Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Coping Profiles and Differences in Psychological Distress and Quality of Life in Clients Undergoing Assisted Reproductive Techniques: A Latent Profile Analysis
Authors Bai J ![]() , Zheng J, Guo N, Dong Y, Wang K
, Zheng J, Guo N, Dong Y, Wang K ![]() , Cheng C
, Cheng C ![]() , Jiang H, Qian L
, Jiang H, Qian L
Received 10 October 2023
Accepted for publication 16 January 2024
Published 5 February 2024 Volume 2024:17 Pages 533—540
DOI https://doi.org/10.2147/JMDH.S444053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jie Bai,1 Jinxia Zheng,1 Nafei Guo,2 Yueyan Dong,1 Ke Wang,1 Cheng Cheng,3 Hui Jiang,2 Lin Qian4
1Shanghai Key Laboratory of Maternal-Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Nursing Department, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 3School of Nursing, Fudan University, Shanghai, People’s Republic of China; 4Nursing Department, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Hui Jiang, Nursing Department, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China, Tel/Fax +86 21-20261221, Email [email protected] Lin Qian, Nursing Department, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China, Email [email protected]
Purpose: Receiving assisted reproductive technology is stressful due to its long-lasting process, which might pose negative impacts on clients’ psychological well-being and quality of life. This study was to investigate coping profiles among couples undergoing assisted reproductive technology and examine their associations with psychological distress and quality of life.
Methods: This cross-sectional study was conducted at the IVF center of a specialized hospital in Shanghai, China. Of 502 eligible clients completed a structured, online survey of socio-demographic information, Dyadic Coping Inventory, Kessler Psychological Stress Scale, and Fertility quality of life. Coping profiles were identified using latent profile analysis and differences between identified profiles on psychological distress and quality of life were examined using analyses of covariance.
Results: A three-profile solution was supported: low dyadic coping group (n = 168, 33.50%), moderate dyadic coping group (n = 241, 48.00%), and high dyadic coping group (n = 93, 18.50%). Significant differences between those groups were found in psychological distress and quality of life.
Conclusion: The findings of this study have revealed dyadic coping profiles in clients undergoing assisted reproductive technology, which are differentially associated with psychological distress and quality of life.
Keywords: assisted reproductive technology, coping, latent profile analysis, psychological distress, quality of life
Introduction
The World Health Organization (WHO) defines infertility as a disease of the reproductive system, characterized by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse.1 Infertility affects approximately 15% of couples worldwide, with ART being a common treatment option.2 Assisted Reproductive Technology (ART) refers to treatments that help infertile couples to conceive children.3 Although ART alleviates the infertile burden of clients and their families, its procedure could be expensive, frustrating, and involve multiple treatment rounds, leading to significant psychological distress. The psychological distress associated with ART is multi-layered, encompassing emotional, cognitive, and social aspects.4 Emotional distress often manifests as feelings of grief, anxiety, and depression. Cognitive distress refers to negative thoughts and beliefs about oneself, one’s partner, and one’s future. Social distress arises from the stigma associated with infertility, the strain on relationships, and the isolation from social networks.5 The increasing effect of these types of distress might result in an impaired quality of life (QoL) for clients undergoing ART. A cross-study has shown that the incidence of anxiety and depression in Chinese women undergoing infertility treatment was 25% and 31%, respectively.6 Qualitative findings also showed that clients following ART felt vulnerable during their pregnancy and experienced a series of negative feelings such as fear.7
Coping refers to the process of dealing with internal and/or external stressful situations using thoughts and actions. Lazarus and Folkman propose the transaction theory of stress and coping to explain how people think and act during real-life stressful events.8 This theoretical framework emphasizes the importance of two processes: appraisal and coping. People usually make appraisals to determine whether the situations are stressful, then manage the situations causing the distress (known as problem-focused coping), and sustain positive well-being (known as emotional-focused coping). Many studies have found a link between people’s coping and their health-related outcomes.9–12 For example, Penley, Tomaka and Wiebe13 found that people who were inclined to use strategies such as distancing, self-control, and confrontive coping might report more negative health outcomes.
