Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Treatment Decisions for Stable Chronic Obstructive Pulmonary Disease in China: An Observational Cross-Sectional Survey Based on Multivariate Discrete Choice Modeling
Authors Cui J, Tang C, Li H, Zhou Y, Li S
Received 23 May 2025
Accepted for publication 26 September 2025
Published 29 October 2025 Volume 2025:20 Pages 3483—3494
DOI https://doi.org/10.2147/COPD.S537500
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Jiangyu Cui, Chunli Tang, Hongjia Li, Yumin Zhou, Shiyue Li
Department of Pulmonary and Critical Care Medicine, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China
Correspondence: Shiyue Li, First Affiliated Hospital of Guangzhou Medical University, No. 28 Qiaozhong Zhong Road, Liwan District, Guangzhou, Guangdong, People’s Republic of China, Tel +86-020-81567289, Email [email protected]
Purpose: To understand the current situation of respiratory and community physicians in China regarding the initial treatments for patients with chronic obstructive pulmonary disease (COPD).
Patients and Methods: A multivariate discrete choice model was applied to simulate patients with stable COPD, and an online questionnaire was randomly provided to respiratory physicians and community physicians. The questionnaire responses and medications prescribed to the simulated patients by the doctors in the different groups were analyzed and compared.
Results: (1) This study surveyed 109 doctors who made prescription decisions for 872 simulated COPD patients. (2) The results of the questionnaire revealed that the percentages of LAMA, LAMA/LABA and triple therapies that could be prescribed in community health care centers were 40.6%, 25%, and 34.4%, respectively. More than 60% of the physicians in the CHC and SH groups prescribed ICS/LABA as an initial regimen for maintenance therapy. (3) Triple therapy accounted for the highest proportion of prescriptions at 49%, followed by dual bronchodilator therapy (29.6%), whereas LAMA monotherapy represented the smallest share, with only 4.9% of prescriptions. Notably, ICS/LABA combination therapy represented a clinically relevant proportion of prescriptions (14.3%). A total of 58.9% of the 170 simulated COPD patients without asthma in the current study were prescribed triple therapy by their physicians. Approximately 60% of the COPD patients in Groups A and B were prescribed triple therapy as an initial treatment regimen, despite blood EOS counts of 100– 300 cells/μL in both groups.
Conclusion: Although most respiratory physicians follow guidelines for the choice of initial therapy for COPD, there are still irregularities in the use of triple therapy. A clinically relevant percentage of physicians, especially community physicians, selected ICS+LABA as the initial treatment choice. These practice irregularities should be the focus of future guidelines for promotion and education.
Keywords: COPD, treatment, cross-sectional survey, multivariate discrete choice modeling
Introduction
Chronic obstructive pulmonary disease (COPD), characterized by persistent airflow limitation from airway/alveolar abnormalities, remains a leading global cause of morbidity and mortality despite being preventable.1 The WHO estimates that the worldwide incidence of COPD is 380 million cases, with projections indicating increasing prevalence due to aging populations.2 In China, epidemiological studies reveal nearly 100 million affected individuals, with COPD ranked as the fifth leading cause of death.3,4 By 2040, COPD is predicted to become the fourth leading cause of mortality worldwide.5
Current COPD management focuses on symptom relief and exacerbation prevention, with long-acting bronchodilators (LAMAs/LABAs) used as cornerstone therapies.6,7 However, the role of inhaled corticosteroids (ICSs) remains contentious. While ICSs reduce exacerbations in patients with elevated eosinophils (EOS≥300 cells/μL), they confer risks, including pneumonia, osteoporosis, and diabetes.8–14 The 2023 GOLD guidelines restrict ICS use to specific subgroups: those with ≥2 moderate or ≥1 severe exacerbations plus EOS≥300 cells/μL or COPD-asthma overlap.1
Real-world practices frequently deviate from guidelines. Although <30% of COPD patients experience frequent exacerbations,15–21 observational studies have shown that 50–80% of COPD patients receive ICS-containing regimens.22–26 Notably, 41.5% of GOLD B patients and 68% of GOLD D patients in Europe received ICS despite limited indications.27 In China, 42.7% of low-risk (GOLD A) patients inappropriately received ICS.28 Systemic overprescription increases adverse events and health care costs.29–31 These discrepancies underscore the need to investigate the drivers of nonadherence to evidence-based recommendations.
This study focused on physicians with extensive experience in managing COPD patients. The aim of this study is to address two critical questions: (1) What are Chinese physicians’ perspectives on primary treatment approaches for COPD? (2) Which patient-specific factors influence their medication prescribing patterns? By answering these questions, we seek to provide actionable insights to bridge the gap between evidence-based recommendations and clinical practice.
Materials and Methods
We invited 110 respiratory medicine specialists and community physicians from different levels of medical institutions (tertiary hospitals, secondary hospitals and community health care centers) in different regions of China to participate in this study. All the physicians surveyed had more than 5 years of practice experience, which included the management and treatment of patients with COPD (≥10 COPD patients managed per month). All the physicians included in this study were divided into the following three groups according to the level of the hospital in which they worked: the community health care center group (CHC group, n=44), the secondary hospital group (SH group, n=33) and the tertiary hospital group (TH group, n=33).
To conduct this survey, a structured online questionnaire was designed and sent to the participating respondents via the internet. The questionnaire consisted of two parts: a survey on the current status of drug accessibility and awareness of commonly used medications for COPD and eight clinical profiles of stable COPD patients with multiple clinical characteristics simulated by multivariate discrete choice modeling (DCM).
In particular, the questionnaire for the current status section consisted of a series of questions about the general situation of the participating physicians (gender, age and education), the level of hospital in which they worked, the number of years they had been in practice, the number of patients with COPD they treated per month, the accessibility of inhaled medication in the hospital in which they worked, the type of guideline they referred to in their diagnostic and therapeutic approach, their perceptions of the main therapeutic drugs used to treat COPD, and the factors influencing the use and discontinuation of ICS.
We determined the characteristics to be used for constructing these simulated patient models on the basis of clinical practice using various clinical indicators relevant to ICS treatment decisions in each of the major diagnostic and treatment guidelines (GOLD Guideline 2023, COPD Diagnostic and Treatment Guideline 2021 revision, and Expert Consensus on the Standardized Management of Glucocorticosteroids for COPD, 2021), including the predicted percentage forced expiratory volume in 1 second (FEV1%pred), modified British medical research council dyspnea scale (mMRC), the number and severity of acute exacerbations in the past year, history of previous pneumonia, peripheral blood EOS count, and history of asthma) and a history of comorbidities such as coronary heart disease and lung cancer. Once the clinical indicators were identified, different levels of values were set according to their characteristics to construct different patient models, as shown in Table 1.
