Back to Journals » Clinical Epidemiology » Volume 18
Timing of Core Sepsis Bundle Elements Initiation in Critically Ill Patients: A Multicenter Target Trial Emulation Study
Authors Li M ![]() , Zhang J, Huang H
, Zhang J, Huang H ![]() , Li J
, Li J ![]() , Zhang B, Zhao S, Peng Z, Han S, Guan J, Yang J, Wang G, Chang Y, Chang P, Yu Z, Zhong T, Liu Z
, Zhang B, Zhao S, Peng Z, Han S, Guan J, Yang J, Wang G, Chang Y, Chang P, Yu Z, Zhong T, Liu Z ![]()
Received 12 December 2025
Accepted for publication 15 January 2026
Published 23 January 2026 Volume 2026:18 588212
DOI https://doi.org/10.2147/CLEP.S588212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Thomas Ahern
Mingxia Li,1,* Jiaqi Zhang,2,* Haozhao Huang,1,* Jiamin Li,1,* Buyao Zhang,3 Shuangping Zhao,3 Zishan Peng,1 Shuzhe Han,4 Jianbin Guan,1 Jingjing Yang,1 Guizhong Wang,1 Yuan Chang,5 Ping Chang,1 Zhaoxian Yu,6 Tao Zhong,1 Zhanguo Liu1
1Department of Critical Care Medicine, Zhujiang Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Internal Emergency Medicine, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 3Department of Critical Care Medicine, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 4Department of Nutrition and Obstetrics and Gynecology, 967th Hospital of the Joint Logistics Support Force of the Chinese People’s Liberation Army, Dalian, Liaoning, People’s Republic of China; 5Department of Gastrointestinal Electrophysiology, College of Medicine, Chosun University, Gwangju, Republic of Korea; 6State Key Laboratory of Respiratory Disease, Institute of Tuberculosis, Guangzhou Medical University and Guangzhou Chest Hospital Affiliated to Guangdong Pharmaceutical University, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhanguo Liu, Department of Critical Care Medicine, Zhujiang Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China, Email [email protected] Ping Chang, Department of Critical Care Medicine, Zhujiang Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Purpose: One-hour sepsis bundle was developed in 2018. However, the optimal timing for antibiotic, fluid resuscitation, and vasopressor initiation in intensive care units (ICUs) remains debated. High-quality randomized evidence is limited, particularly for ICU patients. Therefore, we emulated three target trials using observational data.
Patients and Methods: We conducted a retrospective, multicenter cohort study using data from the Medical Information Mart for Intensive Care-IV database (primary dataset), and two ICU cohorts from China (Zhujiang and Xiangya hospitals). Within a target trial emulation framework with inverse probability of treatment weighting, we constructed three two-arm trials comparing initiation of (1) antibiotics, (2) fluid resuscitation, and (3) vasopressors within 0– 1 hour versus 1– 3 hours after a prespecified time zero.
Results: In the target trial emulations, antibiotic initiation within 1 hour was associated with lower 28-day mortality (HR 0.65; 95% CI 0.54– 0.79) and earlier ICU discharge (competing-risk analysis; SHR 1.20; 95% CI 1.12– 1.27) compared with initiation at 1– 3 hours. For fluid resuscitation, initiating within 1 hour and delivering ≥ 30 mL/kg crystalloid within 3 hours resulted in lower mortality (HR 0.72; 95% CI 0.53– 0.97) and earlier discharge (SHR 1.17; 95% CI 1.02– 1.33). However, vasopressor initiation within 1 hour showed no survival benefit (HR 1.07; 95% CI 0.89– 1.29) or reduction in time to ICU discharge (SHR 1.02; 95% CI 0.95– 1.08). These findings remained consistent across sensitivity and subgroup analyses, including comparisons using a 1– 6 hour window.
Conclusion: In ICUs, early administration of antibiotics and initiation of fluid resuscitation within 1 hour were associated with improved survival and earlier ICU discharge, whereas early vasopressor use was not. These findings might support a bedside emphasis on timely antibiotics and fluids during early resuscitation and provide evidence for refining time targets in future sepsis guidelines.
Keywords: sepsis, septic shock, antibiotic, fluid resuscitation, vasopressor
Introduction
In 2017, sepsis accounted for approximately 20% of all deaths worldwide, and hospitalization costs for sepsis increased annually from 2012 to 2018, representing the substantial health and economic burden. Intensive care units (ICUs), as the primary setting for hospital-acquired sepsis, has a mortality rate of 41.9%.1–3 In 2018, the Surviving Sepsis Campaign (SSC) updated the 3-hour bundle to the 1-hour bundle.4 Regarding the core interventions—antibiotics, fluid resuscitation, and vasopressors—the 2021 update of the SSC sepsis guidelines strongly recommended administering antibiotics within 1 h, weakly recommended initiating resuscitation immediately and completing 30 mL/kg of crystalloids within 3 h, and did not provide a clear recommendation for the timing of vasopressor.5 However, evidence from randomized controlled trials (RCTs) regarding early or delayed bundle implementation remains lacking. Previous retrospective studies have examined the overall impact of the sepsis bundle, but a prospective cohort study showed no significant difference in survival between complete and incomplete 1-hour bundles in emergency departments (EDs).6–8 In prior studies, heterogeneity in the definition of “time zero” has likely contributed to inconsistent estimates of the association between treatment delays and outcomes, underscoring the importance of prespecifying time zero within a target trial framework.9,10 Therefore, we specifically investigated the timing of the three core bundle elements by conducting separate studies on their initiation.
