")
Back to Journals » Patient Preference and Adherence » Volume 17
Predictive Models of Psychological Distress, Quality of Life, and Adherence to Medication in Breast Cancer Patients: A Scoping Review
Authors Pezzolato M , Spada GE, Fragale E , Cutica I , Masiero M, Marzorati C , Pravettoni G
Received 13 September 2023
Accepted for publication 27 November 2023
Published 19 December 2023 Volume 2023:17 Pages 3461—3473
DOI https://doi.org/10.2147/PPA.S440148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
M Pezzolato,1,2,* G E Spada,1,* E Fragale,1 I Cutica,2 M Masiero,1,2 C Marzorati,1 G Pravettoni1,2
1Applied Research Division for Cognitive and Psychological Science, European Institute of Oncology, IRCCS, Milan, Italy; 2Department of Oncology and Hemato-Oncology, University of Milan, Milan, Italy
*These authors contributed equally to this work
Correspondence: G E Spada, Applied Research Division for Cognitive and Psychological Science, IEO European Institute of Oncology IRCCS, Via Ripamonti, 435, Milan, Italy, Tel +39 02 57489.207, Email [email protected]
Purpose: An interplay of clinical and psychosocial variables affects breast cancer patients’ experiences and clinical trajectories. Several studies investigated the role of socio-demographic, clinical, and psychosocial factors in predicting relevant outcomes in breast cancer care, thus developing predictive models. Our aim is to summarize predictive models for specific psychological and behavioral outcomes: psychological distress, quality of life, and medication adherence. Specifically, we aim to map the determinants of the outcomes of interest, offering a thorough overview of these models.
Methods: Databases (PubMed, Scopus, Embase) have been searched to identify studies meeting the inclusion criteria: a breast cancer patients’ sample, development/validation of a predictive model for selected psychological/behavioral outcomes (ie, psychological distress, quality of life, and medication adherence), and availability of English full-text.
Results: Twenty-one papers describing predictive models for psychological distress, quality of life, and adherence to medication in breast cancer were included. The models were developed using different statistical approaches. It has been shown that treatment-related factors (eg, side-effects, type of surgery or treatment received), socio-demographic (eg, younger age, lower income, and inactive occupational status), clinical (eg, advanced stage of disease, comorbidities, physical symptoms such as fatigue, insomnia, and pain) and psychological variables (eg, anxiety, depression, body image dissatisfaction) might predict poorer outcomes.
Conclusion: Predictive models of distress, quality of life, and adherence, although heterogeneous, showed good predictive values, as indicated by the reported performance measures and metrics. Many of the predictors are easily available in patients’ health records, whereas others (eg, coping strategies, perceived social support, illness perceptions) might be introduced in routine assessment practices. The possibility to assess such factors is a relevant resource for clinicians and researchers involved in developing and implementing psychological interventions for breast cancer patients.
Keywords: breast cancer, predictive model, psychological distress, quality of life, adherence, predictors
Introduction
With more than two million new cases in 2020 worldwide, Breast Cancer (BC) is the most frequent form of cancer for incidence and prevalence and the first in mortality among women.1 Moreover, BC’s impact extends beyond its clinical implications, affecting various psychological, relational, and social dimensions and impairing globally patients’ Quality of Life (QoL).2–5
Psychological distress, a state of emotional suffering characterized by various combinations of anxious and depressive symptoms, is widespread among BC patients in every stage of the disease, from diagnosis to survivorship.6–8 Coherently, rates of psychological disorders are higher among BC patients when compared with the general population: recent systematic reviews reported that 32.2% of BC patients suffer from depression and 41.9% from anxiety.9,10 Furthermore, psychological distress is associated with poorer clinical outcomes, such as a higher risk of cancer recurrence, poorer survival, greater all-cause and cancer-related mortality and morbidity,11–14 poorer QoL, and lower adherence to medication.13
QoL refers to how patients perceive their own health, considering its physical, mental, and social dimensions.15,16 QoL is commonly considered one of the key outcomes for BC patients, and its improvement is often one of the main aims of psychological interventions designed for them.16,17 However, although during the last decade an increase in BC patients’ QoL has been reported,16 there are still several disease-related factors that may undermine BC patients’ QoL, such as symptoms (eg, pain and lymphedema), adverse psychological effects (eg, worries, anxiety, depressive symptoms), sexual dysfunctions, and adverse side effects.16,17
One of the issues in which psychological distress and QoL intertwine with clinical aspects is adherence to therapy.18 Among BC patients with a prescription for endocrine therapy, medication adherence rates are commonly suboptimal: a recent review19 reported 5-years adherence rates ranging from 33.3% to 88.6%, with an average decrease of 25.5% for each year of treatment. Non-adhering behaviors originate from a multidimensional array of factors (eg, age, comorbidities, adverse effects). Nonetheless, it is worth noting that depression and poor QoL have been associated with lower medication adherence.19–21 Since optimal adherence rates are associated with better clinical outcomes and better QoL,22–24 supporting BC patients in maintaining optimal adherence is a relevant and actual cancer care goal.
In summary, a complex interplay of clinical and psychosocial variables plays a relevant role in BC patients’ clinical trajectories, shaping their experiences with the disease and affecting their QoL.12,23–26 Several studies investigated socio-demographic, clinical, and psychosocial factors that might influence the subjective variability observed in BC patients on psychological distress, QoL, and adherence. Several predictive models have been developed through different statistical methods (eg, linear regression, logistic regression, structural equation modeling);27–31 some of these models have been further validated in additional samples, testing the model in other groups,28,31 and they have been eventually applied in clinical practice, particularly in patients’ assessment. Indeed, the clinical utility of such predictive models lies in the fact that identifying beforehand patients at a greater risk of severe psychological distress, poor QoL, or medication non-adherence could aid the assessment of those in greater need of psychological interventions.32–35
In the present paper, we reviewed studies in which models have been developed or implemented in order to predict one of the following outcomes in BC patients: (1) psychological distress and adjustment; (2) QoL; and (3) medication adherence. To our knowledge, this is the first review that takes into account models predicting these three relevant outcomes. Thus, the data here collected and commented on will be an important asset for healthcare professionals and researchers working in the field of BC care.