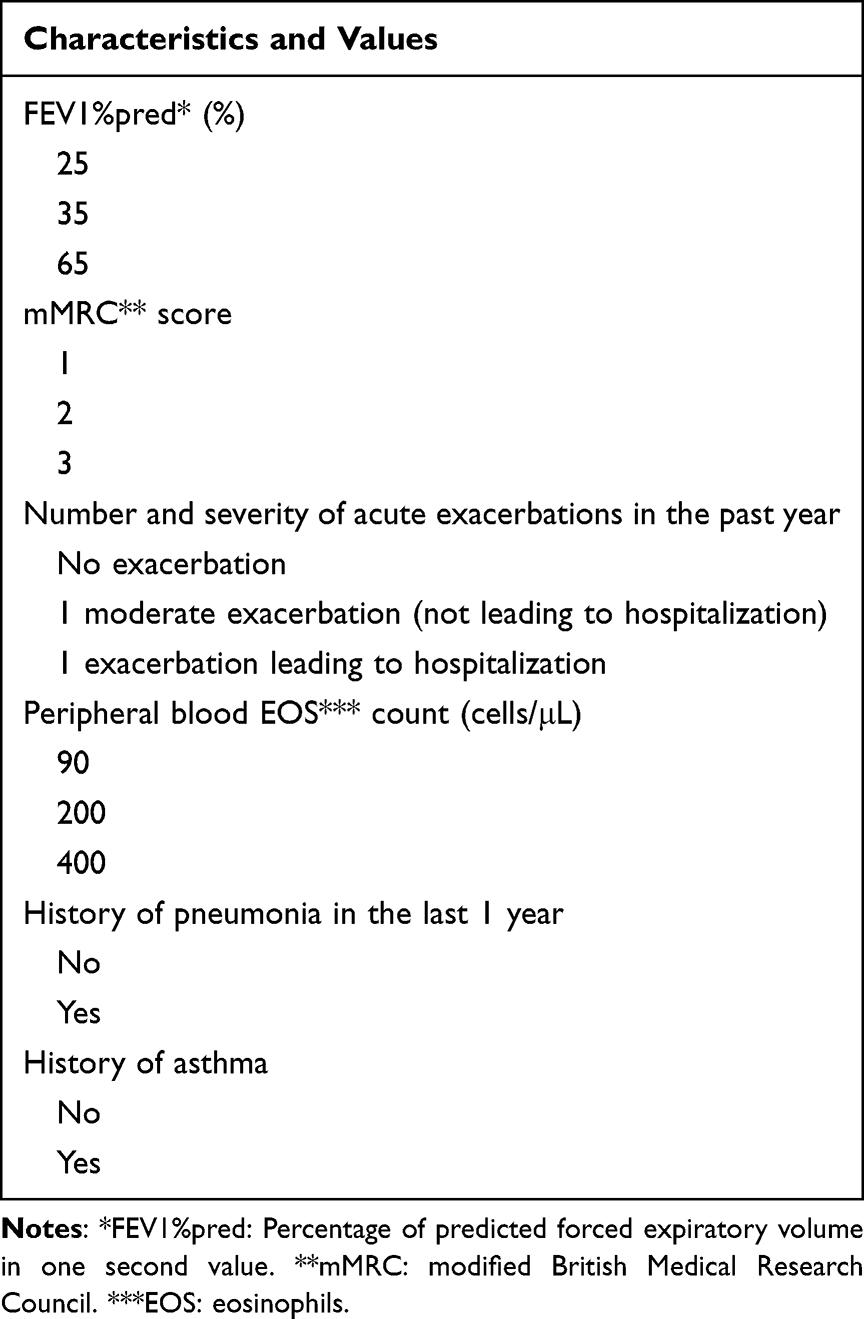 |
Table 1 Characteristics and Specific Values Used to Simulate Patients in Discrete Choice Models |
We have developed a program that allows us to automatically construct simulated patients with a variety of characteristics and values. The patient construction program also automatically assesses (in the background) the subgroups (Group A, B or E) in which the patients are placed based on the patient’s characteristics according to the criteria of the GOLD guideline version 2023; this is done to understand how well the prescribing regimen of the participating physicians aligns with the guidelines. In total, tens of thousands of different patient models can be generated based on the current selection of features and values. The program can also adjust the selection of virtual patient characteristics and values according to the number of respondents and groupings to generate the appropriate number of virtual patients so that a given number of respondents in different groups have access to the same patient data to ensure comparability of results between groups.
All physicians participating in the study were asked to complete questionnaires and then provide the most appropriate initial treatment regimen for simulated COPD patients.
In the present study, continuous variables with a normal distribution are expressed as the mean ± standard deviation, whereas those with a skewed distribution are presented as the median and interquartile range (IQR). Categorical variables are presented as frequencies and percentages. For continuous data comparisons, the independent samples t test was employed for normally distributed data between two groups, and the Mann‒Whitney U-test was used for nonnormally distributed data. Multiple groups were compared (≥3 groups) via the Kruskal‒Wallis H-test. Categorical variables were compared via Pearson’s chi-square test, Fisher’s exact test, or the Mantel‒Haenszel chi-square test, as appropriate. A two-tailed P value <0.05 was considered statistically significant. All the statistical analyses were performed via SPSS statistical software version 26.0 (IBM Corp).
The study protocol was reviewed and fast-track ethics approved by the First Affiliated Hospital of Guangzhou Medical University research ethics committee because this study was a survey of health care professionals, not patients (Ethics approval number: ES-2023-K028-01) (Clinical trial registration number: MR-44-25-059474). The ethics committee granted a waiver of informed consent based on the following considerations: (1) The research exclusively involved physicians as participants through structured questionnaires, with all collected data anonymized using non-interventional clinical research coding systems; (2) The patient cases presented in the survey were computer-generated virtual scenarios that contained no real patient data or personally identifiable information; (3) As a non-interventional study, it did not involve any clinical interventions, investigational drugs, or modifications to existing treatment regimens. The exemption from obtaining informed consent was formally documented in the original ethics approval documents (available upon request). This study strictly adhered to the ethical principles outlined in the Declaration of Helsinki.
Results
Descriptive Results
A total of 110 physicians were invited to participate in this study from January 1 to January 31, 2024; 109 physicians completed the survey by the study cutoff date, with one physician dropping out.
Among the 109 physicians who completed the survey, 49 (45.0%) were male, and 60 (55.0%) were female. The mean age of all the participating physicians was 40.8 ± 7.6 years, with the youngest being 24 years and the oldest being 65 years. The average number of years in practice for all the participating physicians was 15.4 ± 9.1 years. There was no significant difference in age or years of practice among the three groups of physicians. The average number of patients with COPD managed per month by physicians in the CHC group was 17.6 ± 6.1, which was significantly lower than that in the other two groups. Significant differences were also found in the educational backgrounds of the three groups of physicians.
