Back to Journals » Advances in Medical Education and Practice » Volume 16
Transfer of Laparoscopic Skills From Box Trainer Simulation to Real Life: A Bi-Center Study in Pakistan
Authors Aftab R, Ali SM, Ali A, Shahid N, Arja SB ![]() , Ahmed M, Nafees R, Shahid M
, Ahmed M, Nafees R, Shahid M ![]()
Received 25 July 2025
Accepted for publication 25 October 2025
Published 30 October 2025 Volume 2025:16 Pages 2003—2012
DOI https://doi.org/10.2147/AMEP.S556187
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Rabia Aftab,1 Syed Moin Ali,2 Aun Ali,3 Nadia Shahid,4 Sateesh B Arja,5 Muhammad Ahmed,3 Rubab Nafees,3 Madeeha Shahid6
1Department for Educational Development and Anesthesiology, Aga Khan University, Karachi, Pakistan; 2Department for Educational Development, Aga Khan University, Karachi, Pakistan; 3Department for General Surgery, Fazaia Ruth Pfau Medical College, Karachi, Pakistan; 4Department for General Surgery, Ziauddin University, Karachi, Pakistan; 5Medical Education Department, Avalon University School of Medicine, Willemstad, Curacao; 6Department for General Surgery, Niazi Medical and Dental College, Sargodha, Pakistan
Correspondence: Rabia Aftab, Department for Educational Development and Anesthesiology Aga Khan University, Karachi, Pakistan, Tel +923002036450, Email [email protected]
Introduction: Laparoscopic surgery is growing in importance, and laparoscopic training is being incorporated into surgical residency programs in Pakistan, despite limited access to training centers. This study emphasizes the need for residents to acquire essential psychomotor skills through simulation tools like Box Trainers (BTs), which are cost-effective and proven to improve laparoscopic performance. However, gaps remain in standardizing laparoscopic training, and the effectiveness of simulation in skill transfer to real-life surgery is still uncertain. The study aims to evaluate the transferability of skills acquired via BTs and gather residents’ perceptions of their usefulness at two medical centers in Karachi.
Methods: The authors used a quasi-experimental design to assess the effect of a three-month laparoscopic skills simulation training course on surgical and gynecology residents’ surgical performance. The total sample size is 41, and the study was conducted for 13 months. The residents were provided with structured step-by-step training in a hierarchical order of four tasks for three months. The task includes ball transfer, ring transfer, cutting pieces of paper, and suturing and Knotting. A duly qualified surgery faculty member observed all the residents using the Global Operative Assessment of Laparoscopic Skills (GOALS) as an assessment tool at the end of training and in a real-life setting after training. The perceptions were taken via questionnaires.
Results: This study’s findings indicate no significant difference in the scores of residents when shifting from simulation to real-life tasks for ball transfer (p-value of 0.32) and ring transfer (p-value of 0.47). This lack of significant difference suggests that simulation training for these tasks effectively prepared the residents for real-life application. In other words, the skills learned in simulation were successfully translated to real-life scenarios for these tasks. Also, findings reveal a significant improvement in scores from simulation to real-life for precision cutting, simple suturing, and knot tying. This improvement suggests that while residents may initially perform at a similar level in both settings for some tasks, there is an observable enhancement in their ability to perform more complex tasks when transitioning from simulation to real-life.
Discussion: The postgraduate residents demonstrated significant improvements across all tasks, highlighting the productivity of the simulation-based practical training in enhancing and transferring laparoscopic skills.
Keywords: simulation, transfer, laparoscopic skills, residents, surgical education, training box
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zulianto has been published for this article.
Introduction
The development of psychomotor skills has been a special focus of surgical residency programs. The traditional method of teaching these procedures to residents in the operating room, on real patients, and under the supervision of a senior surgeon has been questioned due to concerns about patient safety and ethical considerations. It is no longer considered ethically acceptable for inexperienced trainees to work with patients to hone their skills, and stringent clinical safety regulations have established substantial limitations on the practice of working with real patients. To aid in the training process, prevent adverse patient outcomes, and improve trainees’ performance in the operating room, the focus has shifted to simulators and simulation-based training.
