Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Tumor Burden Thresholds Associated with Successful Downstaging After Yttrium-90 Radioembolization in Hepatocellular Carcinoma Beyond UCSF Criteria
Authors Chiu CH ![]() , Yu CY, Ou HY
, Yu CY, Ou HY ![]() , Tsang LC
, Tsang LC ![]() , Huang PH
, Huang PH ![]() , Weng CC, Lu Y, Chen CL, Cheng YF
, Weng CC, Lu Y, Chen CL, Cheng YF
Received 31 March 2026
Accepted for publication 27 June 2026
Published 10 July 2026 Volume 2026:13 613375
DOI https://doi.org/10.2147/JHC.S613375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Chun-Hua Chiu,1 Chun-Yen Yu,1,* Hsin-You Ou,1 Leung-Chit Tsang,1 Po-Hsun Huang,1 Ching-Chun Weng,2 Yi Lu,2 Chao-Long Chen,3 Yu-Fan Cheng1,*
1Department of Diagnostic Radiology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 2Department of Diagnostic Radiology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan; 3Liver Transplantation Center and Department of Surgery, Kaohsiung Chang Gung Memorial Hospital, and Chang Gung University College of Medicine, Kaohsiung, Taiwan
*These authors contributed equally to this work
Correspondence: Chun-Yen Yu; Yu-Fan Cheng, Email [email protected]; [email protected]
Purpose: Hepatocellular carcinoma (HCC) is frequently diagnosed at advanced stages, limiting access to curative therapies. Yttrium-90 (Y-90) trans-arterial radioembolization (TARE) has been used for tumor downstaging to enable surgical resection or liver transplantation; however, the factors associated with successful downstaging and potential selection thresholds remain unclear.
Patients and Methods: We retrospectively analyzed 65 patients with unresectable HCC exceeding the University of California, San Francisco (UCSF) criteria who underwent Y-90 TARE between 2020 and 2024. Tumor burden parameters, dosimetric features, treatment response, overall survival (OS), and progression-free survival (PFS) were evaluated. Receiver operating characteristic (ROC) analysis was performed to identify exploratory thresholds associated with successful downstaging, and survival outcomes were assessed using Kaplan–Meier methods.
Results: Down-staging to within UCSF criteria was achieved in 58.5% of patients. Successfully down-staged patients had significantly longer OS than non-downstaged patients (median OS, not reached vs. 18.8 months; p = 0.034). ROC analysis identified exploratory tumor burden thresholds associated with downstaging failure, including largest tumor diameter ≥ 7.8 cm, tumor volume ≥ 265 cm3, and a composite tumor number–diameter score > 11. The presence of multiple adverse tumor burden factors was associated with a high likelihood of downstaging failure. When adequate tumor radiation delivery was achieved, a tumor-to-normal uptake ratio (T/N) > 4 predicted successful downstaging in tumors < 7.8 cm, whereas its prognostic value diminished in larger lesions.
Conclusion: Y-90 TARE enables effective downstaging in a substantial proportion of patients with advanced HCC and may facilitate subsequent curative surgery or living donor liver transplantation. Tumor burden metrics and size-dependent T/N ratios were associated with successful downstaging and may assist patient selection for Y-90 TARE. These findings should be considered exploratory and warrant validation in larger prospective studies.
Keywords: Yttrium-90, hepatocellular carcinoma, downstaging, liver transplantation, radioembolization
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy and remains a leading cause of cancer-related mortality worldwide.1–3 Despite improvements in surveillance, a significant proportion of patients continue to present at intermediate or advanced disease stages, limiting eligibility for curative treatments such as resection, ablation, or liver transplantation.4,5 Locoregional therapies play a crucial role in disease control and in downstaging advanced tumors to within transplant criteria.6 Yttrium-90 (Y-90) transarterial radioembolization (TARE) has emerged as an effective locoregional therapy capable of achieving durable tumor response and prolonged time to progression compared with conventional transarterial chemoembolization.7–10 Several studies have demonstrated its potential as a bridging or downstaging therapy.11–15
However, the factors associated with successful downstaging after Y-90 TARE remain incompletely understood. Although the Milan criteria remain the standard benchmark for liver transplantation, the UCSF criteria provide a broader yet well-validated selection framework and are commonly considered in living donor liver transplantation. Therefore, we used post-treatment UCSF status as the primary downstaging endpoint. We hypothesized that baseline tumor burden characteristics and dosimetric parameters may predict successful downstaging to within UCSF criteria after Y-90 TARE. Accordingly, this study aimed to identify factors associated with successful downstaging and to evaluate subsequent surgical conversion and clinical outcomes.
Materials and Methods
Patient Selection
This retrospective study included patients with hepatocellular carcinoma (HCC) treated with yttrium-90 (Y-90) resin microsphere transarterial radioembolization (TARE) at our institution between February 2020 and December 2024. Eligible patients exhibited imaging features diagnostic of HCC, had unresectable disease exceeding the University of California, San Francisco (UCSF) criteria, and preserved liver function (Child–Pugh class A or B). Additional inclusion criteria were a platelet count >100,000/µL and an international normalized ratio (INR) <1.5. Main portal vein thrombosis was considered a relative contraindication. All cases were evaluated by a multidisciplinary tumor board comprising interventional radiologists, nuclear medicine physicians, and hepatologists. Of 67 consecutive patients treated with Y-90 TARE during the study period, 65 patients met the follow-up requirements and were included in the final analysis (Figure 1).
 |
Figure 1 Patient selection and post–Y-90 TARE UCSF stratification define the study cohorts for outcome analysis. From February 2020 to December 2024, 67 patients with unresectable hepatocellular carcinoma (HCC) beyond the University of California, San Francisco (UCSF) criteria were screened. After exclusion of two patients due to inadequate follow-up, 65 patients were included in the final analysis. At 3 months after Yttrium-90 (Y-90) transarterial radioembolization (TARE) with resin microspheres, patients were stratified into post-treatment UCSF-fit (n = 38) and UCSF-unfit (n = 27) groups for outcome analysis. |
Pre-Treatment Evaluation and Staging
Baseline assessment included triphasic contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI). The diagnosis of HCC was established according to the American Association for the Study of Liver Diseases (AASLD) criteria. Tumor staging was performed based on the American Joint Committee on Cancer (AJCC) 8th edition staging system. Liver function was assessed using the Child–Pugh classification. Laboratory evaluations included serum alpha-fetoprotein (AFP), liver function tests, renal function tests, and coagulation profiles.