The results of the comparison of the general data of the three groups of physicians, after they were grouped according to the level of the hospital in which they worked, are detailed in Supplementary Information 1.
Questionnaire Results
The status section questionnaire used in this study contained nine questions and covered multiple issues and results. Therefore, only a subset of the results and questions is presented in this publication; the rest can be found in the supplementary material. The choices made by all the participating physicians in response to the items on the questionnaire are presented in Supplementary Information 2.
According to the physicians’ responses to the questionnaire, the percentages of LAMA, LAMA/LABA and triple therapies that could be prescribed in community health care centers were 40.6%, 25%, and 34.4%, respectively. In the SH group, the proportions of prescriptions for the above three drugs were 66.7%, 81.3% and 78.1%, respectively. In the TH group, these proportions were 86.4%, 95.9% and 90.9%, respectively.
In addition, physicians in the SH group and TH group primarily referred to the new version of the GOLD guidelines when treating COPD (84.8% and 95.5%), whereas a proportion of physicians in the CHC group also referred to the Chinese primary care guidelines32 (12.5%) and the Chinese guidelines for the diagnosis and treatment of COPD33 (31.3%).
More than 60% of the physicians in each group agreed that LAMA therapy was the first-line treatment for COPD, but fewer than half of the physicians in each group agreed that LAMA therapy alone was the most effective treatment for most COPD patients.
Fifty percent of the physicians in the CHC group agreed that “LABA/ICS is the most effective initial treatment option for the majority of patients with COPD”, and only 21.9% agreed that “only certain patients with COPD can benefit from ICS-containing therapy”. In the TH group, these percentages were 25% and 75%, respectively. More than 60% of the physicians surveyed in all three groups recognized LABA/LAMA as the most effective initial treatment for the majority of patients with COPD.
When asked about triple therapy, 53.1% and 42.4% of the physicians in the CHC and SH groups, respectively, considered upgrading to triple therapy in the event of poor COPD control with LAMA therapy. However, only 22.7% of the physicians in the TH group chose this option. The blood EOS count was selected as an indicator to guide triple therapy decisions by more than 80% of the physicians in all three groups.
Multivariate Discrete Choice Experiment Results
In the multivariate discrete choice experiment part of the study, the three groups of physicians made prescribing decisions and drug use recommendations for a total of 872 virtual patients (each physician assessed 8 virtual patients). At the end of the study, we categorized all of the above virtual patients into Groups A, B and E according to the criteria of the 2023 edition of the GOLD guidelines, and data on the main characteristics of the patients in each group are presented in Table 2.
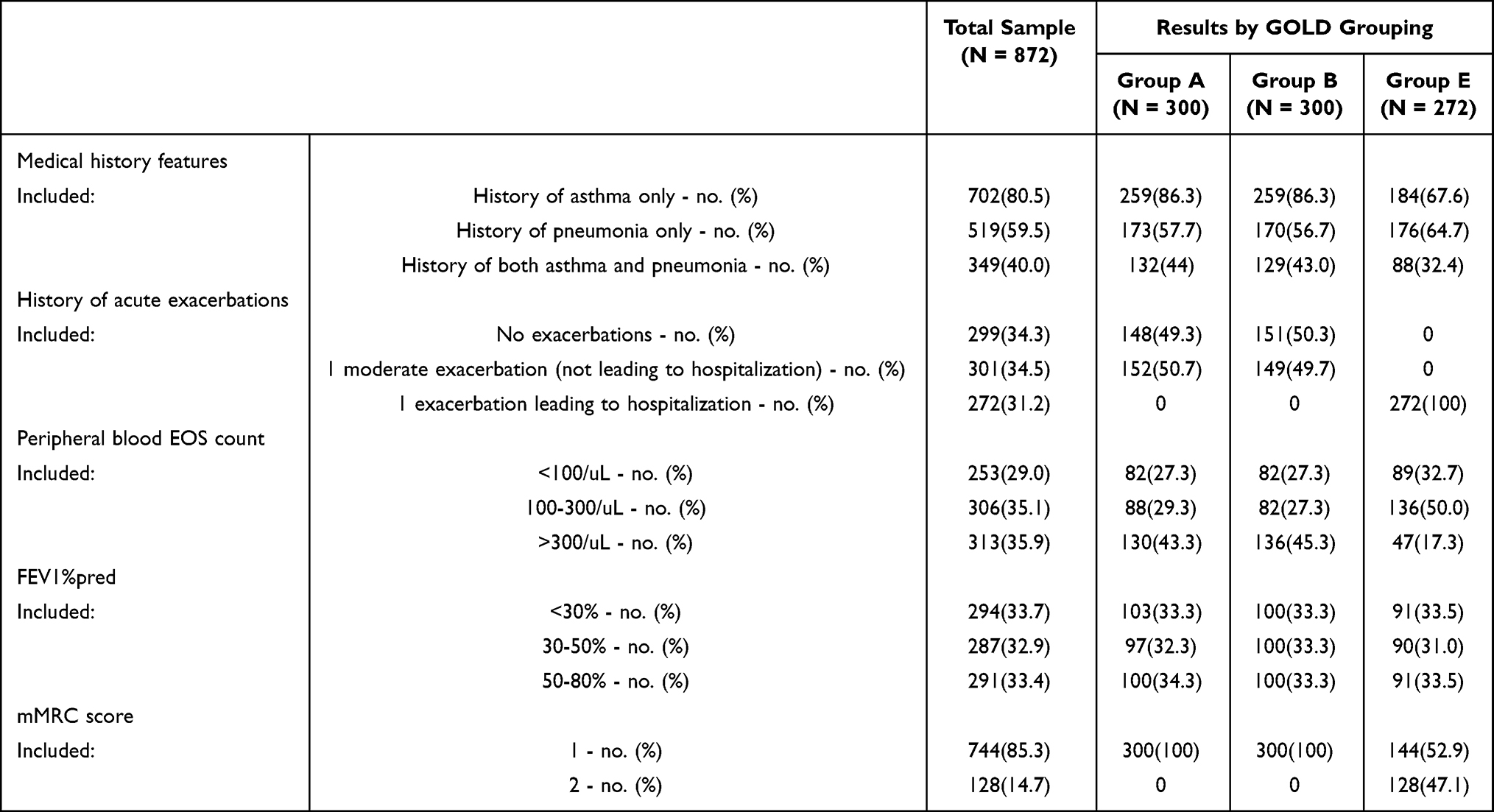 |
Table 2 Distribution of the Clinical Characteristics of Virtual Patients in Different GOLD Subgroups |
Aggregation of the prescribing decisions of all physicians for each patient in the different GOLD groups revealed that triple therapy had the highest proportion of prescriptions, representing nearly half of all prescriptions (49.9%), with more than half of these prescriptions (55.0%) made for patients in Group B. The proportion of prescriptions for LAMA therapy alone was 4.9%, with 5.7% in Group A and 3.0% in Group B. The second-most prescribed drug was the dual bronchodilator, representing 29.6% of total prescriptions, with prescription rates of 26% and 29.3% in Groups A and B, respectively. ICS/LABA was the third-most commonly prescribed drug, representing 14.3% of the total prescriptions. The detailed data are presented in Table 3.