Biologically, earlier antibiotics may improve outcomes by accelerating infection control, and timely fluid resuscitation may restore effective circulating volume; in contrast, earlier vasopressor initiation may not confer uniform benefit if preload correction is incomplete or if microcirculatory responses differ across patients. For antibiotic administration, a preplanned analysis of an RCT showed that in septic shock patients receiving quantitative resuscitation, delaying antibiotic administration by one hour did not increase death risk.11 A retrospective study found that administering antibiotics more quickly within 3 hours was associated with a reduced risk of in-hospital mortality, with a median time to antibiotics of 0.95 hours (interquartile range, 0.35–1.95).6 Conversely, a before-and-after cohort study found no difference in 30-day mortality between giving antibiotics within 1 hour and within 3 hours.12 For early resuscitation in sepsis with hypoperfusion, researchers have extensively explored the sequential and simultaneous approaches of crystalloid infusion and vasopressor administration. Despite its central role in early resuscitation, the optimal timing of vasopressor initiation remains uncertain, with competing hypotheses regarding potential benefits (earlier restoration of perfusion pressure) versus risks or limited efficacy in the absence of adequate volume resuscitation.13,14 Fluid overload may result in organ dysfunction, such as renal and respiratory impairment. However, several RCTs have demonstrated no difference in mortality and adverse event risks between early liberal or standard and restrictive fluid strategies (primarily vasopressors) in septic patients.15,16 A retrospective study have indicated that administering higher intravenous fluid volumes within the first 3 hours was associated with reduced in-hospital mortality in sepsis.17 Nevertheless, more real-world evidence is required to clarify the potential effects of different timing, especially the initiation of fluid resuscitation or vasopressors within 1 hour.
Most previous sepsis bundle studies have been observational and primarily focused on antibiotic administration in emergency department patients.18,19 Compared with emergency department populations, ICU patients with sepsis are typically more severely ill, have a different case mix, and more often receive prior treatments, which may complicate both the feasibility of randomized trials and the evaluation of optimal timing for bundle elements in routine ICU practice.20 For patients in ICUs, delaying fluid resuscitation or vasopressor therapy may be considered unethical, and stringent inclusion and exclusion criteria may further limit the feasibility of RCTs. Thus, within the causal inference framework of target trial emulation by Hernán and Robins, propensity score–based stabilized inverse probability of treatment weighting (IPTW) offers an alternative approach to estimating the effects of bundle timing.21 Target trial emulation applies a causal inference framework to observational data to emulate key design features of a hypothetical randomized trial, thereby helping to reduce confounding and indication bias when RCTs are infeasible.22 Accordingly, we sought to provide element-specific evidence to inform ongoing debates about the prioritization and time targets of the 1-hour sepsis bundle recommendations, particularly in ICU populations.4,23 In this study, we conducted a multinational, retrospective, multicenter cohort study using data from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database in the United States and from the cohorts of Zhujiang Hospital and Xiangya Hospital in China.24 For critically ill sepsis patients, we emulated the following three target trials: the timing of antibiotic administration, the initiation of fluid resuscitation, and the timing of vasopressor therapy to evaluate the optimal timing for core sepsis bundle elements.
Materials and Methods
Study Design and Oversight
We assembled data from three cohorts: the MIMIC-IV database (ICU admissions from 2008 to 2019), Zhujiang (ZJ) Hospital (2023–2025) in Guangzhou, China, and Xiangya (XY) Hospital (2018–2025) in Changsha, China.24 This retrospective observational cohort study was approved by the institutional review boards of Zhujiang Hospital of Southern Medical University, and Xiangya Hospital of Central South University. One investigator (C.Y.) completed the required training and was granted access to download the MIMIC-IV data. All datasets were fully deidentified before analysis, and the informed consent was exempted. To minimize confounding and indication bias inherent in observational research, we emulated three target trials.21,22 We restricted the cohort to patients with the first diagnosis of sepsis in the ICU and compared initiation timing for three sepsis bundle elements—administration of broad-spectrum antibiotics, fluid resuscitation, and vasopressor—initiated within 1-hour (0–1 h) versus 3-hour window (1–3 h) after time zero. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.25 Details of the emulated target trials were provided in Table S1.
Bundle Elements and Time Zero
We restricted analyses to the first episode of sepsis in the ICU. In accordance with the 2016 Sepsis-3 consensus, sepsis was defined as suspected infection and an increase in Sequential Organ Failure Assessment (SOFA) score of at least 2 points from baseline.26 Within this framework, we defined a trial-specific time zero for each bundle element. For the antibiotic timing trial, the time of suspected infection was defined as the earlier of the first antibiotic order or the first microbiological sampling; if the SOFA score increased by ≥2 points within 24 hours of this time, the event was considered to meet the Sepsis-3 definition and this time was taken as time zero. For the fluid resuscitation and vasopressor timing trials, we additionally required haemodynamic instability within 24 hours, defined as the first occurrence of systolic blood pressure <90 mm Hg, mean arterial pressure <65 mm Hg, or blood lactate concentration ≥4 mmol/L; this first episode of hemodynamic instability served as the common time zero for both trials. Therefore, the three target trial emulations used trial-specific time zero definitions, and baseline characteristics were defined relative to each trial’s time zero and may differ across trials. Each bundle element was evaluated within its own emulated target trial using a clinically appropriate definition of time zero; therefore, effect estimates across trials should not be interpreted as directly comparable.
Eligibility Criteria
We included adults admitted to the ICU who met Sepsis 3.0 criteria. We excluded patients who were not on the first ICU admission, pregnant women, not the first sepsis episode, those who died or were discharged within 24 hours after sepsis diagnosis, and those with missing timing variables that precluded of time zero. Patients who died or were discharged within 24 hours were excluded to avoid immortal time bias and to ensure all patients had the opportunity to receive either timing strategy; however, this limits generalizability to patients with extremely early death or rapid clinical improvement. To adhere to the real-world trials for the bundle, we then applied trial-specific exclusions. For the antibiotic timing trial, we excluded patients who had received any antibiotics before time zero and those who did not receive antibiotics after time zero. For the fluid resuscitation trial, we excluded patients who had received more than 3000 mL of crystalloids in the 24 hours before time zero, as well as those who did not receive crystalloids after time zero or who received a cumulative volume of <30 mL per kilogram within 3 hours.15 For the vasopressor timing trial, we excluded patients who had received vasopressors before time zero and those who never received vasopressors. Detailed data extraction flow was shown in Figure S1.
Treatment Strategies
We compared two timing strategies for each bundle element. For antibiotics, we compared administration of the first dose within 0–1 h after time zero with first administration between 1–3 h. For fluid resuscitation, we compared initiation of crystalloid infusion within 0–1 h versus 1–3 h after time zero, requiring a cumulative volume of ≥30 mL/kg to be completed within 3 hours of initiation. For vasopressors, we compared initiation within 0–1 h versus 1–3 h after time zero of any of the following agents: epinephrine, norepinephrine, phenylephrine, vasopressin, dopamine, or dobutamine.
