Back to Journals » Journal of Hepatocellular Carcinoma » Volume 9
Delayed Hepatocellular Carcinoma Recurrence After Liver Transplantation: Comprehensive Clinical Characterization of Case Series
Authors Wong TH ![]() , Ho CM
, Ho CM ![]() , Hsu HH, Wu YM, Ho MC, Lee PH, Hu RH
, Hsu HH, Wu YM, Ho MC, Lee PH, Hu RH
Received 2 August 2022
Accepted for publication 8 October 2022
Published 17 October 2022 Volume 2022:9 Pages 1081—1091
DOI https://doi.org/10.2147/JHC.S383474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Imam Waked
Ta-Hsiang Wong,1,2 Cheng-Maw Ho,3,4 Hsao-Hsun Hsu,3,4 Yao-Ming Wu,3,4 Ming-Chih Ho,3,4 Po-Huang Lee,3,4 Rey-Heng Hu3,4
1Department of Medical Education, National Taiwan University Hospital, Taipei, Taiwan; 2School of Medicine, National Taiwan University, Taipei, Taiwan; 3Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan; 4College of Medicine, National Taiwan University, Taipei, Taiwan
Correspondence: Cheng-Maw Ho, Department of Surgery, National Taiwan University Hospital, 7 Chung-Shan South Road, Taipei, 100, Taiwan, Tel +886-223123456-265914, Email [email protected]
Purpose: Liver transplantation (LT) is the definite curative treatment for hepatocellular carcinoma (HCC), but recurrence can occur even under stringent criteria. “Delayed” HCC recurrence (> 3 years after LT) is not common. Here, we present the clinical features of patients who developed delayed HCC recurrence after LT.
Patients and Methods: We reviewed the data of eligible patients from February 1999 to December 2020 from medical records.
Results: From among 195 (17%) HCC patients who received LT, 34 experienced HCC recurrence, with 5 (15%) delayed recurrence. These five explant tumors were staged T1b–T2, graded II–III, with two vascular invasion and four beyond the Milan criteria. The median time to recurrence was 6.1 years, with the longest interval being nearly 18 years. Recurrence patterns included two extrahepatic, one intrahepatic, and two mixed extrahepatic and intrahepatic recurrences. A drastic increase in serum alpha-fetoprotein levels was observed in four cases 1 year before recurrence. Management of recurrence included locoregional (surgssical resection in three, radiotherapy in three, transarterial chemoembolization in one, radiofrequency ablation in one) and systemic sorafenib use in three. Two patients died within 12– 18 months, one died within 18– 24 months, and two are still alive until the end of the study, with respective 13.5- and 16.5-month survival.
Conclusion: Delayed HCC recurrence could occur over 10 years. Therefore, continual surveillance for recurrence is justified, but biomarkers and intervals or intensities specific for delayed recurrence are not validated, which warrants further validation to facilitate personalized medical care.
Keywords: liver transplantation, hepatocellular carcinoma, recurrence, survival, case series
Introduction
Surgical curative treatments for hepatocellular carcinoma (HCC) include resection and liver transplantation (LT). LT within strict selection criteria yields a lower HCC recurrence rate than tumor resection, especially in those with underlying cirrhosis,1 but it still remains relatively high: at approximately 6%–20%.2
No consensus has been reached regarding the management of post-LT HCC recurrence, and the current strategy is similar to that of patients without LT.3 Treatment options include surgical resection, radiotherapy or other locoregional therapies, systemic therapy with sorafenib, and supportive care.3 Despite treatments, the survival rate in post-LT HCC recurrences is dismal, ranging from 6 to 30 months (median: 12 months).4 Curative-intent treatments lead to better long-term survival,5 which highlights the value of early tumor detection and eradication.
Most recurrences are classified as “early” occurring within 2 years of LT.2,3,6,7 Cases with “delayed” (>3 years post-LT) recurrences are so uncommon that few studies have addressed their characteristics. In the literature, the behavior of late recurrences appears to differ from that of early recurrences in terms of better survival3,8 and a tendency toward extrahepatic metastases.7,9 However, the underlying biological mechanisms remain inconclusive.
Whether delayed recurrences have the same risk factors as early recurrences and whether follow-up strategies for delayed HCC recurrence should be modified are not well explored. Here, we used a transplant cohort of more than 20 years to identify patients with delayed HCC recurrence (>3 years after LT) and analyze their disease course and clinical characteristics to help characterize these patients and establish strategies for early detection.
Materials and Methods
The Institutional Review Board of National Taiwan University Hospital, Taipei, Taiwan, approved this study (REC: 202004053RINB) and consent from patients or next of kin if deceased were obtained for the publication of the cases. This study complies with the Declaration of Helsinki. All organs in this study were donated voluntarily with written informed consent. Transplantation was conducted in accordance with the Declaration of Istanbul.
Patients
The data of patients with delayed post-LT HCC recurrence were retrospectively collected from the medical records of a tertiary transplant center. Demographic and clinical characteristics, including age, sex, past medical history, HCC course, treatments, blood biochemical tests, and histopathological examinations, were reviewed.
Transplant Criteria and Follow-Up After LT
The evaluation process for LT and the follow-up strategy have been described previously.1 Briefly, LT is considered when surgical resection and other locoregional treatments are inapplicable because of no possibility for further resection or poor liver reserve. Preoperative tumor status beyond the University of California San Francisco (UCSF) criteria is regarded as a contraindication for LT.
After LT, all patients received regular monthly or bimonthly follow-up with abdominal ultrasonography and serum alpha-fetoprotein (AFP) level monitoring. Contrast imaging studies (such as computed tomography (CT) and magnetic resonance imaging) and histopathological examinations were performed in case of suspicious lesions or specific complaints. The patients were followed up until death or February 28, 2022.
Treatment of HCC Recurrence
As mentioned, the treatment strategy for post-LT HCC recurrence is based on the same criteria for those without LT.3 All patients were initially evaluated for surgical resection of intrahepatic or extrahepatic recurrences. When surgical resection is not feasible, other locoregional therapies for intrahepatic recurrences (such as radiofrequency ablation (RFA) or transarterial chemoembolization (TACE)) and radiotherapy for extrahepatic recurrences are considered. Systemic therapy with sorafenib was used for patients with distant metastases or major vascular invasion inside a liver with good hepatic reserve.
Statistical Analysis
Data are expressed as median (range) or number (percentage), as appropriate. HCC recurrence probability and overall survival were estimated using the Kaplan–Meier method.