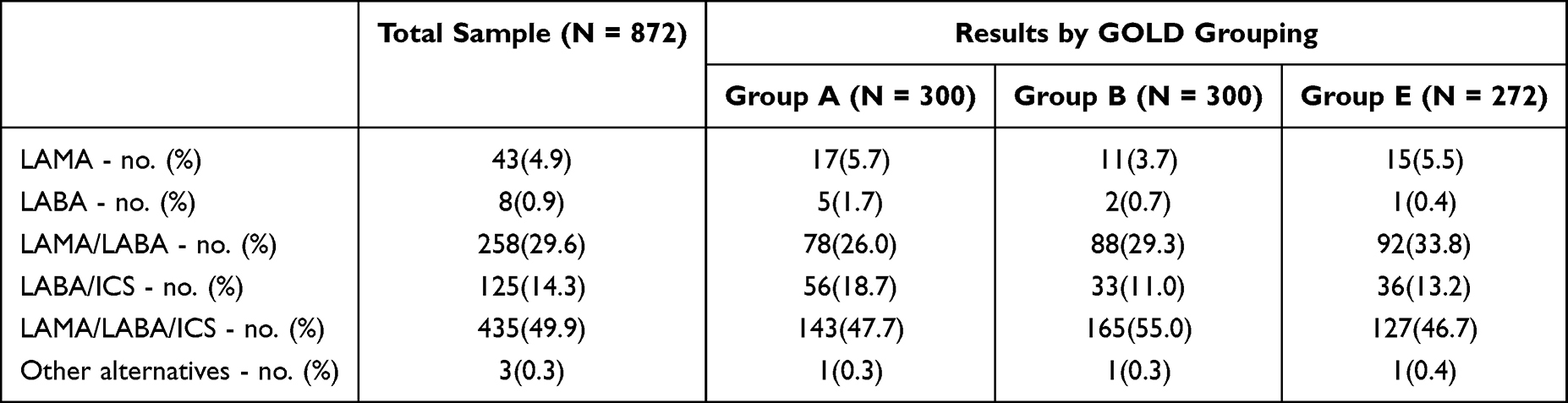 |
Table 3 Prescribing Decisions for Virtual COPD Patients with Different GOLD Groupings |
In a subgroup analysis of virtual patients with different medical histories and blood EOS counts, 58.4% and 67% of all physicians, respectively, prescribed triple therapy as the initial treatment regimen when blood EOS counts were in the range of 100–300/µL in Group A and Group B patients without asthma. The guideline-recommended LAMA drug was prescribed to only 4.9% of patients in Group A. LABA/LAMA, the guideline-recommended drug treatment for Group B, was prescribed to only 14.6% of Group B patients. The detailed data are presented in Table 4.
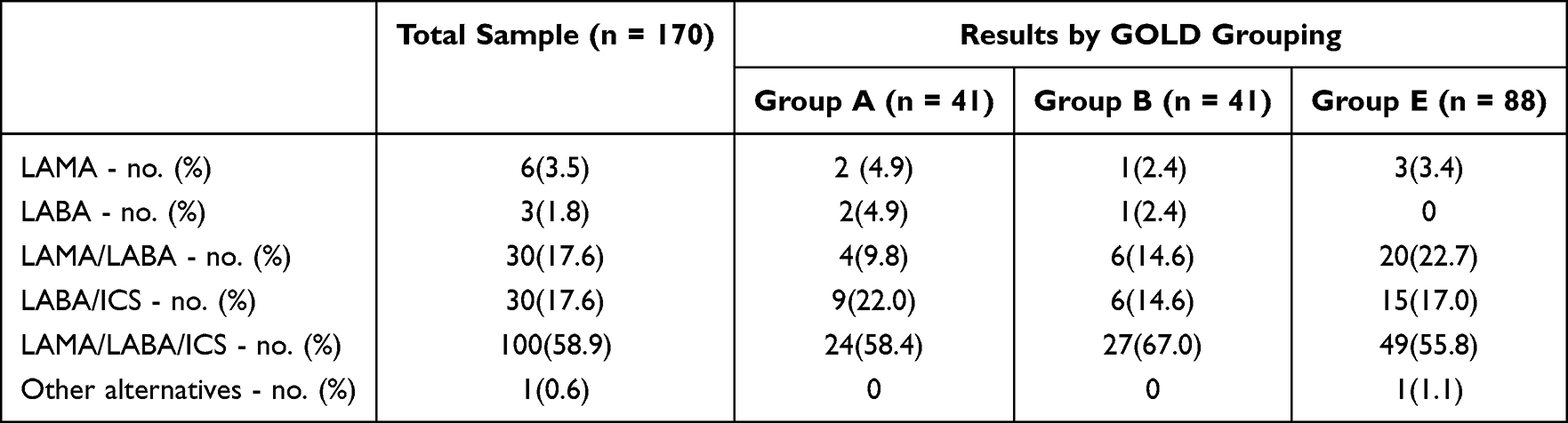 |
Table 4 Prescribing Decisions for Virtual COPD Patients Without Asthma with Different GOLD Groupings |
With respect to the prescribing decisions of physicians in each group of patients without asthma in GOLD Group A, the highest proportion of prescriptions for triple therapy were made by physicians in the TH group (70.6%), and the lowest were made by physicians in the CHC group (41.7%). Physicians in the TH group prescribed ICS-containing medicines for 94.1% of the patients. In contrast, among patients without asthma in Group B, the highest proportion of triple therapy prescriptions was made by physicians in the SH group (75%), and the lowest proportion was made by physicians in the TH group (58.3%). Among patients in Group B, the proportion of ICS-containing medicines prescribed by physicians was also highest in the TH group (88.2%).
