Back to Journals » International Journal of General Medicine » Volume 19
The Predictive Value of the Pan-Immune-Inflammation Value for Atrial Fibrillation Risk in Patients with Coronary Artery Disease: A Multicenter Machine Learning Study
Received 4 November 2025
Accepted for publication 22 January 2026
Published 29 January 2026 Volume 2026:19 579135
DOI https://doi.org/10.2147/IJGM.S579135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Ke He,1 Jinbo Zhao,2 Changjiang Zhang1
1Department of Cardiology, Minda Hospital of Hubei Minzu University, Enshi, Hubei, People’s Republic of China; 2Cardiovascular Disease Center, Central Hospital of Tujia and Miao Autonomous Prefecture, Hubei University of Medicine, Enshi, Hubei, People’s Republic of China
Correspondence: Changjiang Zhang, Email [email protected]
Background: Atrial fibrillation (AF) is a common arrhythmia among patients with coronary heart disease (CHD), and inflammatory response plays a key role in its pathogenesis. The pan-immune-inflammation value (PIV), a novel composite marker reflecting systemic inflammation, has not been fully investigated for its predictive value in AF among CHD patients.
Methods: This multicenter retrospective study enrolled patients diagnosed with CHD by coronary angiography from two tertiary hospitals. Participants were categorized into AF and non-AF groups. Clinical characteristics and laboratory data were collected. Feature selection was performed using multivariate logistic regression, and significant predictors were incorporated into two models: extreme gradient boosting (XGBoost) and multilayer perceptron (MLP). Model performance was evaluated by area under the ROC curve (AUC) and calibration analysis. Model interpretability was assessed using SHAP (SHapley Additive exPlanations) values, and partial dependence plots (PDPs) were applied to explore variable interactions.
Results: Compared with the non-AF group, the AF group had significantly higher levels of PIV, age, AST, WBC, and TBIL. Logistic regression identified PIV, age, and diabetes as independent predictors of AF, while sex, left main coronary artery disease (LM), and AST showed borderline significance. The XGBoost model achieved superior performance (AUC = 0.79 in training and 0.73 in testing) compared to the MLP model (AUC = 0.75 and 0.69, respectively), with better calibration consistency. SHAP analysis indicated that PIV was the most influential feature, with higher values associated with increased AF risk. PDPs further demonstrated synergistic effects between PIV and other key variables.
Conclusion: PIV is a valuable predictor of AF in CHD patients. The XGBoost model outperformed the deep learning model in this context and may serve as a robust tool for individualized AF risk assessment.
Keywords: atrial fibrillation, coronary heart disease, pan-immune-inflammation value, XGBoost, deep learning
Background
Atrial fibrillation (AF) is one of the most common sustained arrhythmias in clinical practice, affecting over 30 million individuals worldwide.1 With the ongoing aging of the population and the high prevalence of cardiovascular diseases, its incidence is expected to rise further.2 AF significantly increases the risk of stroke, heart failure, and all-cause mortality, and poses a substantial burden on healthcare systems.3 Coronary artery disease (CAD) is a frequent comorbidity of AF, and growing evidence highlights the bidirectional relationship between the two. CAD may contribute to the onset and persistence of AF through mechanisms such as myocardial ischemia, increased left atrial pressure, and structural or electrical remodeling.4–6 Conversely, AF may worsen myocardial oxygen demand and exacerbate ischemia, creating a detrimental cycle.7
AF and CAD share several common risk factors, including advanced age, hypertension, diabetes, metabolic disturbances, and chronic inflammation.8,9 In recent years, inflammation has been recognized as a central contributor to both the initiation and progression of CAD and AF.10 It promotes atrial fibrosis, electrophysiological abnormalities, and autonomic remodeling, thereby facilitating the development and maintenance of AF.11,12 The pan-immune-inflammation value (PIV) is a novel composite biomarker derived from neutrophil, monocyte, lymphocyte, and platelet counts, designed to reflect the systemic immune-inflammatory burden.13 PIV has demonstrated predictive value in various disease settings, but its utility in identifying AF risk among patients with CAD remains unclear.
