Back to Journals » Nature and Science of Sleep » Volume 15
Association Between Sleep Efficiency and Hypertension in Chinese Obstructive Sleep Apnea Patients
Authors Xia N, Wang H, Chen Y, Fan XJ, Nie XH ![]()
Received 10 November 2022
Accepted for publication 26 February 2023
Published 10 March 2023 Volume 2023:15 Pages 79—88
DOI https://doi.org/10.2147/NSS.S396893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Ning Xia,1 Hao Wang,2 Yu Chen,1 Xiao-Jun Fan,1 Xiu-Hong Nie1
1Department of Respiratory Diseases, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Xiu-Hong Nie, Department of Respiratory Diseases, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China, Tel +86-18611876008, Email [email protected]
Objective: We aimed to explore the relationship of sleep efficiency (SE) with the prevalence of hypertension in Chinese obstructive sleep apnea (OSA) patients based on polysomnography (PSG) records.
Methods: We studied 2360 patients with OSA and 764 primary snorers who underwent PSG in our hospital. SE was divided into three grades, including ≥ 85%, 80%~84.9%, and < 80%. Hypertension was defined based either on direct blood pressure measurements, under anti-hypertensive treatments or on physician diagnosis. Multivariate logistic regression models were conducted to investigate the association between SE and hypertension.
Results: After adjusting for potential confounding factors, OSA patients with < 80% SE and those with 80% to 84.9% SE were significantly associated with the prevalence of hypertension (OR = 1.248, 95% CI 1.018~1.531, P=0.033; OR = 1.380, 95% CI 1.040~1.832, P=0.026). Compared to primary snorers, OSA combined with < 85% SE increased the odds of hypertension. In stratified analysis by SE, risk of hypertension only in those with < 80% SE was significantly different between OSA and primary snorers. Furthermore, this relationship between reduced SE and hypertension was evident especially in female, younger ages, obese, moderate and severe OSA patients. No significant relationship between reduced SE and hypertension was found in primary snores group.
Conclusion: We found that poor SE was correlated with the prevalence of hypertension in Chinese OSA patients, but not in those with primary snoring. Moreover, this relationship was evident especially in female, younger ages, obese, moderate and severe OSA patients.
Keywords: sleep efficiency, hypertension, obstructive sleep apnea, polysomnography
Plain Language Summary
Former studies found that both OSA and reduced SE were associated with hypertension. However, the relationship between low SE and hypertension in Chinese OSA patients has not been determined. Our results first time demonstrated that poor SE was correlated with the prevalence of hypertension in Chinese OSA patients. This study provided evidences indicating that in addition to AHI and nocturnal hypoxemia, reduced SE may be an important factor of hypertension risk in patients with OSA.
Introduction
Obstructive sleep apnea (OSA) is a common sleep disorder characterized by complete or partial upper airflow cessation during sleep, which affects approximately 17% of men and 9% of women aged 50 to 70 years.1 Previous studies found that approximately 30~50% of OSA patients reported hypertension and OSA was an important cause of hypertension.2–4 Hypertension increased the risk of cardiovascular disease and cardiovascular mortality observed in patients with OSA.5
There are some evidences indicating a close relationship between sleep quality and hypertension. Previous studies have found that poor sleep quality was associated with higher risk of hypertension.6–8 However, the majority of these studies assessed sleep quality only based on subjective measurements,6–8 which are more variable than objective measurements. Sleep efficiency (SE), which is an objective indicator, has been used to evaluate sleep quality. Former studies have already confirmed that poor SE was associated with diabetes, metabolic syndrome, and hypertension.9–12
Because both OSA and SE are separately associated with hypertension, the co-occurrence of poor SE in OSA patients may further increase the risk of hypertension in this population. However, up to now, the relationship between low SE and hypertension in OSA patients has not been determined. The subjects of previous studies only came from European community.12–15 To our knowledge, there is no evidence on the association between SE and hypertension in Chinese OSA patients based on PSG records. Therefore, in this study, we aimed to explore the relationship between SE and the prevalence of hypertension in a large cohort of Chinese OSA patients.
Methods
Subjects
This cross-sectional study included patients from Sleep Medical Center, XuanWu hospital. The study procedure was approved by the ethics committee of XuanWu hospital of Capital Medical University (protocol No. Clinical research 2021–185). As the study was performed retrospectively for reviewing participant PSG records, and involved no manipulation by drug or device, the institutional review board specifically approved the informed consent waiver because of the anonymous and purely observational nature of this study. Patient data confidentiality was covered by compliance with the Declaration of Helsinki.
All participants were Chinese adults (age >18 years) in our study. A comprehensive questionnaire was used for all research subjects to collect information, including general health, tobacco use, alcohol drinking, sleep complaints and medical history. The diagnosis of diabetes mellitus (DM)16 and coronary heart disease (CHD)17 were determined by specialists according to clinical manifestations and auxiliary examinations.
In this study, patients with an apnea hypopnea index (AHI) ≥5 events/hour were classified as OSA group, whereas individuals with an AHI <5 events/hour were regarded as primary snoring group. Patients with OSA were further stratified according to disease severity as follows: mild OSA (AHI 5~15 events/hour), moderate OSA (AHI 15~30 events/hour), and severe OSA (AHI >30 events/hour). The exclusion criteria are as follows: (1) subjects were diagnosed or treated OSA before; (2) individuals were taking sleep-disrupting medical condition; (3) subjects were diagnosed other comorbid sleep disorders; (4) participants slept fewer than 3 hours during PSG or missed BP data.
Blood Pressure Measures
Blood pressure was measured manually in triplicate with a 5-minute interval in the evening before PSG and in the morning after PSG. Recorded BP was the average of the second and third measurements. Hypertension was defined as (1) diastolic BP (DBP)≥90 mmHg and/or systolic BP (SBP)≥140 mmHg at either evening or morning measurement; (2) participants have used anti-hypertensive medication before; (3) subjects were diagnosed hypertension as a clinical history. We used the average of evening and morning BP for analysis.
