Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Anti-IL5/IL5R Treatment in COPD: Should We Target Oral Corticosteroid-Dependent Patients?
Authors Laroche J ![]() , Pelletier G
, Pelletier G ![]() , Boulay M, Côté A, Godbout K
, Boulay M, Côté A, Godbout K
Received 19 September 2022
Accepted for publication 27 March 2023
Published 5 May 2023 Volume 2023:18 Pages 755—763
DOI https://doi.org/10.2147/COPD.S370165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jérémy Laroche,1 Geneviève Pelletier,1 Marie-Ève Boulay,1 Andréanne Côté,1,2 Krystelle Godbout1,2
1Department of Pulmonology and Thoracic Surgery, Quebec Heart and Lung Institute, Laval University, Quebec City, QC, Canada; 2Department of Medicine, Faculty of Medicine, Laval University, Quebec City, QC, Canada
Correspondence: Krystelle Godbout, Department of Pulmonology and Thoracic Surgery, Quebec Heart and Lung Institute, 2725 Chemin Sainte-Foy, Quebec, QC, G1V 4G5, Canada, Tel +1 418 656 4747, Fax +1 418 656 4762, Email [email protected]
Introduction: Monoclonal antibodies targeting interleukin 5 (IL5) or its receptor (IL5R) are frequently used in severe asthma, in which they reduce exacerbations rate and oral corticosteroids (OCS) exposure. Anti-IL5/IL5Rs have been studied in patients with chronic obstructive pulmonary disease (COPD) without convincing benefits. However, these therapies have been used in clinical practice in COPD with apparently good results.
Purpose: To describe the clinical characteristics and therapeutic response of COPD patients treated with anti-IL5/IL5R in a real-world setting.
Patients and Methods: This is a retrospective case series of patients followed at the Quebec Heart and Lung Institute COPD clinic. Men or women, with an established diagnosis of COPD, and treated either with Mepolizumab or Benralizumab were included. Demographics, disease and exacerbation-related data, airway comorbidities, lung function, and inflammatory profile were extracted from patients’ hospital files at baseline visit and 12 months post-treatment. Therapeutic response to biologics was assessed by measuring change in annual exacerbation rate and/or OCS daily dose.
Results: Seven COPD patients treated with biologics were identified (5M:2F). All were found to be OCSdependent at baseline. Radiological evidence of emphysema was found in all patients. One case was diagnosed with asthma before age 40. Residual eosinophilic inflammation was found in 5/6 patients (blood eosinophils count 237 ± 225× 106 cells/L) despite chronic OCS use. After 12 months of anti-IL5 treatment, mean OCS dose dropped from 12.0 ± 7.6 to 2.6 ± 4.3 mg/day, representing a 78% decrease. Annual exacerbations rate was reduced by 88%, from 8.2 ± 3.3 to 1.0 ± 1.2 per year.
Conclusion: Chronic OCS use is a common characteristic of patients treated with anti-IL5/IL5R biological therapies in this real-world setting. In this population, it may be effective in decreasing OCS exposure and exacerbation.
Keywords: COPD, treatment, anti-IL5, monoclonal antibodies, exacerbations, oral corticosteroids
Plain Language Summary
Chronic obstructive pulmonary disease (COPD) is a lung disease most often caused by tobacco smoking. It generally involves airway inflammation, which is triggered by the immune system activation. There are different types of inflammation and one involves the participation of immune cells called eosinophils. Eosinophilic inflammation is most often found in asthma, another airway disease, but some patients with COPD have clinical evidence of it. Biologic therapies have been developed to target specific immune cells or molecules causing inflammation, such as eosinophils.
Biologics targeting eosinophilic inflammation have revolutionized asthma management. They have been studied in COPD without convincing benefits. However, they are sometimes used by clinicians in a selected COPD population with apparently good results. We explored characteristics and response of such COPD patients treated with anti-eosinophilic biologic therapies in a tertiary center. Seven patients were identified and all of them were chronically treated with oral corticosteroids (OCS), a drug known to suppress eosinophilic inflammation. Biologic treatment allowed for a 78% reduction in chronic OCS dose and 88% reduction in flare-up frequency. This magnitude of response is comparable to the effects seen in OCS-dependent asthma. These findings suggest that, as shown in asthma, chronic OCS use might predict response to biologic therapies in COPD. However, OCS-dependent patients are currently excluded from biologic trials in COPD as it is not a recommended treatment in this disease. Our findings might help design future trials studying biologics in COPD.
