Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
The Microbiome in COPD: Emerging Potential for Microbiome-Targeted Interventions
Authors Millares L, Monso E
Received 23 April 2022
Accepted for publication 21 July 2022
Published 12 August 2022 Volume 2022:17 Pages 1835—1845
DOI https://doi.org/10.2147/COPD.S371958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Laura Millares,1,2 Eduard Monso1– 4
1Airway Inflammation Research Group, Parc Taulí Research and Innovation Institute - I3PT – Parc Taulí Foundation, Sabadell, Barcelona, Spain; 2Catalan Institute of Oncology – ICO, Badalona, Barcelona, Spain; 3Biomedical Research Network on Respiratory Diseases (CIBERES), Carlos III Health Institute (ISCIII), Madrid, Spain; 4Autonomous University of Barcelona - UAB, Cerdanyola del Vallès, Barcelona, Spain
Correspondence: Eduard Monso, Institut d’ Investigació i Innovació Parc Taulí - I3PT - Fundació Parc Taulí, Parc Taulí 1, Sabadell, 08208, Spain, Tel +347236673, Fax +347175067, Email [email protected]
Abstract: The aim of interventions over the respiratory microbiome in COPD is to preserve the original microbial flora, focusing in taxa with a demonstrated impact on the prognosis of the disease. Inhaled therapy is the main treatment for COPD, and chronic corticosteroid use is recommended for patients with frequent exacerbations. This therapy, however, increases both the bronchial microbial load and the abundance of potentially pathogenic bacteria in patients with low peripheral eosinophil counts, and to minimize its use in patients without peripheral eosinophilia, when possible, may avoid increases in bacterial loads of microorganisms as Haemophilus influenzae and Streptococcus pneumoniae. In exacerbations antibiotics determine a decrease in the microbial diversity, a change that persists during stability periods in frequent exacerbators. High-diversity bronchial microbiomes are enriched in non-dominant genera and determine low exacerbation frequencies and survival improvement. Limiting the antibiotic use to the treatment of exacerbations which would clearly benefit would favor the diversity of the respiratory microbiome and may have a positive impact on quality of life and survival. Oral antiseptics have shown and effect on the bronchial microbiome that was associated with improvements in quality of life, and the gut microbiome may be also modified through the oral administration of probiotics or prebiotics, that potentially may determine decreases in lung inflammation and bronchial hyperreactivity. High fiber diets also favor the production of anti-inflammatory molecules by the digestive flora, which would reach the respiratory system through the bloodstream. Interventional approaches favoring the preservation of the respiratory microbiome in COPD need first to select accurately the patients who would benefit from long-term inhaled corticosteroids and antibiotic treatments during exacerbations, under the hypothesis that keeping a respiratory microbiome close to the healthy subject would favor the respiratory health. Additionally, high fiber diets may be able to modify the gut microbiome and influence the respiratory system through the gut-lung axis. Therapeutic approaches targeting the microbiome to improve COPD, however, still require clinical validation and the identification of patient subtypes who would benefit the most with their use.
Keywords: microbiome, COPD, treatment, inhaled corticosteroids, antibiotics, diet
The Respiratory Microbiome in the Healthy Subject
The human microbiome refers to all living microorganisms (bacteria, archaea and fungi) which have the body as their habitat, including their genomes and the metabolites they produce. It is mainly lodged on mucosal surfaces, which in the respiratory system include the oropharynx, the bronchial tree and the lung, and its components may act either as commensals, mutualists or pathogens, depending on their capabilities to modulate inflammatory and/or immune responses till levels able to cause disease.1 So far, most studies have focused on the bacterial part of the microbiome, and in this review we will focus on the bacterial community that conform the respiratory microbiome with its relationships with COPD disease patterns, and the possibilities to intervene the bacterial flora to attain positive secondary effects on the respiratory health. Manuscripts addressing the topic published the last ten years have been identified through Pubmed, searching their focus on the effects of treatment on the respiratory microbiome in COPD, assessing the collateral effects on the microbial flora of guideline-recommended treatments and the results of therapies directly attempting to modify the microbiome, as a way to attain an effect on the patterns of the disease.
In the human airway, the microbiome is distributed throughout the upper and lower respiratory tract, with distinct populations and different burdens in the oropharynx, the bronchial tree and the lung.2,3 Bacteria from the oropharynx enter periodically the lower respiratory tract through recurrent microaspiration, and this microbial immigration is later modulated by clearance mechanisms and the local microenvironment. This microbial penetration in the bronchial tree is a main determinant of the bacterial composition and load in the lower airway, which in the healthy subject is dominated by phyla commonly found in the oropharynx, as are Bacteroides and Firmicutes, with Prevotella and Veillonella as predominant genera.4,5
Smoking-Related Changes in the Respiratory Flora
Studies of the oropharynx microbiota in smokers have reported modifications in their microbial composition,6 with decreases in the relative abundance of taxa from the Proteobacteria phylum, paralleled by an enrichment in Actinobacteria. This change in Proteobacteria affects the genera Neisseria, Haemophilus and Aggregatibacter, and is paralleled by additional decreases in genera which are part of other phyla as are Capnocytophaga, Corynebacterium, Porphyromonas, Prevotella, Leptotrichia, Peptostreptococcus, Abiotrophia, Selenomonas and Gemella, severe enough to be considered as dysbiosis.7,8 These changes seem to be restricted to the oropharynx, because they have not been identified neither in sputum samples,9 nor in the lower respiratory tract, when sampled through bronchoalveolar lavage,7 in spite that some changes in the lung microbiome have been reported in smoking animal models, with decreases in genera from the Proteobacteria phylum as are Kluyvera and Mesorhizobium.10 Furthermore, a recovery of the normal microbial composition in the oropharyngeal microbiome have been reported after giving up smoking,8 and all these findings suggest that exposure to smoke results in microbiome changes which are restricted to the upper airway and reversible, and smoking interventions targeting the tobacco use may not determine significant changes in the respiratory microbiome of the bronchial tree and the lung in patients without smoking-related diseases.
The Respiratory Microbiome in COPD
In patients with COPD the lower respiratory flora evolves to a bacterial composition with main differences from the upper airway. The bronchial microbiome show an increase in the relative abundance of Proteobacteria, which include a higher relative abundance of the genus Haemophilus, paralleled by a decrease in Bacteroidetes and Firmicutes, with the Prevotella and Veillonella as the main genera affected by this change.2,3,9 Bronchial diversity declines in severe stages of the disease, with a flora that evolves to a predominance of the Pseudomonas genus in advanced disease.11–13 These changes in the bronchial microbiome may not be paralleled in the lung, because previous work has found higher microbial diversity in bronchoalveolar lavage samples.14,15 How these changes influence the disease is poorly understood, however, and the possibilities to modify the microbial composition of the lower airway with interventions able to restore a normal microbiome composition in stable COPD, and potentially attaining an effect on the respiratory health, have been only partially explored (Table 1). To approach these therapeutic possibilities understanding microbiome-host interactions in the respiratory system and its relationships to COPD pathogenesis would be necessary.