Yttrium-90 TARE Procedure and Dosimetric
Planning for radioembolization followed a standardized two-stage workflow consisting of angiographic mapping and Tc-99m macroaggregated albumin (Tc-99m MAA)–based simulation. During the initial angiographic session, tumor-feeding arteries were identified and evaluated for extrahepatic arterial supply, arterioportal shunting, and lung shunt fraction. In patients with fewer than five tumors, super-selective catheterization of tumor-feeding arteries was considered the preferred strategy. However, because most patients in this cohort presented with multifocal and bilobar disease, Tc-99m MAA was typically administered from the major right, left, and segment IV hepatic arteries to achieve whole-liver coverage rather than a super-selective approach, ensuring consistency between MAA distribution and subsequent therapeutic microsphere deposition.
Tc-99m MAA single-photon emission computed tomography/computed tomography (SPECT/CT) was subsequently performed to quantify tumor-to-normal liver (T/N) uptake ratios and assess lung shunting. Given the predominance of diffuse tumor distribution, whole-liver radioembolization was adopted in the majority of cases. For dosimetric planning, T/N ratios were calculated on a lesion-by-lesion basis. The lesion demonstrating the highest T/N ratio was designated as the index tumor. The lesion with the highest T/N ratio was selected because treatment planning was based on achieving a tumor absorbed dose ≥120 Gy while maintaining the non-tumorous liver dose within established safety limits. This index-lesion approach was used to guide dosimetric calculations and treatment activity determination. In patients with tumors supplied by separate vascular territories (eg, right or left hepatic artery branches), the lesion with the highest uptake within each territory was identified, and the mean T/N ratio across territories was used for dosimetric assessment.
T/N ratios were derived from SPECT/CT by placing regions of interest (ROIs) over the tumor and adjacent normal liver parenchyma. The tumor ROI encompassed the radiotracer-avid tumor region, whereas the background liver ROI was positioned in uninvolved liver parenchyma while avoiding major vessels and imaging artifacts. The reported tumor absorbed dose corresponds to the calculated absorbed dose to the index tumor. All analyses were performed at the patient level using the T/N ratio of the index tumor.
Treatment activity was calculated using the partition model. The dosimetric objective was to deliver an absorbed dose of ≥120 Gy to the index tumor while limiting the absorbed dose to the non-tumorous liver to ≤40 Gy in cirrhotic patients and ≤70 Gy in non-cirrhotic patients, with lung dose maintained below 20 Gy. The ≥120 Gy tumor dose threshold was selected based on prior clinical and dosimetric studies using Y-90 resin microspheres that demonstrated improved tumor response and local control above this level while maintaining acceptable hepatic toxicity. This dosimetric framework was adopted to maximize tumor dose delivery in the setting of heterogeneous tumor perfusion while preserving functional liver reserve.
Yttrium-90 resin microspheres (SIR-Spheres®, Sirtex Medical, Sydney, Australia) were administered according to the catheter positions defined during MAA-based planning. To enhance predictive accuracy and minimize discrepancies between simulation and treatment, the catheter tip was positioned at the same arterial location during both Tc-99m MAA simulation and the subsequent Y-90 radioembolization procedure.
Post-Treatment Follow-Up and Response Assessment
Tumor burden was assessed using contrast-enhanced CT. Lesion size was measured as the maximum diameter of the enhancing (viable) portion of the tumor on arterial phase imaging according to modified Response Evaluation Criteria in Solid Tumors (mRECIST) principles. In patients with multifocal disease, the number of viable lesions and the sum of the largest tumor diameters were recorded. Downstaging to within University of California San Francisco (UCSF) criteria was determined based on post-treatment viable tumor burden. Patients were considered successfully downstaged if the number and size of viable tumors after TARE met UCSF criteria (a single lesion ≤6.5 cm, or up to three lesions each ≤4.5 cm with a total tumor diameter ≤8 cm). Successful downstaging was determined based on the first formal post-treatment imaging assessment performed approximately 3 months after TARE.
Clinical and laboratory follow-up was performed routinely after treatment. In our institutional practice, contrast-enhanced CT is typically performed approximately 6 weeks (1.5 months) after TARE to assess early post-treatment changes and monitor for potential complications. However, formal treatment response assessment and downstaging evaluation were based on imaging performed approximately 3 months after TARE. Patients without available contrast-enhanced CT approximately 3 months after TARE were excluded from the analysis. For the purposes of this study, the CT examination obtained closest to 3 months after treatment (within the routine 1.5–3 month follow-up window) was used for response assessment and cohort stratification according to mRECIST.
Overall survival (OS) was defined as the interval from the date of Y-90 TARE to death from any cause, and progression-free survival (PFS) was defined as the interval from TARE to radiologic progression or death, whichever occurred first.16 Patients without an event were censored at last follow-up.
Ethical Approval
This retrospective study was approved by the Institutional Review Board of the Chang Gung Medical Foundation, Kaohsiung Chang Gung Memorial Hospital (IRB No. 202501374B0). The requirement for informed consent was waived.
Statistical Analysis
Continuous variables are presented as median with interquartile range (IQR) and were compared using the Mann–Whitney U-test. Categorical variables are expressed as counts and percentages and were compared using the chi-square test or Fisher’s exact test, as appropriate.
Univariable analyses were performed to identify factors associated with failure of downstaging after Y-90 TARE. Variables with clinical relevance or p < 0.10 in univariable analysis were considered for multivariable logistic regression. Because tumor burden variables—including largest tumor diameter, tumor volume, and composite tumor number–diameter score—are highly collinear, they were not entered simultaneously into the same model. The primary multivariable model included largest tumor diameter as a continuous variable (per 1 cm increase), with albumin–bilirubin (ALBI) grade included a priori as a clinically relevant adjustment factor. To minimize overfitting, the number of predictors included in each model was limited relative to the number of observed events. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs).