Coherently, the primary aim was to summarize the predictive models currently available in the health field, to report their characteristics, and to map the determinants of the three outcomes of interest. By offering an overview of the scientific literature on these themes, we aim to highlight relevant knowledge that could aid BC patients’ care path, fostering optimal psychological assessment, supporting emotional wellbeing, optimal medication adherence, and good QoL. Due to the wide range of our research questions and the exploratory nature of this work, we chose to adopt the scoping review format.36
Materials and Methods
An online search was conducted in January 2023 in order to identify relevant studies developing or using models to predict specific psychological outcomes (ie, QoL, psychological distress, adjustment, or medication adherence) in BC patients. Three online sources were screened (PubMed, Embase, and Scopus) with the following keywords: (breast cancer) AND (predictive model OR prediction model OR prognostic model OR prediction tool OR predictive tool OR prognostic tool) AND (quality of life OR depression OR anxiety OR distress OR adherence OR compliance OR psychological OR psychosocial). The search criteria did not include any restrictions on publication dates.
Following the extension for scoping reviews of the Preferred Reporting of Items for Systematic Reviews and Meta-Analyses Statement (PRISMA-ScR),37 the initial selection process resulted in the identification of 371 studies. After duplicates removal, 231 articles were screened for title and abstract. Abstracts, commentaries, editorials, letters, meta-analyses, proposals, and reviews were excluded. At the end of this process, 171 studies were excluded, and 60 full-text articles were analyzed. Only research articles that satisfied the following inclusion criteria were considered: 1) study populations consisting of BC patients; 2) development/use of predictive model; 3) psychological outcomes are predicted; 4) papers published in English.
In the screening phase, papers that did not report outcomes of our interest were excluded, as well as studies focused only on medical variables. The screening phase was independently conducted by two authors (M.P., E.F.). Interrater reliability for the assessors was calculated on a dichotomous scale using percentage agreement and Cohen’s k (% of agreement: 72.64% Cohen’s k: 0.377). A third author (G.E.S.) resolved discordances between raters. At the end of the process, 21 papers were selected (see Figure 1 for more details). Most authors (M.P., G.E.S., E.F., I.C.) read selected articles to accept their inclusion in the study.
