Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Development of a Nomogram Model to Predict Post-Transplant Tumor Recurrence in Patients with Hepatocellular Carcinoma Beyond the Milan Criteria Undergoing TACE Bridging Therapy
Authors Wang H, Liu E, Wu M, Gao H, Lv B, Chen G, Zeng X
Received 28 September 2025
Accepted for publication 16 January 2026
Published 17 February 2026 Volume 2026:13 570962
DOI https://doi.org/10.2147/JHC.S570962
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mohamed Shaker
Hao Wang, Encheng Liu, Mei Wu, Haijun Gao, Bing Lv, Guang Chen, Xunjin Zeng
Department of Radiology, Tianjin First Central Hospital, Tianjin, 300384, People’s Republic of China
Correspondence: Guang Chen, Department of Radiology, Tianjin First Central Hospital, No. 24, Fukang Road, Nankai District, Tianjin, 300384, People’s Republic of China, Email [email protected] Xunjin Zeng, Department of Radiology, Tianjin First Central Hospital, No. 24, Fukang Road, Nankai District, Tianjin, 300384, People’s Republic of China, Email [email protected]
Objective: To develop a nomogram based on clinical characteristics for predicting post-transplant tumor recurrence in hepatocellular carcinoma (HCC) patients beyond the Milan criteria who received transarterial chemoembolization (TACE) bridging therapy.
Methods: A retrospective analysis included 73 such patients (29 conventional TACE [cTACE], 44 drug-eluting bead TACE [DEB-TACE]) who underwent liver transplantation at our institution between January 2013 and January 2020, with follow-up until January 2024 (mean: 33.2 ± 6.5 months). Clinical/pathological features were analyzed via univariate and multivariate Cox regression to identify recurrence-related factors, and a nomogram was constructed. Bootstrap validation (B=20) and receiver operating characteristic (ROC) curves (AUC) evaluated its performance.
Results: The 1-, 2-, 3-year cumulative recurrence rates were 17.8%, 23.3%, 24.7% (median recurrence time: 6 months). cTACE group rates (20.7%, 27.6%, 31.0%) were higher than DEB-TACE (15.9%, 20.5%, 20.5%; P=0.034). Independent risk factors: bridging therapy type (HR=2.402, P=0.034), microvascular invasion (HR=3.445, P=0.001), tumor necrosis rate (HR=26.664, P=0.002), pre-TACE AFP (HR=2.750, P=0.004). The nomogram’s AUC for 1-, 2-, 3-year recurrence was 0.740, 0.764, 0.886, with good calibration via bootstrap.
Conclusion: A nomogram based on clinical characteristics accurately predicts post-transplant recurrence in HCC patients beyond the Milan criteria with TACE bridging therapy, providing guidance for optimizing donor allocation.
Keywords: hepatocellular carcinoma, liver transplantation, drug-eluting beads, tumor recurrence
Introduction
Bridging therapy with transarterial chemoembolization (TACE) can reduce recurrence rates and improve survival in patients with hepatocellular carcinoma (HCC) beyond the Milan criteria. However, due to the heterogeneity in tumor biology and liver function among individuals, treatment outcomes may vary, and recurrence rates have been reported to remain as high as 12–30%.1,2 One study found that only 22% of patients with post-transplant recurrence survived beyond 5 years.3 Most recurrences occur within the first 3 years after liver transplantation.4 Therefore, accurate prediction of post-transplant recurrence risk could assist clinicians in optimizing donor allocation strategies.
Tumor biology is considered the fundamental determinant of recurrence. Although pathological biopsy may provide information on tumor biology, pre-transplant biopsy of HCC carries risks such as bleeding and needle tract seeding, making its clinical application controversial.5 Currently, most prediction models for post-transplant HCC recurrence are limited in two key ways: they are primarily based on Western populations (with distinct tumor biology, lower hepatitis B virus-related HCC prevalence, and treatment patterns)6,7 and rarely incorporate TACE bridging therapy—let alone directly compare drug-eluting bead TACE (DEB-TACE) and conventional TACE (cTACE), a critical distinction given DEB-TACE’s growing use as a bridging strategy in China.8,9 This leaves a gap in prognostic tools for Chinese patients with HCC beyond the Milan criteria (a large subgroup in China’s liver transplant cohort, accounting for nearly 65% of HCC transplant recipients) who receive TACE bridging therapy. Hence, the establishment of a patient-tailored prognostic model—one that integrates DEB-TACE vs cTACE outcomes and focuses on this understudied population—is of great clinical significance. While a nomogram itself is a visual tool for presenting multivariate models,10,11 its value here lies in translating the cohort-specific prognostic factors into an intuitive tool for clinical use; crucially, no prior work has developed such a prognostic model (or its nomogram visualization) for post-transplant recurrence in this specific patient group.
In the current study, we addressed this unmet need through a retrospective analysis of 73 Chinese patients with HCC beyond the Milan criteria who received TACE (either DEB-TACE or cTACE) bridging therapy before liver transplantation. We first identified independent prognostic factors for post-transplant tumor recurrence via univariate and multivariate Cox regression analyses, then constructed a nomogram based on these factors to predict 1-, 2-, and 3-year post-transplant recurrence risk, and validated the nomogram’s performance using bootstrap resampling. This work not only compares DEB-TACE and cTACE outcomes in this high-priority cohort but also provides a practical, cohort-specific tool, to guide clinical decision-making in donor allocation (critical amid scarce liver grafts in China) and post-transplant management (tailored follow-up or intervention strategies), ultimately improving personalized care for this understudied patient population.
Materials and Methods
Study Population
A retrospective analysis was conducted on 73 patients with hepatocellular carcinoma (HCC) beyond the Milan criteria who underwent TACE bridging therapy prior to liver transplantation at our center between January 2013 and December 2020 (revised to ensure adequate follow-up duration). All patients were followed up until December 2023 (the latest follow-up cutoff to align with enrollment timelines), with a mean follow-up time of 33.2 ± 6.5 months (range: 10–36 months). The detailed patient selection process is illustrated in Supplementary Figure 1. Among them, 29 patients received conventional TACE (cTACE) bridging therapy and 44 patients received drug-eluting bead TACE (DEB-TACE) bridging therapy. The 1-, 2-, and 3-year cumulative recurrence rates were compared between the two groups. The study was approved by the Institutional Ethics Committee of Tianjin First Central Hospital (approval number: 2015014F). Informed consent was waived because this was a retrospective observational study involving the analysis of existing medical records and no additional invasive procedures or interventions were performed on patients. All patient data were de-identified prior to analysis, with personal identifiers (such as name, medical record number, and contact information) removed or encrypted to ensure strict confidentiality. The handling of patient information strictly adhered to the requirements of the Declaration of Helsinki and relevant national data protection regulations, and no potential risks to patients were incurred. The inclusion and exclusion criteria, as well as TACE procedures, were consistent with those described in the first section.
The selection of cTACE vs DEB-TACE was determined by a multidisciplinary team (MDT) based on institutional protocols and individual patient characteristics, including tumor vascularity (hypervascular vs hypovascular), tumor size (≤5 cm vs >5 cm), liver function reserve (Child-Pugh class A/B), and patient preferences after informed consent. No randomization was performed, as this was a retrospective observational study reflecting real-world clinical practice.
