")
Back to Journals » Patient Related Outcome Measures » Volume 14
The Transthyretin Amyloidosis – Quality of Life (ATTR-QOL) Questionnaire: Development of a Conceptual Model and Disease-Specific Patient-Reported Outcome Measure
Authors O'Connor M , Hsu K, Broderick L , McCausland KL, LaGasse K, Rebello S, Carty M, Lousada I
Received 30 March 2023
Accepted for publication 27 June 2023
Published 7 July 2023 Volume 2023:14 Pages 213—222
DOI https://doi.org/10.2147/PROM.S411721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Meaghan O’Connor,1 Kristen Hsu,2 Lynne Broderick,1 Kristen L McCausland,1 Kaitlin LaGasse,1 Sabrina Rebello,2 Michelle Carty,1 Isabelle Lousada2
1QualityMetric Incorporated LLC, Johnston, RI, USA; 2Amyloidosis Research Consortium, Newton, MA, USA
Correspondence: Kristen Hsu, Amyloidosis Research Consortium, 320 Nevada Street, Suite 210, Newton, MA, 02460, USA, Tel +1-617-467-5170, Email [email protected]
Purpose: Patients with transthyretin amyloidosis (ATTR) experience a wide variety of symptoms and impacts on health-related quality of life (HRQoL). However, the lack of an ATTR-specific patient-reported outcome (PRO) measure has made consistent measurement of HRQoL in ATTR challenging. This paper describes the development of a conceptual model and subsequent content for the Transthyretin Amyloidosis – Quality of Life Questionnaire (ATTR-QOL), an ATTR-specific PRO measure.
Methods: This was a cross-sectional, non-interventional, US-based study. The study design included three stages: 1) a targeted literature review followed by qualitative data collection with patients and experts; 2) development of a conceptual model and PRO measure; and 3) review of the PRO measure using a modified Delphi method, translatability assessment, and interviews with patients and experts. Revisions were made to the measure after each round of review.
Results: Forty-four patients and 29 experts participated in this study. The conceptual model included two primary concepts of interest: symptoms (cardiac, neuropathic–peripheral, neuropathic–autonomic, and other) and impacts (eg, physical, role, and mental/emotional functioning). Seventy-two items were created (32 symptoms; 40 impacts) to align with the model. A recall period of one month was selected based on participant input.
Conclusion: The ATTR-QOL was created with significant patient involvement and guidance from a multidisciplinary group of experts. The mix of patient and clinical perspectives helped to ensure a balanced representation of all relevant disease experiences and clinical specialties. With further refinement from psychometric testing, the ATTR-QOL will provide a standard, comprehensive measure for all ATTR-specific research including both clinical trials and clinical practice.
Keywords: content validity, cardiomyopathy, polyneuropathy, qualitative, clinical outcome assessment
Introduction
Transthyretin amyloidosis (ATTR) is a rare, debilitating disease caused by deposits of misfolded transthyretin proteins in organ systems. There are two types of ATTR: hereditary and wild-type.1 Hereditary ATTR (hATTR or ATTRv) includes more than 120 genotypes and can be further subtyped into cardiomyopathy (hATTR-CM) and polyneuropathy (hATTR-PN) based on the primary organ systems affected.2 The most commonly observed genotype worldwide, V30M, is primarily associated with symptoms of polyneuropathy and was first described in a population of patients in Portugal.3–5 The most commonly observed genotype in the United States, V122I, is typically found in African Americans and is primarily associated with symptoms of cardiomyopathy.4,6,7 It should be noted that as research continues and more variants are better understood, evidence suggests that patients with hATTR may also experience ocular and/or central nervous system involvement.8–10 Wild-type ATTR (ATTRwt) is not caused by any of the known genetic mutations; rather, it typically develops in older age and most often results in cardiomyopathy. Regardless of type, the clinical presentation of ATTR is complex: patients experience a wide variety of symptoms,11–16 and, in turn, many impacts on daily life, including on work, healthcare resource utilization, and overall health-related quality of life (HRQoL).14,17–19
A 2018 multidisciplinary stakeholder meeting hosted by the Amyloidosis Research Consortium (ARC) identified the need for improved understanding and measurement of HRQoL in ATTR as an important research priority in this disease area.20 To date, the lack of an ATTR-specific patient-reported outcome (PRO) measure has hindered the ATTR community’s ability to measure HRQoL in a consistent, comprehensive way. Clinicians, researchers, drug developers, regulatory bodies, and payer evaluation organizations have relied on a combination of PRO measures intended for other conditions to measure symptoms, impacts, and overall HRQoL (eg, Norfolk-QOL-Diabetic Neuropathy, COMPASS-31, Kansas City Cardiomyopathy Questionnaire [KCCQ], SF-36).21 While these instruments have value for the research and treatment of ATTR, the lack of specific attribution to the disease results in gaps in knowledge. Recognizing this need, ARC initiated the development of an ATTR-specific patient-reported outcome (PRO) measure to reflect the patient experience of ATTR and cover the “constellation of symptoms”11 and impacts experienced by ATTR patients that can be a standard measure for all ATTR-specific research (to allow for comparison across studies) and is appropriate for use in both clinical trials and clinical practice. This paper describes the development of a conceptual model of the patient experience of ATTR and PRO measure to evaluate that experience, the Transthyretin Amyloidosis – Quality of Life Questionnaire (ATTR-QOL).
