Back to Journals » International Medical Case Reports Journal » Volume 16
A Case of Young Obese Heart Failure Patient Using Multidisciplinary Treatment Centered on the Fantastic Four Improved Cardio Ankle Vascular Index and Cardiac Function
Authors Ikeda Y ![]() , Iwakawa M, Kiyokawa H, Nakagami T, Kanzaki S, Ogawa A
, Iwakawa M, Kiyokawa H, Nakagami T, Kanzaki S, Ogawa A ![]() , Tabata T, Takahashi M
, Tabata T, Takahashi M ![]() , Kinoshita T
, Kinoshita T ![]() , Shimizu K
, Shimizu K ![]()
Received 3 July 2023
Accepted for publication 7 September 2023
Published 14 September 2023 Volume 2023:16 Pages 545—549
DOI https://doi.org/10.2147/IMCRJ.S424567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuki Ikeda,1 Masahiro Iwakawa,1 Hajime Kiyokawa,1 Takahiro Nakagami,1 Shinya Kanzaki,2 Akihiro Ogawa,2 Tsuyoshi Tabata,3 Mao Takahashi,1 Toshio Kinoshita,1,3 Kazuhiro Shimizu1
1Department of Internal Medicine, Toho University Sakura Medical Center, Chiba, Japan; 2Department of Rehabilitation, Toho University Sakura Medical Center, Chiba, Japan; 3Department of Clinical Functional Physiology, Toho University Sakura Medical Center, Chiba, Japan
Correspondence: Kazuhiro Shimizu, Department of Internal Medicine, Toho University Sakura Medical Center, Chiba, Japan, Tel +81-43-462-8811, Fax +81-43-462-8820, Email [email protected]
Abstract: Obesity-induced heart failure (HF) in young people is a serious problem. The treatments for HF have developed in recent years. The following four basic HF drugs have been widely recognized as the “Fantastic Four”: beta-adrenergic blocking agents, mineralocorticoid receptor antagonists (MRA), sodium glucose transporter 2 inhibitors (SGLT2 inhibitors), and angiotensin receptor neprilysin inhibitors (ARNI). However, the interaction between the heart and blood vessels has not received much attention. The cardio-ankle vascular index (CAVI) is an arterial stiffness index that is unaffected by blood pressure at the time of measurement. A 34-year-old obese man was admitted with dyspnea and edema. His cardiac function was severely impaired, and CAVI was increased. After administration of multidisciplinary HF treatment centered on the “Fantastic Four”, his cardiac function and CAVI improved dramatically in a short time period. This case suggests the importance of improvement both cardiac and vascular function for the treatment of HF.
Keywords: obesity, hypertension, obstructive sleep apnea, arterial stiffness, cardio ankle vascular index
Introduction
Heart failure is a significant medical and economic problem worldwide. Recently, the optimal treatment for heart failure has made remarkable progress. In particular, four basic heart failure drugs, beta-blocking agents, mineralocorticoid receptor antagonists (MRA), sodium glucose transporter 2 inhibitors (SGLT2 inhibitors), and angiotensin receptor neprilysin inhibitors (ARNI), have been termed the “Fantastic Four” and their importance has been widely recognized.1
In the PARADIGM-HF study, ARNI was shown to be advantageous over enalapril, an angiotensin converting enzyme inhibitor, in preventing cardiovascular death or heart failure readmissions in patients with heart failure with reduced ejection fraction.2 ARNI was approved for use in August 2020 in Japan. Hypertension and sleep apnea associated with obesity are important causes of heart failure. The progression of arterial stiffness caused by these factors increases cardiac afterload.
The cardio-ankle vascular index (CAVI) was developed as an arterial stiffness index from the origin of the aorta to the ankle.3,4 The feature of CAVI is that it is independent from blood pressure at the time of measurement, because it is derived from the stiffness beta theory.5 We report here an interesting case of heart failure in an obese young adult that highlights the cardiovascular interaction.
Case Report
A 34-year-old obese man was brought to our hospital with complaints of dyspnea at rest and lower extremity edema. His weight was 136 kg and height was 1.71 metres with a body weight index (BMI) of 46.5 kg/m2. He had no particular medical history up to that time. His history of obesity began at childhood. High blood pressure was noted when he was in high school, but there was no history of hospital visits.
