Back to Journals » Nature and Science of Sleep » Volume 18

Uncontrolled Hypertension from Inappropriate Ventilator Settings in Obstructive Sleep Apnea: A Case Report
Authors Tian SR, Thomas RJ, Ni YN
Received 23 February 2026
Accepted for publication 12 May 2026
Published 30 May 2026 Volume 2026:18 601053
DOI https://doi.org/10.2147/NSS.S601053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah L Appleton
Si-Rui Tian,1,2 Robert Joseph Thomas,3 Yue-Nan Ni1,2
1Department of Respiratory, Critical Care and Sleep Medicine, West China School of Medicine and West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China; 2Department of Respiratory Care, West China School of Medicine and West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 3Division of Pulmonary, Critical Care and Sleep Medicine, Beth Israel Deaconess Medical Center, Boston, MA, USA
Correspondence: Yue-Nan Ni, Department of Respiratory, Critical Care and Sleep Medicine, West China School of Medicine and West China Hospital, Sichuan University, No. 37 Guoxue Alley, Chengdu, 610041, People’s Republic of China, Email [email protected]
Abstract: This case report explores a typical instance of poorly controlled secondary hypertension associated with obstructive sleep apnea (OSA), specifically exacerbated during bilevel positive airway pressure (PAP) therapy, which was an inappropriate ventilator mode. The patient exhibited uncontrolled blood pressure and a high residual apnea-hypopnea index (AHI) while on bilevel therapy. Following a guided retitration of PAP therapy, both blood pressure control and residual AHI improved substantially. This report aims to provide an in-depth analysis of pathophysiological mechanisms underlying PAP therapy interactions with hypertension in OSA patients and to summarize key points for ventilator management in clinical practice.
Keywords: obstructive sleep apnea, bilevel, central sleep apnea, positive airway pressure, hypertension, case report
Case Presentation