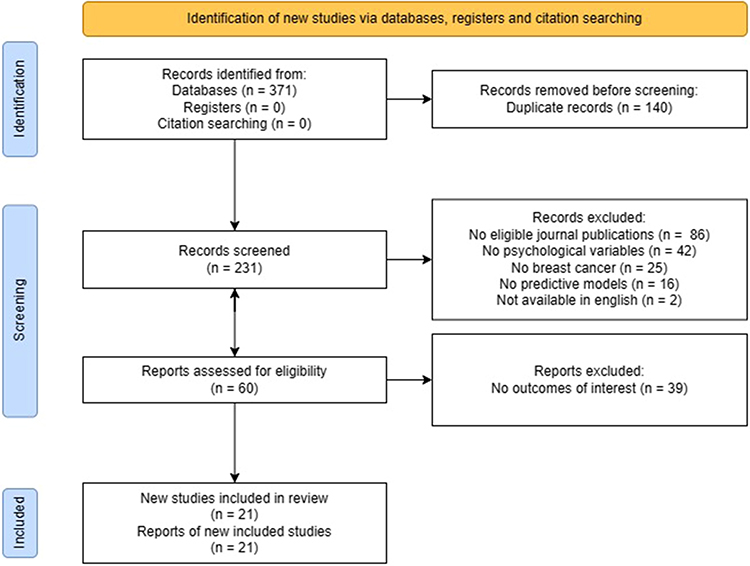 |
Figure 1 PRISMA Flow Diagram for the scoping review process. |
Results
Selection of Sources of Evidence
A first search in the literature identified 236 potential articles. After the screening procedure, 21 of the selected studies met the inclusion criteria for the scoping review. Specifically, nine original studies were focused on the prediction of psychological distress and adjustment, six on the prediction of QoL, and six on the prediction of adherence and treatment discontinuation.
All the included studies reported these outcomes of interest as their primary outcomes.
Characteristics of Selected Studies
Relevant data for each included paper are reported in Table 1 (psychological distress and adjustment), Table 2 (QoL), and Table 3 (adherence).
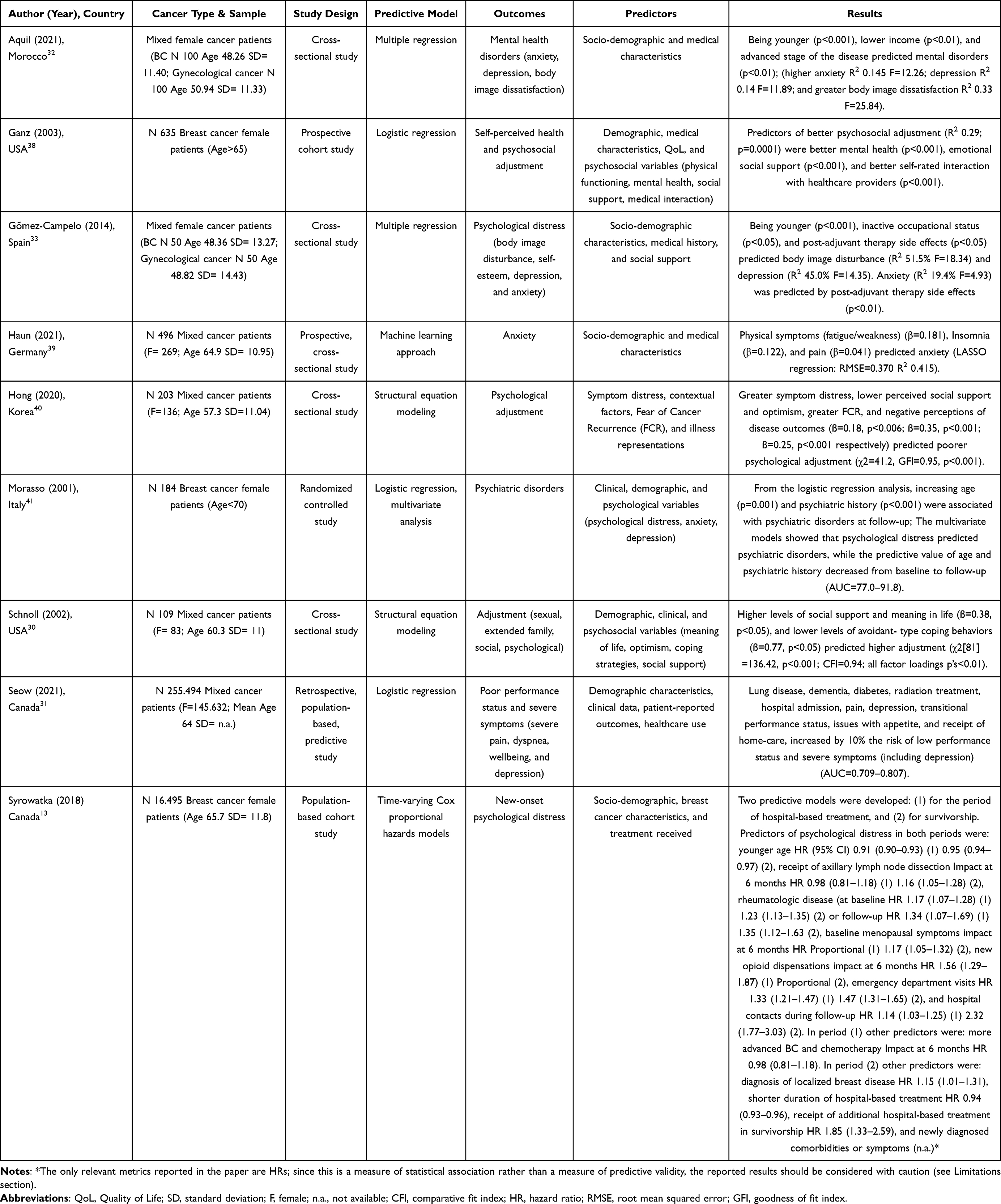 |
Table 1 Original Research Studies on the Prediction of Psychological Distress: Characteristics and Results |
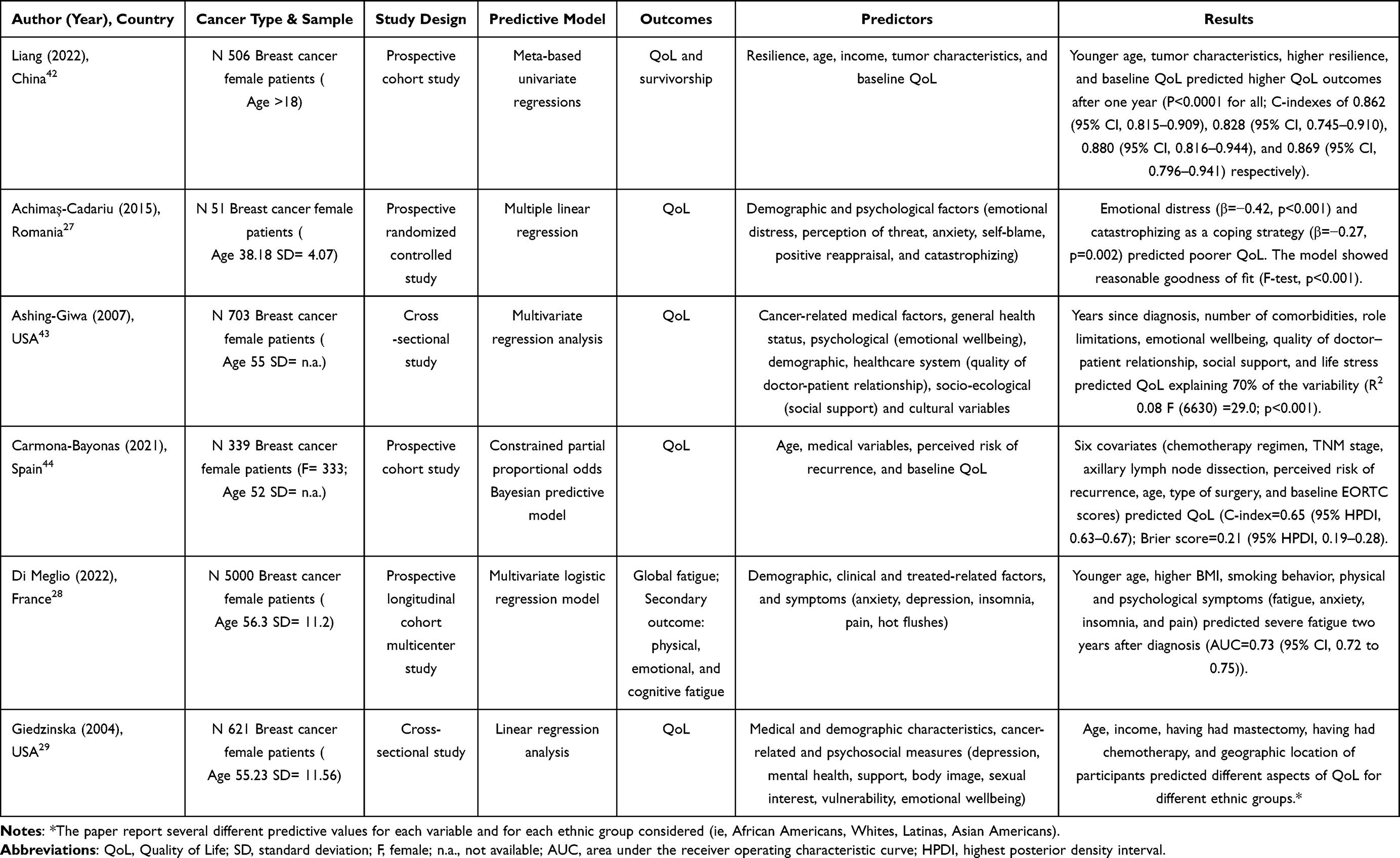 |
Table 2 Original Research Studies on the Prediction of Quality of Life: Characteristics and Results |
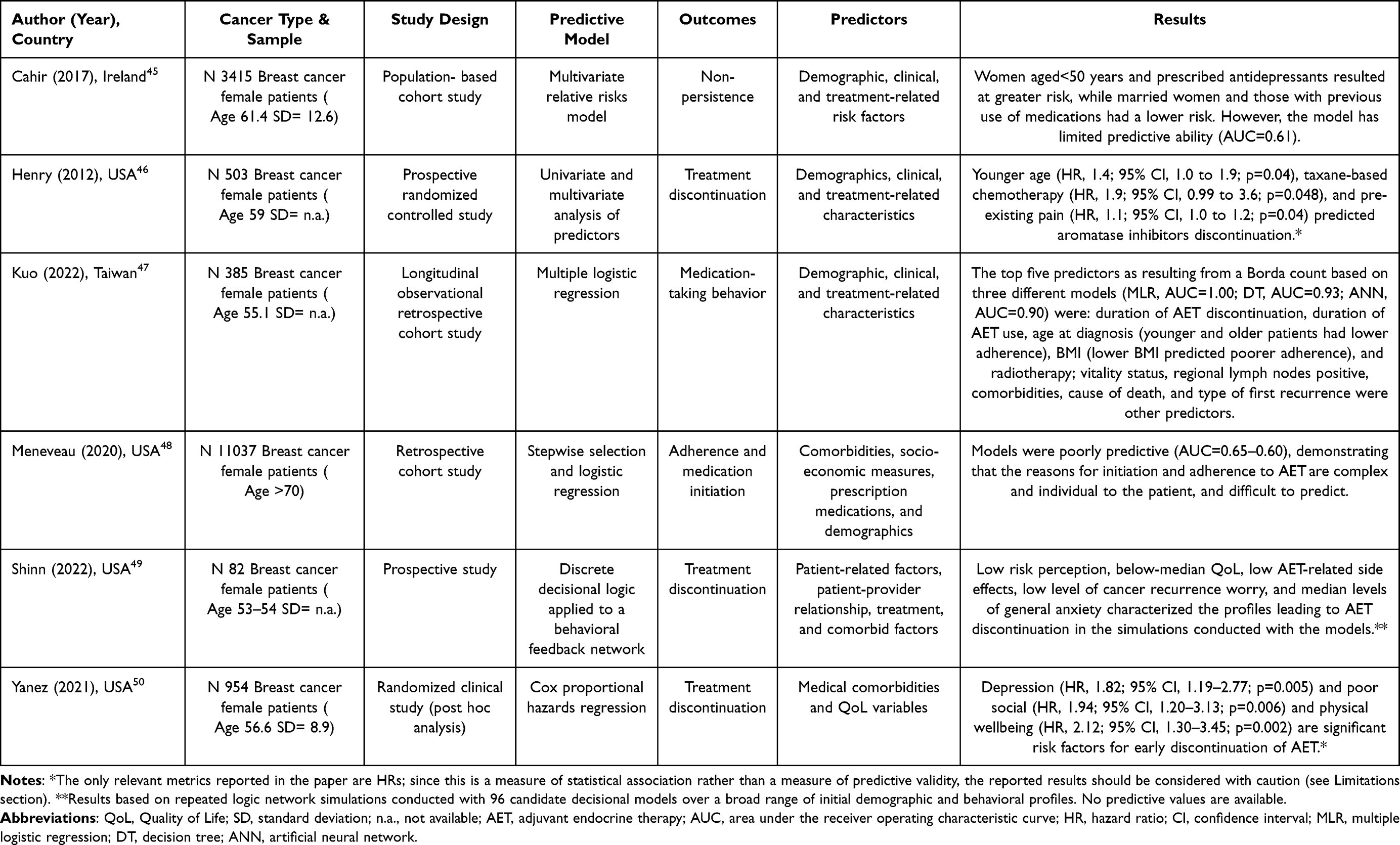 |
Table 3 Original Research Studies on the Prediction of Adherence and Treatment Discontinuation: Characteristics and Results |
Concerning the prediction of psychological distress and adjustment, samples from the nine selected studies included either BC patients only (n = 3)13,38,41 or patients affected by several cancer types, also including BC patients (n = 6).30–33,39,40 Studies were focused on the following outcomes, alone or in combination: self-perceived health, psychiatric disorders, psychological distress and mental health disorders (body image disturbance, self-esteem, depression, and anxiety), psychosocial adjustment (sexual, extended family, social, psychological), new onset of psychological distress or other disorders. Predictive models of such studies adopted different methodologies, and the applied techniques consisted of multivariate regression analysis (logistic or linear), hazards or structural equation modeling, and machine learning approaches.
Concerning the prediction of cancer patients’ QoL (Table 2), all the samples from the six selected studies included BC patients only.27–29,42–44 Such studies investigated the following outcomes: QoL, survivorship, global fatigue, physical, emotional, and cognitive fatigue. Considered predictive models used several methodologies, precisely: univariate or multivariate, logistic or linear regression, and proportional odds Bayesian model.