Polysomnography
All participants underwent overnight PSG monitoring in the sleep medical center of XuanWu Hospital (Australia Compumedics Grael). Sleep data were automatically collected on the computer to analysis (ProFusion PSG Software). SE was defined as the percentage of the time spent asleep to total time in bed and categorized into three grades (≥85%, 80%~84.9%, and <80%). The highest SE percentage group in OSA and primary snoring group was considered as a reference. Wake after sleep onset (WASO) was defined as the total arousal time from the beginning of sleep to the time of waking. Sleep latency (SL) was calculated from lying in bed to sleeping. Total sleep duration was defined as the total sleep time. Total arousal events were calculated as the total number of arousals to the total sleep time. The percentage of rapid eye movement percentage (REM%) was described as percentage of total sleep time. Slow-wave sleep (SWS) was expressed as the third stage of non-REM sleep. AHI was defined as all apnea (more than 90% reduction of airflow for at least 10s) and hypopnea (≥50% reduction of airflow for at least 10s accompanied with more than 3% decrease in arterial oxygen saturation (SaO2)) occurrences per hour of sleep.
Statistical Analysis
Data were presented as mean ± standard deviation (SD) for continuous variables, and categorical variables were presented as percentages. Comparisons between hypertensive and non-hypertensive patients were conducted using ANOVA, independent-sample t-tests or Mann–Whitney U-tests for normally distributed and skewed continuous variables, respectively. Chi-square tests were performed for categorical variables.
Logistic regression models were used to examine the associations of SE and hypertension in all participants, OSA and primary snoring group, respectively. Next, considering the joint effect of OSA and SE, we assessed the association of SE and OSA with hypertension by using primary snoring as a reference group. Moreover, we examined the SE×OSA interaction by comparing OSA to primary snoring in the same SE grade. Model 1 was adjusted for age, sex, BMI (body mass index); Model 2 was adjusted for Model 1 and CHD, DM, tobacco use, and alcohol drinking; Model 3 was adjusted for Model 2, heart rate, oxygen desaturation index, time with sat <90%, daytime sleepiness, lowest oxygen saturation during sleep (Lowest SpO2) and AHI. The unadjusted and adjusted odds ratio (OR) and 95% CI from logistic regression models were used to present the relationship between SE and hypertension in OSA and primary snoring group.
In this study, we divided age into two groups (<60 years and ≥60 years) to assess the relationship between SE and hypertension in OSA patients. Besides, BMI (<30 vs ≥30), sex (male vs female) and AHI (≥15 vs <15) were divided into subgroups to examine the relationship between SE and hypertension in OSA group.
Data were analyzed using SPSS 26.0, and comparisons with P values <0.05 were considered statistically significant.
Results
Basic Characteristics
A total 3124 participants (2360 OSA and 764 primary snoring patients, 46.48±13.25 years) were included in our study. The baseline characteristics of participants are shown in Table 1. The proportion of hypertension in OSA group was significantly higher than primary snoring group (61.6% vs 32.3%). In OSA and primary snoring group, hypertension was more prevalent among subjects who were older, with higher BMI, with more CHD and DM. Furthermore, participants with hypertension had significantly elevated WASO, oxygen desaturation index and AHI compared to controls both in OSA and primary snoring group. On the other hand, SE, total sleep duration, and the lowest SpO2 were significantly lower in individuals with hypertension than in those without hypertension.
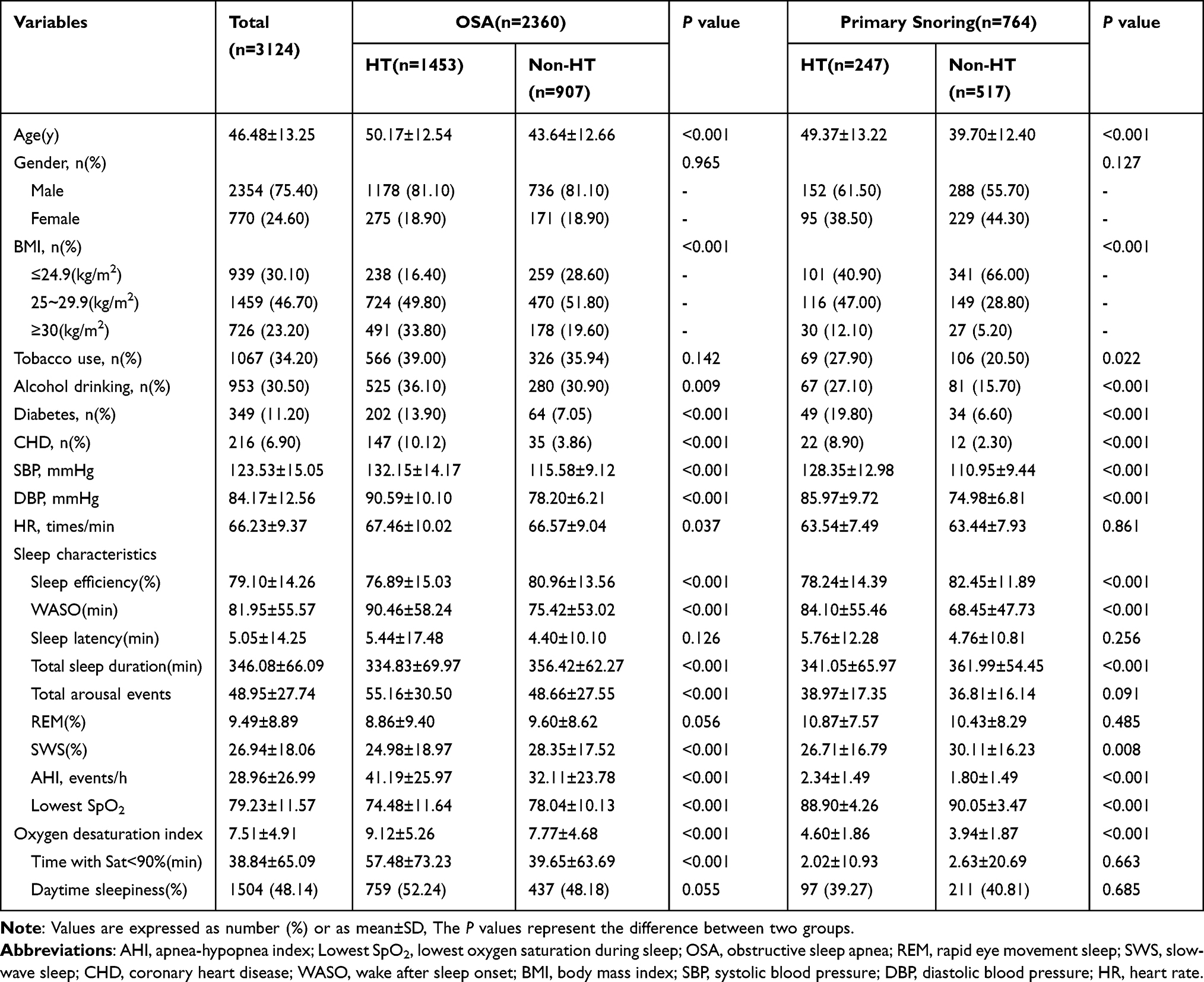 |
Table 1 Clinical Characteristics of 3124 Study Subjects (n = 3124) |
SE and Hypertension
Figure 1 illustrates the frequency of hypertension and BP levels in all patients, OSA and primary snoring group stratified by SE. Compared with the higher percentages of SE (≥85% and 80%~84.9%), those with the lowest percentages of SE (<80%) exhibited higher odds of hypertension and higher levels of SBP and DBP in all participants and OSA patients (Figure 1A-F). In primary snoring group, hypertension was more frequent and SBP was higher in those with <80% SE than those with 80% to 84.9% SE and those with ≥85% SE, not DBP (Figure 1G-I).