All liver grafts in this study were obtained via voluntary donation-written informed consent was provided by deceased donors’ legal representatives (or pre-deceased donors), with no coercion or commercial transactions. All donation procedures strictly adhered to the Declaration of Istanbul (2008, updated 2018) and China’s Regulations on Human Organ Transplantation, overseen by the hospital’s transplant ethics committee.
TACE Procedure Details
All TACE procedures were performed by experienced interventional radiologists (with >10 years of HCC interventional therapy experience) under digital subtraction angiography (DSA) guidance.
cTACE regimen: Chemotherapy drugs included doxorubicin (50–60 mg/m2) + cisplatin (60–80 mg/m2), mixed with Lipiodol (10–20 mL, depending on tumor volume) as the embolization agent. The mixture was injected superselectively into the tumor-feeding artery until stasis of blood flow was observed. Additional gelatin sponges (1–3 mm particles) were used for supplementary embolization if necessary.
DEB-TACE regimen: Drug-eluting beads (DC Beads, Biocompatibles UK Ltd.) with a diameter of 70–150 µm or 100–300 µm were loaded with doxorubicin (30–50 mg per procedure) according to the manufacturer’s protocol. After superselective catheterization of the tumor-feeding artery, the drug-loaded beads were injected sequentially until complete occlusion of the tumor vasculature was confirmed by DSA. No additional Lipiodol or gelatin sponges were used in DEB-TACE.
All patients underwent contrast-enhanced CT/MRI 4–6 weeks after each TACE session to assess tumor response (per mRECIST criteria) and determine the need for repeat TACE. The median number of TACE sessions was 2 (range: 1–4) in both groups.
Among the 73 patients, 29 received cTACE bridging therapy and 44 received DEB-TACE bridging therapy. The 1-, 2-, and 3-year cumulative recurrence rates were compared between the two groups (Figure 1).
 |
Figure 1 Recurrence curves of Group A and Group B. Abbreviations: cTACE, conventional transarterial chemoembolization; DEB-TACE, drug-eluting beads transarterial chemoembolization. Notes: Group A represents patients who received cTACE bridging therapy; Group B represents patients who received DEB-TACE bridging therapy. |
Univariate and Multivariate Cox Regression Analyses of Factors Associated with Recurrence and Establishment of the Nomogram Model
Univariate and multivariate Cox regression analyses of factors associated with recurrence and establishment of the nomogram model: Univariate Cox regression analysis was performed to identify clinical and pathological characteristics associated with post-transplant HCC recurrence among patients with HCC beyond the Milan criteria who underwent TACE bridging therapy. The variables included, with their explicit collection timepoints specified: demographic factors (sex, age, collected at initial hospital admission for TACE); pre-TACE clinical parameters (collected within 3 days before the first TACE session: preoperative AFP [≤400 ng/mL vs >400 ng/mL], MELD score [≤20 vs >20], underlying liver disease [hepatitis vs non-hepatitis], Child-Pugh classification, tumor vascularity [hypervascular vs hypovascular, assessed via contrast-enhanced CT/MRI], maximum tumor diameter [≤5 cm vs >5 cm], tumor distribution [unilobar vs bilobar], tumor number [single vs multiple]); pre-transplant pathological/pseudo-pathological parameters (assessed within 1 week before liver transplantation, or via postoperative pathological examination of the explanted liver: pathological grade [well, moderate, or poorly differentiated], presence of satellite nodules [yes/no], capsule [yes/no], microvascular invasion [no/yes], tumor necrosis rate [≥50% vs <50%, calculated based on contrast-enhanced imaging [pre-transplant] or pathological sections [post-transplant], with pathological results prioritized when available]); and treatment-related factor (bridging therapy type [DEB-TACE vs cTACE, determined by the actual TACE regimen administered]). Variables with significant differences in univariate analysis were further evaluated by multivariate Cox regression to identify independent risk factors for recurrence. A predictive model was then constructed based on these independent risk factors, and a nomogram was generated using R software.
Vascularity (hypervascular vs hypovascular): Assessed via contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI) performed within 3 days before the first TACE session, using the Liver Imaging Reporting and Data System (LI-RADS) v2018 criteria. A tumor was classified as hypervascular if it showed obvious arterial-phase enhancement (greater than the surrounding normal liver parenchyma) followed by washout in the portal venous or delayed phase; hypovascular tumors were defined as those with no arterial-phase enhancement or enhancement equal to or less than the normal liver parenchyma, with no subsequent washout.12,13
Satellite nodules (yes/no): Distinguished from multifocal tumors based on spatial relationship and imaging features, per the American Association for the Study of Liver Diseases (AASLD) guidelines. Satellite nodules were defined as small (≤2 cm in maximum diameter) HCC lesions located within 2 cm of the main tumor, with identical imaging characteristics (arterial enhancement, washout) to the main tumor and no independent blood supply on angiography. In contrast, multifocal tumors were lesions >2 cm in diameter or located >2 cm from the main tumor, with distinct arterial blood supply confirmed by DSA during TACE.14,15
Tumor necrosis rate (≥50% vs <50%): Prioritized for pathological assessment using the explanted liver specimen; when pathological data were unavailable (n=3, due to incomplete tumor sampling), imaging-based assessment via contrast-enhanced CT/MRI (post-last TACE, within 1 week before transplantation) was used as a substitute. For pathological assessment, the explanted liver was sectioned at 5-mm intervals through the entire tumor and its surrounding 2 cm of liver parenchyma (whole-tumor sectioning protocol). Each section was stained with hematoxylin-eosin (HE), and tumor necrosis was defined as areas of eosinophilic, acellular debris with no viable tumor cells. The necrosis rate was calculated as the ratio of necrotic tumor area to total tumor area (measured using ImageJ software v1.8.0) across all sections, averaged from three independent pathological evaluations (by two senior pathologists and one hepatobiliary radiologist, with consensus reached for any discrepancies). For imaging-based assessment, necrosis rate was estimated using the modified Response Evaluation Criteria in Solid Tumors (mRECIST), where non-enhancing areas in the arterial phase were considered necrotic; the rate was calculated as (1 - viable tumor diameter / pre-TACE tumor diameter) × 100%.9,16
Other variables: sex, age, pre-TACE AFP (≤400 ng/mL vs >400 ng/mL, collected within 3 days before the first TACE session), MELD score (≤20 vs >20, calculated within 1 week before transplantation), underlying liver disease (hepatitis vs non-hepatitis), Child-Pugh classification (assessed pre-transplant), maximum tumor diameter (≤5 cm vs >5 cm, measured via pre-TACE contrast-enhanced imaging), tumor distribution (unilobar vs bilobar, based on pre-TACE imaging), tumor number (single vs multiple, defined as ≥2 lesions regardless of size), pathological grade (well, moderate, or poorly differentiated, per WHO classification of liver tumors), capsule (yes/no, identified via pathological examination of explanted liver), microvascular invasion (no/yes, defined per IHPBA criteria17,18), and bridging therapy type (DEB-TACE vs cTACE, based on actual TACE regimen administered).
