Back to Journals » Clinical Ophthalmology » Volume 20
Two-Year Follow-Up of the MINI WELL Non-Diffractive Extended Depth-of-Focus Intraocular Lens: A Retrospective Observational Study
Authors Sborgia A, Curatolo MC, Barattini DF ![]() , Niro A
, Niro A ![]() , Barattini L, Sborgia G
, Barattini L, Sborgia G
Received 11 February 2026
Accepted for publication 15 May 2026
Published 24 June 2026 Volume 2026:20 602800
DOI https://doi.org/10.2147/OPTH.S602800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Alessandra Sborgia,1,2 Maria Cristina Curatolo,3 Dionisio Franco Barattini,4 Alfredo Niro,1 Luca Barattini,5 Giancarlo Sborgia2
1Eye Clinic Dept, Hospital “SS. Annunziata” ASL Taranto, Taranto, Italy; 2Department of Medical Science, NeuroScience and Sense Organs, University of Bari, Bari, Italy; 3Innovation and Medical Science Department, SIFI Spa, Aci Sant’Antonio, Catania, Italy; 4Medical Department, Opera CRO, a Tigermed Company, Timisoara, Romania; 5IT Department, TIGERMED Italy, Genova, Italy
Correspondence: Alessandra Sborgia, Eye Clinic Dept, Hospital “SS. Annunziata” ASL Taranto, Taranto, 74121, Italy, Email [email protected]
Purpose: To describe long-term visual outcomes, functional vision, and safety following implantation of the MINI WELL non-diffractive extended depth-of-focus (EDoF) intraocular lens over a two-year follow-up period.
Materials and methods: This monocentric, retrospective, observational study included patients who underwent cataract surgery with binocular implantation of the MINI WELL non-diffractive EDoF intraocular lens. Visual outcomes were assessed postoperatively over 24 months. Evaluations included monocular and binocular uncorrected and corrected visual acuity at distance, intermediate, and near; defocus curve assessment under photopic conditions; contrast sensitivity; binocular reading performance using Radner Reading Charts; and patient-reported outcomes measured with the Visual Function Questionnaire VF-11R. Safety outcomes included adverse events, secondary surgical interventions, and patient-reported photic phenomena.
Results: Twenty-three patients (46 eyes) completed the two-year follow-up and were included in the analysis. At 24 months, monocular and binocular visual acuity was maintained across all tested distances. Binocular uncorrected distance visual acuity of 20/32 Snellen or better was achieved in all patients. Intermediate and near visual acuity were consistent with common daily visual tasks. The binocular defocus curve demonstrated a smooth decline in visual acuity across intermediate defocus levels without distinct focal gaps. Mean binocular reading speed at near distance met established criteria for fluent reading. Contrast sensitivity remained within manufacturer-defined normative ranges across spatial frequencies. Patient-reported outcomes indicated minimal difficulty in vision-dependent daily activities. No intraoperative or postoperative adverse events, secondary surgical interventions, or clinically relevant late complications were reported. Mild photic phenomena were infrequently reported.
Conclusion: At two years, implantation of the MINI WELL non-diffractive EDoF intraocular lens was associated with maintained visual outcomes, functional intermediate and near vision, and a favorable safety profile. These findings support the long-term stability of visual performance with this EDoF intraocular lens. Larger prospective and comparative studies are warranted to confirm these observations.
Trial Registration: ClinicalTrials.gov identifier NCT04801992.
Keywords: cataract, extended depth-of-focus, intraocular lens, presbyopia, visual performance, safety, defocus curve
Introduction
In developed countries, cataracts are readily treated by phacoemulsification and intraocular lens (IOL) implantation. As the population in these countries continues to age, there is an increasing need for additional correction of intermediate and near vision. Consequently, a wide range of multifocal IOLs have been developed to correct presbyopia following traditional IOL implantation.1–4 Bifocal and trifocal IOLs enhance near, intermediate, and distance vision, thereby reducing reliance on spectacles. However, their use is constrained by photic phenomena and reduced contrast sensitivity (CS). Recently, extended depth-of-focus (EDoF) IOLs have been developed to increase the depth of focus, create a continuous focus rather than multiple distinct foci, and avoid the undesirable effects of multifocal IOLs.5 The Mini WELL (SIFI S.p.A., Catania, Italy) is an aspheric progressive EDoF IOL designed for continuous vision in the range of infinity to near (40 cm) distance. This EDoF IOL comprises three optical zones: an outer monofocal zone and two zones with spherical aberrations of opposite sign, an inner zone inducing positive spherical aberrations, and an intermediate zone inducing negative spherical aberrations (Supplementary Figure 1). The transition between the three optical zones is characterized by a gradual power shift, which supports uninterrupted continuous vision.
Mini WELL was CE-marked in 2014 and has been distributed in Italy since that year, and subsequently in all of Europe. Currently, there are no prospective comparative studies between Mini WELL and trifocal IOLs; however, data are available from in vitro evaluations. In particular, Domínguez-Vicent et al6 reported that Mini WELL showed greater defocus tolerance at near distances and better optical quality at far vision with a 4.5 mm aperture than did the diffractive lens TECNIS Symfony (Johnson & Johnson Vision, Santa Ana, CA, USA). The same author7 reported that the optical quality of the Mini WELL IOL was similar to that of the AT LISA tri 839MP (Carl Zeiss Meditec, AG, Jena, Germany) and Finevision (PhysIOL, Liége, Belgium) at intermediate and near vision foci for the 3.00 mm optical aperture, and it was better than the optical quality of both trifocal IOLs at distance vision when the aperture was set to 4.50 mm.7 Several studies have evaluated the visual performance and safety of patients implanted with Mini WELL.8–13 However, there is no published data on long-term follow-up.
This paper presents the results of a two-year follow-up study on the safety and visual performance of the EDoF IOL Mini WELL. The patient population was derived from one of the sites involved in the previous PSM8 study,14 in which the visual performance of the Mini WELL was evaluated by a postoperative visit conducted between 30 and 60 days after surgery.
Methods
Study Design
This was a retrospective, observational, single-center study carried out at the University of Bari “Aldo Moro”. The present study was conducted in accordance with the principles of Good Clinical Practice, the Declaration of Helsinki, and Italian regulations. The study was approved by the Independent Ethics Committee of “Azienda Ospedaliera Universitaria (AOU) Consorziale Policlinico di Bari” with # 0086214/18/10/2019 on October 9, 2019. Written informed consent was obtained from all the patients. The study was registered in the ClinicalTrials.gov database at https://clinicaltrials.gov/search?term=NCT04801992 (Identifier: NCT04801992). This manuscript adheres to the STROBE cohort reporting guidelines.15
Study Population
The present study included 23 patients (11 male and 12 female) over the age of 18 who had previously participated in the PSM8 study (ClinicalTrials.gov Identifier: NCT02740010) and were observed for an additional two years.