Follow-Up and Outcomes
The primary outcome was 28-day all-cause mortality; patients who were alive on day 28 were censored at that time. Secondary outcomes included time to ICU discharge (analyzed in a competing-risks framework with ICU death as the competing event), and organ support–related outcomes. For organ support, we assessed the days with invasive mechanical ventilation and days with continuous renal replacement therapy (CRRT) during the ICU stay. Patients were followed from time zero until death, loss to follow-up, or hospital discharge.
Statistical Analysis
Overview
Based on the target trial framework proposed by Hernán and Robins, we emulated three two-arm randomized trials (target trial emulations) for antibiotic administration, fluid resuscitation, and vasopressor use.22 For each emulated trial, we compared initiation of the element within 0–1 h after time zero (1-hour strategy) versus 1–3 h (3-hour strategy) (Figure 1a). Patients who initiated treatment between 1 and 6 hours after time zero (6-hour strategy) were included in sensitivity analyses. As shown in Figure 1b, to mitigate indication bias (the tendency to treat more severely ill patients earlier), we used propensity score–based stabilized inverse probability of treatment weighting (IPTW) to construct a pseudo-population with balanced baseline characteristics. For each trial, we fitted a multivariable logistic regression model with receipt of the treatment within 1 hour as the dependent variable. Covariates were measured before time zero and included demographic characteristics (age, sex), comorbidities (hypertension, diabetes, chronic heart failure, chronic kidney disease, and cirrhosis), presumed primary site of infection (pulmonary, intra-abdominal, urinary tract, or bloodstream), and 24-hour windows of physiological and laboratory measurements before time zero. The presumed primary site of infection was derived from diagnosis information documented during the hospitalization (admission/discharge diagnosis records) and categorized as pulmonary, intra-abdominal, urinary tract, or bloodstream infection. As this diagnosis-derived variable lacks a reliable timestamp, it may not strictly reflect information available at the trial-specific time zero. The presumed primary site of infection was treated as a non–mutually exclusive variable; therefore, categories could overlap and the summed proportions may exceed 100%. Laboratory variables were summarized using the worst values within the 24 hours before time zero (maximum values for lactate, white blood cell count, neutrophil percentage, lymphocyte percentage, creatinine, blood urea nitrogen, international normalized ratio, aspartate aminotransferase/alanine aminotransferase, electrolytes, and blood glucose; and minimum values, where applicable, for platelet count, hemoglobin, and albumin). Physiological variables were also summarized using the worst values within the window (minimum values for systolic blood pressure, diastolic blood pressure, mean arterial pressure, and oxygen saturation; and maximum values for heart rate, respiratory rate, and temperature). Arterial blood gas variables were summarized similarly (minimum values for arterial oxygen partial pressure and pH, and maximum values for arterial carbon dioxide partial pressure). We also adjusted for prior treatment exposure, including any vasopressor use in the 6 hours before time zero. Stabilized weights were calculated for each patient and truncated at the extremes to limit the influence of outliers. Covariate balance before and after weighting was assessed using standardized mean differences (SMDs), with an absolute SMD <0.10 taken as evidence of acceptable balance. In the weighted cohorts, we used weighted Kaplan–Meier methods to estimate 28-day survival curves for each strategy and weighted Cox proportional-hazards models to estimate hazard ratios (HRs) for 28-day all-cause mortality. For time to ICU discharge, a competing-risk outcome with ICU death as the competing event, we used weighted Fine–Gray subdistribution hazard models to estimate subdistribution hazard ratios (SHRs). The proportional hazards assumption was assessed, and no meaningful violations were observed. Confidence intervals for HRs and SHRs were obtained using nonparametric bootstrap resampling. Continuous variables are reported as median (interquartile range [IQR], 25th–75th percentile), and categorical as number (percentage). All tests were two-sided, and P < 0.05 was considered statistically significant. Data extraction was performed using PostgreSQL, and statistical analyses were conducted with R and Python.
 |
Figure 1 Target Trial Emulation Flow. Target Trial Emulation Flow. (a) shows the design of the emulated trials. Time zero was defined as the onset of suspected infection (antibiotic trial) or the first episode of hemodynamic instability (fluid resuscitation and vasopressor trials). Initiation of each bundle element within 0–1 hour after time zero defined the 1-hour strategy, and initiation between 1–3 hours defined the 3-hour strategy. The interval from time zero to 1 hour was treated as a grace period for treatment initiation, after which patients were followed for time-to-event outcomes. (b) illustrates the target trial emulation framework used to emulate randomization. In the observed cohort, patients received treatment and were classified according to the 1-hour or 3-hour arm. A propensity-score model estimated the probability of receiving each strategy conditional on baseline covariates (age, comorbidities, site of infection, physiological and laboratory variables, and prior treatments). Stabilized inverse-probability-of-treatment weights were then applied to construct a weighted pseudo-population in which baseline covariates were balanced between arms, approximating a randomized comparison of the 1-hour and 3-hour strategies. |
Sensitivity and Subgroup Analyses
To assess the robustness of the association between initiating each bundle element within 1 hour and 28-day mortality, we performed several sensitivity and subgroup analyses. In sensitivity analyses, we: (1) fitted unweighted Cox models adjusting for confounders to show the “raw” associations without weighting; (2) re-estimated HRs using the same covariate set and propensity score model as in the primary analysis but applying the original, non-truncated stabilized weights to evaluate sensitivity to the truncation strategy; (3) widened the comparison window from 1–3 h to 1–6 h (ie, comparing initiation within 0–1 h vs 1–6 h) to examine the consistency of the early strategy effect over a broader time window; and (4) refitted the propensity score model excluding the presumed primary site of infection covariate to evaluate the robustness of the primary results. For subgroup analyses, we prespecified age, sex, hypertension, diabetes, chronic heart failure, chronic kidney disease, cirrhosis, and any vasopressor administration within 6 hours before time zero as subgroup variables. Within each subgroup, we repeated the IPTW analyses and included an interaction term between treatment strategy and the subgroup variable in the model. Wald tests were used to assess the statistical significance of interaction, and HRs with 95% confidence intervals were reported for each subgroup.