Traditional AF risk models often rely on linear statistical methods, which may fail to capture the complex, nonlinear interactions among clinical variables. In contrast, machine learning (ML) approaches have shown promise in medical prediction tasks, particularly in modeling high-dimensional data, identifying nonlinear relationships, and enabling personalized risk stratification. Therefore, this study aims to evaluate the predictive value of PIV for AF among patients with CAD, leveraging ML algorithms to enhance early identification of individuals at elevated risk.
Methods
Study Population
This retrospective cohort study enrolled hospitalized patients from two medical centers: Enshi Tujia and Miao Autonomous Prefecture Central Hospital and Minda Hospital of Hubei Minzu University. The inclusion period spanned from June 2024 to June 2025. Eligible participants were those undergoing coronary angiography confirmed to have CAD, defined as ≥50% stenosis in at least one major coronary artery. Patients with a history of percutaneous coronary intervention, coronary artery bypass grafting, myocardial infarction, or pre-existing AF were excluded. The patient selection process is illustrated in Figure 1. This study was approved by the Ethics Committee of Enshi Tujia and Miao Autonomous Prefecture Central Hospital (approval number: 202405201). All data were extracted from the electronic medical record system and fully anonymized prior to analysis. No personally identifiable information was accessed. Given the retrospective nature of the study, the requirement for informed consent was waived in accordance with the Declaration of Helsinki.
 |
Figure 1 Flowchart of the study. |
Data Collection
Collected variables included demographics (age, sex), comorbidities (hypertension, diabetes, stroke, dyslipidemia), smoking history, coronary artery involvement (left main [LM], left anterior descending [LAD], left circumflex [LCX], right coronary artery [RCA], and multi-vessel disease), and admission heart rate. Laboratory tests included hematologic indices: white blood cell (WBC) count, neutrophil, lymphocyte, monocyte, platelet counts, hemoglobin, and platelet distribution width (PDW); liver function tests: alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), and direct bilirubin (DBIL); and metabolic/renal parameters: serum creatinine (Cr), fasting blood glucose (Glu), uric acid (UA), total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL), and low-density lipoprotein (LDL). The PIV was calculated as (neutrophil count × platelet count × monocyte count) / lymphocyte count.13
Feature Selection
To enhance model performance and reduce redundancy, we conducted feature selection prior to model building. All clinical and laboratory variables were initially included in a multivariate logistic regression model using the enter method. Variables with p-values < 0.1 were retained, while those with poor association or multicollinearity were excluded. The selected features were subsequently used in predictive modeling.
Model Development, Evaluation, and Interpretation
The selected variables were randomly divided into training (70%) and testing (30%) sets. Two predictive models were developed: Extreme Gradient Boosting (XGBoost) and Multilayer Perceptron (MLP). Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC), and calibration was evaluated with calibration plots comparing predicted probabilities with observed outcomes. The model with superior performance was selected for further interpretability analysis. We applied SHapley Additive exPlanations (SHAP) to interpret the final model. SHAP summary plots and bar plots were generated to assess the magnitude and direction of each feature’s contribution to the model output. SHAP decision plots were used to visualize the cumulative contribution of each variable in individual predictions, illustrating how risk estimates evolved from the model’s baseline output. Additionally, SHAP interaction analysis and contour-based partial dependence plots (PDPs) were constructed to explore potential synergistic effects between key features.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD) if normally distributed and compared using independent-samples t-tests. For non-normally distributed data, medians and interquartile ranges (IQRs) were reported and compared via the Mann–Whitney U-test. Categorical variables were presented as counts and percentages, and compared using Chi-square or Fisher’s exact test as appropriate. A two-sided p-value < 0.05 was considered statistically significant. All analyses were performed using Python (version 3.9) and R (version 4.3.2).
Results
Baseline Characteristics
A total of 3,831 patients were included in this study, of whom 3,380 were in the non-atrial fibrillation (non-AF) group and 451 in the AF group, as shown in Table 1. Compared to the non-AF group, the AF group had a significantly higher proportion of male patients, as well as a greater prevalence of LM, LAD, RCA, and multi-vessel coronary artery disease. In terms of laboratory parameters, the AF group exhibited significantly elevated levels of WBC count, PIV, AST, TBIL, DBIL, serum Cr, and UA. PDW and ALT also showed statistically significant differences. No significant intergroup differences were observed in the prevalence of hypertension, diabetes, stroke history, dyslipidemia, smoking status, LCX involvement, fasting glucose, total cholesterol, triglycerides, HDL, or LDL.