An increasing number of studies have investigated coping in the context of infertility and have documented its significance to health-related outcomes.14,15 For example, Iordăchescu and her team examined the association between anxiety, coping, and difficulties with infertility among 240 infertile women and found that maladaptive coping was positively related to anxiety, while adaptive coping was negatively related to anxiety.16 Prior research explored the associations between psychological distress, dyadic coping, and QoL in Chinese ART couples and found that positive dyadic coping was linked to better QoL, but negative dyadic coping might lead to impaired QoL.17 Another survey in China involving 768 infertile women undergoing ART showed that strategies such as avoidance coping and meaning-based coping might play a significant mediating role between stigma and fertility QoL.18 Research has demonstrated that impaired mental health may increase the likelihood of discontinuing treatment of ART19 and possibly impact pregnancy outcomes,20 thus the associations between coping and its impacts on clients’ outcomes should be investigated due to the significance of ART success for infertile couples.
Coping is a concept with a multidimensional nature and people regularly use more than one coping strategy when facing stressful situations. Research has confirmed that people can be categorized into groups based on their coping.21,22 However, individuals vary significantly in their coping strategies, leading to different coping profiles. A coping profile refers to the unique combination of coping strategies used by a person.23 These coping profiles can significantly influence psychological distress and QoL. For instance, cancer survivors with more adaptive coping reported less cancer-related distress, anxiety, and depression, and better QoL than their peers with more maladaptive coping.24 Despite the importance of coping profiles in managing psychological distress and QoL, there is a paucity of research in the area of clients undergoing ART. This gap in the literature underscores the need for a comprehensive examination of the coping profiles of this population and their impact on psychological distress and QoL.
Latent profile analysis is a promising approach for classifying subgroups within a population based on observed variables.25 In this study, the observed variables are the coping strategies used by clients undergoing ART. The latent profiles are the unique combinations of these coping strategies, which constitute the coping profiles of the clients. The present study aimed to (1) examine the dyadic coping profiles in a population undergoing ART, and (2) compare the levels of psychological distress and QoL across the identified profiles.
The findings of this study will provide valuable insights into the coping profiles of clients undergoing ART and their impact on psychological distress and QoL. This information can be used to develop targeted interventions to enhance the coping skills of this group, thereby reducing their psychological distress and improving their QoL. The study will also contribute to the existing literature on the psychological aspects of ART, offering more evidence of the coping involved in this challenging process towards parenthood.
Materials and Methods
This was a cross-sectional study conducted at the In-vitro Fertilization (IVF) center of Shanghai First Maternity and Infant Hospital, Shanghai, China. The conduct and dissemination of this study followed the checklist for STROBE (STrengthening the Reporting of OBservational studies in Epidemiology).26
The Institutional Review Board of the study venue has reviewed and approved this study (Ref. number: KS21296). We have conducted this study based on the principles of the Declaration of Helsinki. All participants of this study were informed of voluntary participation, anonymity, and confidentiality.
Sample and Procedure
Clients proposing new IVF cycles were screened according to inclusion and exclusion criteria. The criteria for inclusion were: (1) consenting to take part in the study, (2) having no chronic diseases such as hypertension, diabetes, heart diseases, or other major diseases, (3) plans to become pregnant through IVF, and (4) the ability to speak and understand Chinese. Clients who refused to join or were diagnosed with psychiatric disorders were excluded.
Regarding the sample size of this study, Nylund, Asparouhov and Muthén27 suggested that a minimum sample size of 500 might be appropriate for an LPA analysis. We approached 569 clients and 508 would like to participate in this study. The response rate was 89.3%.
Data were collected between July 2022 and March 2023. Participants were recruited from the IVF units of the study venue, where the couple attended medical visits. The primary researcher (JB) used recruitment flyers to recruit potential participants. Clients willing to participate in the survey would be briefed on the aims and procedure of the current study and be asked to provide informed consent. Clients who agreed to participate were given links to the online survey and asked to fill out a set of questionnaires onsite. No incentives were offered for participation in this study. The completion of the online survey took around 20 minutes. The primary researcher (JB) and two trained registered nurses administered the whole process.