Results
Demographics
We initially identified 738 LT recipients between 1999 and 2020, 195 of whom had HCC. Of them, 34 (17%) experienced post-LT HCC recurrence, with five (15%, four men and one woman) experiencing recurrence >3 years after LT (Figure 1). All five patients had undergone live donor LT in their 50s. All were previously diagnosed as having cirrhosis and viral hepatitis (three with hepatitis B and two with hepatitis C). The total follow-up was 48.6 person-years, with a median follow-up of 7.2 (range: 4.8–19.3) years. Table 1 presents the detailed demographic data.
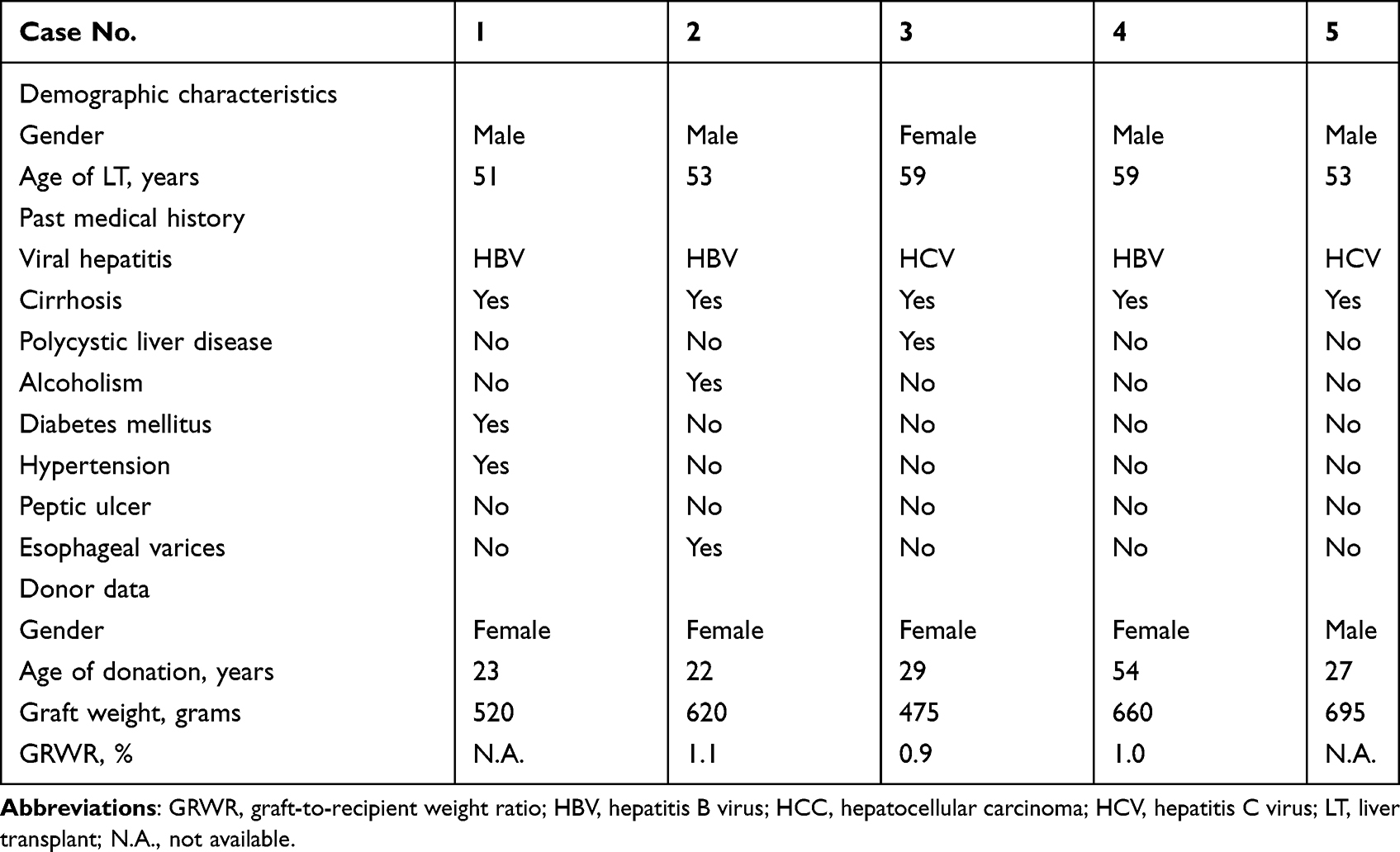 |
Table 1 Demographics (at Transplant) of Liver Transplant Recipients with Delayed HCC Recurrence (Nontumor Factors) |
 |
Figure 1 Flowchart of patient selection. |
Management Before LT
Locoregional therapies were administered prior to LT: TACE (n = 2), ethanol injection (n = 2), RFA (n = 2), and resection (n = 1).
Clinical Characteristics at LT
The median peak serum AFP before LT was 86.1 (range: 7.7–3314.1) ng/mL. Two patients had AFP peak levels within the normal range (<19 ng/mL). On histopathological examination, all explant tumors were stage T1b or T2. Modified Edmondson–Steiner grade was II or III. Two patients had vascular invasion. HCC status in four patients was ultimately classified as beyond the Milan and UCSF criteria. Tables 1 and 2 present the detailed histopathological data.
