Back to Journals » International Journal of Women's Health » Volume 17
Traditional and Non-Traditional Risk Factors of Acute Coronary Syndrome in Young Women: Evidence from the ANCORS-YW Study
Authors Ibdah R ![]() , Al-Nusair M
, Al-Nusair M ![]() , Abuhalimeh R, Mahmoud SA, Laswi B, Rawashdeh S
, Abuhalimeh R, Mahmoud SA, Laswi B, Rawashdeh S ![]() , Hamoudeh A, Kheirallah KA
, Hamoudeh A, Kheirallah KA ![]()
Received 21 May 2024
Accepted for publication 21 December 2024
Published 24 January 2025 Volume 2025:17 Pages 139—152
DOI https://doi.org/10.2147/IJWH.S479229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Marleen van Gelder
Rasheed Ibdah,1,* Mohammed Al-Nusair,1,* Raghad Abuhalimeh,2 Saad A Mahmoud,1 Bushra Laswi,1 Sukaina Rawashdeh,1 Ayman Hamoudeh,3 Khalid A Kheirallah4
1Division of Cardiology, Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2School of Medicine, University of Jordan, Amman, Jordan; 3Department of Cardiology, Istishari Hospital, Amman, Jordan; 4Department of Public Health and Community Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
*These authors contributed equally to this work
Correspondence: Khalid A Kheirallah, Jordan University of Science and Technology, P. O.Box 3030, Irbid, 22110, Jordan, Email [email protected]
Purpose: Young women are at risk of acute coronary syndrome (ACS). They represent a unique population exposed to traditional cardiovascular risk factors and female sex-specific, non-traditional risk factors. The current study aimed to describe traditional and non-traditional risk factors of ACS in young women from the Middle East.
Patients and Methods: The present study used data from the Jordanian, nationwide, multicenter, case-control study, ANCORS-YW. Bivariate analyses and logistic regression models were used to predict independent risk factors of ACS using adjusted odds ratios (AOR) and 95% confidence intervals (CI).
Results: The study included 572 young women (≤ 50-years) with a median age of 45-years, divided into an ACS group (n=154, 26.9%) and a control group with no atherosclerotic cardiovascular disease (n=418, 73.1%). The most common presentation of ACS was non-ST-elevation ACS (n=98, 64%). The ACS group, compared to control group, had higher proportions of type-2 diabetes (41.6%vs.11.7%, p< 0.001), hypertension (53.9%vs.23.4%, p< 0.001), tobacco use (37.7%vs.24.2%, p=0.001), family history of cardiovascular disease (53.2%vs.23.4%, p< 0.001), metabolic syndrome (14.3%vs.2.4%, p< 0.001), and preterm delivery (24.7%vs.16.7%, p=0.032). ACS group had nonsignificantly greater proportions of hypertensive disorders of pregnancy (29.2%vs.22.7%, p=0.109) and gestational diabetes (15.6%vs.10.3%, p=0.081). Multivariable logistic regression analyses identified five independent predictors of ACS: type-2 diabetes (AOR, 95% CI: 3.45, 1.98─5.99), family history of cardiovascular disease (3.33, 2.15─5.17), tobacco use (2.01, 1.26─3.21), hypertension (1.72, 1.07─2.78), and metabolic syndrome (4.35, 1.72─11.03).
Conclusion: Modifiable risk factors play an important role in ACS risk among young women. Efforts should be made to improve primordial and primary prevention in this population.
Keywords: cardiovascular, female, ischemic heart disease, prevention, myocardial infarction
A Letter to the Editor has been published for this article.
Introduction
Cardiovascular disease, including acute coronary syndrome (ACS), remains the most common cause of death worldwide. The prevalence of myocardial infarction is estimated to be above three-percent in the United States, and approximately, every 40 seconds a myocardial infarction will occur.1 The incidence of ACS has been declining for the past few decades. The rates of myocardial infarction-related hospitalization dropped from 1485 per 100,000 person-years in 2002 to 1122 per 100,000 person-years in 2011.1 This trend has not been observed in young women who have been experiencing increasing incidence of ACS.2,3 In the United States, the percentage of women hospitalized for acute myocardial infarction who were young (<55-years) grew from 21% in the period 1995─1999 to 31% in the period 2010─2014 while among men, it did not significantly change (30% to 33%).2 ACS has been historically considered a “man’s disease”, it is now recognized that coronary heart disease (CHD) and ACS are important diseases in young women.4–7 Young women present a unique population with distinct risk factor profile, pathology, and outcomes.2–12 Importantly, young women who experience ACS are more often sicker with greater comorbidity burden and have higher short-term mortality rates, regardless of guidelines-based treatment, which albeit is less frequently pursued in this patient population. Improved prevention strategies for young women are highly warranted and identifying significant risk factors in this population is an important step in informing such strategies, especially as young women show different responses to traditional cardiovascular risk factors and are at risk for non-traditional factors that are either unique to or more prevalent in young women.5,6,9,10 The Middle East has a high burden of cardiovascular disease (CVD), which accounts for one-third of all deaths in the region.13 CHD and premature death due to CHD are more prevalent in the Middle East compared to most other regions of the World.14 This is likely due to the high prevalence of modifiable cardiovascular risk factors such as sedentary lifestyle, smoking, hypertension and type 2 diabetes mellitus (T2D).13 Of note, the Middle East has the highest prevalence of T2D worldwide.15 CHD burden seems to also be greater among young Middle Eastern individuals compared to other World regions.16 Young women from the Middle East have poorer ACS-related outcomes compared to young men. Young, Middle Eastern women hospitalized for ST-segment elevation myocardial infarction (STEMI) are at almost double the risk of in-hospital and one-year mortality compared to young men.17 The causes and risk factors for ACS in the Middle East are underexplored, especially among young women.