 |
Table 1 Baseline Characteristics of the Study Participants |
Feature Selection
As summarized in Table 2, multivariate logistic regression was performed for feature selection. Diabetes, age, and PIV were identified as independent predictors of AF. Additionally, gender, LM disease, and AST showed marginal statistical significance, suggesting potential relevance to AF risk, and were therefore retained for subsequent model development.
 |
Table 2 Multivariable Logistic Regression Analysis |
Model Comparison and Interpretation
Based on the selected features, we constructed two models: an XGBoost classifier and a MLP neural network. As depicted in Figure 2, the XGBoost model achieved AUC values of 0.79 and 0.73 for the training and testing sets, respectively. In comparison, the MLP model achieved slightly lower AUCs of 0.75 and 0.69 (Figure 3). The calibration curve indicated better agreement between predicted and observed outcomes in the XGBoost model, reflecting superior calibration. Consequently, XGBoost was selected as the optimal predictive model for further interpretability analysis. To further elucidate how individual features influenced model predictions, we employed SHAP to interpret the final XGBoost model.
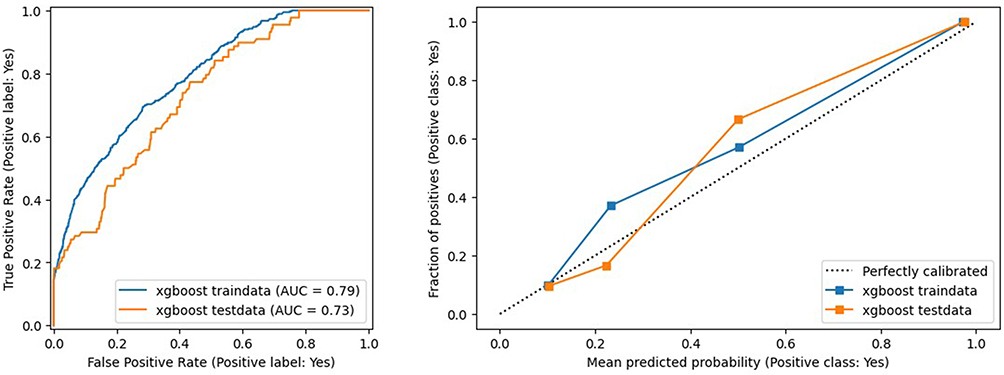 |
Figure 2 ROC curve and calibration plot of the XGBoost model. |
 |
Figure 3 ROC curve and calibration plot of the MLP model. |
The SHAP summary plot (Figure 4a) illustrated the distribution of SHAP values for each feature across all samples. The x-axis indicates each feature’s impact on model output, while color represents feature magnitude (red for high, blue for low). PIV was identified as the most influential predictor, showing consistently positive contributions to AF risk. Other important features included age, diabetes, AST, gender, and LM disease, most of which also had positive associations with the predicted outcome. The SHAP bar plot (Figure 4b) showed the mean absolute SHAP values for each variable, confirming the top six contributors to be PIV, age, diabetes, AST, gender, and LM involvement. This further supports the validity of the feature selection process and its clinical relevance. The SHAP decision plot (Figure 4c) visualized individual trajectories from the base value to final predicted probabilities. Cases with high PIV values showed strong upward contributions to risk, with age and diabetes often acting synergistically.
 |
Figure 4 (a) Feature attributes in SHAP; (b) SHAP-based feature importance ranking; (c) SHAP force plot. |
To explore interactions between PIV and other clinical variables, two-dimensional PDPs were generated (Figure 5), examining PIV in combination with age, gender, diabetes, AST, and LM disease. Contour lines indicate predicted AF probability, with lighter shades representing higher risk. Overall, increasing PIV levels were positively associated with elevated AF risk, across multiple clinical subgroups.