Validation and Evaluation of the Predictive Model
Considering the potential optimism in performance estimation caused by variable selection methods and model overfitting, model validation was performed using a bootstrap resampling method (B=20) to construct calibration curves. The predictive performance of the model for 1-, 2-, and 3-year recurrence was assessed by calculating the area under the receiver operating characteristic (ROC) curve (AUC).
Clinical Application of the Predictive Model
Each variable and its corresponding subcategories were assigned a specific score on the nomogram. The total score yielded an individualized probability of post-transplant HCC recurrence, enabling personalized risk prediction and providing guidance for clinical decision-making and donor allocation.
Statistical Analysis
All statistical analyses were performed using R software (version 4.1.1). Descriptive and comparative analyses were conducted using R basic functions, while survival curves, Cox regression analyses, and nomogram construction were performed using the survminer and rms packages. For continuous variables with normal distribution, results were expressed as mean ± standard deviation ( ± s), and comparisons between groups were conducted using independent-sample t tests. For non-normally distributed continuous variables, results were expressed as median (interquartile range) [M (Q1, Q3)], and intergroup comparisons were performed using the rank-sum test. Categorical variables were expressed as numbers and percentages, with comparisons made using the χ2-test or Fisher’s exact test, as appropriate. A P value <0.05 was considered statistically significant.
± s), and comparisons between groups were conducted using independent-sample t tests. For non-normally distributed continuous variables, results were expressed as median (interquartile range) [M (Q1, Q3)], and intergroup comparisons were performed using the rank-sum test. Categorical variables were expressed as numbers and percentages, with comparisons made using the χ2-test or Fisher’s exact test, as appropriate. A P value <0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 73 patients with hepatocellular carcinoma (HCC) beyond the Milan criteria who received transarterial chemoembolization (TACE) bridging therapy before liver transplantation (LT) were included in this study, with 18 patients (24.7%) developing post-transplant tumor recurrence and 55 patients (75.3%) remaining recurrence-free during follow-up. The baseline clinical and pathological characteristics stratified by recurrence status are summarized in Table 1.
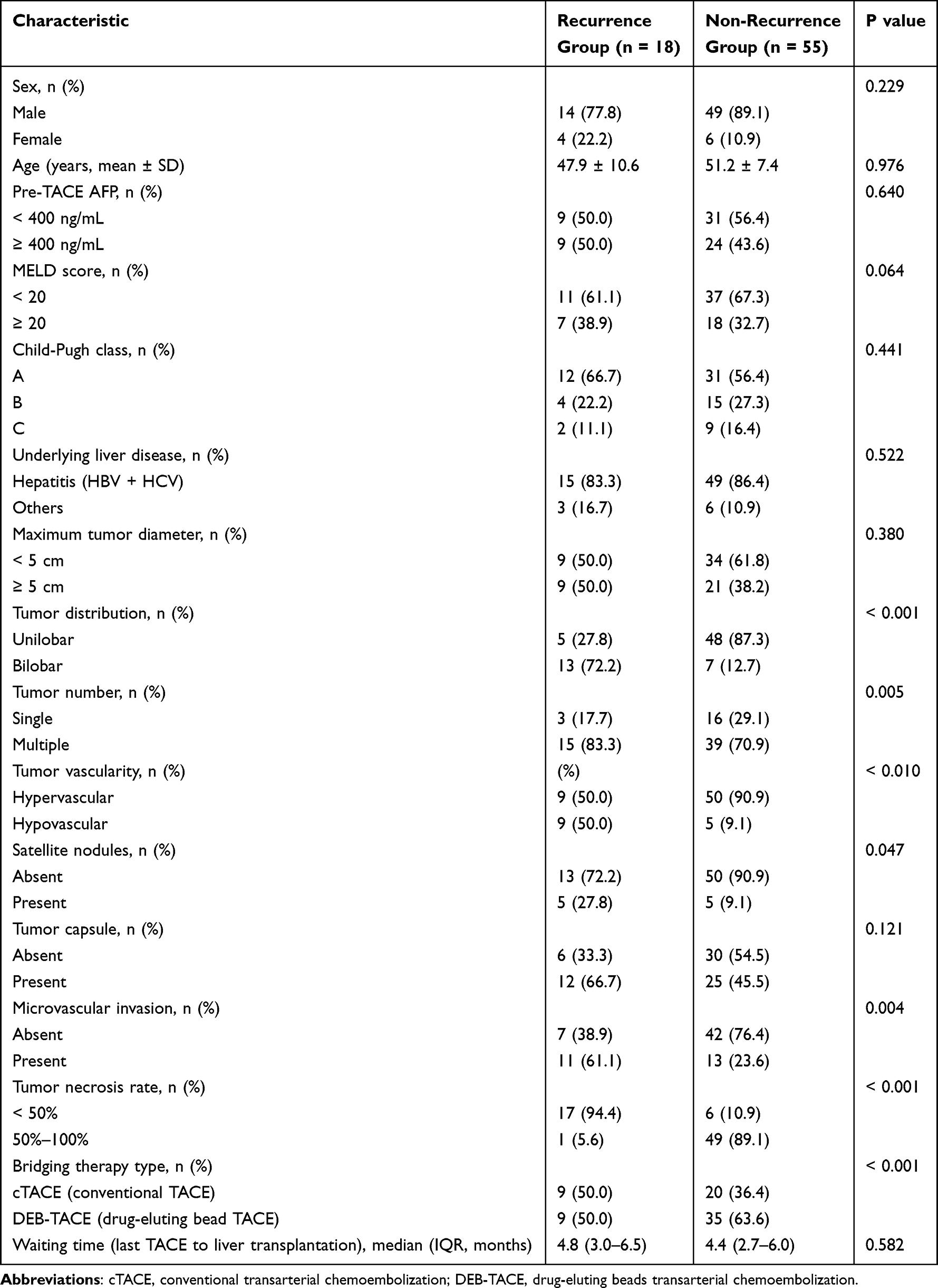 |
Table 1 Clinical Characteristics, Pathological Features, Tumor Necrosis Rate, and Bridging Therapy Type in the Recurrence and Non-Recurrence Groups |
Demographically, the mean age of patients in the recurrence group was 47.9 ± 10.6 years, slightly lower than that in the non-recurrence group (51.2 ± 7.4 years), but the difference was not statistically significant (P = 0.976). In terms of sex distribution, male patients accounted for 77.8% (14/18) of the recurrence group and 89.1% (49/55) of the non-recurrence group, with no significant between-group difference (P = 0.229). The median waiting time between the last TACE session and LT was 4.8 months (interquartile range [IQR]: 3.0–6.5 months) in the recurrence group and 4.4 months (IQR: 2.7–6.0 months) in the non-recurrence group, indicating no significant variation in bridging therapy-to-transplant interval between the two groups (P = 0.582).