Laparoscopic surgery has recently emerged as an advanced technique in Pakistan’s surgical landscape. Due to the growing role of laparoscopy in modern surgery, surgical residency programs have incorporated laparoscopic training in their curriculum.1 Currently, only a few centers offer training in this procedure. Ideally, residents must develop a basic skill set during residency training necessary for their laparoscopic practice in a real-life setting.2 Conducting laparoscopic surgery safely demands specific psychomotor skills from the surgeon. These encompass adapting to the shift from three-dimensional to two-dimensional vision, bi-manual dexterity, managing long instruments with an amplified tremor, addressing the fulcrum effect, and coping with reduced tactile feedback.3
There is increased use of simulation as a teaching tool in laparoscopy. The gold standard for educating surgical residents and optimizing time in the operating room is laparoscopic skills training conducted outside the surgical setting.4 Literature supports the positive impact of this training on residents, contributing to enhanced operative performance. The Box Trainer (BT), a simulator that utilizes standard laparoscopic equipment, is cost-effective and exceptionally versatile.5 It allows residents to undergo training on both animal parts and synthetic inanimate models.6 Studies have demonstrated its validity and its substantial enhancement of laparoscopic skills.2
Lack of basic laparoscopic training has been observed in general surgery and gynecological residency programs. Some surgeons are interested in practicing laparoscopic techniques but lack expertise in how to use the laparoscope.7 Recent technological advances, insufficient training, concerns regarding complications, and a lack of passion to negotiate learning curves make the transition to minimally invasive procedures challenging. During residency training, exposure to laparoscopic and minimal-access surgery is neither standardized nor optimal at some training sites. Furthermore, despite simulations being used in various institutions, it is unknown whether the training being carried out impacts the transfer of skills to the real setting.8
Also, studies from Pakistan have demonstrated measurable improvements in learners’ clinical skills competence through simulation-based learning (eg, among undergraduate nursing students in Karachi) and clinical decision-making skills among final-year nursing students in Swat.9 A recent scoping review of 145 studies from Pakistan highlights that, while simulation use increases, challenges persist with faculty training, access inequalities, and funding, particularly for high-fidelity simulation technologies.10 Regarding cost-effectiveness, although direct economic evaluations of simulation in healthcare in Pakistan are limited, evidence from analogous training programs (eg, research training using video-teleconferencing versus face-to-face in Pakistan) shows that lower-resource modalities can yield significant returns in skills gains per cost invested.11 These data underscore the necessity and timeliness of our study in Pakistan: to map where simulation is used and how cost-efficient and sustainable simulation-based training can be in the local health education landscape. This study explores skill transference of BTs by using “Global Operative Assessment of Laparoscopic Skills (GOALS)”. The objectives of this study are:
1. Assess the transferability of laparoscopic surgical skills from simulation to a real-life setting in low- and middle-income settings after training on Box Trainers. 2. Determine the perception of surgical and gynecological residents on Box-trainers as a training tool at Fazaia Ruth Pfau Medical College, Karachi.
Methodology
This quasi-experimental study included Surgery and Obstetrics and Gynecology residents from two private-sector teaching hospitals of Fazaia Ruth Pfau Medical College in Karachi, Pakistan. After obtaining official permission from the teaching hospitals, the primary investigator and five surgeons developed a three-month training course on BT. The course was conducted in the simulation lab at one of the two hospitals. The study was completed in 13 months. Data collection started in August 2023 and was completed in December 2023. Before the training course, the principal investigator conducted a workshop for the trainers on using GOALS for scoring. After this frame-of-reference training, the residents were assessed for their laparoscopic surgical procedures on GOALS in a real-life setting. These were considered GOALS scores obtained before training; this helped establish the baseline competence. GOALS is an intraoperative, validated assessment tool specific to laparoscopic skills.12 It comprises a 5-item global rating scale, a 10-item checklist, and two visual analogue scales (VAS) (Appendix A). The Box Trainer, a simulator that utilizes standard laparoscopic equipment, is cost-effective and exceptionally versatile. It allows residents to undergo training on both animal parts and synthetic inanimate models. During the early years of surgical residency, organized training on Box Trainers has proven effective in enhancing the laparoscopic skills of residents. The box trainer has a board inside a black training box with rubber gaskets around it to hold the scope and tool cannulas. Utilizing a fiberoptic light source and camera gear, the image is shown on a video monitor. The following tools were employed:
The two forceps open both jaws; the third is a pair of scissors that open both blades and bend left (Maryland Dissector); and the fourth is a modular needle holder with a straight carbide insert and a top lock. The box trainer used in this study belongs to a low-fidelity simulator since the institution has already procured it.
The specialties involving laparoscopic surgery are Surgery and Obstetrics and Gynecology. Each residency is four years’ duration. Residents of years 3 and 4, who attended the complete course, were included. Those who missed three or more BT course sessions and did not give voluntary consent were excluded. Universal sampling was used since all the residents were potentially included in the study. The sample size was initially 44.
Three-month Training Course
Before the commencement of the training, the team organized a one-hour orientation session in which the PI provided details of the course to the residents. The PI also explained the use of data for research purposes. During this session, residents showed concerns regarding using BT and research data. After the clarifications, the residents signed the consent form after ensuring confidentiality and anonymity. A Google Form was emailed to the residents for registration. The residents were provided with structured step-by-step training in the four tasks during the course. These tasks were: (1) ball transfer, (2) Ring Transfer, (3) Circle Cutting and (4) Intra-corporeal square knots. During each session in the course, residents were provided with an orientation, a demonstration of the task, and an opportunity for clarification, followed by supervised practice by a qualified surgeon. After the orientation and demonstration of one task, they were given two weeks for practice on the BT. At the end of the second week, one of the team members observed the residents and provided immediate feedback using GOALS. These were considered “GOALS scores in simulation lab taken immediately after training”. The number of practice sessions for each task varied among the residents depending on their attainment of competence. Each resident was given an equal amount of time for practice. One senior surgeon and two junior faculty members from the surgery and allied departments supervised the practice session. At the end of two weeks, the senior surgeon evaluated all surgical and allied residents for that task quantitatively, who observed each performance and scored them on the GOALS form, along with providing constructive feedback.
GOALS Score in a Real-Life Setting
Once the residents had practiced the skills, the surgical team allowed them to perform the same set of skills on real patients under close supervision and scored them again based on direct observations. The expert surgeon assigned simple, elective, laparoscopic surgical procedures to them. The surgeon directly observed the performance to assess the residents’ ability to perform the procedures on real patients. These were considered “GOALS scores in a real-life setting after training”. Each patient was given a consent form explaining the research. This phase helped provide information to assess how well the skills had been transferred.
The following surgical procedure was chosen to test the skills in real-life scenarios.
General Surgery
- Laparoscopic cholecystectomy
- Laparoscopic appendectomy
Gynecology and Obstetrics
- Lap and dye
- Diagnostic laparoscopy and oophorectomy
An indigenously developed form was used to collect feedback from the residents regarding their perceptions of the three-month box training course. It was a paper-based survey form, as it was more convenient for residents to fill out.