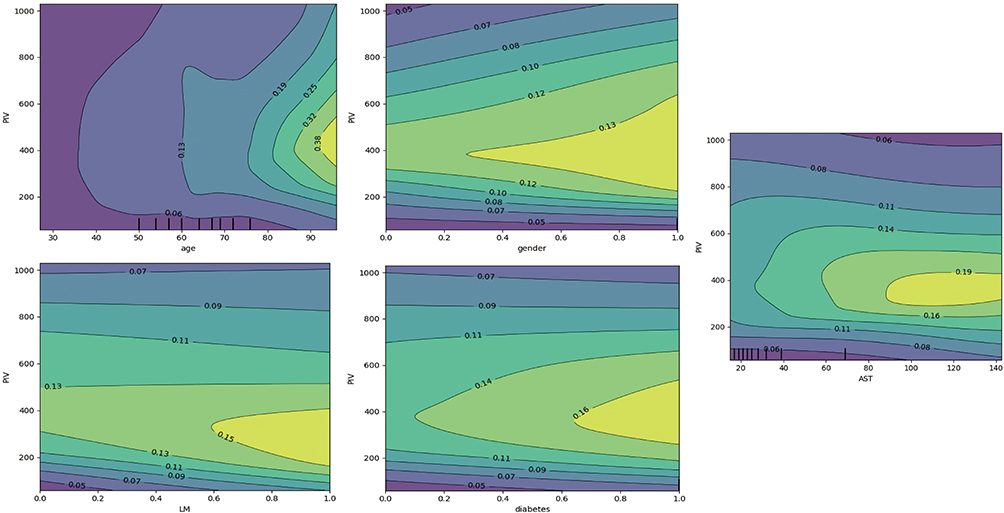 |
Figure 5 PDP-based interaction analysis between PIV and other features. |
Discussion
Through multivariate logistic regression analysis, we identified several variables significantly associated with AF, including the PIV, age, and diabetes. Based on these selected features, we developed two predictive models: an XGBoost algorithm and a MLP neural network. The XGBoost model demonstrated superior performance in both discriminative ability (AUC) and calibration compared to the MLP. Further interpretation using SHAP revealed that PIV was the most influential variable in the XGBoost model, contributing positively to AF risk. Other predictors such as age, diabetes, AST, gender, and left main coronary artery disease also played meaningful roles. PDPs indicated synergistic interactions between PIV and other clinical features in elevating AF risk.
As a composite marker incorporating neutrophils, monocytes, platelets, and lymphocytes, PIV reflects the systemic immune-inflammatory status. Its prognostic value has been reported in diverse conditions, including post-operative AF after off-pump coronary artery bypass grafting (CABG),14 both reduced and preserved ejection fraction heart failure,15 and multiple malignancies.16,17 PIV has also been associated with adverse cardiovascular outcomes and has shown predictive value in various cardiovascular and metabolic conditions.18,19 Large-scale cohort studies have further suggested that elevated PIV is associated with increased all-cause and cause-specific mortality in the general population.20 However, its role in predicting AF among CAD patients has not been thoroughly investigated. This study is the first to systematically evaluate PIV as a risk factor for AF in a CAD population and to confirm its central importance through interpretable machine learning.
Pro-inflammatory cell types, including neutrophils, monocytes, and platelets, play pivotal roles in AF pathogenesis.21–23 Neutrophils contribute to oxidative stress and atrial fibrosis through the release of reactive oxygen species and cytokines.24,25 Monocytes secrete inflammatory mediators like TNF-α and IL-6, promoting tissue remodeling.26 Platelets, beyond their hemostatic function, release PF4 and TGF-β, which activate immune cells and endothelial responses, exacerbating local inflammation.27,28 In contrast, lymphocytes—particularly T cells—act as immune regulators.29 A decline in lymphocyte counts often reflects immune dysregulation and is closely associated with increased AF risk.30 PIV integrates these four cell types into a single metric, offering a comprehensive reflection of the body’s inflammatory-immune imbalance. In addition to systemic inflammation, several clinical and structural factors contribute to atrial fibrillation, including right coronary artery involvement, hypertension, and structural heart disease, which promote atrial remodeling and AF persistence. Accumulating evidence indicates that inflammation and endothelial dysfunction are central drivers of AF initiation and progression, particularly in patients with coronary artery disease. Chronic inflammatory activation and endothelial injury synergistically promote atrial electrical instability and fibrosis, providing a mechanistic basis for the use of PIV as an integrated inflammatory biomarker in AF risk stratification.31–33
Although these factors were not systematically incorporated into the present analysis, they may interact with inflammatory activity and endothelial dysfunction to jointly facilitate atrial electrical and structural remodeling. Future prospective studies integrating PIV with structural and hemodynamic parameters are warranted.