At the time of emergency transport to our hospital, his blood pressure was 204/132 mmHg and his heart rate was 130 bpm (Figure 1A). Saturation with room air was 88%. The lower extremities were markedly swollen (Figure 1B). He was admitted to hospital for treatment of heart failure. His chest X-ray showed cardiomegaly and bilateral mild congestion (Figure 1C). Trans-thoracic echocardiography showed left ventricular end-diastolic diameter of 50 mm, left ventricular ejection fraction of 27% (calculated by the modified Simpson’s method), and mild mitral regurgitation. Plasma B-type natriuretic peptide (BNP) was 729.1 pg/mL, NT-pro BNP was 4250 pg/mL, and estimated glomerular filtration rate was 40.0 mL/min/1.73 m2. His blood glucose level was 114 mg/dL, and hemoglobin A1c was 6.7%. There were no abnormalities of autoantibodies that could cause myocarditis. Random skin biopsies also showed no findings of sarcoidosis or amyloidosis. His laboratory results showed normal thyroid level, such as TSH: 2.87μIU/mL, fT3: 2.87 pg/mL, and fT4: 1.24 ng/dl. Renin, aldosterone and catecholamine levels were also within normal limits.
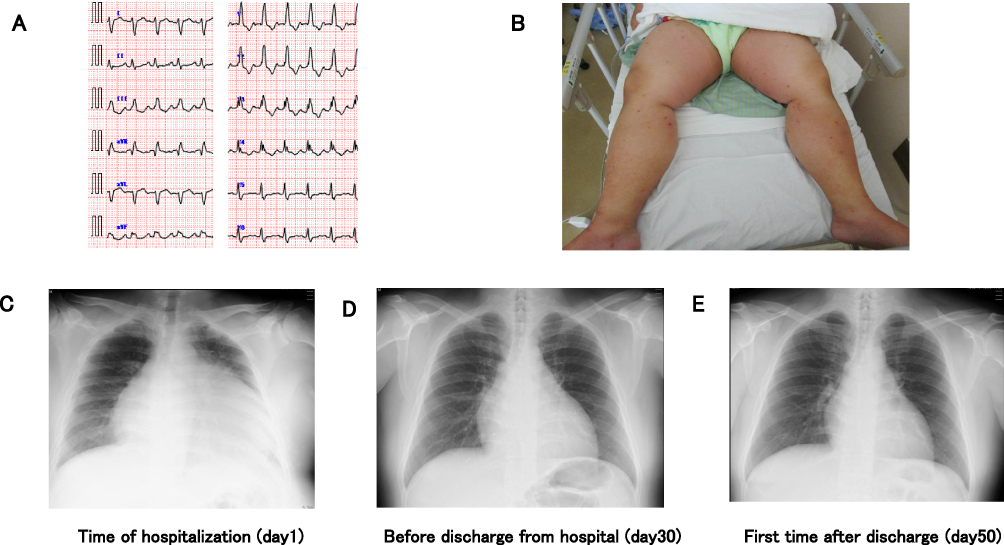 |
Figure 1 Imaging data on admission and clinical course based on chest X-ray. (A) electrocardiography, (B) patient’s edema, (C–E) clinical course based on chest X-ray. |
We administered tolvaptan in addition to furosemide due to the insufficient diuretic effect. Spironolactone as MRA and dapagliflozin as SGLT2 inhibitor were administered from the beginning of hospitalization.
As his systolic blood pressure was markedly elevated, we used valsartan and amlodipine. His weight gradually decreased and his dyspnea improved accordingly. On day 12, his body weight was 110 kg (Figure 2). We started cardiac rehabilitation and bisoprolol was added as a beta-blocker. About 2 weeks later, we replaced valsartan with sacubitril valsartan as ARNI for the treatment of heart failure. His sleep apnea was severe with an apnea hypopnea index as 38.2 times/hour, minimum SpO2 as 66.0%, maximum apnea time as 99.9 seconds in polysomnography. Continuous positive airway pressure (CPAP) therapy was introduced during his admission. On day 39, he was discharged. At that time, his weight had decreased to 103.2 kg. His ejection fraction (EF) had improved to 53%, E/e’ was 12.5, and BNP was 26.8 pg/mL. Furthermore, his CAVI had improved from 10.9 to 4.5 in a short period of time. The post-discharge clinical course is shown in Figure 2 and Table 1. At his first outpatient visit after discharge, his weight was slightly increased. In addition, his CAVI and blood pressure were also increased. We considered that these may be attributed to a change in his diet from his hospital diet. We increased the dose of the Ca antagonist. During his outpatient course, he tried to achieve body weight reduction, but it did not work very well. However, his compliance regarding medication and CPAP use was very good, and his heart failure symptoms were under control. His pulmonary congestion had completely improved (Figure 1D and E).