The intraocular lens (IOL) power was calculated using standard optical biometry and a routinely adopted IOL power calculation formula in clinical practice. Specifically, the SRK/T formula was used for eyes with an axial length greater than 22 mm, whereas the Hoffer Q formula was used for eyes with axial lengths shorter than 22 mm.
All the patients underwent cataract surgery or refractive lens replacement (RLE) by means of conventional phacoemulsification or femtolaser-assisted procedures. Corneal incision size and position were selected according to the surgeon’s routine clinical practice. Surgery was performed with preoperative symmetric keratometric astigmatism < 1.00 D and healthy, nonsurgically treated corneas. The following exclusion criteria were applied: previous corneal surgery (eg, pterygium, refractive surgery), eye diseases with Snellen visual acuity (VA) less than 20/32, pseudoexfoliation, abnormal pupil size and position, use of contact lenses within 30 days prior to the preoperative visit, and corneal warpage.
Data Collection, Time Points, and Study Outcomes
Outcome measures and timing of evaluation are reported in Supplementary Table 1. The baseline ophthalmic examination was performed during the preoperative visit. This included ocular refraction, optical biometry, corneal topography and asphericity, and corneal aberrometry. Quantitative and qualitative evaluations of the visual performance were conducted at 1–2 months and 24 months postsurgery. Monocular and binocular defocus curves were determined under photopic conditions through the addition of positive lenses up to +1 D (1–2 months follow-up) or +2.0 D (24 months follow-up) and negative lenses up to −4.0 D in half-diopter increments.
Early Treatment Diabetic Retinopathy Study (ETDRS) charts with computerized optotypes were used to assess uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA) at a distance of 4 m. Monocular and binocular visual acuity were evaluated by determining the proportion of eyes that achieved visual acuity targets between Snellen 20/20 and Snellen 20/100. The clear vision range, corresponding to Snellen 20/40 (0.30 logMAR) or better, is considered the minimum standard for safe driving in Europe.16 However, in the 24-month long-term study on the visual performance of the Mini WELL, a threshold of 20/32 Snellen (0.2 LogMAR) was considered, in accordance with the updated standard of the American Academy of Ophthalmology.17
Monocular and binocular visual acuity were evaluated in accordance with the medical practice of the involved site using the ETDRS in computerized optotypes, namely, the YANG SMART (SIFI S.p.A., Catania, Italy).
CS was performed with varying spatial frequency grids of 1.5, 3, 6, 12, and 18 cycles per degree (cpd) without glare using the YANG SMART and CSO Vision Chart Device (CSO, Florence, Italy). Absolute values of contrast sensitivity in logarithmic units (logCSs) were measured for each spatial frequency.
The reading performance of the subjects was evaluated using Radner Reading Charts18 at a distance of 40 cm under photopic conditions. Reading speed, expressed in words per minute (WPM), was calculated as the number of words in a sentence divided by the time in seconds required to read the sentence. The incidence of adverse events (AEs), the occurrence of secondary surgeries due to the optical properties of the IOL, and the frequency of visual disturbances and distortions reported by participants were evaluated using the Halo and Glare Simulator (Supplementary Table 2).19,20
Statistical Analysis
Owing to the descriptive and retrospective nature of this study, no formal a priori sample size calculation or statistical hypotheses were planned. However, a post hoc precision-based estimation of the sample size was performed. The required sample size for estimating a proportion with a 95% confidence level and a margin of error of ±5% was calculated using the standard formula:

where Z = 1.96 for a 95% confidence level, p = 0.5 (conservative assumption), and d = 0.05. This resulted in a minimum required sample size of 42 eyes. The final sample included 46 eyes, satisfying this criterion.
The analysis included all available eyes meeting the inclusion criteria during the study period. As both eyes from the same subject could be included, the results should be interpreted with consideration of potential intra-subject correlation. Data are presented using descriptive statistics, with means and standard deviations calculated for continuous variables and frequencies and percentages calculated for discrete variables, with 95% confidence intervals (CIs) provided to indicate the precision of the estimates and to allow an appropriate interpretation of the results in the context of a limited sample size. The analysis was conducted using SAS software (SAS Institute Inc., Cary, NC, USA).
Results
Visual Performance
This study included 11 men and 12 women (23 patients and 46 eyes, totally) who underwent EDoF IOL Mini WELL implantation. The mean age of the patients was 71.57 ± 8.94 years (range: 47.00–84.00).
This observational study started on March 1, 2014, and concluded on June 30, 2017.
Preoperative mean IOL power on the 46 eyes was 20.98 ± 2.76 (with median 22.00). The average corneal keratometry prior to surgery was 43.66 D ± 1.70 D, the mean corneal asphericity (Q-value at 8 mm) was −0.28 ± 0.12, and the mean axial length was 23.60 ± 1.00 mm. The mean photopic pupil diameter was 2.66 ± 0.36 mm, the mean scotopic pupil diameter was 4.40 ± 0.62 mm, and the mean topographic kappa angle was 0.26 ± 0.11 mm. The mean dioptric power of the implanted IOL was 20.98 ± 2.76 D (range: 15.0 D to 26.5 D). There was a clear improvement in average refractive values two years after IOL implantation, compared to the values recorded at the pre-operative visit and the values obtained at the one- or two-month post-operative check-up, where the intraocular lens power was chosen according to an emmetropic refractive target. Subjective refraction data are reported in Table 1.