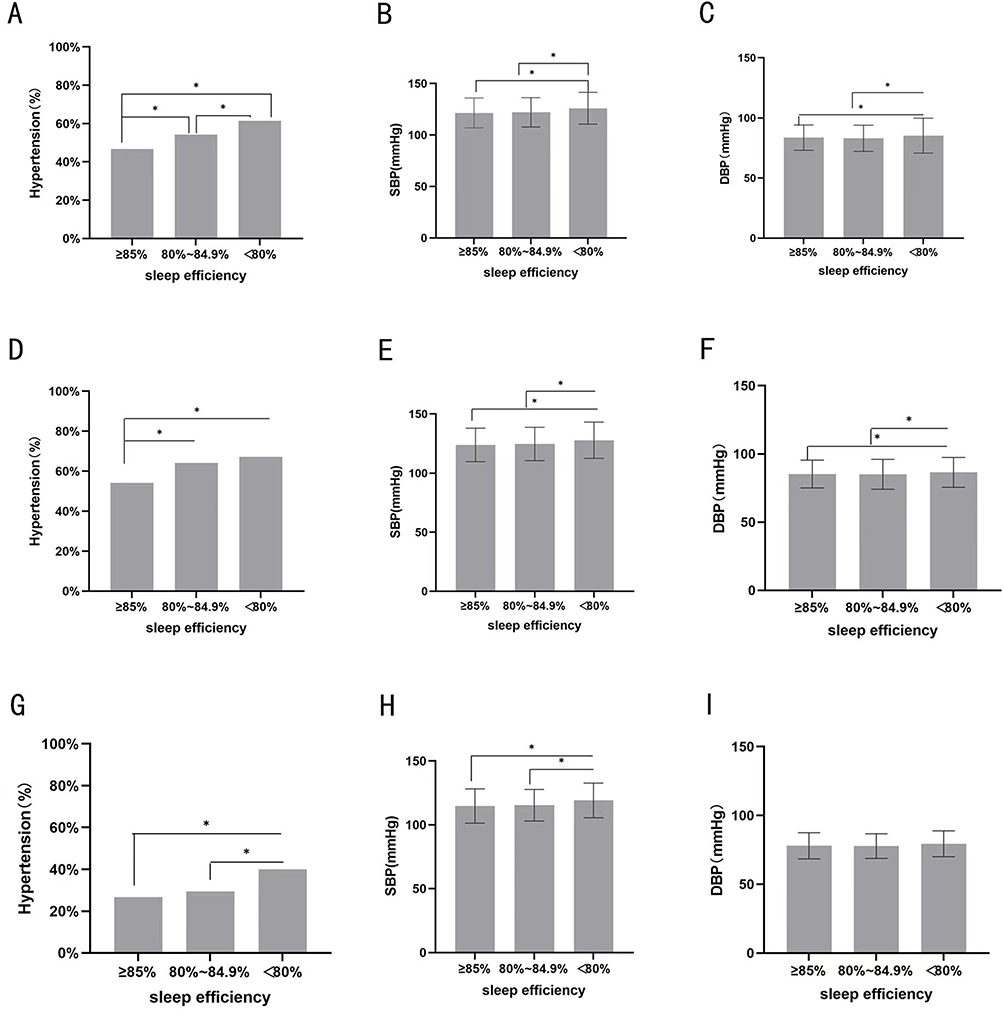 |
Figure 1 Frequency of hypertension and SBP and DBP levels across different grades of SE in all participants, OSA and primary snoring groups. (A) The proportion of hypertension in different SE categories in all participants. (B) SBP in different SE categories in all participants. (C) DBP in different SE categories in all participants. (D) The proportion of hypertension in different SE categories in OSA group. (E) SBP in different SE categories in OSA group. (F) DBP in different SE categories in OSA group. (G) The proportion of hypertension in different SE categories in primary snoring. (H) SBP in different SE categories in primary snoring. (I) DBP in different SE categories in primary snoring. Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure. Notes: Error bars indicate standard deviation. *P < 0.05. |
As shown in Table 2, SE presented a significant association with hypertension only in OSA group. In OSA group, patients with <80% SE and those with 80% to 84.9% SE had significantly higher likelihood of having hypertension than those with ≥85% SE, respectively (OR = 1.248, 95% CI 1.018~1.531, P=0.033; OR = 1.380, 95% CI 1.040~1.832, P=0.026). However, no significant relationship between SE and hypertension was found in the primary snoring group.