Materials and Methods
This cross-sectional, non-interventional, US-based study was designed with 3 stages that included a targeted literature review, concept elicitation with experts and patients, conceptual model and PRO measure development, and evaluation of the content validity of the measure (Figure 1). Prior to commencing the research, the study team formed a steering committee of 8 experts in ATTR (clinicians, patient representatives) to provide insight throughout the development process. This study complies with the Declaration of Helsinki; ethics approval was granted by the WCG Institutional Review Board (#120190335; #20202560).
 |
Figure 1 Study design. |
Stage 1: July 2019–January 2020
A targeted literature review based on records identified in the PubMed and ClinicalTrials.gov databases was conducted to identify the signs, symptoms, and impacts of ATTR and PRO measures commonly used in ATTR studies. The study team identified and extracted data from 26 peer-reviewed articles published between August 2009 and August 2019. Results from the literature review were used to develop a symptom list and a semi-structured interview guide for use in 60-minute, one-on-one interviews with experts in ATTR.
Experts in ATTR, including specialists that commonly treat ATTR (including cardiologists, neurologists, gastroenterologists), researchers, and patient representatives, were recruited using purposive sampling, with the goal of including a mix of clinical perspectives. During interviews, the experts reviewed the symptom list, providing input on wording, organization, and content; discussed the impacts of living with ATTR; and considered other elements of a PRO measure (eg, length of the questionnaire, ideal response options). The interviews were audio-recorded and transcribed verbatim. Two members of the study team (MO’C, LB) conducted the interviews and later coded and analyzed the interview transcripts in NVivo software to identify signs, symptoms, and impacts of ATTR and suggested elements of the PRO measure such as a recall period and mode of administration. These results, along with items from the content-validated ATTR Amyloidosis Patient Symptom Survey (ATTR-PSS),22 which was incorporated into this study, were used to update the symptom list and develop a semi-structured moderator/interview guide for use in a focus group and individual interviews with patients with ATTR.
Participants (ie, US-based adults with hATTR or ATTRwt) were recruited for the patient focus group and individual interviews using purposive sampling, leveraging ARC’s existing networks. The study team aimed for a sample with representation from patients with hATTR-CM, hATTR-PN, and ATTRwt to capture the different experiences of the disease. All participants reviewed and signed a consent form prior to being interviewed.
An in-person, 90-minute patient focus group was conducted at the October 2019 Amyloidosis Support Groups (ASG) ATTR-specific meeting in Chicago, USA. Subsequent individual interviews were conducted remotely using web-based teleconferencing software, allowing for greater geographic diversity. The focus group and interviews were moderated by 2 members of the study team (MO’C, LB). During both the focus group and individual interviews, participants completed and discussed the symptom list and described the impacts of their condition on daily life. The focus group and interviews were audio recorded and transcribed verbatim. Two members of the study team (MO’C, LB) coded and analyzed the transcripts with a focus on confirming and elaborating on the symptoms and impacts identified in the clinician interviews and identifying patient preferences regarding other elements of a PRO (eg, recall period, ideal mode and setting to complete the questionnaire). Because the focus group was conducted first, results from the focus group were used to update the symptom list and adapt the semi-structured interview guide for use in individual interviews. A saturation analysis determined that the patient sample size was sufficient prior to closing patient data collection.
Stage 2: February–April 2020
Findings from Stage 1 were used to develop a conceptual model and items and instructions for the draft measure, and to select an appropriate recall period and item response options. Given the interest in using the ATTR-QOL to help guide treatment decisions (including supportive therapy), the domains and subdomains of the conceptual model were organized according to specific groups of symptoms and impacts that a patient with ATTR may experience. Given the interest in making the ATTR-QOL relevant for both clinical practice and clinical trials, the initial list of items focused on the concepts in the model that could be considered more proximal to the condition of ATTR (ie, the aspects of disease most important to measure and track within these contexts). All items were drafted in US-English.
Stage 3: April 2020–June 2021
The draft measure was reviewed and refined through 2 rounds of a modified Delphi method, 2 rounds of translatability assessment (to explore the suitability of the instrument for translation into other languages), informal interviews with drug developers working in ATTR (to ensure the inclusion of the clinical trial perspective), and formal cognitive debriefing interviews with patients with ATTR.
The 2 rounds of modified Delphi method aimed to collect feedback on the draft measure from experts (including the project steering committee [rounds 1 and 2] and other clinicians and patient representatives [round 2]) with extensive experience in ATTR. Participants, recruited by email using purposive sampling, joined an introductory webinar to learn more about the project and their task and receive a guidance document, the draft measure, and a link to an online survey to submit their feedback. Following the first modified Delphi round, 2 members of the study team (MC, MO’C) conducted informal interviews with drug developers working in ATTR; after the second round, those same developers were given the opportunity to provide feedback through a modified version of the online survey used for the Delphi participants. The study team analyzed the responses from the online surveys using descriptive statistics or thematic coding and analysis, depending on the question type. Notes from the informal interviews were also analyzed using thematic analysis. During analysis, the study team discussed conflicting feedback at length before concluding whether to implement suggested changes to the items.