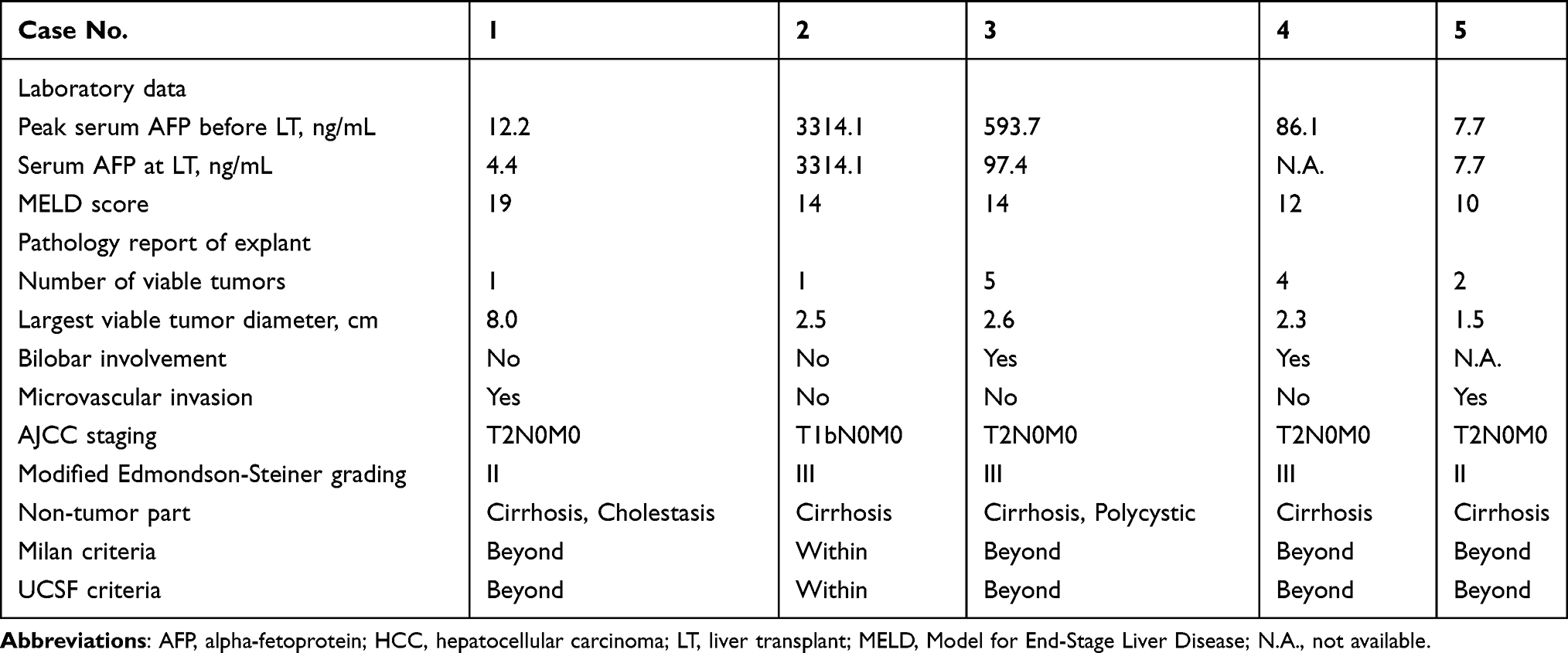 |
Table 2 Demographics (at Transplant) of Liver Transplant Recipients with Delayed HCC Recurrence (Tumor Factors) |
Follow-Up After LT
Immunosuppression protocols were reviewed. FK506 was administered to all patients, and the serial blood concentration is presented in Figure 2A. Mycophenolate mofetil (MMF) was regularly given, except in Case 4. Other immunosuppressants included the short-term perioperative use of basiliximab and steroids.
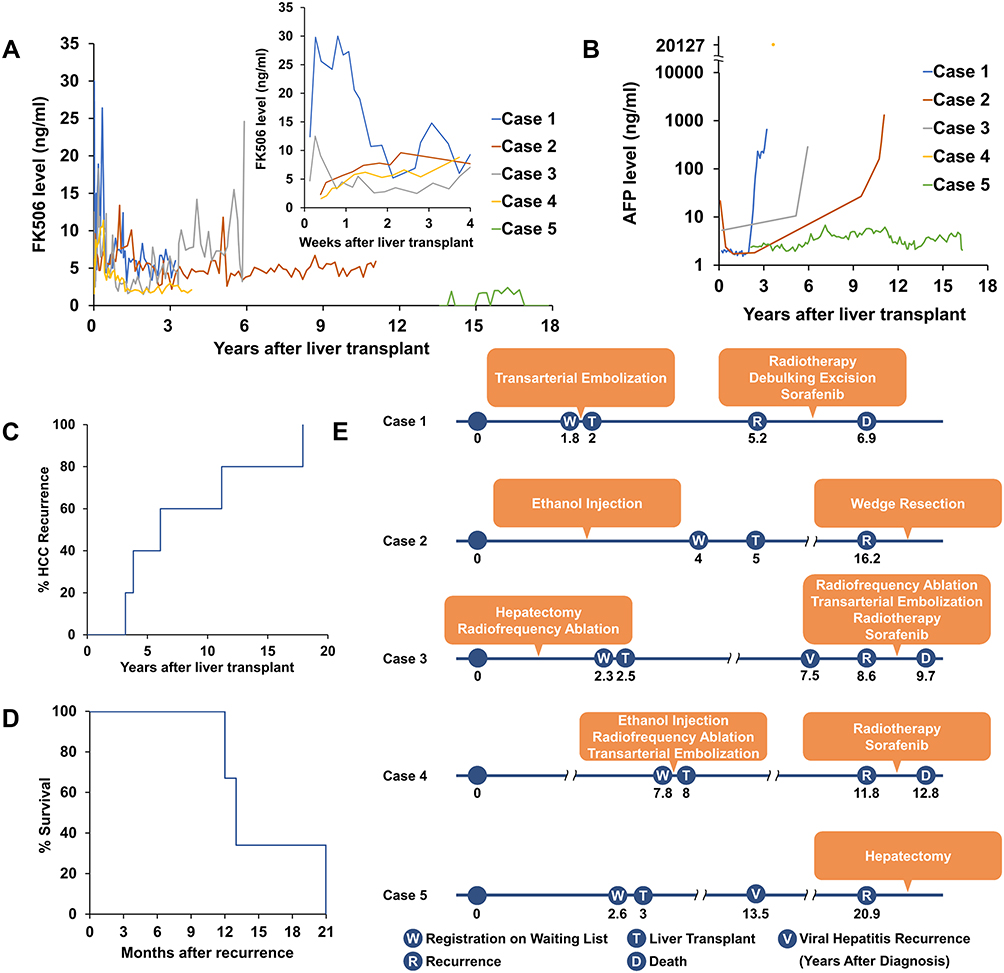 |
Figure 2 Clinical features of liver transplant recipients with delayed HCC recurrence. (A) FK506 level from liver transplant to recurrence (left) and FK506 level in the first month after liver transplant (right). Data of case 5 is incomplete because of the lack of regular follow-up of FK506. (B) Alpha-fetoprotein (AFP) level from liver transplant to recurrence. Data of case 4 is incomplete because of the lack of regular follow-up of AFP. Patient 4’s AFP level at recurrence was 20,127.2 ng/mL. (C) Hepatocellular carcinoma recurrence probability > 3 years after liver transplant. (D) Overall survival after recurrence. (E) Clinical course after the diagnosis of hepatocellular carcinoma. |
Two patients had recurrent hepatitis C infections after LT. Figure 2B illustrates the changes in serum AFP level. Generally, serum AFP considerably increased with time, and HCC recurrence was diagnosed approximately 1 year after the increase. The median recurrence time was 6.1 (range: 3.2–17.9) years, with two cases having a recurrence time of >10 years and one case with recurrence at almost 18 years (Figure 2C). The first identified recurrence site was extrahepatic in three cases, including the bone (n = 2) and lung (n = 1). Recurrences eventually occurred in the bone (n = 4), liver (n = 3), lung (n = 2), and brain (n = 1). Overall, we have two extrahepatic recurrences, one intrahepatic recurrence, and two mixed extrahepatic and intrahepatic recurrence. HCC recurrence involved multiple sites in three cases.