A 53-year-old man with hypertension (values about 152/104 mmHg) and coronary artery disease, post-percutaneous transluminal coronary angioplasty, underwent overnight polysomnography. The study results indicated severe obstructive sleep apnea (OSA) with an apnea-hypopnea index (AHI) of 48.7/h and a nadir oxygen saturation of 68% (Figure 1A).
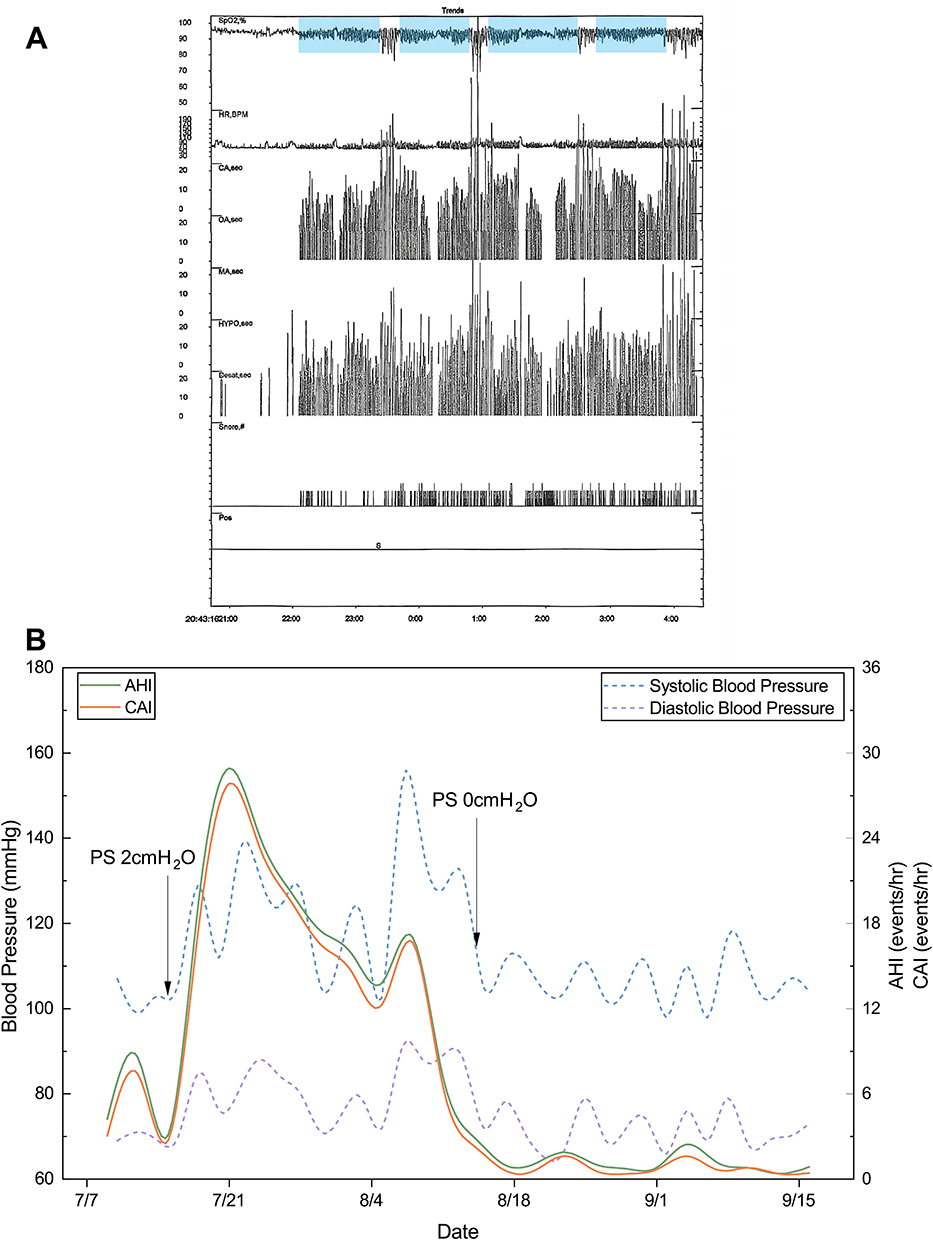 |
Figure 1 Polysomnography results and dynamic blood pressure changes. (A) Polysomnography hypnogram showed many obstructive apnea events and band shape of oxygen desaturation (blue background), which is a characteristic feature of high loop gain-driven sleep apnea. (B) This figure tracks the patient’s AHI and blood pressure over a two-month period, highlighting two specific ventilator mode modifications (indicated by arrows). Abbreviations: SpO2, oxygen saturation; HR, heart rate; CA, central apnea; OA, obstructive apnea; MA, mixed apnea; HYPO, hypopnea; Desat, desaturation; Pos, position; AHI, apnea-hypopnea index; CAI, central apnea index; PS, pressure support. |
Consequently, the patient was initiated on VAuto therapy by a private service with expiratory positive airway pressure (EPAP) at 7 cmH2O, inspiratory positive airway pressure (IPAP) at 14 cmH2O, and a minimum pressure support (PS) at 2 cmH2O. No titration of pressures was done. This pressure choice was based on comfort while awake. However, this ventilator setting resulted in discomfort while using during sleep, and a high residual AHI (7–9/h of use) was noted, mainly machine-detected central events. Blood pressure control was also noted to be poor, around 150/90 mmHg. Auto adjusting continuous positive airway pressure was recommended but was not accepted by the patient as it required further out-of-pocket costs (over and above that already spent on the bilevel ventilator). Therefore, the ventilator was adjusted to EPAP at 7 cmH2O, IPAP at 14 cmH2O and minimum PS at 0 cmH2O to try and reduce the ventilatory effect and accommodate the patient’s wake pressure perception. The AHI quickly decreased to 3.1/h, with good ventilator adherence, and blood pressure normalized to around 105/82 mmHg.