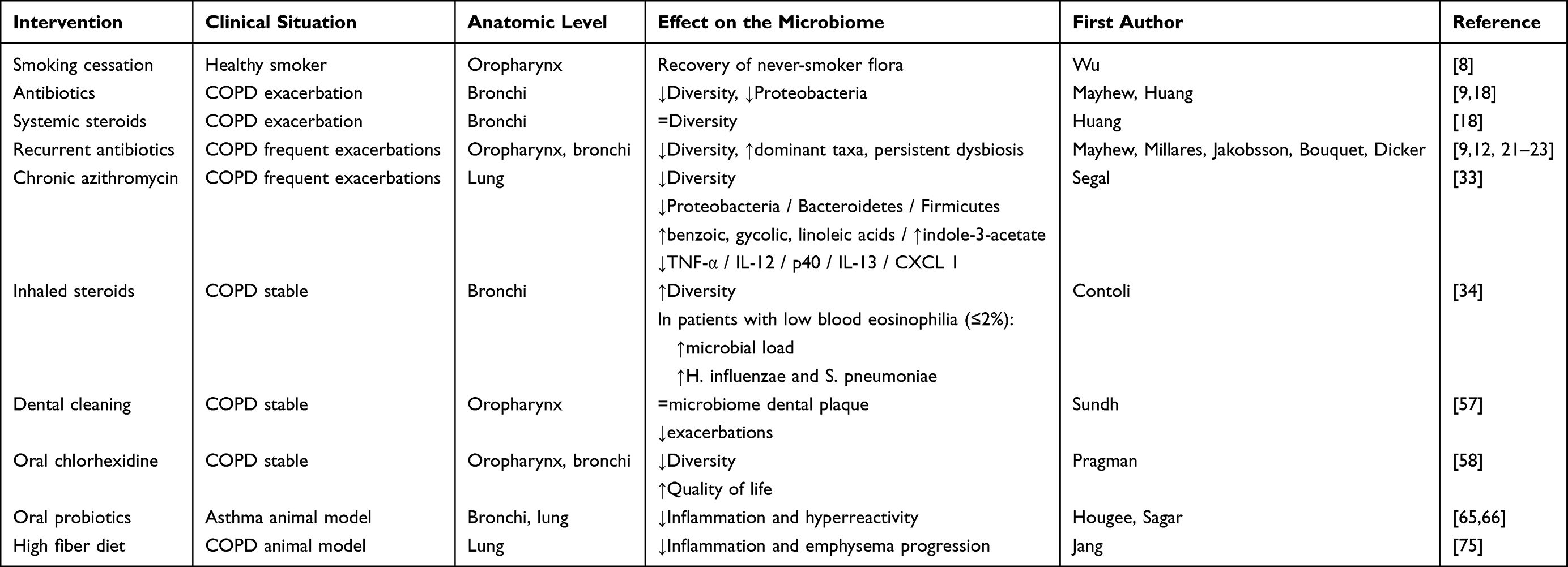 |
Table 1 Interventions on the Microbiome in COPD |
Antibiotic-Treated Exacerbations
During COPD exacerbations the respiratory microbiome changes from its baseline,9,16–18 moving to a predominance of Proteobacteria and genera that include potentially pathogenic bacteria, as are Haemophilus and Moraxella.9,19,20 Treatment given for exacerbations episodes additionally modify the composition of the respiratory microbiome when it includes antibiotics.2,9,18 This treatment determines a decrease in the microbial diversity and the relative abundance of Proteobacteria, while in exacerbations treated only with systemic corticosteroids these decreases are not observed.18 The microbiome changes identified in antibiotic-treated exacerbations are still observed three months after the episode,18 and may persist even longer.21 In fact, frequent exacerbators manifest significant differences in their respiratory microbiome even during their stability periods, with persistent dysbiotic patterns characterized by low microbial diversity and a predominance of some genera from the Proteobacteria phylum, as are Pseudomonas, which often attain a dominant pattern.9,12,22,23 Microbiome composition is different in frequent exacerbators with peripheral eosinophilia (≥2%), however, because this subgroup preserves their microbial diversity and microbiome composition.12,23 Peripheral eosinophilia is closely related to eosinophil abundance in the bronchial tree,24,25 and this trait identifies an endotype that require specific therapeutic approaches.
Current guidelines recommend the use of systemic corticosteroids in COPD exacerbations,26 but recent clinical trials support a restriction in the use of this therapy, limiting its prescription to patients showing peripheral eosinophilia, at least in episodes that do not require an admission.27,28 Huang et al have demonstrated that the treatment of COPD exacerbations with systemic steroids would preserve microbial diversity when antibiotics are not used,18 and an accurate selection of the drugs used for COPD exacerbations need a focus on the avoidance of an overuse of antibiotics in patients who may not attain a clear benefit with the treatment, an approach that would keep the diversity of the bronchial flora, with a potential impact of bronchial inflammatory patterns.
Current criteria for antibiotic treatment of exacerbations are based in the identification of purulence in sputum and the severity of the episode,26 but the use of biomarkers as blood procalcitonin29,30 for the selection of patients to be treated with antibiotics may improve therapeutic approaches to COPD exacerbation, with a potential impact on the diversity and composition of the respiratory microbiome. However, the use of biomarker-based selection of exacerbation treatment still has not shown clear clinically-significant advantages.31
Chronic use of antibiotics in patients suffering from frequent exacerbations is a therapeutic option that improves the recurrence of their acute episodes.32 The mechanisms that determine the positive health impact of this treatment have not been well defined, however, and may be partly mediated by a modification of the respiratory flora. Segal et al have examined the modifications of the lung microbiome, studied through bronchoalveolar lavage, in COPD patients with frequent exacerbations treated daily with azithromycin for a period of eight weeks, and have found a decrease in their microbial diversity, with significant reductions in the taxa of Tissierellaceae, Cytophaga, Flectobacillus, Neisseria, Ralstonia and Rhodospirillaceae.33 This treatment led to the increase in lower airway concentrations of the bacteria-produced metabolites benzoic acid, glycolic acid, indole-3-acetate and linoleic acid, that was paralleled by a decrease in the levels of tumor-necrosis factor (TNF)-α, interleukin (IL)-12, p40, IL-13 and chemokine (C-X-C motif) ligand (CXCL) 1. Glycolic acid and indole-3-acetate reduced the levels of these inflammatory mediators, providing evidence of one of the mechanisms that may be behind the effect of chronic azithromycin use. These observations suggest that azithromycin therapeutic benefit in COPD patients with frequent exacerbations may be at least partly mediated by the interaction between the respiratory microbiome and the host immune system, highlighting the relevance of the understanding of the metabolism of resident bacteria as potential targets for immunomodulation.33
Effects of Inhaled Corticosteroid Treatment on the Respiratory Microbiome
Inhaled corticosteroids are part of the treatment of stable COPD, but its recommendation is currently restricted to patients with blood eosinophilia and/or frequent exacerbations.26 This chronic treatment has a significant impact on the respiratory microbiome,14 as has been clearly shown by Contoli et al in a recent long-term follow-up study of the bronchial microbiome in stable COPD patients who initiated this treatment.34 Steroid users modified their bronchial microbiome in their study, showing significant increases in their bacterial load and diversity, with an overrepresentation of potentially pathogenic bacteria as Haemophilus influenzae and Streptococcus pneumoniae, in agreement with previous work.35,36 The effect of the treatment on these two genera was restricted to the subgroup of patients with low blood eosinophil counts (≤2%) in their study, however, while the microbial load of sputum did not increase in patients with peripheral eosinophilia, who also did not show an increase in the relative abundance of potentially pathogenic bacteria. Accordingly, avoiding the use of inhaled corticosteroids as far as possible in COPD patients without blood eosinophilia may avoid increases in the bacterial loads of microorganisms as Haemophilus influenzae and Streptococcus pneumoniae, which could be potentially harmful.
