Back to Journals » Journal of Inflammation Research » Volume 19
Rethinking Fluid Resuscitation in Septic Shock: A Phase-Adapted, Endothelium-Sparing Approach to Mitigate Capillary Leak
Received 7 December 2025
Accepted for publication 6 February 2026
Published 3 March 2026 Volume 2026:19 587066
DOI https://doi.org/10.2147/JIR.S587066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xin Du
Bin Li,1,2 Ling Zhao1
1Department of Intensive Care Unit, The People’s Hospital Medical Group of Xiangzhou, Zhuhai, Guangdong, People’s Republic of China; 2Department of Pharmacy, The People’s Hospital Medical Group of Xiangzhou, Zhuhai, Guangdong, People’s Republic of China
Correspondence: Ling Zhao, The People’s Hospital Medical Group of Xiangzhou, No. 178, Lanpu Road, Qianshan, Xiangzhou District, Zhuhai, Guangdong, 519000, People’s Republic of China, Email [email protected]
Abstract: Sepsis-induced endothelial dysfunction and the resultant capillary leak syndrome are defining features of septic shock, posing a profound challenge to conventional fluid resuscitation strategies. The long-standing debate over crystalloid versus colloid administration is evolving beyond a simple dichotomy toward a more nuanced, physiologically informed approach. This review critically examines the pathophysiological cascade driving vascular hyperpermeability in sepsis—from endothelial glycocalyx degradation and inflammatory cytokine storms to oxidative stress and nitric oxide dysregulation. We trace the evolution of resuscitation paradigms from early goal-directed therapy to modern conservative approaches, highlighting the limitations of crystalloid-dominant protocols, including intravascular volume depletion despite a positive fluid balance and iatrogenic organ injury. Drawing on evidence from landmark clinical trials (eg, ALBIOS, CRISTAL, SMART) and a pharmacological reappraisal of fluid properties, we argue that a one-size-fits-all strategy is obsolete. Instead, this narrative review synthesizes recent trial evidence and pathophysiological insights to propose the Phase-Adapted, Endothelium-Sparing (PAES) resuscitation strategy, a novel framework that tailors fluid type and volume to the distinct temporal phases of septic shock: Rescue, Optimization, Stabilization, and De-escalation. This model advocates for initial resuscitation with balanced crystalloids, followed by the judicious integration of albumin in specific, high-risk patient subgroups to leverage its unique oncotic and pleiotropic, endothelium-stabilizing effects. We further outline how dynamic hemodynamic monitoring, point-of-care ultrasound, and emerging biomarkers of endothelial injury (eg, syndecan-1, angiopoietin-2) can guide the real-time implementation of this personalized strategy. The PAES framework aims to uncouple macrohemodynamic stabilization from microcirculatory injury, offering a pragmatic pathway to optimize perfusion, mitigate capillary leak, and improve outcomes in this critically ill population.
Keywords: personalized medicine, septic shock, fluid resuscitation, endothelial dysfunction, capillary leak syndrome
Introduction
Sepsis, a dysregulated host response to infection leading to life-threatening organ dysfunction, remains a leading cause of mortality and critical illness worldwide.1 Its most severe manifestation, septic shock, is characterized by profound circulatory, cellular, and metabolic abnormalities. Central to this pathology is a catastrophic failure of the vascular endothelium.2 The endothelium, far from being a passive conduit, is a dynamic organ that governs vascular tone, permeability, inflammation, and hemostasis.3 In sepsis, it becomes the epicenter of a pathological cascade, resulting in widespread vasodilation, microcirculatory disruption, and a dramatic increase in vascular permeability—the so-called capillary leak syndrome.4 This phenomenon leads to massive fluid shifts from the intravascular to the interstitial space, causing profound hypovolemia, tissue edema, and ultimately, multiple organ failure.5,6
For decades, fluid resuscitation has been the cornerstone of septic shock management, aimed at restoring intravascular volume and improving organ perfusion.7 Yet, the optimal approach remains one of the most contentious topics in critical care medicine. The clinical paradigm has undergone a seismic shift, moving from the aggressive, protocolized “early goal-directed therapy” (EGDT) of the early 2000s to more conservative, individualized strategies following the publication of the landmark ProCESS, ARISE, and ProMISe trials.8–11 This evolution reflects a growing recognition of a critical paradox: the very intervention designed to save lives—intravenous fluid—can itself propagate harm. Excessive fluid administration, particularly with crystalloids, contributes to a positive cumulative fluid balance, which is independently associated with increased mortality, prolonged mechanical ventilation, and acute kidney injury (AKI).12,13
The debate has traditionally been framed as a choice between crystalloids and colloids. Crystalloids are inexpensive and readily available, but their poor intravascular retention can exacerbate tissue edema.14 Colloids, particularly albumin, offer superior oncotic pressure and prolonged intravascular residence, but concerns over the safety of synthetic colloids (eg, hydroxyethyl starch [HES]) and the cost of albumin have limited their universal adoption.15,16 However, this simplistic “either/or” debate fails to address the underlying pathophysiology. The central challenge in septic shock resuscitation is not merely to fill the intravascular space, but to do so while actively protecting—or at least not further injuring—the fragile endothelial barrier.
Classically, septic shock has been understood primarily through the lens of macro-circulatory failure—characterized by profound vasoplegia and relative hypovolemia—and cellular metabolic dysexecution. While restoring macro-hemodynamic parameters remains the cornerstone of initial management, this macro-centric view often overlooks the barrier that mediates perfusion: the endothelium. This review challenges the conventional paradigm by reframing fluid resuscitation as a targeted pharmacological intervention. We argue that the choice of fluid, its volume, and its timing must be tailored to the dynamic pathophysiology of the septic endothelium. To this end, we critically synthesize the evidence on fluid pharmacodynamics and clinical outcomes to propose a novel, actionable framework: the Phase-Adapted, Endothelium-Sparing (PAES) resuscitation strategy. This strategy moves beyond a one-size-fits-all approach to align fluid therapy with the four distinct phases of shock management—Rescue, Optimization, Stabilization, and De-escalation. By strategically combining balanced crystalloids with the targeted use of albumin, and guiding therapy with advanced hemodynamic monitoring and biomarkers, the PAES framework provides a rational pathway to restore perfusion while mitigating capillary leak and iatrogenic fluid-related harm.
Search Strategy and Selection Criteria
For this narrative review, we conducted a systematic search of PubMed, Embase, and the Cochrane Library. The search strategy was executed in two phases: an initial broad search (from database inception to October 2025) to identify foundational literature on endothelial dysfunction and fluid resuscitation, followed by focused thematic searches prioritizing the period from January 2014 to October 2025. This timeframe was selected to capture contemporary evidence emerging after the publication of landmark sepsis trials.
We used combinations of medical subject headings terms and free-text keywords related to three core domains: Endothelial Pathophysiology (eg, “endothelial glycocalyx,” “syndecan-1”); Pharmacology of Resuscitation Fluids (eg, “balanced crystalloids,” “albumin,” “ALBIOS,” “SMART”); Clinical Management Strategies (eg, “fluid responsiveness,” “deresuscitation”). We prioritized randomized controlled trials (RCTs), meta-analyses, and international guidelines published in English. The reference lists of retrieved articles were manually screened for additional relevant studies. A comprehensive description of the specific search strings and multi-stage methodology is provided in the Supplementary Material.
The Endothelium: The Epicenter of Septic Shock Pathophysiology
A sophisticated understanding of fluid therapy requires a deep appreciation for its primary target and principal casualty: the vascular endothelium. In sepsis, the endothelium transitions from a guardian of homeostasis to an active participant in a self-amplifying cycle of injury.3,17
Glycocalyx Degradation: The First Line of Defense Breached
The endothelial surface layer (ESL), a delicate gel-like mesh of proteoglycans (eg, syndecans, glypicans) and glycosaminoglycans (eg, heparan sulfate, hyaluronan), is the primary barrier regulating vascular permeability.18 The glycocalyx acts as a molecular sieve, a mechanotransducer of shear stress, and a reservoir of antioxidants and anticoagulants.19 Its degradation is one of the earliest and most critical events in sepsis,20 often occurring within hours of sepsis induction.21 Inflammatory mediators, particularly tumor necrosis factor-alpha (TNF-α), and bacterial endotoxins trigger the release of enzymes like heparanase and matrix metalloproteinases (MMPs), which cleave core components of the glycocalyx from the endothelial surface.22,23
The shedding of these components into the circulation, such as syndecan-1 and hyaluronan fragments, serves as a quantifiable biomarker of endothelial injury and is strongly correlated with sepsis severity, organ dysfunction, and mortality.21,24 The loss of the glycocalyx barrier dramatically increases vascular permeability, allowing plasma proteins and fluid to leak into the interstitium. This process not only causes tissue edema but also impairs microcirculatory flow by promoting leukocyte and platelet adhesion to the now-exposed endothelial cell surface.25,26 Resuscitation itself can be a “second hit”; large volumes of crystalloids, especially unbalanced solutions like 0.9% saline, can further accelerate glycocalyx shedding through dilution of plasma proteins and direct inflammatory effects.4,27 The consequences of this degradation are summarized in Table 1.