The present study describes the risk factors for ACS in young women from the Middle East, using data from the multicenter case-control study, the Atherosclerotic cardiovascular disease Novel and Classical risk factORS in Young Middle Eastern Women (ANCORS-YW) study,18 and taking into account traditional and female sex-specific, non-traditional cardiovascular risk factors as described in previous literature.5
Materials and Methods
Study Population
ANCORS-YW is a multicenter case-control study that consecutively enrolled married women aged 18–50 years-old who were diagnosed to have atherosclerotic cardiovascular disease (ASCVD), and had at least one pregnancy. Each patient was age-matched (±5 years) with two women not known to have ASCVD and who had at least one pregnancy. Enrollment was between August 2021 and October 2023 from 12 hospitals in Jordan. Cases and controls were selected randomly from the hospitals’ patient populations, including from emergency departments, outpatient clinics of different specialties and subspecialties and inpatient wards of different specialties. Anthropometric and demographic profiles, age at enrollment (current age), traditional and non-traditional risk factors, and social determinants of health (place of residence, level of education, and presence of health insurance) were reported for participants in the case and control groups. These data were collected through interviewing the participants and were supplemented by reviewing their electronic medical records. The definition of young women is not well-established in the literature. Most studies define it as younger than 45–55 years.2,8,11 The current study used the age 50 years as an arbitrary cutoff as it also approximates the median age of menopause.
ASCVD included diagnoses in one of the following conditions: ACS, which included ST-segment elevation myocardial infarction (STEMI), and non-ST-segment elevation ACS (NSTE-ACS),19 which encompasses non-ST-segment elevation myocardial infarction (NSTEMI), and unstable angina (UA); major epicardial coronary artery disease (CAD) diagnosed by coronary computed tomographic angiography; stroke; transient ischemic attack; extracranial carotid artery disease; and peripheral arterial disease. Obstructive CAD was defined as luminal narrowing ≥50% of the left main coronary artery, or ≥70% of other epicardial coronary artery.
The study received ethical oversight and Institutional Review Board (IRB) approval from Istishari Hospital IRB (July 29, 2021). It was performed in line with the principles of the Declaration of Helsinki. Each patient signed a written informed consent. The study is registered with ClinicalTrials.gov (NCT04975503).
Diagnostic Criteria
Definition of STEMI was based on the presence of cardiac ischemic chest pain, ST-segment elevation of ≥1.5 in leads V2 to V3 and/or of ≥1 mm in other contiguous chest leads or limb leads on the 12-lead electrocardiogram (EKG), and elevated cardiac biomarkers. NSTEMI was diagnosed by the presence of cardiac ischemic chest pain, ST-segment depression, inverted T wave, or normal EKG and elevated cardiac biomarkers. UA was diagnosed by the presence of ischemic cardiac pain, ST-segment depression, inverted T wave or normal EKG and no elevation of two sequential cardiac biomarkers. Stroke and transient ischemic attack were diagnosed by a neurologist based on standard clinical and imaging criteria. Extracranial carotid artery disease was diagnosed by the presence of atherosclerosis of the common or internal carotid artery evident by arterial Doppler, computed tomography, or invasive angiography. Lower limb peripheral arterial disease was diagnosed based on the presence of lower extremity ischemic pain and/or atherosclerosis evident by arterial Doppler, computed tomography, or invasive angiography.
Exclusion Criteria
For the purposes of this study, cases with diagnoses in ASCVDs other than ACS were excluded to produce two study groups, an ACS group and a control group consisting of young women without ASCVD. The control group of the current study included the same participants in the control group of ANCORS-YW.
Traditional Risk Factors
Eight traditional cardiovascular risk factors were evaluated and reported: hypertension, T2D, history of tobacco use (current or ex-smoker), family history of CVD (first-degree relative: male <55 years, female <65 years), dyslipidemia, obesity according to body mass index (BMI), physical inactivity, and metabolic syndrome. Hypertension was defined as repeated resting blood pressure measurements >140/90mm Hg,20 a prior diagnosis by a treating physician, or use of blood pressure medications. T2D was defined as the presence of classical symptoms of hyperglycemia (polyuria, polydipsia, and unexplained weight loss) and random plasma glucose ≥200 mg/dl; fasting plasma glucose ≥126mg/dl; serum level of glycated hemoglobin ≥6.5g/dl,21 a prior diagnosis of diabetes, or prescription of anti-diabetic medications by a treating physician. Dyslipidemia was defined as an elevated serum level of low-density lipoprotein cholesterol (LDL-C) >70 mg/dl in those with ASCVD or diabetes, and >116 mg/dl in those with no ASCVD or diabetes. Body mass index was calculated by the standard formula (weight [kg]/ height [m2]), and obesity was defined as BMI≥30kg/m2. Diagnosis of metabolic syndrome was confirmed by the presence of at least 3 of the following criteria: hypertension, obesity, serum level of high-density lipoprotein cholesterol (HDL-C) <50mg/dl, and serum level of triglycerides >150mg/dl.
Non-Traditional Risk Factors
Eight female-sex specific, non-traditional risk factors were assessed in the current study: preterm delivery, hypertensive disorders of pregnancy (HDP), gestational diabetes mellitus (GDM), polycystic ovarian syndrome (PCOS), premature menopause, persistent weight gain after delivery, depression, and autoimmune disease. Preterm delivery was defined as a live delivery before 37 weeks of gestation and after 20 weeks of gestation.22 HDP included diagnoses in gestational hypertension, chronic hypertension, and preeclampsia. Systolic blood pressure ≥140mmHg and/or diastolic blood pressure ≥90mmHg on two separate occasions at least four hours apart was used to define hypertension in HDP; accordingly gestational hypertension was defined as hypertension taking place after 20 weeks of gestation in a previously normotensive women; chronic hypertension was defined as hypertension diagnosed before 20 weeks of gestation; and preeclampsia was defined as gestational hypertension plus proteinuria or end-organ damage, or severe hypertension (systolic blood pressure ≥160mmHg or diastolic blood pressure ≥110mmHg).23 GDM was diagnosed based on the 2006 WHO criteria if one or more of the following criteria are met: fasting plasma glucose ≥126 mg/ dl, 2-hplasma glucose ≥200mg/dl following a 75g oral glucose load, and random plasma glucose ≥200 mg/dl in the presence of diabetes symptoms.24 PCOS was defined according to the Rotterdam diagnostic criteria25 (presence of two clinical or biochemical hyperandrogenism features, ovulatory dysfunction, or polycystic ovaries) or based on a prior diagnosis by a gynecologist. Premature menopause was defined as oligo-amenorrhea of more than 12 months associated with serial elevated gonadotropins on three occasions measured 4–6 weeks apart in women under the age of 40 years, or based on a prior diagnosis by a gynecologist. Depression was defined as prior diagnosis by a psychiatrist, or prescription of antidepressant medication.