For liver function-related parameters, the proportion of patients with a pre-transplant MELD score ≥ 20 was 38.9% (7/18) in the recurrence group and 32.7% (18/55) in the non-recurrence group (P = 0.064), showing a trend toward higher MELD scores in the recurrence group but not reaching statistical significance. Child-Pugh class distribution also did not differ significantly between groups: 66.7% (12/18) of recurrence patients and 56.4% (31/55) of non-recurrence patients were classified as Child-Pugh A (P = 0.441). Additionally, underlying liver disease (predominantly hepatitis B virus [HBV] or hepatitis C virus [HCV] infection) was similar between the two groups, with 83.3% (15/18) of recurrence patients and 86.4% (49/55) of non-recurrence patients having viral hepatitis (P = 0.522).
Pre-TACE alpha-fetoprotein (AFP) levels (collected within 3 days before the first TACE session) showed no significant difference between groups: 50.0% (9/18) of recurrence patients and 43.6% (24/55) of non-recurrence patients had pre-TACE AFP ≥ 400 ng/mL (P = 0.640). Tumor size (maximum diameter ≥ 5 cm) was also balanced between the recurrence group (50.0%, 9/18) and non-recurrence group (38.2%, 21/55; P = 0.380).
Univariate analysis revealed that multiple tumor-related pathological and imaging features were significantly associated with post-transplant recurrence (Table 1).
Tumor distribution showed the most striking difference: 72.2% (13/18) of patients in the recurrence group had bilobar tumors, compared to only 12.7% (7/55) in the non-recurrence group (P < 0.001). Similarly, tumor number was linked to recurrence risk: 83.3% (15/18) of recurrence patients had multiple tumors, versus 70.9% (39/55) of non-recurrence patients (P = 0.005). Tumor vascularity (assessed via pre-TACE contrast-enhanced CT/MRI) also differed significantly: 50.0% (9/18) of recurrence patients had hypovascular tumors, while hypovascularity was observed in only 9.1% (5/55) of non-recurrence patients (P < 0.010).
The presence of satellite nodules was more common in the recurrence group: 27.8% (5/18) of recurrence patients had satellite nodules, compared to 9.1% (5/55) of non-recurrence patients (P = 0.047). Pathological features of the explanted liver further highlighted recurrence-related differences: microvascular invasion (MVI) was present in 61.1% (11/18) of recurrence patients, significantly higher than the 23.6% (13/55) rate in non-recurrence patients (P = 0.004). Tumor necrosis rate (prioritized from pathological assessment) was a strong discriminator: 94.4% (17/18) of recurrence patients had tumor necrosis < 50%, whereas 89.1% (49/55) of non-recurrence patients achieved necrosis ≥ 50% (P < 0.001).
Bridging therapy type also impacted recurrence risk: 50.0% (9/18) of recurrence patients received conventional TACE (cTACE), while only 36.4% (20/55) of non-recurrence patients underwent cTACE. Conversely, drug-eluting bead TACE (DEB-TACE) was more prevalent in the non-recurrence group (63.6%, 35/55) than in the recurrence group (50.0%, 9/18), with this difference reaching statistical significance (P < 0.001).
Establishment of the Predictive Model
Univariate Cox regression analysis identified 10 characteristics significantly associated with post-transplant recurrence (all P < 0.05): age, AFP ≥400 ng/mL, MELD score ≥20, bilobar tumor distribution, multiple tumors, hypovascularity, presence of satellite nodules, absence of capsule, presence of microvascular invasion, and absence of bridging therapy (Table 2). Variables with a two-sided P<0.10 (a commonly adopted threshold in clinical prognostic studies to balance sensitivity for potential predictors and avoidance of excessive variable exclusion) were included in multivariate Cox regression to identify independent risk factors, with a two-sided P<0.05 defined as statistically significant. These variables were included in the multivariate Cox regression analysis, which revealed four independent prognostic factors: bridging therapy type [hazard ratio (HR): 2.402; 95% confidence interval (CI): 1.069–5.396; P = 0.034], microvascular invasion (HR: 3.445; 95% CI: 1.675–7.088; P = 0.001), tumor necrosis rate (HR: 26.664; 95% CI: 3.394–209.492; P = 0.002), and AFP (HR: 2.750; 95% CI: 1.382–5.470; P = 0.004) (Table 3). The predictive model was visualized using a nomogram (Figure 2). The nomogram incorporated four variables: bridging therapy type, microvascular invasion, tumor necrosis rate, and pre-TACE AFP. Among these, tumor necrosis rate contributed most to recurrence prediction, followed by microvascular invasion and pre-TACE AFP.
 |
Table 2 Results of Univariate Cox Regression Analysis of Risk Factors for Post-Transplant Recurrence in Patients with HCC Beyond the Milan Criteria Undergoing TACE Bridging Therapy |
 |
Table 3 Multivariate Cox Regression Analysis of Risk Factors for Post-Transplant Recurrence in Patients with HCC Beyond the Milan Criteria Undergoing TACE Bridging Therapy |
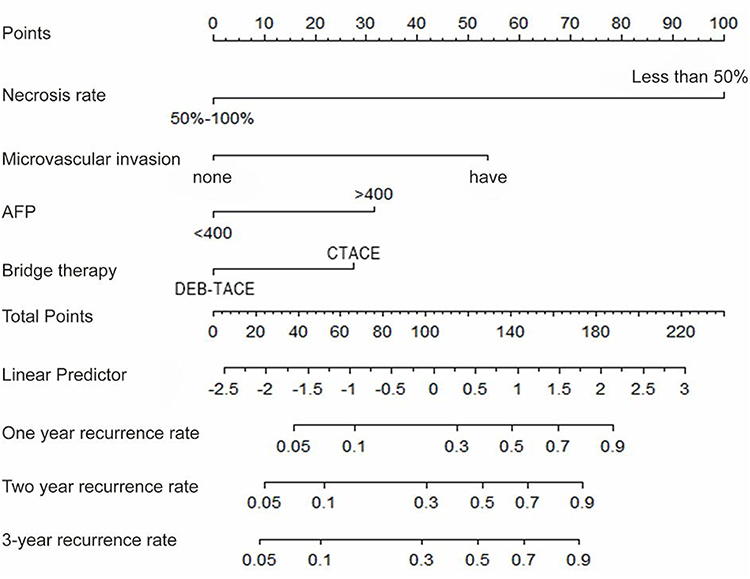 |
Figure 2 Nomogram for predicting post-transplant tumor recurrence in patients with HCC beyond the Milan criteria. Abbreviations: cTACE, conventional transarterial chemoembolization; DEB-TACE, drug-eluting beads transarterial chemoembolization; AFP, alpha-fetoprotein. Notes: Each categorical variable corresponds to a specific score. The total score is calculated based on the characteristics of each variable, from which the probability of tumor recurrence can be derived. |
Predictive Performance of the Model
Nomograms provide a visual tool for individualized risk prediction and are increasingly applied in oncology. Prior studies have developed nomograms based on clinical features to predict prognosis in HCC, but no model has been established for post-transplant recurrence in patients with HCC beyond the Milan criteria undergoing TACE bridging therapy. In this study, we developed nomograms to predict recurrence at 1, 2, and 3 years, with AUC values of 0.740, 0.764, and 0.886, respectively, indicating good predictive accuracy; calibration via bootstrap resampling (B=20) showed excellent agreement between predicted and observed recurrence, supporting its clinical utility for individualized management. Practically, the nomogram can be integrated into workflows in three key ways: pre-transplant, to guide bridging therapy selection (prioritizing DEB-TACE for patients with predicted 3-year recurrence risk >30%) during MDT discussions; for donor allocation, to prioritize recipients with lower risk (<10% 3-year risk) amid scarce organs; and post-transplant, to adjust follow-up intensity (3-month vs 6-month imaging) or interventions (early steroid withdrawal per 2022 Chinese guidelines) for high-risk patients. This integration ensures the nomogram translates from research to practice, directly fulfilling the study’s objective of guiding clinical decision-making for this specific cohort. (Figure 3)
 |
Figure 3 Receiver operating characteristic (ROC) curves for predicting 1-, 2-, and 3-year post-transplant recurrence in patients with HCC beyond the Milan criteria (A, C, E), and calibration plots for 1-, 2-, and 3-year recurrence (B, D, F). Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve. |
Case Presentation of Clinical Application of the Predictive Model
Case 1: A 44-year-old female, Child-Pugh class A, BCLC stage B, with hepatocellular carcinoma located in the right hepatic lobe, scheduled for liver transplantation. Contrast-enhanced CT revealed a maximum tumor diameter of 5.5 cm (Figure 4), exceeding the Milan criteria. Following multidisciplinary team (MDT) discussion, the patient underwent DEB-TACE as bridging downstaging therapy prior to transplantation (Figure 5). One month after DEB-TACE, follow-up abdominal CT showed a residual small nodule (Figure 6). Given the anticipated long waiting time for transplantation, the patient received a second DEB-TACE using 70–150 µm drug-eluting beads for embolization (Figure 7). Two months later, the patient underwent liver transplantation, and postoperative pathology confirmed complete tumor necrosis (Figures 8 and 9). At 3-year follow-up after transplantation, no tumor recurrence was observed.
