Back to Journals » Local and Regional Anesthesia » Volume 18
Ultrasound-Guided Selective Thoracic Nerve Root Block Combined with Continuous Erector Spinae Plane Block for Postherpetic Neuralgia: A Case Report
Authors Zhang H, Fang L ![]() , Jing S
, Jing S ![]() , Bao X
, Bao X
Received 27 March 2025
Accepted for publication 23 September 2025
Published 7 October 2025 Volume 2025:18 Pages 103—109
DOI https://doi.org/10.2147/LRA.S526163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Video abstract of “Thoracic block and erector spinae block in neuralgia” [526163]
Views: 708
Haolin Zhang, Liang Fang, Sheng Jing, Xiaohang Bao
Department of Anaesthesiology, Second Affiliated Hospital, Army Medical University, Chongqing, People’s Republic of China
Correspondence: Xiaohang Bao, Email [email protected]
Background: Both selective nerve root blocks and erector spinae plane blocks are common regional blocks in clinical practice, and they have both been shown to relieve acute and chronic pain from herpes zoster. Although selective nerve root block (SNRB) may be the theoretically most effective method of drug delivery to the DRG and requires only a small dose of drug with few complications associated with it, it does not provide effective analgesia for a prolonged period of time. However, continuous erector spinae plane block is considered to be one of the most promising minimally invasive means of analgesia that not only provides prolonged analgesia but is simple to perform, has fewer complications, and facilitates indwelling catheters. In this case report, we describe the possible synergistic mechanism of action of SNRB, continuous erector spinae plane block, and effective relief of postherpetic neuralgia with improved patient outcome.
Case Presentation: In this case report, we present the case of an 81-year-old woman with comorbidities including diabetes mellitus, hypertension, and a history of multiple surgeries. She suffered from postherpetic herpes zoster pain in her left thoracic back. Despite trying various treatments such as antiviral medication, physical therapy, traditional Chinese medicine, and a single thoracic paraspinal nerve block, the pain persisted. In consultation with her anesthesiologist, the patient opted for a nerve root block combined with a continuous erector spinae plane block. The erector spinae plane catheter was removed after 14 consecutive days of infusion, although hemolytic Staphylococcus was found in the wound secretions sent for examination, antibiotic treatment was not required. At the 2-year follow-up, the patient remained free of pain recurrence.
Conclusion: Selective nerve root block combined with continuous erector spinae plane block relieves herpes zoster acute phase pain and herpes zoster neuralgia and improves patients’ quality of life.
Keywords: postherpetic neuralgia, herpes zoster, continuous erector spinae plane block, selective nerve root block
Introduction
Postherpetic neuralgia (PHN) is a complication of herpes zoster caused by the varicella-zoster virus. It is commonly observed in the elderly and immunocompromised populations and can lead to psychosocial dysfunction and a significant decline in quality of life.1–3 The definition of PHN has not been consistent across studies, with a range of occurrence from ≥1 to ≥6 months after the rash.4 According to the Chinese Expert Consensus on the Management of Postherpetic Neuralgia, pain that persists for more than 1 month after healing of the herpes zoster rash is defined as PHN.5 As China’s population continues to age, the incidence of PHN is increasing. The primary goal in treating PHN is to effectively manage pain and improve sleep and mood disturbances, ultimately enhancing the quality of life for patients. Currently, there are several clinical treatments available, including pharmacotherapy, physiotherapy, Chinese herbal medicine, acupuncture, and nerve blocks. However, there is still a lack of specific treatments for PHN as of now.3,6,7 Nerve block technology can