Statistical Analysis
Continuous variables were reported as median, interquartile range (IQR), and categorical variables were reported as numbers and percentages. Mann–Whitney U-tests and Kruskal Wallis tests were used to compare continuous variables and Pearson chi-square tests were used to compare categorical variables.
Univariate binary logistic regression analysis was performed to investigate whether traditional and non-traditional risk factors were predictive of ACS. Multivariable binary logistic regression models were constructed to identify independent risk factors for ACS. Variance inflation factors (VIF) were calculated to assess for multicollinearity. Multiple models were formed to assess for potentially confounding factors using statistical methods including backward stepwise selection. All tested models yielded similar results and a model that included that included the most clinically relevant factors was reported.
All statistical tests were two-sided. A p-value of <0.05 was considered statistically significant for all tests. IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, N.Y., USA) and Stata/MP release 14.2 (STATA, College Station, TX, USA) were used for statistical analyses.
Results
A total of 627 young women were enrolled in the ANCORS-YW study, including 209 patients with ASCVD and 418 non-ASCVD controls. Of the ASCVD cases, 74% (n=154) had a diagnosis in ACS only. The current analyses included only a total of 572 young women (median age = 45-years) divided into the ACS group (n=154, 26.9%) and the control group (n=418, 73.1%). Thirty-six percent (n=56) of young women with ACS presented with STEMI while 64% (n=98) had NSTE-ACS, of which, 44.8% (n=69) had evidence of obstructive CAD and 18.8% (n=29) did not have obstructive coronary arteries.
Sociodemographic and clinical characteristics of the study groups are provided in Table 1. Young women with ACS were older than controls (46 vs 45-years, p=0.003) and had less post-secondary education (35.1% vs 55.7%, p<0.001). All ACS patients had at least one traditional risk factor while 5% of the control group lacked any traditional risk factors (p=0.005). The median number of traditional risk factors was greater in the ACS group (4 vs 2, p<0.001). The most prevalent traditional risk factors were physical inactivity (74.7%) and obesity (43.2%). History of tobacco use was more common in the ACS group (p=0.001) as were T2D, hypertension, family history of CVD, and metabolic syndrome (p<0.001 for all comparisons) (Figure 1). Dyslipidemia and lipid profile (total cholesterol, triglycerides, LDL-C, and HDL-C) were assessed and reported in around 40% of participants. Still, dyslipidemia was significantly more common in the ACS group (89 vs 70.5, p=0.001). Among smokers, the most commonly used tobacco products were cigarettes (14.7%) followed by hookah (waterpipe) (8.2%) and e-cigarettes (2.4%). Furthermore, ACS patients were more frequent current cigarette smokers and hookah smokers compared to controls (p<0.001) (Supplementary Materials, Table S1). Among current cigarette smokers, ACS patients had greater pack-years compared to the control group (p<0.001) (Supplementary Materials, Table S2). Non-traditional risk factors’ distribution by groups was not statistically significant (64.3% and 64.8%, p=0.903). Preterm delivery was more common among ACS patients (24.7% vs 16.7%, p=0.032) and ACS patients had higher, non-statistically significant, prevalence of HDP (29.2% vs 22.7%, p=0.109) and GDM (15.6% vs 10.3%, p=0.081) (Figure 2). ACS patients had more reported comorbidities with more frequent heart failure (14.3% vs 0.5%, p<0.001) and sleep apnea (3.9% vs 0.5%, p=0.002). ACS patients were more frequently using cardiovascular medications including antiplatelets, lipid lowering agents, beta-blockers, angiotensin-converting enzyme inhibitors/angiotensin-II receptor blockers, and anti-diabetic agents (p<0.001 for all comparisons).