Receiver operating characteristic (ROC) analysis was used to determine optimal cut-off values based on the Youden index, with area under the curve (AUC) and corresponding 95% confidence intervals reported. Sensitivity analyses were performed using the ROC-derived tumor size cut-off (≥7.8 cm). Given the retrospective single-cohort design, these thresholds should be interpreted as exploratory.
Survival outcomes were evaluated using Kaplan–Meier methods, and statistical significance was defined as a two-sided p value <0.05. All analyses were performed using SPSS software (version 27.0; SPSS Inc., Chicago, IL, USA).
Results
Patient Characteristics and Treatment Details
A total of 65 patients exceeding the University of California, San Francisco (UCSF) criteria were included in the final analysis. The cohort consisted of 49 men (75.4%) and 16 women, with a median age of 60 years. Most patients had multifocal disease (87.7%) and bilobar involvement (55.4%). The median number of tumors was 7 (interquartile range [IQR], 2–11), and the median largest tumor diameter was 5.52 cm (IQR, 2.75–8.80). Liver function was well preserved, with 96.9% of patients classified as Child–Pugh class A and 92.3% having an Eastern Cooperative Oncology Group (ECOG) performance status of 0. Portal vein tumor thrombosis was present in three patients (4.6%), all classified as VP2.
All patients received a single session of Y-90 TARE. The median tumor volume was 229 cm3 (IQR, 102.5–353.1), and the median tumor burden was 15.4% (IQR, 8.85–25.5). The median administered activity was 1.2 GBq (IQR, 0.9–1.6). Dosimetric analysis demonstrated a median tumor-absorbed dose of 143.2 Gy (IQR, 118.2–164.7), a non-tumorous liver dose of 32.1 Gy (IQR, 25.3–39.1), and a median lung shunt fraction of 4.7% (IQR, 3.6–6.1).
Downstaging Response and Survival Outcomes
Patients were reassessed three months after TARE and categorized as UCSF-fit or UCSF-unfit. Thirty-eight patients (58.5%) met the UCSF criteria, while 27 patients (41.5%) remained beyond the criteria. Downstaging to within the UCSF criteria was achieved in 38 of 65 patients (58.5%). The median follow-up duration was 24.7 months (95% confidence interval [CI], 16.7–32.7), calculated using the reverse Kaplan–Meier method to account for censoring.
For the entire cohort, the median overall survival (OS) was 35.1 months, and the median progression-free survival (PFS) was 11.0 months. Patients who achieved UCSF-fit status after TARE were associated with improved survival compared with those who did not. Median OS was not reached in the UCSF-fit group, whereas it was 18.8 months in the UCSF-unfit group (log-rank p = 0.034). Median PFS was 14.8 months versus 8.5 months, respectively (log-rank p = 0.011) (Figure 2).
 |
Figure 2 Post–Y-90 TARE UCSF-fit status is associated with significantly improved overall survival. Kaplan–Meier curves of overall survival (OS) in patients who achieved post–Y-90 TARE UCSF-fit status (yellow) compared with those who remained UCSF-unfit (green). Patients in the UCSF-fit group demonstrated significantly longer survival, with median OS not reached versus 18.8 months in the UCSF-unfit group (log-rank p = 0.034). |
In a 3-month landmark analysis performed to mitigate time-dependent bias, the survival advantage associated with post-TARE UCSF-fit status was attenuated and did not reach conventional statistical significance (log-rank p = 0.053) (Supplementary Figure 1).
Treatment response was significantly better in the UCSF-fit group, with complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) rates of 36.8%, 55.3%, 2.6%, and 5.3%, respectively. The CR rate, objective response rate, and disease control rate were all significantly higher in the UCSF-fit group (p = 0.001, 0.002, and 0.022, respectively).
Among surgically managed patients, 10 underwent living donor liver transplantation (LDLT), with median OS not reached and 100% survival at last follow-up, and 8 underwent surgical resection with a median OS of 39.9 months. Surgical patients had significantly superior outcomes compared with nonsurgical patients, with a mean OS of 61.7 versus 23.5 months. Median OS and PFS were not reached in the surgical group, whereas they were 14.4 months and 8.5 months, respectively, in the nonsurgical group (log-rank p = 0.001 and 0.032). Among nonsurgical patients, no significant differences in OS or PFS were observed between UCSF-fit and UCSF-unfit subgroups (Table 1). To account for the potential impact of subsequent curative surgery, a sensitivity analysis excluding patients who underwent surgical resection or living donor liver transplantation was performed. In this analysis, overall survival did not differ significantly between the UCSF-fit and UCSF-unfit groups (log-rank p = 0.689).