Measures
The structured questionnaire includes (1) Social demographic information sheet, (2) Dyadic Coping Inventory (DCI),28 (3) Kessler Psychological Stress Scale (K6),29 and (4) Fertility quality of life (FertiQoL).30
We collected social demographic information such as age, sex, residence, marital status, education level, and diagnosis of infertility.
We used Kessler Psychological Stress Scale (K6)29 to measure participants’ psychological distress in this study. K6 is a six-item instrument on a 5-point Likert Scale (0 = no time, 4 = all the time). The total score is obtained by adding together all items. A higher score suggests more symptoms of psychological distress. In the present study, Cronbach’s α was 0.89 for the K6.
We used the Dyadic Coping Inventory (DCI)28 to measure participants’ behaviors in coping in this study. DCI is a 37-item instrument on a 5-point Likert scale (1 = very rarely, 5 = very often). The DCI examines nine forms of coping including stress communicated by oneself, supportive dyadic coping by oneself, delegated dyadic coping by oneself, negative dyadic coping by oneself, stress communication of the partner, supportive dyadic coping of the partner, delegated dyadic coping of the partner, negative dyadic coping by partner, common dyadic coping, and evaluation of dyadic coping. A higher score reflects more willingness to use the corresponding strategies. In the present study, Cronbach’s α was 0.94 for the DCI.
We used the Fertility quality of life tool (FertiQoL)30 to measure the quality of life of people with fertility issues. The FertiQoL is a 36-item instrument on a Likert scale ranging from 0 to 4. The FertiQoL has subscales across emotional, mind-body, relational, and social and three total scores (core FertiQoL, treatment FertiQoL, and total FertiQoL) ranging from 0 to 100. Two additional items (eg How would you rate your health?) capture a general situation of physical health and QoL. Higher scores on the subscales and total scores suggest better satisfaction with QoL. In the present study, Cronbach’s α was 0.91 for the FertiQoL.
Data Analysis
Data were analyzed using descriptive statistical methods. An LPA was used to identify the potential coping profiles based on the DCI scale. To determine the optimal number of profiles, the Akaike information criterion (AIC),31 sample size–adjusted Bayesian information criterion (sBIC),32 Bootstrapped likelihood ratio test (BLRT),33 and value of entropy were used to examine the model of fitness.34 Analyses of covariance (ANCOVAs) were used to compare the potential coping profiles on psychological distress and FertiQoLs. Potential covariates were explored before performing the ANCOVAs.
To perform the above analyses, the statistical program Mplus (version 7, Microsoft) and the SPSS software, version 26.0 statistical package (SPSS Inc., Chicago, IL, USA) were used. In all cases, p < 0.05 was accepted as statistically significant.
Results
Sample Characteristics
Of 508 participants who took the survey six unfinished questionnaires were excluded. A total of 502 participants (female: 245, 48.8% versus male: 257, 51.2%) were included in this study. Participants aged from 20 to 57 years old, with an average age of 34.22 ± 5.31 years. Other characteristics are presented in Table 1.
 |
Table 1 Characteristics of the Sample |
Based on the scoring rules of each instrument, the mean scores of psychological distress, dyadic coping total, and FertiQoL were 11.79 ± 4.17, 123.15 ± 19.20, and 66.26 ± 13.38, respectively. Other characteristics are presented in Table 2.
