")
Back to Journals » Infection and Drug Resistance » Volume 16
Effects of Intradermal Botulinum Toxin Injections on Herpes Zoster Related Neuralgia
Received 19 December 2022
Accepted for publication 17 March 2023
Published 12 April 2023 Volume 2023:16 Pages 2159—2165
DOI https://doi.org/10.2147/IDR.S401972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Fen Peng,1 Tian-Bao Xia2
1Department of Dermatology, Peking University Third Hospital, Beijing, People’s Republic of China; 2Department of Dermatology, People’s Liberation Army Strategic Support Force Characteristic Medical Center, Beijing, People’s Republic of China
Correspondence: Tian-Bao Xia, Department of Dermatology, People’s Liberation Army Strategic Support Force Characteristic Medical Center, No. 9th Anxiang Beili Road, Chaoyang District, Beijing, 100101, People’s Republic of China, Email [email protected]
Background: Postherpetic neuralgia (PHN), which represents the most common chronic complication of herpes zoster, is characterized by intense pain and is difficult to treat. In fact, no treatments are currently available that can effectively reduce the pain associated with PHN. Recent evidence has been presented indicating that Botulinum toxin (BoNT-A) can serve as an effective and safe treatment for peripheral neuropathic pain.
Objective: The effects of intradermal BoNT-A injections on herpes zoster related neuralgia were investigated in this study.
Methods: Patients diagnosed with herpes zoster related acute neuralgia (N=13 – acute group) and those diagnosed with postherpetic neuralgia (N=17 - PHN group) were enrolled in this study. The two groups were treated with intradermal injections of BoNT-A at the site of their affected pain areas and were then assessed at 1 day, 1 week, 2 weeks, 1 month, 2 months and 3 months after their BoNT-A treatments.
Results: When compared with pre-treatment values, Visual Analogue Scores (VAS) in all patients were all significantly decreased at all times tested following BoNT-A injection. Before treatment, PHN patients had significantly higher VAS than those in the acute group. However, after 1 day of treatment, there was no difference in VAS between the two groups. None of the patients in the acute phase treated with BoNT-A developed PHN.
Conclusion: BoNT-A injections significantly reduced herpetic-related pain and proved to be a more effective treatment for the PHN versus acute pain group. Moreover, an early application of BoNT-A can alleviate the probability of developing PHN.
Keywords: herpes zoster, postherpetic neuralgia, botulinum toxin
Introduction
Herpes zoster (HZ), which represents a reactivation of the Varicella-zoster virus (VZV) in the host, has been reported as a possible adverse event in response to COVID-19 vaccination.1 Postherpetic neuralgia (PHN) is the most common chronic complication of HZ and is characterized by intense pain.2 While the pain associated with HZ typically lasts for 2–4 weeks, PHN is defined by a pain that persists for 4–12 weeks.3 At present, it is believed that the pain of PHN is related to pathological changes such as inflammatory edema, scarring or even hemorrhage resulting from damage to peripheral nerve tissue after an acute VZV infection.4 Pharmacological treatments for herpes zoster neuralgia include pregabalin, gabapentin, antidepressants, anticonvulsants, carbamazepine, lamotrigine, opioids, and topical lidocaine ointments. However, the evidence for these interventions is often inconclusive,5 and the analgesic effect is not obvious. In addition, the side effects associated with these drugs, such as dizziness, ataxia, nausea, vomiting, drowsiness, and rash, can be extremely distressing.6 Therefore, it is especially important to seek a drug that provides better pain relief, longer pain relief time and fewer side effects.
Botulinum toxin type A (BoNT-A), produced by C. botulinum in anaerobic laboratory cultures, is a large molecular weight protein of approximately 900,000 daltons. It is comprised of 150,000 daltons of toxic units noncovalently bound to nontoxic proteins that help protect the toxic units against digestive enzymes.7
Botulinum toxin (BoNT) is a potent neuromodulator that serves as a highly versatile drug capable of exerting numerous clinical effects as applied for both therapeutic and aesthetic purposes.8 The effects of BoNT have been primarily ascribed to its muscle relaxation effects, but it is also widely accepted as a therapeutic procedure in rehabilitation across a range of neurological disorders involving spasticity.9 In addition, recent evidence has been presented indicating that BoNT-A is an effective and safe treatment for peripheral neuropathic pain.10,11
While it has been demonstrated that BoNT-A can be efficacious for the treatment of nerve injury, the specific mechanisms responsible for such effects remain uncertain. Results from recent studies in animal models suggest that botulinum neurotoxin A (BoNT-A) can accelerate nerve regeneration and improve functional recovery after injury to peripheral nerves, with the possible mechanisms proposed for such effects being activation or proliferation of support cells (Schwann cells, mast cells, and macrophages), increased angiogenesis and enhanced blood flow to regenerating nerves.12 With regard to its effects on pain, some possible mechanisms of BoNT-A include retrograde axonal transport of toxins, inhibition of neuropeptides, such as substance P and calcitonin gene-related protein (CGRP), glutamate and deactivation of Na channels.13
In this study, we injected BoNT-A as a treatment for 30 patients with herpes zoster related neuralgia and followed up on the outcomes of this protocol. We also examined the effects of intradermal BoNT-A injections on herpes zoster related neuralgia as involved with PHN.