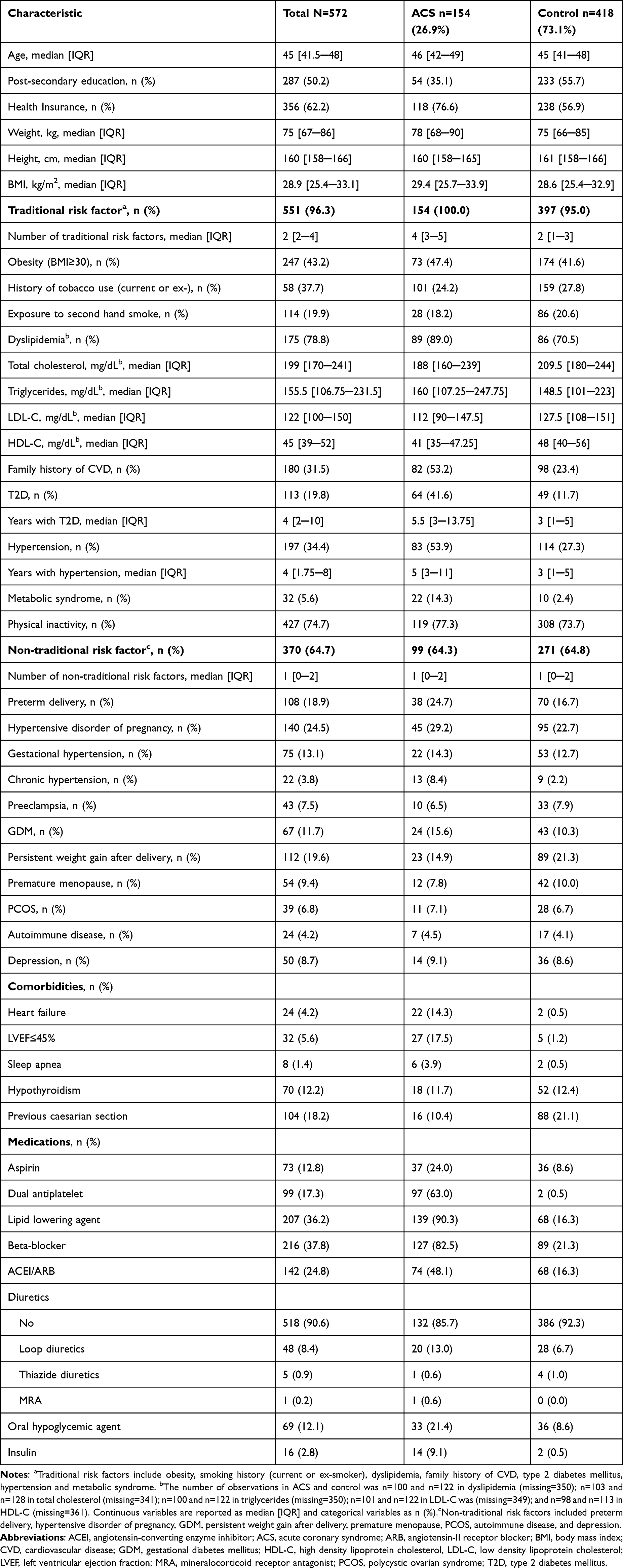 |
Table 1 Sociodemographic and Clinical Characteristics |
 |
Figure 1 Traditional cardiovascular risk factors in young women with acute coronary syndrome. Abbreviations: ACS, acute coronary syndrome; BMI, body mass index; CVD, cardiovascular disease. Note: *Difference is significant at p<0.05 level. |
 |
Figure 2 Non-traditional risk factors in young women with acute coronary syndrome. Abbreviations: ACS, acute coronary syndrome; GDM, gestational diabetes mellitus; HDP, hypertensive disorders of pregnancy; PCOS, polycystic ovarian syndrome. Note: *Difference is significant at p<0.05 level. |
Sub-analyses were performed to describe sociodemographic and clinical characteristics of young women with STEMI and NSTE-ACS (Supplementary Materials, Table S3), as well as young women with NSTE-ACS with obstructive CAD and NSTE-ACS with non-obstructive coronary arteries (Supplementary Materials, Table S4). Young women with NSTE-ACS had greater median number of traditional risk factors compared to young women with STEMI and healthy controls (4 vs 3 vs 2, p<0.001). Young women with STEMI and NSTE-ACS and the control group all had a median of one non-traditional risk factor.
Seventy percent of young women with ACS (n=106) had a history of pursuing coronary revascularization (Table 2). The most commonly performed procedure was percutaneous coronary intervention with stent placement (66.2%).
 |
Table 2 Coronary Revascularization Procedures Pursued in Young Women with Acute Coronary Syndrome |
Twenty-five percent of young women reported regular exercise, with 5.8% exercising less than three hours a week, 16.1% performing 3─5 hours of exercise weekly, and 3.5% reporting over five hours of physical exercise every week (Supplementary Materials, Table S5).
Univariate and multivariable binary logistic regression models were constructed to identify independent predictors of ACS in young women. Crude and adjusted odds ratios (AOR) and 95% confidence intervals (CI) are reported in Table 3. All variables entered into the final multivariable model are reported in Table 3 along with their respective AOR and 95% CI. Independent risk factor for ACS in young women included T2D (AOR 3.45, 95% CI 1.98─5.99), family history of CVD (AOR 3.33, 95% CI 2.15─5.17), history of tobacco use (AOR 2.01, 95% CI 1.26─3.21), hypertension (AOR 1.72, 95% CI 1.07─2.78), and metabolic syndrome (AOR 4.35, 95% CI 1.72─11.03).
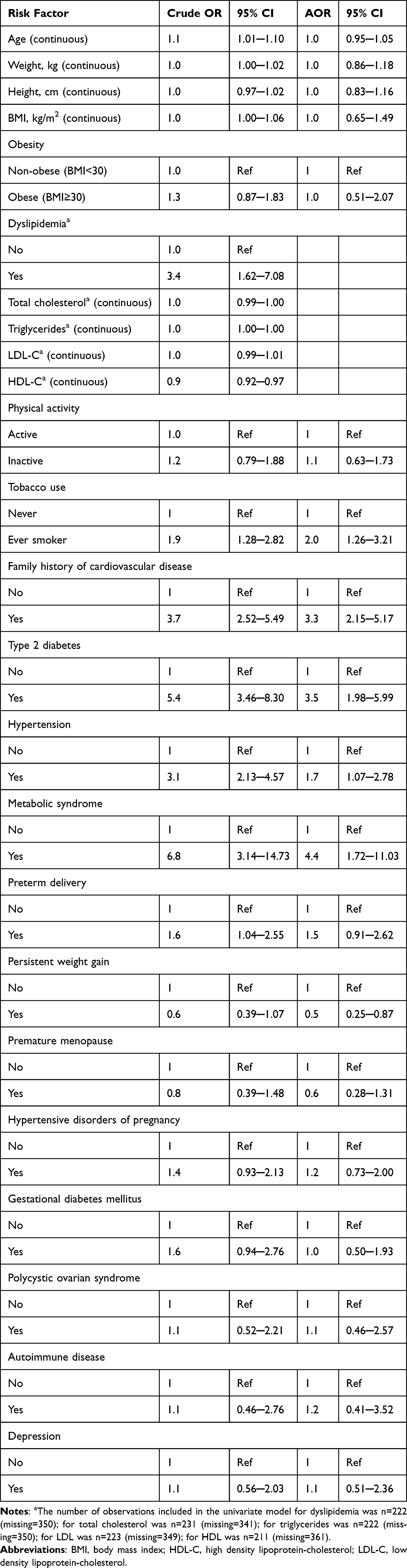 |
Table 3 Univariate and Multivariable Logistic Regression Models for Prediction of Acute Coronary Syndrome in Young Women |
Discussion
Data regarding ACS in young women is scarce especially in developing regions like the Middle East. The current study used a multicenter case-control design to assess traditional and female-sex specific, non-traditional cardiovascular risk factors for ACS in young women. The most common ACS presentation was NSTE-ACS. Traditional risk factors such as history of tobacco use, family history of CVD, T2D, hypertension, and metabolic syndrome were more common in young women with ACS whereas obesity and physical inactivity were comparable in the ACS group and control group. The non-traditional risk factor preterm delivery was more frequently reported in the ACS group. HDP and GDM were also more prevalent in the ACS group although this was not statistically significant. Multivariable logistic regression analysis identified five independent risk factors for ACS in young women: T2D, history of tobacco use, hypertension, metabolic syndrome, and family history of CVD. These finding provide valuable information that can be used to better inform primordial and primary preventive strategies and other public health measures against CHD. This is especially useful in the Middle East, where the need to reduce CVD burden is crucial and the prevalence of modifiable cardiovascular risk factors is high. This is also critical considering the need to design interventions focusing on young women, who represent a high risk and underexplored group.