Interestingly, we found that the XGBoost model outperformed the MLP model in both training and testing sets (AUCs of 0.79 and 0.73 vs 0.75 and 0.69, respectively), suggesting that traditional machine learning algorithms may outperform deep learning models in this setting. This could be attributed to XGBoost’s ability to handle structured tabular data with small-to-moderate sample sizes effectively. In contrast, MLP requires larger datasets and tends to overfit when applied to limited samples. XGBoost also benefits from built-in regularization, automatic feature selection, and better interpretability, making it more practical for clinical use. MLP, being a “black-box” model, lacks transparency, limiting its application in medical decision-making. These factors may explain the robust performance of XGBoost in our study.
Limitations
Several limitations should be acknowledged. First, the study employed a retrospective, dual-center design, which may introduce selection and information bias and limits causal inference. Second, the data were collected at a single time point during initial hospitalization, with no dynamic tracking of inflammatory markers or long-term follow-up, preventing assessment of AF progression or prognosis. Third, although SHAP was used to enhance model interpretability, external validation in prospective, multicenter cohorts is needed to evaluate model generalizability. Finally, some potential confounding factors, such as medication use and certain comorbidities, were not fully accounted for, which may have influenced both PIV levels and AF risk.
Conclusion
This study is the first to evaluate the predictive utility of the PIV for atrial fibrillation in patients with coronary artery disease. Our findings indicate that PIV is an independent and strong predictor of AF. The XGBoost model outperformed deep learning in this setting, providing accurate, well-calibrated, and interpretable predictions. These results highlight the potential of integrating inflammatory markers and machine learning for early risk stratification of AF in CAD populations. From a pathophysiological perspective, these findings further support the central role of systemic inflammation and immune–endothelial dysfunction in atrial remodeling and AF development.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The study was approved by the Ethics Committee of Enshi Tujia and Miao Autonomous Prefecture Central Hospital (Approval No. 202405201).
Acknowledgments
The authors gratefully acknowledge Miss Ling Hou for her early contributions to the conceptual development of this study. She did not participate in the revision, rewriting, or approval of the current version of the manuscript submitted to the International Journal of General Medicine. In accordance with ICMJE authorship criteria, she voluntarily withdrew from authorship and has consented to be acknowledged instead.
Funding
This work was supported by the Natural Science Foundation of Hubei Province (No. JCZRYB202501509).
Disclosure
The authors declare no competing interests in this work.
References
1. Kornej J, Börschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. 2020;127(1):4–9. doi:10.1161/circresaha.120.316340
2. Segan L, Ho Ho WW, Crowley R, et al. Combining polygenic and clinical risk scores in atrial fibrillation risk prediction: implications for population screening. Heart Rhythm. 2025. doi:10.1016/j.hrthm.2025.04.032
3. Niiranen TJ, Schnabel RB, Schutte AE, et al. Hypertension and atrial fibrillation: a frontier review from the AF-SCREEN international collaboration. Circulation. 2025;151(12):863–877. doi:10.1161/circulationaha.124.071047
4. Madsen S, Kjaerulff MLG, Ejlersen JA, et al. Guiding early revascularization using [15O]H2O positron emission tomography myocardial perfusion imaging: impact of atrial fibrillation. Eur Heart J Cardiovasc Imaging. 2024;25(7):958–967. doi:10.1093/ehjci/jeae043