Materials and Methods
Patients
The Medical Ethics Committee of the Strategic Support Force Medical Center in China approved this study, which was conducted in accordance with the Declaration of Helsinki and all study participants provided informed written consents. All participating patients with herpes zoster and PHN were recruited from the Department of Dermatology of the Strategic Support Force Medical Center. Among these patients, the 13 diagnosed with herpes zoster presenting with neuralgia were treated for the first time and were enrolled into the acute group, while 17 patients were diagnosed with PHN. Our definition of PHN consisted of patients experiencing pain persisting ≥90 days following zoster diagnosis. All patients in this study received famciclovir 250 mg tid for 7 days, Mecobalamin for 1 month and some also received painkillers as requested.
Use of Intradermal Botulinum Toxin
The 30 patients were treated with intradermal injections of BoNT-A at the site of the affected pain areas. Injection sites were distributed in a checkerboard-like pattern, with a space of approximately 1.5–2 cm between two injection sites (Figure 1).
 |
Figure 1 Patients were treated with intradermal injections of BoNT/A at the site of the affected pain areas. Injection sites were distributed in a checkerboard-like pattern, with a space of approximately 1.5–2 cm between two injection sites. |
Visual Analogue Score (VAS)
The most frequently used tool for pain measurement in the general population is that of VAS. As this score has been identified as the most sensitive, reproducible and simplest pain scale, it was employed in our current study.
Data Collection
We followed up these patients at 1 day, 1 week, 2 weeks, 1 month, 2 months and 3 months after the BoNT-A treatment. All data, including characteristics of the patients and outcome measures (VAS), were recorded within a questionnaire designed by the investigators of this study. Patients were recruited between May and August of 2020. Each patient underwent a standard assessment procedure and routine follow-up, as performed at 3 months after their BoNT/A injection.
Statistical Analysis
Qualitative variables were expressed as percents and quantitative variables in means ± standard deviations (SD). Data were analyzed using an existing software program (SAS 9.4). To compare the groups at baseline, a t-test was used for quantitative variables and the Fisher’s exact test for qualitative variables. A mixed effect model was used to evaluate VAS between the two groups. The Wilcoxon rank sum test as based on the mixed effect model was used for data failing to demonstrate a normal distribution. A p < 0.05 was required for the results to be considered as statistically significant.
Results
Baseline Population Demographics
Table 1 provides a summary of all the relevant data from the subjects within the acute herpes zoster (N=13; 6 males and 7 females) and PHN (N=17; 9 males and 8 females) groups. Patients in the acute group were slightly younger (median age: 66 years) than those in the PHN group (median age: 70.1 years). Skin lesions were mainly distributed in the region of the trunk, with no significant sex (P=1.00), age (P=0.12) or lesion location (P=0.89) being obtained between the two groups.
 |
Table 1 Summary of Patient Characteristics in Acute and Postherpetic Neuralgia (PHN) Groups |
When compared with pre-treatment values, VAS were all significantly decreased at 1 day, 1 week, 2 weeks, 1 month, 2 months and 3 months after botulinum injection in both the acute and PHN groups (Table 2 and Figure 2).