 |
Figure 4 Contrast-enhanced abdominal CT findings. Notes: CT revealed cirrhosis. The lesion showed marked heterogeneous enhancement during the arterial phase and reduced enhancement in the portal venous phase. Another lesion demonstrated progressive enhancement from the arterial to the portal venous phase, suggesting HCC combined with hemangioma. |
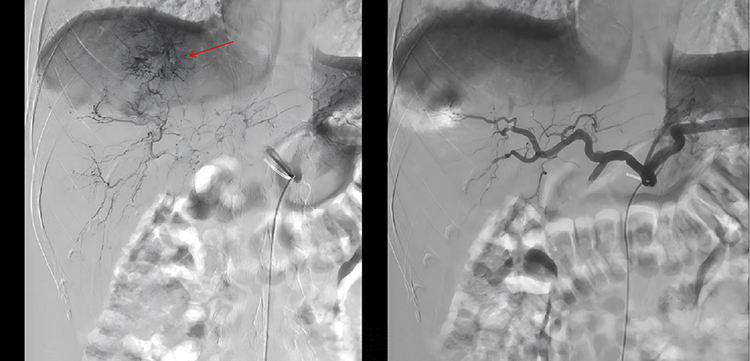 |
Figure 5 Angiographic findings of DEB-TACE. Notes: The red arrow in the left panel indicates the hypervascular region of the hepatocellular carcinoma, corresponding to the tumor’s main blood supply (visualized via contrast agent filling). The right panel shows the catheter positioned at the feeding artery of the tumor, prepared for TACE embolization. |
 |
Figure 6 Follow-up CT 4 weeks after DEB-TACE. Note: The arrow indicates the residual lesion. |
 |
Figure 7 Angiographic findings of repeat DEB-TACE. Notes: Angiography revealed slender and irregular tumor-feeding vessels with a round tumor-staining area (arrow). After successful superselective microcatheterization, 70–150 µm drug-eluting beads were administered for complete embolization. Post-embolization, complete interruption of tumor vessels and disappearance of tumor staining were observed. |
 |
Figure 8 Gross pathology after liver transplantation. Note: The arrows indicate two completely necrotic lesions. |
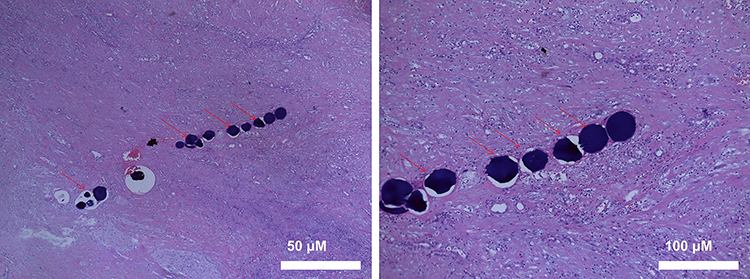 |
Figure 9 Postoperative pathology. Notes: Specimens were sampled according to pathological standards. Histology revealed complete tumor necrosis. Drug-eluting beads (marked by the red arrow) were identified within the necrotic tissue, arranged in a “string-of-beads” pattern. |
Note: This study is retrospective, and prior to manuscript submission, we contacted the patient described in this case to inform her of the purpose of publishing her de-identified clinical details (including imaging findings, treatment process, and follow-up outcomes). The patient voluntarily provided written informed consent for the publication of these case-specific data, and the original consent form has been archived in the medical record management system of Tianjin First Central Hospital for verification if required.
The nomogram was applied to predict the patient’s recurrence risk after liver transplantation (Figure 10). The patient received DEB-TACE bridging therapy, achieved complete tumor necrosis, showed no microvascular invasion, and had a pre-TACE AFP level of 517 ng/mL. By drawing vertical lines upward from each factor to obtain the corresponding scores, summing them to yield a total of 32 points, and projecting downward from the “Total Points” axis, the predicted probability of recurrence was <10%, which was consistent with the actual outcome.