Introduction
During the past two decades, monoclonal antibodies development and commercialization have revolutionized severe asthma management. By targeting precise elements of inflammatory cascade, biological agents neutralizing immunoglobulin E (IgE), interleukin 5 (IL5), its receptor (IL5R) or the receptor of interleukin 4 (IL4R) allow for an important reduction in exacerbations and oral corticosteroids (OCS) exposure in severe asthmatics with a T2 inflammation profile.1–3 IL5 is involved in the recruitment, activation, maturation and survival of eosinophils,4 leading to an increased and sustained eosinophilic infiltration in blood and pulmonary tissues of asthmatics which contributes to disease severity.5 Of the five monoclonal antibodies currently approved in Canada for severe asthma, three target signaling pathways of IL-5 or its receptor (IL5R): Mepolizumab, Benralizumab and Reslizumab. Mepolizumab and Reslizumab target circulating IL5 while Benralizumab binds to the IL5 receptor alpha (IL5Rα) subunit expressed on eosinophils and basophils.4 Now considered revolutionary, these drugs were initially considered clinically ineffective when studied in an unselected asthmatic population.6 This highlights the importance of careful selection of patients in a heterogeneous disease like asthma, especially when studying treatments targeting precise elements of the inflammatory cascade.
Chronic obstructive pulmonary disease (COPD) is another heterogenous inflammatory airway disease characterized by persistent respiratory symptoms and airflow limitation. In contrast to asthma, it appears after years of cigarette smoking or noxious environmental exposures, leading to permanent structural changes and irreversible airflow obstruction.7 By promoting neutrophils infiltration in pulmonary tissues, tobacco smoke leads to a neutrophil-predominant disease.8 However, a small subset of COPD patients displays eosinophilic inflammation. This phenotype has been associated with a higher risk of exacerbations9–11 and better response to oral and inhaled corticosteroids.12–17
Given that eosinophilic inflammation may lead to exacerbations in a number of COPD patients, anti-IL5/5Rs have been studied in eosinophilic COPD in four Phase 3 trials: METREX and METREO studied Mepolizumab and GALATHEA and TERRANOVA studied Benralizumab.18,19 They failed to show convincing benefits despite inclusion criteria similar to asthma trials.1–3 An incorrect selection of the studied population may however have accounted for these inconclusive results.
In clinical practice, physicians occasionally see COPD patients with evidence of significant eosinophilic inflammation contributing to repeated exacerbations. Anti-IL5s are sometimes tried in this population, after informed consent, when the drugs cost can be covered by the patient insurance plan. The benefits seen in clinical practice seem better than what have been reported in clinical trials. We therefore aim to describe the characteristics and therapeutic response of COPD patients treated with anti-IL5 monoclonal antibodies in the real-world setting of a tertiary care center.
Materials and Methods
Study Design
This is a retrospective, longitudinal case series study of patients treated at the Quebec Heart and Lung Institute COPD clinic and who initiated anti-IL5 treatment between March 2017 and March 2021. Data were extracted from the patient’s hospital files before treatment initiation (V0; baseline visit) and after 12 months (± 3 months) of treatment (V1). If less than 12 months had elapsed after the first treatment injection, the last available visit was used for V1.
All patients signed a consent form allowing research staff to access their medical record for research purposes. Written consent to publish the case details has also been obtained from each of the 7 patients. The study was approved by the Quebec Heart and Lung Institute – Laval University ethics committee (CÉR 22093).
Study Participants
Men and women aged 40 years and over, with an established diagnosis of COPD, and who had received at least 3 doses of anti-IL5 therapy (Mepolizumab or Benralizumab) were included in the study. Exclusion criteria were confounding comorbidities such as eosinophilic granulomatosis with polyangiitis (EGPA) or hypereosinophilic syndrome. Anti-IL5s were administered as a subcutaneous injection, according to the approved Canadian dosing scheme for asthma (Mepolizumab 100 mg every 4 weeks, or Benralizumab 30 mg every 4 weeks for 3 doses, then every 8 weeks).
Data Collection
Demographics including age, sex, body mass index (BMI), smoking history and number of pack-year were recorded at baseline visit. Disease and exacerbation-related data, airway comorbidities, lung function and inflammatory profile were collected at V0 and V1. COPD exacerbations were defined as an acute worsening of respiratory symptoms that resulted in additional systemic therapy such as antibiotics and/or oral corticosteroids (OCS).
Study Outcomes
Treatment efficacy was assessed using the reduction in annual exacerbation rate and/or OCS daily dose in OCS-dependent patients, between V0 and V1. Secondary outcomes included change in forced expiratory volume in one second (FEV1) and inflammatory biomarkers (blood eosinophils, sputum eosinophils and FeNO) between V0 and V1. Cases are presented using descriptive statistics. Continuous variables are presented as means (± SD or range) and categorical variables are presented as numbers (%). Although statistical analysis of results such as paired T-tests would have been interesting, the small sample size provided by our case series did not allow for them to be appropriately performed.