Microbiome-Host Interactions
Current knowledge suggests that the respiratory microbiome play a role in COPD pathobiology,37 but little information exists regarding the mechanisms behind the relationship between microbial composition and COPD patterns and progression.2 To understand the role of the microbiome in the natural history of COPD, microbial interactions need to be disclosed and extended to viruses, modulation of the immune system and production of beneficial metabolites by the bacterial flora, as possible mechanisms.38,39 In has been demonstrated that rhinovirus infections are followed by an increase in Proteobacteria abundance in sputum of COPD patients, together with the appearance of bronchial neutrophilia.40 These interactions of the respiratory viruses with the microbiome may modulate disease patterns, but COPD could be also a driver in microbiome imbalances by itself, considering that recurrent exacerbations and chronic mucosal inflammation are associated with an impairment in innate immunity, that may determine further changes in both the bronchial microbiome and virome, in a circular effect.41,42
Data obtained from COPD exacerbations support a main role of the overrepresentation of specific taxa in the increase of bronchial inflammation biomarkers and the appearance of symptoms. Ghebre al cols demonstrated that a predominance of Proteobacteria in bronchial secretions is associated with neutrophilic inflammation and high levels of IL-1β, tumor-necrosis factor (TNF)-α, TNF-R2 and vascular endothelial growth factor, while higher relative abundance of Bacteroidetes is related to eosinophilic inflammation and increased levels of Th2 mediators in bronchial secretions, as are the C-C chemokine ligands (CCL) 13 and 17. They also found that greater proportions of Actinobacteria and Firmicutes were associated with higher levels of Th1 mediators, and these results suggest that the specific microbial profiles characteristic of the identified clusters influence the local inflammatory response in COPD exacerbations.43 Haldar et al used quantitative real-time PCR to approach this hypothesis,44 considering Proteobacteria and Firmicutes abundance in sputum samples recovered from exacerbations, and observed that Gammaproteobacteria was associated with sputum neutrophilia and higher bronchial IL-1β level. This pattern was also associated with an increase of blood C-reactive protein (CRP) levels and a significant lung function decline. Both this microbiome profile and inflammatory biomarkers returned to baseline after the antibiotic treatment of the acute episode. This effect of antibiotics was not identified in exacerbations that keep the abundance of Firmicutes and did not show an increase in Gammaproteobacteria.
Bouquet et al have assessed the microbial burden in sputum samples from a COPD cohort enrolled in stable situation,22 and found Prevotella, Veillonella, Haemophilus and Streptococcus as the most prevalent genera in stable COPD, with Prevotella-predominant microbiomes being associated with the highest diversity. In their study both Prevotella and Veillonella abundances were related to a low exacerbation frequency, suggesting that a predominance of these genera in bronchial secretions would be associated with longer periods of stability. More recently, Wang et al have focused on this topic in a multicohort longitudinal analysis which included more than five hundred COPD patients,45 and observed that in patients with sputum neutrophilia (≥61% neutrophils and <3% eosinophils) the overrepresentation of Haemophilus was associated with a decrease in microbial diversity and high levels of IL-1 and TNF-α, either in stability and during exacerbations. In patients with bronchial neutrophilia who showed a more balanced microbiome, however, levels of these biomarkers were low, while IL-17A was increased. The importance of bronchial neutrophilia with an overrepresentation of Haemophilus in sputum has been also emphasized by Beech et al, who demonstrated that COPD patients in this situation show an impaired lung function.46 Then, these studies show that an increased abundance of potentially pathogenic genera in COPD patients with bronchial neutrophilia cannot be always assumed, because exists a subgroup of COPD patients with increased neutrophil counts who have a balanced microbiome which included Veillonella and Prevotella, in the absence of any microbial overrepresentation. Additionally, Wang et al found that patients with bronchial eosinophilia, fifteen percent of their COPD population, had a bronchial microbiome that kept high diversity and showed an enrichment in up to 31 non-dominant genera, with main differences in Granulicatella, Campylobacter, Gemellaceae and Capnocytophaga. These data support the hypothesis that maintaining a diverse microbiome in bronchial secretions, with a significant presence of Veillonella and Prevotella and in absence of a dominant genus, would keep a specific inflammatory response with low levels of IL-1 and TNF-α and a higher presence of IL-17, both in patients with neutrophilic and eosinophilic bronchial inflammatory patterns.47
Keeping the microbial diversity in bronchial secretions has importance for the survival of COPD patients. Leitao et al48 have reported that patients with higher microbial diversity in bronchial secretions when exacerbated had lower long-term mortality. In their study specific taxa drove this effect, with Veillonella as a genus associated with a high one-year survival. Similar results were found by Dicker et al,23 who reported both an increased exacerbation frequency and mortality in the following years in patients with low microbiome diversity and high relative abundances of the Haemophilus genus in bronchial secretions at enrolment, observing also low bronchial eosinophilia in these patients. Overall, these studies support the hypothesis that a diverse bronchial microbiome improves survival in the mid-term, and, accordingly, therapeutic approaches that maintain the diversity of the respiratory microbial flora in the subglottic airway may attain a significant impact on the quality of life of COPD patients. Results from these cohorts also suggested that the effects of respiratory microbial flora may depend on specific components of the microbiome which may be lost with the decline in bronchial diversity.23,48 Supporting this idea, Rigauts et al, in a study which included in vitro and in vivo analyses, found that Rothia mucilaginosa, a common resident of the oral cavity often detectable in the lower airway in chronic respiratory diseases, show an inhibitory effect on pathogen-induced inflammatory responses.49 Their study included also analyses of sputum samples from a cohort of adults with bronchiectasis, most of them also with COPD,50 where Rothia was negatively correlated with IL-8, IL-1β and matrix metalloproteinases, suggesting that the presence of R. mucilaginosa in the lower airways may mitigate inflammation. However, inflammatory and clinical patterns may not depend on specific taxa, because recent work suggests that these responses would be related to the abundance of sets of bacteria able to modulate cellular functions of other resident bacteria and even the host cells. Sibley et al40 showed in a model that three classes of microorganisms present in oropharyngeal isolates acts synergistically with Pseudomonas aeruginosa, while being avirulent or even beneficial on its own. This synergy involves microbe–microbe interactions that result in the modulation of the virulence of the pathogen. Similar results have been reported by Duan et al,51 who have demonstrated that oropharyngeal bacteria enhanced lung damage caused by P. aeruginosa in an animal model, through an upregulation of the bacterial genome. Commensal respiratory bacteria may also suppress the outgrowth of potential pathogens belonging to the same genus or family,52 and potential new therapeutic approaches might reduce colonization by pathogenic microbes through the increase of colonization of commensal bacteria in the respiratory tract.37,53,54