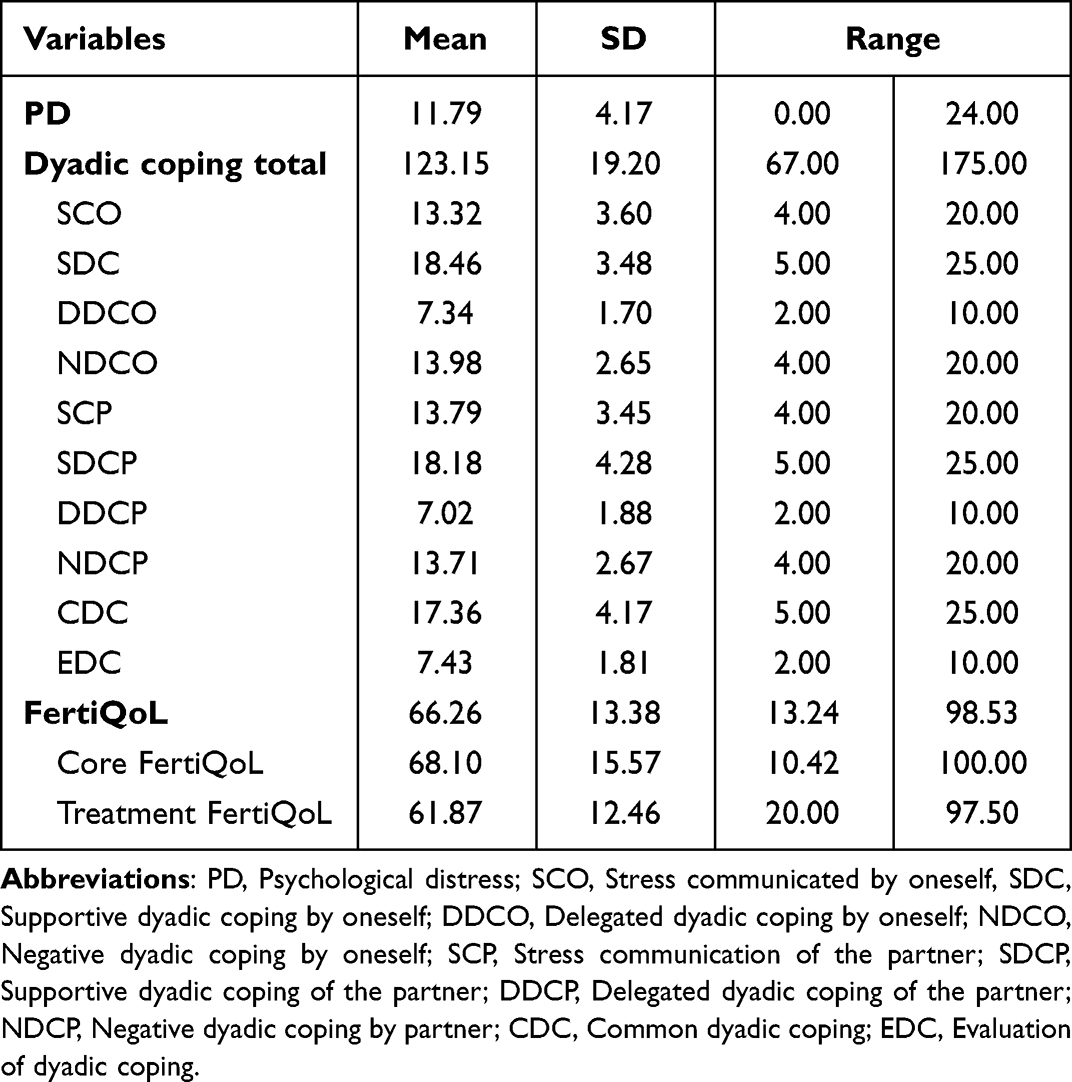 |
Table 2 Descriptive Statistics for Psychological Distress, Dyadic Coping, and FertiQoL |
Coping Profiles
An LPA analysis of scores on the ten coping subscales from the DCI was performed using Mplus 7. Multiple models were analyzed with additional profiles inputted and compared until the current profile (k profile) no longer outperformed the previous one (k − 1 profiles). Finally, the statistical model fit indices for a one- to four-profile solution are shown in Table 3.