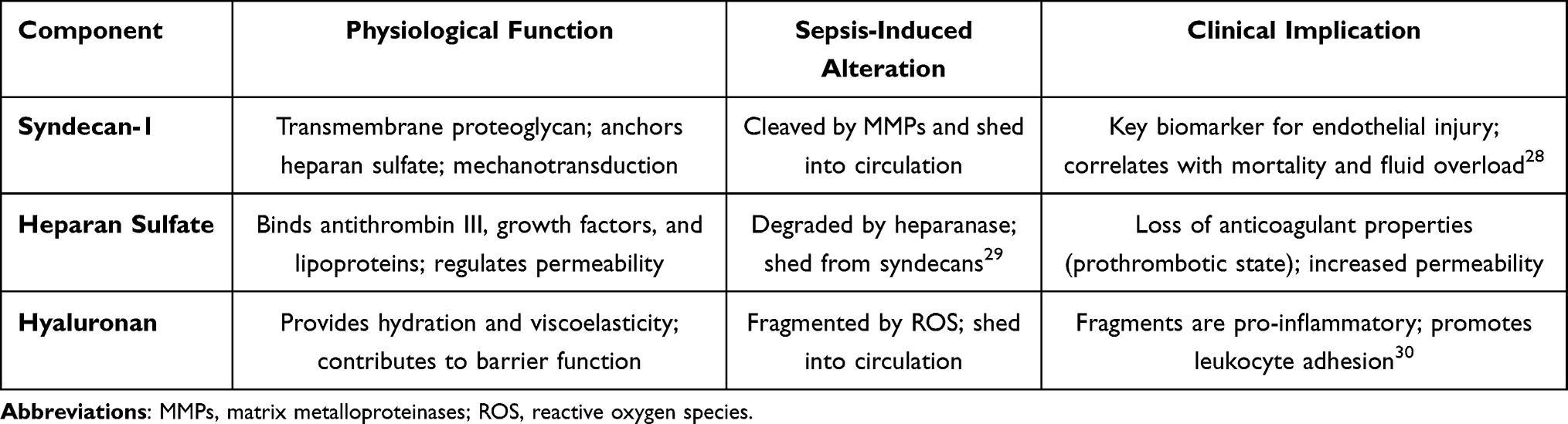 |
Table 1 Endothelial Glycocalyx Components and Their Dysregulation in Sepsis |
Inflammatory Cascade and Endothelial Apoptosis
The systemic inflammatory response in sepsis—often termed a “cytokine storm”—directly targets the endothelium. Pro-inflammatory cytokines like TNF-α and interleukin-6 (IL-6) induce profound changes in endothelial cells. They promote the upregulation of adhesion molecules (eg, E-selectin, ICAM-1), which facilitates neutrophil adhesion and transmigration, propagating inflammation within tissues.31,32 Furthermore, these cytokines disrupt the integrity of inter-endothelial tight junctions by downregulating key structural proteins like VE-cadherin and claudin-5, creating paracellular gaps for fluid extravasation.33
The inflammatory milieu also pushes the endothelium toward a procoagulant state by inducing the expression of tissue factor and downregulating natural anticoagulants like thrombomodulin and protein C.34,35 This contributes to the microthrombi formation and disseminated intravascular coagulation (DIC) often seen in severe sepsis. Finally, sustained inflammatory signaling can trigger programmed cell death (apoptosis) in endothelial cells, leading to denudation of the vascular lining and a complete loss of barrier function.32,36
Oxidative Stress and Nitric Oxide Dysregulation
Sepsis is a state of profound oxidative stress, where the production of reactive oxygen species (ROS) overwhelms the body’s endogenous antioxidant defenses.37,38 Activated neutrophils and endothelial cells themselves generate large amounts of superoxide via NADPH oxidase (NOX) enzymes. This excess ROS has multiple deleterious effects. It directly damages the glycocalyx, causes lipid peroxidation of cell membranes, and activates pro-inflammatory signaling pathways like nuclear factor-kappa B (NF-κB), perpetuating the inflammatory cycle.
Critically, ROS uncouples endothelial nitric oxide synthase (eNOS), the enzyme responsible for producing the vasodilator nitric oxide (NO). Instead of producing NO, uncoupled eNOS generates more superoxide.37 Simultaneously, inducible nitric oxide synthase (iNOS) is upregulated in response to inflammation, leading to a massive, uncontrolled surge in NO production. This “NO storm” is a primary driver of the profound vasodilation and vasopressor-refractory hypotension characteristic of septic shock.39,40 The excess NO also reacts with superoxide to form peroxynitrite, a highly potent oxidant that nitrates proteins, damages DNA, and causes mitochondrial dysfunction, further crippling endothelial cell function and promoting apoptosis (Figure 1).37,38
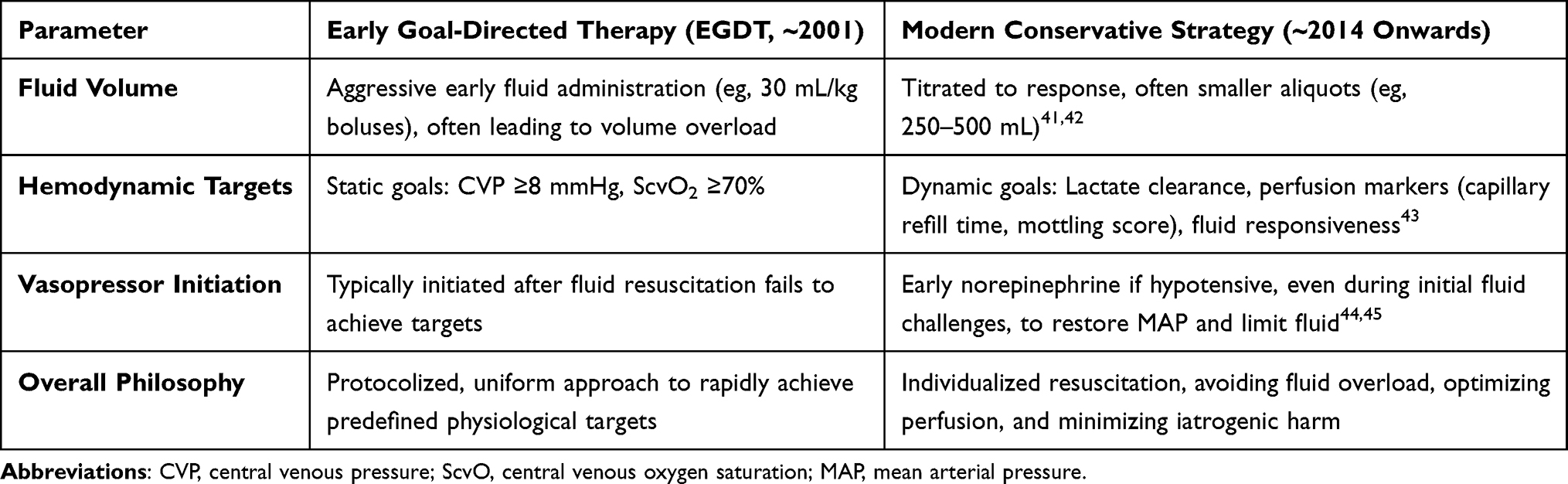 |
Table 2 Evolution of Fluid Resuscitation Paradigms in Sepsis Management |
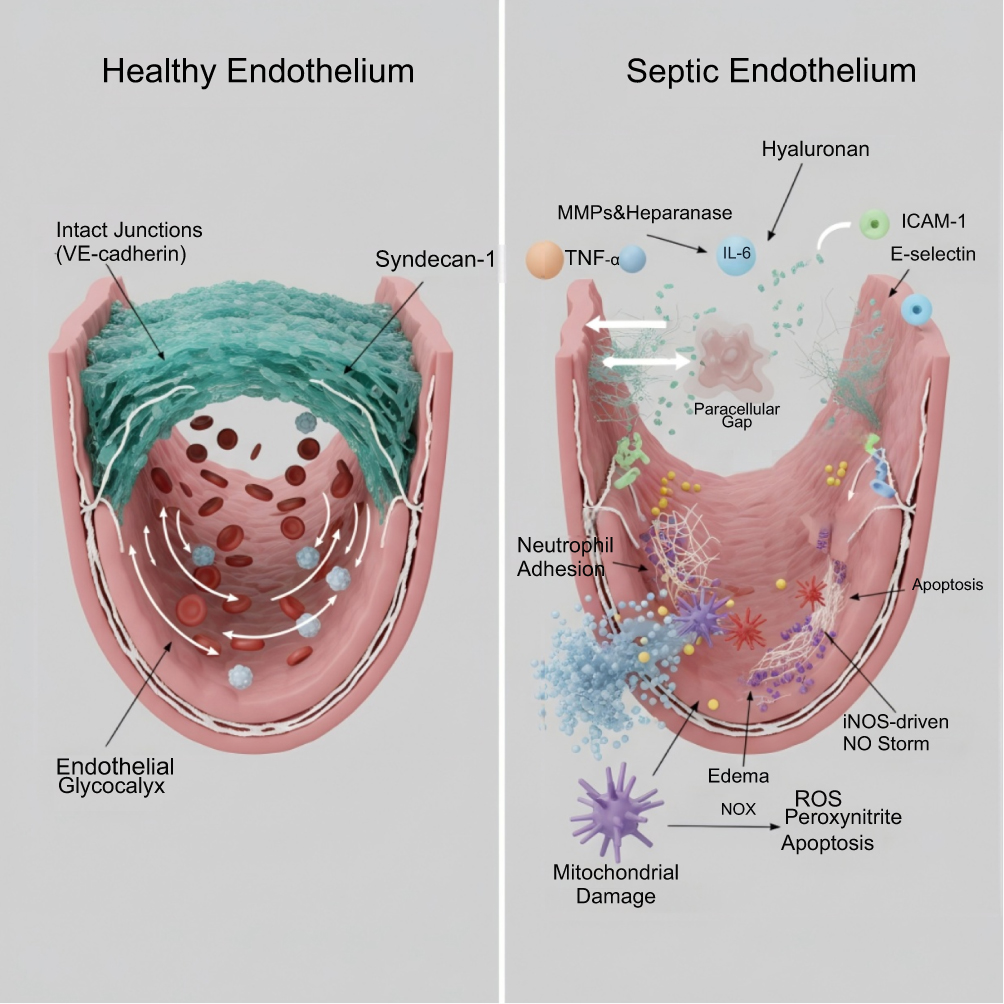 |
Figure 1 Pathophysiological Alterations of the Vascular Endothelium in Septic Shock. This infographic contrasts healthy endothelium with septic endothelium, illustrating key pathological changes. Healthy Endothelium: Shows intact endothelial cells with robust tight junctions (VE-cadherin) and a thick, continuous endothelial glycocalyx. Blood components flow smoothly in the lumen. Septic Endothelium: Depicts glycocalyx degradation (shedding Syndecan-1, Hyaluronan via MMPs, Heparanase), forming paracellular gaps, and causing vascular leakage (Plasma Proteins, Edema). Inflammatory triggers (TNF-α, IL-6) induce ICAM-1/E-selectin expression, promoting Neutrophil Adhesion and Endothelial Apoptosis. Oxidative stress (ROS from NOX) and iNOS-driven NO Storm lead to toxic Peroxynitrite (ONOO−) formation, causing Mitochondrial Damage and further Apoptosis, culminating in endothelial barrier breakdown characteristic of septic shock. |
From Aggressive Protocols to Individualized Care: The Evolution of a Paradigm
The approach to sepsis resuscitation has evolved significantly, reflecting a better understanding of the dangers of fluid overload. The era of rigid, aggressive protocols has given way to a more nuanced, conservative approach, as outlined in Table 2. This shift underscores the importance of individualizing therapy rather than adhering to uniform targets. Current guidelines reflect this evolving understanding but also highlight continuing areas of uncertainty. The 2021 Surviving Sepsis Campaign guidelines suggest using balanced crystalloids over saline and recommend albumin in patients requiring large volumes of crystalloids.46 However, the guidelines also note there is insufficient evidence to recommend a strict restrictive versus liberal fluid strategy within the first 24 hours of resuscitation. Furthermore, the recommendation for albumin relies heavily on conditional benefits observed in subgroup analyses (eg, in septic shock) rather than definitive survival benefits in the broader sepsis population. This ongoing controversy regarding fluid volume limits and patient selection for albumin underlines the limitations of a standardized protocol and the necessity for a more personalized, phase-adapted approach.