Patients in Group E without asthma were further divided into two subgroups according to their blood EOS count (blood EOS count 100–300/µL and >300/µL). For all patients with blood EOS counts >300/µL, physicians in the TH group prescribed ICS-containing medications, with 83.3% of these physicians prescribing triple therapy. A total of 92.9% of the physicians in the CHC group prescribed ICS-containing medications, with 78.6% of these physicians prescribing triple therapy. Among the three groups, the lowest proportion of physicians prescribed ICS-containing medications and triple therapy (80% and 60%, respectively). In contrast, among patients with blood EOS counts of 100–300/µL, the LABA/LAMA regimen was the initial treatment chosen by the highest proportion of physicians in the SH and TH groups (50% and 47.1%, respectively), compared with 25% of physicians in the CHC group. In all three groups, ICS-containing drugs were chosen by 66.7% of the physicians in the CHC group, compared with 50% and 41.2% of the physicians in the SH and TH groups, respectively (Figure 1).
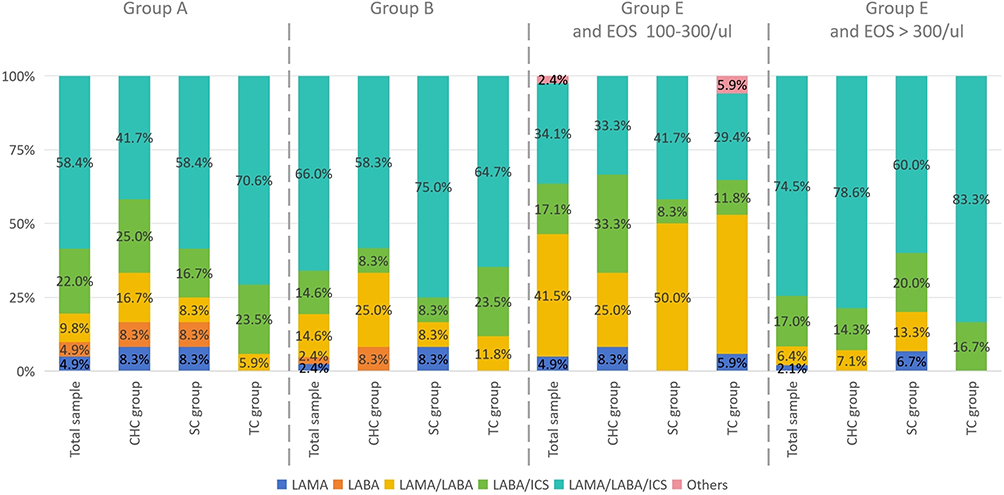 |
Figure 1 Prescribing decisions for virtual COPD patients without asthma with different GOLD groupings and blood EOS counts. |
More than 60% of all COPD patients with comorbid asthma in this study were prescribed ICS-containing medications, with 47.7% prescribed triple therapy and another 32.5% prescribed dual bronchodilator therapy. Among patients in the different GOLD subgroups, the proportion of prescriptions for dual bronchodilator therapy was highest among patients in Group E (39.1%), whereas the proportion of prescriptions for triple therapy was highest among patients in Group B (53.3%) (Figure 2).
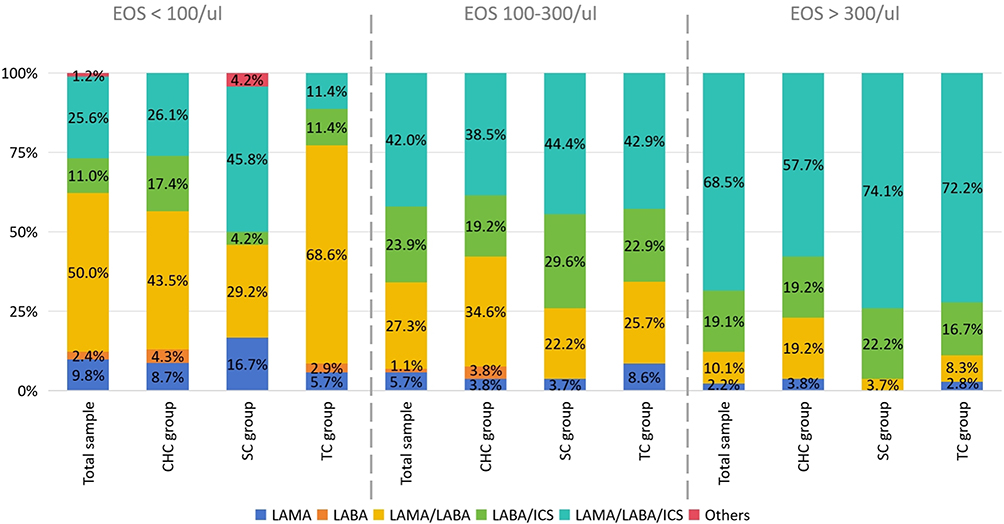 |
Figure 2 Prescribing decisions for virtual COPD patients in GOLD Group A with asthma. |
To understand the specific prescribing decisions made by physicians in each group, we continued to perform subgroup analyses according to the GOLD group and patient characteristics such as the blood EOS count. First, when analyzing the prescribing decisions made for COPD patients in the GOLD A group who had asthma, if the patients had a blood EOS count >300/ul, the proportion of physicians prescribing ICS-containing medications was greater in the SH and TH groups (96.3% and 88.9%, respectively), and the proportion prescribing triple therapy was also greater (74.1% and 72.2%, respectively). When patients had a blood EOS of 100–300/µL, the proportion of physicians prescribing each drug was similar in all three groups, with the proportion of physicians prescribing triple therapy being approximately 40%. When the patients’ blood EOS count was <100/µL, the highest proportion of physicians in the TH group chose dual bronchodilator therapy (68.6%), whereas physicians in the SH group preferred triple therapy (45.8%). Similar decision-making patterns to those for Group A patients were also observed for GOLD B COPD patients who had asthma. However, physician decision-making was more consistent in all three groups when the patient’s blood EOS count was >300/µL, with approximately 70% of all physicians prescribing the triple combination (Figure 3).