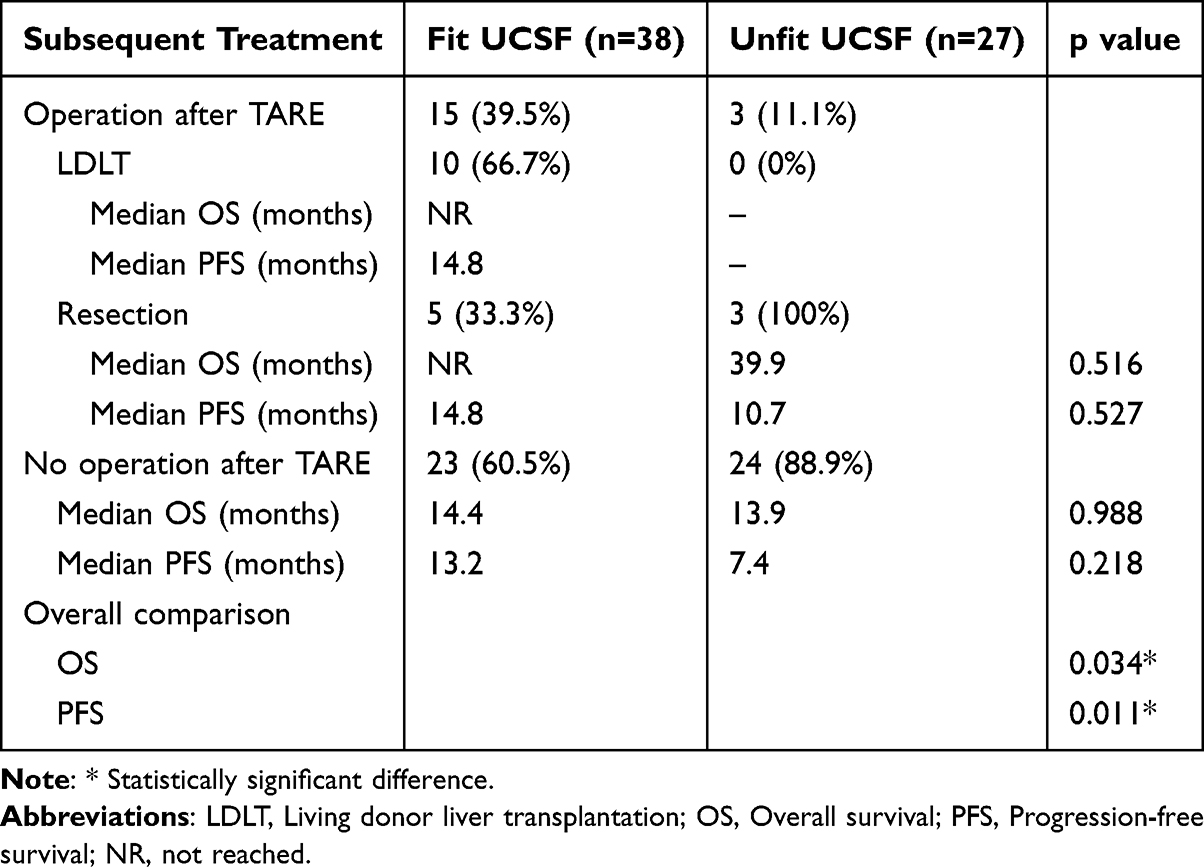 |
Table 1 Overall Survival and Progression-Free Survival Were Recorded and Compared Across Subsequent Treatments |
Predictors of Successful Downstaging
Baseline demographic, clinical, and tumor characteristics were comparable between the two groups. Significant differences between downstaged and non-downstaged patients were identified in largest tumor diameter (OR, 1.22; 95% CI, 1.05–1.41; p = 0.009), tumor volume (OR, 1.004; 95% CI, 1.001–1.007; p = 0.018), tumor burden, Up-to-11 score (OR, 3.96; 95% CI, 1.24–12.65; p = 0.017), and Tumor Burden Score (TBS) grade. Notably, there were no significant differences between the two groups regarding tumor number, tumor location, hepatic vein invasion, portal vein invasion, Albumin-Bilirubin (ALBI) grade, GOT, GPT, albumin, total bilirubin, alpha-fetoprotein (AFP), PIVKA-II, CEA, CA19-9, tumor-to-normal tissue (T/N) ratio, administered total activity, tumor absorbed dose, non-tumor absorbed dose, lung shunting, or lung dose (Table 2).
 |
Table 2 Potential Influencing Factors of Patients’ Tumor Characteristics and Radioembolization Details Based on Post-Y90 Fit or Unfit UCSF Criteria |
In multivariable logistic regression analysis, larger tumor size remained independently associated with failure of downstaging after Y-90 radioembolization (OR per cm increase, 1.21; 95% CI, 1.04–1.41; p = 0.011), after adjustment for liver function as assessed by ALBI grade (Table 3). In sensitivity analysis, when tumor size was dichotomized using the ROC-derived cut-off of 7.8 cm, tumor size ≥ 7.8 cm remained independently associated with failure of downstaging (OR, 4.53; 95% CI, 1.50–13.66; p = 0.007), after adjustment for ALBI grade (Supplementary Table 1).
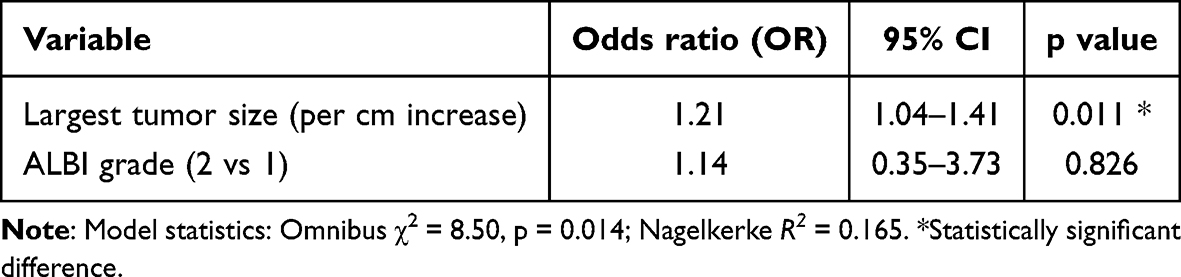 |
Table 3 Multivariable Logistic Regression Analysis for Predictors of Failure of Downstaging After Y-90 TARE |
Receiver operating characteristic (ROC) analysis identified optimal cut-offs associated with successful downstaging: largest tumor diameter 7.8 cm (AUC 0.687, 95% CI 0.556–0.818; p = 0.011), tumor volume 265 cm3 (AUC 0.716, 95% CI 0.588–0.844; p = 0.003), and a composite metric of tumor number plus largest diameter >11 (AUC 0.668, 95% CI 0.535–0.800; p = 0.022) (Figure 3). These thresholds should be interpreted as exploratory given the retrospective single-cohort design.