A recent study based on systems biology recently demonstrated the significant microbiome-host interplay in the respiratory system of COPD patients.55 The authors found that Haemophilus and Moraxella were associated with specific host gene expression profiles, related particularly to immunity and inflammation, suggesting these two genera as key players in the airway bacterial-host interaction. Haemophilus was associated with host responses both in stable state and during exacerbations, while the associations for Moraxella were restricted to exacerbations. In the multivariate analyses of this study Megasphaera and other taxa were associated with a reduced expression of host inflammatory pathways, and could potentially reverse the airway inflammation induced by Haemophilus and Moraxella. Besides, Megasphaera was negatively correlated with sputum neutrophil counts. Megasphaera is a known member of human lung microbiome and has beneficial effects on the host through short-chain fatty acids (SCFAs) production, which are able to inhibit cytokine production and inflammation in the lung microenvironment.55 The behavior of microbial communities differs from those of their individual constituents and their interaction may influence disease progression and treatment efficacy.56 Then, the identification of key bacterial components of the respiratory microbiome may be followed by the induction of changes in this microbial flora, potentially benefiting the respiratory health.
Oral Treatments
Interventions targeting oropharyngeal health have shown a collateral effect on COPD. Sundh et al, in a randomized trial assessing the effect of dental cleaning on COPD evolution demonstrated a positive effect of this intervention over the appearance of exacerbations.57 In their study it was hypothesized that this effect could be mediated by changes on oropharyngeal microbiome, but the investigators did not find significant modifications in the microbial composition of the dental plaque after the intervention, and the hypothesis could not be confirmed. Pragman et al followed a similar approach using chlorhexidine, and observed that, in spite that neither the oral nor the sputum microbiome mass was lowered with the treatment, chlorhexidine was able to modify the diversity of both the oral and the bronchial microbiomes. This effect did not have an impact on systemic inflammatory markers, but treated patients showed a significant improvement in their quality of life, when measured using the Saint Georges Respiratory Questionnaire.58 In spite that it is necessary to consider these studies as unconclusive, they suggested that it is possible to attain an improvement in COPD through the induction of changes in the bronchial microbiome using easily accessible oral cleaning approaches.
Induced modifications of the intestinal microbiome include an additional layer of complexity into the possibilities to improve the respiratory health in COPD patients. Studies of their intestinal microbial composition have shown that specific taxa were associated with a functional progressive impairment.59 An increasing number of studies also indicate that changes in the gut microbial composition may be linked to modifications of systemic inflammatory and immune responses, which would be able to influence the respiratory system, as a contributing part of the gut-lung axis.60 These relationships would be mediated by the passage of microbial mediators, either cytokines or metabolites, into the bloodstream to reach the lung, a mechanism apparently bidirectional, because inflammatory changes in the lung may induce secondary modifications of the gut microbiome.61 The details of how the intestinal flora influence the inflammation and immune responses of the lung, and vice versa, however, are not well known, but keystone species and their spatial organization may drive their functional behavior.62,63
Most studies in chronic respiratory diseases have attempted to modify a limited number of bacterial strains of the intestinal microbiome, using either probiotics or prebiotics, to attain a beneficial effect with the intervention. Probiotics are live microorganisms that may have a positive effect on human health through a change in the composition of the intestinal microbiome, and its main route of administration is oral, either with dairy products supplemented with live bacteria or administering the microorganisms inside a capsule. The most commonly used bacterial genera for this supplementation are Lactobacilli and Bifidobacteria. A change in the intestinal microbial flora may be attained also with the use of prebiotics, non-digestible food ingredients that selectively stimulate the growth and/or activity of one or a restricted number of beneficial bacteria in the gut. Additionally, symbiotic approaches would combine oral probiotics and prebiotics.64
A part of COPD patients shows bronchial hyperreactivity and studies performed in asthma animal models have given useful information for this COPD endotype. An initial study tested six different bacterial strains of Bifidobacterium and Lactobacillus genera to determine their effect on allergic asthma, and found that the oral treatment with Bifidobacterium breve was effective in reducing the allergic response, with a decrease in both lung inflammation and the response to methacholine,65 and a subsequent study has assessed the therapeutic effect of long-term oral treatment with B. breve and Lactobacillus rhamnosus on this inflammatory response, using budesonide as a comparator. L. rhamnosus reduced lung resistance at the same level that budesonide, and both bacterial strains were as effective as the corticosteroid in reducing the inflammatory cellular response. Therefore, these bacteria have strong anti-inflammatory properties that appear to be comparable to budesonide, and may be beneficial in the treatment of obstructive lung diseases.66
Assessing the indirect modulation of the microbiome through the diet, most research has focus on fiber and its effect on inflammatory diseases. There have been associations reported in humans between low fiber diets and higher asthma figures, paralleled in their results by studies showing that Mediterranean diets with high fiber content are associated with a decreased incidence of asthma, at least partly mediated through the gut microbiome.67–69 Dietary fibers are complex carbohydrates consisting of both soluble and insoluble components that cannot be digested by the body, which act as a source of nutrition for intestinal bacteria. Soluble forms, additionally, can be fermented by certain species and lead to physiologically active products as SCFAs, which exert an effect on gut function and can disseminate systemically.54,70–72 SCFAs are potent anti-inflammatory molecules, which reduce chemotaxis and adherence in immune cells, while increasing the release of anti-inflammatory cytokines, and the absorption of these molecules into the systemic circulation has an anti-inflammatory effect in the host.73,74 The use of high-fiber diets in an animal model of COPD have demonstrated to be able to minimize the inflammatory response and the pathological changes associated with emphysema progression.75 Thus, all these studies support the hypothesis that the gut microbiome is able influence lung health through systemic changes induced by microbial metabolites, a mechanism that would be favored by diets with a high fiber content.