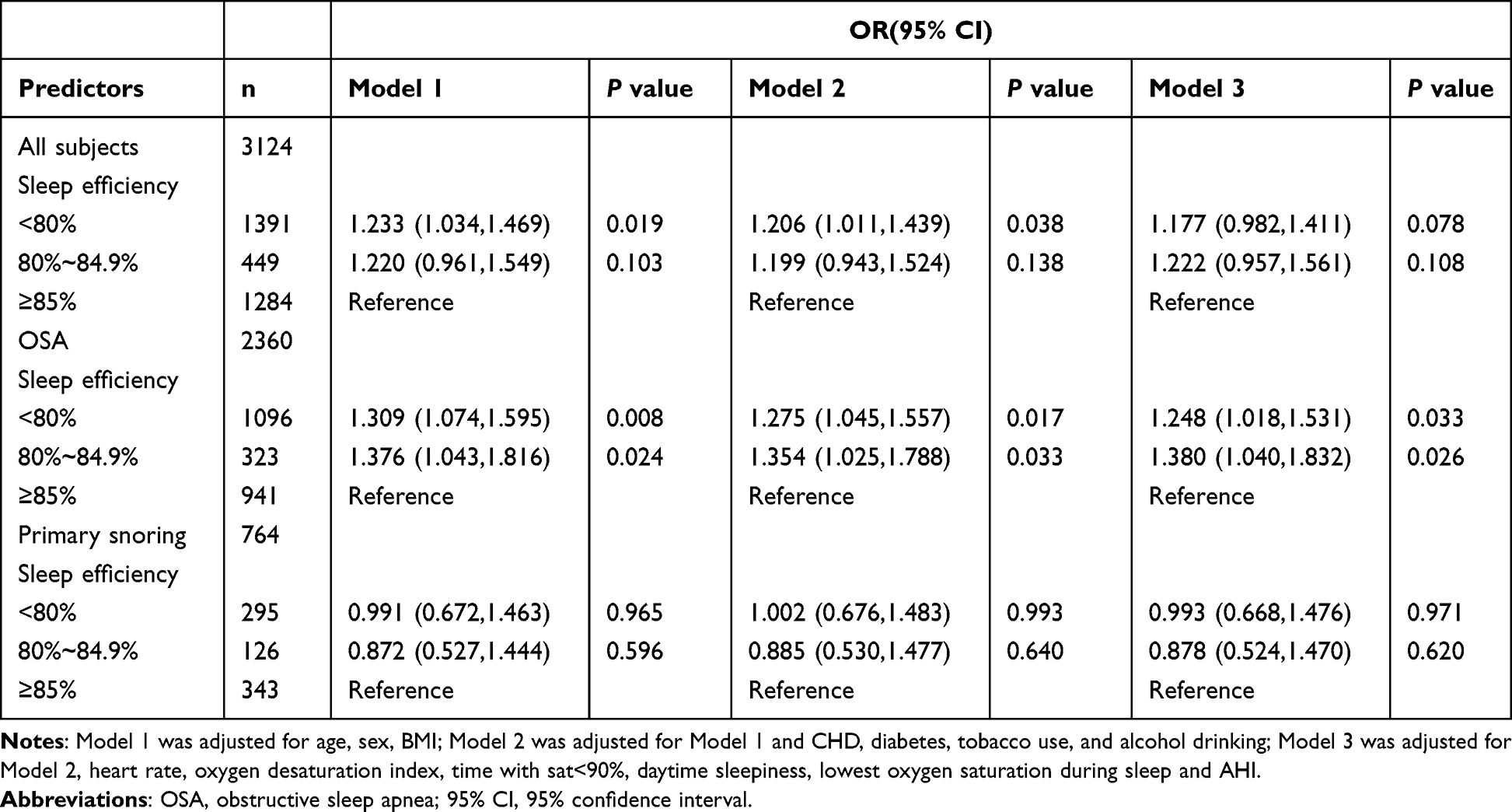 |
Table 2 ORs and 95% CIs for Sleep Efficiency Associated with Hypertension in All Subjects and Subgroup Analysis with or Without OSA |
In Table 3, we examined the joint effect of OSA and SE on hypertension. Compared to primary snoring, patients with OSA with <80% SE and those with 80% to 84.9% SE had significantly increased odds of hypertension (OR = 1.295, 95% CI 1.003~1.671, P=0.047; OR = 1.405, 95% CI 1.017~1.940, P=0.039). In contrast, OSA patients with ≥85% SE did not have significantly higher ratio of hypertension than primary snorers (OR = 1.016, 95% CI 0.783~1.318, P=0.905). We further conducted logistic regression analysis to examine the SE×OSA interaction by comparing OSA to primary snoring in the same SE grade. As compared to primary snoring within the same SE grade, odds of prevalent hypertension in those with OSA with <80% SE were significant (OR = 1.532, 95% CI 1.095~2.143, P=0.013), while odds were not significant in the other two grades (≥85% and 80%~84.9%) (Table 4). These results indicated that in addition to AHI and nocturnal hypoxemia, reduced SE may be an important factor of hypertension risk in patients with OSA.