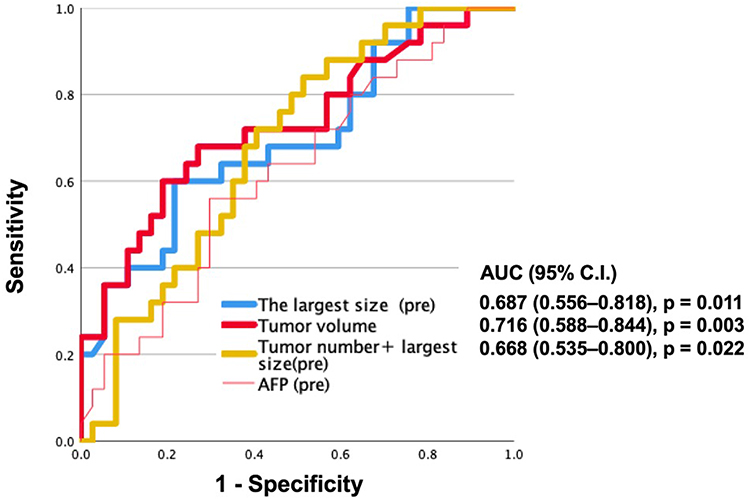 |
Figure 3 Receiver operating characteristic (ROC) curves evaluating pretreatment tumor burden metrics for predicting successful downstaging to within UCSF criteria after Y-90 TARE. The largest tumor diameter (blue), tumor volume (red), and a composite metric combining tumor number and largest tumor diameter (yellow) demonstrated areas under the curve (AUCs) of 0.687 (95% CI, 0.556–0.818; p = 0.011), 0.716 (95% CI, 0.588–0.844; p = 0.003), and 0.668 (95% CI, 0.535–0.800; p = 0.022), respectively. Alpha-fetoprotein (AFP) showed inferior discriminatory performance. |
Individually, a largest tumor diameter ≥ 7.8 cm and tumor volume ≥ 265 demonstrated moderate sensitivity (both 55.6%) with relatively high specificity (78.9% and 81.6%, respectively), whereas the combined criterion of tumor number plus largest diameter ≥ 11 showed higher sensitivity (81.5%) but lower specificity (47.4%). When composite criteria were applied, the sensitivity for predicting treatment failure increased progressively. In particular, the presence of any one of the three criteria (A, B, or C) yielded the highest sensitivity (96.3%) and negative predictive value (93.8%), indicating a very low likelihood of treatment failure when none of these tumor burden thresholds were met (Table 4). To further evaluate the potential interaction between tumor size and tumor number, an interaction term was incorporated into the logistic regression model; however, no significant interaction effect was identified. Detailed results are provided in Supplementary Table 2.
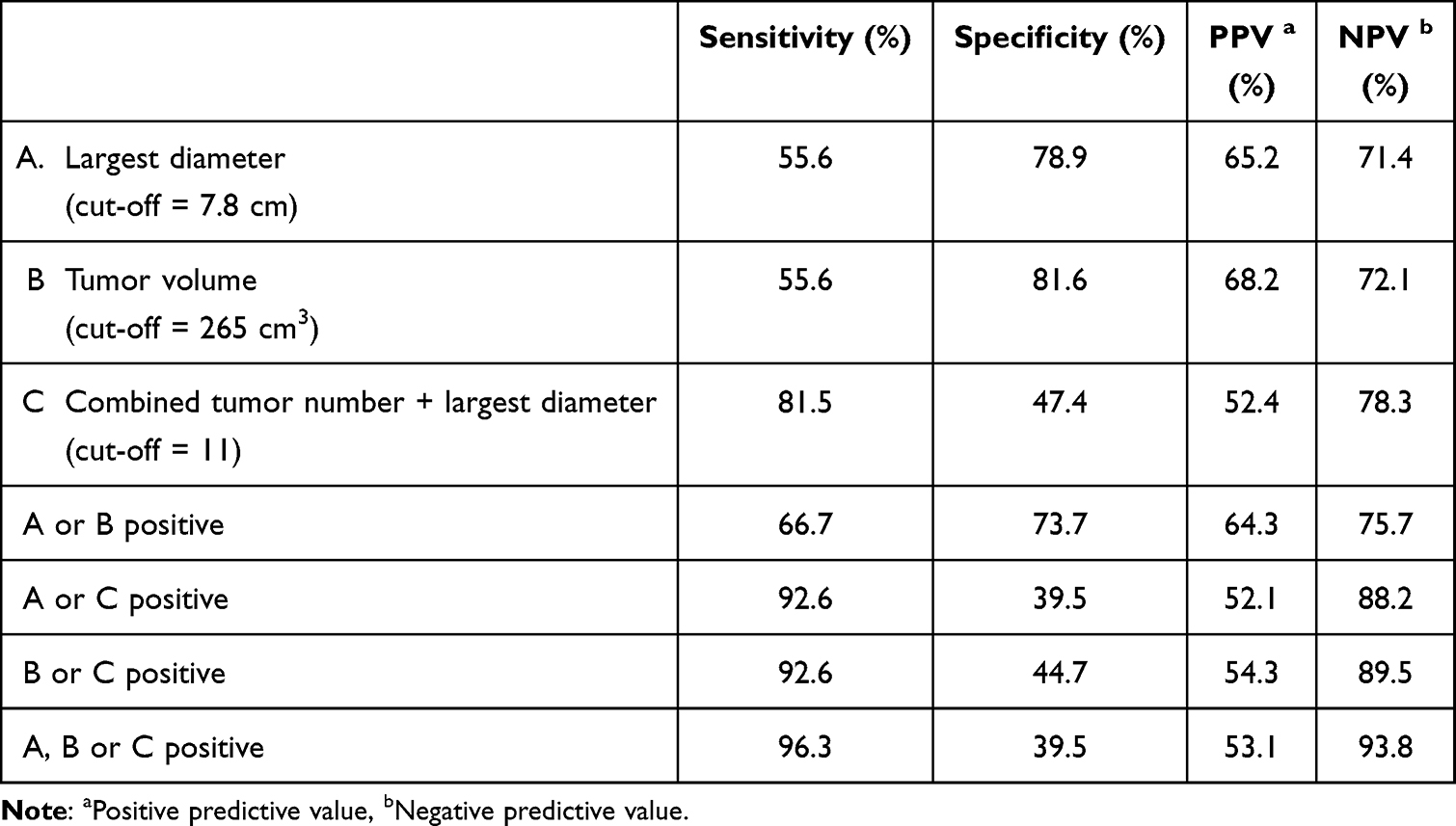 |
Table 4 The Diagnostic Performance of Tumor Burden Parameters for Predicting Successful Downstaging to Within UCSF Criteria After Y-90 TARE |
Tumor-to-Normal Uptake Ratio and Safety Outcomes
Although the overall tumor-to-normal uptake (T/N) ratio did not differ significantly between downstaged and non-downstaged patients, stratified analysis demonstrated that a T/N ratio >4 was significantly associated with successful downstaging to within UCSF criteria in tumors <7.8 cm (p = 0.031) (Table 5 and Figure 4). Treatment was generally well tolerated. With a dosimetric strategy designed to limit radiation exposure to non-tumorous liver parenchyma, no grade 3 or higher ALBI deterioration was observed. One patient (1.5%) developed grade 3 radiation pneumonitis, and no cases of radiation-induced liver disease occurred.