Concerning the prediction of pharmacological adherence (Table 3), all the samples from the six selected studies included BC patients only.45–50 All the studies focused on adherence to oral endocrine therapy, analyzing the following outcomes: medication adherence, medication initiation, non-persistence, medication-taking behavior, and treatment discontinuation. The predictive models used several methodologies: univariate and multivariate analysis, relative risks models, logistic regression analysis, hazard modeling, and discrete decisional logic applied to a behavioral feedback network were considered in the present review.
Consistently with the heterogeneity of the predictive models, several different metrics of models’ performance are reported: these are R-squared (coefficient of determination), beta coefficient, Area Under the Curve (AUC), Concordance index (C-index), Comparative Fit Index (CFI), goodness of fit index (GFI), and root mean squared error (RMSE) (models’ metrics are reported in Tables 1–3).
Synthesis of Results
Psychological Distress and Adjustment
As reported in Table 1, two studies used logistic regression,31,38 two a multivariate regression,32,33 and one a combination of both.41 Two papers used structural equation modeling,30,40 and one13 reported a time varying cox hazard predictive model. Finally, one study39 implemented a machine learning approach.
Such studies highlighted the role of socio-demographic, psychosocial, and medical characteristics as potential predictors of mental health disorders and wellbeing. For example, results showed that younger age,13,32,33 lower income,32 and inactive occupational status33 predicted higher psychological distress. In contrast, Morasso et al41 found that younger age had a protective effect on psychological symptoms.
As concerning medical factors, advanced stage of disease,13,32 therapy side-effects,33 radiation treatment,31 receipt of axillary lymph node dissection, baseline menopausal symptoms,13 and several physical symptoms such as fatigue, insomnia, and pain,31,39 predicted a higher risk to develop symptoms of psychological distress.
Furthermore, mental health issues before disease onset, such as higher anxiety and depression and higher body image dissatisfaction31,32,41 were predictive factors for psychological symptoms development.