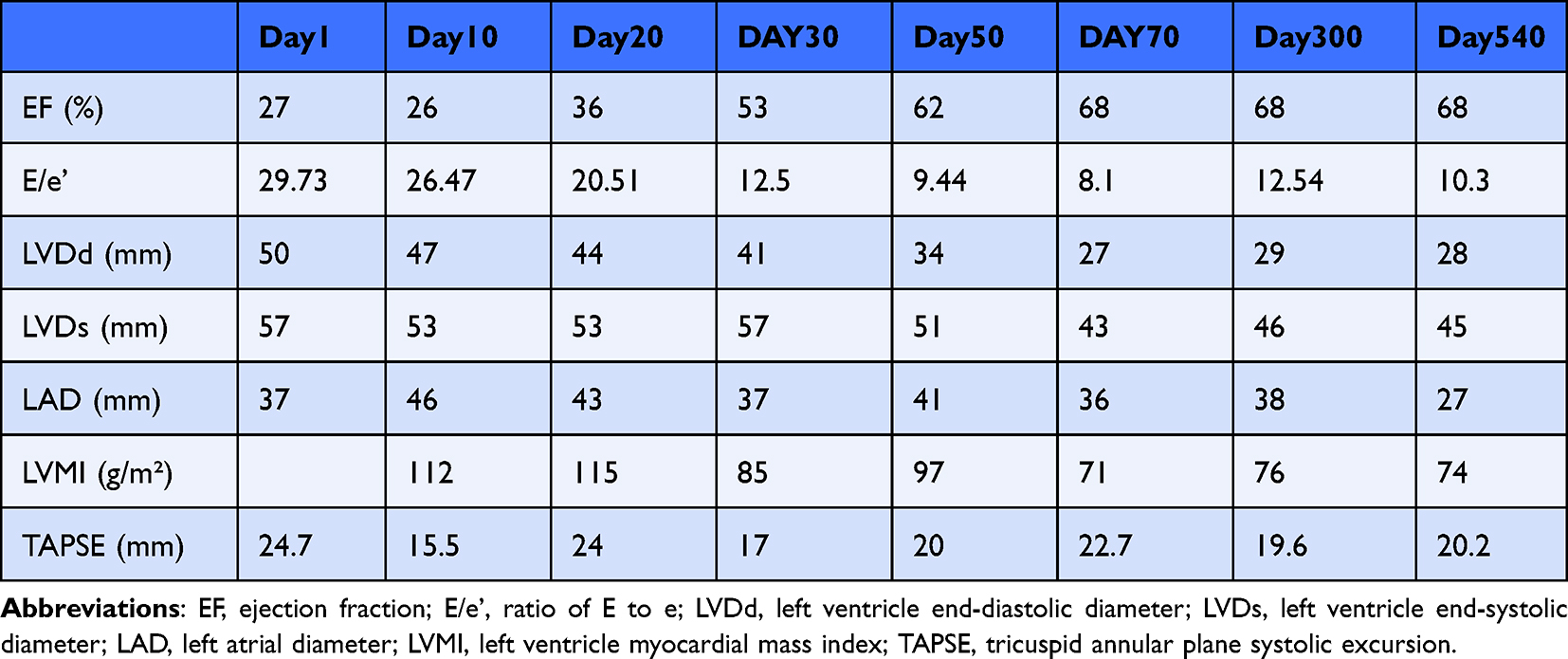 |
Table 1 Clinical Course of Echocardiography |
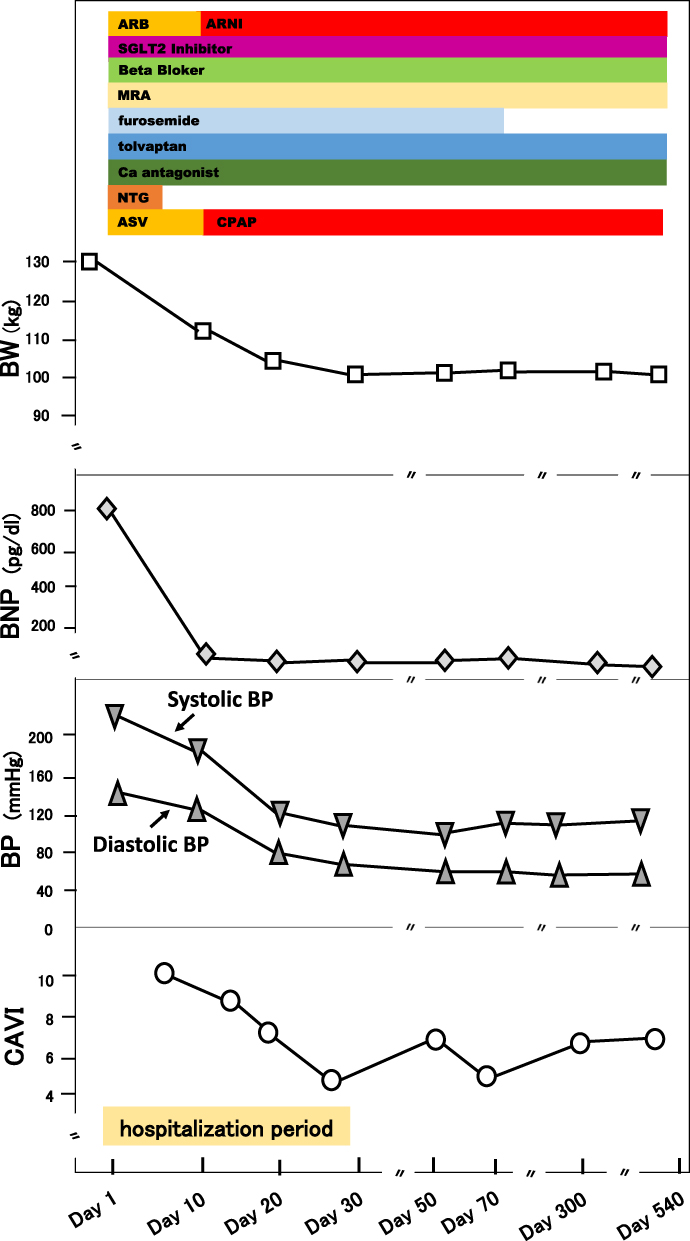 |
Figure 2 Clinical course of the patient. Effectiveness of multidisciplinary treatment centered on the “Fantastic Four”. Abbreviations: BW, body weight; BNP, brain natriuretic peptide; BP, blood pressure; CAVI, cardio-ankle vascular index; ARB, angiotensin II receptor blocker; ARNI, angiotensin receptor-neprilysin inhibition; MRA, mineralocorticoid receptor antagonist; SGLT2 inhibitor, sodium glucose transporter 2 inhibitor; NTG, nitroglycerin; ASV, adaptive servo ventilator; CPAP, continuous positive airway pressure. |
Discussion
We encountered a case of heart failure associated with obesity in a young man. In developed countries, the number of young obese patients is increasing due to high calorie diets and decreased exercise habits.6 Obesity is not only a risk for hypertension, diabetes, and dyslipidemia, but also for heart failure.7 The present patient was a young adult of 34 years old, but he had severe obesity with a BMI of 46.5 kg/m2 and untreated hypertension, and his cardiac function was severely impaired (Table 1). As shown in Figure 2, arterial stiffness as assessed by CAVI was markedly increased at 10.9. The feature of CAVI is that it is independent from blood pressure at the time of measurement. It is recognized that CAVI reflects not only organic stiffening of the arteries but also functional stiffening.4,8 This young obese heart failure patient was treated with the optimal heart failure treatment recently termed the “Fantastic Four”. His body weight decreased from 130 kg to 103 kg during hospitalization. As shown in Figure 2 and Table 1, this patient showed a concomitant improvement in cardiac function within a short period of time. His systolic and diastolic ventricular functions were improved quickly, and his left ventricular mass index was also improved. This phenomenon may be due