deliver drugs directly to the lesion, which has a good curative effect and high safety, and has become a popular treatment method for HZ.8 HZ is caused by the activation of the varicella-zoster virus that is dormant in the dorsal root ganglion (DRG) or cranial sensory ganglion of the spinal cord. This results in a painful blistering rash that is distributed in the dermatomes corresponding to the affected DRG. The DRG is the initial site for the onset of PHN and the sensitization of the central and peripheral nervous system that is associated with the development of HZ due to the reactivation of the dormant virus. The primary target for interventions to manage herpes zoster‐associated pain (ZAP) is the DRG. Selective nerve root block is considered to be the most effective method of drug delivery to the DRG compared to other nerve blocks. Additionally, it requires only small doses of drugs and has few associated complications.9 Ultrasound-guided planar blocks of the erector spinae are a highly effective analgesic treatment for thoracic pain, comparable to Thoracic Epidural Analgesia (TEA) and Thoracic Paravertebral Block (TPVB), with a lower risk profile.10–13 Various studies have indicated that the physical diffusion of local anesthetic into the thoracic paravertebral space and associated nerve structures via a transverse connective tissue complex may be the route of action, leading to the blocking of thoracic and sympathetic nerves. However, these routes are not likely to result in a rapid and significant flow of local anesthetic, but rather a gradual leaking out.11,14,15 A study conducted by Aydin et al6 found that ESPB, when applied to both the dorsal and ventral branches of the spinal nerve, can effectively manage acute herpetic pain. The study also revealed that when combined with oral pregabalin and tramadol, ESPB may provide pain relief for up to three months. Additionally, continuous ESPB may be a viable alternative to TPVB and TEA for managing herpes zoster pain. While both selective thoracic nerve root and erector spinae plane blocks are effective in relieving acute herpes zoster pain, this is the first reported case of combining the two nerve blocks to potentially provide longer-lasting pain relief and reduce the likelihood of postherpetic neuralgia recurrence.
Case Presentation
We report a case of an 81-year-old female patient who was transferred to our hospital from a secondary facility. She presented with pain associated with herpes zoster affecting her left shoulder, chest, and back, which had persisted for two months. A comprehensive examination revealed poorly controlled hypertension, fluctuating around 180/102 mmHg. The patient has a history of diabetes spanning 18 years, with her usual medication proving ineffective in managing her blood sugar levels, which fluctuate between 8 and 14.0 mmol/L. Additionally, she exhibited hypoalbuminemia, severe osteoporosis, hypokalemia, and hypophosphatemia. Her medical history includes a hysterectomy and multiple fracture fixations involving the left hip joint, scapula, ribs, metatarsal bones, and right wrist joint, all contributing to her painful experience. Upon examination, blisters, papules, and local ulcerations with scabs were observed on her left shoulder, back, armpit, intercostal spaces, and the inner side of her left upper arm. Despite receiving acupuncture, wet compresses, antiviral medications, and a single injection of thoracic paravertebral nerve block before undergoing a continuous erector spinae plane block, the patient continued to experience recurrent chest and back pain, with a pain visual analog scale (VAS) score ranging from 8 to 9. This pain frequently occurs at night, significantly impacting the patient’s sleep quality. Verbal and written informed consent to the patient’s inclusion in the study was obtained from her and her relatives. They were informed about the purpose of the report, the nature of the information to be disclosed, and the intended use of any accompanying images.