Women present with NSTE-ACS more frequently than men,1 possibly due to more prevalent ACS with non-obstructive coronary arteries in female patients as well as greater burden of cardiovascular risk factors and comorbidities.6 In the ISACS-TC study, young women with ACS presented more commonly with STEMI than NSTE-ACS.8 However, the incidence of STEMI has been declining over the past decades while NSTE-ACS incidence has been rising,3,26 and it has recently been estimated that around three quarters of new ACS presentations in the United States are NSTE-ACS.19 This opposing trend may reflect a switch in the predominant pathophysiologic mechanism of ACS from plaque rupture to plaque erosion, especially with the increasing use of medical preventive strategies including lipid lowering agents.27 Moreover, plaque erosion occurs more often in young women and is more likely to present as NSTE-ACS.28 Furthermore, studies of registry data have reported a greater propensity for NSTE-ACS among Middle Eastern women.12,29 In the current study, the more common ACS presentation in young women was NSTE-ACS.
Women are at risk of traditional cardiovascular risk factors such as diabetes, hypertension, tobacco smoking, obesity and dyslipidemia.10 However, there are female-unique considerations. At the time of ACS presentation, women usually have a greater burden of risk factors and comorbidities.2 Furthermore, the relative potency of a given risk factor differs from men to women, as diabetes, smoking, and hypertension produce a greater effect in women compared to men while dyslipidemia is a more potent factor in male patients.9,10 A study from Poland reported that diabetes, hypertension, hyperlipidemia, and smoking were independent predictors of ACS in young women.7 Similarly, in a more recent Chinese case-control study of young women with and without ACS,30 diabetes, hypertension and family history of CHD were found to be independently predictive of ACS. The current study supports these findings, as T2D, hypertension, smoking history, metabolic syndrome, and family history of CVD were independently risk factors for ACS. Of note, T2D occurs in women at a younger age than men, exposing them to longer disease duration, which can increase their risk of chronic complications including CVD.5 In addition, it has been demonstrated that diabetes in young women can close the sex-related gap in cardiovascular risk, neutralizing the cardioprotection of premenopause.5
Along with traditional cardiovascular risk factors, young women are also at risk of female sex-unique factors such as adverse pregnancy outcomes, premature menopause and PCOS, as well as risk factors that are substantially more prevalent among women including autoimmune diseases and psychosocial factors such as depression.5,10 HDP are associated with future risk of CVD including hypertension and CHD, and have been added as a risk-enhancer to recent guidelines.5,31,32 A recent registry-based study from Denmark reported an increased incidence of acute myocardial infarction and stroke in the first decade following pregnancies complicated by pre-eclampsia compared to pre-eclampsia-free pregnancies.33 Several hypotheses have been proposed to explain the link between HDP and CVD. The processes causing spiral artery dysfunction in HDP may become generalized and persist beyond pregnancy resulting in systemic vascular remodeling and a picture of accelerated ASCVD. On the other hand, pregnancy has been described as a “natural stress test”, which may uncover underlying cardiovascular risk predisposing to both HDP and CHD.10 In the current study, HDP was associated with a forty percent increase in likelihood of ACS among young women in univariate regression analysis; however, this did not reach statistical significance. GDM is associated with increased risk of T2D and other cardiometabolic risk factors after pregnancy,5,10 which, in turn, can lead to higher incidence of CVD.34 Recent prospective studies from Denmark and the United Kingdom have demonstrated an elevated hazards of myocardial infarction as well as other cardiovascular events among women with history of GDM,35,36 and these findings were confirmed in a meta-analysis.37 In the present study, GDM produced a 61% increase in the odds of having ACS although this was not statistically significant. Preterm delivery is associated with increased risk of CHD and CHD-related mortality. Furthermore, earlier gestational age of preterm birth increases the associated cardiovascular risk.5 In the current study, a history of preterm delivery significantly increased the likelihood of ACS; yet, this effect become non-significant in multivariable analysis. PCOS is associated with insulin resistance and an increased risk of diabetes and cardiometabolic factors.5,10 Furthermore, PCOS has been reported to increase the likelihood of CHD although this association has been controversial, as it is difficult to separate the effects of PCOS from associated diabetes.10 Additionally, studies have suggested ethnic variation in the phenotypic expression of the disease. PCOS-related insulin resistance is most common in East Asian patients while Middle Eastern patients are more likely to present with androgenic signs.38 Furthermore, cardiometabolic factors have been reported to be comparable between Middle Eastern women with and without PCOS.39 Moreover, the Middle Eastern region has the highest prevalence of diabetes worldwide;15 and it has been reported that among women without PCOS, insulin resistance is higher in Middle Eastern women than in Caucasian women from the United Kingdom; however, it is similar among women with PCOS of the two ethnic groups;40 thus PCOS may not effectively increase prevalence of diabetes among Middle Eastern women as much as women from other ethnic groups. In the current study, PCOS was not significantly associated with ACS in young Middle Eastern women. Furthermore, T2D and metabolic syndrome were comparable between young women with and without