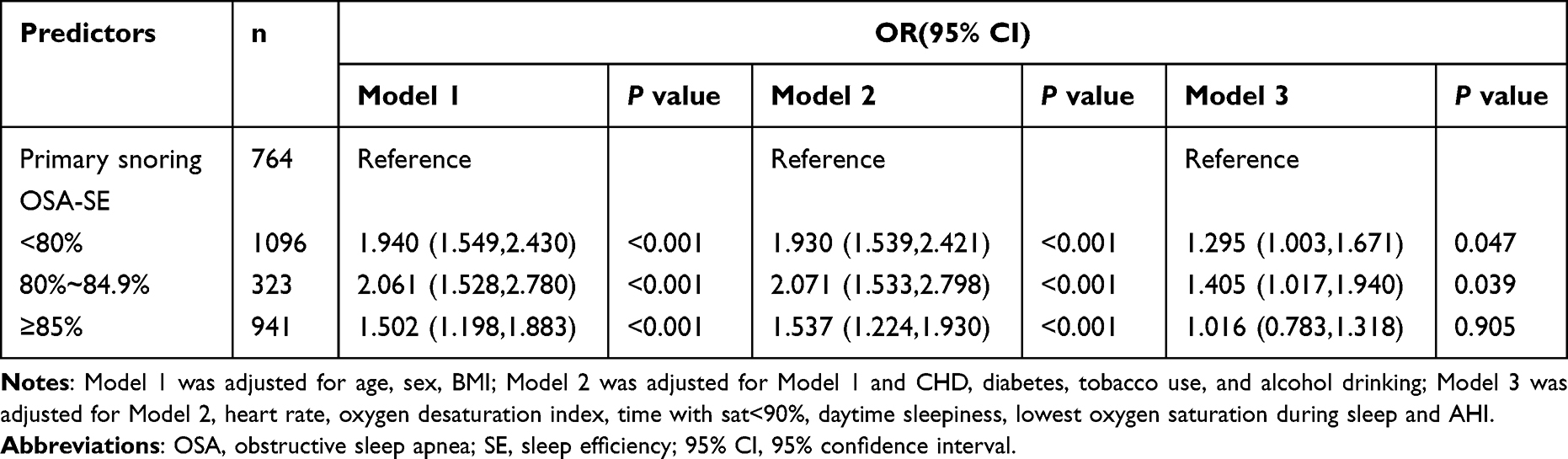 |
Table 3 Adjusted ORs and 95% CIs for the Joint Effect of OSA and Sleep Efficiency on Hypertension |
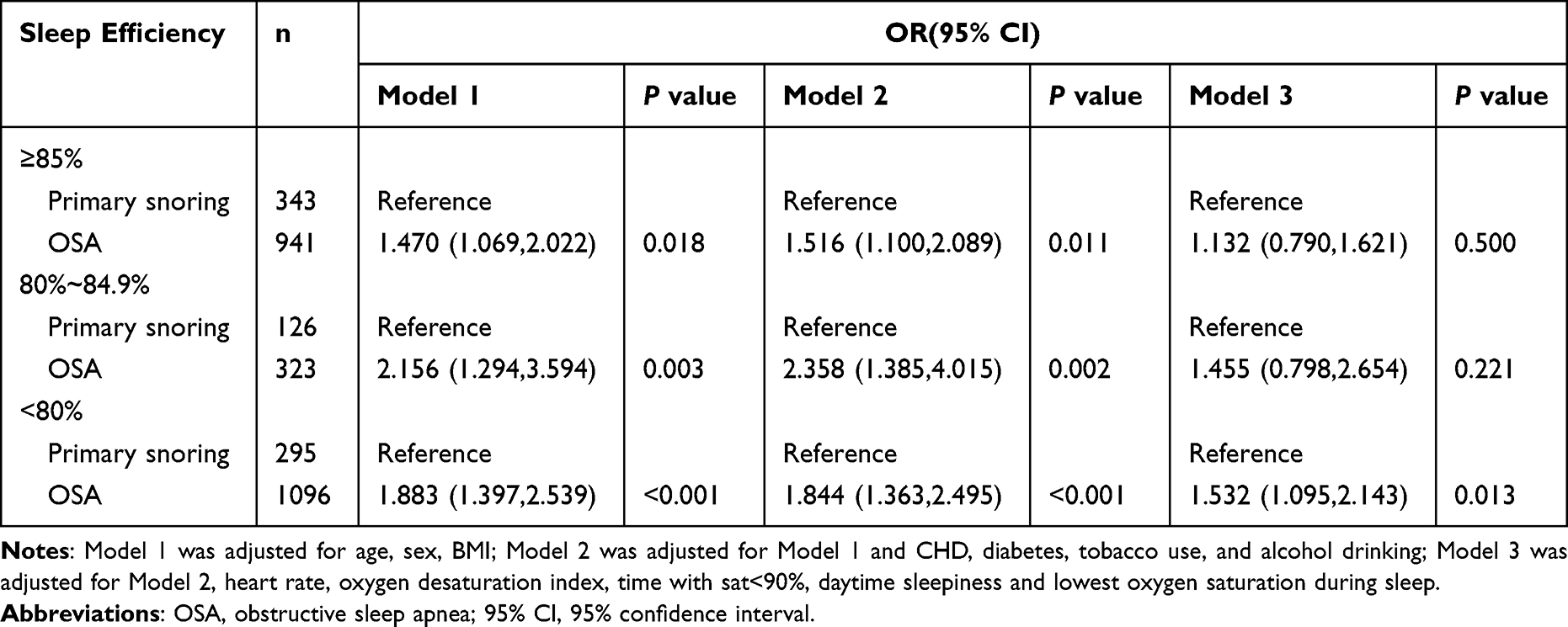 |
Table 4 Adjusted ORs and 95% CIs for the Association Between OSA and Hypertension Across Different Sleep Efficiency |
Subgroup Analysis
We investigated the association between SE and hypertension risk in subgroups analyses with OSA group stratified by age (≥60 years vs <60 years), sex (male vs female), BMI (≥30 kg/m2 vs <30 kg/m2) and AHI (≥15 events/h vs <15 events/h). The association between hypertension and SE was present in female, younger ages (<60 years old), obese, moderate and severe OSA patients (Table 5).