A Pharmacological Reappraisal of Resuscitation Fluids
The choice of resuscitation fluid should be considered a pharmacological intervention with distinct mechanisms of action, pharmacokinetics, and adverse effect profiles. Understanding these differences is fundamental to developing an endothelium-sparing strategy.
Crystalloids: The Double-Edged Sword of Volume Expansion
Crystalloids are the first-line fluid for sepsis resuscitation globally.7 Their primary advantage is the rapid expansion of the extracellular fluid compartment. However, their composition dictates their physiological impact.
Unbalanced Crystalloids (0.9% Saline): Isotonic saline has been the historical workhorse, but its supraphysiological chloride concentration (154 mmol/L) and acidic pH (~5.0–5.5) are increasingly recognized as harmful.14,47 The high chloride load can induce a hyperchloremic metabolic acidosis, which has been linked to renal vasoconstriction, reduced glomerular filtration rate, and an increased incidence of AKI.29,47 Studies have shown that saline administration is associated with more significant glycocalyx degradation compared to balanced solutions.
Balanced Crystalloids (eg, Lactated Ringer’s, Plasma-Lyte): These solutions are formulated to more closely mimic the electrolyte composition of plasma, with lower chloride concentrations and the presence of a buffer (eg, lactate, acetate, gluconate) that is metabolized to bicarbonate.48,49 The landmark SMART trial, which randomized over 15,000 critically ill adults, found that the use of balanced crystalloids resulted in a lower incidence of major adverse kidney events (MAKE) within 30 days (including death, new renal-replacement therapy, or persistent renal dysfunction) compared to saline.50 A prespecified subgroup analysis of patients with sepsis in the SMART trial showed an even more pronounced benefit, with a significant reduction in 30-day mortality (25.2% vs 29.4%). By avoiding severe acid-base disturbances and high chloride loads, balanced solutions appear to be a more physiologically sound and endothelium-friendly choice for initial resuscitation.
Despite these benefits, all crystalloids share a major pharmacokinetic limitation: rapid redistribution into the interstitial space. Only 20–30% of an infused crystalloid bolus remains in the intravascular compartment after one hour.51 This poor volume-expanding efficiency means that large volumes are required to achieve hemodynamic targets, directly contributing to tissue edema, organ congestion, and the well-documented harms of a positive fluid balance (Table 3).
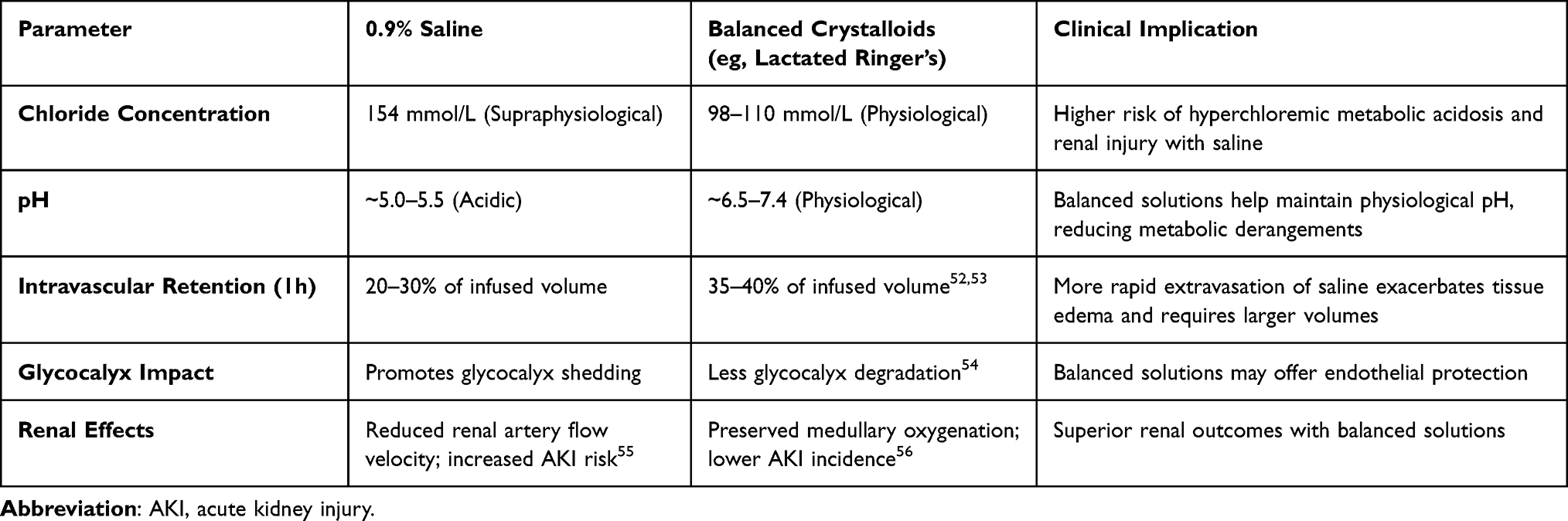 |
Table 3 Comparative Pharmacokinetics and Physiological Effects of Crystalloid Solutions |
Colloids: From Synthetic Risks to Therapeutic Potential
Colloids contain large molecules that are retained in the intravascular space, exerting oncotic pressure to hold and draw fluid in.
Synthetic Colloids (HES, Gelatins): For years, synthetic colloids like HES were championed for their superior volume-expanding properties. However, a wealth of evidence has demonstrated significant harm. Multiple large RCTs (eg, 6S, CRISTAL) have consistently linked HES administration to an increased risk of AKI requiring renal replacement therapy and, in some studies, increased mortality in septic patients.15,57 The mechanisms include direct renal tubular toxicity,58 impaired coagulation,59 and accumulation in tissues. Consequently, major regulatory bodies have issued strong warnings against their use in critically ill patients, effectively removing them from the therapeutic arsenal for sepsis.
Human Albumin: Albumin, the body’s natural colloid, stands in stark contrast to its synthetic counterparts. It is responsible for 70–80% of plasma oncotic pressure and has a much longer intravascular half-life than crystalloids (Figure 2).60 Beyond its oncotic function, albumin possesses remarkable pleiotropic properties that make it a uniquely attractive therapeutic agent in sepsis, as detailed in Table 4.