As regards psychological adjustment, studies found that better mental health at baseline and high perceived emotional and social support30,38 predicted better psychosocial adjustment. In contrast, lower optimism, greater fear of cancer recurrence, negative perceptions of disease outcomes, worst illness representations, and lack of perceived social support predicted poorer psychological adjustment.40
Quality of Life
As concerning patients’ QoL, as reported in Table 2, five out of six of the included studies27–29,42,43 applied a predictive model obtained through univariate or multivariate logistic or linear regressions. One study developed a constrained partial proportional odds Bayesian model.44
Results show that predictors for a good QoL were as follows: high baseline QoL, high resilience, and emotional wellbeing,42–44 low emotional distress or life stress, low limitations due to physical or emotional problems, and low cognitive tendency to catastrophize,27,43 low perceived risk of recurrence,44 not smoking,28 higher income,29 a good quality of doctor–patient relationship, and a high perceived social support.43
Interestingly, while two studies reported that younger age predicted higher QoL,29,42 another one found that “extreme” ages (younger and older patients) were at higher risk of poor QoL,44 and another one reported that younger age predicted a more significant risk of severe fatigue at two years after BC diagnosis.28
Furthermore, some physical conditions, such as Body Mass Index (BMI),28 the presence of comorbidities,43 or symptoms such as fatigue, anxiety, insomnia, and pain,28 and several medical variables such as years since diagnosis,43 tumor characteristics,42,44 type of surgery or treatment received (ie, mastectomy, axillary lymph node dissection, chemotherapy),29,44 accounted for a large part of the variance of QoL.
Adherence
As reported in Table 3, the methodologies used in studies selected for adherence are heterogeneous: risk models,45 logistic regressions,47,48 univariate and multivariate analysis of predictors,46 decisional logic applied to a behavioral feedback network,49 and cox proportional hazard regression.50
These studies analyzed the predictive values of various demographic, clinical, and treatment-related risk factors. Precisely, a higher risk of non-adherence was predicted by younger age45,46 or “extreme” age (younger and older),47 lower BMI,47 taxane-based chemotherapy, pain,46 low risk perception and low level of cancer recurrence worry,49 depression, general anxiety, and poor QoL.49,50 Notably, two of the examined models were reported to show only poor predictive ability, as indicated by the suboptimal area under the receiver-operating characteristics curve values.45,48
Discussion
Results show that socio-demographic and medical characteristics13,31–33,39,41 were the most commonly reported predictors for psychological distress. In particular, younger age has been shown to predict the onset of psychological distress in three of the selected articles,13,32,33 but one paper reported that advanced age, together with psychiatric history and baseline psychological distress, is a predictor of the occurrence of psychiatric disorders.41 A possible explanation for such inconsistency might be the different definitions and measures of psychological distress used. Indeed, the outcome of interest in Morasso et al study41 was the presence of a psychiatric disorder identified by a psychiatrist during an interview with the help of the Structured Clinical Interview for DSM-III-R.51 In contrast, other studies assessed the presence of psychological distress through the Hospital Anxiety and Depression Scale,52 the Body Image Scale,53 the Beck Depression Inventory,54 and the Beck Anxiety Inventory,32,33,55 or through medical health records data.13 Other possible explanations for this discrepancy may be found in cultural and geographical differences between the participants. Indeed, Morasso et al study41 was conducted in Italy, while the others were conducted respectively in Morocco, Spain, and Canada.13,32,33 Other socio-demographic factors that predict psychological distress are lower income32 and inactive occupational status.33 This may be explained by the fact that these socio-demographic characteristics are possible causes of psychological distress, given the uncertainty, worries, and economic difficulties they may generate. Therefore, it is reasonable to expect that, when combined with an illness such as BC, they result in greater levels of psychological distress.
Similarly, several clinical characteristics showed predictive value in psychological distress models. These were advanced stages of the tumor,32 the presence of symptoms such as pain, insomnia, fatigue/weakness,33,39,40 psychiatric history and baseline psychological distress,31,41 comorbidities,13,31 and treatment-related factors, such as adverse side-effects, hospital admissions, emergency department visits, radiation therapy, chemotherapy, opioid dispensation, and receipt of home-care.13,31,33 These characteristics are all indexes of worst general clinical conditions, both on physical and psychological levels. Only three studies developed predictive models of psychological adjustment.30,38,40 Interestingly, all of them highlighted the role of specific psychological determinants such as social support, coping strategies, interactions with healthcare providers, optimism, fear of cancer recurrence, and illness perceptions.30,38,40 It is worth noting that four out of nine studies developing predictive models for psychological distress took into account only clinical and sociodemographic variables. Since the role of psychological variables has been suggested by the other models reviewed,30,38,40 the consideration of baseline psychological variables as predictors may further improve such models. Introducing psychological assessment for BC patients in the clinical routine could increase the availability of these data, thus helping to close this gap.
Concerning QoL, predictive models have recognized a possible predictive role of psychological variables on QoL, except for Giedzinska et al.29 More in detail, results showed that resilience, anxiety, emotional wellbeing/distress, quality of patient–doctor relationship, social support, perceived risk of recurrence, life stress, coping strategies, and baseline QoL, are all psychological predictors of QoL.27,28,42–44 Other commonly reported predictors were demographic and medical variables such as age, income, BMI, smoking behavior, concomitant symptoms, tumor characteristics, comorbidities, treatment regimen, and having received surgical intervention.27,29,42–44 The multidimensional nature of the predictors identified is consistent with the multidimensional nature of the concept of QoL, which refers to physical, mental, and social dimensions.15,16
Finally, all the studies focusing on non-adherence considered adherence to endocrine therapy. These medicines are often taken orally, generally for five to ten years, thus charging the burden of their correct and regular assumption on the patients themselves.56 Demographics and clinical variables, and treatment-related factors45–50 were relevant predictors of non-adherence. Notably, depression was found to predict medication non-adherence,45,50 thus confirming what has already been reported by previous studies in this field.19
It is worth noting that two of the studies focusing on adherence reported poor predictive value.45,48 This further confirms the complex nature of medication-taking behaviors: the interaction of several factors and the role of patients’ subjectivity make adherence to medication difficult to predict.19,20
Many of the predictors included in the considered models are easily available in patients’ health records (eg, clinical history, socio-demographic variables, cancer-related or treatment-related data) and can therefore be readily used by clinicians and researchers in order to assess patients’ risks. On the contrary, those predictors that are not commonly found in patients’ health records (eg, coping strategies, perceived social support, illness perceptions) may be introduced in routine assessment practices in hospitals and cancer clinics.
To conclude, considering the outcomes retrieved in the current scoping review, we have shown that predictive models of distress, QoL, and adherence outcomes, although various and heterogeneous in the considered predictors and in statistical methods, generally presented good scores in the reported performance measures and metrics. Implementing such models in clinical practice might support healthcare professionals in early identifying patients at risk of psychological comorbidities, non-adherence, and a lower QoL providing tailored interventions.