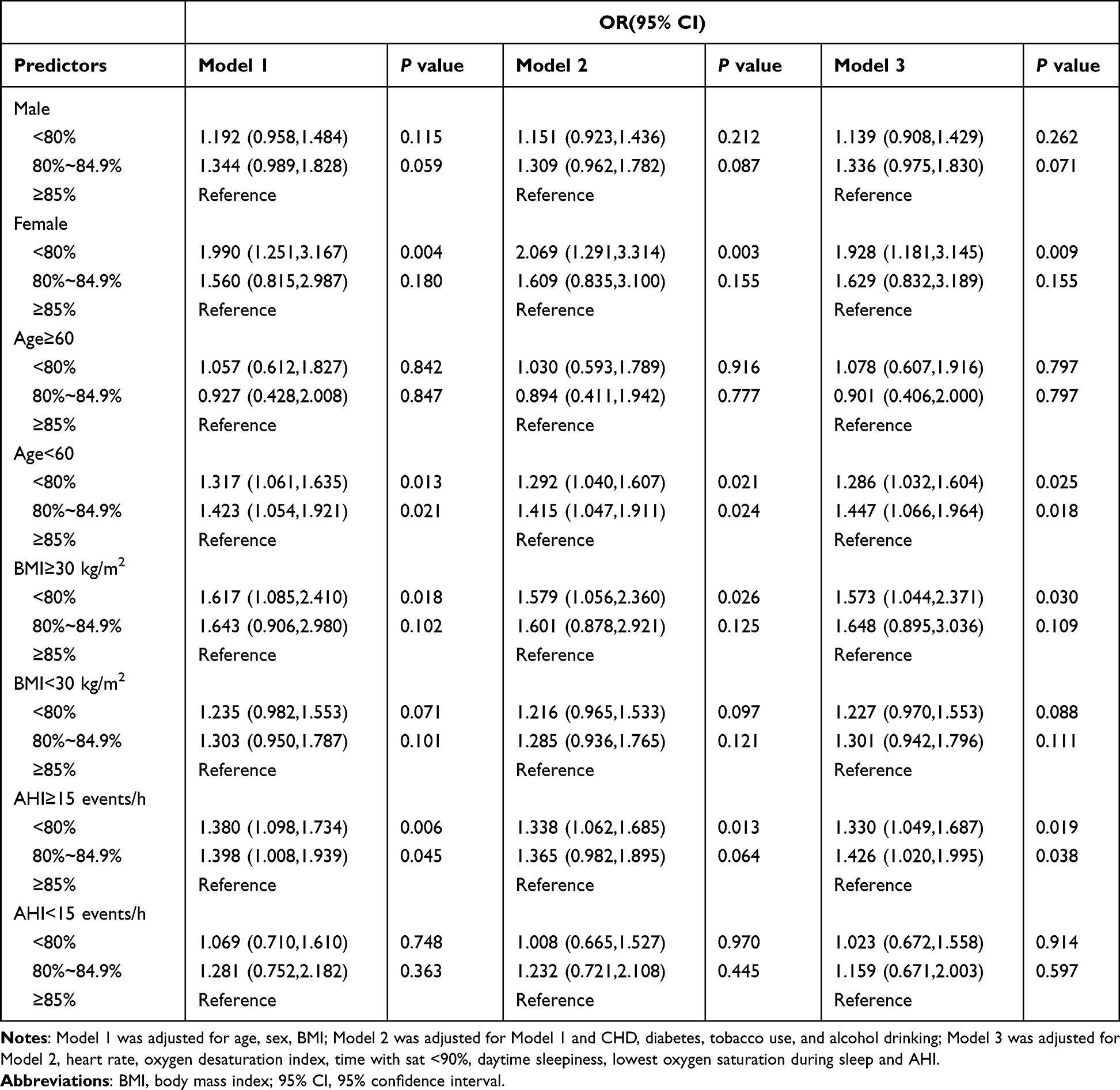 |
Table 5 ORs and 95% CIs for Sleep Efficiency Associated with Hypertension in Subgroup OSA Patients |
Discussion
We examined the association between SE and the prevalence of hypertension in a large population of OSA and primary snoring patients. Our results found that poor SE (<85%) measured by PSG was associated with hypertension risk only in OSA subjects. This relationship was evident especially in female, younger ages (<60 years old), obese, moderate and severe OSA patients.
SE is an objective indicator to evaluate sleep quality. Multiple cross-sectional and longitudinal studies have demonstrated a significant relationship between SE and hypertension.12–15,18–21 Four cross-sectional studies found that reduced SE, as measured by actigraphy or a contactless biomotion sleep sensor, was significantly related to an increased prevalence of hypertension12–14,20 and impaired flow-mediated dilation,21 which implicating poor sleep as a CVD risk factor. Furthermore, two longitudinal studies reported that lower SE was independently associated with higher risk of hypertension18 and BP nondipping19 after a mean follow-up of 7 and 7.4 years, respectively. Nevertheless, in the majority of these studies, participants almost came from community. The effect of decreased SE on hypertension in OSA patients has not been fully explored.
In a retrospective study of 151 OSA patients who underwent PSG, Friedman et al11 found that subjects with resistant hypertension were associated with a reduction in sleep efficiency of 7.9% and 10.2% compared to subjects with controlled hypertension and normotension, respectively. Another cross-sectional study13 found that individuals with reduced SE had a higher level of SBP/DBP and a higher prevalence of hypertension, including sleep disordered breathing (SDB) subjects. Furthermore, Ramos et al14 demonstrated that participants (included mild SDB patients) with hypertension had a decreased sleep efficiency compared with participants without hypertension. Our results were consistent with the prior studies that OSA patients with reduced SE measured by PSG were associated with a higher risk of hypertension. Moreover, when examining the joint effect of OSA and SE on hypertension, compared to primary snoring, patients with OSA with <80% SE and those with 80% to 84.9% SE had significantly increased odds of hypertension. Our study provided evidences indicating that in addition to AHI and nocturnal hypoxemia, reduced SE may be an important factor of hypertension risk in patients with OSA. However, on the other hand, Thomas et al22 found that SE was not associated with either nocturnal hypertension or nondipping SBP in subjects, which including likelihood of OSA patients. The reason why the results were different from our study may be that SE was determined by subjective methods, and OSA was determined using the STOP-Bang questionnaire. Besides, in our study, there was no significant relationship between SE and hypertension in the primary snoring group, which was different from former studies. Zhao et al13 found that reduced SE was significantly associated with the prevalence of hypertension in participants with AHI <5 events/h. Participants were different ethnic groups and almost middle-aged and older population may be the reason of inconsistent results.
The subgroup analysis showed that the association between hypertension and SE was observed in female, those <60 years old, obese, moderate and severe OSA patients. The results of two former studies were consistent with our results that younger OSA patients were associated with a higher risk of hypertension,23,24 reflecting the reduced cardiovascular risk for older OSA individuals. As for the association between sex and SE, Kocevska et al demonstrated that women (≥41 years) reported a marginally lower SE than men from a meta-analysis about sleep characteristics in 1.1 million people.25 Furthermore, hypertension was more prevalent in women with OSA,26 and the significant relationship between SE and higher BP was driven by women and not men.27 It is thus conceivable that, OSA women exhibited significant association between hypertension and SE in our study. Moreover, former studies18,28 found that poor SE and BMI ≥30 kg/m2 significantly increased the risk of hypertension. The relationship between OSA and BP is most closely associated with the degree of obesity.29 Therefore, in our population, the association between hypertension and SE was extremely significant in obese OSA patients.