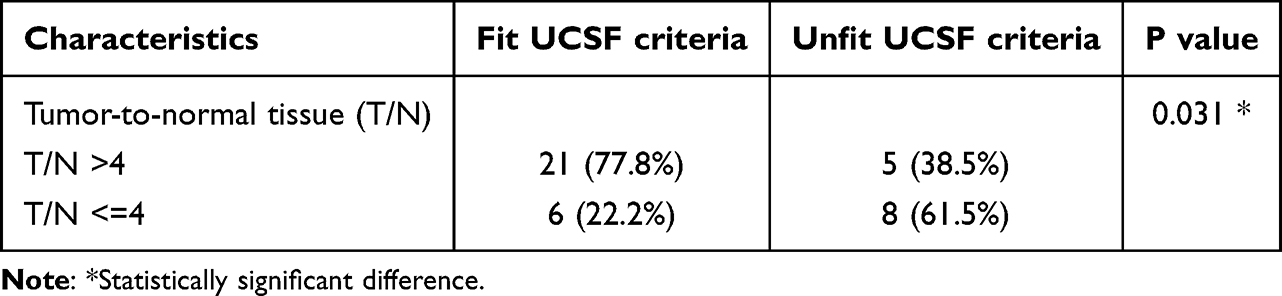 |
Table 5 Association Between T/N Ratio and Successful Downstaging Among Patients with Largest Tumor Diameter ≤7.8 cm |
 |
Figure 4 Representative case illustrating size-related heterogeneity of Y-90 distribution and treatment response. (a) Baseline contrast-enhanced CT shows a large, poorly defined hepatocellular carcinoma in the right hepatic lobe. (b) Tc-99m MAA SPECT/CT demonstrates heterogeneous intratumoral uptake, indicating uneven microsphere distribution. (c) Follow-up CT at 3 months after Y-90 TARE reveals residual viable tumor and a newly developed enhancing lesion (circled), consistent with incomplete tumor coverage and disease progression. |
Discussion
This study demonstrates that Y-90 transarterial radioembolization can achieve meaningful downstaging in patients with hepatocellular carcinoma who initially exceed the UCSF transplantation criteria. More than half of the cohort achieved successful downstaging. Patients who were successfully downstaged were more likely to proceed to curative treatments. Nevertheless, improved survival was largely observed in patients who subsequently underwent resection or LDLT. These findings are consistent with prior reports suggesting that TARE can serve as an effective downstaging strategy for patients beyond conventional transplant criteria. Collectively, our results highlight the potential role of successful TARE downstaging as a pathway to curative therapies for carefully selected patients with advanced HCC.
Our findings are consistent with emerging evidence, including emerging prospective data, showing that TARE provides superior tumor control and delays progression compared with other locoregional therapies.15 Yet, clinically meaningful predictors of successful downstaging remain incompletely defined, largely due to heterogeneous patient selection and inconsistent reporting across studies. Despite the predominance of multifocal and bilobar HCC in our cohort—features typically associated with limited transplant eligibility—a substantial proportion of patients achieved successful downstaging. These observations suggest that, in carefully selected patients, the downstaging potential of TARE may extend beyond conventional expectations.
After Y-90 TARE, a considerable proportion of patients proceeded to surgery—most commonly living-donor liver transplantation—highlighting its role as an effective bridge to curative therapy. Surgically treated patients demonstrated markedly superior survival, underscoring the clinical relevance of successful downstaging. However, sensitivity analysis excluding surgical patients showed no significant survival difference between UCSF-fit and UCSF-unfit groups, suggesting that the survival advantage observed in the overall cohort may largely reflect access to curative surgery rather than downstaging status alone. In addition, we identified three tumor burden parameters—the largest tumor diameter, total tumor volume, and a combined tumor number–diameter score—as practical predictors of downstaging success that may help refine candidate selection within transplant-oriented treatment strategies.
Under preserved liver function, tumor burden emerged as a key determinant of downstaging success in our cohort, consistent with and extending prior evidence linking baseline tumor characteristics to transplant eligibility. The “up-to-seven” rule proposed by Mazzaferro et al established a composite metric of tumor size and number as a prognostic benchmark for transplantation, and subsequent analyses have confirmed that larger tumor burden reduces the likelihood of successful downstaging.4,17,18 Our findings align with this paradigm: larger tumor size, increased tumor volume, and a greater combined tumor number and size were each associated with an elevated risk of treatment failure following Y-90 radioembolization.
Through ROC analysis, we identified several tumor burden thresholds associated with successful downstaging, including a largest tumor diameter of 7.8 cm, tumor volume of 265 cm3, and a composite tumor number–diameter score greater than 11. Notably, this composite threshold exceeds the traditional “up-to-seven” criterion, suggesting that Y-90 TARE may enable downstaging beyond conventional size–number limits in selected patients. However, given the retrospective nature of this study and the single-cohort design, these thresholds should be interpreted as exploratory and hypothesis-generating. No internal or external validation was performed, and therefore these cutoffs should not be considered definitive clinical thresholds. Furthermore, the presence of multiple adverse tumor burden factors was associated with a lower likelihood of successful downstaging, highlighting the potential value of integrating volumetric metrics and composite burden indices into patient selection.
Importantly, the combined use of these parameters demonstrated a strong rule-out capability. Patients who did not meet any of the three predefined criteria (largest diameter, tumor volume, or combined tumor number and size) showed a high probability of treatment success, reflected by a negative predictive value of 93.8%. Conversely, fulfillment of one or more criteria was associated with an increased likelihood of downstaging failure. Taken together, these findings support a more nuanced and comprehensive approach to identifying candidates for TARE and suggest that carefully selected patients with substantial tumor burden may still achieve successful downstaging and subsequently become eligible for curative transplantation.