The scores of GOALS before the start of the BT training, at the end, and on real patients were statistically analyzed using R version 4.5.1. The p-values of < 0.05 were regarded as significant. Cronbach’s alpha was used to determine the internal consistency of the feedback form. A repeated measure ANOVA was used to compare the three sets of data collected, while a paired t-test was employed to compare the data between groups.
Results
Among the 44 residents, 41 (93%) completed the training program. Out of these, 21 (51.2%) were in residency year three (R3), and 20 (48.8%) were in residency year four (R4). 27 (65.9%) residents were from General Surgery, while 14 (34.1%) were from Gynecology. This cohort had 27 (65.9%) female and 14 (34.1%) male residents. Please refer to Table 1.
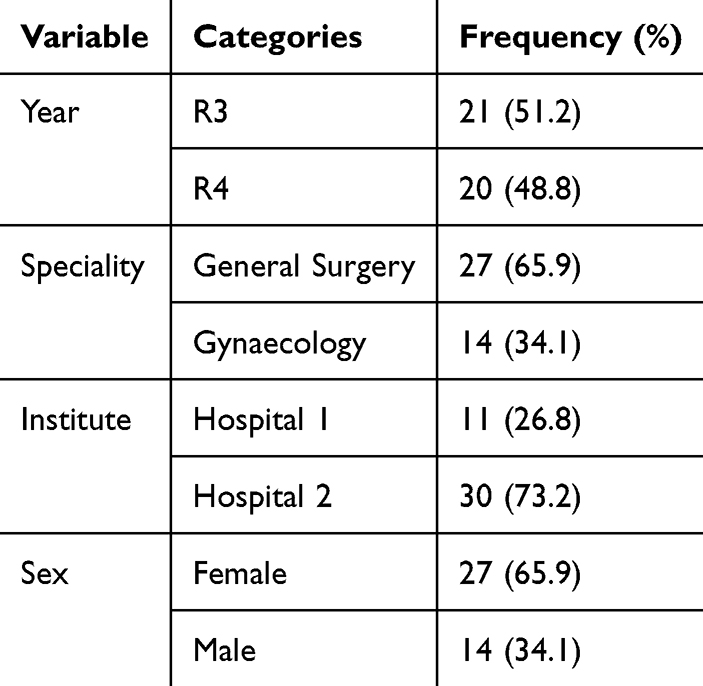 |
Table 1 Frequency of the Participants |
Resident performance was recorded and scored on four different tasks in (i) pre-training, (ii) simulation, and (iii) post-training (real-life) phases of data collection.
Task 1 – Ball Transfer
The performance in Task 1 was evaluated across three settings and between two groups as shown in Table 2. When the scores were compared between the three groups, it was statistically significant (p = 0.001), proving the transfer of skills from simulation to a real-life setting. In pair-wise comparison, the difference was statistically significant between pre-training and simulation scores and between pre-training and real-life assessment scores, confirming the effect of simulation-based training on the transfer of skills. However, this difference was statistically insignificant between simulation and real-life assessment scores, indicating that the skill was maintained when transitioned from simulation to a real-life setting.
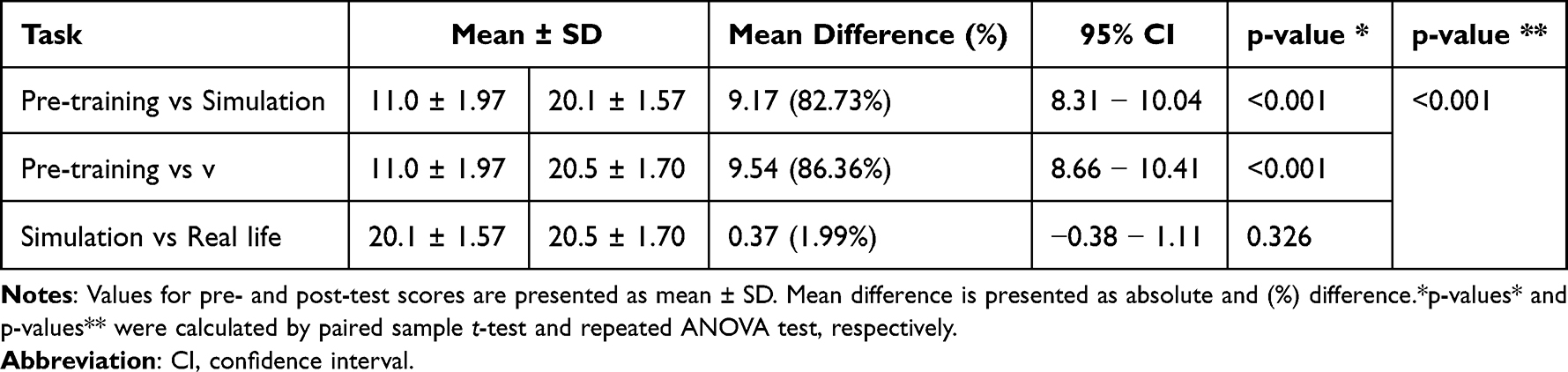 |
Table 2 Task 1 – Ball Transfer – Arranging the Beads in A Linear Pattern, T Pattern, And Circle |
Task 2 – Ring Transfer
The performance in Task 2 was evaluated across three settings and between two groups, as shown in Table 3. When the scores were compared between the three groups, it was statistically significant (p = 0.001), proving the transfer of skills from simulation to a real-life setting. In pair-wise comparison, the difference was statistically significant between pre-training and simulation scores and between pre-training and real-life assessment scores, confirming the effect of simulation-based training on the transfer of skills. However, this difference was statistically insignificant between simulation and real-life assessment scores, indicating that the skill was maintained when transitioned from simulation to a real-life setting.