Conclusion
The aim of interventions over the human microbiome in COPD are based on the hypothesis that keeping the microbial flora as close as possible to the healthy subject, focusing in taxa with a demonstrated impact on the prognosis of the disease, would have a positive impact on the respiratory health (Table 2). Actions on COPD begin with smoking cessation, but most microbiome changes associated with tobacco use are restricted to the upper airway, and smoking interventions would not determine significant changes in the lower airway microbiome. The next treatment step in COPD is the introduction of inhalers, and corticosteroid as a chronic treatment is recommended for patients with frequent exacerbations. In patients with low blood eosinophil counts, however, this therapy increases both bronchial microbial load and abundance of potentially pathogenic bacteria, and a restriction in the use of inhaled corticosteroids in COPD patients who do not show peripheral eosinophilia, when possible, could probably avoid increases in the bacterial loads of potentially pathogenic microorganisms as are Haemophilus influenzae and Streptococcus pneumoniae.
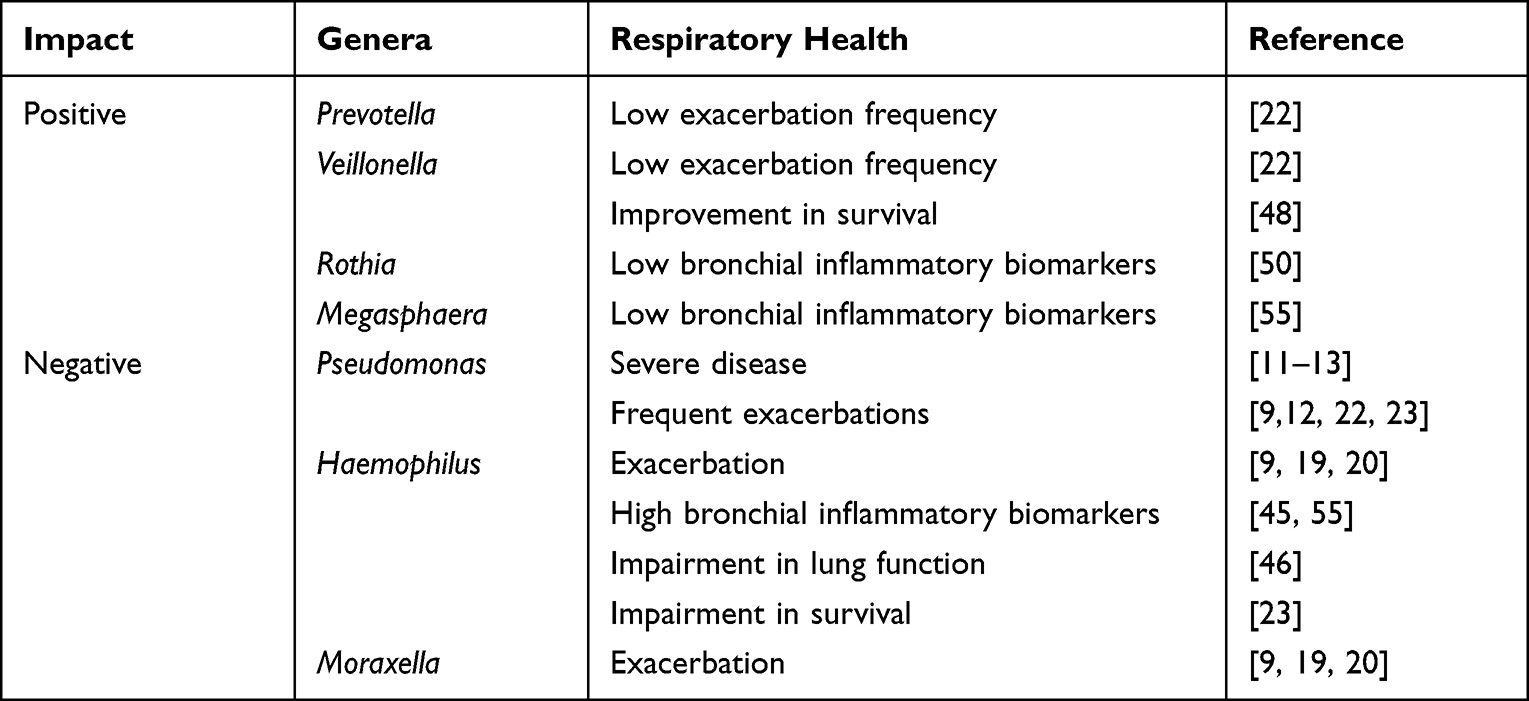 |
Table 2 Genera Part of the Bronchial Microbiome with a Demonstrated Impact on COPD |
Antibiotics are commonly used in COPD when exacerbations appear and determine a decrease in the microbial diversity of the respiratory tract, a change still observed months after the treatment, that persists during stability periods in frequent exacerbators. High-diversity bronchial microbiomes show an enrichment in non-dominant genera which include Prevotella and Veillonella, and is associated with decreased levels of local inflammatory mediators, low exacerbation frequencies and higher survival. It is possible that therapeutic approaches that maintain the diversity of the respiratory microbial flora in the bronchial tree show a positive impact on the quality of life in COPD patients, even increasing survival. Treatment of COPD exacerbations with systemic steroids favor microbial diversity, and the introduction of antibiotics in the therapy of acute episodes needs to be restricted to the recommendations of the guidelines, avoiding antibiotic overuse.
Oral interventions may improve lung health in COPD patients. Chlorhexidine has shown and effect on the bronchial microbiome associated with an improvement in the quality of life of the treated patients, and the intestinal microbiome may be also modified using oral administration of probiotics or prebiotics. The addition of Bifidobacterium breve and Lactobacillus rhamnosus to the diet decreases lung inflammation and bronchial hyperreactivity in animal models, and high fiber diets favors the production of physiologically active products by the gut microbial flora in these models, which can disseminate systemically, some of them potent anti-inflammatory molecules.
Interventional approaches targeting the respiratory microbiome in COPD need first to consider accurately the patients who would benefit from long-term inhaled corticosteroids and antibiotic treatment during exacerbations, because the use of these therapies would modify the bronchial microbiome, potentially impairing its diversity and favoring the overrepresentation of potentially pathogenic taxa. New interventions with potential effects on COPD include oropharyngeal antiseptics as chlorhexidine, and high fiber diets, that have shown in preliminary studies its capability to decrease systemic inflammatory mediators and are able to influence the respiratory system through the gut-lung axis. The hypothesized effects of these therapeutic approaches, however, still need additional research to be confirmed, and also would require the identification of the subtypes of patients who could benefit the most with their use.