Results
Participants
Seven COPD patients (5M:2F) received an anti-IL5 in our COPD clinic. Baseline characteristics are shown in Table 1. All had radiological evidence of emphysema and had a severely impaired lung function with a mean FEV1 of 34.6 ± 13.2%. One patient was a never smoker (case 5) but was diagnosed with a genetic form of COPD. One patient had a previous diagnosis of asthma (before age 40) and two had a historical FEV1 reversibility of more than 200 mL, but less than 400 mL.
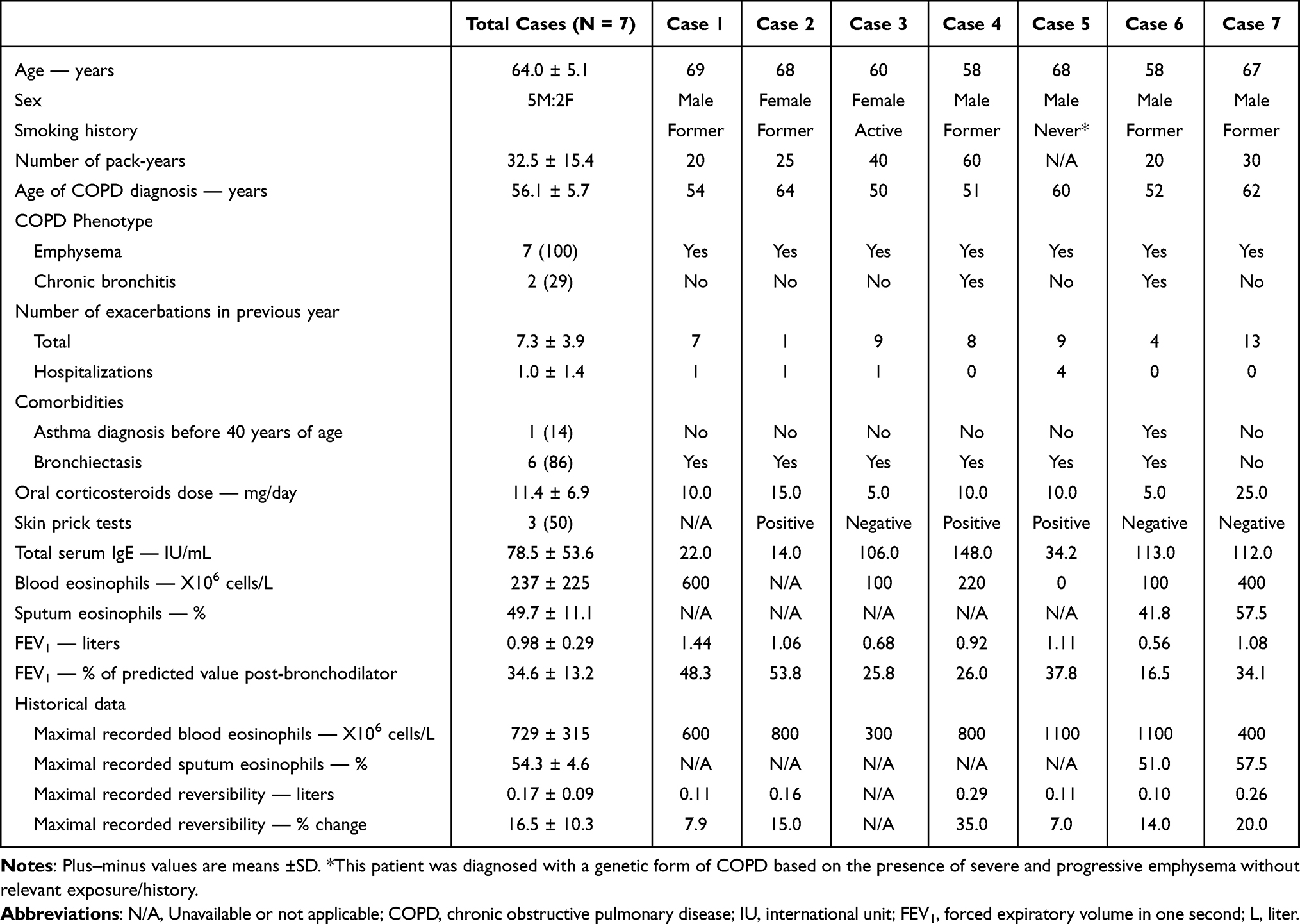 |
Table 1 Participants Characteristics at Baseline (V0) |
All patients were OCS-dependent at baseline. Despite chronic use of OCS, 6/7 patients remained frequent exacerbators (exacerbation rate 7.3 ± 3.9) and 5/6 had evidence of residual eosinophilic inflammation (blood eosinophil levels 237 ± 225×106 cells/L). Before chronic OCS use, the mean blood eosinophils count was 729 ± 315×106 cells/L. Sputum eosinophils were only available for cases 6 and 7 and were respectively 41.8% and 57.5%.