Methods (Investigations and Treatment)
Upon admission to the operating room, the patient’s vital signs were monitored: heart rate (HR) at 89 bpm, blood pressure at 180/102 mmHg, peripheral oxygen saturation (SpO2) at 97%, and body temperature at 36.3°C. After establishing intravenous access, dexmedetomidine was administered immediately at a dose of 1 μg/kg·min, and after 10 minutes, it was adjusted to 0.5 μg/kg·min for continuous sedation, and the mask continued oxygen (5 L/min). Standard surgical disinfection and draping were performed, followed by the placement of a Doppler ultrasound low-frequency convex array probe (2–6 MHz) laterally on the lumbar region. A long-axis scan was utilized to locate the 12th rib, gradually scanning towards the 5th rib and then towards the mid-spine to identify the 5th transverse process. The probe was subsequently rotated 90 degrees to visualize the 5th spine, transverse process, and vertebral plate in the same ultrasound plane. Further adjustments were made to locate the intervertebral foramen beneath the vertebral plate. An in-plane puncture technique was then employed to puncture the outer edge of the vertebral plate, with the needle gently directed towards the intervertebral foramen until a breakthrough was observed. The position of the puncture needle was confirmed using X-ray imaging to ensure it was outside the thoracic intervertebral foramen dura and away from both intravascular and subarachnoid spaces. After retracting the needle, 2 mL of the therapeutic solution was slowly injected without the presence of cerebrospinal fluid, blood, or gas. This technique was similarly applied to complete the 3rd and 4th thoracic nerve root blocks. After a successful thoracic nerve root block, the 6th transverse process was localized using a linear array probe (8–14 MHz) in parallel with the midline paraspinal opening of approximately 3 cm, and two layers of muscle were visible on the surface of the bony acoustic shadow of the transverse process, from superficial to deep, the rhomboid and erector spinae muscles, respectively. The patient was entered caudally, and the tip of the needle was withdrawn free of cerebrospinal fluid, blood, and gas when it reached the surface of the 5th transverse process or touched the transverse process bone. 20 mL of 0.2% ropivacaine hydrochloride injection (registration number: H20140763, AstraZeneca AB) was injected into the deep surface of the erector spinae muscle (Figure 1A). Ultrasound showed that the deep surface of the erector spinae muscle was pushed open, and a dark area of hypoechoic fluid appeared on the surface of the transverse process. The 18G cannula was then fixed to exit the 20G puncture needle, a 20G nylon epidural catheter (Perifix® PinPad) was placed for 5 cm (Figure 1B), 2 mL of 0.9% sodium chloride solution was pushed in to ensure the catheter tip was positioned (Figure 1C), and the catheter was attached to a luer lock connector with an antimicrobial filter and secured to the patient’s back using a surgical sterile dressing.
 |
Figure 1 Ultrasound-guided puncture needle and catheter tip position. (A) Tip of the puncture needle reaches the transverse process. (B) Catheter placed in the plane of the erector spinae muscle. (C) Local anesthetic injected through the catheter. Abbreviations: ESM, erector spinae muscle; TM, trapezius muscle; T5, Transverse process of the fifth thoracic vertebra; T6, Transverse process of the sixth thoracic vertebra. |
After the completion of the regional block, the patient was placed in the prone position while all vital signs remained stable Throughout the operation, the patient breathed smoothly and without discomfort. Thirty minutes following the conclusion of the regional block, the pain sensation in the left side of the thoracic back, T2-T9, at the block plane was significantly reduced by the needle prick method. The pain VAS score was registered as 0, prompting the connection of a pulsatile analgesic pump. The drug formulation and parameters of the analgesic pump included ropivacaine 600mg, dexmedetomidine 50 μg, and 0.9% saline 236mL, with the first dose recorded at 10mL, PCA 5mL/time, 10mL injected for every 3h interval, and a lock time of 30 minutes. After receiving no special observation, the patient was safely returned to the ward.
Outcome and Follow-Up
Patients were assessed at the bedside 12 hours after regional block surgery, and pain VAS was recorded as zero. Patient-reported sleep VAS score of 9, indicating good sleep quality. Patients underwent postoperative analgesia using an erector spinae plane block and experienced significant improvements in pain and sleep over the next 14 days (Figure 2). On the fourteenth day, the patient had a low-grade fever (37.3°C), and there was a small amount of yellowish-white discharge at the catheter puncture site. After 12 hours of removal of the vertical spinal plane catheter, the patient’s pain VAS score was zero. Three days later, hemolytic Staphylococcus was found, but the patient did not have a fever, and the catheter puncture wound was dry, and there was no redness or swelling, so clinical pharmacy experts considered that it was a fixed value bacteria on the skin surface and did not need antibiotic treatment for the time being. The patient’s erector spinae plane puncture site and left shoulder, armpit, left upper arm, and anterior chest are clean, dry, and crusted with no residual signs of trauma, blood, or exudate. Telephone follow-up at 1, 3, 6, and 12 months after surgery, patients did not report recurrence of chest pain or back pain.