 |
Table 3 Statistical Model Fit for Coping Profiles |
The first profile (n = 168; 33.50%) was representative of individuals with low scores in scores on ten coping subscales. This profile was labeled low dyadic coping (LDC). The second profile (n = 241; 48.00%) characterized individuals with moderate levels of on those subscales. This profile was labeled moderate dyadic coping (MDC). The last profile (n = 93; 18.50%) showed individuals with high levels of coping on SCO, SDC, DDCO, and so on coping strategies. Therefore, this profile was labeled high dyadic coping (HDC). See Table 4.
 |
Table 4 Conditional Response Means and Standard Deviations for Three-Profile LPA Solution |
Differences in Psychological Distress and QoL
Analyses of covariance were performed to compare the coping-based profile groups on psychological distress and QoL. Before the ANCOVAs, several potential covariates such as age, education level, income, and time of diagnosis were examined between groups. Those analyses showed significant differences between the groups on clients’ education level. Thus, education level was entered as a covariate in both ANOVA models.
The first ANCOVA (F= 12.58, p < 0.001) compared groups on psychological distress controlling for education level showed that LDC group (13.20 ± 4.82), MDC group (11.31 ± 3.64), and HDC group (10.47 ± 3.46). The second ANCOVA (F= 20.69, p < 0.001) compared groups on FertiQoL controlling for education level showed significant differences between the LDC group (59.63 ± 13.13), MDC group (67.78 ± 12.12), and HDC group (74.30 ± 11.26).
Discussion
Receiving ART is related to multiple stressors that might impair the psychological well-being and mental health of infertile clients. It becomes progressively significant to obtain a better understanding of potential coping profiles in this population. Therefore, the present study focused on identifying coping profile groups among clients undergoing ART and comparing the coping-profile groups on psychological distress and FertiQoL.
Coping Profiles
We identified three latent coping profiles, which resembled the coping identified in the past study, such as high dyadic coping, medium dyadic coping, and low dyadic coping.35 Similar to past findings, we also observed most participants reported low levels of dyadic coping. The plausible reason for the low level might be that the treatment of IVF posed pressure to infertile clients, which decreased the level of dyadic coping. Applying the person-oriented approach such as the LPA approach, our findings help to deliver a unique standpoint by revealing distinct latent patterns and confirming the multidimensional nature of coping.36 Depending on the various stressors during ART, healthcare professionals should consider identifying different coping profiles in their clients and provide appropriate support promptly.
Differences in Psychological Distress and QoL
In line with previous findings,37,38 we found that the clients in the high dyadic coping group reported less psychological distress and better FertiQoL. A possible reason was that clients in high dyadic coping groups might conduct more stress communication with their spouses, receive more support from spouses, and impose less stress on their spouses. More specifically, when couples are dedicated to supporting each other, they feel they can depend on the resources of their significant other. This engagement towards shared objectives enhances their ability to perceive themselves as more effective in dealing with and overcoming stressful events such as infertility.39 Previous research has demonstrated the positive effect of dyadic coping such as receiving support (both within and between levels) on relationship satisfaction and marital adjustment of both partners, which in turn better QoL. Thus, the more the clients had the experience of participating in the coping process complementary, the less they struggled with the process of ART.
Limitations
This study had limitations. Given the nature of cross-sectional design, causal directions cannot be identified between the studied variables. We used a voluntary sampling approach other than a consecutive approach. In addition, we adopted a dyadic coping scale but we did not study one’s coping and the effect of the partner’s coping on one’s own and each other’s psychological distress or QoL, further research might consider detecting mutual effects in couples with models of assessing dyadic relationships such as Actor Partner Interdependence Model (APIM). Last, the presence of other chronic health conditions, which might affect psychological distress and QoL of the sample, was not surveyed.
Implications
The current study has provided valuable insights that had significant implications for both research and clinical practice in the field of caring for clients undergoing ART. For research, the study suggested the importance of considering individual differences in coping strategies when examining psychological distress and QoL. Future research should continue to explore the different coping profiles, as this can provide a more nuanced understanding of the psychological experiences of this population. In particular, longitudinal research could be beneficial in tracking the changes in coping profiles through time and their impacts on psychological distress and QoL. This might help identify critical periods of increased psychological distress and decreased QoL, which could then be targeted for intervention. Moreover, future research could also investigate the factors that influence the development of different coping profiles. For instance, individual characteristics such as personality, earlier experiences with stress, and social support could play a significant role in shaping coping profiles. Understanding these factors could provide valuable insights into how to enhance the coping of clients undergoing ART.