The mechanisms accounting for the association between reduced SE and hypertension remain unknown. It is possible that poor SE with hypertension may be through stimulation of sympathetic nervous system, as measured by increased secretion of catecholamines.30 Moreover, reduced SE led to low sleep quality, which was demonstrated to damage endothelial function,21,31 increase baseline brachial artery diameter,27 aortic arterial stiffness32 and carotid intima-media thickness,33 resulting in hypertension and cardiovascular diseases.
There are several strengths in this study. This is the first study to investigate the interaction between reduced SE and hypertension using PSG records in Chinese OSA patients. Moreover, use of a large sample increases generalizability in our study. However, there are still some limitations in our study. First, our study is retrospective, cross-sectional study, and the association between SE and hypertension requires further study to prove. Second, we only measured sleep using one night of PSG, which may do not provide accurate information. Even though some studies found that actigraphy and PSG produced similar estimates of sleep duration and efficiency,34,35 wrist actigraphy had an advantage because it allowed for multiple sleep monitoring. Thirdly, we obtained only clinic BP measurements. The definition of hypertension was based on the BP measurement and participants medical history, which may produce the bias of the result. Finally, the participants were Chinese, and our findings may not be applicable in other ethnic groups.
Conclusion
In conclusion, our results show that poor SE is correlated with the prevalence of hypertension in Chinese OSA patients, but not in those with primary snoring. Further studies with longitudinal designs are needed to determine the temporal association between SE and hypertension in patients with OSA.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study procedure was approved by the ethics committee of XuanWu hospital of Capital Medical University (protocol No. Clinical research 2021-185). The institutional review board specifically approved the informed consent waiver because of the anonymous and purely observational nature of this study. Patient data confidentiality was covered by compliance with the Declaration of Helsinki.
Consent for Publication
All authors agreed to submit the manuscript for publication with all details, including images, tables and data.
Acknowledgments
The authors thank the patients who participated in this study. We appreciate Lianguo Zhang and Lili Zhang for technical help.
Funding
Supported by research grants from Capital Medical University Research Project (grant number: XWJL-2019035). The investigators are solely responsible for the design, conduct, data analysis and interpretation of this study, writing the manuscript, and the decision to submit the manuscript for publication, without any influence from the financial supporters.
Disclosure
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
References
1. Veasey SC, Rosen IM, Solomon CG. Obstructive sleep apnea in adults. N Engl J Med. 2019;380(15):1442–1449. doi:10.1056/NEJMcp1816152
2. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378–1384. doi:10.1056/NEJM200005113421901
3. Hou H, Zhao Y, Yu W, et al. Association of obstructive sleep apnea with hypertension: a systematic review and meta-analysis. J Glob Health. 2018;8(1):010405. doi:10.7189/jogh.08.010405
4. Oscullo G, Torres G, Campos-Rodriguez F, et al. Resistant/Refractory hypertension and sleep apnoea: current knowledge and future challenges. J Clin Med. 2019;8(11):Nov. doi:10.3390/jcm8111872
5. Xie C, Zhu R, Tian Y, Wang K. Association of obstructive sleep apnoea with the risk of vascular outcomes and all-cause mortality: a meta-analysis. BMJ Open. 2017;7(12):e013983. doi:10.1136/bmjopen-2016-013983
6. Ma GY, Cai L, Fan LM, et al. Association of socioeconomic factors and prevalence of hypertension with sleep disorder among the elderly in rural southwest China. Sleep Med. 2020;71:106–110. doi:10.1016/j.sleep.2020.03.006
7. Yuan Y, Heizhati M, Wang L, et al. Poor sleep quality is associated with new-onset hypertension in a diverse young and middle-aged population. Sleep Med. 2021;88:189–196. doi:10.1016/j.sleep.2021.10.021
8. Rahim A, McIsaac MA, Aronson KJ, Smith PM, Tranmer JE. The Associations of Shift Work, Sleep Quality, and Incidence of Hypertension in Ontario Adults: a population-based study. Can J Cardiol. 2021;37(3):513–518. doi:10.1016/j.cjca.2020.09.003
9. Yan B, Zhao B, Fan Y, et al. The association between sleep efficiency and diabetes mellitus in community-dwelling individuals with or without sleep-disordered breathing. J Diabetes. 2020;12(3):215–223. doi:10.1111/1753-0407.12987
10. Erdim I, Akcay T, Yilmazer R, Erdur O, Kayhan FT. Is metabolic syndrome associated with obstructive sleep apnea in obese adolescents? J Clin Sleep Med. 2015;11(12):1371–1376. doi:10.5664/jcsm.5266
11. Friedman O, Bradley TD, Ruttanaumpawan P, Logan AG. Independent association of drug-resistant hypertension to reduced sleep duration and efficiency. Am J Hypertens. 2010;23(2):174–179. doi:10.1038/ajh.2009.220
12. Doyle CY, Ruiz JM, Taylor DJ, et al. Associations between objective sleep and ambulatory blood pressure in a community sample. Psychosom Med. 2019;81(6):545–556. doi:10.1097/PSY.0000000000000711
13. Zhao J, Wang W, Wei S, Yang L, Wu Y, Yan B. Fragmented sleep and the prevalence of hypertension in middle-aged and older individuals. Nat Sci Sleep. 2021;13:2273–2280. doi:10.2147/NSS.S337932
14. Ramos AR, Weng J, Wallace DM, et al. Sleep patterns and hypertension using actigraphy in the Hispanic community health study/study of Latinos. Chest. 2018;153(1):87–93. doi:10.1016/j.chest.2017.09.028
15. Didikoglu A, Maharani A, Tampubolon G, Canal MM, Payton A, Pendleton N. Longitudinal sleep efficiency in the elderly and its association with health. J Sleep Res. 2020;29(3):e12898. doi:10.1111/jsr.12898