Three patients underwent surgical therapy for HCC recurrence, including pelvis debulking excision (n = 1), lung wedge resection (n = 1), and hepatectomy (n = 1). Systemic sorafenib was administered to three patients. Other managements for the recurrence included TACE (n = 1), RFA (n = 1), and radiotherapy (n = 3).
The median postrecurrence survival was 13.5 (range: 12–21) months, with an estimated 6-, 12-, 18-, and 24-month survival following recurrence of 100%, 100%, 33%, and 0%, respectively (Figure 2D). Two patients were still alive (40%) at the last follow-up, with one 13.5-month survivor and one 16.5-month survivor. Detailed clinical information on follow-up after LT is listed in Table 3. Case 4 received no regular follow-up for AFP and Case 5 received no regular follow-up for FK506 during the time between LT and HCC recurrence.
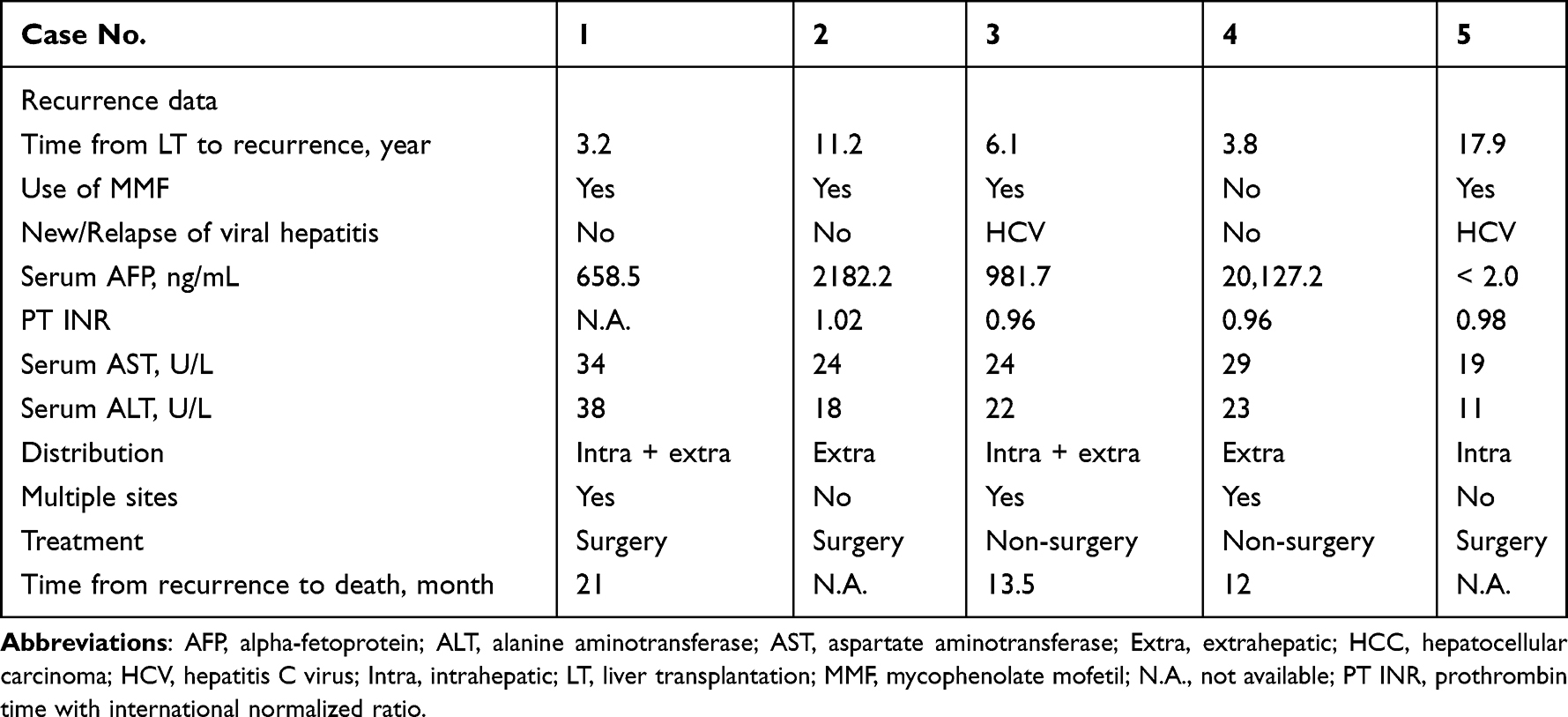 |
Table 3 Demographics (at Recurrence) of Liver Transplant Recipients with Delayed HCC Recurrence |
Course of Each Patient
The disease course for each patient before and after LT is presented in Figure 2E and summarized below.
Case 1
A 51-year-old man had cirrhosis and hepatitis B infection. In an annual health examination, an HCC lesion was noted. He received TACE, followed by LT. There was one tumor, 8 cm in diameter, with vascular invasion in the explant liver. The nontumor part had cirrhosis and cholestasis. The donated liver was donated voluntarily by the patient’s daughter.
About 3 years after LT, pain in the buttocks was noted. A mass lesion involving the right ischial bone and pubic bone was revealed, and a diagnosis of HCC recurrence was made. The patient underwent debulking excision. Pain was relieved after surgery. He was able to walk by himself with the help of physical therapists. Radiotherapy and sorafenib were also administered. No obvious adverse drug reaction was noted. However, approximately 20 months later, multiple metastases were found in the liver, bilateral lungs, and brain. He then died of cancer 21 months after HCC recurrence.
Case 2
A 53-year-old man had a history of cirrhosis, alcoholism, and hepatitis B infection. A hepatic tumor was found in the routine follow-up for cirrhosis. After the diagnosis of HCC, he received an ethanol injection, but progressed elevation of liver enzymes and bilirubin was noted. Therefore, LT was suggested. A tumor, 2.5 cm in diameter, without vascular invasion was found in the explant liver. Case 2 was the only one with explant tumors within the Milan criteria and UCSF criteria. The donated liver was donated voluntarily by the patient’s daughter.