Implication and Suggestions for Research and Practice
Psychological interventions support emotional well-being and improve QoL.57,58 Furthermore, they can also reduce symptoms such as pain and fatigue,59–61 foster patients’ adherence to medications,62,63 and even improve overall survival.64,65 Unfortunately, offering psychological interventions to an increasing number of BC patients may not be feasible or cost-effective.66 By applying the predictive models reviewed here, it is possible to target psychological interventions to those patients who benefit the most from them, reducing healthcare-related costs and optimizing the BC care path. Specifically, the predictive models may identify patients at high risk of psychological distress, medication non-adherence, or poorer QoL. This may lead to prompt interventions reducing healthcare-related costs, and ultimately improving BC patients’ outcomes.
Given the presented results of this review, it seems that younger patients who show greater levels of distress or depressive symptoms, poorer coping ability or well-being might benefit from interventions aimed at preventing psychological comorbidities and adherence. Further, interventions addressing patients’ QoL are effective for patients reporting insomnia, pain, anxiety, or distress. The introduction of psychological and behavioral assessments would allow to map patients’ characteristics and identify patients potentially in need of a preventive intervention, thus allowing to improve therapeutic support. Within this framework, the synthesis outlined in this work might be a relevant resource for clinicians and researchers involved in developing and implementing psychological interventions for BC patients.
Limitations
This work has some worth-to-note limitations. First, the included studies display great heterogeneity concerning their characteristics and the applied methodologies, which may reduce the results’ interpretability. The predictive models reviewed have been developed using several different statistical methods (eg, multiple logistic regression, linear regression, machine learning approaches) and different metrics have been considered to measure the models’ performance (eg, ROC AUC, goodness of fit index, root mean squared error). Notably, three included studies did not report any measure of predictive validity, but only measures of statistical association (ie, hazard ratios), thus their results should be considered with caution13,46,50 (see Table 1 and Table 3); this is in line with what suggested by Varga et al67 in a recent systematic review: the authors documented the frequent misuse of the term “prediction” in studies involving only statistical association analyses.
Further, the predictive models generated predictions for different specific time points along the cancer care path (eg, 6-month, 1-year, 2-year). We argued that this might partially explain the differences encountered among the results. Furthermore, the use of different questionnaires and scales to measure the outcomes of interest and the great variability in sample dimensions (ranging from 51 to 255.494 patients), may further decrease the comparability of these studies.
The decision to focus on three different outcomes has contributed to the great heterogeneity of the included studies. Yet, this may be justified by the exploratory nature of this work and by our interest in mapping the predictors of a large range of issues relevant to BC care (ie, psychological distress, QoL, and medication adherence).
Finally, among the studies on psychological distress, only three considered samples entirely composed of BC patients.13,38,41 The other six explored mixed samples with different cancer types, although always including at least a sub-group of BC patients.
Conclusion
Predictive models taken into account could aid the early-identification of those BC patients that could benefit from tailored psychological interventions. Therefore, clinicians and researchers should consider these findings when implementing routine assessments in order to intervene early whenever a high risk of poorer outcomes is highlighted.
Acknowledgments
Massimo Pezzolato is a PhD student in Medical Humanities within the European School of Molecular Medicine (SEMM) at the University of Milan, Italy.
Disclosure
The study was supported by Pfizer Inc. Miss Gea E. Spada reports grants from European Institute of Oncology, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Ferlay J, Ervik M, Lam F, et al. Global cancer observatory: cancer today. Lyon, France: International Agency for Research on Cancer; 2020. Available from: https://gco.iarc.fr/today.
2. Meier F, Cairo Notari S, Bodenmann G, Revenson TA, Favez N. We are in this together — aren’t we? Congruence of common dyadic coping and psychological distress of couples facing breast cancer. Psychooncology. 2019;28(12):2374–2381. doi:10.1002/pon.5238
3. Nakamura ZM, Deal AM, Nyrop KA, et al. Serial assessment of depression and anxiety by patients and providers in women receiving chemotherapy for early breast cancer. Oncologist. 2021;26(2):147–156. doi:10.1002/onco.13528
4. Ofei SD, Teye-Kwadjo E, Amankwah-Poku M, et al. Determinants of posttraumatic growth and quality of life in Ghanaian breast cancer survivors. Cancer Invest. 2023;2023:1–35.
5. Zhang J, Zhou Y, Feng Z, Xu Y, Zeng G. Longitudinal trends in anxiety, depression, and quality of life during different intermittent periods of adjuvant breast cancer chemotherapy. Cancer Nurs. 2018;41(1):62–68. doi:10.1097/NCC.0000000000000451
6. Aitken LA, Hossan SZ. The psychological distress and quality of life of breast cancer survivors in Sydney, Australia. Healthc. 2022;10(10):2017. doi:10.3390/healthcare10102017
7. Maass SWMC, Boerman LM, Verhaak PFM, Du J, de Bock GH, Berendsen AJ. Long-term psychological distress in breast cancer survivors and their matched controls: a cross-sectional study. Maturitas. 2019;130:6–12. doi:10.1016/j.maturitas.2019.09.003
8. Mertz BG, Bistrup PE, Johansen C, et al. Psychological distress among women with newly diagnosed breast cancer. Eur J Oncol Nurs. 2012;16(4):439–443. doi:10.1016/j.ejon.2011.10.001
9. Hashemi SM, Rafiemanesh H, Aghamohammadi T, et al. Prevalence of anxiety among breast cancer patients: a systematic review and meta-analysis. Breast Cancer. 2020;27:166–178. doi:10.1007/s12282-019-01031-9
10. Pilevarzadeh M, Amirshahi M, Afsargharehbagh R, Rafiemanesh H, Hashemi SM, Balouchi A. Global prevalence of depression among breast cancer patients: a systematic review and meta-analysis. Breast Cancer Res Treat. 2019;176:519–533. doi:10.1007/s10549-019-05271-3
11. Bhattacharya M, Parsons H, Call K, Blaes A, McAlpine D. Impact of a pre-existing diagnosis of mental illness on stage of breast cancer diagnosis among older women. Breast Cancer Res Treat. 2023;197(1):201–210. doi:10.1007/s10549-022-06793-z
12. Kanani R, Davies EA, Hanchett N, Jack RH. The association of mood disorders with breast cancer survival: an investigation of linked cancer registration and hospital admission data for South East England. Psychooncology. 2016;25(1):19–27. doi:10.1002/pon.4037
13. Syrowatka A, Hanley JA, Weir DL, Dixon WG, Meguerditchian AN, Tamblyn R. Ability to predict new-onset psychological distress using routinely collected health data: a population-based cohort study of women diagnosed with breast cancer. JNCCN J Natl Compr Cancer Netw. 2018;16(9):1065–1073. doi:10.6004/jnccn.2018.7038
14. Wang X, Wang N, Zhong L, et al. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: a systematic review and meta-analysis of 282,203 patients. Mol Psychiatry. 2020;25:3186–3197. doi:10.1038/s41380-020-00865-6
15. Ayalew TL, Wale BG, Haile KE, Zewudie BT, Feleke MG. Health-related quality of life and associated factors among cancer patients in Ethiopia: systematic review and meta-analysis. PLoS One. 2022;17:1.