Acknowledgments
Manuscript preparation has been partly funded by Instituto de Salud Carlos III – Fondo de Investigación Sanitaria PI18/00934 and Agència de Gestió d’Ajuts Universitaris i de Recerca – AGAUR.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dima E, Kyriakoudi A, Kaponi M, et al. The lung microbiome dynamics between stability and exacerbation in chronic obstructive pulmonary disease (COPD): current perspectives. Respir Med. 2019;157:1–6. doi:10.1016/j.rmed.2019.08.012
2. Budden KF, Shukla SD, Rehman SF, et al. Functional effects of the microbiota in chronic respiratory disease. Lancet Respir Med. 2019;7(10):907–920. doi:10.1016/S2213-2600(18)30510-1
3. Dickson RP, Erb-Downward JR, Freeman CM, et al. Spatial variation in the healthy human lung microbiome and the adapted island model of lung biogeography. Ann Am Thorac Soc. 2015;12(6):821–830. doi:10.1513/AnnalsATS.201501-029OC
4. Charlson ES, Bittinger K, Haas AR, et al. Topographical continuity of bacterial populations in the healthy human respiratory tract. Am J Respir Crit Care Med. 2011;184(8):957–963. doi:10.1164/rccm.201104-0655OC
5. Bassis CM, Erb-Downward JR, Dickson RP, et al. Analysis of the upper respiratory tract microbiotas as the source of the lung and gastric microbiotas in healthy individuals. mBio. 2015;6(2):e0037–e15. doi:10.1128/mBio.00037-15
6. Charlson ES, Chen J, Custers-Allen R, et al. Disordered microbial communities in the upper respiratory tract of cigarette smokers. PLosOne. 2010;5(12):e15216. doi:10.1371/journal.pone.0015216
7. Morris A, Beck JM, Schloss PD, et al. Comparison of the respiratory microbiome in healthy nonsmokers and smokers. Am J Respir Crit Care Med. 2013;187(10):1067–1075. doi:10.1164/rccm.201210-1913OC
8. Wu J, Peters BA, Dominianni C, et al. Cigarette smoking and the oral microbiome in a large study of American adults. ISME J. 2016;10:2435–2446. doi:10.1038/ismej.2016.37
9. Mayhew D, Devos N, Lambert C, et al. Longitudinal profiling of the lung microbiome in the AERIS study demonstrates repeatability of bacterial and eosinophilic COPD exacerbations. Thorax. 2018;73(5):422–430. doi:10.1136/thoraxjnl-2017-210408
10. Li KJ, Chen ZL, Huang Y, et al. Dysbiosis of lower respiratory tract microbiome are associated with inflammation and microbial function variety. Respir Res. 2019;20(1):272. doi:10.1186/s12931-019-1246-0
11. Garcia-Nuñez M, Millares L, Pomares X, et al. Severity-related changes of bronchial microbiome in chronic obstructive pulmonary disease. J Clin Microbiol. 2014;52(12):4217–4223. doi:10.1128/JCM.01967-14
12. Millares L, Pascual S, Montón C, et al. Relationship between the respiratory microbiome and the severity of airflow limitation, history of exacerbations and circulating eosinophils in COPD patients. BMC Pulm Med. 2019;19(1):112. doi:10.1186/s12890-019-0867-x
13. Einarsson GG, Comer DM, McIIreavey L, et al. Community dynamics and the lower airway microbiota in stable chronic obstructive pulmonary disease, smokers and healthy non-smokers. Thorax. 2016;71(9):795–803. doi:10.1136/thoraxjnl-2015-207235
14. Pragman AA, Kim HB, Reilly CS, Wendt C, Isaacson RE. The lung microbiome in moderate and severe chronic obstructive pulmonary disease. PLoS One. 2012;7(10):e47305. doi:10.1371/journal.pone.0047305
15. Cabrera-Rubio R, García-Núñez M, Setó L, et al. A Microbiome diversity in the bronchial tracts of patients with chronic obstructive pulmonary disease. J Clin Microbiol. 2012;50(11):3562–3568. doi:10.1128/JCM.00767-12
16. Huang YJ, Kim E, Cox MJ, et al. A persistent and diverse airway microbiota present during chronic obstructive pulmonary disease exacerbations. OMICS. 2010;14(1):9–59. doi:10.1089/omi.2009.0100
17. Jubinville E, Veillette M, Milot J, et al. Exacerbation induces a microbiota shift in sputa of COPD patients. PLoS One. 2018;13(3):e0194355. doi:10.1371/journal.pone.0194355
18. Huang YJ, Sethi S, Murphy T, Nariya S, Boushey HA, Lynch SV. Airway microbiome dynamics in exacerbations of chronic obstructive pulmonary disease. J Clin Microbiol. 2014;52(8):2813. doi:10.1128/JCM.00035-14
19. Millares L, Ferrari R, Gallego M, et al. Bronchial microbiome of severe COPD patients colonized by Pseudomonas aeruginosa. Eur J Clin Microbiol Infect Dis. 2014;33(7):1101–1111. doi:10.1007/s10096-013-2044-0
20. Huang YJ, Boushey HA. The sputum microbiome in chronic obstructive pulmonary disease exacerbations. Ann Am Thorac Soc. 2015;12(Suppl 2):S176–S180. doi:10.1513/AnnalsATS.201506-319AW
21. Jakobsson HE, Jernberg C, Andersson AF, Sjölung-Karlsoson M, Jansson JK, Engstrand L. Short-term antibiotic treatment has differing long-term impacts on the human throat and gut microbiome. PLoS One. 2010;5(3):e9836. doi:10.1371/journal.pone.0009836
22. Bouquet J, Tabor DE, Silver JS, et al. Microbial burden and viral exacerbations in a longitudinal multicenter COPD cohort. Respir Res. 2020;21(1):77. doi:10.1186/s12931-020-01340-0
23. Dicker AJ, Huang JTJ, Lonergan M, et al. The sputum microbiome, airway inflammation and mortality in chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2021;147(1):158–167. doi:10.1016/j.jaci.2020.02.040
24. Eltboli O, Mistry V, Barker B, Brightling CE. Relationship between blood and bronchial submucosal eosinophilia and reticular basement membrane thickening in chronic obstructive pulmonary disease. Respirology. 2015;20(4):667–670. doi:10.1111/resp.12475
25. Negewo NA, McDonald VM, Baines KJ, et al. Peripheral blood eosinophils: a surrogate marker for airway eosinophilia in stable COPD. Int J COPD. 2016;11:1495–1504. doi:10.2147/COPD.S100338
26. Global Initiative for Chronic Obstructive Lung Disease. 2022 GOLD Reports. Available from: https://goldcopd.org/2022-gold-reports-2.