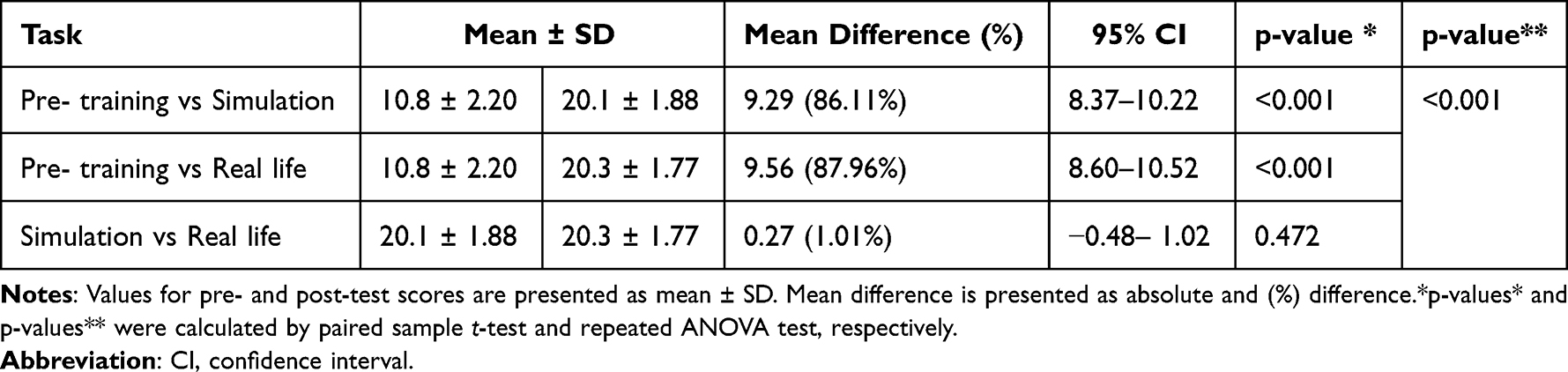 |
Table 3 Task 2 – Ring Transfer – Placing the Rings on The Pegs on Straight and Curved and Disassembling Them |
Task 3 – Precision Cutting
The performance in Task 3 was evaluated across three settings and between two groups as shown in Table 4. When the scores were compared between the three groups, it was statistically significant (p = 0.001), proving the transfer of skills from simulation to a real-life setting. In pair-wise comparison, the difference was statistically significant between pre-training and simulation scores and between pre-training and real-life assessment scores, confirming the effect of simulation-based training on the transfer of skills. However, this difference was also statistically significant between simulation and real-life assessment scores, indicating that the skill was performed even better when transitioned from simulation to a real-life setting.
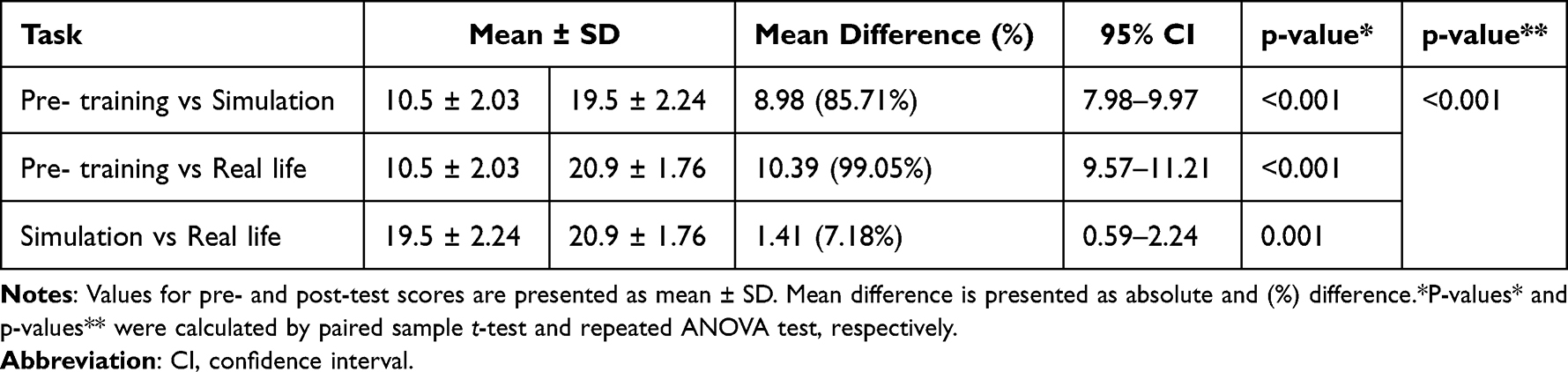 |
Table 4 Task 3 – Precision Cutting – Cutting A Semicircle on A Piece of Paper |
Task 4: Simple Suture and Knot Tying
The performance in Task 4 was evaluated across three settings and between two groups as shown in Table 5. When the scores were compared between the three groups, it was statistically significant (p = 0.001), proving the transfer of skills from simulation to a real-life setting. In pair-wise comparison, the difference was statistically significant between pre-training and simulation scores and between pre-training and real-life assessment scores, confirming the effect of simulation-based training on the transfer of skills. However, this difference was also statistically significant between simulation and real-life assessment scores, indicating that the skill was performed even better when transitioned from simulation to a real-life setting.