Two translatability assessments of the items and instructions were conducted for 7 languages: French, German, Italian, Japanese, Portuguese, Spanish and Swedish. Translation experts evaluated the difficulty of translating the draft measure into each target language using a standardized scale. An initial translatability assessment occurred following the first Delphi process; updates were made to improve readability and ease of translation. A final translatability assessment was conducted after the second modified Delphi modified/informal drug developer reviews. Revisions were made following each assessment.
Two members of the study team (MO’C, LB) conducted 75-minute, individual cognitive debriefing interviews with patients with ATTR by phone or webcam. Patients were recruited using purposive sampling through messaging on ARC’s media channels and follow-up with patients who expressed interest during Stage 1 of the research. All participants reviewed and signed a consent form prior to being interviewed. Interviews followed a semi-structured interview guide designed to assess the relevance, comprehensibility, and comprehensiveness of the ATTR-QOL.23–25 Participants completed the draft ATTR-QOL using the think-aloud method (a standardized approach to cognitive debriefing that reduces interviewer bias and provides important insights into participant comprehension)26 and then answered a series of pre-determined questions and ad hoc probes. Interviews were audio-recorded and transcribed verbatim. Two members of the study team (MO’C, LB) coded the transcripts in NVivo software and used thematic analysis to identify any parts of the ATTR-QOL that required revisions.
Throughout Stage 3, the ATTR-QOL items and instructions were revised (based on analyses) for readability and/or understandability. An item tracking matrix documented the progression of items and instructions from initial through final versions.
Results
Study Participants
A total of 44 patients and 29 experts participated in this study from Stage 1 through Stage 3 (Table 1 and Table 2).
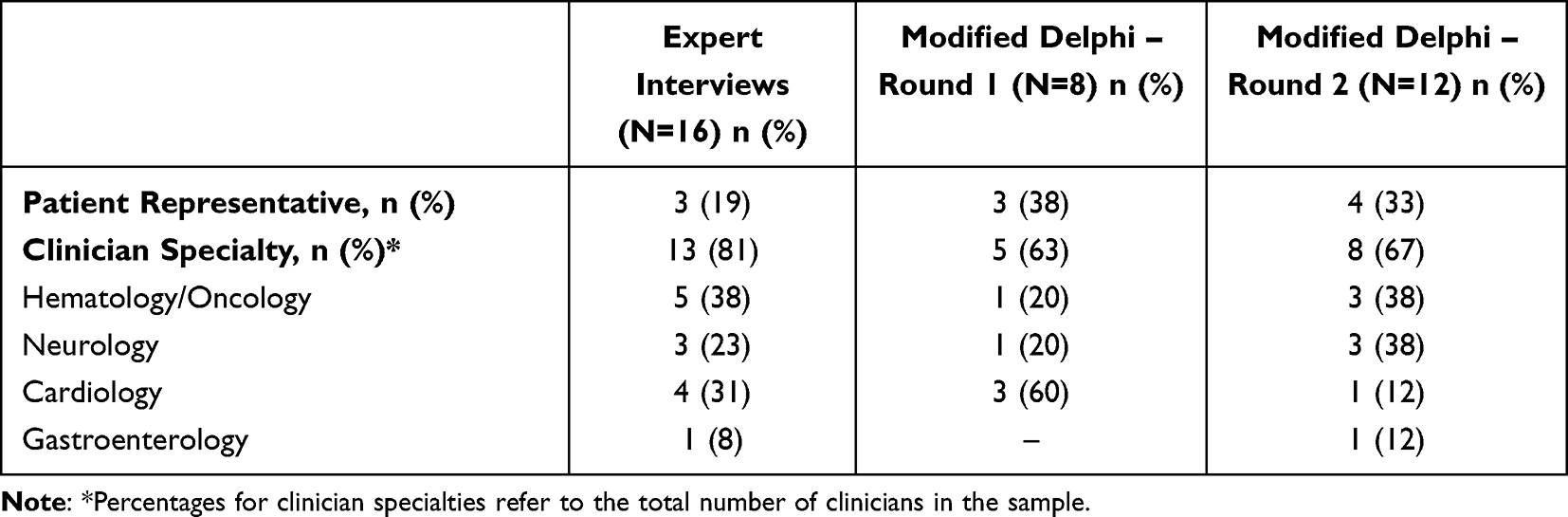 |
Table 1 Expert Participants by Data Collection Mode |
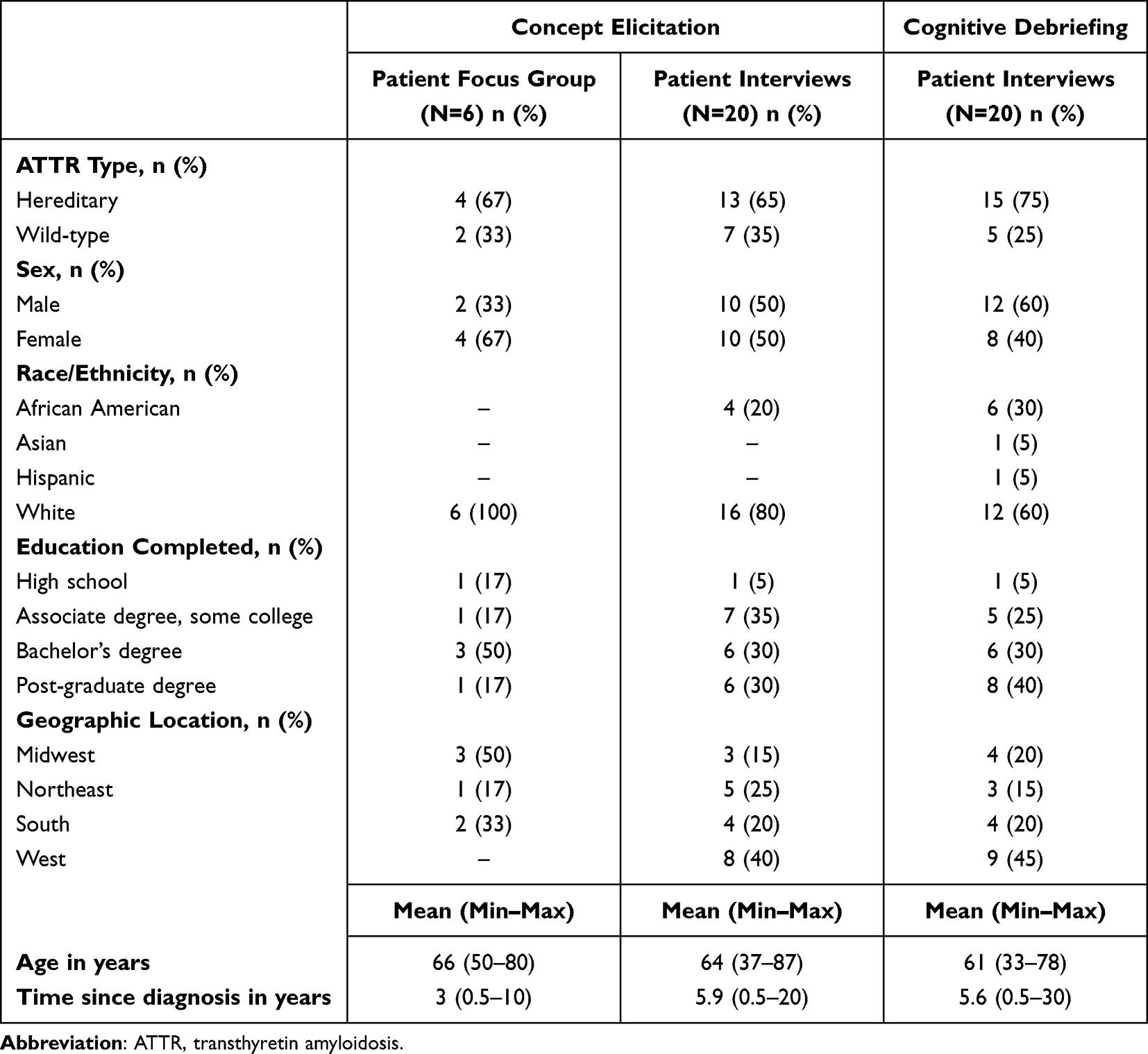 |