Therapeutic Response
Five patients had completed 12 months of anti-IL5/IL5R treatment at the time of data extraction. In these patients, the mean OCS dose was reduced from 12.0 ± 7.6 to 2.6 ± 4.3 mg/day, corresponding to a 78% decrease from baseline (Figure 1). Three patients completely stopped using OCS. Despite the reduction in OCS dose, patients’ annual exacerbation rate was decreased by 88%, from 8.2 ± 3.3 to 1.0 ± 1.2 (Figure 2). Post-treatment outcomes are presented in Table 2.
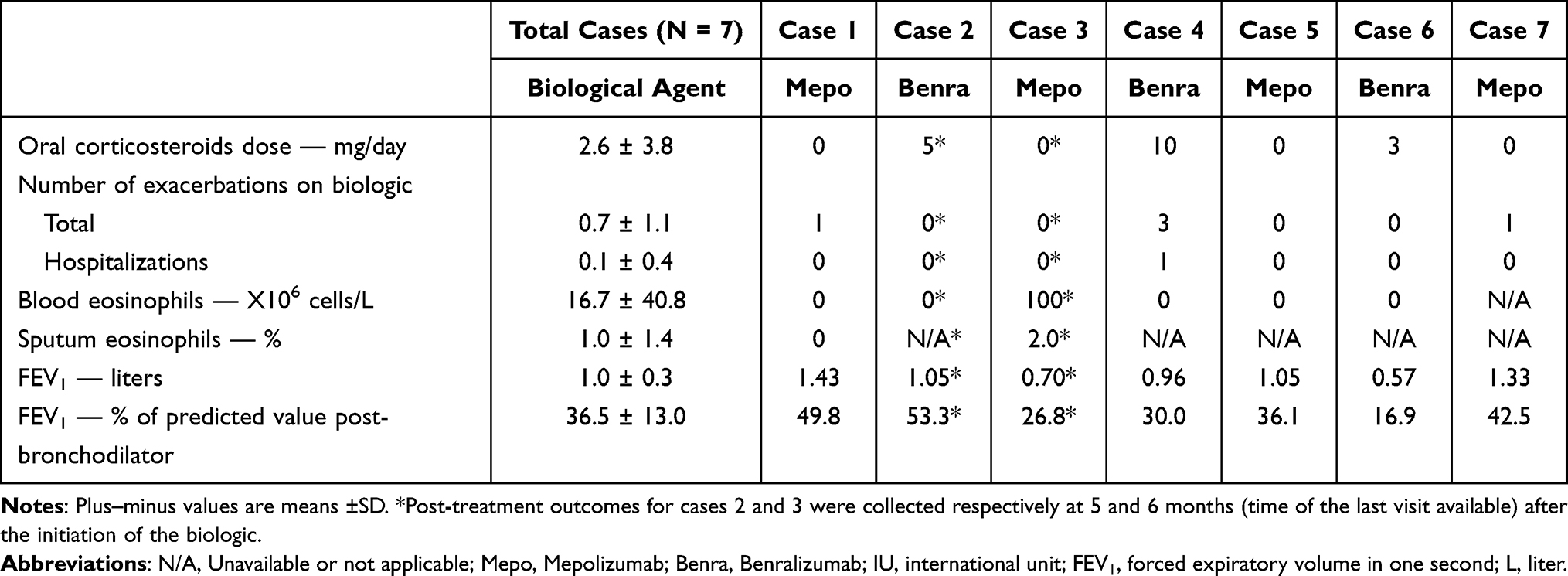 |
Table 2 Post-Treatment Outcomes (V1) |
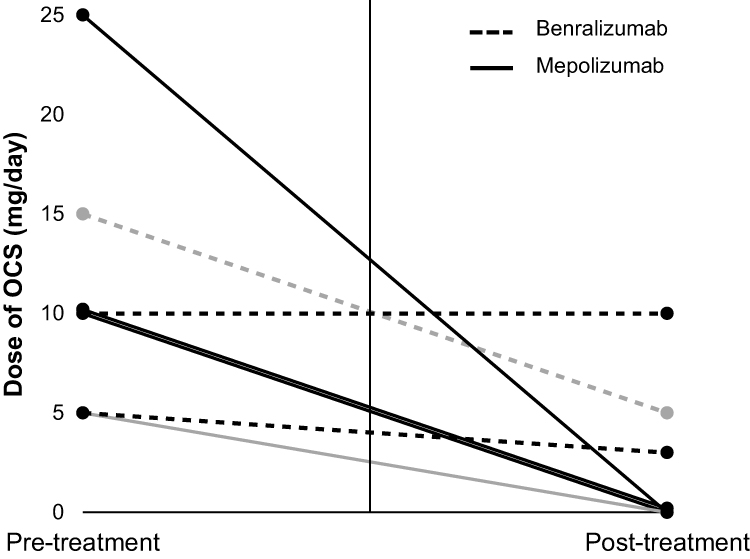 |
Figure 1 Daily oral corticosteroids intake. Abbreviation: OCS, oral corticosteroids. Notes: Cases that had not completed 12 months of anti-IL5/5R treatment at the time of data collection are represented by grey lines. Oral corticosteroids intake for cases 2 and 3 were collected respectively at 5 and 6 months (time of the last visit available) after the initiation of the biologic. |
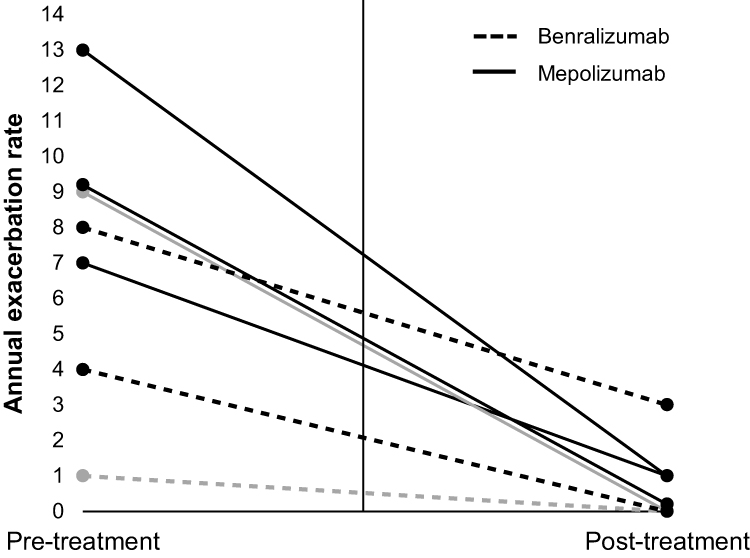 |
Figure 2 Annual exacerbation rate. Notes: Cases that had not completed 12 months of anti-IL5/5R treatment at the time of data collection are represented by grey lines. Annual exacerbation rate for cases 2 and 3 were collected respectively at 5 and 6 months (time of the last visit available) after the initiation of the biologic. |
Other Outcomes
After one year of biological treatment, the mean blood eosinophils count was reduced from 237 ± 225 to 0.0 ± 0.0×106 cells/L (Figure 3). One case had residual blood eosinophil inflammation (100 X 106 cells/L) but had not completed 12 months of anti-IL5 at the time of data collection (Table 2). Sputum eosinophils change could not be evaluated because of insufficient data. There was a non-clinically significant increase in mean FEV1 from 0.98 ± 0.29 to 1.07 ± 0.30 L between V0 and V1.