16. American Diabetes A. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2021. Diabetes Care. 2021;44(Suppl Supplement_1):S15–S33. doi:10.2337/dc21-S002
17. Joseph J, Velasco A, Hage FG, Reyes E. Guidelines in review: comparison of ESC and ACC/AHA guidelines for the diagnosis and management of patients with stable coronary artery disease. J Nucl Cardiol. 2018;25(2):509–515. doi:10.1007/s12350-017-1055-0
18. Ma CC, Gu JK, Bhandari R, et al. Associations of objectively measured sleep characteristics and incident hypertension among police officers: the role of obesity. J Sleep Res. 2020;29(6):e12988. doi:10.1111/jsr.12988
19. Lyu B, Hagen EW, Ravelo LA, Peppard PE. Blood pressure dipping and sleep quality in the Wisconsin Sleep Cohort. J Hypertens. 2020;38(3):448–455. doi:10.1097/HJH.0000000000002283
20. Hirata T, Nakamura T, Kogure M, et al. Reduced sleep efficiency, measured using an objective device, was related to an increased prevalence of home hypertension in Japanese adults. Hypertens Res. 2020;43(1):23–29. doi:10.1038/s41440-019-0329-0
21. Hill LK, Wu JQ, Hinderliter AL, Blumenthal JA, Sherwood A. Actigraphy-derived sleep efficiency is associated with endothelial function in men and women with untreated hypertension. Am J Hypertens. 2021;34(2):207–211. doi:10.1093/ajh/hpaa167
22. Thomas SJ, Booth JN 3rd, Jaeger BC, et al. Association of sleep characteristics with nocturnal hypertension and nondipping blood pressure in the CARDIA Study. J Am Heart Assoc. 2020;9(7):e015062. doi:10.1161/JAHA.119.015062
23. Ren R, Covassin N, Zhang Y, et al. Interaction between slow wave sleep and obstructive sleep apnea in prevalent hypertension. Hypertension. 2020;75(2):516–523. doi:10.1161/HYPERTENSIONAHA.119.13720
24. Khamsai S, Mahawarakorn P, Limpawattana P, et al. Prevalence and factors correlated with hypertension secondary from obstructive sleep apnea. Multidiscip Respir Med. 2021;16(1):777. doi:10.4081/mrm.2021.777
25. Kocevska D, Lysen TS, Dotinga A, et al. Sleep characteristics across the lifespan in 1.1 million people from the Netherlands, United Kingdom and United States: a systematic review and meta-analysis. Nat Hum Behav. 2020;5(1):113–122. doi:10.1038/s41562-020-00965-x
26. Mokhlesi B, Ham SA, Gozal D. The effect of sex and age on the comorbidity burden of OSA: an observational analysis from a large nationwide US health claims database. Eur Respir J. 2016;47(4):1162–1169. doi:10.1183/13993003.01618-2015
27. Thosar SS, Chess D, Bowles NP, et al. Sleep efficiency is inversely associated with brachial artery diameter and morning blood pressure in midlife adults, with a potential sex-effect. Nat Sci Sleep. 2021;13:1641–1651. doi:10.2147/NSS.S329359
28. Chirakalwasan N, Teerapraipruk B, Simon R, et al. Comparison of polysomnographic and clinical presentations and predictors for cardiovascular-related diseases between non-obese and obese obstructive sleep apnea among Asians. J Clin Sleep Med. 2013;9(6):553–557. doi:10.5664/jcsm.2748
29. Khan MA, Mathur K, Barraza G, et al. The relationship of hypertension with obesity and obstructive sleep apnea in adolescents. Pediatr Pulmonol. 2020;55(4):1020–1027. doi:10.1002/ppul.24693
30. Lusardi P. Effects of insufficient sleep on blood pressure in hypertensive patients A 24-h study. Am J Hypertens. 1999;12(1):63–68. doi:10.1016/S0895-7061(98)00200-3
31. Cooper DC, Ziegler MG, Milic MS, et al. Endothelial function and sleep: associations of flow-mediated dilation with perceived sleep quality and rapid eye movement (REM) sleep. J Sleep Res. 2014;23(1):84–93. doi:10.1111/jsr.12083
32. Del Brutto OH, Mera RM, Penaherrera E, Costa AF, Penaherrera R, Castillo PR. On the association between sleep quality and arterial stiffness: a population study in community-dwelling older adults living in rural Ecuador (The Atahualpa Project). J Clin Sleep Med. 2019;15(8):1101–1106. doi:10.5664/jcsm.7798
33. Kadoya M, Koyama H, Kurajoh M, et al. Sleep, cardiac autonomic function, and carotid atherosclerosis in patients with cardiovascular risks: HSCAA study. Atherosclerosis. 2015;238(2):409–414. doi:10.1016/j.atherosclerosis.2014.12.032
34. Withrow D, Roth T, Koshorek G, Roehrs T. Relation between ambulatory actigraphy and laboratory polysomnography in insomnia practice and research. J Sleep Res. 2019;28(4):e12854. doi:10.1111/jsr.12854
35. Lehrer HM, Yao Z, Krafty RT, et al. Comparing polysomnography, actigraphy, and sleep diary in the home environment: the Study of Women’s Health Across the Nation (SWAN) Sleep Study. SLEEP Advances. 2022;3(1):zpac001. doi:10.1093/sleepadvances/zpac001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Elevated Central Chemosensitivity in Obstructive Sleep Apnea Patients with Hypertension
Wang X, Luo J, Huang R, Xiao Y
Nature and Science of Sleep 2022, 14:855-865
Published Date: 3 May 2022
Comparison of Ring Pulse Oximetry Using Reflective Photoplethysmography and PSG in the Detection of OSA in Chinese Adults: A Pilot Study
Zhao R, Xue J, Zhang X, Peng M, Li J, Zhou B, Zhao L, Penzel T, Kryger M, Dong XS, Gao Z, Han F
Nature and Science of Sleep 2022, 14:1427-1436
Published Date: 18 August 2022
Time Under 90% Oxygen Saturation and Systemic Hypertension in Patients with Obstructive Sleep Apnea Syndrome
Wang L, Wei DH, Zhang J, Cao J
Nature and Science of Sleep 2022, 14:2123-2132
Published Date: 30 November 2022
New Metrics from Polysomnography: Precision Medicine for OSA Interventions
Guo J, Xiao Y
Nature and Science of Sleep 2023, 15:69-77
Published Date: 9 March 2023
A Case of Young Obese Heart Failure Patient Using Multidisciplinary Treatment Centered on the Fantastic Four Improved Cardio Ankle Vascular Index and Cardiac Function
Ikeda Y, Iwakawa M, Kiyokawa H, Nakagami T, Kanzaki S, Ogawa A, Tabata T, Takahashi M, Kinoshita T, Shimizu K
International Medical Case Reports Journal 2023, 16:545-549
Published Date: 14 September 2023