Table 2 Patient Participants by Data Collection Mode |
Stage 1
Based on data extracted from the literature review, the study team developed a list of 23 symptoms of ATTR and identified three areas of daily life typically impacted by the disease: physical health, emotional health, and work/productivity. The study team also identified 10 PRO measures that have been used in ATTR-related research.
Sixteen experts (clinicians, n=13; patient representatives, n=3), participated in concept elicitation interviews, confirming the relevance of the symptom list (with some suggestions for more patient-friendly language) and recommending the addition of several others. Experts confirmed impacts on the aforementioned three areas of patients’ lives, and added impacts on social life, independence, finances.
Six patients with ATTR (hATTR, n=4; ATTRwt, n=2) participated in the concept elicitation focus group, confirming the updated list of symptoms (informed by the ATTR-PSS), and highlighting 4 areas of daily life impacted by ATTR: physical functioning, mental health/emotional wellbeing, social life, and finances.
Twenty patients with ATTR (hATTR, n=13; ATTRwt, n=7) participated in individual concept elicitation interviews, confirming and elaborating on the findings from the focus group. Results from the individual interviews informed revisions to a handful of items on the symptom list—primarily to make the word choice more patient-friendly—and 2 additional areas of daily life impacted by ATTR: pastimes and planning.
Each group of participants also discussed their preferences for various elements of an ATTR-specific PRO measure, such as recall period, response options, and mode of administration. For example, a recall period of 4 weeks was identified as appropriate as both clinicians and patients agreed that ATTR symptoms do not fluctuate a lot over time and that 4 weeks would be a reasonable amount of time to remember accurately.
Although the initial study design allowed for the possibility of developing a measure for each type of ATTR, expert and patient feedback suggested that 1 PRO measure, with items addressing the full spectrum of symptoms and impacts across types and subtypes, could adequately cover both hATTR and ATTRwt.
