112. doi:10.1016/j.breast.2019.01.012
49. Yang Y, Qi H, Li W, et al. Predictors and trajectories of fear of cancer recurrence in Chinese breast cancer patients. J Psychosom Res. 2023;166:111177. doi:10.1016/j.jpsychores.2023.111177
50. Wang L, Hong BY, Kennedy SA, et al. Predictors of unemployment after breast cancer surgery: a systematic review and meta-analysis of observational studies. J Clin Oncol. 2018;36(18):1868–1879. doi:10.1200/JCO.2017.77.3663
51. Puigpinós-Riera R, Graells-Sans A, Serral G, et al. Anxiety and depression in women with breast cancer: social and clinical determinants and influence of the social network and social support (DAMA cohort). Cancer Epidemiol. 2018;55:123–129. doi:10.1016/j.canep.2018.06.002
52. Borrescio-Higa F, Droller F, Valenzuela P. Financial distress and psychological well-being during the COVID-19 pandemic. Int J Public Health. 2022;67:1604591. doi:10.3389/ijph.2022.1604591
53. de Boer AG, Taskila T, Ojajärvi A, van Dijk FJ, Verbeek JH. Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA. 2009;301(7):753–762. doi:10.1001/jama.2009.187
54. Islam T, Dahlui M, Majid HA, Nahar AM, Mohd Taib NA, Su TT. Factors associated with return to work of breast cancer survivors: a systematic review. BMC Public Health. 2014;14 Suppl 3(Suppl 3):S8. doi:10.1186/1471-2458-14-S3-S8
55. Banning M. Employment and breast cancer: a meta-ethnography. Eur J Cancer Care. 2011;20(6):708–719.
56. Meng L, Gao CR, Wang HC, et al. Positive psychological capital, post-traumatic growth, social support, and quality of life in patients with systemic lupus erythematosus: a cross-sectional study. Lupus. 2024;33(5):470–480. doi:10.1177/09612033241238051
57. Shen A, Qiang W, Wang Y, Chen Y. Quality of life among breast cancer survivors with triple negative breast cancer--role of hope, self-efficacy and social support. Eur J Oncol Nurs. 2020;46:101771. doi:10.1016/j.ejon.2020.101771
58. Sihvola S, Kuosmanen L, Kvist T. Resilience and related factors in colorectal cancer patients: a systematic review. Eur J Oncol Nurs. 2022;56:102079. doi:10.1016/j.ejon.2021.102079
59. Chen JJ. Psychological Capital Status of Breast Cancer Patients and the Intervention on Breast Cancer Patients. Yanbian University; 2022.
60. Boelhouwer IG, van Vuuren T. Psychological capital and work functioning of workers with recurrent or metastatic cancer beyond return to work. Palliative Supportive Care. 2024;22(5):1102–1108. doi:10.1017/S1478951524000233
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychometric Properties and Factorial Analysis of the Arabic McGill-QoL Questionnaire in Breast Cancer
Omar MTA, Alnahdi AH
Breast Cancer: Targets and Therapy 2023, 15:813-824
Published Date: 14 November 2023
Predictive Models of Psychological Distress, Quality of Life, and Adherence to Medication in Breast Cancer Patients: A Scoping Review
Pezzolato M, Spada GE, Fragale E, Cutica I, Masiero M, Marzorati C, Pravettoni G
Patient Preference and Adherence 2023, 17:3461-3473
Published Date: 19 December 2023
Coping Profiles and Differences in Psychological Distress and Quality of Life in Clients Undergoing Assisted Reproductive Techniques: A Latent Profile Analysis
Bai J, Zheng J, Guo N, Dong Y, Wang K, Cheng C, Jiang H, Qian L
Journal of Multidisciplinary Healthcare 2024, 17:533-540
Published Date: 5 February 2024
Latent Profile Analysis and Determinants of Marital Adjustment in Patients with Breast Cancer
Chen XF, Shen C, Gu ZF, Dong C, Zhuang Y, Lu LH, Lu P, Li YJ
Journal of Multidisciplinary Healthcare 2024, 17:5799-5809
Published Date: 5 December 2024
Quality of Life in Breast Cancer Patients in Saudi Arabia: A Systematic Review
Aljadani FF, Nughays RO, Alharbi GE, Almazroy EA, Elyas SK, Danish HE, Alanazi RT, Aldrees BA, Jadkarim GA, Mikwar Z
Breast Cancer: Targets and Therapy 2025, 17:171-186
Published Date: 18 February 2025