Recent studies have emphasized the importance of adequate tumor dose for treatment response. Although the overall tumor-to-normal uptake (T/N) ratio was not significantly associated with downstaging in our cohort, its predictive value in tumors smaller than 7.8 cm suggests that microsphere distribution may remain relevant in selected patients. Prior studies have shown that microsphere deposition correlates with therapeutic efficacy;19,20 however, this relationship progressively deteriorates with increasing tumor size, as size itself becomes the dominant constraint. In tumors exceeding 7.8 cm, heterogeneous arterial supply and intratumoral complexity frequently result in uneven Y-90 distribution and the formation of underdosed regions (“cold spots”), even in the presence of a favorable T/N ratio.18–22 These cold spots likely serve as reservoirs for viable tumor cells and represent a critical driver of treatment failure and early recurrence, thereby fundamentally limiting the interpretability and prognostic utility of this global, averaged dosimetric metric. In contrast, while a high T/N ratio has been shown to remain essential in the setting of multifocal small HCCs —where individual tumor dose is low and normal liver tolerance is dose-limiting—treatment success in large HCCs appears to be governed primarily by the feasibility of achieving adequate volumetric dose coverage rather than preferential uptake alone. Collectively, these findings suggest that tumor size and uptake-based parameters should be interpreted together when evaluating candidates for TARE-based downstaging. Further studies are needed to validate these observations and clarify their clinical utility.
In conclusion, Y-90 TARE offers meaningful downstaging potential for advanced HCC, allowing a substantial proportion of patients to become eligible for resection or transplantation. The identified tumor burden metrics and T/N ratio findings should be considered exploratory and may assist patient selection for future validation studies.
The study has several limitations. First, its retrospective design and relatively small sample size limit the generalizability of the findings. Second, imaging follow-up intervals were not completely uniform, and dosimetric estimates may vary across operators. In addition, detailed information regarding locoregional or systemic therapies before referral for Y-90 TARE was not consistently available because of the retrospective nature of the study and referral patterns, and therefore could not be included in the analysis. Because T/N ratio analysis was based on the index lesion with the highest uptake, it may not fully capture intrapatient heterogeneity in patients with multifocal or bilobar disease. Third, reliance on pre-therapy MAA SPECT/CT without verification using post-therapy Y-90 PET/CT or Bremsstrahlung SPECT which may be significant difference critical to interpreting T/N effects and threshold behaviors. Fourth, downstaging status is determined after treatment initiation, and unadjusted survival comparisons may be influenced by time-dependent bias. The observed survival differences should therefore be interpreted cautiously, as post-treatment UCSF status is a time-dependent variable and survival outcomes were likely influenced by subsequent surgical conversion. However, the overall survival difference remained directionally consistent in a 3-month landmark analysis, although statistical significance was attenuated, likely reflecting reduced power after landmark restriction. Fifth, the ROC-derived cut-offs were not internally validated using resampling techniques, and the observed AUCs were modest, suggesting that these thresholds should be interpreted as clinically pragmatic rather than definitive predictors. Furthermore, 25 patients (38.5%) in the present cohort overlapped with a previously published institutional Y-90 radioembolization study. However, the previous report focused on overall treatment outcomes, whereas the current analysis addressed a distinct research objective involving downstaging beyond UCSF criteria. Nevertheless, the study provides exploratory thresholds that may help generate hypotheses and guide future validation studies in TARE-based downstaging.
Conclusions
Yttrium-90 transarterial radioembolization provides meaningful downstaging potential for selected patients with hepatocellular carcinoma initially beyond the UCSF criteria. More than half of the patients were successfully downstaged, increasing eligibility for curative therapies. Successful downstaging was associated with improved survival, particularly among patients who subsequently underwent resection or living donor liver transplantation. Tumor burden parameters, including largest tumor diameter, tumor volume, and combined tumor number–diameter score, may help identify candidates most likely to benefit from treatment. These findings suggest exploratory tumor burden thresholds that may assist patient selection for Y-90 TARE and support its role in expanding surgical and transplant opportunities in advanced HCC.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Chang Gung Medical Foundation, Kaohsiung Chang Gung Memorial Hospital (protocol code: 202501374B0). The requirement for informed consent was waived due to the retrospective nature of the study.
All living donor liver transplantations were performed with voluntary written informed consent obtained from both donors and recipients and were conducted in accordance with the principles of the Declaration of Istanbul.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to Institutional Review Board regulations and patient confidentiality but are available from the corresponding author (Yu-Fan Cheng) upon reasonable request and with approval from the Institutional Review Board.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study and the use of anonymized clinical data, as approved by the Institutional Review Board.