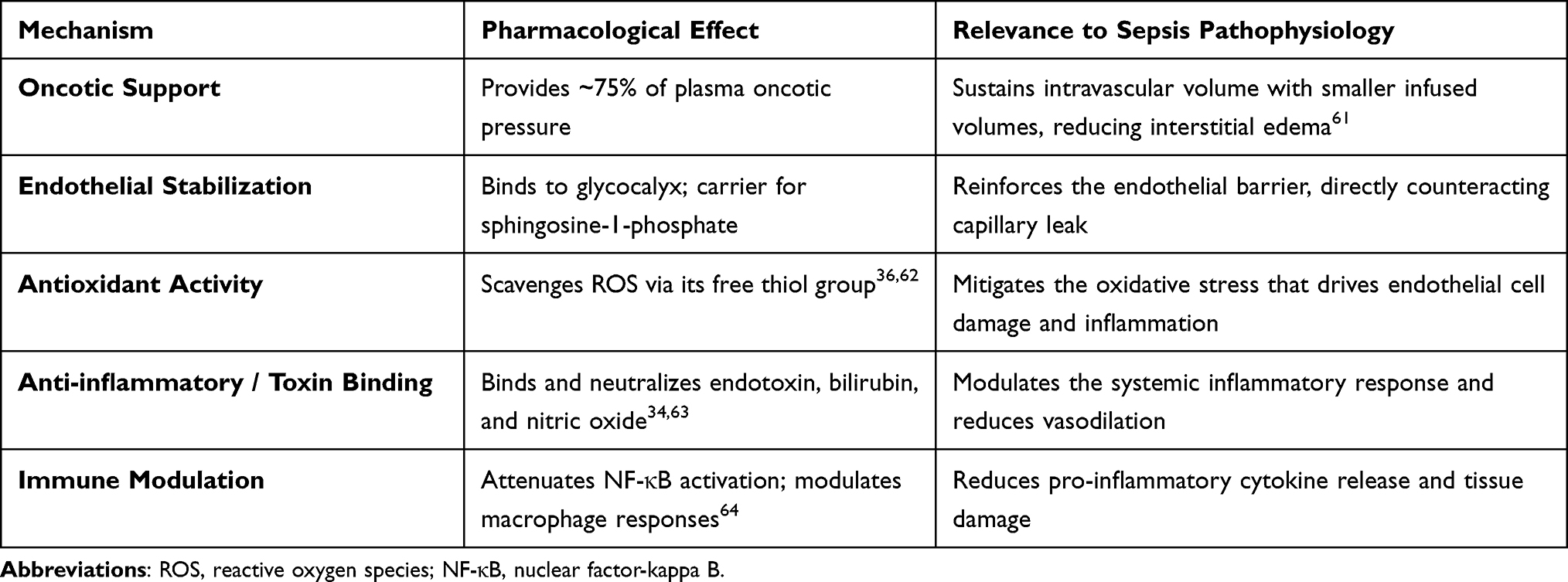 |
Table 4 The Unique Pleiotropic Effects of Albumin in Sepsis |
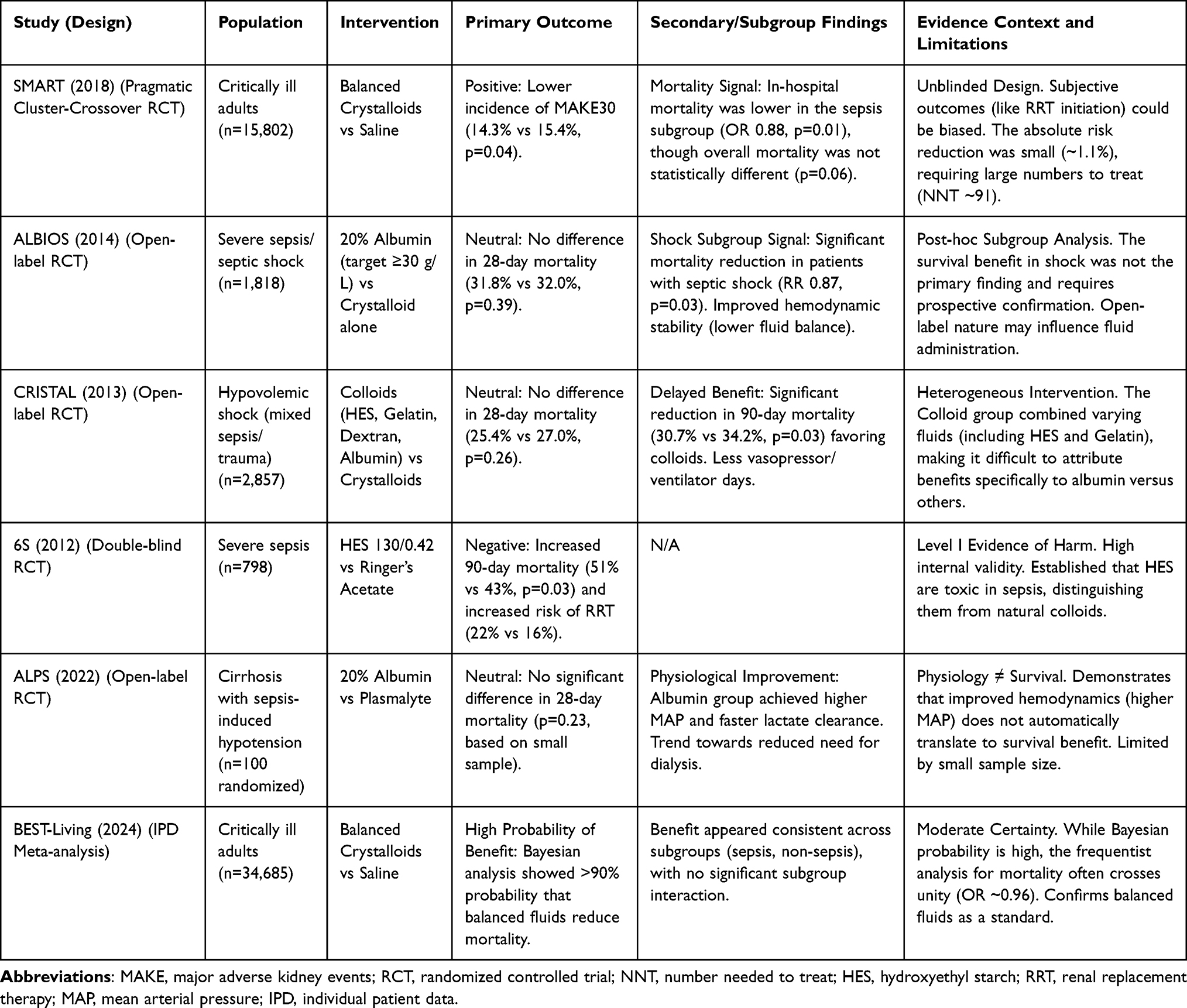 |
Table 5 Summary of Landmark Fluid Trials in Sepsis and Critical Illness |
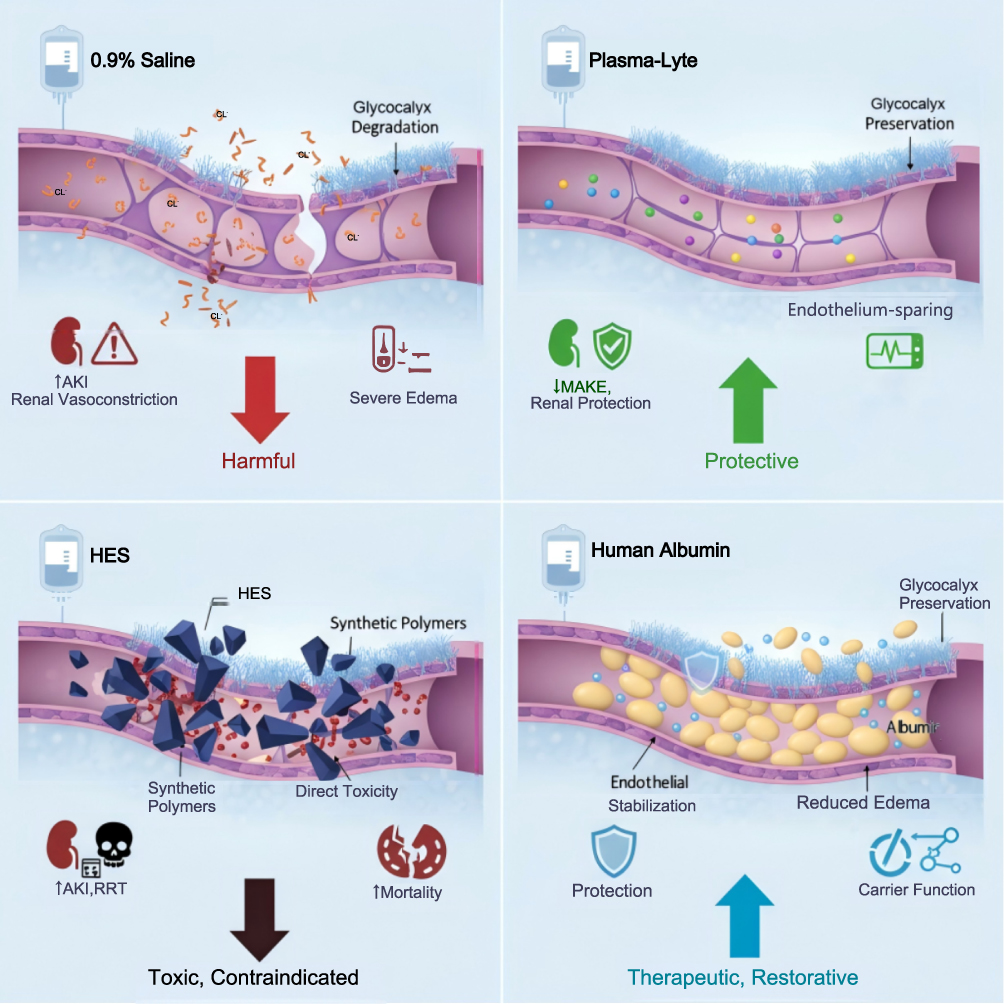 |
Figure 2 Conceptual Schematic of Fluid-Endothelium Interactions. This diagram illustrates the proposed mechanistic effects of resuscitation fluids on the endothelial glycocalyx. Unbalanced crystalloids (0.9% Saline) are depicted as promoting glycocalyx degradation, a mechanism linked in preclinical models to edema and renal injury. Balanced crystalloids support endothelial integrity, aligning with clinical data suggesting reduced renal risks. Synthetic colloids (HES) show direct toxicity and are contraindicated due to proven mortality risks. Human albumin is illustrated providing oncotic support and theoretical endothelial stabilization. Notes: These depictions represent pathophysiological hypotheses. While the physiological rationale is strong, clinical benefits for albumin were primarily observed in septic shock subgroups rather than the overall population in landmark trials like ALBIOS. |
Clinical evidence for albumin remains heterogeneous and subject to ongoing debate. The landmark ALBIOS trial, which randomized 1,818 patients with severe sepsis to receive 20% albumin found no difference in 90-day mortality in the overall population (Table 5). This neutral primary outcome highlights that albumin is not a panacea for all sepsis phenotypes.