Stage 2
Using findings from Stage 1, the draft conceptual model was designed with 2 components, (1) Symptoms and comorbidities, and (2) Impacts, under which were organized more specific domains (eg, cardiac symptoms, neuropathic symptoms, physical impacts, role impacts).
Guided by the conceptual model, the draft set of items generated for the ATTR-QOL included 34 items assessing frequency and severity of symptoms; 40 items assessing the degree to which respondents felt their everyday life was impacted by ATTR; and 11 possible comorbidities. Likert-like scale response options and a 4-week recall period were used for all symptom and impact items.
Stage 3
After each round of review conducted during Stage 3, items were revised or removed based on participant feedback (Figure 2).
 |
Figure 2 Example of item modification process. |
Eight experts (comprising the project steering committee) participated in the first round of the modified Delphi. Based on participant feedback, 7 items in the questionnaire were changed to clarify or improve readability. Twenty patients with ATTR participated in cognitive debriefing interviews. Participants clearly understood both the symptom and impact items and were able to answer them using the provided response options. Based on participant feedback, 7 items were revised to improve wording and 3 items were removed. For example, 1 symptom (“stress related to ATTR”) was removed because of participant feedback that this was not a symptom of ATTR, rather, a result of having a rare condition with few treatment options. Cognitive debriefing further confirmed the instructions were clear and that the recall period was appropriate. Twelve experts, including a mix of clinicians (n=8) and patient representatives (n=4), participated in the second modified Delphi process. Participants found the items comprehensive. Minor modifications were implemented based on participant feedback (eg, updated item wording and removal of redundant items). No items were revised based on the initial translatability assessment, but further detail or clarification was added to a list of concepts for future translations of the items and instructions. The follow-up translatability assessment resulted in the revision of one item.
Final Conceptual Model and ATTR-QOL
The final conceptual model includes 12 groups of specific health experiences comprising 7 health concepts (cardiac, neuropathic – peripheral, neuropathic – autonomic, and other; physical, role, and mental/emotional) that define 2 concepts of interest (symptoms, impacts) (Figure 3).
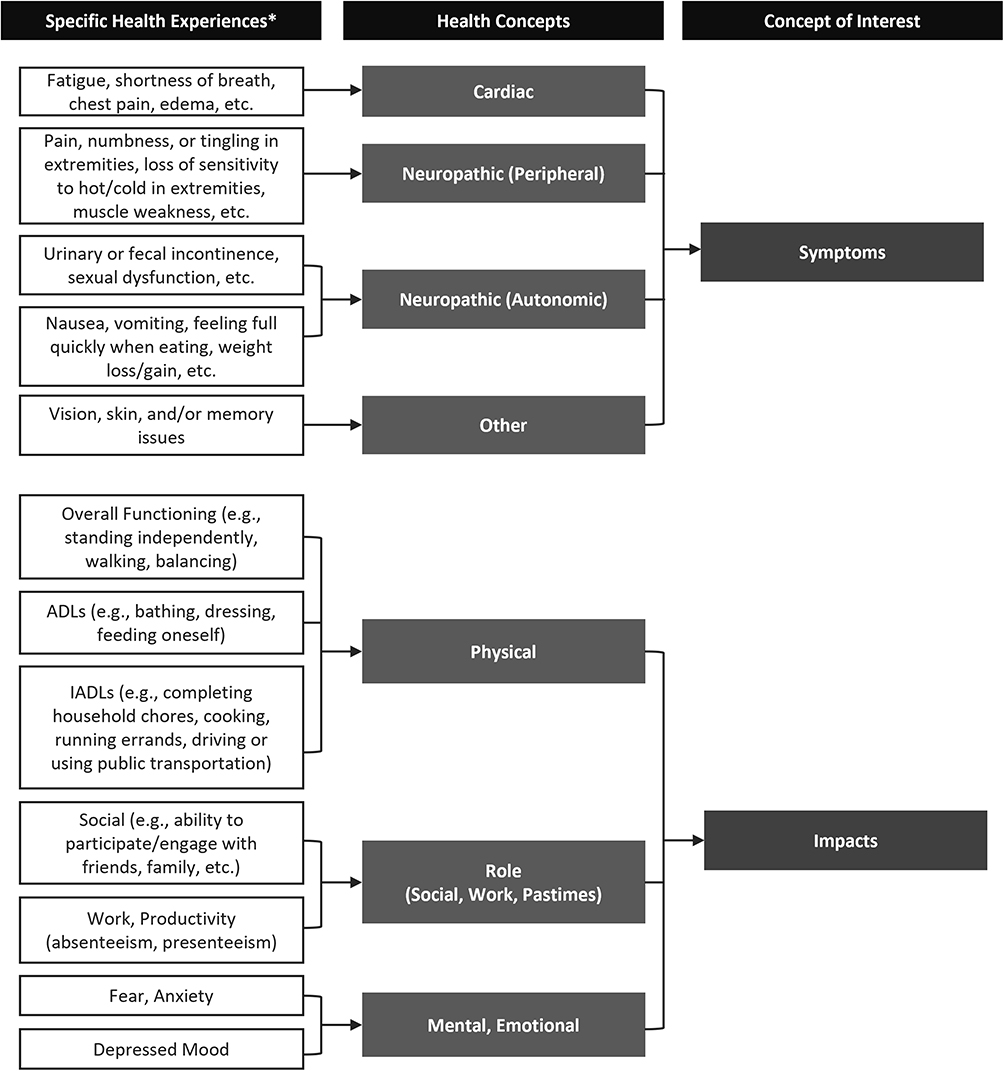 |
Figure 3 Conceptual model for the ATTR-QOL. *Health experiences listed are not exhaustive. Abbreviations: ADLs, activities of daily living; IADLs, instrumental activities of daily living. |
The final set of items generated for the ATTR-QOL reflects the specific health experiences outlined in the conceptual model. Thirty-two items provide coverage of the symptom-specific concepts of interest; respondents are asked to indicate the frequency (“never”, “rarely”, “sometimes”, “often”, and “always”) and severity (“not applicable”, “mild”, “moderate”, and “severe”) of those 32 symptoms in the past 4 weeks. A single item asks about unintentional weight loss or gain over the past 12 months.