One year following the treatment, the ventilator was switched without physician authorization to VAuto with EPAP at 5 cmH2O, IPAP at 11 cmH2O and PS at 2 cmH2O by a salesperson. The patient still had very good ventilator adherence with 7–8 hours nightly use. Subsequently, the patient presented to the emergency department due to palpitations and was found to have a sustained elevation in blood pressure, up to 159/113 mmHg. No underlying cause for the poorly controlled blood pressure was identifiable. A clinic visit revealed that the AHI and blood pressure had been uncontrolled since the ventilator settings were altered, a correlation supported by the data in Figure 1B. After resuming the parameters as EPAP at 7 cmH2O, IPAP at 14 cmH2O and PS at 0 cmH2O, at which point the bilevel ventilator was effectively functioning in a continuous positive airway pressure mode, his blood pressure was well-controlled at 106/64 mmHg, and the residual AHI was 1.1/h of use within a week. These positive outcomes were sustained throughout a one-month follow-up.
Discussion
OSA is a causative factor for secondary hypertension.1 While PAP serves as the first-line treatment for OSA, its effect on blood pressure is characterized by considerable interindividual variability.2–4 This case illustrates that ventilator settings can significantly impact blood pressure despite good adherence, especially if endotype information is ignored.
The residual AHI on PAP was accompanied by a significant increase in central sleep apnea (CSA) events following VAuto therapy. The underlying pathophysiology of this PAP-emergent CSA is likely related to high loop gain (HLG),5,6 but in this case amplified by bilevel ventilation. The band-like oxygen desaturation is considered typical for periodic breathing/HLG, while the individual respiratory events during such periods may still have the morphology of obstructive apnea/hypopnea. Loop gain is an engineering concept used to describe the stability of a negative feedback control system, whose essence during sleep is the physiological sensitivity to changes in CO2.7 As the PS required to induce instability was quite small, the patient probably had some elevation in loop gain already (oximetry “banding”), which was then amplified. This may have increased carotid body output and caused elevated blood pressure.
OSA patients with hypertension possess a less stable respiratory control system and heightened sensitivity to CO2 fluctuations, which predisposes them to CSA.8 PS from a bilevel mode can lead to a marked increase in the patient’s minute ventilation and fluctuations of CO2. CSA occurs when the level of partial pressure of CO2 in arterial blood drops below the “apneic threshold”, thus counteracting therapeutic benefits on obstructive pathology.9 Consistent with this mechanism, we recorded that during VAuto therapy, the central AHI reached a maximum of 27.84/h, which also corresponded to the period with uncontrolled blood pressure. Furthermore, this observation aligns with the 2025 American Academy of Sleep Medicine clinical practice guideline for the treatment of central sleep apnea in adults. The recommendation states that bilevel without a backup rate should not be used for treating CSA, including PAP-emergent CSA, because it can worsen CSA and periodic breathing.10
Mechanisms for the elevated blood pressure in this patient remain speculative, but could be one or more of the following, possibly synergistically: 1) sleep fragmentation from CSA could result in night-time blood pressure surges and baroreflex resetting;11 2) long central apneas can be associated with substantial hypoxia and cause sympathetic activation through activating the carotid body (which is already likely sensitive, given CSA propensity and substantial pre-morbid nocturnal hypoxia);12 3) there is a particularly disruptive effect of patient-ventilator desynchrony, which can cause hemodynamic instability and amplified blood pressure surges.13 This case suggests that daytime spillover effects are possible.
This case report has several limitations that should be acknowledged. The evidence linking pressure manipulation to blood pressure fluctuations remains indirect, as we did not perform any simultaneous blood pressure monitoring and pressure titration during sleep examination. Clarifying this association would require synchronized evaluation at multiple time points. Additionally, as a single case report with only one sample, the generalizability of our findings is inherently limited, and the observations require confirmation in larger cohorts or prospective studies before any clinical recommendations can be derived. Last, transcutaneous CO2 or end-tidal CO2 monitoring was not performed. Therefore, the proposed mechanism of CO2-mediated ventilatory instability relies on indirect evidence of the band‑like oxygen desaturation pattern.