Results
We combined data from the MIMIC-IV, ZJ, and XY cohorts to emulate three target trials evaluating the timing of antibiotics, fluid resuscitation, and vasopressor initiation. Baseline and laboratory characteristics of the included patients were shown in Tables S2–S4. In the antibiotic timing trial, 7,801 patients were included. Of these, 5,496 (70.5%) received the antibiotic within 0–1 h after time zero and 2,305 (29.5%) between 1–3 h. After application of stabilized IPTW, the weighted cohort comprised 7,800 patients (5,574 in the 1-hour group and 2,226 in the 3-hour group), with good covariate balance between groups (Table 1 and Figure S2). Using the onset of hemodynamic instability as time zero, 1,411 patients met the eligibility criteria for the fluid resuscitation trial. Among them, 793 initiated crystalloid infusion within 0–1 h and received a cumulative volume ≥30 mL/kg within 3 h, and 618 between 1–3 h; the corresponding weighted patients were 794 and 615, respectively (Table S5 and Figure S3). In the vasopressor timing trial, 3,688 patients started vasopressors within 0–1 h and 1,786 between 1–3 h; after weighting, the cohort included 3,688 and 1,729 patients in the 1-hour and 3-hour groups, respectively (Table S6 and Figure S4).
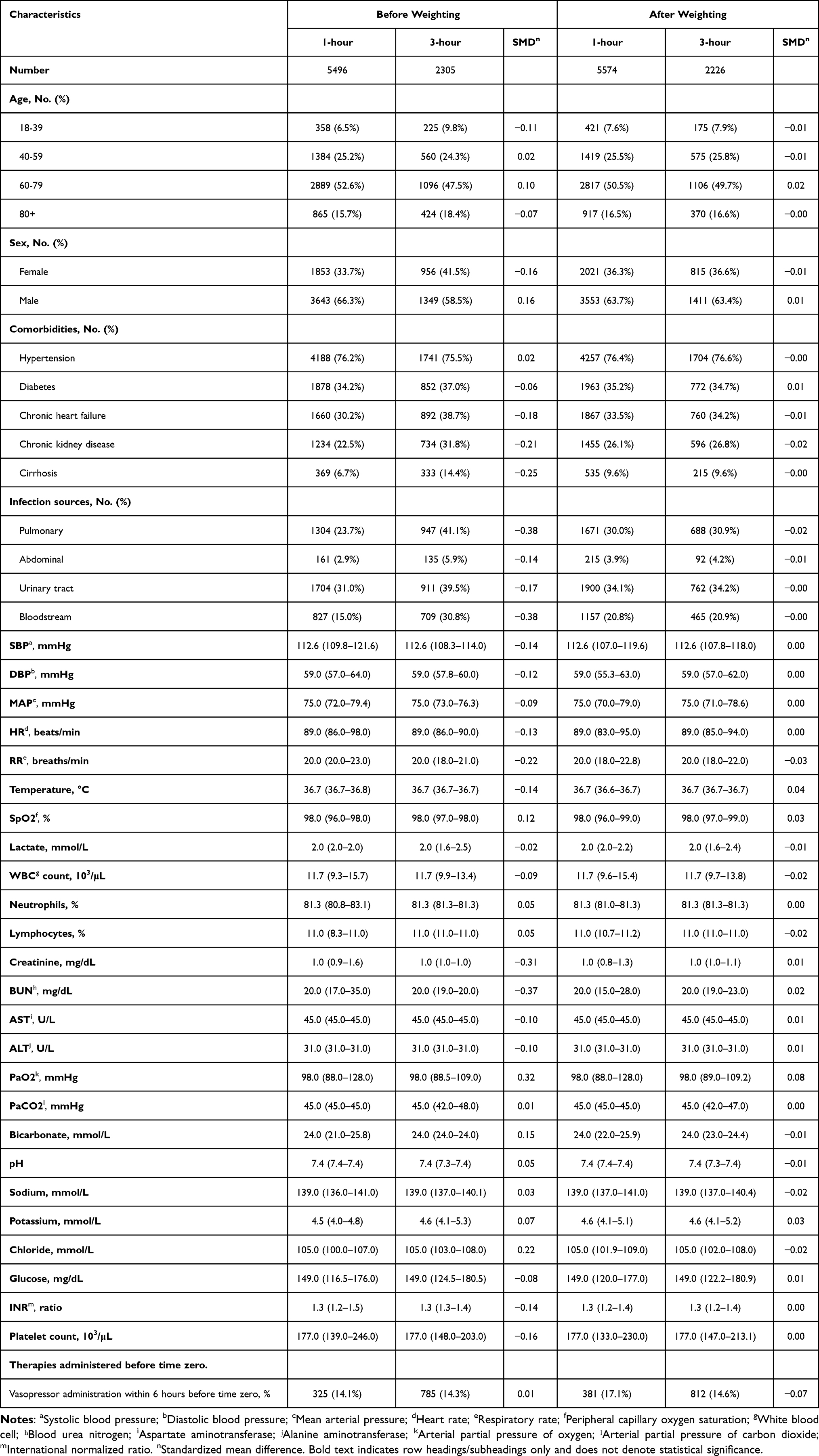 |
Table 1 Baseline Characteristics of Patients in the Antibiotic Cohort, Before and After Inverse Probability of Treatment Weighting |
Timing of Antibiotic Administration
Baseline characteristics before and after weighting for patients receiving antibiotics were shown in Table 1. After inverse probability weighting, the overall 28-day mortality was 6.5%. The weighted 28-day mortality was lower in the 1-hour group than in the 3-hour group (5.6% vs 8.8%). Time to ICU discharge was slightly shorter in the 1-hour group (3.7 ± 5.8 vs 4.1 ± 5.8 days), whereas the days with mechanical ventilation and CRRT were similar between groups (Table 2). Weighted Kaplan–Meier curves showed clear separation between the 1-hour and 3-hour strategies. Early antibiotic administration within 1 hour after time zero was associated with a lower risk of 28-day all-cause mortality (HR, 0.65; 95% CI, 0.54–0.79). For time to ICU discharge, the 1-hour strategy was associated with earlier ICU discharge (SHR, 1.20; 95% CI, 1.12–1.27) (Figures 2 and 3).