The remaining 40 items provide coverage of the impact-specific concepts of interest, including items focused on impacts of ATTR on physical function (balance, gross and fine motor function, activities of daily living [ADLs], instrumental activities of daily living [IADLs]), social life, mental health, and work and productivity. Most of the items share an item stem that ensures attribution to ATTR (eg, “In the past 4 weeks, how much has ATTR impacted your ability to…”). Excepting 1 question which asks about the respondent’s employment status, all impact items are answered on a 5-point scale (“not at all”, “a little”, “some”, “a lot”, and “completely; I cannot do it at all” or “extremely”, depending on the item).
Two optional sets of items are also included: one asking the patient to identify which type of ATTR they have, and 1 asking the patient to identify which of 11 common comorbidities they have experienced at any time. These items can be included at the discretion of the administrator, depending on what information is already known about the patient’s medical history.
Discussion/Conclusion
The ATTR-QOL, developed and refined based on expert and patient feedback, represents an important step forward in patient-centered care and research in ATTR. While continued research into biomarkers that can indicate disease presence and track disease progression is essential, equally important is the need for an instrument that captures the patient's experience of this rare disease. The comprehensive list of symptoms in the ATTR-QOL addresses the different ways that the disease manifests—from those indicative of cardiac involvement to those specific to peripheral and autonomic neuropathy—regardless of ATTR type, allowing for the use of one measure across ATTR types and symptomatology. Items addressing the HRQoL impacts touch on key aspects of daily life that patients and experts agree are influenced by ATTR, including everything from physical functioning to work and productivity to mental health.
The strengths of this study include its alignment with the recommendations and standards set forth by key regulatory bodies (eg, US FDA, EMA) and thought leaders (eg, ISOQOL, PROTEUS Consortium) for PRO measure development; significant patient involvement at each step of the process; input and guidance from a multidisciplinary group of experts, ensuring a balanced representation of all relevant clinical specialties; and a resulting PRO measure useful across ATTR types and primary symptomatology.
This study emphasized the inclusion of patient input through the use of recommended qualitative research methods that ensure the centrality of the patient voice.23,27,28 Concept elicitation, the approach used in the focus group and first set of expert and patient interviews, uses phenomenological inquiry, or open-ended questions, to extract patient descriptions of the symptoms, impacts, and other aspects of their condition.29 Using data generated from concept elicitation interviews as well as the ATTR-PSS, also developed using extensive patient input, to inform PRO measure-development ensures that the patient's voice and experience is at the foundation of the instrument. Cognitive debriefing—a qualitative approach used during PRO measure evaluation—aims to assess patient understanding of all aspects of a measure as well as evaluate the relevance and importance of each item in relation to the experience of the patient.23,30,31 Ultimately, the results of cognitive debriefing can be used to determine whether a specific instrument can be considered “fit for purpose” within a specific population.31
In addition to incorporating the patient voice, the study team deliberately sought input from a multidisciplinary group of experts, ensuring that no one clinical specialty or perspective could dominate, and the resulting items could be useful across ATTR type and purposes (eg, clinical practice or clinical trials). The mix of clinicians and researchers that participated in the expert interviews, steering committee, and modified Delphi rounds represented the specialties that commonly treat patients with ATTR, including cardiology, neurology, gastroenterology, internal medicine, and hematology/oncology. The drug developers who also reviewed the questionnaire provided insights relevant to their treatments, whether they treat neuropathies or cardiac manifestations, and experience with regulatory bodies.
Much of the research in ATTR has approached the types (hATTR and ATTRwt) and subtypes (hATTR-CM and hATTR-PN) as distinct from one another, as evidenced by two other ATTR-specific PRO measures created during the course of this study.21,22 The decision to create a single measure that addresses symptoms and impacts across both types and avoids categorizing patients a priori (by type or subtype) was the result of listening closely to patients and experts. Patient input showed the heterogeneity of the symptoms and impacts experienced by those living with ATTR, regardless of type. Expert input confirmed that dividing hATTR patients by subtype (ie, primarily polyneuropathy or cardiomyopathy) and characterizing them by mutually exclusive sets of symptoms can often result in missed information. This finding is in line with research from Damy et al,32 who, in their effort to create a core dataset for hATTR, emphasize the importance of capturing all symptoms, regardless of the organ system, and Wajnsztajn et al and Sabbour et al who have identified polyneuropathy among patients with ATTRwt (typically thought to manifest as only cardiomyopathy).33–35 By including a set of items for use across types, the ATTR-QOL can better capture the true variability and “constellation of symptoms” that characterize ATTR, giving clinicians a more complete picture of their patients and researchers a more complete understanding of the overlaps between types while also reducing the reporting burden and standardizing data collection.