 |
Table 2 Comparisons of Pre- versus Post-Botulinum Toxin VAS as a Function of Different Times Following Treatment in the Acute and PHN Groups |
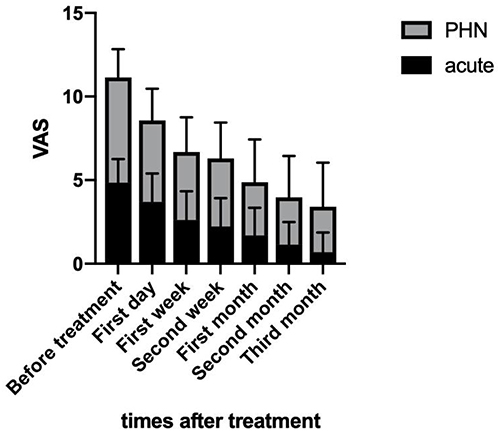 |
Figure 2 Comparisons of VAS before and at varying times post-Botulinum Toxin treatment in the acute and PHN groups. |
When comparing VAS between the acute and PHN groups, VAS in the PHN group were significantly higher than that of the acute group before Botulinum Toxin treatment. At one day after Botulinum Toxin treatment, there were no statistically significant differences in VAS between the two groups (Table 3).
 |
Table 3 Comparisons of VAS in the Acute versus PHN Group |
Discussion
In this study, we assessed the capacity for BoNT-A injections to relieve herpetic-related pain. We found that BoNT-A therapy was more effective in the treatment of PHN versus acute pain. When compared with pre-treatment values, Visual Analogue Scores (VAS) in all patients were all significantly decreased at all times tested following BoNT-A injection. Before treatment, PHN patients had significantly higher VAS than those in the acute group. However, after 1 day of treatment, there was no difference in VAS between the two groups. Interestingly, none of the patients using BoNT-A in the acute phase developed PHN, suggesting that an early application of BoNT-A can effectively alleviate the probability of developing PHN.
PHN-associated pain is considered neuropathic.14 Neuropathic pain (NP) results from a lesion or disease affecting the somatosensory nervous system and encompasses common neurological pain syndromes such as trigeminal neuralgia (TN), postherpetic neuralgia (PHN), diabetic neuropathic pain (DN) and postsurgical neuralgia.15 With reactivation of varicella zoster virus, there is inflammation of the dorsal root ganglia and nociceptive pathway, with the result that spontaneous discharge and activation thresholds are significantly changed. Pain and temperature detection systems are then hypersensitive to photomechanical stimulation, resulting in severe pain.16,17 Treatment of PHN consists of an early application of antiviral drugs and topical or systemic use of analgesics. Topical analgesics include a 5% lidocaine patch and capsaicin, systemic analgesics such as gabapentin and opioid analgesics may often be necessary.18,19 Results from some recent studies have demonstrated that electroacupuncture can be effective in treating the acute pain of Herpes Zoster and low-level laser therapy can reduce the incidence of PHN.2,20 Moreover, there are some case reports documenting the efficacy of toxins in patients with PHN refractory to conventional treatments in terms of VAS score reduction, with an analgesic duration ranging from 52 to 64 days and a good degree of tolerability.14,21
However, data regarding the efficacy of BoNT-A on acute pain and PHN of herpes zoster have yet to be presented. Here, we now provide data demonstrating that BoNT-A was effective not only in patients with acute herpes zoster pain and PHN but also reduced the occurrence of herpes zoster PHN.
Botulinum toxin type A has been used for years in the fields of neurology, rehabilitation and physical medicine and has proven to be an innocuous and effective therapy.13,22 It seems that BoNT-A might also be effective for the comprehensive management of neuropathic pain, especially for diabetic polyneuropathy.23 BoNT-A can accelerate nerve regeneration and improve functional recovery after injury to peripheral nerves.12 Moreover, BoNT-A has the capacity to promote wound healing by attenuating the release of norepinephrine and many neurotransmitters, which inhibit vasoconstriction and increase blood flow and, in this way, may exert some positive effects on chronic ulcers. Ischemic ulcers, secondary to Raynaud’s phenomenon, seem to be the most likely type of ulcers that have benefited from BoNT-A.24 Results from a recent study have revealed that an injection of botulinum toxin (BoNT) into the glabellar region of the head served as a novel therapeutic approach for the treatment of depression. The theoretical foundation of BoNT is not specific for depression but may apply to any disorder associated with an excess of negative emotionality.25 Interestingly, there is a case report of a patient experiencing psoriasis and post-stroke spasticity, who demonstrated psoriatic lesion remission following local BoNT-A injections that were administered for the treatment of upper limb spasticity.8 Psoriasis is a complex immune-mediated inflammatory disorder which, on the basis of our previous study, was found to involve the nervous system.26
BoNT/A may represent an effective therapeutic option for PHN. Some case-reports documented the efficacy of the toxin in patients with PHN refractory to conventional treatments in terms of VAS score reduction at a mean dose of 100 U, with an analgesic effect duration ranging from 52 to 64 days and a good tolerability.14,21,27
A long-lasting BoNT/A therapeutic effect has been confirmed in a RCT on 30 adults with PHN in which only the 13 subjects randomized to BoNT/A achieved a >50% reduction in VAS score (NNT=1.2, 95% CI, 2–1; ARR=0.87, 95% CI, 055–096; P<0.001). Notably, BoNT/A improvement in pain and sleep scores persisted for 16 weeks.28
These studies of injectable botulinum toxin type A for postherpetic neuralgia were similar to our trial results.