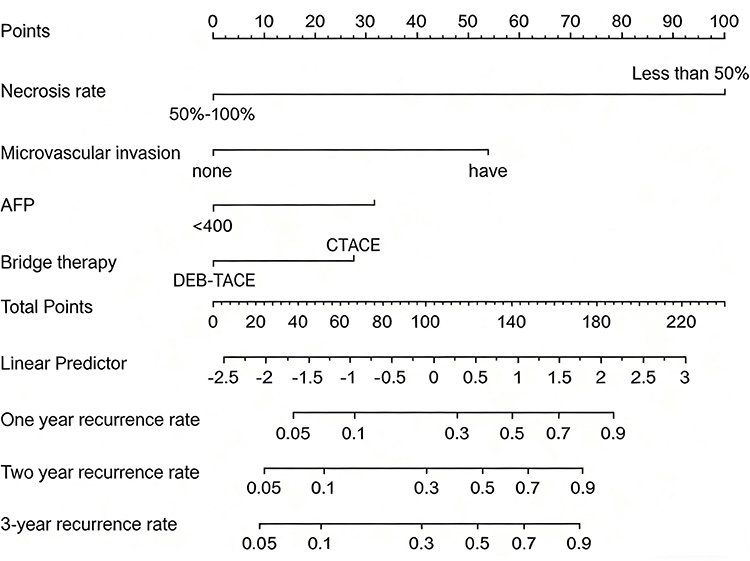 |
Figure 10 Nomogram prediction of recurrence risk. This nomogram incorporates clinical factors including tumor necrosis rate (categories: 50%–100% or less than 50%), microvascular invasion (categories: “none” or “have”), AFP level (category: <400 ng/mL), and bridge therapy (categories: DEB-TACE or CTACE); to apply this nomogram, first identify the patient’s corresponding category for each factor on the respective axis, map this category to the top “Points” scale to obtain the points allocated to that factor, sum the points of all factors to calculate the “Total Points” (middle axis), then map the “Total Points” to the “Linear Predictor” axis followed by the 1-, 2-, and 3-year recurrence rate axes (bottom axes) to derive the predicted recurrence probabilities. Abbreviation: AFP, alpha-fetoprotein. |
Discussion
Data from the China Liver Transplant Registry (CLTR) indicate that nearly 65% of liver transplant recipients with hepatocellular carcinoma (HCC) in China present with tumors beyond the Milan criteria.19 Study have reported that up to 42% of such patients undergo local bridging therapy prior to transplantation20 However, due to tumor heterogeneity, post-transplant recurrence rates still vary. In the present study, among 73 patients with HCC beyond the Milan criteria who underwent TACE bridging therapy, the 1-, 2-, and 3-year cumulative recurrence rates were 17.8%, 23.3%, and 24.7%, respectively. Predicting recurrence after transplantation in patients receiving bridging therapy has important clinical implications, and may assist in optimizing donor allocation.
In this retrospective study of 73 patients with HCC beyond the Milan criteria who underwent TACE bridging therapy, we compared recurrence rates at 1, 2, and 3 years between cTACE and DEB-TACE groups. Clinical characteristics, pathological features, bridging therapy type, and tumor necrosis rate (≥50%) were included in the analysis. Independent prognostic factors were identified by univariate and multivariate Cox regression analyses, and a nomogram was developed. The main findings were: (1) patients treated with DEB-TACE bridging had lower 1-, 2-, and 3-year post-transplant recurrence rates compared with those treated with cTACE; (2) bridging therapy type, microvascular invasion (MVI), pre-TACE AFP, and tumor necrosis rate were independent risk factors for post-transplant recurrence; and (3) the nomogram model based on these factors provided accurate prediction of recurrence risk and may assist in optimizing donor allocation.
Analysis of Risk Factors for Recurrence After Transplantation in Patients with HCC Beyond the Milan Criteria Undergoing TACE Bridging Therapy
Current liver transplant criteria for HCC typically include tumor size, tumor number, total tumor volume, AFP level, response to downstaging therapy, tumor differentiation, and presence of MVI.21 In our study, we analyzed clinical and pathological features, tumor necrosis rate, and bridging therapy type, including sex, age, waiting time, pre-TACE AFP, MELD score, underlying liver disease, Child-Pugh class, tumor distribution, maximum tumor diameter, tumor number, vascularity, satellite nodules, capsule, MVI, tumor necrosis rate, and bridging therapy type. We found that patients treated with DEB-TACE bridging had lower recurrence rates than those treated with cTACE. Moreover, patients with tumor necrosis ≥50% had better prognosis than those with <50%, and DEB-TACE was associated with a higher proportion of necrosis ≥50% compared with cTACE. Therefore, both bridging therapy type and tumor necrosis rate were incorporated into our analysis. Cox regression confirmed bridging therapy type, MVI, pre-TACE AFP, and tumor necrosis rate as independent risk factors for recurrence.
Bridging therapy type itself was identified as an independent predictor of recurrence. A prior study reported that if patients beyond the Milan criteria could be successfully downstaged to within the criteria, their 5-year survival after transplantation was comparable to that of patients who initially met the Milan criteria.22 Downstaging therapies mainly include transarterial interventions (TACE, TARE) and ablative therapies such as percutaneous ethanol injection (PEI), radiofrequency ablation (RFA), and microwave ablation (MWA).23 Bridging therapy, also known as neoadjuvant therapy, not only reduces tumor size and number but may also reflect tumor biology and can serve as a selection criterion for donor allocation. TACE-induced tumor necrosis is closely associated with post-transplant recurrence.24 Patients achieving pathologic complete response (pCR) can achieve recurrence and survival rates similar to those of patients within the Milan criteria.25 Although imaging criteria such as mRECIST are widely used to assess response, pathological assessment provides a more accurate measure of tumor necrosis and biological behavior. Our results confirmed that tumor necrosis rate is an independent risk factor for recurrence, with the highest contribution in the nomogram.
Pre-TACE AFP level partially reflects tumor burden and biology.26 However, AFP is elevated in only ~30% of HCC patients, limiting its diagnostic utility.27 Instead, AFP is considered more valuable as a prognostic marker. A study suggest that patients with pre-transplant AFP >1000 ng/mL are unsuitable for transplantation due to the high risk of recurrence.28 Conversely, significant reduction of AFP by bridging therapy has been associated with improved outcomes.29 Based on the 2024 edition of the Chinese guidelines for HCC, we used 400 ng/mL as the cutoff and found AFP ≥400 ng/mL to be an independent risk factor for recurrence. In our cohort, 45.2% (33/73) of patients had AFP ≥400 ng/mL before TACE. Novel biomarkers such as microRNAs have emerged as promising predictors of recurrence and may represent future research directions.
Microvascular invasion (MVI) is a well-recognized independent risk factor for recurrence.30 MVI is defined as microscopic nests of tumor cells within endothelial-lined vessels, most often involving branches of the portal vein. Pathological classification is as follows: M0, no MVI; M1 (low risk), ≤5 foci within ≤1 cm of the tumor; and M2 (high risk), >5 foci or foci >1 cm from the tumor. MVI and satellite nodules may represent different stages of intrahepatic spread. In our study, the incidence of MVI was 32.9% (24/73), while satellite nodules occurred in 13.7% (10/73). MVI remains an important indicator of tumor aggressiveness and prognosis after transplantation, with its incidence positively correlated with tumor size.30 Although preoperative biopsy may detect MVI, risks of bleeding, seeding, and sampling error limit its clinical use.31 Recently, serum biomarkers, microRNAs, and radiomics have been investigated as non-invasive predictors of MVI, which warrant further research.32
Tumor number is another important variable in many transplant criteria. However, its prognostic role remains controversial. Some studies suggest a strong association with recurrence, particularly when the number exceeds three, while others report no significant relationship.16 In our cohort, tumor number was not identified as an independent risk factor, with the Milan criterion cutoff of 5 cm as reference.