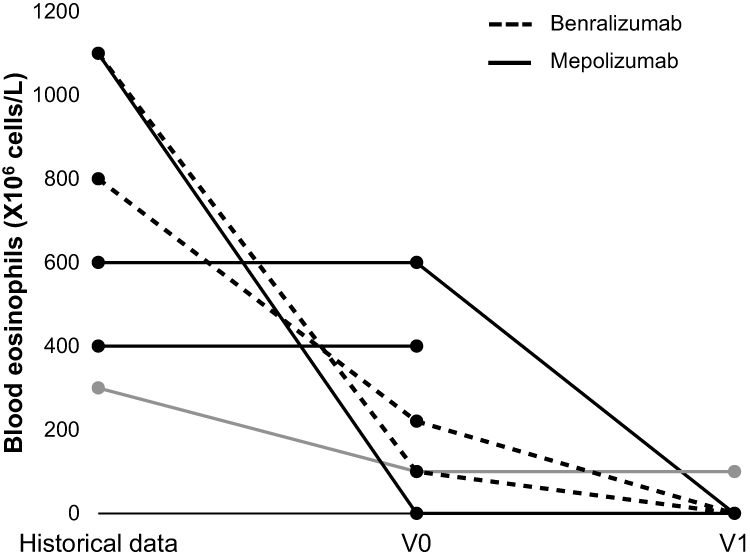 |
Figure 3 Blood eosinophils levels. Notes: Historical blood eosinophil level was measured in the last 3 years before baseline visit (V0). Cases that had not completed 12 months of anti-IL5/5R treatment at the time of data collection are represented by grey lines. Blood eosinophil levels for cases 2 and 3 were collected respectively at 5 and 6 months (time of the last visit available) after the initiation of the biologic. |
Discussion
To our knowledge, this case series is the first to report the benefits of anti-IL5/IL5R therapies in COPD patients chronically treated with OCS. In this real-world setting study, COPD patients selected for treatment with anti-IL5 were all OCS-dependent and displayed significant blood and/or sputum eosinophilic inflammation, either on OCS or prior to their initiation. These observed improvements parallel the benefits demonstrated in OCS-dependent asthma, decreasing OCS use and exacerbation rates.1–3
Four phase 3 parallel-group trials have reported results of anti-IL5/IL5R therapy in eosinophilic COPD patients.18,19 In these trials, the eosinophilic phenotype was defined using blood eosinophils counts: ≥150 × 106 cells/L at screening or ≥300 × 106 cells/L during the previous year for Mepolizumab trials (METREX and METREO),18 and ≥220 × 106 cells/L at screening for Benralizumab trials (GALATHEA and TERRANOVA).19 In these selected populations, only the METREX trial, studying Mepolizumab, reached statistical significance in an efficacy endpoint, reducing exacerbations by 18% compared to placebo. These results are far from the 50% exacerbation rate reduction seen in asthma with these therapies.20,21 However, with an exacerbation rate reduction of 88%, our case series suggests that, when appropriately selected, COPD patients may have a similar response to asthmatics with anti-IL5s.