The clinical utility of BoNT-A originates from its ability to block muscular contractions by inhibiting neurotransmission between peripheral nerve cells and muscle fibers.29 For example, BoNT-A has been shown to inhibit the release of calcitonin gene-related peptide (CGRP) and Substance P (SP).13 When BoNT-A enters nerve cells, its capacity for division prevents acetylcholine release into the neuromuscular junction and thus blocks muscle fiber contraction.30 And, when injected into the subcutaneous region of the dermis, BoNT-A reduced acetylcholine release from autonomic nerve terminals. BoNT-A has also been used as a safe and effective method to enhance primary focal hyperhidrosis in armpits, palms and feet due to its ability to reduce the hyperactive function of eccrine glands.31 However, the underlying mechanisms of BoNT-A in the treatment of herpes zoster related neuralgia are not clear. Some possible mechanisms may include a retrograde axonal transport of the toxin, inhibition of neuropeptides, such as substance P and calcitonin gene-related protein (CGRP), glutamate and deactivation of Na channels.13 Each of these possible mechanisms warrant further investigation.
This study has some limitations. Notably, it suffers from a lack of a double-blind randomization and placebo control. There is also a possibility for selection bias in this study, as patients with more serious concomitant diseases were not enrolled in this study. However, in our observations, patients with more severe PHN and more extensive rash tended to receive an injection of BoNT-A as an alternative treatment. Therefore, more randomized controlled trials will be required to corroborate and substantiate our results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Anant P, Mohamad G, Uwe W. Herpes zoster: a review of clinical manifestations and management. Viruses. 2022;14(2):192.
2. Chen YT, Wang HH, Wang TJ, et al. Early application of low-level laser may reduce the incidence of postherpetic neuralgia (PHN). J Am Acad Dermatol. 2016;75(3):572–577. doi:10.1016/j.jaad.2016.03.050
3. Wollina U, Machetanz J. Herpes zoster und postzosterische Neuralgie. Der Hautarzt. 2016;67:653–665. doi:10.1007/s00105-016-3834-y
4. Forbes HJ, Bhaskaran K, Thomas SL, et al. Quantification of risk factors for postherpetic neuralgia in herpes zoster patients. Neurology. 2016;87:94–102. doi:10.1212/WNL.0000000000002808
5. Dosenovic S, Jelicic Kadic A, Miljanovic M, et al. Interventions for neuropathic pain: an overview of systematic reviews. Anesth Analg. 2017;125(2):643–652. doi:10.1213/ANE.0000000000001998
6. Shackleton T, Ram S, Black M, Ryder J, Clark GT, Enciso R. The effi- cacy of botulinum toxin for the treatment of trigeminal and postherpetic neuralgia: a systematic review with meta-analyses. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016;122(1):61–71. doi:10.1016/j.oooo.2016.03.003
7. Schantz EJ, Johnson EA. Botulinum toxin: the story of its development for the treatment of human disease. Perspect Biol Med. 1997. doi:10.1353/pbm.1997.0032
8. Nicolae PM, Cristina B, Gabriela IM, et al. Botulinum toxin use for modulating neuroimmune cutaneous activity in psoriasis. Medicina. 2022;58(6):813. doi:10.3390/medicina58060813
9. Popescu MN, Petca RC, Beiu C, et al. Efficiency of different preparations of botulinum toxin type A, Xeomin and Dysport, in the management of spastic upper limb after stroke. Rehabilitation. 2019;70(10):3490–3494.