Application of Nomograms in Predicting Prognosis of HCC
Nomograms provide a visual tool for individualized risk prediction and are increasingly applied in oncology. Prior studies have developed nomograms based on clinical features to predict prognosis in HCC,10 but no model has been established for post-transplant recurrence in patients with HCC beyond the Milan criteria undergoing TACE bridging therapy. In this study, we developed nomograms to predict recurrence at 1, 2, and 3 years, with AUC values of 0.740, 0.764, and 0.886, respectively, indicating good predictive accuracy. Calibration using bootstrap resampling (B = 20) showed excellent agreement between predicted and observed recurrence. Thus, a nomogram incorporating both clinical and pathological features offers high clinical utility, enabling individualized management of transplant recipients.11 For high-risk patients, the 2022 Chinese guidelines recommend strategies such as early steroid withdrawal or steroid-free regimens and reduced calcineurin inhibitor use post-transplant to lower recurrence risk.
This study has notable limitations. First, the nomogram was developed and internally validated using a single-center, retrospective cohort (n=73), and external validation with multi-center data was not feasible in the current study—primarily due to the lack of standardized, shared datasets for our specific patient subgroup (HCC beyond Milan criteria with TACE bridging therapy) across regional institutions. Second, our primary endpoint focused on post-transplant tumor recurrence, and immature follow-up data (median: 33.2 months) precluded robust analysis of overall survival (OS), which would further contextualize the nomogram’s link to long-term patient outcomes. To address these gaps, we are actively establishing collaborations with three tertiary liver transplant centers in northern China to prospectively collect a harmonized external cohort (target n=80) over the next 12–18 months. We will also extend follow-up of our original cohort to December 2025 to accumulate mature OS data, with the goal of validating the nomogram externally and integrating OS as a secondary endpoint in future work. The final potential limitation of this study is the absence of external validation (multi-center cohort or temporal split validation). Due to the limited availability of collaborative institutional data on hepatocellular carcinoma patients receiving TACE bridging therapy beyond the Milan criteria, we relied solely on internal bootstrap validation (B=20) to evaluate model stability. Future studies with larger, multi-center cohorts are recommended to further validate the nomogram’s performance and generalizability to diverse clinical settings. A further limitation is the lack of decision curve analysis (DCA) to evaluate the nomogram’s net clinical benefit. DCA was not performed due to current constraints in computational resources and access to specialized statistical tools for threshold-based benefit calculation. We plan to conduct DCA once these resources are available, as it will be critical to confirming whether the nomogram can guide clinical decisions (donor allocation, follow-up intensity) with tangible patient benefits.
Conclusion
In summary, in patients with HCC beyond the Milan criteria undergoing liver transplantation, DEB-TACE bridging therapy was associated with lower recurrence rates than cTACE. Bridging therapy type, MVI, pre-TACE AFP, and tumor necrosis rate were identified as independent risk factors. A nomogram based on these four factors demonstrated favorable predictive performance and may serve as a valuable tool for clinical decision-making and donor allocation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from corresponding author Guang Chen (Email: [email protected]) or co-corresponding author Xunjin Zeng (Email: [email protected]) upon reasonable request. All data requests will be processed in compliance with institutional data protection policies.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and the Declaration of Istanbul. The study protocol was approved by the Institutional Ethics Committee of Tianjin First Central Hospital (Approval No.: 2015014F). Informed consent for reviewing medical records was waived by the committee due to the retrospective nature of the study, which involved de-identified patient data and posed no additional risks to participants. Strict measures were implemented to ensure the confidentiality of patient information, including anonymization of all clinical and demographic data during data collection and analysis. For individual case details included in the manuscript, written informed consent for publication was obtained from all relevant patients. Additionally, all organ donations involved in the study were voluntary, and written informed consent was provided by the donors or their legal representatives in accordance with national regulations and the Declaration of Istanbul.
Consent for Publication
This is a retrospective observational study. For the individual case presented in the “Case presentation of clinical application of the predictive model” section, the patient was informed of the publication purpose and content of her de-identified case details after the study data were collected. The patient provided written informed consent for publication, and the consent form is archived in the medical record system of Tianjin First Central Hospital. For the retrospective analysis of aggregated patient data (excluding individual case disclosure) in other parts of the study, the Institutional Ethics Committee of Tianjin First Central Hospital (approval number: 2015014F) confirmed that additional consent for publication was unnecessary, in line with the Declaration of Helsinki and national ethical guidelines for retrospective research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Salem R, Gilbertsen M, Butt Z, et al. Increased quality of life among hepatocellular carcinoma patients treated with radioembolization, compared with chemoembolization. Clin Gastroenterol Hepatol. 2013;11(10):1358–1365.e1351. doi:10.1016/j.cgh.2013.04.028
2. Salem R, Gordon AC, Mouli S, et al. Y90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2016;151(6):1155–1163.e1152. doi:10.1053/j.gastro.2016.08.029
3. Roayaie S, Schwartz JD, Sung MW, et al. Recurrence of hepatocellular carcinoma after liver transplant: patterns and prognosis. Liver Transplant. 2004;10(4):534–17. doi:10.1002/lt.20128
4. Sapisochin G, Goldaracena N, Astete S, et al. Benefit of treating hepatocellular carcinoma recurrence after liver transplantation and analysis of prognostic factors for survival in a large Euro-American series. Ann Surg Oncol. 2015;22(7):2286–2294. doi:10.1245/s10434-014-4273-6
5. Shimamura T, Akamatsu N, Fujiyoshi M, et al. Expanded living-donor liver transplantation criteria for patients with hepatocellular carcinoma based on the Japanese nationwide survey: the 5-5-500 rule - a retrospective study. Transplant Int. 2019;32(4):356–368. doi:10.1111/tri.13391
6. Peng ZH, Sun HC. Recurrence of hepatocellular carcinoma after liver transplantation. Chin J Digest Surg. 2016;15(05):444–447.