For clinical practice, this study has emphasized the importance of assessing the coping profiles of clients undergoing ART. This assessment could be incorporated into the preliminary consultation and follow-up appointments. By understanding the clients’ coping profiles, healthcare professionals could tailor their care to meet the unique needs of each client. The study also indicated the need for interventions to enhance the coping skills of clients undergoing ART. These interventions could be delivered individually or in group forms and could be combined with the general ART plans. For instance, psychosocial interventions such as cognitive-behavioral therapy are potentially valuable in developing coping strategies.40 Also, the study highlighted the importance of providing psychological support to clients undergoing ART. The psychological support could include counseling, psychoeducation, and stress management techniques, delivered by a multidisciplinary team, including psychologists, social workers, and nurses.
Conclusion
Together, the findings of this study have expanded our knowledge regarding dyadic coping in ART clients by examining coping profiles with an LPA and emphasized the importance of considering individual differences in coping strategies when examining psychological distress and QoL. It also highlighted the necessity for interventions to enhance the coping skills of these clients, as well as the provision of psychological support. These findings could inform the development of more effective and tailored care for clients undergoing ART.
Funding
This study is supported by the Shanghai Municipal Health Commission Clinical Medical Research Special Youth Project (Reference number: 20204Y0132) and the Research Grant of Shanghai First Maternity and Infant Hospital (Reference number: 2023HL05).
Disclosure
The authors have no conflicts of interest to declare that are relevant to the content of this article.
References
1. World Health Organization. Infertility. Available from: https://www.who.int/news-room/fact-sheets/detail/infertility.
2. Sharlip ID, Jarow JP, Belker AM, et al. Best practice policies for male infertility. Fertil Steril. 2002;77(5):873–882. doi:10.1016/s0015-0282(02)03105-9
3. National Center for Chronic Disease Prevention and Health Promotion DoRH. What is assisted reproductive technology? Available from: https://www.cdc.gov/art/whatis.html.
4. Clifton J, Domar AD. Chapter 10 - Psychological distress and infertility: prevalence, impact, and interventions. In: Vaamonde D, Hackney AC, Garcia-Manso JM, editors. Fertility, Pregnancy, and Wellness. Elsevier; 2022:163–181.
5. Taebi M, Kariman N, Montazeri A, Majd HA. Infertility stigma: a qualitative study on feelings and experiences of infertile women. Int J Fertil Steril. 2021;15(3):189.
6. Wang L, Tang Y, Wang Y. Predictors and incidence of depression and anxiety in women undergoing infertility treatment: a cross-sectional study. PLoS One. 2023;18(4):e0284414. doi:10.1371/journal.pone.0284414
7. Huang MZ, Sun YC, Gau ML, Puthussery S, Kao CH. First-time mothers’ experiences of pregnancy and birth following assisted reproductive technology treatment in Taiwan. J Health Popul Nutr. 2019;38(1):10. doi:10.1186/s41043-019-0167-3
8. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. Springer; 1984.