Asthma is an eosinophil-predominant disease, which is not the case of COPD. Using an imperfect albeit convenient biomarker such as blood eosinophils may result in more misclassification (false positive or false negative) of eosinophilic-driven disorders in low prevalence diseases such as COPD. Indeed, studies have shown that the correlation of blood to sputum eosinophils is weaker in COPD when compared to asthma, suggesting that blood eosinophils are a less efficient biomarker to identify patient with an eosinophilic phenotype in this disease.22 Therefore, selecting the COPD study population for anti-IL5 trials based on the same eosinophils criteria as asthmatics may have contributed to the deceiving results of these drugs in COPD. More specific predictors of eosinophilic disease in COPD are required to identify patients that may respond to biologic therapy.
Our small study suggests that, as shown in asthma, OCS use could be a predictor of response to anti-IL5 therapies in COPD.23 Patients treated with daily OCS are however systematically excluded from trials studying monoclonal antibodies in COPD, including those currently ongoing. One should understand that, although OCS is a recognized treatment for severe asthma, they are not recommended for daily use in COPD due to a lack of clear demonstrated benefits and potential for harm.24 There is however a role for chronic OCS in COPD with eosinophilic airway inflammation as shown in a 2007 study by Siva et al.12 In this randomized control trial (RCT), 40% of COPD patients received regular OCS to reduce their sputum eosinophils and this strategy was associated with a 62% reduction in severe exacerbations. Even though guidelines do not recommend it, regular OCS are sometimes used in clinical practice in selected COPD patients with recurrent exacerbations needing frequent OCS bursts to reduce the overall steroid burden. Long-term OCS use have however been associated with an increased mortality risk in COPD and strategies are therefore needed to replace its use, even if already limited in this disease.25 Including these patients in future anti-IL5 trials should be considered.
The impressive reduction in exacerbations with anti-IL5 in our patients suggests that most of their exacerbations were eosinophilic. This would be an unusual finding as most COPD patients have a heterogeneity in the nature of their exacerbation. A study investigating biomarkers expression in acute exacerbation of COPD identified four biologic clusters population for exacerbation events: bacterial-predominant, viral-predominant, eosinophilic-predominant or pauciinflammatory.26 Among the twenty-five percent of COPD patients identified with eosinophilic-predominant exacerbations, only 60% of their exacerbations were eosinophilic. This intra-patient variability in exacerbations nature potentially limits the maximal benefit of anti-IL5s in COPD. However, with an 88% reduction in exacerbations twelve months after anti-IL5 initiation, our study population seemed to display more homogeneous eosinophilic exacerbations. Once again, their OCS-dependent status is probably responsible as clinicians are probably more likely to continue long-term OCS in COPD patients who improve dramatically after their introduction. It is yet unclear whether this chronic OCS response should be used to identify COPD patients with eosinophilic exacerbations who might be candidate for biologics, but according to our study results, it certainly deserves further consideration.
One could wonder if the OCS-dependent COPD patients of our case series are not merely severe asthmatics, explaining the good response to OCS and anti-IL5 therapy. Distinguishing asthma from COPD is indeed challenging in older individuals with a history of smoking, as typical features of asthma are also more prevalent in COPD. For example, a significant bronchodilator response is found in up to 50% of COPD patients, without necessarily indicating an overlap.27 All our cases had radiological emphysema, confirming a COPD component to their airway disease. Although one patient was a never smoker, he suffered from severe and progressive panlobular emphysema in the absence of relevant exposure/history and a lung resection specimen from a lung volume reduction surgery revealed no pathological disease other than emphysema. Alpha-one antitrypsin deficiency (AATD) screening was negative, but the patient had a familial history of premature emphysema, suggesting an unidentified non-AATD genetic COPD. The COPD diagnosis in this never smoker therefore seems appropriate. Only one patient had a previous diagnosis of asthma, hence a definitive asthma-COPD overlap (ACO). No other patient of our series met the criteria for ACO, as defined by an international panel of expert in 2016.28 We can then safely assume that, except for one patient with ACO, our case series was mainly composed of COPD patients.