5. Pandey AC, Bidaoui G, Younes H, Tsakiris E, Marrouche NF. The senescent heart and atrial fibrillation. Heart Rhythm. 2025. doi:10.1016/j.hrthm.2025.06.005
6. Vickneson K, Gharaviri A, Vigneswaran V, et al. Peri-atrial adipose tissue inflammation in atrial fibrillation: quantification of electrophysiological effects using electroanatomic mapping. JACC Clin Electrophysiol. 2025. doi:10.1016/j.jacep.2025.04.023
7. Frederiksen TC, Dahm CC, Preis SR, et al. The bidirectional association between atrial fibrillation and myocardial infarction. Nat Rev Cardiol. 2023;20(9):631–644. doi:10.1038/s41569-023-00857-3
8. Mekhael M, Marrouche N, Hajjar AHE, Donnellan E. The relationship between atrial fibrillation and coronary artery disease: understanding common denominators. Trends Cardiovasc Med. 2024;34(2):91–98. doi:10.1016/j.tcm.2022.09.006
9. Zheng Y, He JQ. Common differentially expressed genes and pathways correlating both coronary artery disease and atrial fibrillation. Excli J. 2021;20:126–141. doi:10.17179/excli2020-3262
10. Natorska J, Ząbczyk M, Undas A. Neutrophil extracellular traps (NETs) in cardiovascular diseases: from molecular mechanisms to therapeutic interventions. Kardiol Pol. 2023;81(12):1205–1216. doi:10.33963/v.kp.98520
11. Osmancik P, Bacova B, Hozman M, et al. Myocardial damage, inflammation, coagulation, and platelet activity during catheter ablation using radiofrequency and pulsed-field energy. JACC Clin Electrophysiol. 2024;10(3):463–474. doi:10.1016/j.jacep.2023.11.001
12. Roy A, O’Shea C, Dasí A, et al. Early atrial remodeling drives arrhythmia in fabry disease. Circ Arrhythm Electrophysiol. 2025;18(7):e013352. doi:10.1161/circep.124.013352
13. Su Z, Cao L, Chen H, et al. Obesity indicators mediate the association between the aggregate index of systemic inflammation (AISI) and type 2 diabetes mellitus (T2DM). Lipids Health Dis. 2025;24(1):176. doi:10.1186/s12944-025-02589-4
14. Dolapoglu A, Avci E. Relationship between pan-immune- inflammation value and in major cardiovascular and cerebrovascular events in stable coronary artery disease patients undergoing on-pump coronary artery bypass graft surgery. J Cardiothorac Surg. 2024;19(1):241. doi:10.1186/s13019-024-02691-1
15. Dervis E, Yakut I, Inan D. The prognostic significance of the pan-immune-inflammation value in patients with heart failure with reduced ejection fraction. Diagnostics. 2025;15(13). doi:10.3390/diagnostics15131617
16. Ucar MA, Tombak A, Akdeniz A, et al. Immune and inflammation markers as a predictor of overall survival in patients with hematologic malignancies: a retrospective cohort study. Medicina. 2025;61(6). doi:10.3390/medicina61061019
17. D’Indinosante M, Guidi G, Giannarelli D, et al. Laparoscopic tumor load as an independent prognostic marker in advanced ovarian cancer: a 3-year cohort study. Int J Gynecol Cancer. 2025;35(8):101965. doi:10.1016/j.ijgc.2025.101965
18. Zhou Q, Xue J, Hao L. Pan-immune-inflammation value and mortality in the US adult MASLD: a nonlinear NHANES analysis. BMC Gastroenterol. 2025;25(1):460. doi:10.1186/s12876-025-04064-x
19. Mohammed AQ, Liu L, Alifu J, et al. Association of novel inflammatory and metabolic markers with mortality in individuals with overweight and obesity. Nutr Metab Cardiovasc Dis. 2025;35(3):103859. doi:10.1016/j.numecd.2025.103859
20. Zhang Y, Yue Y, Sun Z, et al. Pan-immune-inflammation value and its association with all-cause and cause-specific mortality in the general population: a nationwide cohort study. Front Endocrinol. 2025;16:1534018. doi:10.3389/fendo.2025.1534018
21. Steinhubl SR, Eikelboom JW, Hylek EM, Dauerman HL, Smyth SS, Becker RC. Antiplatelet therapy in prevention of cardio- and venous thromboembolic events. J Thromb Thrombolysis. 2014;37(3):362–371. doi:10.1007/s11239-013-1023-8
22. Niskala A, Heijman J, Dobrev D, Jespersen T, Saljic A. Targeting the NLRP3 inflammasome signalling for the management of atrial fibrillation. Br J Pharmacol. 2024;181(24):4939–4957. doi:10.1111/bph.16470