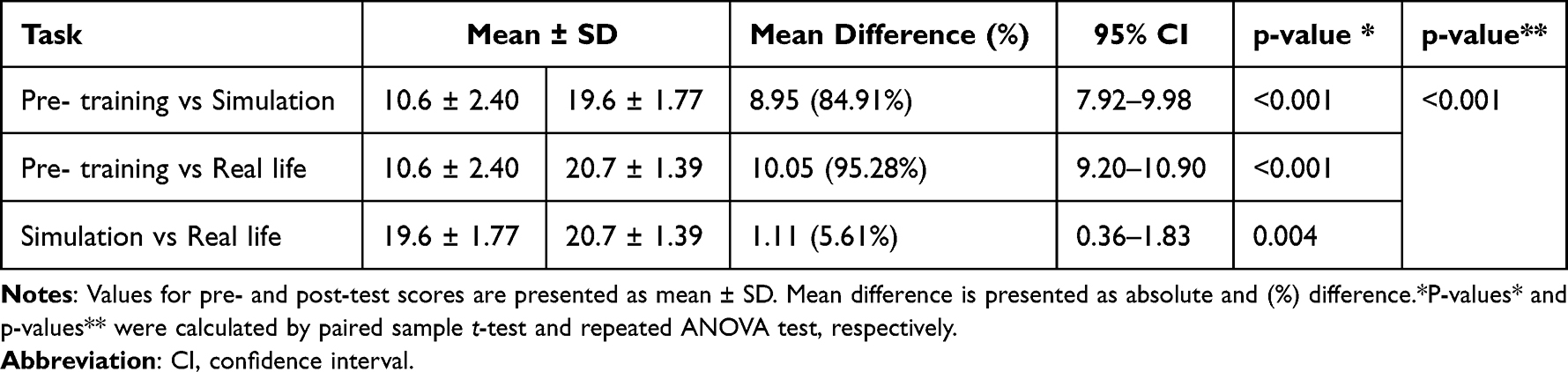 |
Table 5 Task 4 – Simple Suture and Knot Tying |
All 41 residents filled out the feedback form. Cronbach’s Alpha was found to be 0.64. For the sake of summarization, the responses of “strongly agree” and “agree” were merged into a single category, “agree.” Similarly, “strongly disagree” and “disagree” were incorporated into “disagree.”
The findings summarized in Table 6 indicate that in the residents found cohort BT is a highly valued tool in laparoscopic surgical training to be highly valuable, contributing significantly to skill acquisition, confidence building, and anxiety reduction. However, two items received special attention; only 24.3% of respondents were satisfied with the time given to them for BT training. Only 31.7% agreed they could effectively track their learning progress during BT training. 97% of residents expressed their satisfaction that BT training reduced their anxiety about performing laparoscopic surgery. In comparison, 83% of residents felt training on BT helped them to apply the simulated skill to real patients.
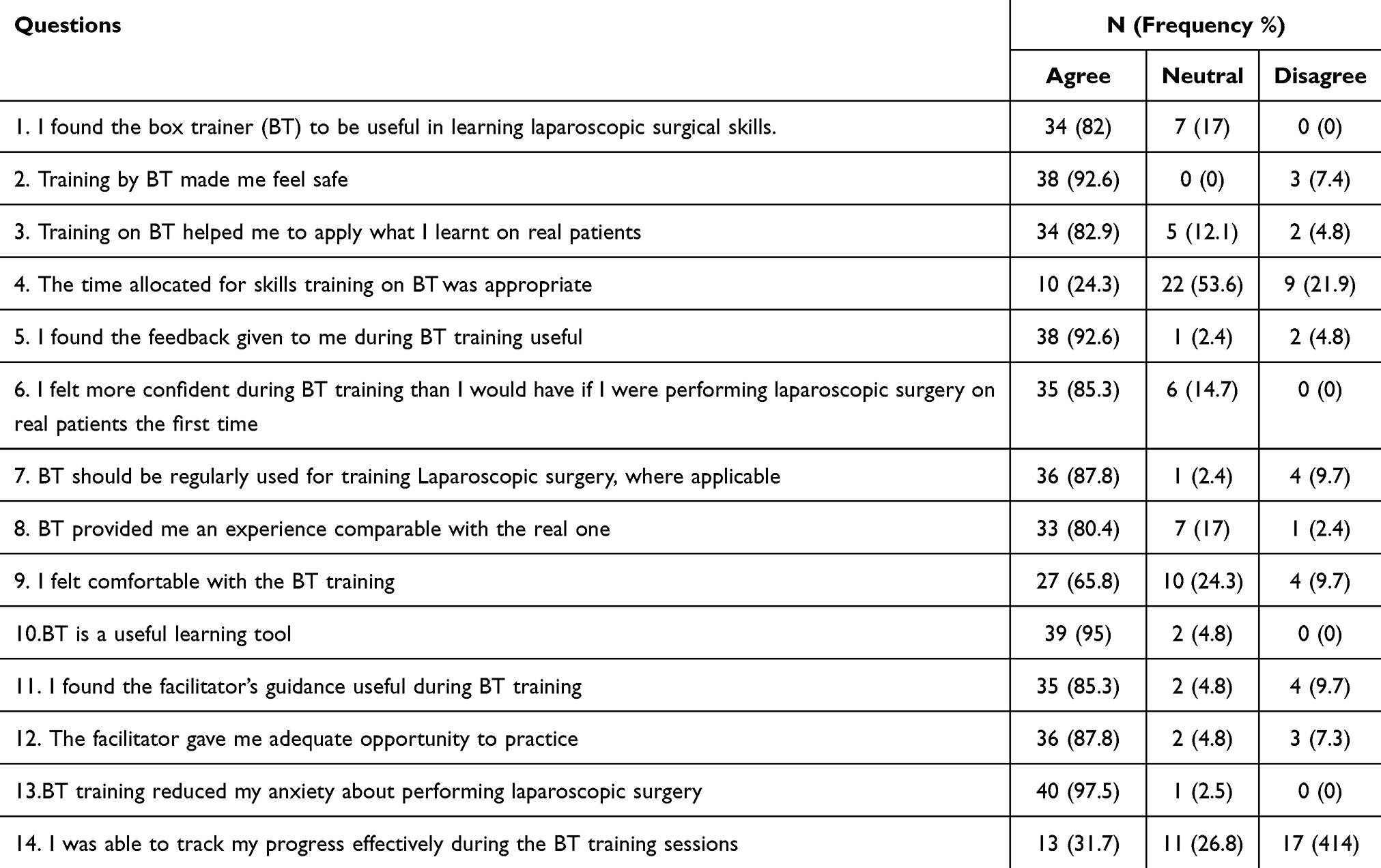 |
Table 6 Resident Perception of BT as a Training Tool |
Discussion
This study’s findings indicate no significant difference in the scores of residents when shifting from simulation to real-life tasks for ball transfer and ring transfer. This lack of significant difference suggests that simulation training for these tasks effectively prepared the residents for real-life application. In other words, the skills learned in simulation were successfully translated to real-life scenarios for these tasks. The existing literature provides a mixed view on the transferability of skills from simulation to real-life contexts. Studies such as those by Cook et al (2014) and Elendu et al (2024) suggest that simulation-based training can effectively translate skills to real-life settings, especially for procedural tasks. However, the effectiveness of this transfer can vary depending on the task’s complexity and the simulation’s quality. For simpler tasks like ball transfer and ring transfer, it appears that the simulation adequately mimicked the real-life environment, leading to no significant differences in performance. The lack of a significant difference for ball transfer and ring transfer could indicate that these tasks are less complex and may not require extensive hands-on practice beyond what is provided by simulation. The simulation environment likely provided a sufficient approximation of real-life conditions for these tasks, thus aligning the performance in both settings. This consistency supports the idea that simulation can be an effective training tool for simpler tasks.13,14
On the other hand, our findings reveal a significant improvement in scores from simulation to real-life for precision cutting, simple suturing, and knot tying. This improvement suggests that while residents may initially perform at a similar level in both settings for some tasks, there is an observable enhancement in their ability to perform more complex tasks when transitioning from simulation to real-life. Literature supports these findings, as studies by Imaizumi et al (2023), Orzech et al (2012), and Palter et al (2013) highlight that simulation training is particularly beneficial for complex skills that require higher levels of precision and technique. These tasks often involve more nuanced skills that may not be fully replicated in a simulated environment. As a result, the hands-on experience of real-life practice can significantly improve performance.15–17 The significant improvement observed for precision cutting, simple suturing, and knot tying suggests that these skills benefit from the additional practice and feedback that real-life tasks provide. The real-life environment may offer variables and challenges not fully captured in simulations, such as variations in tissue resistance and real-time adjustments, which contribute to skill refinement. Therefore, enhanced performance in real-life settings indicates that while simulations are valuable, they may need to be complemented with practical experience for complex tasks to achieve optimal skill development. The effectiveness of simulation training in surgical education has been widely studied and has been particularly effective in improving laparoscopic skills. A study conducted by Charokar & Modi (2021) examined the effectiveness of a structured 12-week laparoscopic training module for 16 residents from the General Surgery & Obstetrics and Gynecology departments. The study’s findings indicate that faculty-guided simulation training was feasible and well-accepted, supporting its incorporation into formal postgraduate training programs.18