to the improvement of cardiac preload associated with weight reduction, as well as the improvement of cardiac afterload by renin-angiotensin system inhibitors. Shimizu et al reported a short-term decrease in CAVI in an experiment with nitroglycerin administration for healthy young adults.8 Given his young age, the marked reduction in CAVI from 10.9 to 4.5 was attributed to the patient’s vascular function reaction to the powerful treatment regimen known as the Fantastic Four. Cardiovascular interaction has recently been demonstrated using CAVI, not only in the left heart system but also in the right heart system.9,10 Recently, much evidence has been reported on SGLT2 inhibitors and ARNI for heart failure.11–13 However, there has not yet been a report using CAVI that focuses on effects of the “Fantastic Four” on the cardiovascular interaction. In this case report, the effects of weight reduction and Fantastic Four on the effectiveness of heart failure treatment cannot be strictly separated. However, the possibility of CAVI as an indicator reflecting cardiac afterload was suggested in this case report.
In conclusion, we have encountered a young obese heart failure patient who showed marked improvement in heart function and vascular function after multidisciplinary treatment of heart failure centered on the “Fantastic Four”. The importance of heart failure treatment targeting the heart and blood vessels was suggested by this case.
Ethics and Consent
All procedures followed were in accordance with the ethical standards of the Responsible Committee on Human Experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent was obtained from the patient for being included in this report. The authors confirm that written consent for submission and publication of this case report including images and associated text has been obtained from the patient in line with CARE guidance. This case report was approved by Toho University (2022-149).