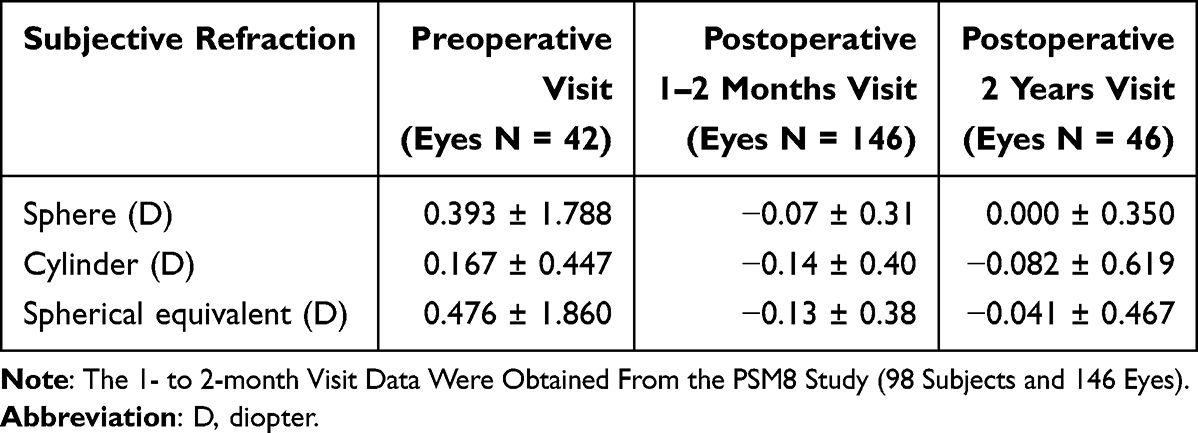 |
Table 1 Subjective Refraction at the Preoperative, 1–2 Month, and 2-Year Postoperative Follow-Up Visits |
Figure 1 illustrates defocus curve assessments obtained at different postoperative time points under distinct testing conditions. This comparison was conducted using two samples of different sizes: the monocular defocus curve at the 1-2-month visit in 164 eyes and the binocular defocus curve at the 24-month visit in 46 eyes. The monocular defocus curve data at the 1–2 month postoperative visit were derived from a previously published clinical investigation (PSM8). Given the different testing conditions (monocular versus binocular) and sample sizes, defocus curve data were analyzed descriptively and were not intended to support longitudinal or comparative inferences.
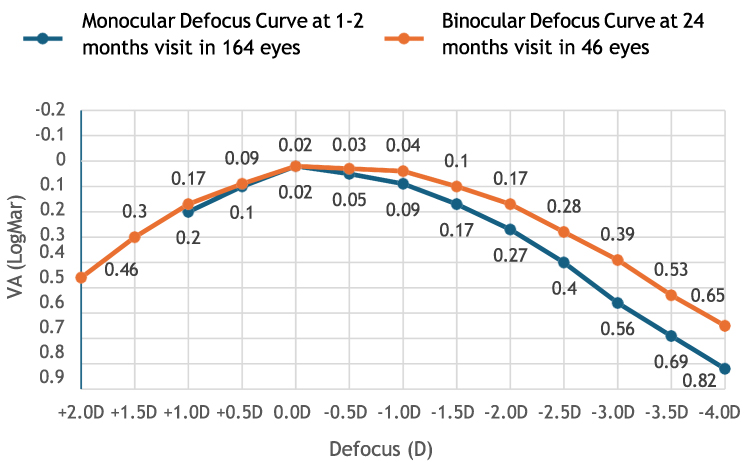 |
Figure 1 Defocus curve assessments obtained under photopic conditions at different postoperative evaluations. Data are presented for descriptive purposes only. Abbreviations: D, diopter; VA, visual acuity. |
Monocular and binocular defocus curves were measured using ETDRS charts at a distance of 4 meters, and visual acuity (VA) was evaluated at different simulated distances using lenses with powers ranging from +1.0 diopter (D) to −4.0 D and from +2.0 D to −4.0 D, respectively. Both the monocular and binocular defocus curves showed a gradual decrease in VA with increasing negative defocus levels. There was no decrease in performance or VA gaps in the intermediate range, and there was no sharp decrease in acuity in the near zone. The single-peak “inverted V” profile of both defocus curves indicates that the Mini WELL provides a continuous range of focus with VA that gradually declines as the distance from the subject changes. A clear range of 0.3 logMAR or better (20/40 Snellen) from +1.0 D to −2.0 D was achieved in the monocular defocus curves. At the 24-month follow-up, the binocular defocus curve demonstrated a mean visual acuity of 0.3 logMAR or better (20/40 Snellen) across defocus values up to −2.5 D, and functional visual acuity levels across a broad range of defocus values.
Visual acuity was assessed at the 24-month follow-up under both monocular and binocular conditions at distance, intermediate and near testing distances (4 m, 100 cm, 63 cm and 40 cm) (Figure 2).
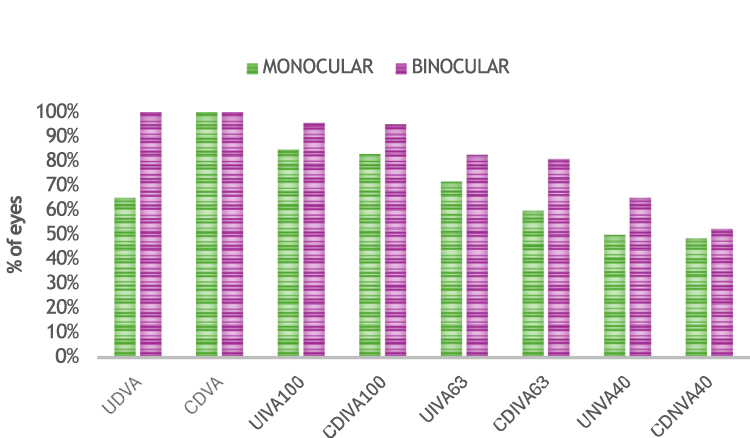 |
Figure 2 Distribution of monocular and binocular visual acuity outcomes at distance, intermediate and near testing distances at the 24-month postoperative follow-up. Visual acuity is reported as the proportion of eyes achieving 20/32 Snellen or better. Abbreviations: UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; UIVA100, uncorrected intermediate visual acuity at 100 cm; DCIVA100, distance corrected intermediate visual acuity at 100 cm; UIVA63, uncorrected intermediate visual acuity at 63 cm; DCIVA63, distance corrected intermediate visual acuity at 63 cm; UIVA40, uncorrected intermediate visual acuity at 40 cm; DCIVA40, distance corrected intermediate visual acuity at 40 cm. |
These results indicate that 65.20% and 100% of patients achieved monocular and binocular uncorrected distance visual acuity (UDVA), respectively, while 20/32 Snellen-corrected distance visual acuity (CDVA) was achieved in 100% of patients in both monocular and binocular vision. Figure 3 evidenced also a large difference in monocular UDVA to binocular UDVA (60 to 100%). The mean values at the 24-month follow-up are reported in Table 2.