Conclusion
Several critical lessons emerge from this case: 1) pressure manipulation should be performed exclusively under medical supervision, and not by the patient or a salesperson; 2) in susceptible patients, even minimal PS during bilevel therapy can trigger PAP-emergent CSA, destabilizing respiratory control and amplifying HLG, which may further worsen hypertension; 3) a high residual apnea can be addressed through a logical clinical mechanistic approach; 4) bilevel ventilation is not appropriate for the typical OSA patient.
Abbreviation
AHI, apnea-hypopnea index; CSA, central sleep apnea; EPAP, expiratory positive airway pressure; HLG, high loop gain; IPAP, inspiratory positive airway pressure; OSA, obstructive sleep apnea; PAP, positive airway pressure; PS, pressure support; SpO2, oxygen saturation.
Data Sharing Statement
All data supporting the findings of this case report are included within the article. Due to concerns regarding patient privacy and confidentiality, more detailed raw clinical data are not publicly available to protect the patient’s identity.
Ethics Approval and Informed Consent Statements
This study was performed in line with the principles of the Declaration of Helsinki. Publication of this case report was approved by the Biomedical Ethics Review Committee of West China Hospital, Sichuan University (Approval No. 2024-233).
Written informed consent was obtained from the patient prior to the commencement of this study for the publication of this case report and any accompanying images.
This case report was prepared in accordance with the CARE guidelines. The authors confirm that the manuscript adheres to the CARE reporting standards to ensure comprehensive, transparent, and accurate reporting of this case.
Author Contributions
Ms. Si-Rui Tian: Writing – original draft; Writing – review and editing; Visualization.
Dr. Robert Joseph Thomas: Conceptualization; Project administration; Supervision; Writing – review and editing.
Dr. Yue-Nan Ni: Conceptualization; Funding acquisition; Resources; Supervision; Writing – review and editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (82300118).
Disclosure
Dr. Robert Thomas reports the following conflicts of interest: financial relationships with MyCardio, LLC and Sleepcare Asia; personal fees from Guidepoint Global and GLG Councils, all outside the submitted work. Dr. Thomas is co-inventor and patent holder of the ECG-derived sleep spectrogram (cardiopulmonary coupling), which is licensed by Beth Israel Deaconess Medical Center to MyCardio, LLC, with royalties paid. He holds two patents licensed to Sleepcare Asia: (1) respiratory self-similarity for detection of high loop gain apnea, and (2) Enhanced Expiratory Rebreathing Space (EERS) for treatment of high loop gain sleep apnea. He is also co-inventor and patent holder (unlicensed) of the Positive Airway Pressure Gas Modulator, which is being developed for treatment of central/complex sleep apnea, and co-inventor of licensed auto-CPAP software to DeVilbiss-Drive. He consults for Guidepoint Global and GLG Councils.
All authors declare there are no other conflicting interests for this study.