During follow-up, general conditions had been good. About 11 years after LT, persistent elevation of AFP level was noted. CT was arranged and revealed a 1.9-cm solid nodule in the left lung, which was later diagnosed as HCC recurrence. Consequently, a video-assisted left upper lung wedge resection was performed. He recovered well after the surgery. He was alive at the end of the study (13.5 months postrecurrence).
Case 3
A 59-year-old woman had cirrhosis, polycystic liver disease, and hepatitis C infection. She also had early-stage breast cancer and had undergone modified radical mastectomy and chemotherapy more than 20 years ago. HCC was found in routine follow-ups for cirrhosis. Hepatectomy and RFA were performed, but HCC recurrence was found near major vessels, so LT was suggested. Pathology reports of the explant liver noted five tumors with the largest tumor diameter of 2.6 cm and bilobar involvement. The donated liver was donated voluntarily by the patient’s niece (fifth degree relative).
Recurrent hepatitis C (HCV) was detected very early after transplantation, and liver panels were normal during follow-up. Treatment with direct-acting antiviral agents (DAA) (ombitasvir, paritaprevir, ritonavir and dasabuvir) was initiated about 5 years after LT, when these drugs became available in Taiwan. The treatment lasted for about half a year, and HCV viral load became undetectable. Six years after LT (4 months after completion of DAA treatment), CT revealed a 3.5-cm lesion in the liver and TACE and RFA were performed. Later, multiple recurrent lesions appeared in the liver in follow-up. Besides, a 6-cm tumor over the rib of the lower chest was found, so radiotherapy was given. Sorafenib was also administered but then discontinued due to lethargy after the use of the drug. Cancer death occurred 13 months after HCC recurrence.
Case 4
A 59-year-old man had cirrhosis and hepatitis B infection. He had received ethanol injection, RFA, and TACE before LT. In the explant liver, there were four tumors with bilobar involvement. The largest tumor diameter was 2.3 cm. No vascular invasion was noted. The donated liver was donated voluntarily by the patient’s younger sister.
Approximately 4 years after LT, multiple HCC recurrence was observed in the pelvis involving the left iliac crest. Radiotherapy and sorafenib were administered. Later, CT indicated multiple metastases in the multiple thoracic vertebrae. Because of the poor response to target therapy and radiotherapy, the patient preferred supportive care only. He died 12 months after the diagnosis of HCC recurrence.
Case 5
A 53-year-old man had cirrhosis and hepatitis C infection. He underwent LT for severe cirrhosis and liver failure. Surprisingly, two HCC lesions with vascular invasion were noted in the explant liver. The largest tumor diameter was 1.5 cm. The donated liver was donated voluntarily by the patient’s son.
Recurrent HCV was detected very early after transplantation and liver panels were normal during follow-up. Similar to Case 3, HCV treatment was not initiated until DAA became available. Treatment with DAAs (glecaprevir, pibrentasvir) was initiated about 16 years after LT. The treatment lasted for about 2 months, and HCV viral load became undetectable. Almost 18 years after LT (19 months after completion of DAA treatment), a single 2.5-cm HCC tumor was revealed on routine abdominal echography. Hepatectomy was then performed without complications. The nontumor part was cirrhotic. The patient recovered well after the surgery. He was alive at the end of the study (16.5 months postrecurrence).
Discussion
In this study, we focused on recurrences >3 years post-LT, with a median recurrence time of 6.1 (range: 3.2–17.9) years. We reviewed patient profiles to identify possible risk factors for delayed post-LT HCC recurrence. Some possible risk factors shared by our patients are as follows: a medical history of viral hepatitis, explant tumors beyond the Milan criteria (solitary tumor ≤5 cm or 2–3 tumors with none >3 cm)10 or the UCSF criteria (solitary tumor ≤6.5 cm or 2–3 tumors with none >4.5 cm and total tumor diameter ≤8 cm),11 less well-differentiated tumors (modified Edmondson-Steiner grade II–III),12 and administration of immunosuppressants. This study contributes to the literature by providing a comprehensive review of clinical characteristics, and our results warrant further external validation.
A systematic review of 23 studies, including 1921 post-LT HCC recurrence cases, reported the median post-LT HCC recurrence time to be approximately 1.3 years (range: 0.6–2.2).4 While mostly within the first 2 years, some HCC recurrences occur >2 years post-LT. Verna et al suggested different plausible explanations for early and late post-LT HCC recurrences.13 Early recurrences could occur due to undetected extrahepatic metastases that may be present before LT and owing to circulating HCC clones engrafting and growing in a target organ after LT.13 Late recurrences (including delayed recurrence) could be a result of a second unknown hit, leading to late engrafting of HCC cells that are less in number and remain latent for a long time after LT.13
Immunosuppressants affect the integrity of the immune system, which leads to the escape of mutated cells and viral infections from immunosurveillance. Currently, calcineurin inhibitors are the backbone of immunosuppression protocols in LT. In vitro studies and animal models have shown that a high dosage of calcineurin inhibitors can upregulate tumor development through several pathways involving transforming growth factor β or Rho/Rho associated kinase.14,15 Moreover, calcineurin inhibitors are related to pancreatic β-cell apoptosis and impaired insulin secretion.16–18 Consequently, they can cause diabetes mellitus, which is a recognized risk factor for HCC.19 In fact, high exposure to calcineurin inhibitors within the first 30 days, but not thereafter, has been reported to nearly triplicate the risk of HCC recurrence.20 Additionally, the use of mammalian targets of rapamycin inhibitors is highly recommended based on previous studies, but further trials are warranted to generate robust evidence to guide the clinical use of these regimens.4 Whether immunosuppressant is also a risk factor for delayed post-LT HCC recurrence must be further studied.
Recurrent HCV after LT was detected in case 3 and case 5, and the time elapsed between completion of DAA treatment and HCC diagnosis was 4 and 19 months, respectively. While some previous studies suggested an increased HCC recurrence rate with DAA treatment,21 subsequent studies showed that DAA treatment is not associated with increased recurrence for HCC.22–24 A study comprising 3 large prospective multicenter cohorts showed that there was no evidence to suggest that DAAs heighten the risk of HCC recurrence, notably following curative HCC treatment including LT.25 A meta-analysis revealed that DAA treatment significantly reduces the risk of HCC recurrence compared to an interferon regimen and no intervention.26
The median survival time for post-LT HCC recurrences is 12 (range: 6–30) months.4 A nationwide cohort analysis in Taiwan reported that the 1- and 2-year postrecurrence survival rates were 57% and 35%, respectively.3 The survival rate of late recurrence (>2 years) cases seems to be prolonged (median 14.3 months; interquartile range, 6.6–32.6). This is consistent with studies that have shown that a longer time to recurrence is associated with higher postrecurrence survival.4 Almost all such studies (n = 13) compared the early and late recurrence groups, although the cutoff point to define late recurrence varied: 9 months (n = 1), 1 year (n = 8), 2 years (n = 3), and 3 years (n = 1).4 The correlation between shorter recurrence times and poor survival may be explained by original HCC cells circulating in the body and triggered by immunosuppressive therapy to develop tumor.4
In addition to prolonged survival, our cohort also exhibited a tendency of distal metastases, with four extrahepatic HCC recurrences and three involving multiple sites. This was consistent with previous studies that have shown that more extrahepatic involvement is seen in late recurrences, whereas more intrahepatic involvement is seen in early recurrences.7,9 This also reflects the difference in tumor biology between early and late recurrences, but the mechanism remains unexplored.