9. Meier C, Bodenmann G, Mörgeli H, Jenewein J. Dyadic coping, quality of life, and psychological distress among chronic obstructive pulmonary disease patients and their partners. Int J Chron Obstruct Pulmon Dis. 2011;6:583–596. doi:10.2147/copd.S24508
10. Molgora S, Fenaroli V, Acquati C, De Donno A, Baldini MP, Saita E. Examining the role of dyadic coping on the marital adjustment of Couples Undergoing Assisted Reproductive Technology (ART). Front Psychol. 2019;10:415. doi:10.3389/fpsyg.2019.00415
11. Weitkamp K, Feger F, Landolt SA, Roth M, Bodenmann G. Dyadic coping in couples facing chronic physical illness: a systematic review. Front Psychol. 2021;12:722740. doi:10.3389/fpsyg.2021.722740
12. Yurkiw J, Johnson MD. Perceived stress, supportive dyadic coping, and sexual communication in couples. J Soc Pers Relat. 2021;38(5):1729–1737. doi:10.1177/0265407521996446
13. Penley JA, Tomaka J, Wiebe JS. The association of coping to physical and psychological health outcomes: a meta-analytic review. J Behav Med. 2002;25(6):551–603. doi:10.1023/a:1020641400589
14. Zurlo MC, Cattaneo Della Volta MF, Vallone F. Re-examining the role of coping strategies in the associations between infertility-related stress dimensions and state-anxiety: implications for clinical interventions with infertile couples. Front Psychol. 2020;11:614887. doi:10.3389/fpsyg.2020.614887
15. Chernoff A, Balsom AA, Gordon JL. Psychological coping strategies associated with improved mental health in the context of infertility. Arch Women’s Mental Health. 2021;24:73–83.
16. Iordăchescu DA, Paica CI, Boca AE, et al. Anxiety, difficulties, and coping of infertile women. Healthcare. 2021;9(4). doi:10.3390/healthcare9040466
17. Bai J, Zheng J, Dong Y, Wang K, Cheng C, Jiang H. Psychological distress, dyadic coping, and quality of life in infertile clients undergoing assisted reproductive technology in China: a single-center, cross-sectional study. J Multidiscip Healthc. 2022;15:2715–2723. doi:10.2147/jmdh.S393438
18. Jing X, Gu W, Zhang L, et al. Coping strategies mediate the association between stigma and fertility quality of life in infertile women undergoing in vitro fertilization-embryo transfer. BMC Women's Health. 2021;21(1):386. doi:10.1186/s12905-021-01525-9
19. Pedro J, Sobral MP, Mesquita-Guimarães J, Leal C, Costa ME, Martins MV. Couples’ discontinuation of fertility treatments: a longitudinal study on demographic, biomedical, and psychosocial risk factors. J Assist Reprod Genet. 2017;34(2):217–224. doi:10.1007/s10815-016-0844-8
20. Terzioglu F, Turk R, Yucel C, Dilbaz S, Cinar O, Karahalil B. The effect of anxiety and depression scores of couples who underwent assisted reproductive techniques on the pregnancy outcomes. Afr Health Sci. 2016;16(2):441–450. doi:10.4314/ahs.v16i2.12
21. Rzeszutek M, Pięta M, Van Hoy A, et al. Coping profiles, depression, and body image anxiety during the Covid-19 pandemic: comparative analysis of females with thyroid diseases and a non-clinical sample. PLoS One. 2023;18(3):e0282302. doi:10.1371/journal.pone.0282302
22. January AM, Kelly EH, Russell HF, Zebracki K, Vogel LC. Patterns of coping among caregivers of children with spinal cord injury: associations with parent and child well-being. Fam Syst Health. 2019;37(2):150–161. doi:10.1037/fsh0000415
23. Doron J, Trouillet R, Maneveau A, Ninot G, Neveu D. Coping profiles, perceived stress and health-related behaviors: a cluster analysis approach. Health Promot Int. 2015;30(1):88–100. doi:10.1093/heapro/dau090
24. Cheng CT, Ho SMY, Liu WK, et al. Cancer-coping profile predicts long-term psychological functions and quality of life in cancer survivors. Support Care Cancer. 2019;27(3):933–941. doi:10.1007/s00520-018-4382-z
25. Helm SV, Li X, Curran MA, Barnett MA. Coping profiles in the context of global environmental threats: a person-centered approach. Anxiety Stress Coping. 2022;35(5):609–622. doi:10.1080/10615806.2021.2004132
26. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
27. Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a monte carlo simulation study. Struct Equat Model. 2007;14(4):535–569. doi:10.1080/10705510701575396
28. Bodenmann G, Arista LJ, Walsh KJ, Randall AK. Dyadic Coping Inventory. In: Lebow J, Chambers A, Breunlin DC, editors. Encyclopedia of Couple and Family Therapy. Springer International Publishing; 2018:1–5.
29. Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–976. doi:10.1017/s0033291702006074
30. Boivin J, Takefman J, Braverman A. The Fertility Quality of Life (FertiQoL) tool: development and general psychometric properties. Fertil Steril. 2011;96(2):409–415.e3. doi:10.1016/j.fertnstert.2011.02.046
31. Akaike H. A new look at the statistical model identification. IEEE Trans Autom Control. 1974;19(6):716–723. doi:10.1109/TAC.1974.1100705
32. Schwarz G. Estimating the dimension of a model. Ann Stat. 1978;6(2):461–464.
33. Arminger G, Stein P, Wittenberg J. Mixtures of conditional mean- and covariance-structure models. Psychometrika. 1999;64(4):475–494. doi:10.1007/BF02294568
34. Muthén B. Latent variable analysis: growth mixture modeling and related techniques for longitudinal data; 2004.
35. Cai T, Qian J, Huang Q, Yuan C. Distinct dyadic coping profiles in Chinese couples with breast cancer. Support Care Cancer. 2021;29(11):6459–6468. doi:10.1007/s00520-021-06237-2
36. Nagy L, Balázs K. Typical coping patterns: a person-centered approach to coping. New Ideas Psychol. 2023;70:101023. doi:10.1016/j.newideapsych.2023.101023
37. Li J, Liu L, Chen M, Su W, Yao T, Li X. Effect of intimacy and dyadic coping on psychological distress in pancreatic cancer patients and spousal caregivers. Front Psychol. 2023;14:1040460. doi:10.3389/fpsyg.2023.1040460
38. Muijres P, Weitkamp K, Bodenmann G, Jenewein J. Discrepancies in dyadic coping: associations with distress and quality of life in couples facing early stage dementia. Front Psychol. 2023;14:1056428. doi:10.3389/fpsyg.2023.1056428
39. Brandão T, Schulz MS, Matos PM. Psychological adjustment after breast cancer: a systematic review of longitudinal studies. Psycho Oncolo. 2017;26(7):917–926. doi:10.1002/pon.4230
40. Wesner AC, Gomes JB, Detzel T, Blaya C, Manfro GG, Heldt E. Effect of cognitive-behavioral group therapy for panic disorder in changing coping strategies. Compreh Psychiatry. 2014;55(1):87–92. doi:10.1016/j.comppsych.2013.06.008
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychological Distress, Dyadic Coping, and Quality of Life in Infertile Clients Undergoing Assisted Reproductive Technology in China: A Single-Center, Cross-Sectional Study
Bai J, Zheng J, Dong Y, Wang K, Cheng C, Jiang H
Journal of Multidisciplinary Healthcare 2022, 15:2715-2723
Published Date: 29 November 2022
Predictive Models of Psychological Distress, Quality of Life, and Adherence to Medication in Breast Cancer Patients: A Scoping Review
Pezzolato M, Spada GE, Fragale E, Cutica I, Masiero M, Marzorati C, Pravettoni G
Patient Preference and Adherence 2023, 17:3461-3473
Published Date: 19 December 2023
Problematic Use of Internet Associates with Poor Quality of Life via Psychological Distress in Individuals with ADHD
Chen CY, Lee KY, Fung XCC, Chen JK, Lai YC, Potenza MN, Chang KC, Fang CY, Pakpour AH, Lin CY
Psychology Research and Behavior Management 2024, 17:443-455
Published Date: 9 February 2024
The Sequelae and Moderators of Influence of Dandruff on Mental Health Among Mainland Chinese Adults
Chan CS, Smith T, He Z, Garter C
Clinical, Cosmetic and Investigational Dermatology 2024, 17:1333-1346
Published Date: 11 June 2024
Psychological-Symptom Mismatch Phenotypes and Their Clinical Implications in Patients with Chronic Obstructive Pulmonary Disease
Cai Y, Ren X, Wang K, Cheng H
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:593901
Published Date: 11 June 2026