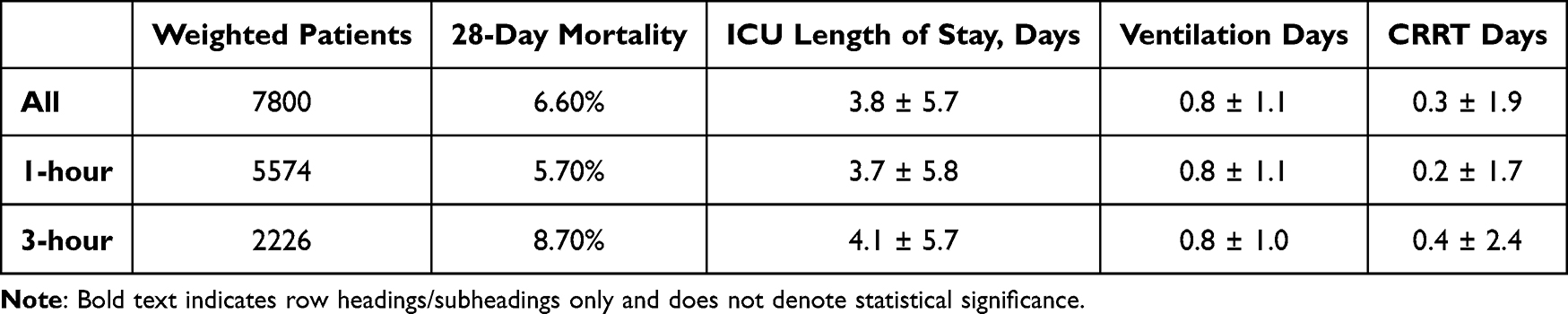 |
Table 2 28-Day Mortality, Time to ICU Discharge, Ventilation Days, and CRRT Days in the Antibiotic Cohort After Inverse-Probability-of-Treatment Weighting |
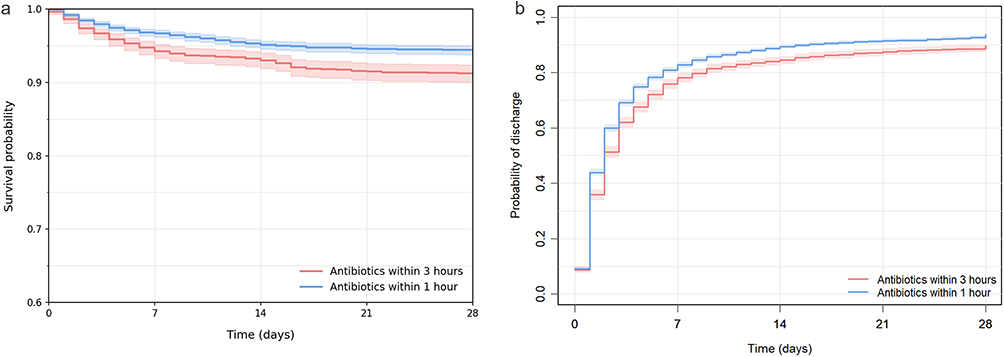 |
Figure 2 Kaplan–Meier curves and cumulative incidence curves in the antibiotic cohort. Kaplan–Meier curves and cumulative incidence curves in the antibiotic cohort. (a) shows inverse probability–weighted Kaplan–Meier curves for 28-day all-cause mortality, comparing patients who received antibiotics within 1 hour after time zero with those who received antibiotics between 1 and 3 hours. (b) shows the corresponding weighted cumulative incidence curves for ICU discharge, treating ICU death as a competing event. |
 |
Figure 3 Hazard ratios for 28-day mortality and time to ICU discharge outcome in the antibiotic cohort. Hazard ratios for 28-day mortality and time to ICU discharge outcome in the antibiotic cohort. The plot shows hazard ratios and subdistribution hazard ratios (squares) with 95% confidence intervals (horizontal lines) comparing administration of antibiotics within 1 hour versus 1–3 hours after time zero. The dashed vertical line represents a ratio of 1.0 (no difference between strategies). For 28-day mortality, a hazard ratio <1 indicates a lower death risk with antibiotics within 1 hour. For time to ICU discharge, a subdistribution hazard ratio >1 indicates a shorter time to ICU discharge with antibiotics within 1 hour. Note: Bold text indicates row headings/subheadings only and does not denote statistical significance. |
We performed sensitivity and subgroup analyses to test the robustness of these findings (Table S7). Results were consistent across all three sensitivity analyses. Notably, when the comparison window was expanded to 0–1 h versus 1–6 h, early antibiotic administration remained associated with lower 28-day mortality (HR, 0.73; 95% CI, 0.60–0.86), in line with the primary analysis. Results were similar when the presumed primary site of infection was excluded from the propensity score model (HR, 0.63; 95% CI, 0.51–0.76). The benefit of 1-hour antibiotics was preserved across predefined subgroups, with no statistically significant evidence of interaction.
Timing of Fluid Resuscitation Initiation
The characteristics for patients receiving crystalloids were described in Table S5. After weighting, the overall 28-day mortality was 12.8%. The weighted 28-day mortality was lower in the 1-hour group than in the 3-hour group (11.4% vs 14.7%). Time to ICU discharge was similar between groups (4.2 ± 5.7 vs 4.0 ± 5.2 days), as were the days with mechanical ventilation and CRRT (Table S8). Weighted Kaplan–Meier curves and HRs showed that initiation of fluid resuscitation within 1 hour after time zero was associated with a reduced risk of 28-day mortality (HR, 0.72; 95% CI, 0.53–0.97). Additionally, the 1-hour strategy was associated with earlier ICU discharge (SHR, 1.17; 95% CI, 1.02–1.33) (Figures S5 and S6).
The 28-day benefits of initiation within 1 h were consistent across the three sensitivity analyses. In the sensitivity analysis comparing a broader window (0–1 vs 1–6 h), early fluid resuscitation remained associated with lower 28-day mortality (HR, 0.73; 95% CI, 0.52–0.98). Additionally, excluding the presumed primary site of infection covariate yielded similar results (HR, 0.74; 95% CI, 0.54–1.00). The potential survival benefit of early fluid resuscitation was broadly consistent across predefined clinical subgroups (Table S9).
Timing of Vasopressor Administration
The baseline characteristics were detailed in Table S6. After weighting, the overall 28-day mortality was 12.8%. The weighted 28-day mortality was slightly higher in the 1-hour group than in the 3-hour group (13.0% vs 12.2%), whereas time to ICU discharge was marginally shorter (5.1 ± 6.5 vs 5.6 ± 6.6 days; Table S10). Weighted Kaplan–Meier curves showed no clear separation between the two strategies (Figure S7). Initiation of vasopressors within 1 hour after time zero was not associated with 28-day mortality (HR, 1.07; 95% CI, 0.89–1.29). Similarly, there was no clear association with time to ICU discharge (SHR, 1.02; 95% CI, 0.95–1.08; Figure S8).