References
1. Jones DW, Ferdinand KC, Taler SJ, et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM guideline for the prevention, detection, evaluation and management of high blood pressure in adults: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2025;152(11):e114–5. doi:10.1161/CIR.0000000000001356
2. Barbé F, Durán-Cantolla J, Sánchez-de-la-torre M, et al. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;307(20):2161–2168. doi:10.1001/jama.2012.4366
3. Muxfeldt ES, Margallo V, Costa LM, et al. Effects of continuous positive airway pressure treatment on clinic and ambulatory blood pressures in patients with obstructive sleep apnea and resistant hypertension: a randomized controlled trial. Hypertension. 2015;65(4):736–742. doi:10.1161/HYPERTENSIONAHA.114.04852
4. Kasiakogias A, Tsioufis C, Thomopoulos C, et al. Effects of continuous positive airway pressure on blood pressure in hypertensive patients with obstructive sleep apnea: a 3-year follow-up. J Hypertens. 2013;31(2):352–360. doi:10.1097/HJH.0b013e32835bdcda
5. Stanchina M, Robinson K, Corrao W, et al. Clinical use of loop gain measures to determine continuous positive airway pressure efficacy in patients with complex sleep apnea. a pilot study. Ann Am Thorac Soc. 2015;12(9):1351–1357. doi:10.1513/AnnalsATS.201410-469BC
6. Roberts EG, Raphelson JR, Orr JE, LaBuzetta JN, Malhotra A. The pathogenesis of central and complex sleep apnea. Curr Neurol Neurosci Rep. 2022;22(7):405–412. doi:10.1007/s11910-022-01199-2
7. Wellman A, Jordan AS, Malhotra A, et al. Ventilatory control and airway anatomy in obstructive sleep apnea. Am J Respir Crit Care Med. 2004;170(11):1225–1232. doi:10.1164/rccm.200404-510OC
8. Wang X, Luo J, Huang R, Xiao Y. The elevated central chemosensitivity in obstructive sleep apnea patients with hypertension. Nat Sci Sleep. 2022;14:855–865. doi:10.2147/NSS.S362319
9. Javaheri S, Barbe F, Campos-Rodriguez F, et al. Sleep apnea: types, mechanisms, and clinical cardiovascular consequences. J Am Coll Cardiol. 2017;69(7):841–858. doi:10.1016/j.jacc.2016.11.069
10. Badr MS, Khayat RN, Allam JS, et al. Treatment of central sleep apnea in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2025;21(12):2181–2191. doi:10.5664/jcsm.11858
11. Seravalle G, Mancia G, Grassi G. Sympathetic nervous system, sleep, and hypertension. Curr Hypertens Rep. 2018;20(9):74. doi:10.1007/s11906-018-0874-y
12. Nanduri J, Peng YJ, Yuan G, Kumar GK, Prabhakar NR. Hypoxia-inducible factors and hypertension: lessons from sleep apnea syndrome. J Mol Med. 2015;93(5):473–480. doi:10.1007/s00109-015-1274-2
13. Gunn S, Naik S, Bianchi MT, Thomas RJ. Estimation of adaptive ventilation success and failure using polysomnogram and outpatient therapy biomarkers. Sleep. 2018;41(9). doi:10.1093/sleep/zsy033
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Elevated Central Chemosensitivity in Obstructive Sleep Apnea Patients with Hypertension
Wang X, Luo J, Huang R, Xiao Y
Nature and Science of Sleep 2022, 14:855-865
Published Date: 3 May 2022
Time Under 90% Oxygen Saturation and Systemic Hypertension in Patients with Obstructive Sleep Apnea Syndrome
Wang L, Wei DH, Zhang J, Cao J
Nature and Science of Sleep 2022, 14:2123-2132
Published Date: 30 November 2022
Association Between Sleep Efficiency and Hypertension in Chinese Obstructive Sleep Apnea Patients
Xia N, Wang H, Chen Y, Fan XJ, Nie XH
Nature and Science of Sleep 2023, 15:79-88
Published Date: 10 March 2023
A Case of Young Obese Heart Failure Patient Using Multidisciplinary Treatment Centered on the Fantastic Four Improved Cardio Ankle Vascular Index and Cardiac Function
Ikeda Y, Iwakawa M, Kiyokawa H, Nakagami T, Kanzaki S, Ogawa A, Tabata T, Takahashi M, Kinoshita T, Shimizu K
International Medical Case Reports Journal 2023, 16:545-549
Published Date: 14 September 2023
Chin Tuck Exercise and Obstructive Sleep Apnea: A Case Report

Alsaeed S
Nature and Science of Sleep 2025, 17:2343-2349
Published Date: 29 September 2025