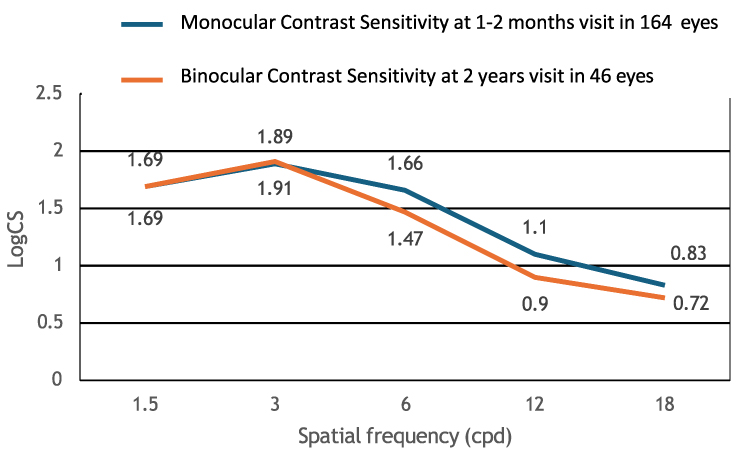 |
Figure 3 Contrast sensitivity measurements obtained under photopic conditions. Data from different postoperative evaluations and testing conditions are presented for descriptive purposes only. Contrast sensitivity is expressed in cycles per degree. Abbreviations: cpd, cycles per degree; CS, contrast sensitivity. |
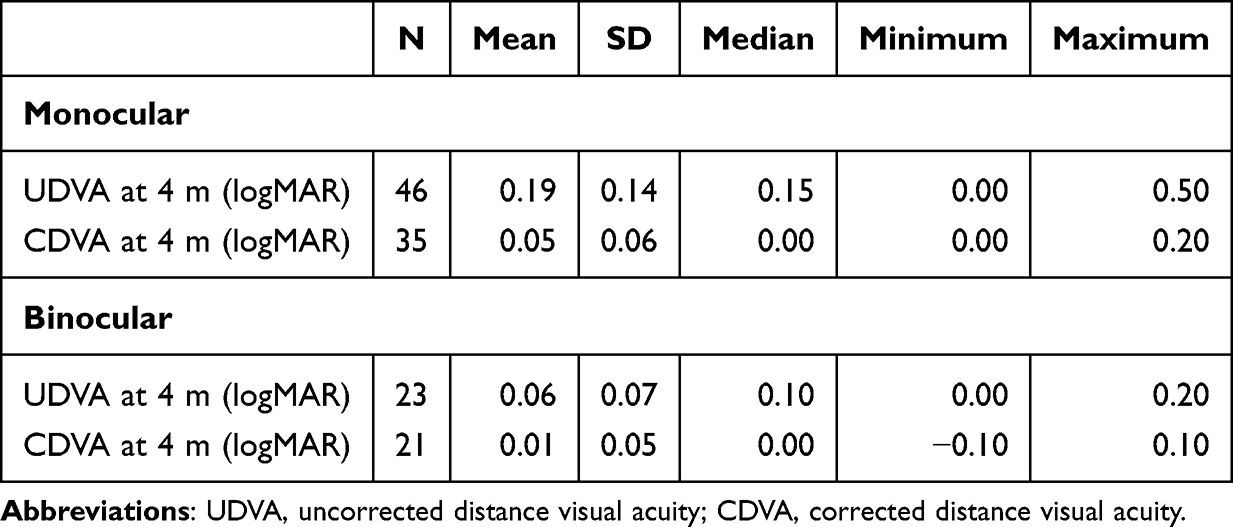 |
Table 2 Monocular and Binocular UDVA at 4 m and Monocular and Binocular CDVA at 4 m at the 24-Month Follow-Up Visit |
Intermediate visual acuity (VA) was tested at both 100 and 63 cm, with and without correction. Monocular and binocular uncorrected intermediate visual acuity (UIVA100) at 100 cm were achieved in 84.8% and 95.7% of patients, respectively, with similar results observed for distance-corrected intermediate visual acuity (DCIVA100) (Table 3).
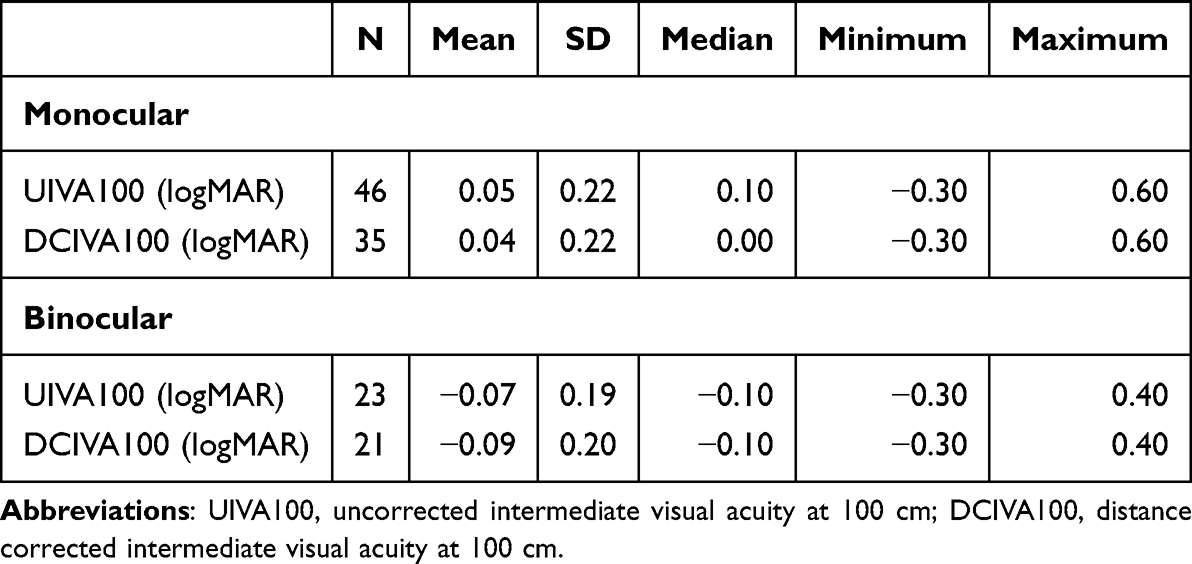 |
Table 3 Monocular and Binocular UIVA100 cm (High Contrast) and Monocular and Binocular DCIVA100 cm (High Contrast) at the 24-Month Follow-Up Visit |
Monocular and binocular uncorrected intermediate visual acuity at 63 cm (UIVA63) were achieved in 71.7% and 82.6% of patients, respectively, and similar results were achieved for distance-corrected intermediate visual acuity (DCIVA63) (Table 4).