Sensitivity and subgroup analyses supported these findings. When the comparison window was broadened to 0–1 h versus 1–6 h, the HR for 28-day mortality was 0.96 (95% CI, 0.85–1.27). Excluding the presumed primary site of infection did not change the estimate (HR, 1.08; 95% CI, 0.90–1.31). Across all prespecified subgroups, associations between early vasopressor initiation and mortality were similar, with no statistically significant evidence of interaction (Table S11).
Discussion
In this multicenter cohort study, we assessed the timing of three core sepsis bundle components—antibiotic administration, fluid resuscitation, and vasopressor initiation. We found that administration of antibiotics within 1 hour and initiation of fluid resuscitation within 1 hour were associated with lower 28-day mortality. These findings remained consistent across multiple sensitivity analyses. However, early vasopressor within 1 hour was not associated with improved survival. Taken together, these results provide supportive real-world evidence for the 1-hour bundle recommended in the Surviving Sepsis Campaign guidelines.4
A meta-analysis in sepsis suggested that earlier antibiotic administration was associated with improved outcomes but also highlighted substantial heterogeneity in how “early” treatment was defined and considerable ambiguity around the definition of “time zero”.27 A retrospective study in emergency department patients reported that earlier antibiotic administration within a 3-hour window was associated with lower mortality in sepsis.6 Furthermore, initiating antibiotics within 1 h could reduce death risk compared with later administration in patients with septic shock.19 In our study, we also observed a significant association between 1-hour antibiotics and lower 28-day mortality. Importantly, prior studies have focused on emergency department patients, whereas our cohort consisted of ICU patients with the first episode of sepsis. A recent machine learning study using the MIMIC-IV database showed that adherence to parts of the SSC guidelines including administering antibiotics within 1 h reduced 28-day mortality in patients admitted to the ICU; however, it did not exclude patients who had received antibiotics before inclusion.28 Our emulated trial addressed this gap by specifically evaluating patients without prior antibiotic exposure.
Early initiation of fluid resuscitation could be regarded as a liberal approach to fluid management.29 The Conservative versus Liberal Approach to Fluid Therapy of Septic Shock in Intensive Care (CLASSIC) trial showed that the median cumulative fluid volume in the standard fluid strategy increased by 2,013 mL over 90 days compared with the restrictive strategy but did not improve survival.16 However, survivors of septic shock tended to receive large fluid volumes early within 3 hour,17 which was consistent with our findings. The 1- hour fluid resuscitation group had higher 28-day survival than the 3-hour group. These results suggest that, in the early phase of septic shock, timely restoration of effective circulating volume might be crucial.
For vasopressors, the SSC 1-hour bundle recommends initiating vasopressors during or after fluid resuscitation when hypotension persists, emphasizing a “fluids first, vasopressors as needed” approach.4 The Crystalloid Liberal or Vasopressors Early Resuscitation in Sepsis (CLOVERS) trial demonstrated no difference in death risk among patients managed using the fluid- and vasopressor-first strategy.15 A randomized trial reported that early norepinephrine administration combined with fluid infusion improved shock control but did not reduce mortality.14 Consistently, we did not observe a survival benefit of initiating vasopressors within 1 hour compared with 1–3 hours. The lack of a survival benefit with earlier vasopressor initiation may reflect incomplete preload restoration, heterogeneity of shock phenotypes, or effects on the microcirculation; these possibilities remain speculative and warrant prospective study. Additionally, the absence of an observed survival benefit with earlier vasopressor initiation should be interpreted in light of limited precision, and the confidence intervals do not exclude modest clinically meaningful benefit or harm. Taken together with our findings on fluid resuscitation, these results suggest that, in the early resuscitation phase, prioritizing rapid fluid administration to augment circulating volume may confer more survival benefit than further accelerating vasopressor initiation to increase perfusion pressure.
This study has several strengths. First, we focused on patients with a first episode of sepsis in the ICU, addressing the gap left by previous sepsis bundle studies that mainly included patients in the ED.6,8,30,31 Second, we applied a target trial emulation framework with stabilized inverse probability weighting to separately evaluate the timing of antibiotics, fluids, and vasopressors, thereby reducing indication bias common in observational analyses.21,32 Third, we integrated the MIMIC-IV database with two ICU cohorts from China (Zhujiang and Xiangya hospitals), which enhanced the generalizability of our findings. Fourth, we implemented strict inclusion and exclusion criteria, ensuring our study closely approximates real-world RCTs. Finally, the consistency of results across sensitivity and subgroup analyses supported the robustness of the primary findings.
This study had several limitations. First, we did not evaluate patients who fully adhered to all 1- and 3-hour bundle elements, focusing instead on the timing of the three core treatment elements and their impact on outcomes, indicating that we could not determine the combined effect of the full bundle at different timepoints on prognosis. Second, despite pooling three cohorts and applying a target trial emulation approach, the effective sample sizes for the fluid resuscitation and vasopressor timing trials remained relatively modest, which might have limited the precision of effect estimates. Third, because we pooled the three cohorts, our estimates should be interpreted as an across-center average effect; however, unmeasured center-level differences (eg, practice patterns, illness severity, prior treatment, and coding habits) may persist, and MIMIC-IV contributed the largest proportion of patients, which may affect generalizability. Fourth, pathogen-stratified analyses were not feasible across the three cohorts because microbiology data completeness and coding differed between databases, and many patients had negative cultures or lacked comparable pathogen information. Fifth, we did not investigate different treatment timings of clinical phenotypes of sepsis owing to the lack of etiological data and sample size.33–35 Accordingly, heterogeneity of treatment effects across clinically relevant phenotypes cannot be excluded, and some patients may respond differently to early fluid resuscitation or vasopressor strategies. Additionally, we explored the effects of initiating bundle elements within 1 hour in the ICU using target trials; however, these target trials could not replace RCTs. Future studies, including pragmatic randomized trials or hybrid effectiveness–implementation designs, are warranted to validate these timing targets in routine ICU practice, particularly to clarify the optimal timing of vasopressor initiation. Notably, RCTs on the 1-hour sepsis bundle in the ED remained lacking. We look forward to the results of the upcoming cluster RCT by Frank et al on patients with sepsis in the ED.36 Finally, while target trial emulation strengthens causal inference from observational data, these findings cannot substitute for randomized controlled trials and should be interpreted as complementary, guideline-informing evidence. Because this study emulates target trials using observational data, our estimates should be interpreted as associations under the prespecified design and modeling assumptions rather than definitive causal effects.