The survival rate of post-LT HCC recurrences is dismal. Curative-intent treatments lead to better long-term survival,5 highlighting the value of early tumor detection. However, no consensus on post-LT HCC recurrence surveillance exists. Because of the tendency toward distal metastases, the American Association for the Study of Liver Diseases (AASLD) guidelines currently recommend chest and abdominal CT scans.27,28 Additionally, elevated serum AFP levels correlate with HCC recurrence, independent of the timing or location of the recurrence.29 However, the intensity of surveillance and the optimal timing and duration are uncertain. A balance is required between the recurrence risk, yield, medical cost, and possible side effects, and several risk stratification models have been developed to guide surveillance. A study reviewed such models and reported that the most frequently employed predictors were serum AFP levels, tumor size, vascular invasion, tumor number, and tumor differentiation.30 Three models were recommended in the systematic review based on the study design, overall quality, simplicity, and external validation and how well a predicted probability of HCC recurrence matches the observed risk at the individual level,30 namely the RETREAT score31 (Mehta, 2016), AFP model32 (Duvoux, 2012), and the score by Decaens,33 2010. Notably, the study end point of these models was 5 years post-LT. The validity of their risk prediction models for recurrence >5 years post-LT remains to be established.
Table 4 presents a summary of the application of these models to HCC recurrence cases. Overall, our patients have a lower score in these models, particularly Patient 5, who scored the lowest in each model and was stratified into a low-risk group in each model. Patient 5 also had the longest recurrence time—nearly 18 years post-LT. In fact, this may be a case of de novo HCC rather than a recurrence of the original HCC cells. Although molecular profiling is required to make a definitive distinction, this case has many similarities to previously reported cases of de novo HCCs after LT. First, de novo HCCs after LT generally appear without distant metastases. Second, the main risk factor for de novo HCC after LT is the recurrence of hepatitis or cirrhosis in the transplanted liver.34 Third, de novo HCCs generally occur after a much longer period than HCC recurrence. The incidence of de novo HCC likely increases over time after LT because of the increasing use of “marginal” livers and cumulative exposure to environmental hepatocarcinogens.34–36 HCC can take decades to develop, with the longest reported recurrence case diagnosed 22 years after LT.34 Immunosuppressive therapy following LT is also a risk factor and may cause accelerated carcinogenesis because HCC usually occurs after approximately 30 years in HCV-infected native livers.34,37
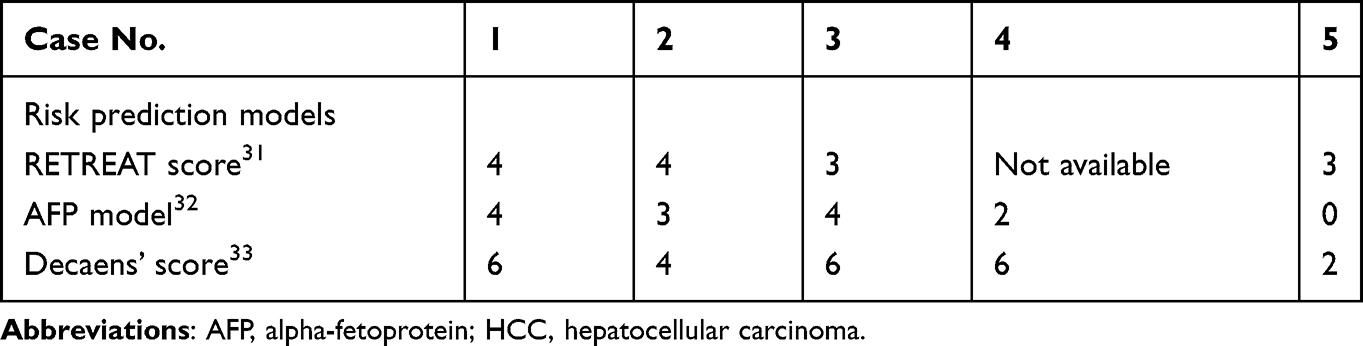 |
Table 4 Application of Risk Prediction Models to Liver Transplant Recipients with Delayed HCC Recurrence |
The use of liquid biopsies as predictors of late recurrence has potential in the future, including circulating tumor cells, circulating cell-free tumor DNA (ctDNA), and extracellular vesicles.38 Several meta-analyses have highlighted the prognostic value of circulating tumor cells in various cancers.38 ctDNA is present in plasma samples of many types of tumors that had not apparently metastasized or released tumor cells into the circulation.39 Notably, circulating tumor cells and ctDNA are extremely rare. By contrast, extracellular vesicles derived from tumor cells are abundant in blood and could potentially be used as biomarkers for prognosis.40,41 Additionally, analysis of molecular biomarkers, including DNA alterations, aberrant gene expression, and microRNA toward HCC risk stratification, although challenging, offers considerable hope.42
This study was limited by the retrospective study design and small sample size. However, the nature of the wide-span interval and rarity in occurrence make conducting a larger scale study or a prospective study difficult. Further multicenter or international collaboration is required to elucidate hazy features.
Conclusions
In our study, 5 of 34 (15%) of cases of post-LT HCC recurrence occurred >3 years after LT, with two occurring after >10 years. Consequently, continual follow-up for HCC recurrence is justified, even after many years. However, the surveillance tool and the intensity of surveillance or optimal timing and duration are uncertain, especially for HCC recurrence >3 years post-LT. Further studies are warranted to characterize such patients and clarify the biological mechanisms that facilitate personalized follow-up strategies in these patients.