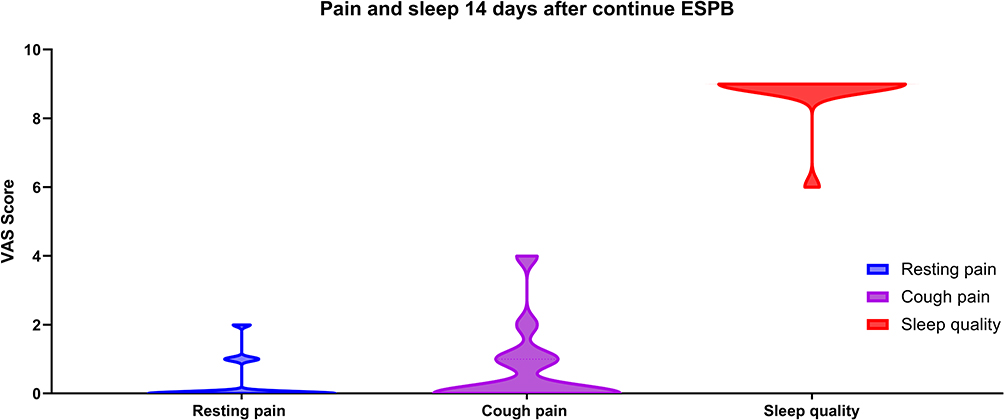 |
Figure 2 Pain and sleep 14 days after continuing ESPB. Abbreviations: POD, postoperative day; ESPB: erector spinae plane block. |
Discussion
Our case report is characterized by significant pain relief for two weeks and improved sleep quality and quality of life for the patient with no recurrence at 2 years postoperatively, suggesting that ultrasound-guided selective thoracic nerve root block combined with continuous vertical spinal muscle plane block has a significant role in improving the prognosis of PHN. Because of the risk of infection associated with prolonged indwelling catheters in the erector spinae plane, medications cannot be infused through the catheter for prolonged periods of time for prolonged treatment. This is the first case report in an elderly population with PHN to report significant improvement in pain and no recurrence of ZAP at 2 years postoperatively, and the patient did not take antiviral medications or receive other prophylaxis after surgery.
PHN is the most common clinical sequel of HZ, referring to neuropathic pain that persists after the outbreak phase of HZ.16 Risk factors for PHN include female gender, advanced age, severe rash and pain during acute HZ episodes, severe immunosuppression, autoimmune diseases, and diabetes.17,18 Although pharmacological therapies are available, less than half of patients experience more than 50% pain relief with first-line medications.19 Treatment with selective nerve root blocks during the acute phase of HZ can greatly reduce the duration of PHN to 2.4 years, but no treatment is fully effective for PHN. In this case, a combination of superimposed mechanisms or different treatments with multiple mechanisms of action is required.19
Nerve blocks, radiofrequency ablation, and spinal cord stimulation (SCS) are commonly employed minimally invasive interventional procedures. Nerve blocks reversibly interrupt nerve conduction, reducing nociceptive input to alleviate or treat pain and disrupt the vicious cycle of herpetic neuralgia, while also improving blood circulation.8 Furthermore, nerve blocks are relatively straightforward for novices to master, cost-effective, and consequently more readily adopted within healthcare settings. The optimal efficacy of spinal cord stimulation (SCS) remains under investigation. Whilst newer approaches such as high-frequency SCS and burst SCS are increasingly utilised clinically, their analgesic mechanisms differ significantly from conventional SCS.20 The use of radiofrequency ablation for PHN is contentious. Although it provides demonstrable analgesic benefit, a proportion of patients experience inadequate pain relief and high short-term recurrence rates, often necessitating supplementary pain management strategies. Additionally, radiofrequency ablation carries a risk of neurodestruction, potentially leading to neurological deficits.21,22 Consequently, nerve blocks are more frequently employed in the management of ZAP. Ultrasound-guided thoracic nerve root blocks are a promising technique that involves injecting a small amount of fluid near the intervertebral foramen to allow more effective drug delivery to the spinal DRG. Selective nerve root blocks are considered the most effective method of drug delivery to the DRG, and treatment with selective nerve root blocks during the acute and subacute phases of HZ can cure PHN within 2.4 to 5 years. Ultrasound-guided planar block of the erector spinae is another promising technique because it involves safe and easy catheter placement, provides adequate analgesia in patients with HZ, and may reduce the incidence of PHN. Continuous erector spinae plane blocks can provide significant relief of acute pain and reduce the incidence of PHN in patients with HZ, significantly improving the quality of life and sleep disturbance.