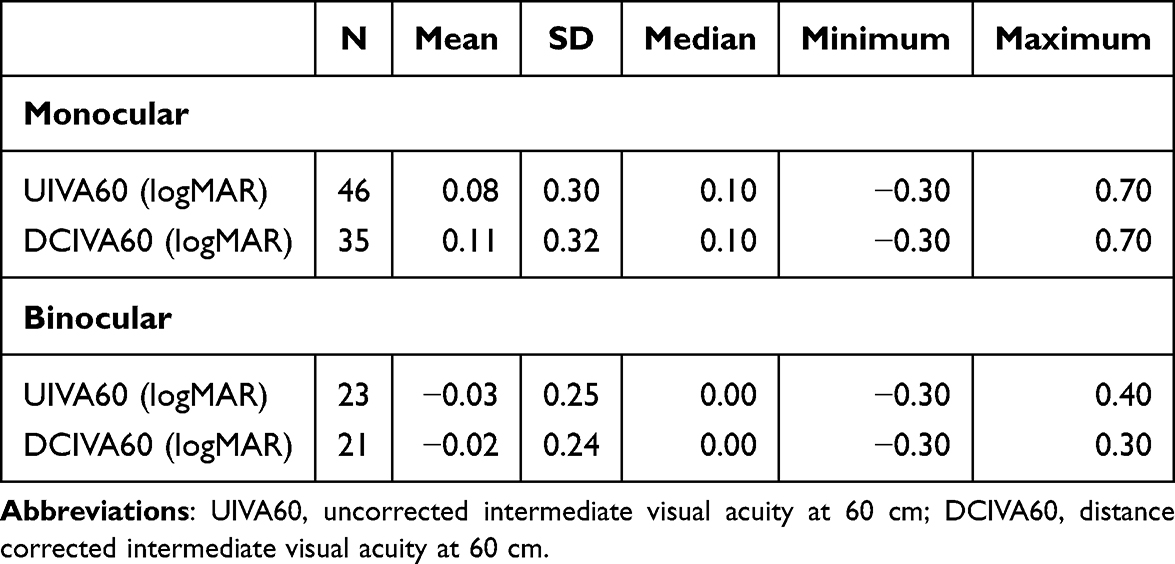 |
Table 4 Monocular and Binocular UIVA60 (High Contrast) and Monocular and Binocular DCIVA60 (High Contrast) at the 24-Month Follow-Up Visit |
Similarly, high percentages were achieved for uncorrected and corrected near visual acuity at 40 cm (UNVA40 and DCNVA40). In terms of binocular vision, 65.2% and 52.4% of the patients demonstrated a visual acuity of 20/32 Snellen (Table 5).
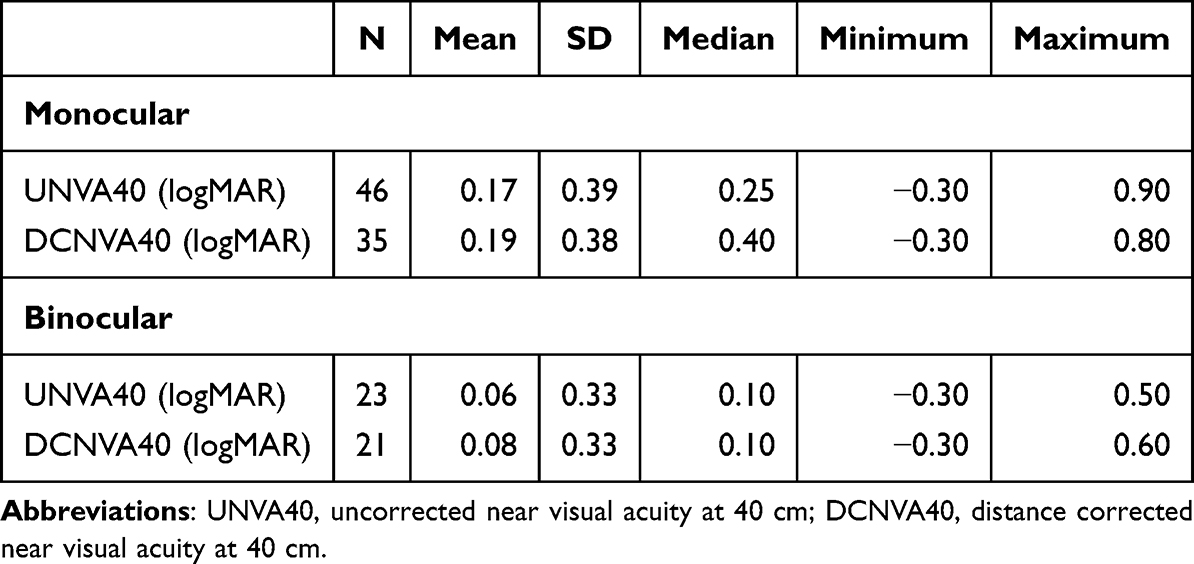 |
Table 5 Monocular and Binocular UNVA40 (High Contrast) and Monocular and Binocular DCNVA40 (High Contrast) at the 24-Month Follow-Up Visit |
These findings provide evidence that the Mini WELL exhibits favorable visual performance when evaluated over an extended period.
Based on the standard minimum reading speed of 80 WPM for fluent reading,20 at 2 years, the mean reading ability was fluent at the common book print size (0.5 logRAD).
At the two-year follow-up, contrast sensitivity values were within manufacturer-defined normative ranges at lower spatial frequencies, while reduced sensitivity was observed at higher spatial frequencies. Binocular contrast sensitivity measurements obtained at 24 months are reported in the context of monocular contrast sensitivity data previously published at the 1–2 month postoperative evaluation in the PSM8 study. Across spatial frequencies, contrast sensitivity values remained within ranges considered compatible with functional vision in pseudophakic eyes under both photopic and lower luminance conditions (Figure 3).
The Visual Function Questionnaire, VF-11R (VF-11R), was used in our study to evaluate the degree of difficulty in performing 12 vision-dependent activities (eg, reading and watching television) in patients who did not use glasses. Higher scores (indicating “No” or “A little”) are indicative of better visual functioning and, thus, greater ability to perform the activity. Conversely, higher scores (indicating “a great deal” or “unable to do the activity”) indicate poorer visual functioning and, consequently, diminished ability to perform the activity.21
The VF-11R revealed that the majority of patients exhibited minimal difficulties in reading small prints (82.6%), reading a newspaper or a book (82.6%), reading a large-print book or a large-print newspaper or numbers on a telephone (82.6%), recognizing people when they are close (82.6%), seeing steps, stairs, or curbs (86.9%), reading traffic signs, street signs, or store signs (82.6%), and performing fine handwork such as sewing, knitting, crocheting, and carpentry (86.9%). They also exhibited the capacity to write checks or fill out forms (78.2%) and to participate in sports such as bowling, handball, tennis, and golf (82.7%). The data also indicate that 78.2% of respondents engaged in leisure activities such as playing games such as bingo, dominos, card games, and mahjong, while 78.3% participated in sports such as bowling, handball, tennis, and golf. Finally, 78.2% of the respondents engaged in leisure activities such as cooking, while 78.3% watched television (Supplementary Table 3).