Our study aligns with these earlier findings, showing significant improvements in laparoscopic skills on the simulator after training. These results are consistent with those reported by Dhariwal et al (2007).19 Appleton and Huguelet (2016) found that simulation is an effective teaching tool for residents. Studies have shown that simulators significantly enhance laparoscopic surgery training.20 A prospective, blinded, comparative study was conducted by Sadia et al (2019) in Pakistan. The effectiveness of box simulators was assessed by teaching the 72 gynecologists’ basic laparoscopic skills through six hands-on workshops. The results concluded that simulators significantly improved intraoperative skills performance.21 Khan et al (2020) conducted a quasi-experimental, single-arm, prospective cohort study involving 33 residents from the General Surgery and Gynecology programs. The intervention was a day-long laparoscopic skills workshop featuring lectures, videos and hands-on practice. The results showed higher Direct Observation Procedural Skills (DOPS) post-workshop scores with a p-value = 0.011.22 Resident perception offered invaluable insights into the strengths and weaknesses of BT as a training tool. Our study revealed that 97.5% of residents reported a significant reduction in anxiety about performing laparoscopic surgery after BT training. Additionally, 85.3% felt more confident using the BT. This suggests that simulation-based training plays a crucial role in enhancing residents’ confidence and reducing anxiety before performing real-life surgical procedures. Existing literature supports these findings. Anxiety reduction is crucial for surgical performance, as lower stress levels are associated with better decision-making, improved technical skills, and enhanced patient safety. For instance, Seltzer et al (2023) and Nicol et al (2016) both demonstrated that BTs effectively reduce anxiety and increase confidence among surgical residents.23,24 Seltzer’s study highlighted that BTs contribute to confidence in surgical fields, while Nicol’s study showed a significant reduction in anxiety among residents engaged with simulation training. In this study, 95% of residents agreed that BT is a valuable learning tool, reflecting its perceived effectiveness in improving laparoscopic skills. Chummun et al (2012) found that a formal laparoscopic training program using a “take-home” BT was preferred among participants for its practical use outside traditional training environments.25 The high percentage of residents recognizing BT’s utility reinforces its role as an effective educational tool in surgical training. The BT’s practicality and effectiveness in skill enhancement align with studies that underscore its value in providing hands-on training experiences. Resident dissatisfaction with providing support during the course needs to be explored. This dissatisfaction may be due to the lack of structured feedback and variability in feedback from different faculty members, which likely led to confusion and uncertainty regarding their progress. The importance of structured feedback in simulation-based training is well-documented. Studies such as Hatala et al (2014) and Parmar & Delaney (2011) emphasize that structured feedback and debriefing improve skill acquisition and reduce errors.26,27 Eppich et al (2015) further highlights the role of debriefing in enhancing learning outcomes and patient safety. Consistent, structured feedback is essential for optimizing learning and improving performance in simulation training. The findings suggest that incorporating structured feedback mechanisms could enhance the effectiveness of BT training and contribute to better skill development and patient safety.28 This study was conducted in Pakistan, a low to middle-income country with context-specific health system barriers, providing crucial insights into operationalizing and achieving simulation training effectiveness within resource-limited contexts. The study provides evidence for cost-effective training in regions that lack advanced technologies (such as virtual reality simulators) by showcasing the potential for BT to supplement surgical skills.