In this case, a combination regimen of ropivacaine hydrochloride, VitB12 injection, compound betamethasone injection, and dextromethorphan was used for treating PHN. Ropivacaine can block the conduction of neuropathic pain signals for a long period by further blocking the action of nociceptive nerve stimulation on the nerve root. Compound betamethasone injection is a long-acting glucocorticoid preparation that can inhibit the production of inflammatory factors, increase local microcirculatory blood flow, and reduce the local edema of the nerve root. VitB12 injection can participate in the formation of neuro-lipoproteins, improve the nutrition of the diseased nerve, and promote nerve repair. Dexmedetomidine, a highly selective α2 agonist, can effectively prolong the anesthesia time and significantly reduce postoperative pain. By blocking a mixture of ropivacaine and dexmedetomidine injected early in the HZ, dexmedetomidine tromethamine can effectively reduce the incidence of PHN by acting directly on the dorsal root ganglion and presynaptic α2 adrenergic receptors. In two basic studies, dexmedetomidine showed its analgesic efficacy in vincristine-induced pain neuropathic rats and spinal nerve ligation model rats.23,24 Based on animal and clinical studies, dextromethorphan tromethamine is believed to be effective in reducing the incidence of PHN by nerve blockade with a mixture of ropivacaine and dextromethorphan injected early in the HZ.25 The mechanism may be, on the one hand, that dextromethorphan acts directly on the dorsal root ganglion, leading to inhibition of substance P release in the injurious pathway; on the other hand, dextromethorphan acts on the presynaptic α2 adrenergic receptor and reduces neurotransmitter release by inhibiting calcium inward flow. Therefore, the case was treated with good efficacy in this case. While there have been positive therapeutic outcomes observed in PHN patients treated with a combination of selective nerve root block and continuous erector spinae plane block, further confirmation through prospective randomized clinical studies is necessary. Infection associated with an indwelling catheter was our main concern, so we performed a thoracic nerve root and continuous vertical spinal muscle plane block in a strictly sterile laminar flow operating room, and dressed the patient with strictly sterile chlorhexidine-containing sponge dressings, and disinfected the wounds and changed the dressings every 24 hours. In addition, we worked with the endocrinologist to control the patient’s blood glucose slightly below 11.1 mmol/L and strengthened the nutrition to prevent the albumin from falling below 35 g/dl. Unfortunately, on the 14th day of the catheterization, the patient developed a fever and yellow secretion from the catheter puncture site, and the catheter was withdrawn in order to avoid further deterioration of the condition.
Herpes zoster acute-phase pain and postherpetic neuralgia constitute ZAP, and there is continuity between them in terms of the mechanism of occurrence and clinical manifestations, with no clear-cut point of separation, so it is not appropriate to completely separate the diagnosis and treatment process of the two, but rather to treat them as a whole, and to recognize and manage them comprehensively. Therefore, clinicians should try to cross the “barriers” between dermatology, pain medicine, neurology, anesthesiology, and other related departments, and take the reduction of the occurrence of ZAP, especially the occurrence of PHN, as the main medical decision-making basis and value orientation, and break through the “academic boundaries” formed by the clinicians of the above departments due to the differences in their professional backgrounds. This will break through the “academic boundaries” formed by clinicians of the above departments due to their different professional backgrounds, and enable patients with herpes zoster to receive timely, effective, systematic, and standardized medical care and treatment as much as possible during the consultation process.