Although a prespecified subgroup analysis of patients with septic shock revealed a significant mortality benefit (43.6% vs 49.9%, p = 0.03), this finding represents secondary evidence and must be interpreted with caution.65 The discrepancy between the strong physiological rationale and the mixed clinical results suggests the presence of competing mechanisms. In patients where shock is driven primarily by profound vasoplegia or cellular metabolic dysexecution (cytopathic hypoxia) rather than hypovolemia and capillary leak, albumin’s oncotic benefits may be negligible.
Similarly, the recent ALPS trial in cirrhotic patients with sepsis-induced hypotension found no difference in 28-day mortality, reinforcing the lack of a universal survival benefit, although albumin did improve hemodynamics and lactate clearance.66 Consequently, the PAES framework advocates for a targeted, rather than routine, use of albumin, specifically prioritizing it for the ‘Optimization’ phase in patients with refractory shock who are most likely to benefit from its oncotic and endothelial-protective properties.
Proposal: The Phase-Adapted, Endothelium-Sparing Resuscitation Strategy
The existing evidence compels a move away from a rigid, one-size-fits-all approach to a dynamic, physiologically-driven strategy. We propose the PAES framework, which aligns fluid therapy with the four recognized phases of sepsis resuscitation, integrating the best evidence for fluid choice, volume, and monitoring at each stage. This strategy builds on concepts of fluid responsiveness and deresuscitation, prioritizing endothelial health.
Phase 1: Rescue (0–6 Hours)
The immediate goal is to reverse shock and restore perfusion to vital organs.7 During this phase, patients exhibit significant vasodilation and hypovolemia.
Action: Initial resuscitation should begin with a bolus of balanced crystalloids (eg, 20–30 mL/kg), as recommended by the Surviving Sepsis Campaign. However, subsequent fluid should be administered in smaller, titrated boluses (eg, 250–500 mL) guided by frequent reassessment of fluid responsiveness using dynamic measures, not static pressures like central venous pressure (CVP).41,67
Rationale: Balanced crystalloids provide rapid volume expansion while mitigating the risks of hyperchloremic acidosis associated with saline.50 Early and aggressive use of norepinephrine to maintain a mean arterial pressure (MAP) of ≥65 mmHg is crucial to restore vascular tone and limit the total volume of crystalloid required, preventing unnecessary fluid accumulation.
Phase 2: Optimization (6–24 Hours)
After the initial rescue, the goal shifts from rapid volume loading to carefully optimizing cardiac output and tissue perfusion while actively preventing fluid overload. Many patients will no longer be fluid responsive at this stage.
Action: Fluid administration should be restricted to patients who demonstrate clear evidence of fluid responsiveness. For these patients, titrated balanced crystalloids remain the primary choice. However, this is the critical phase to consider the integration of 20% albumin.68,69 Albumin should be considered in patients with refractory shock requiring escalating vasopressor doses despite initial crystalloid resuscitation, those with documented severe hypoalbuminemia (<25 g/L), or those with emerging evidence of severe capillary leak (eg, high biomarker levels) or peripheral tissue hypoperfusion.70,71
Rationale: In this context, albumin is used not just as a volume expander but as a therapeutic agent to enhance vasopressor sensitivity, stabilize the endothelium, and sustain intravascular volume with a smaller fluid load, as suggested by the ALBIOS septic shock subgroup analysis and the ALPS trial. This “crystalloid-sparing” effect can help limit the accumulation of interstitial edema, and its pleiotropic effects contribute to microvascular integrity.72
Phase 3: Stabilization (24–72 Hours)
By this phase, the acute shock has typically resolved, but the patient remains critically ill with significant organ dysfunction and accumulated tissue edema from the initial resuscitation. The primary goal is to maintain a state of euvolemia.73
Action
All routine “maintenance” intravenous fluids should be ceased. Fluid administration should be limited to that required for medication delivery and enteral nutrition. The target is a neutral or zero cumulative fluid balance.74
Rationale
The focus shifts from “resuscitation” to “support.” Preventing further fluid accumulation is paramount to allow for organ recovery, particularly of the kidneys and lungs. A persistent positive fluid balance in this phase is strongly associated with adverse outcomes, including increased mortality and prolonged mechanical ventilation.12,13
Phase 4: De-Escalation (>72 Hours)
This is the active fluid removal phase, often termed “deresuscitation.” The goal is to achieve a negative fluid balance to mobilize interstitial edema and facilitate liberation from mechanical ventilation and other organ support.75
Action
This phase involves the judicious use of diuretics (eg, furosemide) in patients with adequate renal function or the initiation of renal replacement therapy with ultrafiltration in those with persistent AKI.73,76
Rationale
Mobilizing the “third-spaced” fluid reduces organ congestion, improves pulmonary compliance, and is associated with shorter intensive care unit (ICU) stays and improved survival.13,41 Careful monitoring for hemodynamic tolerance to fluid removal is critical (Figure 3).
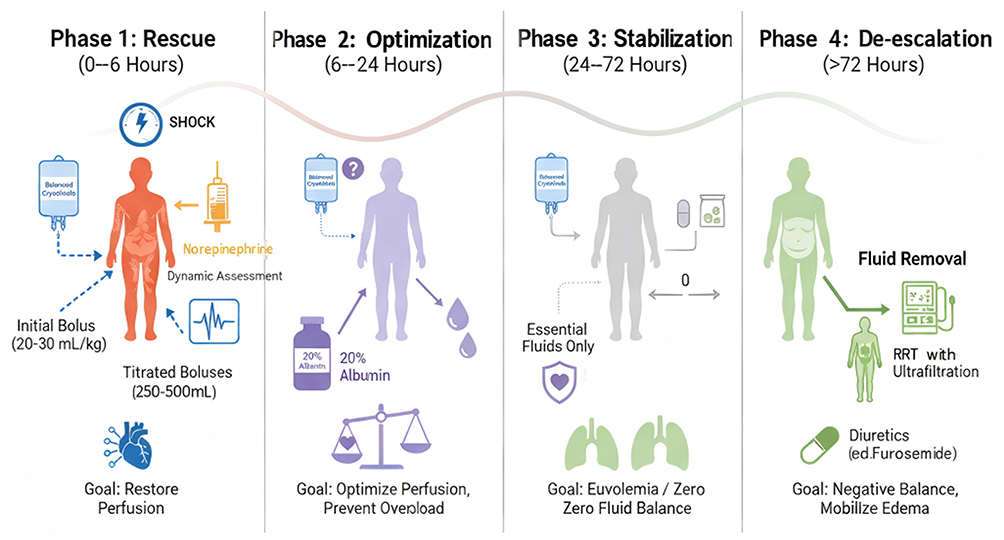 |
Figure 3 The Proposed Phase-Adapted, Endothelium-Sparing (PAES) Resuscitation Strategy. This diagram illustrates a conceptual framework tailoring fluid management to four phases. The Rescue phase (0–6 hours) prioritizes perfusion restoration with balanced crystalloids and early vasopressors. The Optimization phase (6–24 hours) aims to prevent overload, proposing the use of 20% albumin to potentially stabilize the endothelium in specific phenotypes. The Stabilization phase (24–72 hours) targets a zero fluid balance, while the De-escalation phase (>72 hours) focuses on active fluid removal via diuretics or ultrafiltration. Notes: This algorithm integrates physiological principles with current evidence but represents a theoretical proposal for personalized care that requires prospective validation before routine implementation. |
Guiding the PAES Strategy: The Role of Advanced Monitoring and Biomarkers
Implementing the PAES framework effectively requires moving beyond traditional static monitoring and embracing a modern, multimodal approach to assess the patient’s fluid status and endothelial health in real time.