The ATTR-QOL that resulted from this study will undergo psychometric testing with a large group of patients with ATTR (hATTR and ATTRwt) to further refine the measure. Doing so will help to identify items that are redundant (ie, provide the same information, statistically) or do not provide sufficient information—and thus, should be removed to improve the performance of the measure—establish appropriate scales for the measure, and evaluate instrument’s measurement properties.
Acknowledgments
The authors would like to acknowledge the patients and experts who participated in this research. Interim results from the research to develop the ATTR-QOL were shared as poster presentations at the 2020 and 2022 International Society of Amyloidosis (ISA) conferences (available in the ISA abstract books at https://amyloid.memberclicks.net/assets/docs/Libro_ISA(1).pdf and https://www.isaamyloidosis.org/assets/docs/ISA22_Abstract%20Book_final.pdf respectively, and the ARC website at https://arciorg.wpengine.com/wp-content/uploads/2020/02/PRO-poster.pdf), and oral presentations at the 3rd European ATTR Amyloidosis Meeting (Euro TTR, 2021) and 2022 International Society for Quality of Life Research (ISOQOL) conferences (ISOQOL available in Quality of Life Research at https://link.springer.com/article/10.1007/s11136-022-03257-1).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding for this research study was provided by the Amyloidosis Research Consortium thanks to contributions from Ionis (Akcea), Alnylam, and Pfizer and in-kind contributions from Prothena.
Disclosure
KH, SR, and IL are employees of ARC and they also report grants from Alnylam, Akcea, and Pfizer to ARC, during the conduct of the study; In addition, KH reports that the instrument ATTR-QOL used is an intellectual property owned by ARC, and will be licensed for a fee to recoup costs. MO′C, LB, KL, KLM, and MC are employees of QualityMetric Inc (QM), which received funding from ARC to conduct the study. The authors report no other conflicts of interest in this work.
References
1. Cleveland Clinic. Amyloidosis: ATTR; 2019. Available from: https://my.clevelandclinic.org/health/diseases/17855-amyloidosis-attr.
2. Sekijima Y. Transthyretin (ATTR) amyloidosis: clinical spectrum, molecular pathogenesis and disease-modifying treatments. J Neurol Neurosurg Psychiatry. 2015;86(9):1036–1043. doi:10.1136/jnnp-2014-308724
3. Adams D, Koike H, Slama M, et al. Hereditary transthyretin amyloidosis: a model of medical progress for a fatal disease. Nat Rev Neurol. 2019;15(7):387–404. doi:10.1038/s41582-019-0210-4
4. Coelho T, Ericzon FR, et al. A guide to transthyretin amyloidosis; 2016.
5. Obi CA, Mostertz WC, Griffin JM, et al. ATTR epidemiology, genetics, and prognostic factors. Methodist DeBakey Cardiovasc J. 2022;18:17–26. doi:10.14797/mdcvj.1066
6. Maurer MS, Hanna M, Grogan M, et al. Genotype and phenotype of transthyretin cardiac amyloidosis: THAOS (Transthyretin Amyloid Outcome Survey). J Am Coll Cardiol. 2016;68(2):161–172. doi:10.1016/j.jacc.2016.03.596
7. Shije JZ, Bautista MAB, Smotherman C. The frequency of V122I transthyretin mutation in a cohort of African American individuals with bilateral carpal tunnel syndrome. Front Neurol. 2022;13:949401. doi:10.3389/fneur.2022.949401
8. Minnella AM, Rissotto R, Antoniazzi E, et al. Ocular involvement in hereditary amyloidosis. Genes. 2021:12. doi:10.3390/genes12070955
9. Sousa L, Coelho T, Taipa R. CNS involvement in hereditary transthyretin amyloidosis. Neurology. 2021;97(24):1111–1119. doi:10.1212/WNL.0000000000012965
10. Taipa R, Sousa L, Pinto M, et al. Neuropathology of central nervous system involvement in TTR amyloidosis. Acta Neuropathol. 2023;145(1):113–126. doi:10.1007/s00401-022-02501-9
11. Adams D, Suhr OB, Dyck PJ, et al. Trial design and rationale for APOLLO, a Phase 3, placebo-controlled study of patisiran in patients with hereditary ATTR amyloidosis with polyneuropathy. BMC Neurol. 2017;17(1):181. doi:10.1186/s12883-017-0948-5
12. Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis, prognosis, and therapy of transthyretin amyloidosis. J Am Coll Cardiol. 2015;66(21):2451–2466. doi:10.1016/j.jacc.2015.09.075
13. González-López E, Gagliardi C, Dominguez F, et al. Clinical characteristics of wild-type transthyretin cardiac amyloidosis: disproving myths. Eur Heart J. 2017;38(24):1895–1904. doi:10.1093/eurheartj/ehx043
14. Gertz MA. Hereditary ATTR amyloidosis: burden of illness and diagnostic challenges. Am J Manag Care. 2017;23:S107–S112.