Conclusion
With this case, we preliminarily conclude that the combination of selective nerve root block and continuous erector spinae plane block can alleviate the symptoms of postherpetic neuralgia, improve the long-term efficacy, and enhance the quality of life of patients. However, synergistic effects of drugs or between drugs, as well as the possibility of self-healing in the natural course of the patient’s disease, cannot be excluded. Therefore, more randomized controlled trials with different lesion sites, different doses of local anesthetics, and different infusion patterns are needed to confirm their safety, optimal timing, and generalizability.
Ethics Approval
Institutional approval from the Ethics Committee/Institutional Review Board of the Second Affiliated Hospital of Army Medical University for the publication of this case report was not required.
Patient Consent
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
Acknowledgments
We would like to thank the patients and their families for their support throughout the treatment process.
Disclosure
The authors have no conflicts of interest for this work.
References
1. Feller L, Khammissa RAG, Fourie J, et al. Postherpetic neuralgia and trigeminal neuralgia. Pain Res Treat. 2017;2017:1681765. doi:10.1155/2017/1681765
2. Forbes HJ, Bhaskaran K, Thomas SL, et al. Quantification of risk factors for postherpetic neuralgia in herpes zoster patients: a cohort study. Neurology. 2016;87(1):94–102. doi:10.1212/WNL.0000000000002808
3. Gross GE, Eisert L, Doerr HW, et al. S2k guidelines for the diagnosis and treatment of herpes zoster and postherpetic neuralgia. J Dtsch Dermatol Ges. 2020;18(1):55–78.
4. Harpaz R, Ortega-Sanchez IR, Seward JF, et al. Prevention of herpes zoster: recommendations of the advisory committee on immunization practices (ACIP). MMWR Recomm Rep. 2008;57(RR–5):
5. Yu S, Wan Y, Wan Q, et al. Chinese expert consensus on diagnosis and treatment of postherpetic neuralgia. Chin J Pain Med. 2016;22(3):161–167.
6. Aydin T, Balaban O, Ahiskalioglu A, et al. Ultrasound-guided erector spinae plane block for the management of herpes zoster pain: observational study. Cureus. 2019;11(10):e5891. doi:10.7759/cureus.5891
7. Wen B, Wang Y, Zhang C, et al. Efficacy of different interventions for the treatment of postherpetic neuralgia: a Bayesian network meta-analysis. J Int Med Res. 2020;48(12):300060520977416. doi:10.1177/0300060520977416
8. Kim HJ, Ahn HS, Lee JY, et al. Effects of applying nerve blocks to prevent postherpetic neuralgia in patients with acute herpes zoster: a systematic review and meta-analysis. Korean J Pain. 2017;30(1):3–17. doi:10.3344/kjp.2017.30.1.3
9. Doo AR, Choi JW, Lee JH, et al. The efficacy of selective nerve root block for the long-term outcome of postherpetic neuralgia. Korean J Pain. 2019;32(3):215–222. doi:10.3344/kjp.2019.32.3.215
10. Jo Y, Park S, Oh C, et al. Regional analgesia techniques for video-assisted thoracic surgery: a frequentist network meta-analysis. Korean J Anesthesiol. 2022;75(3):231–244. doi:10.4097/kja.21330
11. Lin J, Liao Y, Gong C, et al. Regional analgesia in video-assisted thoracic surgery: a bayesian network meta-analysis. Front Med. 2022;9:842332. doi:10.3389/fmed.2022.842332
12. Sandeep B, huang X, Li Y, et al. A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: a network meta-analysis. Int J Surg. 2022;105:106840. doi:10.1016/j.ijsu.2022.106840
13. Tsui BCH, Fonseca A, Munshey F, et al. The erector spinae plane (ESP) block: a pooled review of 242 cases. J Clin Anesth. 2019;53:29–34. doi:10.1016/j.jclinane.2018.09.036
14. Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth. 2021;68(3):387–408. doi:10.1007/s12630-020-01875-2
15. Scimia P, Basso Ricci E, Droghetti A, et al. The ultrasound-guided continuous erector spinae plane block for postoperative analgesia in video-assisted thoracoscopic lobectomy. Reg Anesth Pain Med. 2017;42(4):537. doi:10.1097/AAP.0000000000000616
16. Wei S, Li X, Wang H, et al. Analysis of the risk factors for postherpetic neuralgia. Dermatology. 2019;235(5):426–433. doi:10.1159/000500482
17. Forbes HJ, Thomas SL, Smeeth L, et al. A systematic review and meta-analysis of risk factors for postherpetic neuralgia. Pain. 2016;157(1):30–54. doi:10.1097/j.pain.0000000000000307
18. Zhou H, Wang Z, Jin H, et al. A systematic review and meta-analysis of independent risk factors for postherpetic neuralgia. Ann Palliat Med. 2021;10(12):12181–12189. doi:10.21037/apm-21-3028
19. Schmader K. Herpes Zoster. Clin Geriatr Med. 2016;32(3):539–553. doi:10.1016/j.cger.2016.02.011
20. heijmans L, Joosten EA. Mechanisms and mode of action of spinal cord stimulation in chronic neuropathic pain. Postgrad Med. 2020;132(sup3):17–21. doi:10.1080/00325481.2020.1769393
21. Peng Z, guo J, Zhang Y, et al. Development of a model for predicting the effectiveness of pulsed radiofrequency on zoster-associated pain. Pain Ther. 2022;11(1):253–267. doi:10.1007/s40122-022-00355-3
22. Usmani H, Dureja GP, Andleeb R, et al. Conventional radiofrequency thermocoagulation vs pulsed radiofrequency neuromodulation of ganglion impar in chronic perineal pain of nononcological origin. Pain Med. 2018;19(12):2348–2356. doi:10.1093/pm/pnx244
23. Lee HG, Choi JI, Kim YO, et al. The role of alpha-2 adrenoceptor subtype in the antiallodynic effect of intraplantar dexmedetomidine in a rat spinal nerve ligation model. Neurosci Lett. 2013;557 Pt B:118–122. doi:10.1016/j.neulet.2013.10.002
24. Park HJ, Kim YH, Koh HJ, et al. Analgesic effects of dexmedetomidine in vincristine-evoked painful neuropathic rats. J Korean Med Sci. 2012;27(11):1411–1417. doi:10.3346/jkms.2012.27.11.1411
25. Yang F, Liao P, You Y, et al. The effectiveness of repetitive paravertebral block with ropivacaine and dexmedetomidine for the prevention of postherpetic neuralgia in patients with acute herpes zoster. Postepy Dermatol Alergol. 2022;39(1):116–120. doi:10.5114/ada.2021.106021
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fire Needling Acupuncture for Adult Patients with Acute Herpes Zoster: Protocol of a Systematic Review and Meta-Analysis
Liu L, Chen Q, Yang J, Gang W, Zhao L, Lyu T, Jing X, Zhang CS, Li B
Journal of Pain Research 2022, 15:2161-2170
Published Date: 2 August 2022
Comparison of a One- versus Two-Week Treatment with Famciclovir Upon Reductions in Pain and Occurrence of Postherpetic Neuralgia in Herpes Zoster: A Randomized Open-Label Trial
Peng F, He H, Xia T, Lv S
Infection and Drug Resistance 2023, 16:721-726
Published Date: 2 February 2023
Effects of Intradermal Botulinum Toxin Injections on Herpes Zoster Related Neuralgia
Peng F, Xia TB
Infection and Drug Resistance 2023, 16:2159-2165
Published Date: 12 April 2023
The Effect of CT-Guided Pulsed Radiofrequency Combined with Ozone Injection on Zoster-Associated Pain: A Retrospective Study
Wang X, Yu J, Han CF, He JD, Yang WQ, Wang Q, Chen JP
Journal of Pain Research 2023, 16:1321-1332
Published Date: 20 April 2023
Exploring the Link Between Diabetes, Herpes Zoster, and Post-Herpetic Neuralgia: Insights From Mendelian Randomization
Yang X, Li D, Chen Y, Zhang X, Zhao Q
Journal of Pain Research 2025, 18:1479-1489
Published Date: 21 March 2025