Limitations
This study involves a brief follow-up period in which skill retention and transferability were assessed and rapid improvement was demonstrated; however, long-term sustainment of those gains needs to be explored. The long-term impact of BT training on residents’ performance might be more thoroughly evaluated with a long-term follow-up. The choice of specific box trainers as a training tool could influence the observed outcomes. Various simulators are available in the market, each with distinct features and capabilities (eg, haptics, visual fidelity, feedback mechanisms). These variations may affect student engagement, learning outcomes, and ultimately, the transfer of laparoscopic skills. Future research should explore the impact of different platforms to determine the generalizability of my findings and identify the optimal features for practical surgical simulation training. The results should be interpreted cautiously as potential confounding factors such as prior exposure, other training, or additional learning experiences outside the study may have influenced participants’ outcomes. Future research should aim to control these variables by collecting baseline data on participants’ prior experiences or incorporating follow-up measures to isolate the intervention’s effects more effectively.
Future Implications
Advances in Knowledge
This study demonstrates that structured box trainer courses significantly enhance laparoscopic skills, with a measurable and positive impact on residents’ performance in real surgical settings. It validates the effectiveness of simulation-based training in bridging the gap between theory and practice. By comparing performance in both environments, the study reinforces the value of simulation as a critical component in surgical education and provides evidence supporting its integration into residency programs. The bi-center design further strengthens the generalizability of the findings.
Application for Patient Care
This study supports integrating simulation-based training to improve patient safety and surgical outcomes. By demonstrating that skills acquired through box trainer courses translate effectively to real-life operating room performance, it advocates for structured simulation as a preparatory step before independent surgical practice. Enhanced resident competence leads to fewer intraoperative errors, improved efficiency, and better patient care. The findings highlight how investing in simulation builds technical skills and directly contributes to safer surgical environments and more confident, capable surgeons.
Conclusions
The study concludes that BT may be used to effectively train surgical residents in basic laparoscopic skills and promote transferring these skills to real-life surgical practice. This study focused on the immediate effects of simulation-based training on the residents’ laparoscopic skills in patients. Since this study included residents from only two surgical specialties, others should be included to assess the generalizability of simulation-based skills transfer. Further research could be done to evaluate the effect of such training on skills retention in real-life settings. The study provides evidence for cost-effective training in middle or low-income settings.
Ethics Approval
Ethical approval was obtained by both Ziauddin University and Fazaia Ruth Pfau Medical College, Karachi. Also, approval was taken from Jinnah Sindh Medical University (JSMU/IRB/2023/741 dated 22-09-2023) as a part of the thesis.
Acknowledgments
Dr Masood Ahmed, Principal, FRPMC.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. Sheriff HM, Ghauri AU, Shalabi H, Javed IN. Laparoscopic surgery-surgical trainees’ practices. J Rwp Med Coll. 2015;19:33–35.
2. Supe A, Prabhu R, Harris I, Downing S, Tekian A. Structured training on box trainers for first year surgical residents: does it improve retention of laparoscopic skills? A randomized controlled study. J Surg Educ. 2012;69(5):624–632. doi:10.1016/j.jsurg.2012.05.002
3. Schreuder HW, CB VDB, Hazebroek EJ, Verheijen RH, Schijven MP. Laparoscopic skills training using inexpensive box trainers: which exercises to choose when constructing a validated training course. BJOG. 2011;118(13):1576–1584. doi:10.1111/j.1471-0528.2011.03146.x
4. Bellows CF, Smith AA. Laparoscopic skills training of surgical residents: a comparison of two proficiency-based independent approaches. Mini-Invasive Surgery. 2017 ;1:126–132. doi:10.20517/2574-1225.2017.12
5. Oussi N, Enochsson L, Henningsohn L, Castegren M, Georgiou E, Kjellin A. Trainee performance after laparoscopic simulator training using a Blackbox versus LapMentor. J Surg Res. 2020;250. doi:10.1016/j.jss.2019.12.039
6. Munz Y, Kumar BD, Moorthy K, Bann S, Darzi A. Laparoscopic virtual reality and box trainers: is one superior to the other? Surgical endoscopy and other interventional techniques. Surg Endoscopy. 2004;18:485–494. doi:10.1007/s00464-003-9043-7
7. Raees M, Hussain SS, Zeb L. The impact of a series of laparoscopic surgery workshops in gynecology practices-observations in a tertiary care hospital. J Med Sci. 2022;30(2):131–133.