Conclusion
In this study, administration of antibiotics and initiation of fluid resuscitation within 1 hour were associated with lower 28-day mortality and earlier ICU discharge. However, initiating vasopressors within 1 hour did not show significant survival benefits. These findings apply to ICU patients with a first episode of sepsis and may not generalize to emergency department populations. As an observational target trial emulation, our results are intended to inform guideline refinement and bedside prioritization rather than to establish definitive causality, and they provide element-specific evidence to help address gaps in the sepsis bundle literature.
Abbreviations
CI, Confidence Interval; CLASSIC, Conservative versus Liberal Approach to Fluid Therapy of Septic Shock in Intensive Care; CLOVERS, Crystalloid Liberal or Vasopressors Early Resuscitation in Sepsis; CRRT, Continuous Renal Replacement Therapy; ED, Emergency Department; HR, Hazard Ratio; ICU, Intensive Care Unit; IPTW, Inverse Probability of Treatment Weighting; MIMIC-IV, Medical Information Mart for Intensive Care-IV; RCT, Randomized Controlled Trial; SHR, Subdistribution Hazard Ratio; SOFA, Sequential Organ Failure Assessment; SSC, Surviving Sepsis Campaign; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; ZJ, Zhujiang Hospital; XY, Xiangya Hospital.
Data Sharing Statement
De-identified data from the development cohorts (MIMIC-IV and eICU-CRD) are available from PhysioNet (The Research Resource for Complex Physiologic Signals; https://physionet.org/) upon approval of a proposal and completion of the required data use agreement. Clinical data from the validation cohorts (Zhujiang Hospital and Xiangya Hospital) were used under license for this study and, owing to institutional privacy regulations and data transfer agreements, are not publicly available but may be obtained from the corresponding author upon reasonable request and with permission of the participating institutions.
Ethics Approval and Informed Consent
The MIMIC-IV databases are publicly available via PhysioNet to credentialed researchers (authorized investigator for this study: C.Y.; ID:14644112). The Medical Ethics Committees of Zhujiang Hospital of Southern Medical University (authorized investigator: L.Z.; Nos.2025-KY-237-01) and Xiangya Hospital of Central South University (authorized investigator: Z.S.; Nos.2024030214) approved the use of institutional data for this study. All datasets were fully de-identified prior to analysis, and the requirement for informed consent was waived. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
This work was supported by the National Science and Technology Major Project of China (Nos. 2025ZD01908101, to Y.Z.), the National Natural Science Foundation of China (Nos. 82472176 and 81971859, to L.Z.), and the Science and Technology Program of Guangzhou (No. 2025A04J3775, to Z.T.). We are deeply grateful to the patients whose data contributed to this study; their participation is indispensable to advancing data-intensive research in critical care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Science and Technology Major Project of China (Nos. 2025ZD01908101, to Y.Z.), National Natural Science Foundation of China (Nos. 82472176 and 81971859, to L.Z.), and the Science and Technology Program of Guangzhou (No. 2025A04J3775, to Z.T.).
Disclosure
The authors declare no competing interests in this work.
References
1. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–13. doi:10.1016/S0140-6736(19)32989-7
2. Fleischmann-Struzek C, Mellhammar L, Rose N, et al. Incidence and mortality of hospital-and ICU-treated sepsis: results from an updated and expanded systematic review and meta-analysis. Intensive Care Med. 2020;46:1552–1562. doi:10.1007/s00134-020-06151-x
3. Buchman TG, Simpson SQ, Sciarretta KL, et al. Sepsis among medicare beneficiaries: 1. The burdens of sepsis, 2012–2018. Crit Care Med. 2020;48(3):276–288. doi:10.1097/CCM.0000000000004224
4. Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign bundle: 2018 update. Intensive Care Med. 2018;44:925–928. doi:10.1007/s00134-018-5085-0
5. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063–e1143. doi:10.1097/CCM.0000000000005337
6. Seymour CW, Gesten F, Prescott HC, et al. Time to treatment and mortality during mandated emergency care for sepsis. N Engl J Med. 2017;376(23):2235–2244. doi:10.1056/NEJMoa1703058
7. Gilbert JA. Sepsis care bundles: a work in progress. Lancet Respir Med. 2018;6(11):821–823. doi:10.1016/S2213-2600(18)30362-X
8. Prachanukool T, Sanguanwit P, Thodamrong F, Suttapanit K. The 28-day mortality outcome of the complete hour-1 sepsis bundle in the emergency department. Shock. 2021;56(6):969–974. doi:10.1097/SHK.0000000000001815
9. Weinberger J, Rhee C, Klompas M. A critical analysis of the literature on time-to-antibiotics in suspected sepsis. J Infect Dis. 2020;222(Suppl 2):S110–s118. doi:10.1093/infdis/jiaa146
10. Im Y, Kang D, Ko RE, et al. Time-to-antibiotics and clinical outcomes in patients with sepsis and septic shock: a prospective nationwide multicenter cohort study. Crit Care. 2022;26(1):19. doi:10.1186/s13054-021-03883-0
11. Puskarich MA, Trzeciak S, Shapiro NI, et al. Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol. Crit Care Med. 2011;39(9):2066–2071. doi:10.1097/CCM.0b013e31821e87ab
12. Venkatesh B, Schlapbach L, Mason D, et al. Impact of 1-hour and 3-hour sepsis time bundles on patient outcomes and antimicrobial use: a before and after cohort study. Lancet Regional Health–Western Pacific. 2022;18.
13. Hamzaoui O, Shi R. Early norepinephrine use in septic shock. J Thorac Dis. 2020;12(Suppl 1):S72–s77. doi:10.21037/jtd.2019.12.50
14. Permpikul C, Tongyoo S, Viarasilpa T, Trainarongsakul T, Chakorn T, Udompanturak S. Early use of norepinephrine in septic shock resuscitation (CENSER). A randomized trial. Am J Respir Crit Care Med. 2019;199(9):1097–1105. doi:10.1164/rccm.201806-1034OC
15. National Heart L, Prevention BI. Network EToALICT. Early restrictive or liberal fluid management for sepsis-induced hypotension. N Engl J Med. 2023;388(6):499–510.