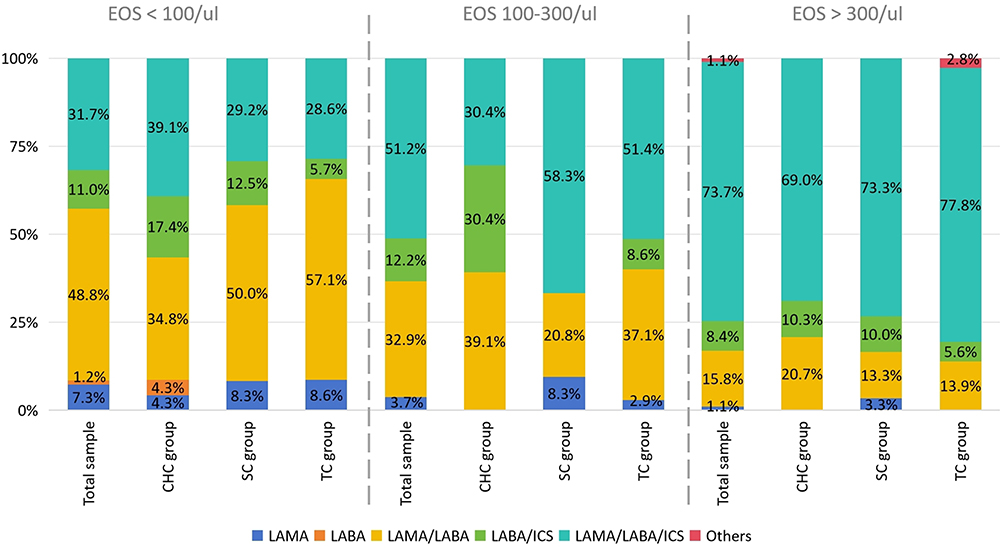 |
Figure 3 Prescribing decisions for virtual COPD patients in GOLD Group B with asthma. |
The GOLD Group E patients with comorbid asthma in this study could be divided into two subgroups on the basis of blood EOS counts of 100–300/µL and <100/µL. In the EOS 100–300/µL group, physicians preferred triple therapy (56.8%), whereas in the EOS <100/µL group, dual bronchodilator therapy was the most commonly selected treatment (53.9%) (Figure 4).
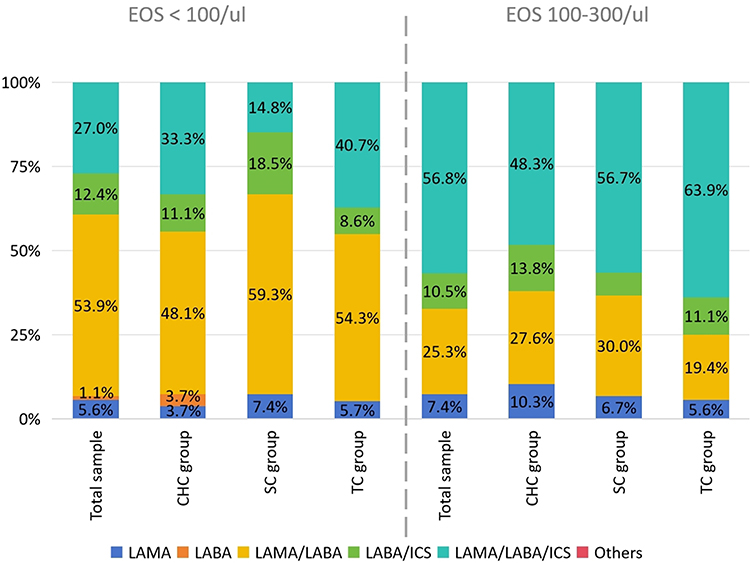 |
Figure 4 Prescribing decisions for virtual COPD patients in GOLD Group E with asthma. |
Discussion
From the questionnaires in this study, we found that LAMA, LAMA/LABA and triple therapy, which are the most commonly used treatments for COPD recommended by the current GOLD guidelines, were not prescribed in more than 50% of the community health care centers. In CHCs, the ICS/LABA and ICS regimens remain the primary treatments for COPD. In particular, the proportion of dual bronchodilator and triple therapy for Group E patients is insufficiently low in CHCs, which may leave CHCs with inadequate medication for long-term management of this patient group. When examining the guidelines that physicians most often refer to when prescribing treatment, the main reference for physicians in the SH and TH groups was the new version of the GOLD guidelines, whereas a proportion of physicians in the CHC group referred to national primary care guidelines and guidelines for the diagnosis and treatment of COPD. As the GOLD recommendations are updated once a year, compared to the less frequent updating of the national guidelines, this situation may also have led to differences in the selected treatment options among the three groups of physicians. A similar situation has been reported in other studies. In 2015, Davis et al34 conducted a study of physician knowledge and implementation of GOLD treatment recommendations and reported that 58% of primary care physicians reported being aware of the GOLD recommendations, whereas 93% of pulmonologists reported being aware of the recommendations. Our survey also found that only 68.2% of the physicians would stop using ICSs if there was no indication for their use. A 2019 study also revealed that merely 55% of COPD patients treated with ICSs met the criteria for recommended discontinuation.35 These findings suggest that physicians need to improve their treatment approach in accordance with the latest guidelines for treating COPD.
In the present study, in response to the questionnaire about the ICS/LABA regimen, more than 60% of the physicians in the CHC and SH groups recognized that ICS/LABA as an initial maintenance therapy is effective in preventing acute exacerbations in patients with COPD. However, the new 2024 GOLD guidelines no longer recommend prescribing LABAs/ICSs to patients with COPD and prefer the LABA/LAMA/ICS regimen if ICS treatment is indicated, as triple therapy has been shown to be superior to LABA/ICS treatment in several studies. In addition, 14.3% of all physicians surveyed had LABA/ICS as their preferred treatment option in the multivariate discrete choice experiment. In the previous questionnaire, we reported that a small number of physicians in the CHC and SH groups referred to national guidelines for the treatment of COPD, which were updated relatively slowly. In these guidelines, LABAs/ICSs are listed as one of the recommended regimens to treat some COPD patients. This situation may have led to these differences in the choice of treatment among the physicians in the three groups.
We also found that 58.9% of the 170 COPD patients without asthma in the current study were prescribed triple therapy by their physicians. This percentage was even higher than the proportion of triple therapy prescribed to all patients (49.9%). In particular, approximately 60% of the COPD patients in Groups A and B were prescribed triple therapy as an initial treatment regimen, despite blood EOS counts of 100–300 cells/µL in both groups. The GOLD 2023 recommendation for the ICS has been revised from “consider use” to “favor use” for patients with a blood EOS count of 100-–300 cells/µL. However, the GOLD guidelines also caution that the use of blood EOS counts to predict the impact of ICS should always be used in conjunction with a clinical assessment of the risk of exacerbation (eg, history of acute exacerbation). Neither Group A nor Group B COPD patients in this study had a history of severe acute exacerbations leading to hospitalization; thus, we believe that there may be misuse of triple therapy in this group of patients. Such inappropriate use of triplet therapy in Group A and B patients also occurs in clinical practice. In a recent study of a German COPD cohort,36 two-thirds of the patients in the GOLD A and B groups received ICS. A recent study in Denmark reported that 39–55% of GOLD stage B patients were treated with ICS-containing drugs.37 This finding reflects the fact that physicians are not always accurate in determining the clinical risk of Group A or Group B patients with COPD. Physicians may inappropriately adopt an unnecessary conclusions regarding the patient’s complex history or laboratory parameters, or they may be overly conservative in their assessment, leading to a false amplification of the patient’s own risk and the adoption of inappropriate treatment regimens.