PCOS (20.5% and 19.7%, p=0.902; 5.1% and 5.6%, p=0.896; respectively) (unreported data). Premature menopause is associated with increased risk of CVD, which has been suggested to be due to early withdrawal of the protective effects of estrogen.5,10 However, in the current study, premature menopause was less common among young women with ACS compared to the control group although this was not statistically significant. The mean time from menopause to incidence of CVD in women has been reported to be around 13.5 years;41 thus, the cutoff of 50 years used to define young women in the present study may have underestimated history of premature menopause among women with ACS. Persistent weight gain after pregnancy is associated with increased cardiometabolic risk.42 A study of Saudi women from the RAHMA cohort reported an increase in cardiometabolic factors, including metabolic syndrome among women with greater postpartum weight retention.43 In a Danish cohort study, Kirkegaard et al 44 demonstrated that risk of CVD is not generally evident in women with persistent weight gain after pregnancy and is dependent on pre-pregnancy BMI. They reported that women with pre-pregnancy normal/underweight BMI and persistent weight gain were at increased risk of CVD while those who were overweight/obese pre-pregnancy did not show significant increase in CVD risk. In the current study, persistent weight gain was associated with decreased likelihood of ACS. However, among the current study population, young women with a history of persistent weight gain were more commonly obese (61.6% vs 38.7%, p<0.001) and had greater prevalence of metabolic syndrome (10.7% vs 4.3%, p=0.009) compared to those without postpartum persistent weight gain (unreported data).
Autoimmune diseases such as systemic lupus erythematosus and rheumatoid arthritis are important risk factors for CVD in women, as their prevalence is considerably higher among women compared to men.5,10 Autoimmune disease can cause accelerated atherosclerosis as well as coronary microvascular dysfunction leading to premature CHD. Furthermore, CVD has been reported to be the most common cause of death in systemic lupus erythematosus.5 However, autoimmune diseases are less common than other traditional and non-traditional cardiovascular risk factors.30 In the current study, autoimmune disease had a relatively low prevalence overall (4.2%), and was similar in the ACS and control groups. Psychosocial factors including depression are also more common in women than men.3 Depression has been associated with CHD as well as poor prognosis following ACS, especially among young women.3,5,10 The relationship between depression and CHD may be a result of greater prevalence of depressive symptoms among CHD patients or due to activation of adverse biological pathways in depression patients such as increased sympathetic tone, inflammation, and endothelial and platelet dysfunction.45 On the other hand, depression is associated with harmful behavior including tobacco smoking, poor diet, and physical inactivity, which increase cardiovascular risk. In the present study, depression did not increase the likelihood of ACS among young women. However, depression was associated with greater prevalence of smoking history (42% vs 26.4%, p=0.019) compared to young women without history of depression (unreported data).
Strengths and Limitations
The current study provides a comprehensive description of the risk factors for ACS in young women from the Middle East using a multicenter case-control design. Participants were recruited from 12 hospitals in Jordan, which included both private-sector and public-sector centers. This provided a study population which was more representative of Jordanian young women. The risk factors investigated in the study included traditional cardiovascular risk factors as well as non-traditional, female sex-specific risk factors. However, the study is not without limitations. The case-control design exposes the study to the limitations of observational studies. The current study used secondary data obtained from the ANCORS-YW study. The specific indications for the medications used by the participants were not reported in the ANCORS-YW study and specific serum levels were not targeted to initiate certain medications. Future studies should consider the associations between risk factor management and ACS, specifically how risk factors are managed, what interventions/medications are used for risk factor control, the number interventions required to achieve risk factor control and whether control is achieved or not. The current study assessed the risk of ACS in young women while considering multiple non-traditional risk factors. Still, other factors that may play a role in cardiovascular risk among this population may have not been assessed such as anemia. Future studies should consider assessing such factors. The ANCORS-YW study identified participants with premature menopause (<40-years). However, it did not record menopause in those between the age 40–50. Given the cutoff age of 50-years in our study population, premature menopause likely had a considerably greater impact on ACS compared to menopause occurring at age 40 to 50-years. Still, future studies assessing cardiovascular risk in young women should consider menopause at all ages. Furthermore, although extensive risk factors were included in the analysis, it is possible that some potentially confounding factors may have been missed. Still, traditional cardiovascular risk factors emerged as independent predictors of ACS in young women.
Conclusion
Young women are at risk for ACS. Modifiable risk factors including T2D, smoking, and hypertension play an important role in ACS risk, and primordial and primary preventive strategies for CVD should be encouraged in young women. Family history of premature CVD is also a strong independent predictor of ACS in young women, highlighting the importance of inherited CVD risk factors in this patient population.