Abbreviations
AFP, alpha-fetoprotein; CT, computed tomography; ctDNA, cell-free tumor DNA; GRWR, graft recipient weight ratio; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; LT, liver transplant; MELD, Model for End-Stage Liver Disease; MMF, mycophenolate mofetil; PT INR, prothrombin time with international normalized ratio; RETREAT, The Risk Estimation of Tumor Recurrence After Transplant; RFA, radiofrequency ablation; TACE, transarterial chemoembolization; UCSF, University of California San Francisco.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank the coordinator (Ms. Hui-Ying Lin and Ms. Min-Heuy Lin) for their helpful efforts in data collection.
This study was funded by National Taiwan University Hospital (NTUH-MS394). The funder played no role in the study design, data analysis, or manuscript drafting.
The abstract of this paper was presented at the Asian Transplant Week 2021 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Korean J Transplant 2021; 35(Suppl 1): S135-S135:
https://www.koreamed.org/SearchBasic.php?RID=2521341.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Ho CM, Lee PH, Chen CL, Ho MC, Wu YM, Hu RH. Long-term outcomes after resection versus transplantation for hepatocellular carcinoma within UCSF criteria. Ann Surg Oncol. 2012;19(3):826–833. doi:10.1245/s10434-011-1975-x
2. Lee DD, Sapisochin G, Mehta N, et al. Surveillance for HCC after liver transplantation: increased monitoring may yield aggressive treatment options and improved postrecurrence survival. Transplantation. 2020;104(10):2105–2112. doi:10.1097/TP.0000000000003117
3. Ho CM, Lee CH, Lee MC, et al. Survival after treatable hepatocellular carcinoma recurrence in liver recipients: a nationwide cohort analysis. Front Oncol. 2020;10:616094. doi:10.3389/fonc.2020.616094
4. Al-Ameri A, Yu X, Zheng S. Predictors of post-recurrence survival in hepatocellular carcinoma patients following liver transplantation: systematic review and meta-analysis. Transplant Rev. 2022;36(1):100676. doi:10.1016/j.trre.2021.100676
5. Sapisochin G, Goldaracena N, Astete S, et al. Benefit of treating hepatocellular carcinoma recurrence after liver transplantation and analysis of prognostic factors for survival in a large Euro-American series. Ann Surg Oncol. 2015;22(7):2286–2294. doi:10.1245/s10434-014-4273-6
6. Bodzin AS, Lunsford KE, Markovic D, Harlander-Locke MP, Busuttil RW, Agopian VG. Predicting mortality in patients developing recurrent hepatocellular carcinoma after liver transplantation: impact of treatment modality and recurrence characteristics. Ann Surg. 2017;266(1):118–125. doi:10.1097/SLA.0000000000001894
7. Schreibman IR, Bejarano P, Martinez EJ, Regev A. Very late recurrence of hepatocellular carcinoma after liver transplantation: case report and literature review. Transplant Proc. 2006;38(9):3140–3143. doi:10.1016/j.transproceed.2006.08.095
8. Hu Z, Zhou J, Li Z, et al. Time interval to recurrence as a predictor of overall survival in salvage liver transplantation for patients with hepatocellular carcinoma associated with hepatitis B virus. Surgery. 2015;157(2):239–248. doi:10.1016/j.surg.2014.09.018
9. Chok KS, Chan SC, Cheung TT, Chan AC, Fan ST, Lo CM. Late recurrence of hepatocellular carcinoma after liver transplantation. World J Surg. 2011;35(9):2058–2062. doi:10.1007/s00268-011-1146-z
10. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–699. doi:10.1056/NEJM199603143341104
11. Yao FY, Ferrell L, Bass NM, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33(6):1394–1403. doi:10.1053/jhep.2001.24563
12. Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer. 1954;7(3):462–503. doi:10.1002/1097-0142(195405)7:3<462::AID-CNCR2820070308>3.0.CO;2-E
13. Verna EC, Patel YA, Aggarwal A, et al. Liver transplantation for hepatocellular carcinoma: management after the transplant. Am J Transplant. 2020;20(2):333–347. doi:10.1111/ajt.15697
14. Maluccio M, Sharma V, Lagman M, et al. Tacrolimus enhances transforming growth factor-beta1 expression and promotes tumor progression. Transplantation. 2003;76(3):597–602. doi:10.1097/01.TP.0000081399.75231.3B
15. Ogawa T, Tashiro H, Miyata Y, et al. Rho-associated kinase inhibitor reduces tumor recurrence after liver transplantation in a rat hepatoma model. Am J Transplant. 2007;7(2):347–355. doi:10.1111/j.1600-6143.2006.01647.x
16. Øzbay LA, Smidt K, Mortensen DM, Carstens J, Jørgensen KA, Rungby J. Cyclosporin and tacrolimus impair insulin secretion and transcriptional regulation in INS-1E beta-cells. Br J Pharmacol. 2011;162(1):136–146. doi:10.1111/j.1476-5381.2010.01018.x
17. Soleimanpour SA, Crutchlow MF, Ferrari AM, et al. Calcineurin signaling regulates human islet {beta}-cell survival. J Biol Chem. 2010;285(51):40050–40059. doi:10.1074/jbc.M110.154955
18. Chakkera HA, Mandarino LJ. Calcineurin inhibition and new-onset diabetes mellitus after transplantation. Transplantation. 2013;95(5):647–652. doi:10.1097/TP.0b013e31826e592e
19. El-Serag HB, Hampel H, Javadi F. The association between diabetes and hepatocellular carcinoma: a systematic review of epidemiologic evidence. Clin Gastroenterol Hepatol. 2006;4(3):369–380. doi:10.1016/j.cgh.2005.12.007
20. Rodríguez-Perálvarez M, Tsochatzis E, Naveas MC, et al. Reduced exposure to calcineurin inhibitors early after liver transplantation prevents recurrence of hepatocellular carcinoma. J Hepatol. 2013;59(6):1193–1199. doi:10.1016/j.jhep.2013.07.012
21. Conti F, Buonfiglioli F, Scuteri A, et al. Early occurrence and recurrence of hepatocellular carcinoma in HCV-related cirrhosis treated with direct-acting antivirals. J Hepatol. 2016;65(4):727–733. doi:10.1016/j.jhep.2016.06.015
22. Cabibbo G, Petta S, Calvaruso V, et al. Is early recurrence of hepatocellular carcinoma in HCV cirrhotic patients affected by treatment with direct-acting antivirals? A prospective multicentre study. Aliment Pharmacol Ther. 2017;46(7):688–695. doi:10.1111/apt.14256
23. Pawlotsky JM, Negro F, Aghemo A, et al. European Association for the Study of the Liver EASL recommendations on treatment of hepatitis C: final update of the series. J Hepatol. 2020;73:1170–1218.