Limitations
This series being retrospective in nature and involving a small sample size, its results must be taken cautiously. A selection bias may have occurred as COPD patients treated with anti-IL5/5Rs in our institution were first offered to enroll in ongoing clinical trials studying biological therapies in COPD. To be included in this case series, they either refused to participate in the trials or did not meet the inclusion criteria. Another selection bias was introduced by the need for the drug to be covered by the patients’ insurance plan.
The nature of the exacerbations was not assessed, therefore any results involving exacerbation are affected by the clinician evaluation and ensuing choice of treatment. It however reflects the current real-world use of biologic therapy in COPD patients. It is yet unknown if the benefits reported in this study are sustainable over time.
Conclusion
In conclusion, our case series suggests that monoclonal antibodies targeting IL5 or its receptor may be effective in decreasing OCS exposure and exacerbation rate among eosinophilic COPD patients treated with chronic OCS. These findings need further validation but may serve to better select the population to be included in clinical trials studying biologic therapy in COPD.
Acknowledgments
Jeremy Laroche received a summer scholarship from Laval University for working on this study.
Disclosure
Dr Andréanne Côté reports grants from GSK, advisory boards, presentations from Sanofi, GSK, AstraZeneca, and valeo, outside the submitted work. Dr Krystelle Godbout reports personal fees, advisory board Co Investigator in industry sponsored research from AstraZeneca, personal fees from Boehringer Ingelheim, personal fees from Covis, personal fees, advisory board Co Investigator in industry sponsored research from GlaxoSmithKline, personal fees, advisory board Co Investigator in industry sponsored research from Sanofi, personal fees from Novartis, personal fees from Valeo, personal fees from TEVA, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Farne HA, Wilson A, Powell C, Bax L, Milan SJ. Anti-IL5 therapies for asthma. Cochrane Database Syst Rev. 2017;9(9):CD010834. doi:10.1002/14651858.CD010834.pub3
2. Nair P, Wenzel S, Rabe KF, et al. Oral glucocorticoid-sparing effect of benralizumab in severe asthma. N Engl J Med. 2017;376(25):2448–2458. doi:10.1056/NEJMoa1703501
3. Bel EH, Wenzel SE, Thompson PJ, et al. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. 2014;371(13):1189–1197. doi:10.1056/NEJMoa1403291
4. Pelaia C, Paoletti G, Puggioni F, et al. Interleukin-5 in the pathophysiology of severe asthma. Front Physiol. 2019;10:1514. doi:10.3389/fphys.2019.01514
5. Schleich FN, Chevremont A, Paulus V, et al. Importance of concomitant local and systemic eosinophilia in uncontrolled asthma. Eur Respir J. 2014;44(1):97–108. doi:10.1183/09031936.00201813
6. Flood-Page P, Swenson C, Faiferman I, et al. A study to evaluate safety and efficacy of mepolizumab in patients with moderate persistent asthma. Am J Respir Crit Care Med. 2007;176(11):1062–1071. doi:10.1164/rccm.200701-085OC
7. GOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2022 report). Available from: https://goldcopd.org/wp-content/uploads/2021/12/GOLD-REPORT-2022-v1.1-22Nov2021_WMV.pdf.