Dynamic Hemodynamic Assessment
Static measures like CVP are notoriously poor predictors of fluid responsiveness. Instead, dynamic assessments that evaluate the heart-lung interaction during mechanical ventilation (eg, stroke volume variation [SVV], pulse pressure variation [PPV]) or simulate a fluid bolus (eg, passive leg raise [PLR]) should be used to guide fluid decisions in the Rescue and Optimization phases.45,67 A positive response (eg, >10–15% increase in stroke volume) indicates that the patient is on the steep part of their Frank-Starling curve and may benefit from further fluid. A negative response signals that further fluid is unlikely to improve cardiac output and will only increase the risk of overload.
Point-of-Care Ultrasound
Point-of-Care Ultrasound (POCUS) has become an indispensable tool at the bedside for guiding fluid therapy.
Fluid Responsiveness
Measurement of the inferior vena cava (IVC) diameter and its respiratory variation can help estimate right atrial pressure and predict fluid responsiveness.77
Fluid Tolerance
Lung ultrasound is highly sensitive for detecting interstitial edema (seen as “B-lines”). The appearance or worsening of B-lines is a strong signal of pulmonary congestion and a clear indication to stop fluid administration.72
Cardiac Function
A focused cardiac ultrasound can rapidly assess left and right ventricular function, identify pre-existing cardiac dysfunction that would predispose to fluid overload, and evaluate the heart’s response to a fluid challenge. POCUS can reduce unnecessary fluid administration and improve adherence to conservative fluid strategies.78
Biomarkers of Endothelial Injury and Capillary Leak
The next frontier in personalizing fluid resuscitation is the integration of biomarkers that directly reflect the state of the endothelium.79 Elevated circulating levels of syndecan-1 are a direct measure of glycocalyx degradation. Angiopoietin-2, a protein released from activated endothelial cells, is a key mediator of vascular destabilization and permeability.80 High levels of these markers can identify patients with the most severe capillary leak and who might benefit most from endothelium-stabilizing therapies like albumin.24,69 While not yet standard practice, these biomarkers hold immense promise for identifying patients at highest risk for harm from aggressive crystalloid resuscitation. Future clinical trials should aim to test biomarker-guided algorithms within the PAES framework.81
Capillary Refill Time
Capillary refill time (CRT) provides a real-time window into the microcirculation, shifting the resuscitation focus from abstract metabolic markers like lactate to tangible end-organ perfusion.82 The landmark ANDROMEDA-SHOCK trial validated this approach, demonstrating that a CRT-targeted strategy reduced organ dysfunction and fluid administration compared to lactate-guided resuscitation. The subsequent ANDROMEDA-SHOCK-2 trial confirmed that a personalized hemodynamic protocol targeting CRT was superior to usual care for a hierarchical composite outcome, primarily by shortening the duration of vital support.83,84
Thus, CRT acts as both a titratable target during the Rescue and Optimization phases and, crucially, a physiological “stop signal” to prevent iatrogenic fluid overload, anchoring the entire framework in the patient’s real-time microcirculatory status.
Limitations, Potential Risks, and Future Directions
The PAES framework offers a physiologically grounded approach to fluid resuscitation; however, several limitations and potential risks must be acknowledged before widespread implementation. First, the strategy relies heavily on accurate phase identification. Phase misclassification poses a significant safety risk: if a clinician incorrectly categorizes a patient in the “Rescue” phase as being in the “Optimization” phase, premature fluid restriction could exacerbate hypoperfusion and precipitate acute kidney injury. Conversely, aggressive deresuscitation in a patient with unresolved hemodynamic instability could lead to recurrent hypotension and organ ischemia.
Second, implementation failures may arise from the framework’s reliance on advanced monitoring. The interpretation of fluid responsiveness and POCUS findings is operator-dependent, and variability in clinician expertise could lead to inconsistent application of the protocol. Finally, it is crucial to distinguish hypothesis from evidence. While individual components of PAES are supported by trials like SMART and ALBIOS, the integrated, multi-stage strategy itself remains a theoretical framework. It represents a proposal for personalization rather than a validated standard of care.
To bridge the gap between this theoretical framework and clinical practice, several key questions remain:
Prospective Validation
The PAES strategy, as a composite intervention, must be tested rigorously in large-scale randomized controlled trials against current standard care to demonstrate its safety and impact on patient-centered outcomes.
Biomarker-Guided Therapy
RCTs are needed to determine if a strategy of administering albumin based on specific biomarker thresholds (eg, syndecan-1 >40 ng/mL or angiopoietin-2 >12 ng/mL) improves outcomes compared to clinical judgment alone.85
Novel Endothelium-Protective Fluids
Research is ongoing into novel fluid formulations that combine volume support with active endothelial repair, such as those containing hyaluronan-based fluids or sphingosine-1-phosphate analogues. These preclinical candidates hold promise for directly targeting glycocalyx repair and reducing microvascular injury.44,86,87
The “Capillary Leak Index”
The development and validation of a composite score that integrates clinical signs of edema, POCUS findings, and multiple biomarkers could provide a more holistic and reliable measure of capillary integrity to guide therapy in real-time.88
Cost-Effectiveness in Resource-Limited Settings
While albumin shows promise, its high cost ($350/L versus $5/L for crystalloids) remains a significant barrier, especially in resource-limited settings.89 Further research on cost-effectiveness and optimal implementation strategies in diverse healthcare environments is crucial.
Variability in Adherence to Protocols: Studies indicate significant variability in clinician adherence to nuanced fluid resuscitation protocols.76 Development of robust educational programs and integration of decision-support systems are vital for successful implementation of strategies like PAES.90
Conclusion
Fluid resuscitation in septic shock is at a critical inflection point. The simplistic debate of crystalloids versus colloids is being replaced by a more sophisticated, physiologically-driven approach centered on the preservation of endothelial function. The PAES strategy offers a pragmatic and evidence-based framework to guide this modern approach. Operationally, this entails prioritizing initial resuscitation with balanced crystalloids, followed by the rational, targeted use of albumin in the optimization phase for the sickest patients, and concluding with dynamic assessment-guided active de-escalation. However, it is important to emphasize that while grounded in current physiological evidence, this framework requires rigorous prospective validation before it is adopted for widespread routine implementation. This strategy seeks to uncouple hemodynamic stabilization from iatrogenic harm. The integration of dynamic hemodynamic monitoring, point-of-care ultrasound, and emerging biomarkers will be essential to personalize this strategy at the bedside. By shifting our focus from merely filling a tank to actively protecting a fragile barrier, we can aspire to a future where fluid resuscitation is not only life-saving but also organ-sparing, ultimately improving the survival and quality of life for patients battling septic shock.
Abbreviations
PAES, Phase-Adapted, Endothelium-Sparing; EGDT, Early Goal-Directed Therapy; AKI, Acute Kidney Injury; HES, Hydroxyethyl Starch; TNF-α, Tumor Necrosis Factor-Alpha; MMPs, Matrix Metalloproteinases; ROS, Reactive Oxygen Species; ESL, Endothelial Surface Layer; IL-6, Interleukin-6; DIC, Disseminated Intravascular Coagulation; NOX, NADPH Oxidase; NF-κB, Nuclear Factor-Kappa B; eNOS, Endothelial Nitric Oxide Synthase; NO, Nitric Oxide; iNOS, Inducible Nitric Oxide Synthase; CVP, Central Venous Pressure; ScvO2, Central Venous Oxygen Saturation; MAP, Mean Arterial Pressure; ICU, Intensive Care Unit; MAKE, Major Adverse Kidney Events; RCTs, Randomized Controlled Trials; IVC, Inferior Vena Cava; POCUS, Point-of-Care Ultrasound; SVV, Stroke Volume Variation; PPV, Pulse Pressure Variation; PLR, Passive Leg Raise; CRT, Capillary Refill Time.
Author Contributions
Bin Li: Conceptualization, Visualization, Methodology, Writing – original draft. Ling Zhao: Conceptualization, Project administration, Methodology, Writing – original draft, Writing – review & editing, Supervision. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The author(s) declare no competing interests.
References
1. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–15. doi:10.1016/S0140-6736(19)32989-7
2. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
3. Joffre J, Hellman J, Ince C, Ait-Oufella H. Endothelial Responses in Sepsis. Am J Respir Crit Care Med. 2020;202(3):361–370. doi:10.1164/rccm.201910-1911TR
4. Smart L, Hughes D. The Effects of Resuscitative Fluid Therapy on the Endothelial Surface Layer. Front Vet Sci. 2021;8:661660. doi:10.3389/fvets.2021.661660
5. Best MW, Jabaley CS. Fluid Management in Septic Shock: a Review of Physiology, Goal-Directed Therapy, Fluid Dose, and Selection. Curr Anesthesiol Rep. 2019;9(2):167–175. doi:10.1007/s40140-019-00330-3
6. Jaffee W, Hodgins S, McGee WT. Tissue Edema, Fluid Balance, and Patient Outcomes in Severe Sepsis: an Organ Systems Review. J Intensive Care Med. 2018;33(9):502–509. doi:10.1177/0885066617742832
7. Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: international Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021;49(11):e1063–e1143. doi:10.1097/CCM.0000000000005337
8. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368–1377. doi:10.1056/NEJMoa010307
9. ProCESS Investigators, Yealy DM, Kellum JA, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370(18):1683–1693.
10. ARISE Investigators; ANZICS Clinical Trials Group, Peake SL, Delaney A, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371(16):1496–1506.