16. Meyhoff TS, Hjortrup PB, Wetterslev J, et al. Restriction of intravenous fluid in ICU patients with septic shock. N Engl J Med. 2022;386(26):2459–2470. doi:10.1056/NEJMoa2202707
17. Lee SJ, Ramar K, Park JG, Gajic O, Li G, Kashyap R. Increased fluid administration in the first three hours of sepsis resuscitation is associated with reduced mortality: a retrospective cohort study. Chest. 2014;146(4):908–915. doi:10.1378/chest.13-2702
18. Liu VX, Fielding-Singh V, Greene JD, et al. The timing of early antibiotics and hospital mortality in sepsis. Am J Respir Crit Care Med. 2017;196(7):856–863. doi:10.1164/rccm.201609-1848OC
19. Im Y, Kang D, Ko R-E, et al. Time-to-antibiotics and clinical outcomes in patients with sepsis and septic shock: a prospective nationwide multicenter cohort study. Crit Care. 2022;26:1–10. doi:10.1186/s13054-021-03883-0
20. Leisman DE, Angel C, Schneider SM, D’Amore JA, D’Angelo JK, Doerfler ME. Sepsis presenting in hospitals versus emergency departments: demographic, resuscitation, and outcome patterns in a multicenter retrospective cohort. J Hosp Med. 2019;14(6):340–348. doi:10.12788/jhm.3188
21. Hernán MA, Robins JM. Using big data to emulate a target trial when a randomized trial is not available. Am J Epidemiol. 2016;183(8):758–764. doi:10.1093/aje/kwv254
22. Hernán MA, Wang W, Leaf DE. Target trial emulation: a framework for causal inference from observational data. JAMA. 2022;328(24):2446–2447. doi:10.1001/jama.2022.21383
23. Kalantari A, Rezaie SR. Challenging the One-hour Sepsis Bundle. West J Emerg Med. 2019;20(2):185–190. doi:10.5811/westjem.2018.11.39290
24. Johnson A, Bulgarelli L, Pollard T, Horng S, Celi LA, Mark R. Mimic-iv. PhysioNet; 2020:49–55. Available from: https://physionet.org/content/mimiciv/10/.
25. Von Elm E, Altman DG, Egger M, et al. The strengthening the reporting Of observational studies In epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
26. Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):762–774. doi:10.1001/jama.2016.0288
27. Asner SA, Desgranges F, Schrijver IT, Calandra T. Impact of the timeliness of antibiotic therapy on the outcome of patients with sepsis and septic shock. J Infect. 2021;82(5):125–134. doi:10.1016/j.jinf.2021.03.003
28. Kalimouttou A, Lerner I, Cheurfa C, Jannot A-S, Pirracchio R. Machine-learning-derived sepsis bundle of care. Intensive Care Med. 2023;49(1):26–36. doi:10.1007/s00134-022-06928-2
29. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368–1377. doi:10.1056/NEJMoa010307
30. Baghdadi JD, Brook RH, Uslan DZ, et al. Association of a care bundle for early sepsis management with mortality among patients with hospital-onset or community-onset sepsis. JAMA Intern Med. 2020;180(5):707–716. doi:10.1001/jamainternmed.2020.0183
31. Rhee C, Yu T, Wang R, et al. Association between implementation of the severe sepsis and septic shock early management bundle performance measure and outcomes in patients with suspected sepsis in US hospitals. JAMA Netw Open. 2021;4(12):e2138596–e2138596. doi:10.1001/jamanetworkopen.2021.38596
32. McCormick N, Yokose C, Lu N, et al. Comparative effectiveness of sodium-glucose cotransporter-2 inhibitors for recurrent nephrolithiasis among patients with pre-existing nephrolithiasis or gout: target trial emulation studies. BMJ. 2024;387.
33. Seymour CW, Kennedy JN, Wang S, et al. Derivation, validation, and potential treatment implications of novel clinical phenotypes for sepsis. JAMA. 2019;321(20):2003–2017. doi:10.1001/jama.2019.5791
34. Xu Z, Mao C, Su C, et al. Sepsis subphenotyping based on organ dysfunction trajectory. Critical Care. 2022;26(1):197. doi:10.1186/s13054-022-04071-4
35. Yang A, Kennedy JN, Reitz KM, et al. Time to treatment and mortality for clinical sepsis subtypes. Crit Care. 2023;27(1):236. doi:10.1186/s13054-023-04507-5
36. Frank HE, Evans L, Phillips G, et al. Assessment of implementation methods in sepsis: study protocol for a cluster-randomized hybrid type 2 trial. Trials. 2023;24(1):620. doi:10.1186/s13063-023-07644-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation and Prognostic Assessment of Low T3 Syndrome and Norepinephrine Dosage for Patients with Sepsis: A Retrospective Single-Center (Cohort) Study
Zhang J, Fu S, Liu F, Wan J, Wu S, Jiang G, Tao W, Zhou W, Qian K
International Journal of General Medicine 2022, 15:4837-4847
Published Date: 10 May 2022
Impaired Circulating Antibody-Secreting Cells Generation Predicts the Dismal Outcome in the Elderly Septic Shock Patients
Xu H, Li T, Zhang X, Li H, Lv D, Wang Y, Huo F, Bai J, Wang C
Journal of Inflammation Research 2022, 15:5293-5308
Published Date: 13 September 2022
Progress in the Clinical Assessment and Treatment of Myocardial Depression in Critically Ill Patient with Sepsis
Shen XD, Zhang HS, Zhang R, Li J, Zhou ZG, Jin ZX, Wang YJ
Journal of Inflammation Research 2022, 15:5483-5490
Published Date: 20 September 2022
Rethinking Pediatric Sepsis and Septic Shock: Beyond International Consensus Criteria
Shamavu GK, Mohamoud F
Pediatric Health, Medicine and Therapeutics 2025, 16:61-65
Published Date: 4 March 2025
Rethinking Fluid Resuscitation in Septic Shock: A Phase-Adapted, Endothelium-Sparing Approach to Mitigate Capillary Leak
Li B, Zhao L
Journal of Inflammation Research 2026, 19:587066
Published Date: 3 March 2026