27. Bafadhel M, McKenna S, Terry S, et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease: a randomized placebo-controlled trial. Am J Respir Crit Care Med. 2012;186(1):48–55. doi:10.1164/rccm.201108-1553OC
28. Sivapalan P, Lapperre TS, Janner J, et al. Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): a multicentre, randomised, controlled, open-label, non-inferiority trial. Lancet Respir Med. 2019;7(8):699–709. doi:10.1016/S2213-2600(19)30176-6
29. Schuetz P, Christ-Crain M, Thomann R, Falconnier C, Wolbers M, Widmer I. Effect of procalcitonin-based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial. JAMA. 2009;302(10):1059–1066. doi:10.1001/jama.2009.1297
30. Schuetz P, Müller B, Christ-Crain M, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2012;2012(9):CD007498.
31. Wang JX, Zhang SM, Li XH, Zhang Y, Xu ZY, Cao B. Acute exacerbations of chronic obstructive pulmonary disease with low serum procalcitonin values do not benefit from antibiotic treatment: a prospective randomized controlled trial. Int J Infect Dis. 2016;48:40–45. doi:10.1016/j.ijid.2016.04.024
32. Albert RK, Connet J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med. 2011;365(8):689–698. doi:10.1056/NEJMoa1104623
33. Segal LN, Clemente JC, Wu BG, et al. Randomized, double-blind, placebo-controlled trial with azithromycin select for anti-inflammatory microbial metabolites in the emphysematous lung. Thorax. 2017;72(1):13–22. doi:10.1136/thoraxjnl-2016-208599
34. Contoli M, Pauletti A, Rossi MR, et al. Long-term effects of inhaled corticosteroids on sputum bacterial and viral loads in COPD. Eur Respir J. 2017;50(4):1700451. doi:10.1183/13993003.00451-2017
35. Wilkinson TM, Patel IS, Wilks M, Donaldson GC, Wedzicha JA. Airway bacterial load and FEV1 decline in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2003;167(8):1090–1095. doi:10.1164/rccm.200210-1179OC
36. Garcha DS, Thurston SJ, Patel ARC, et al. Changes in the prevalence and load of airway bacteria using quantitative PCR in stable and exacerbated COPD. Thorax. 2012;67(12):1075–1080. doi:10.1136/thoraxjnl-2012-201924
37. Ditz B, Christenson S, Rossen J, et al. Sputum microbiome profiling in COPD: beyond singular pathogen detection. Thorax. 2020;75(4):338–344. doi:10.1136/thoraxjnl-2019-214168
38. Tagg JR, Dierksen KP. Bacterial replacement therapy: adapting “germ warfare” to infection prevention. Trends Biotechnol. 2003;21(5):217–223. doi:10.1016/S0167-7799(03)00085-4
39. Shukla SD, Budden KF, Neal R, Hansbro PM. Microbiome effects on immunity, health and disease in the lung. Clin Transl Immunol. 2017;6(3):e133. doi:10.1038/cti.2017.6
40. Molyneaux PL, Mallia P, Cox MJ, et al. Outgrowth of the bacterial airway microbiome after rhinovirus exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;188(10):1224–1231. doi:10.1164/rccm.201302-0341OC
41. Wang Z, Bafadhel M, Haldar K, et al. Lung microbiome dynamics in COPD exacerbations. Eur Respir J. 2016;47(4):1082–1092. doi:10.1183/13993003.01406-2015
42. Dickson RP, Martinez FJ, Huffnagle GB. The role of the microbiome in exacerbations of chronic lung diseases. Lancet. 2014;384(9944):691–702. doi:10.1016/S0140-6736(14)61136-3
43. Ghebre MA, Pang PH, Diver S, et al. Biological exacerbation clusters demonstrate asthma and chronic obstructive pulmonary disease overlap with distinct mediator and microbiome profiles. J Allergy Clin Immunol. 2018;141(6):2027–2036. doi:10.1016/j.jaci.2018.04.013
44. Haldar K, Bafadhel M, Lau K, et al. Microbiome balance in sputum determined by PCR stratifies COPD exacerbations and shows potential for selective use of antibiotics. PLoS One. 2017;12(8):e0182833. doi:10.1371/journal.pone.0182833
45. Wang Z, Locantore N, Haldar K, et al. Inflammatory endotype- associated airway microbiome in chronic obstructive pulmonary disease clinical stability and exacerbations. A multicohort longitudinal analysis. Am J Respir Crit Care Med. 2021;203(12):1488–1502. doi:10.1164/rccm.202009-3448OC
46. Beech AS, Lea S, Kolsum U, et al. Bacteria and sputum inflammatory cell counts; a COPD cohort analysis. Respir Res. 2020;21(1):289. doi:10.1186/s12931-020-01552-4
47. Mannion JM, McLoughlin RM, Lalor SJ. The airway microbiome-IL-17 axis: a critical regulator of chronic inflammatory disease. Clin Rev Allergy Immunol. 2022. doi:10.1007/s12016-022-08928-y
48. Leitao Filho FS, Alotaibi NM, Ngan D, et al. Sputum microbiome is associated with 1-year mortality after chronic obstructive pulmonary disease hospitalizations. Am J Respir Crit Care Med. 2019;199(10):1205–1213. doi:10.1164/rccm.201806-1135OC
49. Rigauts C, Aizawa J, Taylor S, et al. Rothia mucilaginosa is an antiinflammatory bacterium in the respiratory tract of patients with chronic lung disease. Eur Respir J. 2022;59. doi:10.1183/13993003.01293-2021
50. Rogers GB, Zain NMM, Bruce KD, et al. A novel microbiota stratification system predicts future exacerbations in bronchiectasis. Ann Am Thorac Soc. 2014;11(4):496–503. doi:10.1513/AnnalsATS.201310-335OC
51. Duan K, Dammel C, Stein J, Rabin H, Surette MG. Modulation of Pseudomonas aeruginosa gene expression by host microflora through interspecies communication. Mol Microbiol. 2003;50(5):1477–1491. doi:10.1046/j.1365-2958.2003.03803.x
52. Iwase T, Uehara Y, Shinji H, et al. Staphylococcus epidermidis Esp inhibits Staphylococcus aureus biofilm formation and nasal colonization. Nature. 2010;465(7296):346–349. doi:10.1038/nature09074
53. Erb-Downward JR, Thompson DL, Han MK, et al. Analysis of the lung microbiome in the “healthy” smoker and in COPD. PLoS One. 2011;6(2):e16384. doi:10.1371/journal.pone.0016384
54. Trompette A, Gollwitzer ES, Yadava K, et al. Gut microbiota metabolism of dietary fiber influences allergic airway disease and hematopoiesis. Nat Med. 2014;20(2):159–166. doi:10.1038/nm.3444