11. Mouncey PR, Osborn TM, Power GS, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372(14):1301–1311. doi:10.1056/NEJMoa1500896
12. Zampieri FG, Bagshaw SM, Semler MW. Fluid Therapy for Critically Ill Adults With Sepsis: a Review. JAMA. 2023;329(22):1967–1980. doi:10.1001/jama.2023.7560
13. Meyhoff TS, Møller MH, Hjortrup PB, et al. Lower vs Higher Fluid Volumes During Initial Management of Sepsis: a Systematic Review With Meta-Analysis and Trial Sequential Analysis. Chest. 2020;157(6):1478–1496. doi:10.1016/j.chest.2019.11.050
14. Lira A, Pinsky MR. Choices in fluid type and volume during resuscitation: impact on patient outcomes. Ann Intensive Care. 2014;4(1):38. doi:10.1186/s13613-014-0038-4
15. Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367(2):124–134. doi:10.1056/NEJMoa1204242
16. Myburgh JA, Finfer S, Bellomo R, et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N Engl J Med. 2012;367(20):1901–1911. doi:10.1056/NEJMoa1209759
17. Daniel M, Bedoui Y, Vagner D, et al. Pathophysiology of Sepsis and Genesis of Septic Shock: the Critical Role of Mesenchymal Stem Cells (MSCs). Int J Mol Sci. 2022;23(16):9274. doi:10.3390/ijms23169274
18. Foote CA, Soares RN, Ramirez-Perez FI, et al. Endothelial Glycocalyx. Compr Physiol. 2022;12(4):3781–3811. doi:10.1002/cphy.c210029
19. Chen L. Glycocalyx in Sepsis Resuscitation. Crit Care Nurs Q. 2016;39(1):38–41. doi:10.1097/CNQ.0000000000000095
20. Martin L, Koczera P, Zechendorf E, et al. The Endothelial Glycocalyx: new Diagnostic and Therapeutic Approaches in Sepsis. BioMed Res Int. 2016;2016:3758278. doi:10.1155/2016/3758278
21. Iba T, Maier CL, Helms J, Ferrer R, Thachil J, Levy JH. Managing sepsis and septic shock in an endothelial glycocalyx-friendly way: from the viewpoint of surviving sepsis campaign guidelines. Ann Intensive Care. 2024;14(1):64. doi:10.1186/s13613-024-01301-6
22. Goligorsky MS, Sun D. Glycocalyx in Endotoxemia and Sepsis. Am J Pathol. 2020;190(4):791–798. doi:10.1016/j.ajpath.2019.06.017
23. Zhan JH, Wei J, Liu YJ, et al. Sepsis-associated endothelial glycocalyx damage: a review of animal models, clinical evidence, and molecular mechanisms. Int J Biol Macromol. 2025;295(Pt 1):139548. doi:10.1016/j.ijbiomac.2025.139548
24. Nelson A, Berkestedt I, Bodelsson M. Circulating syndecan-1 and heparan sulfate in septic shock. Acta Anaesthesiol Scand. 2014;58(4):451–458.
25. Inagawa R, Okada H, Takemura G, et al. Ultrastructural Alteration of Pulmonary Capillary Endothelial Glycocalyx During Endotoxemia. Chest. 2018;154(2):317–325. doi:10.1016/j.chest.2018.03.003
26. McMullan RR, McAuley DF, O’Kane CM, Silversides JA. Vascular leak in sepsis: physiological basis and potential therapeutic advances. Crit Care. 2024;28(1):97. doi:10.1186/s13054-024-04875-6
27. Torres LN, Chung KK, Salgado CL, et al. Low-volume resuscitation with normal saline is associated with microvascular endothelial dysfunction after hemorrhage in rats, compared to colloids and balanced crystalloids. Crit Care. 2017;21(1):174. doi:10.1186/s13054-017-1745-7
28. Hou PC, Filbin MR, Wang H, et al. Endothelial Permeability and Hemostasis in Septic Shock: results From the ProCESS Trial. Chest. 2017;152(1):22–31. doi:10.1016/j.chest.2017.01.010
29. Kolářová H, Ambrůzová B, Svihálková Šindlerová L, et al. Modulation of endothelial glycocalyx structure under inflammatory conditions. Mediators Inflamm. 2014;2014:694312. doi:10.1155/2014/694312
30. Diebel LN, Liberati DM, Martin JV. Acute hyperglycemia increases sepsis related glycocalyx degradation and endothelial cellular injury: a microfluidic study. Am J Surg. 2019;217(6):1076–1082. doi:10.1016/j.amjsurg.2018.12.066
31. Boisramé-Helms J, Kremer H, Schini-Kerth V, Meziani F. Endothelial dysfunction in sepsis. Curr Vasc Pharmacol. 2013;11(2):150–160.
32. Sygitowicz G, Sitkiewicz D. Molecular mechanisms of organ damage in sepsis: an overview. Braz J Infect Dis. 2020;24(6):552–560. doi:10.1016/j.bjid.2020.09.004
33. Girardis M, David S, Ferrer R, et al. Understanding, assessing and treating immune, endothelial and haemostasis dysfunctions in bacterial sepsis. Intensive Care Med. 2024;50(10):1580–1592. doi:10.1007/s00134-024-07586-2
34. Levi M, van der Poll T. Coagulation and sepsis. Thromb Res. 2017;149:38–44. doi:10.1016/j.thromres.2016.11.007
35. Uchimido R, Schmidt EP, Shapiro NI. The glycocalyx: a novel diagnostic and therapeutic target in sepsis. Crit Care. 2019;23(1):16. doi:10.1186/s13054-018-2292-6
36. Bermejo-Martin JF, Martín-Fernandez M, López-Mestanza C, et al. Shared Features of Endothelial Dysfunction between Sepsis and Its Preceding Risk Factors (Aging and Chronic Disease). J Clin Med. 2018;7(11):400. doi:10.3390/jcm7110400
37. Joffre J, Hellman J. Oxidative Stress and Endothelial Dysfunction in Sepsis and Acute Inflammation. Antioxid Redox Signal. 2021;35(15):1291–1307. doi:10.1089/ars.2021.0027
38. Singh J, Lee Y, Kellum JA. A new perspective on NO pathway in sepsis and ADMA lowering as a potential therapeutic approach. Crit Care. 2022;26(1):246. doi:10.1186/s13054-022-04075-0
39. Lambden S. Bench to bedside review: therapeutic modulation of nitric oxide in sepsis-an update. Intensive Care Med Exp. 2019;7(1):64. doi:10.1186/s40635-019-0274-x
40. Pascual-Ramirez J, Koutrouvelis A. The nitric oxide pathway antagonists in septic shock: meta-analysis of controlled clinical trials. J Crit Care. 2019;51:34–38. doi:10.1016/j.jcrc.2019.01.013
41. Ladzinski AT, Thind GS, Siuba MT. Rational Fluid Resuscitation in Sepsis for the Hospitalist: a Narrative Review. Mayo Clin Proc. 2021;96(9):2464–2473. doi:10.1016/j.mayocp.2021.05.020
42. Mekontso Dessap A, AlShamsi F, Belletti A, et al. European Society of Intensive Care Medicine (ESICM) 2025 clinical practice guideline on fluid therapy in adult critically ill patients: part 2-the volume of resuscitation fluids. Intensive Care Med. 2025;51(3):461–477. doi:10.1007/s00134-025-07840-1
43. Graziani M, Gasperini L, Gasperini C, Maraziti G, De Pascale G, Becattini C. Comparison of non-invasive strategies to drive fluid resuscitation in sepsis or septic shock: a meta-analysis of RCTs. Intern Emerg Med. 2025. doi:10.1007/s11739-025-04179-9
44. Ospina-Tascón GA, Hernandez G, Alvarez I, et al. Effects of very early start of norepinephrine in patients with septic shock: a propensity score-based analysis. Crit Care. 2020;24(1):52. doi:10.1186/s13054-020-2756-3
45. Douglas IS, Alapat PM, Corl K, et al. Physiology of fluid responsiveness in sepsis. Am J Respir Crit Care Med. 2019;199(9):P21–P22. doi:10.1164/rccm.19911P21
46. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
47. Smorenberg A, Ince C, Groeneveld AJ. Dose and type of crystalloid fluid therapy in adult hospitalized patients. Perioper Med. 2013;2(1):17. doi:10.1186/2047-0525-2-17
48. Severs D, Hoorn EJ, Rookmaaker MB. A critical appraisal of intravenous fluids: from the physiological basis to clinical evidence. Nephrol Dial Transplant. 2015;30(2):178–187. doi:10.1093/ndt/gfu005
49. Garnacho-Montero J, Fernández-Mondéjar E, Ferrer-Roca R, et al. Crystalloids and colloids in critical patient resuscitation. Med Intensiva. 2015;39(5):306–315.
50. Semler MW, Self WH, Wanderer JP, et al. Balanced Crystalloids versus Saline in Critically Ill Adults. N Engl J Med. 2018;378(9):829–839. doi:10.1056/NEJMoa1711584
51. Byrne L, Van Haren F. Fluid resuscitation in human sepsis: time to rewrite history? Ann Intensive Care. 2017;7(1):4. doi:10.1186/s13613-016-0231-8
52. Douglas JJ, Walley KR. Fluid choices impact outcome in septic shock. Curr Opin Crit Care. 2014;20(4):378–384. doi:10.1097/MCC.0000000000000116
53. Liu C, Mao Z, Hu P, et al. Fluid resuscitation in critically ill patients: a systematic review and network meta-analysis. Ther Clin Risk Manag. 2018;14:1481–1497. doi:10.2147/TCRM.S175080
54. Wang G, Zhang H, Liu D, et al. Resuscitation fluids as drugs: targeting the endothelial glycocalyx. Chin Med J. 2022;135(2):142–151.