The GOLD guidelines state that patients with COPD who also have asthma should be treated with ICS. However, in the present multivariate discrete choice study, we found that physicians did not prescribe ICS-containing therapies to all COPD patients with comorbid asthma. By analyzing subgroups of COPD patients with comorbid asthma, we identified a common pattern in the way physicians prescribe medicines. One of the main reasons for this phenomenon may be changes in blood EOS counts in people with COPD. A possible explanation is that a blood EOS count of less than 100/µL raises concerns among physicians about the efficacy of ICS therapy, leading to a conflict in their choice of medication, which results in the abandonment of ICS and the selection of a dual bronchodilator. These findings also suggest that the blood EOS count interferes with the dosing regimen of COPD patients with comorbid asthma, in addition to affecting the prescription of triple therapy.
Our findings reveal persistent gaps between COPD guideline recommendations and real-world prescribing, particularly concerning inappropriate triple therapy use in low-risk patients. To address these, we propose actionable strategies targeting key stakeholders. For physicians, especially in community health centers where limited drug access prevails, targeted continuing medical education should prioritize blood eosinophil-guided ICS decision-making, emphasizing discontinuation when eosinophils <100 cells/μL and pneumonia risks from unnecessary ICS. Healthcare systems should embed guideline-concordant prescribing metrics into quality audits, particularly auditing Group A/B patient regimens where overtreatment is prevalent.
Our study has several limitations. First, the small sample size of physicians included in our current study does not fully reflect the characteristics of the overall prescribing behavior of pulmonologists and general practitioners in China. Second, in this study, we were limited by the sample size of the physicians and did not include all combinations of patients in the multivariate discrete choice experiments (especially COPD patients in Groups A and B who did not have comorbid asthma in other possible combinations); this resulted in an inability to derive the overall characteristics of prescribing behavior for the entire population of COPD patients. All of these limitations must be addressed by future research studies with larger sample sizes. In addition, the characteristics of the patients whom physicians encounter in real-life settings are much more diverse, and our multivariate discrete choice experiments select only some of the common clinical characteristics; these characteristics do not fully reflect the true patient situation, which will need to be explored by conducting larger experiments incorporating a larger number of patient-related factors in the future. Third, although physician-related factors are closely related to their hospitals (geographical location, hospital grade, etc)., there remain differences in the characteristics of the physicians themselves (eg, level of education, title, number of patients treated, etc.) within the same hospital level or even within the same hospital. A more in-depth subgroup analysis of the physician group is needed to determine the exact impact of these physician-related factors on prescribing behavior. The current study was limited by the number of physicians participating in the study, which was insufficient to support such an analysis; again, a subsequent study with a larger sample size is needed to answer these questions. Finally, as a cross-sectional study, our study was unable to evaluate whether the observed prescriptions would improve outcomes (eg, reduce deterioration) or iatrogenic harm (eg, ICS induced pneumonia), and whether those overtreated prescriptions would unnecessarily persist. These contents need to be discovered through longitudinal research and long-term tracking of doctors’ prescriptions.
Conclusions
Physicians do not thoroughly adhere to the latest GOLD guidelines when managing COPD patients in GOLD Groups A and B, where triple therapy is overused. This overtreatment poses dual threats: clinically, it exposes patients to preventable ICS-related complications like pneumonia and osteoporosis; economically, it will escalates healthcare costs in primary care settings due to redundant medications and adverse event management. These risks are amplified in resource-constrained community health centers where formulary limitations already challenge optimal care. Targeted interventions must therefore prioritize guideline education and drug access reform to mitigate both patient harm and systemic waste.
Data Sharing Statement
All the data, models, and codes used during the study were provided by a third party. Deidentified data are available from the corresponding author (Shiyue Li) upon reasonable request.
Ethics Approval and Informed Consent
Our study protocol was reviewed and fast-track ethics approved by the First Affiliated Hospital of Guangzhou Medical University research ethics committee because this study was a survey of healthcare professionals, not patients (Ethics approval number: ES-2023-K028-01) (Clinical trial registration number: MR-44-25-059474).
Acknowledgments
The authors would like to thank Shengjing Hospital of China Medical University, Henan People’s Hospital, Second Affiliated Hospital of Xi’an Jiaotong University, Tongji Hospital Tongji Medical College of HUST, Zhongshan Hospital Affiliated with Fudan University, Second Affiliated Hospital Zhejiang University, West China Hospital of Sichuan University, First Affiliated Hospital of Chongqing Medical University, Second Xiangya Hospital of Central South University and Nanfang Hospital of Southern Medical University for providing support for the execution of this study. The authors are grateful for the financial support of the Beijing Life Oasis Public Service Center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
None of the authors have any relevant relationships to disclose.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: 2023 report. 2020. Available from: https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023ver-1.3-17Feb2023_WMV.pdf.