Data Sharing Statement
The data used in this study is available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funds, grants, or other support was received.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Martin SS, Aday AW, Almarzooq ZI, et al. 2024 heart disease and stroke statistics: a report of us and global data from the American heart association. Circulation. 2024;149:e000–e000. doi:10.1161/CIR.0000000000001209
2. Arora S, Stouffer GA, Kucharska-Newton AM, et al. Twenty year trends and sex differences in young adults hospitalized with acute myocardial infarction. Circulation. 2019;139(8):1047–1056. doi:10.1161/CIRCULATIONAHA.118.037137
3. Chandrasekhar J, Gill A, Mehran R. Acute myocardial infarction in young women: current perspectives. Int J Womens Health. 2018;10:267–284. doi:10.2147/IJWH.S107371
4. Minissian MB, Mehta PK, Hayes SN, et al. Ischemic heart disease in young women: JACC review topic of the week. J Am Coll Cardiol. 2022;80(10):1014–1022. doi:10.1016/j.jacc.2022.01.057
5. Cho L, Davis M, Elgendy I, et al. Summary of updated recommendations for primary prevention of cardiovascular disease in women: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(20):2602–2618. doi:10.1016/j.jacc.2020.03.060
6. Bucholz EM, Strait KM, Dreyer RP, et al. Editor’s choice-sex differences in young patients with acute myocardial infarction: a VIRGO study analysis. Eur Hear Journal Acute Cardiovasc Care. 2017;6(7):610–622. doi:10.1177/2048872616661847
7. Bęćkowski M, Gierlotka M, Gąsior M, et al. Risk factors predisposing to acute coronary syndromes in young women ≤45 years of age. Int J Cardiol. 2018;264:165–169. doi:10.1016/j.ijcard.2018.03.135
8. Ricci B, Cenko E, Vasiljevic Z, et al. Acute coronary syndrome: the risk to young women. J Am Heart Assoc. 2017;6(12):e007519. doi:10.1161/JAHA.117.007519
9. Lu Y, Li SX, Liu Y, et al. Sex-specific risk factors associated with first acute myocardial infarction in young adults. JAMA Netw Open. 2022;5(5):e229953. doi:10.1001/jamanetworkopen.2022.9953
10. Young L, Cho L. Unique cardiovascular risk factors in women. Heart. 2019;105(21):1656–1660. doi:10.1136/heartjnl-2018-314268
11. Mehilli J, Presbitero P. Coronary artery disease and acute coronary syndrome in women. Heart. 2020;106(7):487LP–492. doi:10.1136/heartjnl-2019-315555
12. Cader FA, Banerjee S, Gulati M. Sex differences in acute coronary syndromes: a global perspective. J Cardiovasc Dev Dis. 2022;9(8). doi:10.3390/jcdd9080239
13. WHO Regional Office for the Eastern Mediterranean. Health and well-being profile of the Eastern Mediterranean Region: an overview of the health situation in the region and its countries in 2019. 2020. Available from: https://applications.emro.who.int/docs/9789290223399-eng.pdf?ua=1&ua=1.
14. Aminorroaya A, Saeedi Moghaddam S, Tavolinejad H, et al. Burden of ischemic heart disease and its attributable risk factors in North Africa and the Middle East, 1990 to 2019: results from the GBD study 2019. J Am Heart Assoc. 2023;13(2):e030165. doi:10.1161/JAHA.123.030165
15. International Diabetes Federation. IDF diabetes atlas, 10th Edn.; 2021. Available from: https://www.diabetesatlas.org.
16. Traina MI, Almahmeed W, Edris A, Murat Tuzcu E. Coronary heart disease in the Middle East and North Africa: current status and future goals. Curr Atheroscler Rep. 2017;19(5):24. doi:10.1007/s11883-017-0659-9
17. Shehab A, Bhagavathula AS, Alhabib KF, et al. Age‐related sex differences in clinical presentation, management, and outcomes in ST‐segment–elevation myocardial infarction: pooled analysis of 15 532 patients from 7 Arabian Gulf registries. J Am Heart Assoc. 2020;9(4):e013880. doi:10.1161/JAHA.119.013880
18. Hammoudeh AJ, Jallad M, Khader Y, et al. Atherosclerotic cardiovascular disease novel and traditional risk factors in middle eastern young women. the ANCORS-YW study. Glob Heart. 2024;19(1):59. doi:10.5334/gh.1341
19. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes. Circulation. 2014;130(25):e344–e426. doi:10.1161/CIR.0000000000000134
20. Unger T, Borghi C, Charchar F, et al. 2020 international society of hypertension global hypertension practice guidelines. Hypertension. 2020;75(6):1334–1357. doi:10.1161/HYPERTENSIONAHA.120.15026
21. ElSayed NA, Aleppo G, Aroda VR, et al. 2. classification and diagnosis of diabetes: standards of care in diabetes—2023. Diabetes Care. 2022;46(Supplement_1):S19–S40. doi:10.2337/dc23-S002
22. Simhan HN. Practice bulletin no. 171: management of preterm labor. Obstet Gynecol. 2016;128(4):e155––e164.
23. The American College of Obstetricians and Gynecologists, Gestational hypertension and preeclampsia: ACOG practice bulletin, number 222. Obstet Gynecol. 2020,June;135(6):e237–e260 doi:10.1097/AOG.0000000000003891.