55. Chang R, Holcomb JB. Choice of Fluid Therapy in the Initial Management of Sepsis, Severe Sepsis, and Septic Shock. Shock. 2016;46(1):17–26. doi:10.1097/SHK.0000000000000577
56. Zampieri FG, Cavalcanti AB, Di Tanna GL, et al. Balanced crystalloids versus saline for critically ill patients (BEST-Living): a systematic review and individual patient data meta-analysis. Lancet Respir Med. 2024;12(3):237–246. doi:10.1016/S2213-2600(23)00417-4
57. Annane D, Siami S, Jaber S, et al. Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically ill patients presenting with hypovolemic shock: the CRISTAL randomized trial. JAMA. 2013;310(17):1809–1817. doi:10.1001/jama.2013.280502
58. Tseng CH, Chen TT, Wu MY, Chan MC, Shih MC, Tu YK. Resuscitation fluid types in sepsis, surgical, and trauma patients: a systematic review and sequential network meta-analyses. Crit Care. 2020;24(1):693. doi:10.1186/s13054-020-03419-y
59. Krzych ŁJ, Czempik PF. Effect of fluid resuscitation with balanced solutions on platelets: in vitro simulation of 20% volume substitution. Cardiol J. 2018;25(2):191–196.
60. Heshmati SM, Ebrahimi A, Rasouli HR. Fluid resuscitation, which fluid is the best for each patient? A systematic review and meta analysis. Iran Red Crescent Med J. 2017;19(3):e41729.
61. Wiedermann CJ. Moderator Effect of Hypoalbuminemia in Volume Resuscitation and Plasma Expansion with Intravenous Albumin Solution. Int J Mol Sci. 2022;23(22):14175. doi:10.3390/ijms232214175
62. Oudemans-van Straaten HM, Ostermann M, Schetz M. Plasma-free sulfhydryl groups, antioxidants, and endothelial dysfunction in sepsis and septic shock. J Crit Care. 2011;26(4):
63. Vincent JL, De Backer D, Wiedermann CJ. Fluid management in sepsis: the potential beneficial effects of albumin. J Crit Care. 2016;35:161–167. doi:10.1016/j.jcrc.2016.04.019
64. Dubick MA, Gibson RS, Barr JL, et al. Evaluation of resuscitation fluids for maintaining human endothelial cell antioxidant status in vitro. FASEB J. 2016;30(S1):
65. Caironi P, Tognoni G, Masson S, et al. Albumin replacement in patients with severe sepsis or septic shock. N Engl J Med. 2014;370(15):1412–1421. doi:10.1056/NEJMoa1305727
66. Maiwall R, Kumar A, Pasupuleti SSR, et al. A randomized-controlled trial comparing 20% albumin to plasmalyte in patients with cirrhosis and sepsis-induced hypotension [Alps trial]. J Hepatol. 2022;77(3):670–682. doi:10.1016/j.jhep.2022.03.043
67. Monnet X, Marik P, Teboul JL. Passive leg raising for predicting fluid responsiveness: a systematic review and meta-analysis. Intensive Care Med. 2016;42(12):1935–1947. doi:10.1007/s00134-015-4134-1
68. Cusack RAF, Rodríguez A, Cantan B, et al. Microcirculation properties of 20% albumin in sepsis; a randomised controlled trial. J Crit Care. 2025;87:155039. doi:10.1016/j.jcrc.2025.155039
69. Wiedermann CJ. Phases of fluid management and the roles of human albumin solution in perioperative and critically ill patients. Curr Med Res Opin. 2020;36(12):1961–1973. doi:10.1080/03007995.2020.1840970
70. Patel S, Green A, Wolfe Y, et al. The Impact of Positive Fluid Balance on Sepsis Subtypes: a Causal Inference Study. Crit Care Res Pract. 2023;2023:2081588. doi:10.1155/2023/2081588
71. Gabarre P, Desnos C, Morin A, et al. Albumin versus saline infusion for sepsis-related peripheral tissue hypoperfusion: a proof-of-concept prospective study. Crit Care. 2024;28(1):43. doi:10.1186/s13054-024-04827-0
72. Juffermans NP, van den Brom CE, Kleinveld DJB. Targeting Endothelial Dysfunction in Acute Critical Illness to Reduce Organ Failure. Anesth Analg. 2020;131(6):1708–1720. doi:10.1213/ANE.0000000000005023
73. Ostermann M, Alshamsi F, Artigas Raventos A, et al. European Society of Intensive Care Medicine Clinical Practice Guideline on fluid therapy in adult critically ill patients: part 3-fluid removal at de-escalation phase. Intensive Care Med. 2025;51(10):1749–1763. doi:10.1007/s00134-025-08058-x
74. Bakker J, Kattan E, Annane D, et al. Current practice and evolving concepts in septic shock resuscitation. Intensive Care Med. 2022;48(2):148–163. doi:10.1007/s00134-021-06595-9
75. Silversides JA, Major E, Ferguson AJ, et al. Conservative fluid management or liberal fluid management for critically ill adults with sepsis or septic shock. Cochrane Database Syst Rev. 2022;4(4):CD012894.
76. Ravi C, Johnson DW. Optimizing Fluid Resuscitation and Preventing Fluid Overload in Patients with Septic Shock. Semin Respir Crit Care Med. 2021;42(5):698–705. doi:10.1055/s-0041-1733898
77. Kaselitz TB, Seymour CW. Point-of-Care Ultrasound in Sepsis and Septic Shock. JAMA. 2025;333(19):1720–1721. doi:10.1001/jama.2025.1983
78. Boyd JH, Sirounis D, Maizel J, Slama M. Echocardiography as a guide for fluid management. Crit Care. 2016;20(1):274. doi:10.1186/s13054-016-1407-1
79. Wong HR, Lindsell CJ. An Enrichment Strategy For Sepsis Clinical Trials. Shock. 2016;46(6):632–634. doi:10.1097/SHK.0000000000000693
80. Sela DP, Raman S, Obonyo NG, et al. Resuscitation-associated endotheliopathy (RAsE): a conceptual framework based on a systematic review and meta-analysis. Syst Rev. 2023;12(1):236. doi:10.1186/s13643-023-02406-y
81. Sharawy N, Lehmann C. New directions for sepsis and septic shock research. J Surg Res. 2015;194(2):339–346. doi:10.1016/j.jss.2014.12.014
82. Hernandez G, Carmona P, Ait-Oufella H. Monitoring capillary refill time in septic shock. Intensive Care Med. 2024;50(4):580–582. doi:10.1007/s00134-024-07361-3
83. Hernández G, Ospina-Tascón GA, Damiani LP, et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: the ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA. 2019;321(7):654–664. doi:10.1001/jama.2019.0071
84. ANDROMEDA-SHOCK-2 Investigators for the ANDROMEDA Research Network, Spanish Society of Anesthesiology, Reanimation and Pain Therapy (SEDAR), and Latin American Intensive Care Network (LIVEN), Hernandez G, Ospina-Tascón GA, Ospina-Tascón GA, et al. Personalized Hemodynamic Resuscitation Targeting Capillary Refill Time in Early Septic Shock: the ANDROMEDA-SHOCK-2 Randomized Clinical Trial. JAMA. 2025;334(22):1988–1999. doi:10.1001/jama.2025.20402.
85. Fernández-Sarmiento J, Molina CF, Salazar-Pelaez LM, et al. Biomarkers of Glycocalyx Injury and Endothelial Activation are Associated with Clinical Outcomes in Patients with Sepsis: a Systematic Review and Meta-Analysis. J Intensive Care Med. 2023;38(1):95–105. doi:10.1177/08850666221109186
86. Edwards TH, Hoareau GL. Fluids of the Future. Front Vet Sci. 2020;7:623227. doi:10.3389/fvets.2020.623227
87. Joannes-Boyau O, Le Conte P, Bonnet MP, et al. Guidelines for the choice of intravenous fluids for vascular filling in critically ill patients, 2021. Anaesth Crit Care Pain Med. 2022;41(3):101058. doi:10.1016/j.accpm.2022.101058
88. Ramasco F, Nieves-Alonso J, García-Villabona E, et al. Challenges in Septic Shock: from New Hemodynamics to Blood Purification Therapies. J Pers Med. 2024;14(2):176. doi:10.3390/jpm14020176
89. Tigabu BM, Davari M, Kebriaeezadeh A, et al. A Cost-effectiveness Analysis of Albumin in Septic Shock: a Patient-level Data Analysis. Clin Ther. 2019;41(11):2297–2307.e2. doi:10.1016/j.clinthera.2019.08.023
90. Aboodi MS, Chen J, Hope AA, et al. Exploring the clinical decision-making process in approaches to fluid resuscitation and vasopressor administration in septic shock: a qualitative think-aloud study. Am J Respir Crit Care Med. 2019;199(9):A7034.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Timing of Core Sepsis Bundle Elements Initiation in Critically Ill Patients: A Multicenter Target Trial Emulation Study
Li M, Zhang J, Huang H, Li J, Zhang B, Zhao S, Peng Z, Han S, Guan J, Yang J, Wang G, Chang Y, Chang P, Yu Z, Zhong T, Liu Z
Clinical Epidemiology 2026, 18:588212
Published Date: 23 January 2026