10. Intiso D, Basciani M, Santamato A, Intiso M, Di Rienzo F. Botulinum toxin type A for the treatment of neuropathic pain in neuro-rehabilitation. Toxins. 2015;7:2454–2480. doi:10.3390/toxins7072454
11. Vincent H, Sebastien S, Valeria M. Efficacy and safety of botulinum A toxin for the treatment of chronic peripheral neuropathic pain: a systematic review of randomized controlled trials and meta-analysis. Eur J Pain. 2022;26:980–990. doi:10.1002/ejp.1941
12. Michael A, Sabine P, Sharma Shashi K, et al. Preclinical evidence for the role of Botulinum Neurotoxin A (BoNT/A) in the treatment of peripheral nerve injury.microorganisms. 2022;10(5):886. doi:10.3390/microorganisms10050886
13. Anupam DG, Suzanne E, Jessica S, et al. A systematic review and meta-analysis of efficacy of botulinum toxin A for neuropathic pain. Toxins. 2022;14(1):36. doi:10.3390/toxins14010036
14. Sotiriou E, Apalla Z, Panagiotidou D, et al. Severe post-herpetic neuralgia successfully treated with botulinum toxin A: three case reports. Acta Derm Venereol. 2009;89:214–215. doi:10.2340/00015555-0609
15. Egeo G, Fofi L, Barbanti P. Botulinum neurotoxin for the treatment of pain. Front Neurol. 2020;11. doi:10.3389/fneur.2020.00716
16. Woolf CJ, Shotland P, Coggeshall RE. Peripheral nerve injury triggers central sprouting of myelinated afférents. Nature. 1992;335:75–78. doi:10.1038/355075a0
17. Kost RG, Strauss SE, Wood AJJ. post herpetic neuralgia pathogenesis, treatment, and prevention: a review article. N Engl J Med. 1996;4:32–40. doi:10.1056/NEJM199607043350107
18. Till W, Chris P, Andrea R-D. The capsaicin 8% patch for neuropathic pain in clinical practice: a retrospective analysis. Pain Med. 2013;14:1202–1211. doi:10.1111/pme.12143
19. Tyring SK. Management of herpes zoster and postherpetic neuralgia. J Am Acad Dermatol. 2007;57:136–142. doi:10.1016/j.jaad.2007.09.016
20. Kelin H, Fengjia N, Yi H, et al. Efficacy and safety of electroacupuncture for pain control in herpes zoster: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2022;2022:4478444. doi:10.1155/2022/4478444
21. Ruiz HC, Bermejo P. Botulinum toxin type A in the treatment of neuropathic pain in a case of postherpetic neuralgia. Neurologia. 2008;23:259–262.
22. Lorenzo L, de Sire A, Arianna F, et al. Multidimensional effectiveness of botulinum toxin in neuropathic pain: a systematic review of randomized clinical trials. Toxins. 2022;14(5):308. doi:10.3390/toxins14050308
23. Mehrdad T, Meghdad S, Ali S, et al. The effect of intradermal botulinum toxin a injections on painful diabetic polyneuropathy. Diabetes Metab Syndr. 2020;14:1823–1828. doi:10.1016/j.dsx.2020.09.019
24. Waranaree W, Vasanop V. Botulinum toxin type A for the treatment of skin ulcers: a review article. Toxins. 2022;14(6):406. doi:10.3390/toxins14060406
25. Axel WM, Michelle M, Kruger Tillmann HC, et al. Treatment of depression with botulinum toxin. Toxins. 2022;14(6):383. doi:10.3390/toxins14060383
26. Fen P, Siqi Z, Xuan Z, et al. Calcitonin gene-related peptide upregulates IL-17A and IL-22 in γδ-T cells through the paracrine effect of Langerhans cells on LC/γδ-T co-culture model. J Neuroimmunol. 2022;364:577792. doi:10.1016/j.jneuroim.2021.577792
27. Liu HT, Tsai SK, Kao MC, Hu JS. Botulinum toxin A relieved neuropathic pain in a case of post-herpetic neuralgia. Pain Med. 2006;7:89–91. doi:10.1111/j.1526-4637.2006.00100.x
28. Apalla Z, Sotiriou E, Lallas A, Lazaridou E, Ioannides D. Botulinum toxin A in postherpetic neuralgia: a parallel, randomized, double blind, single-dose, placebo-controlled trial. Clin J Pain. 2013;29:857–864. doi:10.1097/AJP.0b013e31827a72d2
29. Chen S. Clinical uses of botulinum neurotoxins: current indications, limitations and future developments. Toxins. 2012;4:913–939. doi:10.3390/toxins4100913
30. Ababneh OH, Cetinkaya A, Kulwin DR. Long-term efficacy and safety of botulinum toxin A injections to treat blepharospasm and hemifacial spasm. Clin Exp Ophthalmol. 2014;42:254–261. doi:10.1111/ceo.12165
31. Carmichael NME, Dostrovsky JO, Charlton MP. Peptide-mediated transdermal delivery of botulinum neurotoxin type A reduces neurogenic inflammation in the skin. Pain. 2010;149:316–324. doi:10.1016/j.pain.2010.02.024
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.