24. López Stewart G. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy: a world health organization guideline. Diabet Res Clin Pract. 2014;103(3):341–363. doi:10.1016/j.diabres.2013.10.012
25. The Rotterdam ESHRE/ASRM‐sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19(1):41–47. doi:10.1093/humrep/deh098
26. Hedayati T, Yadav N, Khanagavi J. Non–ST-segment acute coronary syndromes. Cardiol Clin. 2018;36(1):37–52. doi:10.1016/j.ccl.2017.08.003
27. Fahed AC, Jang IK. Plaque erosion and acute coronary syndromes: phenotype, molecular characteristics and future directions. Nat Rev Cardiol. 2021;18(10):724–734. doi:10.1038/s41569-021-00542-3
28. Varghese T, Wenger NK. Non-ST elevation acute coronary syndrome in women and the elderly: recent updates and stones still left unturned. F1000Research. 2018;7(1865):1865. doi:10.12688/f1000research.16492.1
29. Reda A, Ashraf M, Soliman M, et al. The pattern of risk-factor profile in Egyptian patients with acute coronary syndrome: Phase II of the Egyptian cross-sectional cardiorisk project. Cardiovasc J Afr. 2019;30(2):87–94. doi:10.5830/CVJA-2018-074
30. Liu R, Xu F, Zhou Y, Liu T. The characteristics of risk factors in Chinese young women with acute coronary syndrome. BMC Cardiovasc Disord. 2020;20(1):290. doi:10.1186/s12872-020-01577-z
31. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73(24):e285–e350. doi:10.1016/j.jacc.2018.11.003
32. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the American College of Cardiology/American Heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;74(10):1376–1414. doi:10.1016/j.jacc.2019.03.009
33. Hallum S, Basit S, Kamper-Jørgensen M, Sehested TSG, Boyd HA. Risk and trajectory of premature ischaemic cardiovascular disease in women with a history of pre-eclampsia: a nationwide register-based study. Eur J Prev Cardiol. 2023;30(6):506–516. doi:10.1093/eurjpc/zwad003
34. Sun J, Kim GR, Lee SJ, Kim HC. Gestational diabetes mellitus and the role of intercurrent type 2 diabetes on long-term risk of cardiovascular events. Sci Rep. 2021;11(1):21140. doi:10.1038/s41598-021-99993-4
35. Yu Y, Soohoo M, Sørensen HT, Li J, Arah OA. Gestational diabetes mellitus and the risks of overall and type-specific cardiovascular diseases: a population- and sibling-matched cohort study. Diabetes Care. 2021;45(1):151–159. doi:10.2337/dc21-1018
36. Lee SM, Shivakumar M, Park JW, et al. Long-term cardiovascular outcomes of gestational diabetes mellitus: a prospective UK Biobank study. Cardiovasc Diabetol. 2022;21(1):221. doi:10.1186/s12933-022-01663-w
37. Xie W, Wang Y, Xiao S, Qiu L, Yu Y, Zhang Z. Association of gestational diabetes mellitus with overall and type specific cardiovascular and cerebrovascular diseases: systematic review and meta-analysis. BMJ. 2022;378:e070244. doi:10.1136/bmj-2022-070244
38. Zhao Y, Qiao J. Ethnic differences in the phenotypic expression of polycystic ovary syndrome. Steroids. 2013;78(8):755–760. doi:10.1016/j.steroids.2013.04.006
39. Farhadi-Azar M, Behboudi-Gandevani S, Rahmati M, et al. The prevalence of polycystic ovary syndrome, its phenotypes and cardio-metabolic features in a community sample of Iranian population: Tehran Lipid and Glucose Study. Front Endocrinol. 2022;13:825528. doi:10.3389/fendo.2022.825528
40. Butler AE, Abouseif A, Dargham SR, Sathyapalan T, Atkin SL. Metabolic comparison of polycystic ovarian syndrome and control women in Middle Eastern and UK Caucasian populations. Sci Rep. 2020;10(1):18895. doi:10.1038/s41598-020-75109-2
41. Zhu D, Chung HF, Dobson AJ, et al. Age at natural menopause and risk of incident cardiovascular disease: a pooled analysis of individual patient data. Lancet Public Heal. 2019;4(11):e553–e564. doi:10.1016/S2468-2667(19)30155-0
42. Kew S, Ye C, Hanley AJ, et al. Cardiometabolic implications of postpartum weight changes in the first year after delivery. Diabetes Care. 2014;37(7):1998–2006. doi:10.2337/dc14-0087
43. Wahabi HA, Fayed AA, Tharkar S, Esmaeil SA, Bakhsh H. Postpartum weight retention and cardiometabolic risk among Saudi Women: a follow-up study of RAHMA Subcohort. Biomed Res Int. 2019;2019:2957429. doi:10.1155/2019/2957429
44. Kirkegaard H, Bliddal M, Støvring H, et al. Maternal weight change from prepregnancy to 18 months postpartum and subsequent risk of hypertension and cardiovascular disease in Danish women: a cohort study. PLOS Med. 2021;18(4):e1003486. doi:10.1371/journal.pmed.1003486
45. Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. 2017;14(3):145–155. doi:10.1038/nrcardio.2016.181
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cardiovascular Prognosis of Subclinical Chronic Obstructive Pulmonary Disease in Patients with Suspected or Confirmed Coronary Artery Disease
Ferreira EJP, Cardoso LVSC, Matos CJO, Mota IL, Lira JMC, Lopes MEG, Santos GV, Almeida MLD, Aguiar-Oliveira MH, Sousa ACS, Melo EV, Oliveira JLM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1899-1908
Published Date: 29 August 2023
Identifying Risk Factors for Cardiovascular Events Among Active-Duty Service Members and Veterans Prescribed Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
Forbes WL, Petway J, Gressler LE, Thorfinnson H, Costantino RC, Atkinson TJ
Journal of Pain Research 2024, 17:1133-1144
Published Date: 15 March 2024
Correlations Between Acute Coronary Syndrome and Novel Inflammatory Markers (Systemic Immune-Inflammation Index, Systemic Inflammation Response Index, and Aggregate Index of Systemic Inflammation) in Patients with and without Diabetes or Prediabetes
Tuzimek A, Dziedzic EA, Beck J, Kochman W
Journal of Inflammation Research 2024, 17:2623-2632
Published Date: 29 April 2024
Generation of Risk Score for Serious Non-Steroidal Anti-Inflammatory Drug (NSAID) Induced Cardiovascular Events (NAÏVE) Among Active-Duty Service Members and Veterans
Atkinson TJ, Petway J, Forbes WL, Thorfinnson H, Costantino RC, Gressler LE
Journal of Pain Research 2025, 18:1081-1094
Published Date: 6 March 2025
Development and Internal Validation of a Prediction Model for Major Cardiovascular and Respiratory Events in Chronic Obstructive Pulmonary Disease: Nationwide Primary Care Electronic Medical Records Cohort Study
Gale CP, Bhutani M, Chan JSK, Townend J, Patel MS, Sadatsafavi M, Henley W, Ariti C, Carter V, Couper A, Hubbard R, Kocks JWH, Pullen R, Skinner D, Price D
Pragmatic and Observational Research 2026, 17:551291
Published Date: 10 March 2026