55. Wang Z, Maschera B, Lea S, et al. Airway host-microbiome interactions in chronic obstructive pulmonary disease. Respir Res. 2019;20(1):113. doi:10.1186/s12931-019-1085-z
56. Limoli DH, Hoffman LR. Help, hinder, hide and harm: what can we learn from the interactions between Pseudomonas aeruginosa and Staphylococcus aureus during respiratory infections? Thorax. 2019;74(7):684–692. doi:10.1136/thoraxjnl-2018-212616
57. Sundh J, Tanash H, Arian R, et al. Advanced dental cleaning is associated with reduced risk of COPD exacerbations. A randomized controlled trial. Int J COPD. 2021;16:3203–3215. doi:10.2147/COPD.S327036
58. Pragman AA, Fieberg AM, Reilly CS, Wendt C. Chlorhexidine oral rinses for symptomatic COPD: a randomised, blind, placebo-controlled preliminary study. BMJ Open. 2021;11(12):e50271. doi:10.1136/bmjopen-2021-050271
59. Chiu YC, Lee SW, Liu CW, Lan TY, Shih-Hsin WL. Relationship between gut microbiota and lung function decline in patients with chronic obstructive pulmonary disease: q 1-year follow-up study. Respir Res. 2022;23:10. doi:10.1186/s12931-022-01928-8
60. Keely S, Talley NJ, Hansbro PM. Pulmonary-intestinal cross-talk in mucosal inflammatory disease. Mucosal Immunol. 2012;5(1):7–18. doi:10.1038/mi.2011.55
61. Dumas A, Bernard L, Poquet Y, Lugo-Villarino G, Neyrolles O. The role of the lung microbiota and the gut-lung axis in respiratory infectious diseases. Cell Microbiol. 2018;20(12):e12966. doi:10.1111/cmi.12966
62. Kolenbrander PE, Palmer RJ, Periasamy S, Jakubovics NS. Oral multispecies biofilm development and the key role of cell-cell distance. Nat Rev Microbiol. 2010;8(7):471–480. doi:10.1038/nrmicro2381
63. Lai HC, Lin TL, Chen TW, et al. Gut microbiota modulates COPD pathogenesis: role of anti-inflammatory Parabacteroides goldsteinii lipopolysaccharide. Gut. 2022;71(2):309–321. doi:10.1136/gutjnl-2020-322599
64. Gollwitzer ES, Marsland BJ. Microbiota abnormalities in inflammatory airway diseases - Potential for therapy. Pharmacol Ther. 2014;141(1):32–39. doi:10.1016/j.pharmthera.2013.08.002
65. Hougee S, Vriesema AJM, Wijering SC, et al. Oral treatment with probiotics reduces allergic symptoms in ovalbumin-sensitized mice: a bacterial strain comparative study. Int Arch Allergy Immunol. 2010;151(2):107–117. doi:10.1159/000236000
66. Sagar S, Morgan ME, Chen S, et al. Bifidobacterium breve and Lactobacillus rhamnosus treatment is as effective as budesonide at reducing inflammation in a murine model for chronic asthma. Respir Res. 2014;15(1):46. doi:10.1186/1465-9921-15-46
67. Devereux G. The increase in the prevalence of asthma and allergy: food for thought. Nat Rev Immunol. 2006;6(1):869–874. doi:10.1038/nri1958
68. Noverr MC, Huffnagle GB. The “microflora hypothesis” of allergic diseases. Clin Exp Allergy. 2005;35(12):1511–1520. doi:10.1111/j.1365-2222.2005.02379.x
69. Huffnagle GB. Increase in dietary fiber dampens allergic responses in the lung. Nat Med. 2014;20(2):120–121. doi:10.1038/nm.3472
70. Cummings JH, Hill MJ, Bone ES, Branch WJ, Jenkins DJ. The effect of meat protein and dietary fiber on colonic function and metabolism. II. Bacterial metabolites in feces and urine. Am J Clin Nutr. 1979;32(10):2094–2101. doi:10.1093/ajcn/32.10.2094
71. Cummings JH, Pomare EW, Branch WJ, Naylor CP, Macfarlane GT. Short chain fatty acids in human large intestine, portal, hepatic and venous blood. Gut. 1987;28(1):1221–1227. doi:10.1136/gut.28.10.1221
72. Flint HJ, Bayer EA, Rincon MT, Lamed R, White BA. Polysaccharide utilization by gut bacteria: potential for new insights from genomic analysis. Nat Rev Microbiol. 2008;6(2):121–131. doi:10.1038/nrmicro1817
73. Vaughan A, Frazer ZA, Hansbro PM, Yang IA. COPD and the gut-lung axis: the therapeutic potential of fibre. J Thorac Dis. 2019;11(suppl 17):S2173–S2180. doi:10.21037/jtd.2019.10.40
74. Li N, Dai Z, Wang Z, et al. Gut microbiota dysbiosis contributes to the development of chronic obstructive pulmonary disease. Respir Res. 2021;22:274. doi:10.1186/s12931-021-01872-z
75. Jang YO, Kim OH, Kim SJ, et al. High-fiber diets attenuate emphysema development via modulation of gut microbiota and metabolism. Sci Rep. 2021;11(1):7008. doi:10.1038/s41598-021-86404-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pulmonologists’ Opinion on the Use of Inhaled Corticosteroids in Chronic Obstructive Pulmonary Disease Patients in Spain: A Cross-Sectional Survey
Miravitlles M, González-Torralba F, Represas-Represas C, Pomares X, Márquez-Martín E, González C, Amado C, Forné C, Alonso S, Alcázar B, Barrecheguren M, Jurado Mirete JM, Naval E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1577-1587
Published Date: 12 July 2022
Anti-IL5/IL5R Treatment in COPD: Should We Target Oral Corticosteroid-Dependent Patients?
Laroche J, Pelletier G, Boulay M, Côté A, Godbout K
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:755-763
Published Date: 5 May 2023
Lack of Clinical Control in COPD Patients Depending on the Target and the Therapeutic Option
Soler-Cataluña JJ, Huerta A, Almagro P, González-Segura D, Cosío BG
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1367-1376
Published Date: 6 July 2023
Risk of Pneumonia in Patients with COPD Initiating Fixed Dose Inhaled Corticosteroid (ICS) / Long-Acting Bronchodilator (LABD) Formulations Containing Extrafine Beclometasone Dipropionate versus Patients Initiating LABD Without ICS
Price D, Henley W, Cançado JED, Fabbri LM, Kerstjens HA, Papi A, Roche N, Şen E, Singh D, Vogelmeier CF, Nudo E, Carter V, Skinner D, Vella R, Soriano JB, Kots M, Georges G
Pragmatic and Observational Research 2024, 15:1-16
Published Date: 20 January 2024
Withdrawal of Inhaled Corticosteroids from Patients with COPD; Effect on Exacerbation Frequency and Lung Function: A Systematic Review
Georgiou A, Ramesh R, Schofield P, White P, Harries TH
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1403-1419
Published Date: 21 June 2024