15. Wixner J, Mundayat R, Karayal ON, et al. THAOS: gastrointestinal manifestations of transthyretin amyloidosis - common complications of a rare disease. Orphanet J Rare Dis. 2014;9(1):61. doi:10.1186/1750-1172-9-61
16. Coelho T, Maurer MS, Suhr OB. THAOS - the transthyretin amyloidosis outcomes survey: initial report on clinical manifestations in patients with hereditary and wild-type transthyretin amyloidosis. Curr Med Res Opin. 2013;29:63–76. doi:10.1185/03007995.2012.754348
17. Denoncourt RN, Adams D, Gonzalez-Duarte A, et al. Burden of illness for patients with hereditary attr amyloidosis with polyneuropathy begins with symptom onset and increases with disease progression. Value Health. 2016;19(7):A436. doi:10.1016/j.jval.2016.09.518
18. Grogan M, Dispenzieri A, Carlsson M, et al. Description of the health-related quality of life of transthyretin amyloid cardiomyopathy subjects from the transthyretin amyloidosis outcomes survey. J Card Fail. 2017;23(8):S102. doi:10.1016/j.cardfail.2017.07.298
19. Stewart M, Loftus J, Lenderking WR, et al. Characterizing disease burden in an ultra-rare disease in the United States: transthyretin (TTR) amyloidosis patients and caregivers. Value Health. 2013;16(7):A386. doi:10.1016/j.jval.2013.08.365
20. Amyloidosis research consortium advancing amyloidosis: a research roadmap. Available from: https://www.arci.org/wp-content/uploads/2019/03/ARC-White-Paper-Final-v3.pdf.
21. Aimo A, Rapezzi C, Perfetto F, et al. Quality of life assessment in amyloid transthyretin (ATTR) amyloidosis. Eur J Clin Invest. 2021;51(11):e13598. doi:10.1111/eci.13598
22. Rizio AA, Broderick LE, White MK, et al. Content validation of the ATTR amyloidosis patient symptom survey: findings from patient and clinician cognitive debriefing interviews. Patient Relat Outcome Meas. 2020;11:149–160. doi:10.2147/PROM.S264034
23. Patrick DL, Burke LB, Gwaltney CJ, et al. Content validity-establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO good research practices task force report: part 2–assessing respondent understanding. Value Health. 2011;14:978–988. doi:10.1016/j.jval.2011.06.013
24. Terwee CB, Prinsen CA, Chiarotto A, et al. COSMIN methodology for assessing the content validity of PROMs: user manual, version 1.0; 2018.
25. Crossnohere NL, Brundage M, Calvert MJ, et al. International guidance on the selection of patient-reported outcome measures in clinical trials: a review. Qual Life Res. 2021;30(1):21–40. doi:10.1007/s11136-020-02625-z
26. Willis G. Cognitive Interviewing. Thousand Oaks, California: SAGE Publications; 2005.
27. US Food and Drug Administration. Patient-focused drug development: collecting comprehensive and representative input: guidance for industry, food and drug administration staff, and other stakeholders; 2020. Available from: https://www.fda.gov/media/139088/download.
28. Patrick DL, Burke LB, Gwaltney CJ, et al. Content validity-establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO good research practices task force report: part 1-eliciting concepts for a new PRO instrument. Value Health. 2011;14:967–977. doi:10.1016/j.jval.2011.06.014
29. Cheng KKF, Clark AM. Qualitative methods and patient-reported outcomes. Int J Qual Methods. 2017;16(1):160940691770298. doi:10.1177/1609406917702983
30. US Food and Drug Administration. Guidance for industry patient-reported outcome measures: use in medical product development to support labeling claims; 2009. Available from: https://www.fda.gov/downloads/drugs/guidances/ucm193282.pdf.%20Updated%20March%2023,%202017.
31. US Food and Drug Administration. Patient-focused drug development guidance public workshop: methods to identify what is important to patients and select, develop or modify fit-for-purpose clinical outcomes assessments; 2018. Available from: https://www.fda.gov/downloads/Drugs/NewsEvents/UCM620708.pdf.
32. Damy T, Conceição I, García-Pavía P, et al. A simple core dataset and disease severity score for hereditary transthyretin (ATTRv) amyloidosis. Amyloid. 2021:1–10. doi:10.1080/13506129.2021.1931099
33. Wajnsztajn Yungher F, Kim A, Boehme A, et al. Peripheral neuropathy symptoms in wild type transthyretin amyloidosis. J Peripher Nerv Syst. 2020;25:265–272. doi:10.1111/jns.12403
34. Sabbour H, Hasan KY, Al Badarin F, et al. From clinical clues to final diagnosis: the return of detective work to clinical medicine in cardiac amyloidosis. Front Cardiovasc Med. 2021;8:644508. doi:10.3389/fcvm.2021.644508
35. O’Connor M, Broderick L, Brown D, et al. Comparison of symptoms experienced by patients with ATTRwt and hATTR: findings from the development of an ATTR-specific PRO.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.