At 2 years, the total average score was 86.5 ±23.1, with the highest mean score reported for “reading traffic signs, street signs, or store signs” (89.1 ±19.7) and “seeing steps, stairs or curbs” (89.1 ±21.1) questions and the lowest mean score (83.7 ±25.7) reported for “writing checks or filling out forms” (Supplementary Table 4).
Overall, VF-11R results indicated limited self-reported difficulty in performing vision-dependent daily activities without spectacle correction. Although the VF-11R assesses functional vision in daily activities, it was not specifically designed to quantify dysphotopsia symptoms.
Safety
During the two-year follow-up period, no intraoperative or postoperative adverse events, postoperative complications, subjective posterior capsule opacification, or posterior capsulotomy procedures were observed in this cohort.
Patient-reported photic phenomena were assessed at the 24-month follow-up using a structured halo and glare evaluation (Supplementary Figure 2). A significant difference was observed between the proportion of subjects reporting any photic disturbance and those reporting no visual disturbance (chi-square test for proportions, p < 0.0001). Among the enrolled patients, two individuals (8.70%) reported mild glare symptoms classified as G1. Halo phenomena were reported by four patients: one case classified as H1 (4.35%), two cases classified as H2 (8.70%), and one case classified as H3 (4.35%).
Given the limited sample size and the descriptive nature of the study, the absence of observed adverse events should not be interpreted as evidence of rare event exclusion. These safety findings are therefore presented as observational and exploratory and require confirmation in larger, prospectively designed studies with adequate statistical power.
Discussion
Considering the paucity of long-term (>24 months) clinical data on non-diffractive EDoF intraocular lenses, a retrospective observational design was considered appropriate to explore outcome stability and late safety signals.
This study assessed the long-term safety and performance of the EDoF Mini WELL in a cohort of 23 patients who underwent postsurgery visits with 2 years of follow-up.
The following limitations must be clearly caveated:
Although no formal a priori sample size calculation was performed due to the retrospective and descriptive design of the study, a post hoc precision-based estimation was conducted. Assuming a 95% confidence level and a margin of error of ±5% for proportion estimates, a minimum sample size of 42 eyes would be required. The final sample of 46 eyes included in this analysis therefore meets this threshold for descriptive precision. Nevertheless, given the limited sample size and the inclusion of both eyes from some subjects, the study results should be interpreted with caution.
The same considerations could be made regarding the representativeness of the included population. In fact, the number of included eyes was underpowered for performing any inferential comparisons or finding rare safety events.
Population selection: All included patients were subjects of a completed study which agreed to undergo a 24-month follow-up at the center. This could be considered a potential selection bias.
Given the exploratory nature of the study, the retrospective design, lack of a control group, and descriptive analyses with CIS were acceptable However, these factors resulted in an inability to specify the primary outcomes and prevented the use of adjusted tests for paired data. Consequently, the study did not support any causal or comparative claims.
The twenty-four-month follow-up period was appropriate for assessing mid- to long-term visual stability and common late complications, such as posterior capsule opacification (PCO) and neuroadaptation. However, it cannot rule out rare late events.
The final limitation of the study was a potential conflict of interest. In fact, the authors transparently declared the involvement of a Sponsor employee in the medical writing and editing of the manuscript.
To the best of our knowledge, this study is the longest follow-up study of an EDoF-IOL. It provides long-term observational data on the visual performance and photic phenomena associated with this lens. Implantation of the Mini WELL at the two-year follow-up resulted in marked improvement in mean refractive values, satisfactory VA, and fluent reading performance (91.3% of patients were able to read fluently binocularly at bookprint size). These remarkable performances exhibited by the patients have been reflected in their responses to the VF-11R, which indicated a high degree of management of their personal and social routines in daily life. The defocus curves under photopic conditions showed consistent performance at 2 years in comparison to the values obtained at the 1–2 month visit in the 98 subjects (146 eyes) enrolled in the PSM8 study, which was a noteworthy finding, given that the evaluation at the two-year follow-up was conducted binocularly rather than monocularly.
With regard to contrast sensitivity at the two-year follow-up, measurements are reported descriptively across spatial frequencies and luminance conditions. The Mean contrast sensitivity values remained within ranges consistent with values commonly reported in the literature for age-matched pseudophakic populations, with lower values observed at higher spatial frequencies. For contextual purposes, contrast sensitivity data obtained at approximately one to two months after intraocular lens implantation in the same cohort are presented in Table 6. Given the different testing conditions and the descriptive nature of the analysis, no longitudinal inference regarding changes in contrast sensitivity over time can be drawn.
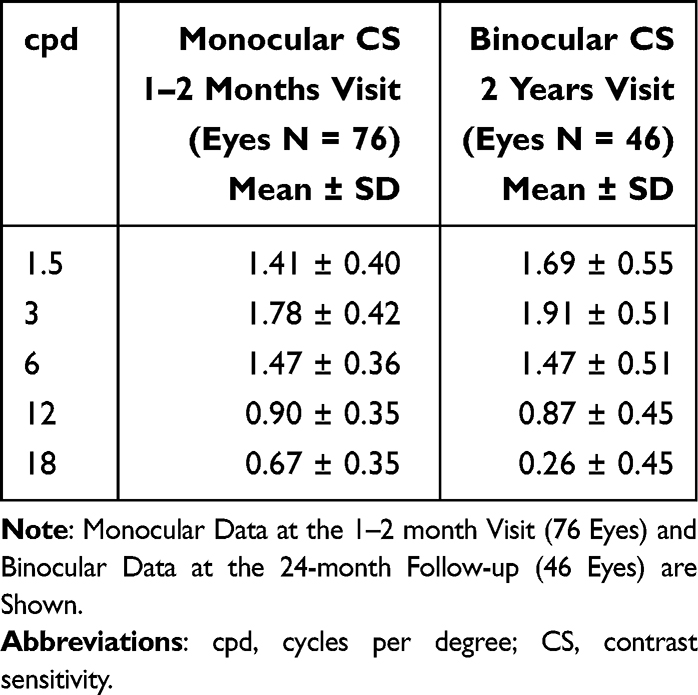 |
Table 6 Descriptive Contrast Sensitivity Measurements Obtained in the Same Patient Cohort at Different Postoperative Evaluations |
Furthermore, the Mini WELL score exhibited a favorable safety profile at the two-year follow-up. The mean strength of halos and glares (4.6%) was classified as “none” according to the strength function classification of halos and glares,22 which categorizes halos as none (0–25%), mild (25–50%), moderate (50–75%), or severe (75–100%). This finding is of particular significance given that the perception of visual disturbances is a frequent issue related to IOLs. Numerous studies have highlighted the association between patient satisfaction and the minimization of disruptive visual phenomena, such as halos and glare.23,24
Indeed, the persistence of such symptoms has been reported as a relevant factor contributing to patient dissatisfaction and, in some cases, to the request for intraocular lens exchange. In the present study, the low incidence of patient-reported photic phenomena observed at the two-year follow-up may be interpreted in the context of stable functional visual outcomes over time. Visual neuroadaptation has been proposed as one of several mechanisms potentially involved in patient adaptation to presbyopia-correcting intraocular lenses.25,26
However, neuroadaptation was not directly assessed in the present study, and no causal inference regarding its role in the observed outcomes can be drawn.