16. Mokhtari-Hessari P, Montazeri A. Health-related quality of life in breast cancer patients: review of reviews from 2008 to 2018. Health Qual Life Outcomes. 2020;18:1–25. doi:10.1186/s12955-020-01591-x
17. Javan Biparva A, Raoofi S, Rafiei S, et al. Global quality of life in breast cancer: systematic review and meta-analysis. BMJ Support Palliat Care. 2022;1:1–9.
18. Jiang H, Dong Y, Zong W, Zhang X, Xu H, Jin F. The relationship among psychosocial adaptation, medication adherence and quality of life in breast cancer women with adjuvant endocrine therapy. BMC Women's Health. 2022;22(1). doi:10.1186/s12905-022-01722-0
19. Yussof I, Mohd Tahir NA, Hatah E, Mohamed Shah N. Factors influencing five-year adherence to adjuvant endocrine therapy in breast cancer patients: a systematic review. Breast. 2022;62:22–35. doi:10.1016/j.breast.2022.01.012
20. Pinheiro LC, Wheeler SB, Reeder-Hayes KE, Samuel CA, Olshan AF, Reeve BB. Investigating associations between health-related quality of life and endocrine therapy underuse in women with early-stage breast cancer. J Oncol Pract. 2017;13(5):e463–71. doi:10.1200/JOP.2016.018630
21. Inotai A, Ágh T, Maris R, et al. Systematic review of real-world studies evaluating the impact of medication non-adherence to endocrine therapies on hard clinical endpoints in patients with non-metastatic breast cancer. Cancer Treat Rev. 2021;100:102264. doi:10.1016/j.ctrv.2021.102264
22. Stahlschmidt R, Ferracini AC, de Souza CM, de Medeiros LM, Juliato CRT, Mazzola PG. Adherence and quality of life in women with breast cancer being treated with oral hormone therapy. Support Care Cancer. 2019;27(10):3799–3804. doi:10.1007/s00520-019-04671-x
23. Bai X, Zhang X, Xiang W, et al. Time tracking and multidimensional influencing factors analysis on female breast cancer mortality: evidence from urban and rural China between 1994 to 2019. Front Public Heal. 2022;2022:10.
24. Coughlin SS. Social determinants of breast cancer risk, stage, and survival. Breast Cancer Res Treat. 2019;177:537–548. doi:10.1007/s10549-019-05340-7
25. Emerson MA, Reeve BB, Gilkey MB, et al. Job loss, return to work, and multidimensional well-being after breast cancer treatment in working-age Black and White women. J Cancer Surviv. 2022;17:805–814. doi:10.1007/s11764-022-01252-6
26. Veličković K, Borrebaeck CAK, Bendahl PO, et al. One-year recovery from breast cancer: importance of tumor and treatment-related factors, resilience, and sociodemographic factors for health-related quality of life. Front Oncol. 2022;12. doi:10.3389/fonc.2022.891850
27. Achimaș-Cadariu P, Iancu M, Pop F, Vlad C, Irimie A. Psychological screening and health related quality of life in Romanian breast cancer survivors. J Evid Based Psychother. 2015;15(2):267.
28. Di Meglio A, Havas J, Soldato D, et al. Development and validation of a predictive model of severe fatigue after breast cancer diagnosis: toward a personalized framework in survivorship care. J Clin Oncol. 2022;40(10):1111–1123. doi:10.1200/JCO.21.01252
29. Giedzinska AS, Meyerowitz BE, Ganz PA, Rowland JH. Health-related quality of life in a multiethnic sample of breast cancer survivors. Ann Behav Med. 2004;28(1):39–51. doi:10.1207/s15324796abm2801_6
30. Schnoll RA, Knowles JC, Harlow L. Correlates of adjustment among cancer survivors. J Psychosoc Oncol. 2002;20(1):37–59. doi:10.1300/J077v20n01_03
31. Seow H, Tanuseputro P, Barbera L, et al. Development and validation of a prediction model of poor performance status and severe symptoms over time in cancer patients (PROVIEW+). Palliat Med. 2021;35(9):1713–1723. doi:10.1177/02692163211019302
32. Aquil A, El Kherchi O, El Azmaoui N, et al. Predictors of mental health disorders in women with breast and gynecological cancer after radical surgery: a cross-sectional study. Ann Med Surg. 2021;65:102278. doi:10.1016/j.amsu.2021.102278
33. Gõmez-Campelo P, Bragado-álvarez C, Hernández-Lloreda MJ. Psychological distress in women with breast and gynecological cancer treated with radical surgery. Psychooncology. 2014;23(4):459–466. doi:10.1002/pon.3439
34. Kourou K, Manikis G, Poikonen-Saksela P, et al. A machine learning-based pipeline for modeling medical, socio-demographic, lifestyle and self-reported psychological traits as predictors of mental health outcomes after breast cancer diagnosis: an initial effort to define resilience effects. Comput Biol Med. 2021;131:104266. doi:10.1016/j.compbiomed.2021.104266
35. Lopes C, Severo M, Fontes F, et al. Trajectories of anxiety and depression symptoms over five years since breast cancer diagnosis: results of the NEON-BC prospective study. Healthc. 2022;10(4):661. doi:10.3390/healthcare10040661
36. Munn Z, Peters MDJ, Stern C, et al. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18:143. doi:10.1186/s12874-018-0611-x
37. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
38. Ganz PA, Guadagnoli E, Landrum MB, Lash TL, Rakowski W, Silliman RA. Breast cancer in older women: quality of life and psychosocial adjustment in the 15 months after diagnosis. J Clin Oncol. 2003;21(21):4027–4033. doi:10.1200/JCO.2003.08.097
39. Haun MW, Simon L, Sklenarova H, Zimmermann-Schlegel V, Friederich H-C, Hartmann M. Predicting anxiety in cancer survivors presenting to primary care - A machine learning approach accounting for physical comorbidity. Cancer Med. 2021;10(14):5001–5016. doi:10.1002/cam4.4048
40. Hong SJ, Shin NM, Jung S. A predictive model of fear of cancer recurrence for patients undergoing chemotherapy. Support Care Cancer. 2020;28:4173–4181. doi:10.1007/s00520-019-05245-7
41. Morasso G, Costantini M, Viterbori P, et al. Predicting mood disorders in breast cancer patients. Eur J Cancer. 2001;37(2):216–223. doi:10.1016/S0959-8049(00)00390-7
42. Liang MZ, Tan Y, Knobf MT, et al. Resilience index improves prediction of 1-year decreased quality of life in breast cancer. J Cancer Surviv. 2022;2022:1–10.