8. Shaikh A, Khaliq T. simulation based training improves laparoscopic surgical skills in trainee surgeons. Pakistan Armed Forces Med J. 2021;doi:10.51253/pafmj.v71iSuppl-1.3709
9. Ahmed Z, Hussain A, Badil, et al. Effectiveness of simulation based learning on clinical skills competence among undergraduate nursing students. IJBR. 2025;3(5):284–287. DOI:10.70749/ijbr.v3i5.1142
10. Bajwa M, Najeeb F, Alnazzawi H, Ayub A, Bell JG, Sadiq F. A scoping review of pakistani healthcare simulation: insights for lower-middle-income countries. Cureus. 2024;16(12):e76485. doi:10.7759/cureus.76485
11. Dodani S, Songer T, Ahmed Z, Laporte RE. Building research capacity in developing countries: cost-effectiveness of an epidemiology course taught by traditional and video-teleconferencing methods in Pakistan. Telemed J E Health. 2012;18(8):621–628. doi:10.1089/tmj.2011.0262
12. Guerrero-Antolino P, Gutiérrez-Sánchez C, Millán-Scheiding M. Assessment tools for minimally invasive surgery simulation programmes: a narrative review. Ann Laparosc Endosc Surg. 2024;9. doi:10.21037/ales-23-66.
13. Cook KE, Murowchick E. Do literature review skills transfer from one course to another? Psychol. Learn. Teach. 2014;13(1):3–11. doi:10.2304/plat.2014.13.1.3
14. Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/MD.0000000000038813
15. Imaizumi K, Ichikawa N, Homma S, et al. Effect of continuous box-trainer training on laparoscopic skills of surgical residents: a prospective, observational study. in vivo. In Vivo. 2023;37(1):476–482. doi:10.21873/invivo.13102
16. Orzech N, Palter VN, Reznick RK, Aggarwal R, Grantcharov TP. A comparison of 2 ex vivo training curricula for advanced laparoscopic skills: a randomized controlled trial. Ann Surg. 2012;255(5):833–839. doi:10.1097/SLA.0b013e31824aca09
17. Palter VN, Orzech N, Reznick RK, Grantcharov TP. Validation of a Structured Training and Assessment Curriculum for Technical Skill Acquisition in Minimally Invasive Surgery: A Randomized Controlled Trial; 2013. doi:10.1097/SLA.0b013e31827051cd
18. Charokar K, Modi JN. Simulation-based structured training for developing laparoscopy skills in general surgery and obstetrics & gynecology postgraduates. J Educ Health Promot. 2021;10(1):387. doi:10.4103/jehp.jehp_48_21
19. Dhariwal AK, Prabhu RY, Dalvi AN, Supe AN. Effectiveness of box trainers in laparoscopic training. J Minim Access Surg. 2007;3(2):57–63. doi:10.4103/0972-9941.33274
20. Appleton S, Huguelet P. Laparoscopy skills simulation for the obstetrics and gynecology resident. Mededportal. 2016;12:10460. doi:10.15766/mep_2374-8265.10460
21. Khan S, Bilqis H, Arshad F, Bano N, Chaudhri R. Use of box simulators for the improvement of laparoscopic skills in the field of gynaecology. J. Soc. Obstet. Gynaecol. Pak. 2019;9(3):176–181.
22. Khan MR, Shariff AH, Nasim S, Sayyed RH, Effendi MS, Pinjani S. Effectiveness of laparoscopic skills workshop on enhancing knowledge and skills of surgical residents and its comparison with DOPS (direct observation of procedural skills) scores: prospective cohort study. Med Sci Educator. 2020;30:861–867. doi:10.1007/s40670-020-00966-5
23. Seltzer H, Swayze E, Thottathil L, et al. The impact of homemade laparoscopic box trainers on medical student surgical skills: a randomized control pilot study. Surgical Innovation. 2023;30(1):84–93. doi:10.1177/15533506221094956
24. Nicol LG, Walker KG, Cleland J, Partridge R, Moug SJ. Incentivising practice with take-home laparoscopic simulators in two UK Core Surgical Training programmes. BMJ Simul. Technol. Enhanc. Learn. 2016;2(4):112. doi:10.1136/bmjstel-2016-000117
25. Chummun K, Burke JP, O’Sullivan R, Prendiville W. The influence of a ‘take home’box trainer on laparoscopic performance for gynaecological surgeons. Gynecol Surg. 2012;9:303–308. doi:10.1007/s10397-011-0720-6
26. Hatala R, Cook DA, Zendejas B, Hamstra SJ, Brydges R. Feedback for simulation-based procedural skills training: a meta-analysis and critical narrative synthesis. Adv Health Sci Educ. 2014;19:251–272. doi:10.1007/s10459-013-9462-8
27. Parmar S, Delaney CP. The role of proximate feedback in skills training. the surgeon. Surgeon. 2011;9:S26–7. doi:10.1016/j.surge.2010.11.006
28. Eppich WJ, Hunt EA, Duval-Arnould JM, Siddall VJ, Cheng A. Structuring feedback and debriefing to achieve mastery learning goals. Acad Med. 2015;90(11):1501–1508. doi:10.1097/ACM.0000000000000934
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Enhancing Pediatric Residency Training Through Peer-Education Based Gamified Simulation
Scaglione M, Calandrino A, Puzone L, Bottino G, Conte A, Striano P, Maghnie M
Advances in Medical Education and Practice 2025, 16:1621-1626
Published Date: 3 September 2025