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bauersachs J. Heart failure drug treatment: the fantastic four. Eur Heart J. 2021;42(6):681–683. doi:10.1093/eurheartj/ehaa1012
2. McMurray JJ, Packer M, Desai AS, et al.; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004. doi:10.1056/NEJMoa1409077
3. Shirai K, Utino J, Otsuka K, Takata M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J Atheroscler Thromb. 2006;13(2):101–107. doi:10.5551/jat.13.101
4. Hayashi K, Yamamoto T, Takahara A, Shirai K. Clinical assessment of arterial stiffness with cardio-ankle vascular index: theory and applications. J Hypertens. 2015;33(9):1742–1757. doi:10.1097/HJH.0000000000000651
5. Shirai K, Song M, Suzuki J, et al. Contradictory effects of β1- and α1-aderenergic receptor blockers on cardio-ankle vascular stiffness index (CAVI) - CAVI independent of blood pressure. J Atheroscler Thromb. 2011;18(1):49–55. doi:10.5551/jat.3582
6. Ng M, Fleming T, Robinson M, et al. Global, regional and national prevalence of overweight and obesity in children and adults 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766–781. doi:10.1016/S0140-6736(14)60460-8
7. Tromp J, Paniagua SMA, Lau ES, et al. Age dependent associations of risk factors with heart failure: pooled population based cohort study. BMJ. 2021;372:n461. doi:10.1136/bmj.n461
8. Shimizu K, Yamamoto T, Takahashi M, Sato S, Noike H, Shirai K. Effect of nitroglycerin administration on cardio-ankle vascular index. Vasc Health Risk Manag. 2016;12:313–319. eCollection 2016. doi:10.2147/VHRM.S106542
9. Tabata T, Shimizu K, Morinaga Y, et al. The relationship between cardio-ankle vascular index and left atrial phasic function in hypertensive patients with preserved ejection fraction. Front Med Technol. 2021;3:724089. eCollection 2021. doi:10.3389/fmedt.2021.724089
10. Tabata T, Sato S, Ohno R, et al. Cardio-vascular interaction evaluated by speckle-tracking echocardiography and cardio-ankle vascular index in hypertensive patients. Int J Mol Sci. 2022;23(22):14469. doi:10.3390/ijms232214469
11. Packer M, Anker SD, Butler J, et al.; EMPEROR-Reduced Trial Committees and Investigators. Empagliflozin in patients with heart failure, reduced ejection fraction, and Volume overload: EMPEROR-reduced trial. J Am Coll Cardiol. 2021;77(11):1381–1392. doi:10.1016/j.jacc.2021.01.033
12. Solomon SD, de Boer RA, DeMets D, et al. Dapagliflozin in heart failure with preserved and mildly reduced ejection fraction: rationale and design of the DELIVER trial. Eur J Heart Fail. 2021;23(7):1217–1225. doi:10.1002/ejhf.2249
13. McMurray JJ, Packer M, Desai AS, et al.; PARADIGM-HF Committees and Investigators. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur J Heart Fail. 2013;15(9):1062–1073. doi:10.1093/eurjhf/hft052
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Time Under 90% Oxygen Saturation and Systemic Hypertension in Patients with Obstructive Sleep Apnea Syndrome
Wang L, Wei DH, Zhang J, Cao J
Nature and Science of Sleep 2022, 14:2123-2132
Published Date: 30 November 2022
Sacubitril/Valsartan Shows Improvement of the Cardio-Ankle Vascular Index in a Hypertensive Patient
Shimizu K, Tabata T, Iwakawa M, Sato S, Kinoshita T
International Medical Case Reports Journal 2023, 16:461-465
Published Date: 22 August 2023
Effect of Weight Loss on the Apnea Hypopnea Index is Related to Waist Circumference in Chinese Adults with Overweight and Obesity
Ren Y, Cui X, Zhu X, Guo H, Zhou Q, Yuan P, Cheng H, Wu W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:453-463
Published Date: 27 January 2024
Resistance Training in Cardiovascular Diseases: A Review on Its Effectiveness in Controlling Risk Factors
Nazir A, Heryaman H, Juli C, Ugusman A, Martha JW, Moeliono MA, Atik N
Integrated Blood Pressure Control 2024, 17:21-37
Published Date: 18 March 2024
Metabolic Syndrome and Tendon Disease: A Comprehensive Review
Lai C, Li R, Tang W, Liu J, Duan XD, Bao D, Liu H, Fu S
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1597-1609
Published Date: 9 April 2024