43. Ashing-Giwa KT, Tejero JS, Kim J, Padilla GV, Hellemann G. Examining predictive models of HRQOL in a population-based, multiethnic sample of women with breast carcinoma. Qual Life Res. 2007;16:413–428. doi:10.1007/s11136-006-9138-4
44. Carmona-Bayonas A, Calderón C, Hernández R, et al. Prediction of quality of life in early breast cancer upon completion of adjuvant chemotherapy. NPJ Breast Cancer. 2021;7(1):92. doi:10.1038/s41523-021-00296-8
45. Cahir C, Barron TI, Sharp L, Bennett K. Can demographic, clinical and treatment-related factors available at hormonal therapy initiation predict non-persistence in women with stage I–III breast cancer? Cancer Causes Control. 2017;28:215–225. doi:10.1007/s10552-017-0851-9
46. Henry NL, Azzouz F, Desta Z, et al. Predictors of aromatase inhibitor discontinuation as a result of treatment-emergent symptoms in early-stage breast cancer. J Clin Oncol. 2012;30(9):936. doi:10.1200/JCO.2011.38.0261
47. Kuo CC, Wang HH, Tseng LP. Using data mining technology to predict medication‐taking behaviour in women with breast cancer: a retrospective study. Nursing Open. 2022;9(6):2646–2656. doi:10.1002/nop2.963
48. Meneveau MO, Keim-Malpass J, Camacho TF, Anderson RT, Showalter SL. Predicting adjuvant endocrine therapy initiation and adherence among older women with early-stage breast cancer. Breast Cancer Res Treat. 2020;184:805–816. doi:10.1007/s10549-020-05908-8
49. Shinn E, Busch BE, Jasemi N, et al. Network modeling of complex time-dependent changes in patient adherence to adjuvant endocrine treatment in ER+ breast cancer. Frontiers in Psychology. 2022;2022:4172.
50. Yanez B, Gray RJ, Sparano JA, et al. Association of modifiable risk factors with early discontinuation of adjuvant endocrine therapy: a post hoc analysis of a randomized clinical trial. JAMA Oncol. 2021;7(8):1196–1202. doi:10.1001/jamaoncol.2021.1693
51. Spitzer RL, Williams JBW, Gibbon M, First MB. The structured clinical interview for DSM-III-R (SCID): i: history, rationale, and description. Arch Gen Psychiatry. 1992;49(8):624–629. doi:10.1001/archpsyc.1992.01820080032005
52. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
53. Hopwood P, Fletcher I, Lee A, Al Ghazal S. A body image scale for use with cancer patients. Eur J Cancer. 2001;37(2):189–197. doi:10.1016/S0959-8049(00)00353-1
54. Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: twenty-five years of evaluation. Clin Psychol Rev. 1988;8(1):77–100. doi:10.1016/0272-7358(88)90050-5
55. Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. doi:10.1037/0022-006X.56.6.893
56. Greer JA, Amoyal N, Nisotel L, et al. A systematic review of adherence to oral antineoplastic therapies. Oncologist. 2016;21(3):354–376. doi:10.1634/theoncologist.2015-0405
57. Hwang KS, Lee KH, Yang CM, Lee HJ, Lee SY. Effects of psychosocial interventions for patients with breast cancer: a meta-analysis. Clin Psychopharmacol Neurosci. 2023;21(1):118–125. doi:10.9758/cpn.2023.21.1.118
58. Lai J, Song H, Ren Y, Li S, Xiao F. Effectiveness of supportive-expressive group therapy in women with breast cancer: a systematic review and meta-analysis. Oncol Res Treat. 2021;44:252–260. doi:10.1159/000515756
59. Wong WM, Chan DNS, He X, So WKW. Effectiveness of pharmacological and nonpharmacological interventions for managing the fatigue–sleep disturbance–depression symptom cluster in breast cancer patients undergoing chemotherapy. Cancer Nurs. 2022;46:E70–E80. doi:10.1097/NCC.0000000000001048
60. Johannsen M, Farver I, Beck N, Zachariae R. The efficacy of psychosocial intervention for pain in breast cancer patients and survivors: a systematic review and meta-analysis. Breast Cancer Res Treat. 2013;138(3):675–690. doi:10.1007/s10549-013-2503-4
61. Abrahams HJG, Knoop H, Schreurs M, et al. Moderators of the effect of psychosocial interventions on fatigue in women with breast cancer and men with prostate cancer: individual patient data meta-analyses. Psychooncology. 2020;29:1772–1785. doi:10.1002/pon.5522
62. Ream ME, Walsh EA, Jacobs JM, et al. Brief relaxation training is associated with long-term endocrine therapy adherence among women with breast cancer: post hoc analysis of a randomized controlled trial. Breast Cancer Res Treat. 2021;190(1):79–88. doi:10.1007/s10549-021-06361-x
63. Arch JJ, Crespi CM, Levin ME, et al. Randomized controlled pilot trial of a low-touch remotely-delivered values intervention to promote adherence to adjuvant endocrine therapy among breast cancer survivors. Ann Behav Med. 2022;56(8):856–871. doi:10.1093/abm/kaab118
64. Mustafa M, Carson-Stevens A, Gillespie D, Edwards AGK. Psychological interventions for women with metastatic breast cancer. Cochrane Database Syst Rev. 2013;2013:1.
65. Andersen BL, Yang HC, Farrar WB, et al. Psychologic intervention improves survival for breast cancer patients: a randomized clinical trial. Cancer. 2008;113(12):3450–3458. doi:10.1002/cncr.23969
66. Elting LS, Shih YCT. The economic burden of supportive care of cancer patients. Support Care Cancer. 2004;12:219–226. doi:10.1007/s00520-003-0513-1
67. Varga TV, Niss K, Estampador AC, Collin CB, Moseley PL. Association is not prediction: a landscape of confused reporting in diabetes – a systematic review. Diabetes Res Clin Pract. 2020;170:108497. doi:10.1016/j.diabres.2020.108497
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.