8. Barnes PJ. Immunology of asthma and chronic obstructive pulmonary disease. Nat Rev Immunol. 2008;8(3):183–192. doi:10.1038/nri2254
9. Zhu J, Qiu YS, Majumdar S, et al. Exacerbations of bronchitis: bronchial eosinophilia and gene expression for interleukin-4, interleukin-5, and eosinophil chemoattractants. Am J Respir Crit Care Med. 2001;164(1):109–116. doi:10.1164/ajrccm.164.1.2007050
10. Yun JH, Lamb A, Chase R, et al. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2018;141(6):2037–2047. doi:10.1016/j.jaci.2018.04.010
11. Kerkhof M, Sonnappa S, Postma DS, et al. Blood eosinophil count and exacerbation risk in patients with COPD. Eur Respir J. 2017;50(1):1700761. doi:10.1183/13993003.00761-2017
12. Siva R, Green RH, Brightling CE, et al. Eosinophilic airway inflammation and exacerbations of COPD: a randomised controlled trial. Eur Respir J. 2007;29(5):906–913. doi:10.1183/09031936.00146306
13. Brightling CE, Monteiro W, Ward R, et al. Sputum eosinophilia and short-term response to prednisolone in chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 2000;356(9240):1480–1485. doi:10.1016/S0140-6736(00)02872-5
14. Pascoe S, Barnes N, Brusselle G, et al. Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: analysis of the IMPACT trial. Lancet Respir Med. 2019;7(9):745–756. doi:10.1016/S2213-2600(19)30190-0
15. Pascoe S, Locantore N, Dransfield MT, Barnes NC, Pavord ID. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3(6):435–442. doi:10.1016/S2213-2600(15)00106-X
16. Bafadhel M, McKenna S, Terry S, et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease: a randomized placebo-controlled trial. Am J Respir Crit Care Med. 2012;186(1):48–55. doi:10.1164/rccm.201108-1553OC
17. Bafadhel M, Peterson S, De Blas MA, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6(2):117–126. doi:10.1016/S2213-2600(18)30006-7
18. Pavord ID, Chanez P, Criner GJ, et al. Mepolizumab for Eosinophilic chronic obstructive pulmonary disease. N Engl J Med. 2017;377(17):1613–1629. doi:10.1056/NEJMoa1708208
19. Criner GJ, Celli BR, Brightling CE, et al. Benralizumab for the prevention of COPD exacerbations. N Engl J Med. 2019;381(11):1023–1034. doi:10.1056/NEJMoa1905248
20. Ortega HG, Liu MC, Pavord ID, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014;371(13):1198–1207. doi:10.1056/NEJMoa1403290
21. Bleecker ER, FitzGerald JM, Chanez P, et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet. 2016;388(10056):2115–2127. doi:10.1016/S0140-6736(16)31324-1
22. Pignatti P, Visca D, Cherubino F, et al. Do blood eosinophils strictly reflect airway inflammation in COPD? Comparison with asthmatic patients. Respir Res. 2019;20(1):145. doi:10.1186/s12931-019-1111-1
23. Bleecker ER, Wechsler ME, FitzGerald JM, et al. Baseline patient factors impact on the clinical efficacy of benralizumab for severe asthma. Eur Respir J. 2018;52(4):1800936. doi:10.1183/13993003.00936-2018
24. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
25. Chang YP, Lai CH, Lin CY, et al. Mortality and vertebral fracture risk associated with long-term oral steroid use in patients with chronic obstructive pulmonary disease: a systemic review and meta-analysis. Chron Respir Dis. 2019;16:1479973119838280. doi:10.1177/1479973119838280
26. Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662–671. doi:10.1164/rccm.201104-0597OC
27. Calverley PM, Albert P, Walker PP. Bronchodilator reversibility in chronic obstructive pulmonary disease: use and limitations. Lancet Respir Med. 2013;1(7):564–573. doi:10.1016/S2213-2600(13)70086-9
28. Sin DD, Miravitlles M, Mannino DM, et al. What is asthma-COPD overlap syndrome? Towards a consensus definition from a round table discussion. Eur Respir J. 2016;48(3):664–673. doi:10.1183/13993003.00436-2016
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Omalizumab Treatment Over a 16-Year Follow-Up: When a Clinical Trial Meets Real-Life
Menzella F, Fontana M, Contoli M, Ruggiero P, Galeone C, Capobelli S, Simonazzi A, Catellani C, Scelfo C, Castagnetti C, Livrieri F, Facciolongo N
Journal of Asthma and Allergy 2022, 15:505-515
Published Date: 21 April 2022
FIDEPOC: Consensus on Inspiratory Flow and Lung Deposition as Key Decision Factors in COPD Inhaled Therapy
González-Torralba F, Baloira A, Abad A, Fuster A, García-Rivero JL, García-Sidro P, Márquez-Martín E, Palop M, Soler N, Velasco JL
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1005-1015
Published Date: 4 May 2022
The Microbiome in COPD: Emerging Potential for Microbiome-Targeted Interventions
Millares L, Monso E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1835-1845
Published Date: 12 August 2022
Use of Remote Cardiorespiratory Monitoring is Associated with a Reduction in Hospitalizations for Subjects with COPD
Polsky M, Moraveji N, Hendricks A, Teresi RK, Murray R, Maselli DJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:219-229
Published Date: 3 March 2023
Exacerbations and Real-World Outcomes After Single-Inhaler Triple Therapy of Budesonide/Glycopyrrolate/Formoterol Fumarate, Among Patients with COPD: Results from the EROS (US) Study
Strange C, Tkacz J, Schinkel J, Lewing B, Agatep B, Swisher S, Patel S, Edwards D, Touchette DR, Portillo E, Feigler N, Pollack M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2245-2256
Published Date: 12 October 2023