24. Probst A, Dang T, Bochud M, Egger M, Negro F, Bochud P-Y. Role of hepatitis C virus genotype 3 in liver fibrosis progression--a systematic review and meta-analysis. J Viral Hepat. 2011;18(11):745–759. doi:10.1111/j.1365-2893.2011.01481.x
25. ANRS collaborative study group on hepatocellular carcinoma (ANRS CO22 HEPATHER, CO12 CirVir and CO23 CUPILT cohorts). Lack of evidence of an effect of direct-acting antivirals on the recurrence of hepatocellular carcinoma: data from three ANRS cohorts. J Hepatol. 2016;65(4):734–740. doi:10.1016/j.jhep.2016.05.045
26. Frazzoni L, Sikandar U, Metelli F, et al. Hepatocellular carcinoma recurrence after hepatitis c virus therapy with direct-acting antivirals. a systematic review and meta-analysis. J Clin Med. 2021;10(8):1694. doi:10.3390/jcm10081694
27. Rajendran L, Ivanics T, Claasen MP, Muaddi H, Sapisochin G. The management of post-transplantation recurrence of hepatocellular carcinoma. Clin Mol Hepatol. 2022;28(1):1–16. doi:10.3350/cmh.2021.0217
28. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of liver diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
29. Alshahrani AA, Ha SM, Hwang S, et al. Clinical features and surveillance of very late hepatocellular carcinoma recurrence after liver transplantation. Ann Transplant. 2018;23:659–665. doi:10.12659/AOT.910598
30. AAM Al-Ameri, Wei X, Wen X, et al. Systematic review: risk prediction models for recurrence of hepatocellular carcinoma after liver transplantation. Transpl Int. 2020;33(7):697–712. doi:10.1111/tri.13585
31. Mehta N, Heimbach J, Harnois DM, et al. Validation of a risk estimation of tumor recurrence after transplant (RETREAT) score for hepatocellular carcinoma recurrence after liver transplant. JAMA Oncol. 2017;3(4):493–500. doi:10.1001/jamaoncol.2016.5116
32. Duvoux C, Roudot-Thoraval F, Decaens T, et al. Liver transplantation for hepatocellular carcinoma: a model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology. 2012;143(4):986–94.e3; quiz e14–5. doi:10.1053/j.gastro.2012.05.052
33. Decaens T, Roudot-Thoraval F, Badran H, et al. Impact of tumour differentiation to select patients before liver transplantation for hepatocellular carcinoma. Liver Int. 2011;31(6):792–801. doi:10.1111/j.1478-3231.2010.02425.x
34. Trevisani F, Garuti F, Cucchetti A, Lenzi B, Bernardi M. De novo hepatocellular carcinoma of liver allograft: a neglected issue. Cancer Lett. 2015;357(1):47–54. doi:10.1016/j.canlet.2014.11.032
35. Adam R, McMaster P, O’Grady JG, et al. Evolution of liver transplantation in Europe: report of the European Liver Transplant Registry. Liver Transpl. 2003;9(12):1231–1243. doi:10.1016/j.lts.2003.09.018
36. Angelico M, Cillo U, Fagiuoli S, et al. Liver Match, a prospective observational cohort study on liver transplantation in Italy: study design and current practice of donor-recipient matching. Dig Liver Dis. 2011;43(2):155–164. doi:10.1016/j.dld.2010.11.002
37. Tong MJ, el-Farra NS, Reikes AR, Co RL. Clinical outcomes after transfusion-associated hepatitis C. N Engl J Med. 1995;332(22):1463–1466. doi:10.1056/NEJM199506013322202
38. Sauer S, Reed DR, Ihnat M, Hurst RE, Warshawsky D, Barkan D. Innovative approaches in the battle against cancer recurrence: novel strategies to combat dormant disseminated tumor cells. Front Oncol. 2021;11:659963. doi:10.3389/fonc.2021.659963
39. Bettegowda C, Sausen M, Leary RJ, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med. 2014;6(224):224ra24. doi:10.1126/scitranslmed.3007094
40. Huang T, Deng CX. Current progresses of exosomes as cancer diagnostic and prognostic biomarkers. Int J Biol Sci. 2019;15(1):1–11. doi:10.7150/ijbs.27796
41. Mathew M, Zade M, Mezghani N, Patel R, Wang Y, Momen-Heravi F. Extracellular vesicles as biomarkers in cancer immunotherapy. Cancers. 2020;12(10):2825. doi:10.3390/cancers12102825
42. von Felden J, Villanueva A. Role of molecular biomarkers in liver transplantation for hepatocellular carcinoma. Liver Transpl. 2020;26(6):823–831. doi:10.1002/lt.25731
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
CT-Based Radiomics for the Recurrence Prediction of Hepatocellular Carcinoma After Surgical Resection
Wang F, Chen Q, Zhang Y, Chen Y, Zhu Y, Zhou W, Liang X, Yang Y, Hu H
Journal of Hepatocellular Carcinoma 2022, 9:453-465
Published Date: 23 May 2022
Recurrent Hepatocellular Carcinoma: Patterns, Detection, Staging and Treatment
Papaconstantinou D, Tsilimigras DI, Pawlik TM
Journal of Hepatocellular Carcinoma 2022, 9:947-957
Published Date: 3 September 2022
Portal Venous and Hepatic Arterial Coefficients Predict Post-Hepatectomy Overall and Recurrence-Free Survival in Patients with Hepatocellular Carcinoma: A Retrospective Study
Li YK, Wu S, Wu YS, Zhang WH, Wang Y, Li YH, Kang Q, Huang SQ, Zheng K, Jiang GM, Wang QB, Liang YB, Li J, Lakang Y, Yang C, Li J, Wang JP, Kui X, Ke Y
Journal of Hepatocellular Carcinoma 2024, 11:1389-1402
Published Date: 9 July 2024
Diabetes Mellitus Negatively Impacts Outcomes of HBV-Related Hepatocellular Carcinoma Following Thermal Ablation
Wu KC, Lee IC, Liu CA, Chiu NC, Hsu SJ, Lee PC, Wu CJ, Chi C, Luo JC, Hou MC, Huang YH
Journal of Hepatocellular Carcinoma 2024, 11:2257-2267
Published Date: 19 November 2024
Optimizing Hepatocellular Carcinoma Selection for Liver Transplantation: The Impact of an Integrated MELD-ALBI Score on Post-Transplant Outcomes
Alkhatib A, Gomaa AI, Abdel-Razek W
Journal of Hepatocellular Carcinoma 2026, 13:614920
Published Date: 12 June 2026