7. Yao FY, Ferrell L, Bass NM, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33(6):1394–1403. doi:10.1053/jhep.2001.24563
8. Pompili M, Francica G, Ponziani FR, Iezzi R, Avolio AW. Bridging and downstaging treatments for hepatocellular carcinoma in patients on the waiting list for liver transplantation. World J Gastroenterol. 2013;19(43):7515–7530. doi:10.3748/wjg.v19.i43.7515
9. Lee DD, Samoylova M, Mehta N, et al. The mRECIST classification provides insight into tumor biology for patients with hepatocellular carcinoma awaiting liver transplantation. Liver Transplant. 2019;25(2):228–241. doi:10.1002/lt.25333
10. Tian X, Song Q, Xie F, et al. Papillary thyroid carcinoma: an ultrasound-based nomogram improves the prediction of lymph node metastases in the central compartment. Eur Radiol. 2020;30(11):5881–5893. doi:10.1007/s00330-020-06906-6
11. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–180. doi:10.1016/s1470-2045(14)71116-7
12. Tabu K, Mawatari S, Oda K, et al. Hypovascular tumors developed into hepatocellular carcinoma at a high rate despite the elimination of hepatitis C virus by direct-acting antivirals. PLoS One. 2020;15(8):e0237475. doi:10.1371/journal.pone.0237475
13. Tan J, Mathy RM, Chang DH, Tang T, Zhang ZS, Xiao YD. Combined transarterial iodized oil injection and computed tomography-guided thermal ablation for hepatocellular carcinoma: utility of the iodized oil retention pattern. Abdominal Radiol. 2022;47(1):431–442. doi:10.1007/s00261-021-03305-3
14. Chen QF, Li W, Yu SC, et al. Consensus of minimally invasive and multidisciplinary comprehensive treatment for hepatocellular carcinoma - 2020 Guangzhou recommendations. Front Oncol. 2021;11:621834. doi:10.3389/fonc.2021.621834
15. Zheng DX, Chen YX, Sun J, et al. Stereotactic body radiation therapy in patients with centrally located hepatocellular carcinoma: a retrospective, single-arm, multi-center study. Clin Trans Radiation Oncol. 2024;46:100767. doi:10.1016/j.ctro.2024.100767
16. Sapisochin G, Goldaracena N, Laurence JM, et al. The extended Toronto criteria for liver transplantation in patients with hepatocellular carcinoma: a prospective validation study. Hepatology. 2016;64(6):2077–2088. doi:10.1002/hep.28643
17. Iguchi T, Shirabe K, Aishima S, et al. New pathologic stratification of microvascular invasion in hepatocellular carcinoma: predicting prognosis after living-donor liver transplantation. Transplantation. 2015;99(6):1236–1242. doi:10.1097/tp.0000000000000489
18. Jotz RF, Horbe AF, Coral GP, Fontana PC, de Morais BG, de Mattos AA. Results of transarterial chemoembolization of hepatocellular carcinoma as a bridging therapy to liver transplantation. Radiologia brasileira. 2023;56(5):235–241. doi:10.1590/0100-3984.2023.0040
19. Ling Q. Commentary: a preoperative model for predicting microvascular invasion and assisting in prognostic stratification in liver transplantation for HCC regarding empirical criteria. Transl Oncol. 2021;14(12):101234. doi:10.1016/j.tranon.2021.101234
20. Bauschke A, Altendorf-Hofmann A, Ardelt M, Kissler H, Tautenhahn H-M, Settmacher U. Impact of successful local ablative bridging therapy prior to liver transplantation on long-term survival in patients with hepatocellular carcinoma in cirrhosis. J Cancer Res Clin Oncol. 2020;146(7):1819–1827. doi:10.1007/s00432-020-03215-9
21. Xu XF, Diao YK, Zeng YY, et al. Association of severity in the grading of microvascular invasion with long-term oncological prognosis after liver resection for early-stage hepatocellular carcinoma: a multicenter retrospective cohort study from a hepatitis B virus-endemic area. Int J Surg. 2023;109(4):841–849. doi:10.1097/js9.0000000000000325
22. Tırnova I, Kanmaz T. Liver transplantation for HCC within and beyond Milan Criteria: single center experience with literature review. Front Surg. 2025;12:1594361. doi:10.3389/fsurg.2025.1594361
23. Wang Z, Wang Y, Gao P, Ding J. Immune checkpoint inhibitor resistance in hepatocellular carcinoma. Cancer Lett. 2023;555:216038. doi:10.1016/j.canlet.2022.216038
24. Atanasov G, Dino K, Schierle K, et al. Recipient hepatic tumor-associated immunologic infiltrates predict outcomes after liver transplantation for hepatocellular carcinoma. Ann Transplant. 2020;25:e919414. doi:10.12659/aot.919414
25. Nutu A, Justo I, Marcacuzco A, et al. Liver transplantation for hepatocellular carcinoma using grafts from uncontrolled circulatory death donation. Sci Rep. 2021;11(1):13520. doi:10.1038/s41598-021-92976-5
26. He C, Zhang X, Li C, et al. Changes of alpha-fetoprotein levels could predict recurrent hepatocellular carcinoma survival after trans-arterial chemoembolization. Oncotarget. 2017;8(49):85599–85611. doi:10.18632/oncotarget.20343
27. Tang Z, Li X, Zheng Y, Liu J, Liu C, Li X. The role of competing endogenous RNA network in the development of hepatocellular carcinoma: potential therapeutic targets. Front Cell Develop Biol. 2024;12:1341999. doi:10.3389/fcell.2024.1341999
28. Mahmud N, John B, Taddei TH, Goldberg DS. Pre-transplant alpha-fetoprotein is associated with post-transplant hepatocellular carcinoma recurrence mortality. Clin Transplant. 2019;33(7):e13634. doi:10.1111/ctr.13634
29. Pei YX, Su CG, Liao Z, Li WW, Wang ZX, Liu JL. Comparative effectiveness of several adjuvant therapies after hepatectomy for hepatocellular carcinoma patients with microvascular invasion. World J Gastrointestinal Surg. 2024;16(2):554–570. doi:10.4240/wjgs.v16.i2.554
30. Jonas S, Bechstein WO, Steinmüller T, et al. Vascular invasion and histopathologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology. 2001;33(5):1080–1086. doi:10.1053/jhep.2001.23561
31. Chen X, Li Q, Xun XD, Zhou HY. Impact of microvascular invasion on progression-free survival in patients with solitary small hepatocellular carcinoma after surgery. Chin J Hepatobil Surg. 2016;22(02):94–98.
32. Liu M, Wang L, Zhu H, et al. A preoperative measurement of serum MicroRNA-125b may predict the presence of microvascular invasion in hepatocellular carcinomas patients. Transl Oncol. 2016;9(3):167–172. doi:10.1016/j.tranon.2016.03.002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Low MARCO Expression is Associated with Poor Survival in Patients with Hepatocellular Carcinoma Following Liver Transplantation
Zhang Q, Wei Y, Li Y, Jiao X
Cancer Management and Research 2022, 14:1935-1944
Published Date: 11 June 2022
Delayed Hepatocellular Carcinoma Recurrence After Liver Transplantation: Comprehensive Clinical Characterization of Case Series
Wong TH, Ho CM, Hsu HH, Wu YM, Ho MC, Lee PH, Hu RH
Journal of Hepatocellular Carcinoma 2022, 9:1081-1091
Published Date: 17 October 2022
The Fibrinogen-to-Albumin Ratio (FAR) Predicts Prognosis in Hepatocellular Carcinoma Patients After Liver Transplantation: Development and Validation of a Novel Nomogram
Ye XY, Leng AX, He Q, Ji Z, Ma J
Journal of Hepatocellular Carcinoma 2026, 13:588619
Published Date: 8 April 2026
Liver Transplantation After Radiotherapy-Antiangiogenesis-Immune Checkpoint Blockade Combination Therapy in Hepatocellular Carcinoma with Major Portal Vein Tumor Thrombosis: A Propensity Score Matching Analysis
Zhao Y, Song J, Li K, Li T, Li W, Yang Y, Tong X, Xiao Y, Xu G, Lu Q, Li G, Li G, Dong J
Journal of Hepatocellular Carcinoma 2026, 13:570163
Published Date: 8 May 2026
Tumor Burden Thresholds Associated with Successful Downstaging After Yttrium-90 Radioembolization in Hepatocellular Carcinoma Beyond UCSF Criteria
Chiu CH, Yu CY, Ou HY, Tsang LC, Huang PH, Weng CC, Lu Y, Chen CL, Cheng YF
Journal of Hepatocellular Carcinoma 2026, 13:613375
Published Date: 10 July 2026