The outcomes of this study, previously reported in a preprint available on ResearchSquare (https://www.researchsquare.com/article/rs-4723302/v1), align with earlier investigations of the Mini WELL8–13 and improve our knowledge of the long-term effects of IOL placement. The long-term safety of the product was confirmed by the absence of device deficiencies, product-related postoperative complications, and product-related serious adverse effects (AEs), including secondary surgical interventions (SSIs), 2 years after surgery. The findings of the present study are consistent with previously published clinical investigations of the Mini WELL IOL8–13 and provide additional observational data on visual and safety outcomes over an extended follow-up period. Over two years of follow-up, no device-related deficiencies, postoperative complications, or serious adverse events (SAEs), including secondary surgical interventions (SSIs), were observed in the study cohort. The absence of adverse events in this cohort should be interpreted with caution, as the study was not designed to identify rare complications.
Although this study is limited by its descriptive nature and small sample size, its long-term follow-up data may be enhanced in the future with the results of additional long-term postmarket investigations involving a larger patient population.
Conclusion
Long-term evaluation of extended depth-of-focus intraocular lenses is important to assess the durability of visual outcomes and functional vision. In this retrospective observational study, implantation of the MINI WELL non-diffractive extended depth-of-focus intraocular lens was associated with maintenance of refractive and visual outcomes over a two-year follow-up period, providing functional vision across distance, intermediate and near ranges with a low incidence of patient-reported photic phenomena.
Contrast sensitivity and reading performance remained within ranges compatible with everyday visual requirements, and no late-onset adverse events or secondary surgical interventions were observed. Although limited by its retrospective design, small sample size and lack of a control group, this study provides additional long-term observational data on the performance and safety of the MINI WELL extended depth-of-focus intraocular lens. These findings contribute to the existing evidence on EDoF technologies and suggest that the MINI WELL intraocular lens may be considered among available options for patients seeking sustained functional vision with minimal visual disturbances.
Abbreviations
AE, Adverse event; AOU, Azienda Ospedaliera Universitaria; CDVA, Corrected distance visual acuity; CI, confidence intervals; cpd, cycles per degree; CS, Contrast sensitivity; D, Diopter; DCIVA, Distance corrected intermediate visual acuity; DCNVA, Distance corrected near visual acuity; EDoF, Extended depth-of-focus; ETDRS, Early Treatment of Diabetic Retinopathy Study; IOL, Intraocular lens; logCS, contrast sensitivity in logarithmic units; logMAR, Logarithm of the minimal angle of resolution; logRAD, Logarithm of Reading Acuity Determination; SSI, Secondary surgical intervention; UDVA, Uncorrected distance visual acuity; UIVA, Uncorrected intermediate visual acuity; UNVA, Uncorrected near visual acuity; VA, Visual acuity; VF-11R, Visual Function Questionnaire; WPM, Word per minute.
Data Sharing Statement
The full protocol and the datasets analyzed for the study are available from the corresponding author upon reasonable request.
Ethical Statement
Ethics approval was obtained from the Independent Ethics Committee of “Azienda Ospedaliera Universitaria (AOU) Consorziale Policlinico di Bari” with # 0086214/18/10/2019 on October 9th, 2019. This study was conducted in accordance with the ethical standards of the Declaration of Helsinki. Written informed consent was obtained from any subject enrolled in the study.
Acknowledgments
Warm thanks to Salvatore Bianco MD on behalf of Opera CRO for support in medical writing and Marius Ardelean for statistical analysis. The authors thank SIFI S.p.A., Catania, Italy, for the image used in Figure 1, which was used with permission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Support for this clinical investigation and medical writing assistance was funded by SIFI S.p.A., Via Ercole Patti 36, 95025, Lavinaio, Aci S. Antonio (Catania), Italy.
Disclosure
CC is an employee at SIFI SpA, the funder of the study. DFB is employed at the Opera Contract Research Organization, the CRO that monitored the study; also reports grants from SIFI SpA, during the conduct of the study. LB is a former internship at TIGERMED Italy Srl, the company involved in data management of the study. AS, AN, and GS declare no conflicts of interest.