2. World Health Organization. The top 10 causes of death. 2024. Available from: http://www.who.int.
3. Zhong N, Wang C, Yao W, et al. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey. Am J Respir Crit Care Med. 2007;176(8):753–760. doi:10.1164/rccm.200612-1749OC
4. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
5. Foreman KJ, Marquez N, Dolgert A, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018;392(10159):2052–2090. doi:10.1016/S0140-6736(18)31694-5
6. Singh D. Pharmacological treatment of stable chronic obstructive pulmonary disease. Respirology. 2021;26(7):643–651. doi:10.1111/resp.14046
7. Contoli M, Morandi L, Di Marco F, Carone M. A perspective for chronic obstructive pulmonary disease (COPD) management: six key clinical questions to improve disease treatment. Expert Opin Pharmacother. 2021;22(4):427–437. doi:10.1080/14656566.2020.1828352
8. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
9. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
10. Agusti A, Fabbri LM, Singh D, et al. Inhaled corticosteroids in COPD: friend or foe? Eur Respir J. 2018;52(6):1801219. doi:10.1183/13993003.01219-2018
11. Miravitlles M, Auladell-Rispau A, Monteagudo M, et al. Systematic review on long-term adverse effects of inhaled corticosteroids in the treatment of COPD. Eur Respir Rev. 2021;30(160):210075. doi:10.1183/16000617.0075-2021
12. Kumarathas I, Harsløf T, Andersen CU, et al. The risk of osteoporosis in patients with asthma. Eur Clin Respir J. 2020;7(1):1763612. doi:10.1080/20018525.2020.1763612
13. Dahl R. Systemic side effects of inhaled corticosteroids in patients with asthma. Respir Med. 2006;100(8):1307–1317. doi:10.1016/j.rmed.2005.11.020
14. Matera MG, Cardaci V, Cazzola M, Rogliani P. Safety of inhaled corticosteroids for treating chronic obstructive pulmonary disease. Expert Opin Drug Saf. 2015;14(4):533–541. doi:10.1517/14740338.2015.1001363
15. Koblizek V, Milenkovic B, Barczyk A, et al. Phenotypes of COPD patients with a smoking history in Central and Eastern Europe: the POPE study. Eur Respir J. 2017;49(5):1601446. doi:10.1183/13993003.01446-2016
16. Monteagudo M, Nuñez A, Solntseva I, et al. Treatment pathways before and after triple therapy in COPD: a population-based study in primary care in Spain. Arch Bronconeumol. 2021;57(3):205–213. doi:10.1016/j.arbres.2020.07.032
17. Kardos P, Vogelmeier C, Worth H, et al. A two-year evaluation of the ‘real life’ impact of COPD on patients in Germany: the DACCORD observational study. Respir Med. 2017;124:57–64. doi:10.1016/j.rmed.2017.02.007
18. Brusselle G, Price D, Gruffydd-Jones K, et al. The inevitable drift to triple therapy in COPD: an analysis of prescribing pathways in the UK. Int J Chron Obstruct Pulmon Dis. 2015;10:2207–2217. doi:10.2147/COPD.S91694
19. Yun JH, Lamb A, Chase R, et al. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2018;141(6):2037–2047.e10. doi:10.1016/j.jaci.2018.04.010
20. Buhl R, Criée CP, Kardos P, et al. Dual bronchodilation vs triple therapy in the “real-life” COPD DACCORD study. Int J Chron Obstruct Pulmon Dis. 2018;13:2557–2568. doi:10.2147/COPD.S169958
21. Vogelmeier CF, Kostikas K, Fang J, et al. Evaluation of exacerbations and blood eosinophils in UK and US COPD populations. Respir Res. 2019;20(1):178. doi:10.1186/s12931-019-1130-y
22. Yawn BP, Suissa S, Rossi A. Appropriate use of inhaled corticosteroids in COPD: the candidates for safe withdrawal. NPJ Prim Care Respir Med. 2016;26(1):16068. doi:10.1038/npjpcrm.2016.68
23. Graf J, Jörres RA, Lucke T, Nowak D, Vogelmeier CF, Ficker JH. Medical treatment of COPD. Dtsch Arztebl Int. 2018;155(37):599–605. doi:10.3238/arztebl.2018.0599
24. Cataldo D, Derom E, Liistro G, et al. Overuse of inhaled corticosteroids in COPD: five questions for withdrawal in daily practice. Int J Chron Obstruct Pulmon Dis. 2018;13:2089–2099. doi:10.2147/COPD.S164259
25. Casas A, De Oca MM, Menezes AM, et al. Respiratory medication used in COPD patients from seven Latin American countries: the LASSYC study. Int J Chron Obstruct Pulmon Dis. 2018;13:1545–1556. doi:10.2147/COPD.S154097
26. Yang T, Cai B, Cao B, et al. Treatment patterns in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL). Ther Adv Respir Dis. 2023;17:17534666231158283. doi:10.1177/17534666231158283
27. Vestbo J, Vogelmeier CF, Small M, Siddall J, Fogel R, Kostikas K. Inhaled corticosteroid use by exacerbations and eosinophils: a real-world COPD population. Int J Chron Obstruct Pulmon Dis. 2019;14:853–861. doi:10.2147/COPD.S189585
28. Zeng Y, Cai S, Chen Y, et al. Current status of the treatment of COPD in China: a multicenter prospective observational study. Int J Chron Obstruct Pulmon Dis. 2020;15:3227–3237. doi:10.2147/COPD.S274024
29. Souliotis K, Miguel LS, Hillas G, et al. The cost-saving switch from inhaled corticosteroid-containing treatments to dual bronchodilation: a two-country projection of epidemiological and economic burden in chronic obstructive pulmonary disease. Ther Adv Respir Dis. 2020;14:1753466620926802. doi:10.1177/1753466620926802
30. Fens T, Van Der Pol S, Kocks JWH, Postma MJ, Van Boven JFM. Economic impact of reducing inappropriate inhaled corticosteroids use in patients with chronic obstructive pulmonary disease: ISPOR’s guidance on budget impact in practice. Value Health. 2019;22(10):1092–1101. doi:10.1016/j.jval.2019.05.006
31. Palli SR, Frazer M, DuCharme M, Buikema AR, Anderson AJ, Franchino-Elder J. Differences in real-world health and economic outcomes among patients with COPD treated with combination tiotropium/olodaterol versus triple therapy. J Manag Care Spec Pharm. 2020;26(10):1363–1374. doi:10.18553/jmcp.2020.20159
32. Chinese Medical Association. Chinese medical journals publishing house, Chinese society of general practice. Guideline for primary care of chronic obstructive pulmonary disease. Chin J Gen Pract. 2018;17(11):856–870.
33. Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society, Chronic Obstructive Pulmonary Disease Committee of Chinese Association of Chest Physician. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021). Zhonghua Jie He He Hu Xi Za Zhi. 2021;44(3):170–205. doi:10.3760/cma.j.cn112147-20210109-00031
34. Davis KJ, Landis SH, Oh YM, et al. Continuing to confront COPD international physician survey: physician knowledge and application of COPD management guidelines in 12 countries. Int J Chron Obstruct Pulmon Dis. 2015;10:39–55. doi:10.2147/COPD.S70162
35. Sulku J, Janson C, Melhus H, et al. A cross-sectional study assessing appropriateness of inhaled corticosteroid treatment in primary and secondary care patients with COPD in Sweden. Int J Chron Obstruct Pulmon Dis. 2019;14:2451–2460. doi:10.2147/COPD.S218747
36. Madsen F, Ulrik CS, Dirksen A, et al. Patient-administered sequential spirometry in healthy volunteers and patients with α1-antitrypsin deficiency. Respir Med. 1996;90(3):131–138. doi:10.1016/S0954-6111(96)90154-7
37. Løkke A, Hilberg O, Lange P, et al. Disease trajectories and impact of one moderate exacerbation in gold B COPD patients. Int J Chron Obstruct Pulmon Dis. 2022;17:569–578. doi:10.2147/COPD.S344669
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Microbiome in COPD: Emerging Potential for Microbiome-Targeted Interventions
Millares L, Monso E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1835-1845
Published Date: 12 August 2022
Anti-IL5/IL5R Treatment in COPD: Should We Target Oral Corticosteroid-Dependent Patients?
Laroche J, Pelletier G, Boulay M, Côté A, Godbout K
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:755-763
Published Date: 5 May 2023
Lack of Clinical Control in COPD Patients Depending on the Target and the Therapeutic Option
Soler-Cataluña JJ, Huerta A, Almagro P, González-Segura D, Cosío BG
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1367-1376
Published Date: 6 July 2023