23. Wu CL, Yin R, Wang SN, Ying R. A review of CXCL1 in cardiac fibrosis. Front Cardiovasc Med. 2021;8:674498. doi:10.3389/fcvm.2021.674498
24. He L, Liu R, Yue H, et al. Interaction between neutrophil extracellular traps and cardiomyocytes contributes to atrial fibrillation progression. Signal Transduct Target Ther. 2023;8(1):279. doi:10.1038/s41392-023-01497-2
25. Rodríguez-Espinosa O, Rojas-Espinosa O, Moreno-Altamirano MM, López-Villegas EO, Sánchez-García FJ. Metabolic requirements for neutrophil extracellular traps formation. Immunology. 2015;145(2):213–224. doi:10.1111/imm.12437
26. Sun L, Li H, Li X, et al. Dysregulation of immune cells and platelet-monocyte aggregates in chronic thromboembolic pulmonary hypertension. Respir Res. 2025;26(1):245. doi:10.1186/s12931-025-03284-9
27. Schroer AB, Ventura PB, Sucharov J, et al. Platelet factors attenuate inflammation and rescue cognition in ageing. Nature. 2023;620(7976):1071–1079. doi:10.1038/s41586-023-06436-3
28. Rachidi S, Metelli A, Riesenberg B, et al. Platelets subvert T cell immunity against cancer via GARP-TGFβ axis. Sci Immunol. 2017;2(11). doi:10.1126/sciimmunol.aai7911
29. Huang S, Kang Y, Liu T, Xiong Y, Yang Z, Zhang Q. The role of immune checkpoints PD-1 and CTLA-4 in cardiovascular complications leading to heart failure. Front Immunol. 2025;16:1561968. doi:10.3389/fimmu.2025.1561968
30. Liu Z, Nguyen Khuong J, Borg Caruana C, et al. The prognostic value of elevated perioperative neutrophil-lymphocyte ratio in predicting postoperative atrial fibrillation after cardiac surgery: a systematic review and meta-analysis. Heart Lung Circ. 2020;29(7):1015–1024. doi:10.1016/j.hlc.2019.11.021
31. Batta A, Hatwal J, Batta A, Verma S, Sharma YP. Atrial fibrillation and coronary artery disease: an integrative review focusing on therapeutic implications of this relationship. World J Cardiol. 2023;15(5):229–243. doi:10.4330/wjc.v15.i5.229
32. Batta A, Hatwal J, Panda P, Sharma Y, Wander GS, Mohan B. Impact of initial high sensitivity C-reactive protein on outcomes in nonvalvular atrial fibrillation: an observational study. Future Cardiol. 2024;20(5–6):295–303. doi:10.1080/14796678.2024.2354110
33. Nso N, Bookani KR, Metzl M, Radparvar F. Role of inflammation in atrial fibrillation: a comprehensive review of current knowledge. J Arrhythm. 2021;37(1):1–10. doi:10.1002/joa3.12473
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Large Burden of Stroke Incidence in People with Cardiac Disease: A Linked Data Cohort Study
Robinson K, Katzenellenbogen JM, Kleinig TJ, Kim J, Budgeon CA, Thrift AG, Nedkoff L
Clinical Epidemiology 2023, 15:203-211
Published Date: 18 February 2023
Development of a Nomogram That Predicts the Risk of Atrial Fibrillation in Patients with Coronary Heart Disease
Cao X, Sun Y, Chen Y, Tang C, Yu H, Li X, Gu Z
Risk Management and Healthcare Policy 2024, 17:1815-1826
Published Date: 9 July 2024
Nomogram Model for Identifying the Risk of Coronary Heart Disease in Patients with Chronic Obstructive Pulmonary Disease Based on Deep Learning Radiomics and Clinical Data: A Multicenter Study
Bian H, Qian H, Zhu S, Xue J, Qi L, Peng X, Li M, Zheng Y, Xu P, Zhao H, Jiang J
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3045-3057
Published Date: 2 September 2025
Machine Learning Models for Identifying the Risk of Chronic Kidney Disease in Patients with Coronary Heart Disease: A Retrospective Study
He T, Zhao J, Hou L, Su K, Li Y
International Journal of General Medicine 2025, 18:7327-7340
Published Date: 5 December 2025
Development and Validation of an Explainable Machine Learning Model for Predicting Repeat Catheter Ablation for Atrial Fibrillation: A Single-Center Retrospective Cohort Study
Shang S, Lv H, Ma G, Wei M, Wang K, Lu Y, Tang B
International Journal of General Medicine 2026, 19:574069
Published Date: 23 March 2026