Acknowledgments
We thank Hsin-Yi Chien, Chih-Yun Lin, and the Biostatistics Center of Kaohsiung Chang Gung Memorial Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Grant CMRPG8Q0901 from the Chang Gung Memorial Hospital, R.O.C. This work was also supported by Grant NSTC 113-2314-B-182A-080 and 114-2314-B-182A-015 from the National Science and Technology Council, R.O.C.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu W, Rao Q, An Y, Li M, Zhang Z. Identification of biomarkers for Barcelona clinic liver cancer staging and overall survival of patients with hepatocellular carcinoma. PLoS One. 2018;13(8):e0202763. doi:10.1371/journal.pone.0202763
2. Kudo M, Oanh BT, Chen CJ, et al. Roadmap for HCC surveillance and management in the Asia Pacific. Cancers. 2025;17(12):1928. doi:10.3390/cancers17121928
3. Kim E, Viatour P. Hepatocellular carcinoma: old friends and new tricks. Exp Mol Med. 2020;52(12):1898–14. doi:10.1038/s12276-020-00527-1
4. Frankul L, Frenette C. Hepatocellular carcinoma: downstaging to liver transplantation as curative therapy. J Clin Transl Hepatol. 2021;9(2):220–226. doi:10.14218/JCTH.2020.00037
5. European Association for the Study of the L. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
6. Toso C, Mentha G, Kneteman NM, Majno P. The place of downstaging for hepatocellular carcinoma. J Hepatol. 2010;52(6):930–936. doi:10.1016/j.jhep.2009.12.032
7. Tan DJH, Lim WH, Yong JN, et al. UNOS down-staging criteria for liver transplantation of hepatocellular carcinoma: systematic review and meta-analysis of 25 studies. Clin Gastroenterol Hepatol. 2023;21(6):1475–1484. doi:10.1016/j.cgh.2022.02.018
8. Salem R, Gordon AC, Mouli S, et al. Y90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2016;151(6):1155–1163e2. doi:10.1053/j.gastro.2016.08.029
9. Salem R, Gabr A, Riaz A, et al. Institutional decision to adopt Y90 as primary treatment for hepatocellular carcinoma informed by a 1000-patient 15-year experience. Hepatology. 2018;68(4):1429–1440. doi:10.1002/hep.29691
10. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
11. Zori AG, Ismael MN, Limaye AR, et al. Locoregional therapy protocols with and without radioembolization for hepatocellular carcinoma as bridge to liver transplantation. Am J Clin Oncol. 2020;43(5):325–333. doi:10.1097/COC.0000000000000678
12. Yu CY, Huang PH, Tsang LL, et al. Yttrium-90 radioembolization as the major treatment of hepatocellular carcinoma. J Hepatocell Carcinoma. 2023;10:17–26. doi:10.2147/JHC.S385478
13. Whitlock RS, Loo C, Patel K, et al. Transarterial radioembolization treatment as a bridge to surgical resection in pediatric hepatocellular carcinoma. J Pediatr Hematol Oncol. 2021;43(8):e1181–e1185. doi:10.1097/MPH.0000000000002089
14. Villalobos A, Wagstaff W, Guo M, et al. Predictors of successful yttrium-90 radioembolization bridging or downstaging in patients with hepatocellular carcinoma. Can J Gastroenterol Hepatol. 2021;2021:9926704. doi:10.1155/2021/9926704
15. Tabone M, Calvo A, Russolillo N, et al. Downstaging unresectable hepatocellular carcinoma by radioembolization using 90-yttrium resin microspheres: a single center experience. J Gastrointest Oncol. 2020;11(1):84–90. doi:10.21037/jgo.2019.06.01
16. Baloji A, Kalra N, Chaluvashetty S, et al. Efficacy of Yttrium-90 transarterial radioembolisation in advanced hepatocellular carcinoma: an experience with hybrid angio-computed tomography and glass microspheres. J Clin Exp Hepatol. 2024;14(3):101342. doi:10.1016/j.jceh.2023.101342
17. Bonne L, Deroose CM, Verslype C, et al. Resin-based yttrium-90 radioembolization as a bridging or downstaging treatment to liver transplantation for hepatocellular carcinoma. J Vasc Interv Radiol. 2025;36(2):282–292. doi:10.1016/j.jvir.2024.10.021
18. Mazzaferro V, Sposito C, Bhoori S, et al. Yttrium-90 radioembolization for intermediate-advanced hepatocellular carcinoma: a Phase 2 study. Hepatology. 2013;57(5):1826–1837. doi:10.1002/hep.26014
19. Garin E, Palard X, Rolland Y. Personalised dosimetry in radioembolisation for HCC: impact on clinical outcome and on trial design. Cancers. 2020;12(6):1557. doi:10.3390/cancers12061557
20. Gabr A, Riaz A, Johnson GE, et al. Correlation of Y90-absorbed radiation dose to pathological necrosis in hepatocellular carcinoma: confirmatory multicenter analysis in 45 explants. Eur J Nucl Med Mol Imaging. 2021;48(2):580–583. doi:10.1007/s00259-020-04976-8
21. Willowson KP, Tapner M, Team QI, Bailey DL. A multicentre comparison of quantitative (90)Y PET/CT for dosimetric purposes after radioembolization with resin microspheres: the QUEST Phantom Study. Eur J Nucl Med Mol Imaging. 2015;42(8):1202–1222. doi:10.1007/s00259-015-3059-9
22. Sangro B, Salem R, Kennedy A, Coldwell D, Wasan H. Radioembolization for hepatocellular carcinoma: a review of the evidence and treatment recommendations. Am J Clin Oncol. 2011;34(4):422–431. doi:10.1097/COC.0b013e3181df0a50
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Low MARCO Expression is Associated with Poor Survival in Patients with Hepatocellular Carcinoma Following Liver Transplantation
Zhang Q, Wei Y, Li Y, Jiao X
Cancer Management and Research 2022, 14:1935-1944
Published Date: 11 June 2022
Delayed Hepatocellular Carcinoma Recurrence After Liver Transplantation: Comprehensive Clinical Characterization of Case Series
Wong TH, Ho CM, Hsu HH, Wu YM, Ho MC, Lee PH, Hu RH
Journal of Hepatocellular Carcinoma 2022, 9:1081-1091
Published Date: 17 October 2022
Development of a Nomogram Model to Predict Post-Transplant Tumor Recurrence in Patients with Hepatocellular Carcinoma Beyond the Milan Criteria Undergoing TACE Bridging Therapy
Wang H, Liu E, Wu M, Gao H, Lv B, Chen G, Zeng X
Journal of Hepatocellular Carcinoma 2026, 13:570962
Published Date: 17 February 2026
The Fibrinogen-to-Albumin Ratio (FAR) Predicts Prognosis in Hepatocellular Carcinoma Patients After Liver Transplantation: Development and Validation of a Novel Nomogram
Ye XY, Leng AX, He Q, Ji Z, Ma J
Journal of Hepatocellular Carcinoma 2026, 13:588619
Published Date: 8 April 2026
Liver Transplantation After Radiotherapy-Antiangiogenesis-Immune Checkpoint Blockade Combination Therapy in Hepatocellular Carcinoma with Major Portal Vein Tumor Thrombosis: A Propensity Score Matching Analysis
Zhao Y, Song J, Li K, Li T, Li W, Yang Y, Tong X, Xiao Y, Xu G, Lu Q, Li G, Li G, Dong J
Journal of Hepatocellular Carcinoma 2026, 13:570163
Published Date: 8 May 2026