References
1. Steinert RF. Visual outcomes with multifocal intraocular lenses. Curr Opin Ophthalmol. 2000;11(1):12–12. doi:10.1097/00055735-200002000-00004
2. Leyland M, Zinicola E. Multifocal versus monofocal intraocular lenses in cataract surgery: a systematic review. Ophthalmology. 2003;110(9):1789–1798. doi:10.1016/S0161-6420(03)00722-X
3. Blaylock JF, Si Z, Vickers C. Visual and refractive status at different focal distances after implantation of the ReSTOR multifocal intraocular lens. J Cataract Refract Surg. 2006;32(9):1464–1473. doi:10.1016/j.jcrs.2006.04.011
4. Lehmann R, Waycaster C, Hileman K. A comparison of patient-reported outcomes from an apodized diffractive intraocular lens and a conventional monofocal intraocular lens. Curr Med Res Opin. 2006;22(12):2591–2602. doi:10.1185/030079906X158039
5. Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol. 2020;9(3):194–202. doi:10.1097/APO.0000000000000296
6. Dominguez-Vicent A, Esteve-Taboada JJ, Del Aguila-Carrasco AJ, Ferrer-Blasco T, Montes-Mico R. In vitro optical quality comparison between the Mini WELL Ready progressive multifocal and the TECNIS Symfony. Graefes Arch Clin Exp Ophthalmol. 2016;254(7):1387–1397. doi:10.1007/s00417-015-3240-7
7. Dominguez-Vicent A, Esteve-Taboada JJ, Del Aguila-Carrasco AJ, Monsalvez-Romin D, Montes-Mico R. In vitro optical quality comparison of 2 trifocal intraocular lenses and 1 progressive multifocal intraocular lens. J Cataract Refract Surg. 2016;42(1):138–147. doi:10.1016/j.jcrs.2015.06.040
8. Tognetto D, Cecchini P, Giglio R, Turco G. Surface profiles of new-generation IOLs with improved intermediate vision. J Cataract Refract Surg. 2020;46(6):902–906. doi:10.1097/j.jcrs.0000000000000215
9. Giers BC, Khoramnia R, Varadi D, et al. Functional results and photic phenomena with new extended-depth-of-focus intraocular Lens. BMC Ophthalmol. 2019;19(1):197. doi:10.1186/s12886-019-1201-3
10. Auffarth GU, Moraru O, Munteanu M, et al. European, multicenter, prospective, non-comparative clinical evaluation of an extended depth of focus intraocular lens. J Refract Surg. 2020;36(7):426–434. doi:10.3928/1081597X-20200603-01
11. Ruiz-Mesa R, Blanch-Ruiz J, Ruiz-Santos M, Montes-Mico R. Optical and visual quality assessment of an extended depth-of-focus intraocular lens based on spherical aberration of different sign. Int Ophthalmol. 2021;41(3):1019–1032. doi:10.1007/s10792-020-01659-z
12. Nicula CA, Rednik AM, Nicula AP, Bulboaca AE, Nicula D, Horvath KU. Long term visual outcomes in cataract surgery with bilateral implantation of the extended depth of focus intraocular lens - mini WELL ready type. Rom J Ophthalmol. 2022;66(4):317–325. doi:10.22336/rjo.2022.58
13. Nowik KE, Nowik K, Kanclerz P, Szaflik JP. Clinical performance of extended depth of focus (EDOF) intraocular lenses - a retrospective comparative study of mini WELL ready and symfony. Clin Ophthalmol. 2022;16:1613–1621. doi:10.2147/OPTH.S341698
14. Savini G, Balducci N, Carbonara C, et al. Functional assessment of a new extended depth-of-focus intraocular lens. Eye. 2019;33(3):404–410. doi:10.1038/s41433-018-0221-1
15. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) Statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
16. Bron AM, Viswanathan AC, Thelen U, et al. International vision requirements for driver licensing and disability pensions: using a milestone approach in characterization of progressive eye disease. Clin Ophthalmol. 2010;23(4):1361–1369. doi:10.2147/OPTH.S15359
17. MacRae S, Holladay JT, Glasser A, et al. Special report: American academy of ophthalmology task force consensus statement for extended depth of focus intraocular lenses. Ophthalmology. 2017;124(1):139–141. doi:10.1016/j.ophtha.2016.09.039
18. Radner W. Reading charts in ophthalmology. Graefes Arch Clin Exp Ophthalmol. 2017;255(8):1465–1482. doi:10.1007/s00417-017-3659-0
19. Gutiérrez R, Jiménez JR, Villa C, Valverde JA, Anera RG. Simple device for quantifying the influence of halos after lasik surgery. J Biomed Opt. 2003;8(4):663–667. doi:10.1117/1.1607333
20. Castro JJ, Jiménez JR, Ortiz C, Alarcón A, Anera RG. New testing software for quantifying discrimination capacity in subjects with ocular pathologies. J Biomed Opt. 2011;16:015001. doi:10.1117/1.3526702
21. Whittaker SG, Lovie-Kitchin J. Visual requirements for reading. Optom Vis Sci. 1993;70(1):54–65. doi:10.1002/j.1538-9235.1993.tb03071.x
22. Gothwal VK, Wright TA, Lamoureux EL, Pesudovs K. Measuring outcomes of cataract surgery using the Visual Function Index-14. J Cataract Refract Surg. 2010;36(7):1181–1188. doi:10.1016/j.jcrs.2010.01.029
23. Tarib I, Kasier I, Herbers C. Postoperative results in patients implanted with a novel enhanced depth of focus intraocular lens. EC Ophthalmol. 2018;9(4):192–202.
24. Morya AK, Nishant P, Singh A, Sinha S, Shah RC. A retrospective comparative performance analysis of multifocal eyecryl Actv IOL and the world’s first progressive polyfocal autofocus pro IOL. Clin Ophthalmol. 2025;19:1387–1399. doi:10.2147/OPTH.S521607
25. Zhu D, Karki S, Dhariwal M, Soini E, Asseburg C. Patient-reported outcomes of visual disturbances with a trifocal intraocular lens: a meta-analysis. Ophthalmol Ther. 2025;14(2):379–390. doi:10.1007/s40123-024-01085-9
26. Rosa AM, Miranda ÂC, Patrício MM, et al. Functional magnetic resonance imaging to assess neuroadaptation to multifocal intraocular lenses. J Cataract Refract Surg. 2017;43(10):1287–1296. doi:10.1016/j.jcrs.2017.07.031
27. Zhang L, Lin D, Wang Y, et al. Comparison of visual neuroadaptations after multifocal and monofocal intraocular lens implantation. Front Neurosci. 2021;15:648863. doi:10.3389/fnins.2021.648863
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Refractive and Visual Outcomes of a Monofocal Non-Constant Aberration Aspheric Intraocular Lens
Hernández-Martínez A, Díaz-del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tañá-Rivero P
Clinical Ophthalmology 2022, 16:2521-2530
Published Date: 10 August 2022
The REVIVE Study: Long Term Outcomes of a Novel Non-Diffractive Extended Vision IOL versus Monofocal Control IOL
Shafer BM, McCabe C, Reiser H, Newsom TH, Berdahl J
Clinical Ophthalmology 2022, 16:3945-3950
Published Date: 28 November 2022
Clinical Outcomes After Bilateral Implantation of a Diffractive Trifocal Intraocular Lens: A Worldwide Pooled Analysis of Prospective Clinical Investigations

Kohnen T, Lapid-Gortzak R, Ramamurthy D, Bissen-Miyajima H, Maxwell A, Kim TI, Modi S
Clinical Ophthalmology 2023, 17:155-163
Published Date: 10 January 2023
Prospective Randomized Single-Masked Study of Bilateral Isofocal Optic-Design or Monofocal Intraocular Lenses
Ang RET, Stodulka P, Poyales F
Clinical Ophthalmology 2023, 17:2231-2242
Published Date: 4 August 2023
Clinical Outcomes of a Monofocal, Optimized, Aspheric, Hydrophobic Acrylic Intraocular Lens Implant
García-Tomás B, Marín-Sánchez JM, García-Elskamp C, Alcon-Ruiz E, Montesinos-López L, García Martínez-Lozano B
Clinical Ophthalmology 2023, 17:3215-3224
Published Date: 27 October 2023